
Orientation
Biofeedback training (BFT) and neurofeedback training (NFT) involve the same learning processes we use to develop motor skills or master a videogame. An individual acts (breathes effortlessly), observes the results (heart rate variability increases), and repeats this action during meetings with clients. Clients actively learn to regulate their psychophysiology (Thompson & Thompson, 2016).
Biofeedback is also a "psychophysiological mirror" that teaches individuals to monitor, understand, and change their physiology (Peper, Shumay, & Moss, 2012). Graphic © 1979 Erik Peper.
NFT is a branch of BFT that provides real-time displays using an electroencephalograph (EEG), as opposed to an electromyograph (EMG), heart rate variability (HRV), skin temperature, or other psychophysiological measures. An electroencephalograph monitors brain electrical activity (e.g., brainwaves), while an electromyograph detects muscle action potentials from skeletal muscles. These modalities differ in the signals they detect, process, and display (Collura, 2014).
The Process of Neurofeedback
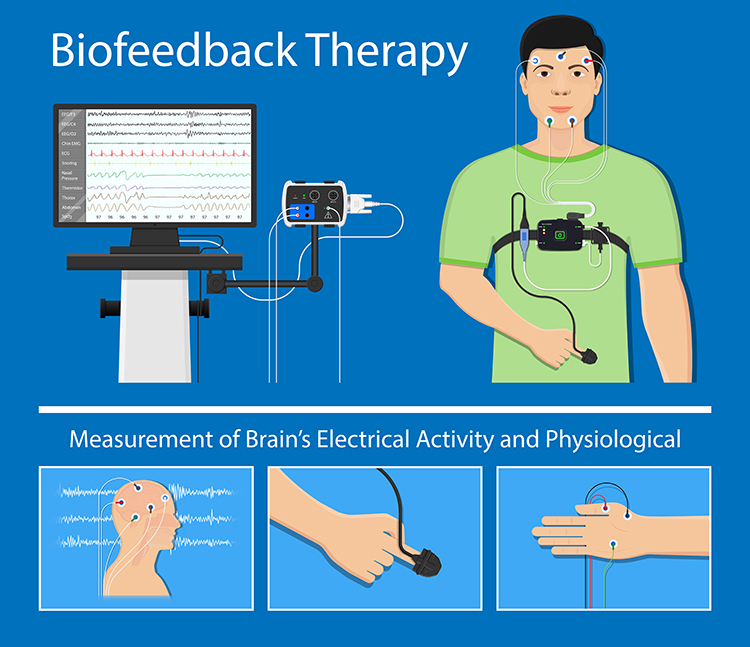
Neurofeedback is the process of interacting with an electronic device that measures and feeds back information about brain electrical activity.
The goals of this process are to:
(1) ensure correct regulatory function in the brain's neuromodulating systems
(2) encourage global neuropsychophysiological change
(3) correct specific, distinct, identifiable disorders or barriers to optimal performance that result from underlying dysregulation
(4) enhance performance by optimizing nervous system functioning
What Neurofeedback Does
(1) Neurofeedback provides accurate, timely, and helpful information to the client in the form of visual, auditory, or tactile feedback that responds to meaningful changes in monitored neuronal systems
(2) Neurofeedback training promotes flexibility, resilience, and choice
Click on the link to view Neurofeedback Overview, produced by the International Society for Neuroregulation and Research (ISNR). Graphic © ibreakstock/Shutterstock.com.

BFT may be more effective when training promotes mindfulness. A mindfulness approach teaches clients to focus on their immediate feelings, cognitions, and sensations in an accepting and non-judgmental way, to distinguish between what can and cannot be changed, and to change the things they can (Khazan, 2013).
Clients can become stuck when they focus on outcomes they cannot immediately control. For example, James, an undergraduate Psychology major, was diagnosed with ADHD. For example, James, an undergraduate Psychology major, was diagnosed with ADHD. When he ruminated about his mistakes on daily quizzes, this undermined his motivation to study and resulted in lower scores. He could not study while he worried about his quiz performance. When James learned to accept occasional mistakes without fear, his studying and course grade improved. James succeeded by changing what he could: his reaction to unavoidable errors. Graphic © Ivelin Radkov/Shutterstock.com

MCP Blueprint Coverage
This unit addresses I. Orientation to Neurofeedback (1 hour). This unit covers Definitions of Neurofeedback, History and Development of Neurofeedback, Overview of Principles of Human Learning as They Apply to Neurofeedback, and Assumptions Underlying Neurofeedback.
A. DEFINITIONS OF BIOFEEDBACK AND NEUROFEEDBACK

This section covers covers Definitions of Biofeedback and Neurofeedback, Physiological Monitoring and Modulation Are Not Biofeedback, and Quantum Biofeedback and LenyosisTM.
Since neurofeedback is a specialized application of biofeedback, we will start with the Biofeedback Alliance and Nomenclature Task Force definition (Schwartz, 2010).
Biofeedback Alliance and Nomenclature Task Force (2008)
Biofeedback is a process that enables an individual to learn how to change physiological activity for the purposes of improving health and performance. Precise instruments measure physiological activity such as brainwaves, heart function, breathing, muscle activity, and skin temperature. These instruments rapidly and accurately 'feed back' information to the user. The presentation of this information — often in conjunction with changes in thinking, emotions, and behavior — supports desired physiological changes. Over time, these changes can endure without continued use of an instrument.The main elements of this definition are that (1) biofeedback is a learning process that teaches an individual to control her physiological activity, (2) biofeedback training aims to improve health and performance, (3) instruments rapidly monitor an individual's performance and display it back to them, (4) the individual uses this feedback to produce physiological changes, (5) changes in thinking, emotions, and behavior often accompany and reinforce physiological changes, and (6) these changes become independent of external feedback from instruments. Graphic © rumruay/Shutterstock.com.
The Biofeedback Certification International Alliance (BCIA) emphasized that neurofeedback is a form of biofeedback in its Blueprint of Knowledge.
Biofeedback Certification International Alliance (2016) definition of neurofeedback
Neurofeedback is employed to modify the electrical activity of the CNS, including EEG, event-related potentials, slow cortical potentials and other electrical activity either of subcortical or cortical origin. Neurofeedback is a specialized application of biofeedback of brainwave data in an operant conditioning paradigm. The method is used to treat clinical conditions as well as to enhance performance.
The International Society for Neurofeedback and Research (ISNR) provided a comprehensive definition of neurofeedback that described the similarities and differences between neurofeedback and biofeedback.
International Society for Neurofeedback and Research (2010) definition of neurofeedback
Like other forms of biofeedback, NFT uses monitoring devices to provide moment-to-moment information to an individual on the state of their physiological functioning. The characteristic that distinguishes NFT from other biofeedback is a focus on the central nervous system and the brain. Neurofeedback training (NFT) has its foundations in basic and applied neuroscience as well as data-based clinical practice. It takes into account behavioral, cognitive, and subjective aspects as well as brain activity.This definition was ratified by the ISNR Board of Directors on January 10, 2009, and edited on June 11, 2010. It emphasizes that neurofeedback is a "self-regulation method" that teaches clients to voluntarily change central nervous system activity. It draws a sharp distinction between neurofeedback and neuromodulatory approaches like audio-visual entrainment (AVE) and rTMS that alter the brain by exposing it to a stimulus. While these are potentially valuable adjunctive procedures, they do not provide feedback of brain activity nor teach self-regulation.
NFT is preceded by an objective assessment of brain activity and psychological status. During training, sensors are placed on the scalp and then connected to sensitive electronics and computer software that detect, amplify, and record specific brain activity. Resulting information is fed back to the trainee virtually instantaneously with the conceptual understanding that changes in the feedback signal indicate whether or not the trainee's brain activity is within the designated range. Based on this feedback, various principles of learning and practitioner guidance, changes in brain patterns occur and are associated with positive changes in physical, emotional, and cognitive states. Often the trainee is not consciously aware of the mechanisms by which such changes are accomplished although people routinely acquire a 'felt sense' of these positive changes and often are able to access these states outside the feedback session.
NFT does not involve either surgery or medication and is neither painful nor embarrassing. When provided by a licensed professional with appropriate training, generally trainees do not experience negative side-effects. Typically trainees find NFT to be an interesting experience. Neurofeedback operates at a brain functional level and transcends the need to classify using existing diagnostic categories. It modulates the brain activity at the level of the neuronal dynamics of excitation and inhibition which underlie the characteristic effects that are reported.
Research demonstrates that neurofeedback is an effective intervention for ADHD and Epilepsy. Ongoing research is investigating the effectiveness of neurofeedback for other disorders such as Autism, headaches, insomnia, anxiety, substance abuse, TBI and other pain disorders, and is promising.
Being a self-regulation method, NFT differs from other accepted research-consistent neuro-modulatory approaches such as audio-visual entrainment (AVE) and repetitive transcranial magnetic stimulation (rTMS) that provoke an automatic brain response by presenting a specific signal. Nor is NFT based on deliberate changes in breathing patterns such as respiratory sinus arrhythmia (RSA) that can result in changes in brain waves. At a neuronal level, NFT teaches the brain to modulate excitatory and inhibitory patterns of specific neuronal assemblies and pathways based upon the details of the sensor placement and the feedback algorithms used, thereby increasing flexibility and self-regulation of relaxation and activation patterns.
Perspective
Two issues that require clarification are the focus of biofeedback and NFT and the possibility or likelihood of negative side effects.First, the ISNR definition states: "The characteristic that distinguishes NFT from other biofeedback is a focus on the central nervous system and the brain." This description supports the view that while NFT is top-down, biofeedback training (BFT) is bottom-up. A more nuanced explanation is that both NFT and BFT involve top-down and bottom-up interventions. The arbitrary differentiation between body-centered and central nervous system (CNS) interventions results from an incomplete understanding of the interconnections between these systems. For example, the CNS is instrumental in modifying behaviors like respiration, and changes in respiration modulate CNS activity. Hyperventilation leading to hypocapnia causes a general slowing of the EEG (Takahashi, 2005).
Therefore, NFT and BFT share components like breathing, education about the training process, mindfulness, and problem-solving, involving the "central nervous system and the brain." Likewise, since the central and peripheral nervous systems cooperate through complex feedback and feedforward loops, we can conceptualize them as one complex integrated system.
For example, providers who work with inattention may begin with heart rate variability biofeedback (HRVB), which trains clients to increase the difference in the time intervals between successive heartbeats. Whereas attention involves brainstem, subcortical, and cortical networks, successful HRVB training (which is often characterized as bottom-up) may significantly increase continuous attention and make NFT unnecessary or may facilitate improved outcomes when followed by NFT for this condition.
Second, the ISNR definition claims: "When provided by a licensed professional with appropriate training, generally trainees do not experience negative side-effects." Hammond and Kirk (2008) marshaled evidence from randomized controlled trials (RCTs) and anecdotal reports that when applied incorrectly, neurofeedback can be associated with adverse reactions like anxiety, depression, emotional lability, explosiveness, incontinence, OCD, and sedation.
Hammond and Kirk did not rigorously evaluate the anecdotal reports supplied by trainers for length or severity of disruption resulting from NFT. In most cases, such effects are temporary unless reinforced by continuing incorrect training approaches (J. S. Anderson, personal communication, June 6, 2016).
Rogel et al. (2015) reported that a randomized, sham-controlled, double-blind study found no statistically significant differences in the number of side effects reported between sham and upper alpha and SMR treatment groups. The SMR group had a higher number of reported headaches.
Core Elements of Neurofeedback
The client-trainer relationship is the foundation of BFT and NFT. Neurofeedback is most effective when clients and providers are mindful because this promotes self-awareness and a sense of agency. Neurofeedback promotes self-regulation when a trainer provides effective coaching (Khazan, 2019).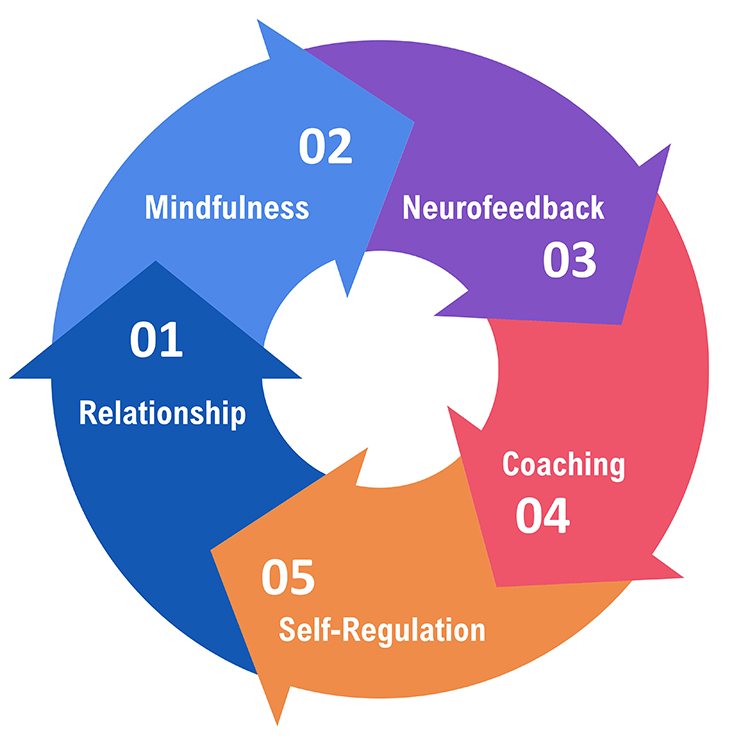
Physiological Monitoring and Modulation Are Not Biofeedback
Physiological monitoring, detecting biological activity like blood pressure, is only one biofeedback component. When nurses measure your blood pressure, this is physiological monitoring. Nurses provide biofeedback when they report these values to you because this gives you information about your biological performance. When your nurse announces that your blood pressure was 120/70, this closes the loop and allows you to refine your self-awareness and control of your physiology. Graphic © Sean Locke Photography/Shutterstock.com.

Listen to a mini-lecture on Physiological Monitoring and Modulation © BioSource Software LLC.
Likewise, modulation, stimulating the nervous system to produce psychophysiological change, is not biofeedback because it acts on your body instead of providing you with information about its performance. For example, a physical therapist might treat back pain through a modality called muscle stimulation. A current delivered to postural muscles fatigues them so that they cannot produce painful spasms. After muscle stimulation brings spasms under control, a physical therapist can initiate surface electromyographic (SEMG) biofeedback to teach the patient to increase awareness and control of postural muscle contraction. Graphic © DreamBig/Shutterstock.com.

Similarly, various devices that input signals into the central nervous system are not biofeedback devices but are generally known as entrainment devices. These include Audio-Visual Entrainment (AVE), Cranial Electrotherapy Stimulation (CES), repetitive Transcranial Magnetic Stimulation (rTMS), repetitive Transcranial Direct Current Stimulation (rTDCS), pulsed ElectroMagnetic Frequency Stimulation (pEMF), and others. These interventions may be useful and may provide an effective adjunct to biofeedback. However, since they do not provide information directly to the individual in a learning paradigm, they are not biofeedback. They represent treatment, not training. For this reason, providers should confirm that the use of these modalities falls within their scope of practice. An AVE device, is shown below.

Quantum Biofeedback and LenyosisTM
Slawecki (2009) cautioned consumers in "How to Distinguish Legitimate Biofeedback/Neurofeedback Devices."
The Sept. 3, 2009 Seattle Times published an exposé on pseudo-biofeedback devices: "Miracle Machines: The 21st-Century Snake Oil."
Appending biofeedback to a product's name does not make it biofeedback. Exposing clients to electromagnetic fields is modulation. Since biofeedback provides clients with real-time performance information to guide self-regulation, Quantum Biofeedback and LenyosysTM devices fall outside this definition.
Quantum Biofeedback
Quantum Biofeedback (EPFX / SCIO / XRROID / QXCI) devices do not provide individuals with immediate information regarding their performance. Marketers advertise that these instruments monitor, diagnose, and correct cellular abnormalities at a quantum level without providing peer-reviewed data. Critics claim that treatment with these devices may result in false diagnoses and delay effective treatment for medical disorders.
The following information was retrieved from the Empowering Change in You site on December 27, 2009. Note the disclaimer about "curing" medical conditions and explanation that it produces changes through stress management:
The function of the Quantum Biofeedback/EPFX is similar to a virus-scan on a computer. It focuses on your energetic body, which offers a more complete view of each facet of your health. Based on Quantum Physics, it runs a comprehensive test that measures the body’s frequencies. The system then contributes frequencies designed to resonate within the body, thus creating balance.
The human body is composed of a biochemical structure and an electromagnetic field. It performs best when these functions are balanced with one another and in complete harmony. Unfortunately, the daily stresses of life that confront each and every one of us takes its toll on the human body. Stress reduction is essential for wellness. This energy work is non-invasive.
It is important to remember that energetic medicine does not "cure" health problems. It addresses them specifically by making energetic corrections and rebalancing the system through stress management.
LenyosysTM
LenyosysTM describes its pulsed electromagnetic technology as a "body-biofeedback modality":Ideal as a complement to neurofeedback and biofeedback therapy, BRT is a body-biofeedback modality that helps to address the physical and somatic symptoms of both simple and complex health issues including digestive problems, systemic inflammation, muscle and joint aches, drug and alcohol addiction, allergies and hypersensitivities, stress, trauma and chronic illness. Whether used before, right after or in between sessions, BRT works in tandem with neurofeedback and biofeedback to create synergies that relax the client, enhance the therapy session and improve end results.

Pulsed electromagnetic treatment is modulation--not biofeedback. Instead of providing double-blind studies of their product's effectiveness, the marketers provide references for the application of Pulsed Electromagnetic Field Therapy (PEMF) and magnetism for specific applications.
Glossary
adverse reactions: iatrogenic effects like anxiety and sedation associated with BFT and NFT.
biofeedback: (1) learning process that teaches an individual to control her physiological activity, (2) the aim of biofeedback training is to improve health and performance, (3) instruments rapidly monitor an individual's performance and display it back to her, (4) the individual uses this feedback to produce physiological changes, (5) changes in thinking, emotions, and behavior often accompany and reinforce physiological changes, and (6) these changes become independent of external feedback from instruments. Information about psychophysiological performance is obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
bottom-up interventions: training that directly targets peripheral nervous system networks.
central nervous system: the division of the nervous system that includes the brain, spinal cord, and retina.
classical conditioning: unconscious associative learning process that modifies reflexive behavior and prepares us to respond to future situations rapidly.
electroencephalograph: an instrument that measures brain electrical activity.
electromyograph: an instrument that measures skeletal muscle action potentials.
entrainment devices: instruments that input signals such as light, sound, or electricity into the central nervous system.
feedback: in cybernetic theory, orders to act to correct small errors to prevent larger future errors in a closed system.
feedforward: in cybernetic theory, orders to perform an action based on anticipated conditions in an open system.
heart rate variability biofeedback: the display of beat-to-beat changes in heart rate that include changes in the RR intervals between consecutive heartbeats.
homeostasis: a state of dynamic constancy achieved by stabilizing conditions about a setpoint, whose value may change over time, proposed by Bernard and Cannon.
mindfulness: accepting and non-judgmental focus of attention on the present on a moment-to-moment basis.
modulation: stimulating the nervous system to produce psychophysiological change.
neurofeedback: information about EEG activity obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
operant conditioning: an unconscious associative learning process that modifies the form and occurrence of voluntary behavior by manipulating its consequences.
peripheral nervous system: nervous system subdivision that includes autonomic and somatic branches.
physiological monitoring: measurement of biological activity like EEG activity.
self-regulation: control of your behavior (e.g., voluntary increase in low-beta amplitude).
top-down interventions: training that directly targets central nervous system frontal, parietal, and limbic networks.
REVIEW FLASHCARDS ON QUIZLET
Click on the Quizlet logo to review our chapter flashcards.

Assignment
Now that you have completed this unit, how would you explain neurofeedback to a client? How would you explain the relationship between biofeedback and neurofeedback training?
References
Biofeedback Certification International Alliance (2016). Blueprint of knowledge statements for board certification in neurofeedback. Retrieved from http://www.bcia.org/files/public/EEGBlueprint.pdf
Collura, T. F. (2014). Technical foundations of neurofeedback. Routledge.
Hammond, D. C., & Kirk, L. (2008). First, do not harm: Adverse effects and the need for practice standards in neurofeedback. Journal of Neurotherapy, 12(1), 79-88. https://doi.org/10.1080/10874200802219947
International Society for Neurofeedback and Research (2016). Definition of neurofeedback. Retrieved from http://www.isnr.org/#!neurofeedback-introduction/c18d9
Khazan, I. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. John Wiley & Sons, Ltd.
Khazan, I. (2019). Biofeedback and mindfulness in everyday life: Practical solutions for improving your health and performance. W. W. Norton & Company.
Rogel, A., Guez, J., Getter, N., Keha, E., Cohen, T., Amor, T., & Todder, D. (2015). Transient adverse side effects during neurofeedback training: A randomized, sham-controlled, double blind study. Applied Psychophysiology and Biofeedback, 40(3), 209-218. https://doi.org/10.1007/s10484-015-9289-6
Schwartz, M. S. (2010). A new improved universally accepted official definition of biofeedback: Where did it come from? Why? Who did it? Who is it for? What's next? Biofeedback, 24, 88-90. https://doi.org/10.5298/1081-5937-38.3.88
Takahashi, T. (2005). Activation methods. In E. Niedermeyer & F. Lopes da Silva (Eds.). Electroencephalography: Basic principles, clinical applications, and related fields (5th ed.). Lippincott, Williams & Wilkins.
Thompson, M., & Thompson, L. (2016). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
B. HISTORY AND DEVELOPMENT OF NEUROFEEDBACK
This section covers Early Antecedents, Cybernetic Theory, Operant Conditioning, The Evolution of EEG Rearch and Practice, Contributors To EEG Research, and Neurofeedback Research.
"History depends on who writes it and who survives it. It is shaped by those who promote it and those who contribute to it. The official history of American biofeedback started in 1969 at the Surf Rider Inn in Santa Monica, California. Barbara Brown, a Veterans Administration (VA) electroencephalography (EEG) researcher, organized this meeting and placed her feisty stamp on the field. Here, the separate threads of scientific research into the possibility of autoregulation and the autoregulation practices of millennia-old meditative techniques coalesced." (Peper & Shaffer, 2010, p. 142)
Graphic from Biofeedback: Yoga of the West, narrated by Elmer Green and created by Hartley Productions.

The concept of self-regulation (voluntary control of biological processes) is ancient, despite our recent rediscovery of them. Hindus practiced systems of yoga more than 3,000 years ago in India. Before the term biofeedback was popularized in 1969, contributors repeatedly demonstrated this learning process without understanding its implications and broader application.
Claude Bernard (1865) proposed that the body strives to maintain a steady state (milieu interieur).
Walter Cannon (1914) expanded on this concept when discussing stress (a force that acts to disturb internal homeostasis) and homeostasis (a steady state).

Hans Selye (1963) studied the endocrine effects of chronic stress, proposed the three-stage General Adaptation Syndrome, and popularized the term stress in The Stress of Life (1956).
Bell, Tarchanoff, and Bair pioneered the contemporary study of self-regulation.
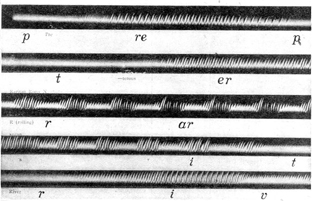
Alexander Graham Bell (1872) studied teaching the deaf to speak using biofeedback.
He investigated Leon Scott's phonautograph, which translated sound vibrations into tracings on smoked glass to show their acoustic waveforms.
Bell also examined Koenig's manometric flame, which displayed sounds as patterns of light. The photographs below are from R. Victor Jones (Bruce, 1973).
Ivan Tarchanoff (1885) showed that voluntary control of heart rate could be reasonably direct (cortical-autonomic) and did not depend on "cheating" by altering breathing rate.

J. H. Bair (1901) studied voluntary control of the retrahens muscle that wiggles the ear. He found that subjects learned this skill by inhibiting interfering muscles. This was a solid demonstration of skeletal muscle self-regulation.
Cybernetic Theory
Norbert Wiener (1948) developed cybernetic theory that proposed that systems are controlled by monitoring their results. Your home heating system is an excellent example of a cybernetic system. Cybernetic theory contributed concepts like system variable (what is controlled), setpoint (goal), feedback (corrective instructions), and feedforward (instructions based on anticipated conditions).
At the landmark 1969 conference at the Surfrider Inn in Santa Monica, the participants coined the term biofeedback from Weiner's feedback (Moss, 1998).
"This group needed a name, and the two candidates were biofeedback and autoregulation. Just before the final vote, someone in the audience yelled out that autoregulation sounded like government control of cars. This spontaneous comment created a tipping point, the consensus shifted to biofeedback, and the Biofeedback Research Society (BRS) was born." (Peper & Shaffer, 2010, p. 142)
Operant Conditioning
Edward Thorndike (1911) advanced the term instrumental learning to describe voluntary responses that obtain a desired outcome. His law of effect proposed that successful responses are mechanically stamped in by their successful consequences.

B. F. Skinner's (1938) operant conditioning research expanded on Thorndike's law of effect. He argued that animals repeat responses followed by favorable consequences based on extensive laboratory findings.
Skinner introduced several concepts that have influenced biofeedback theory. Reinforcement is a process where the consequence of a voluntary response increases the likelihood it will be repeated. Consequences that strengthen responses are called reinforcers. Punishment is a process that actively suppresses responses. A negative consequence such as a punishment following a voluntary response decreases the likelihood that the response will be repeated. Consequences that weaken responses are called punishers.
Based on Skinner's work, researchers used operant theory to divide physiological responses into those that could be voluntarily controlled and those that could not. "From its inception, biofeedback had to overcome the entrenched paradigm that individuals could not voluntarily control autonomic functions. Researchers who applied B. F. Skinner's work to biofeedback used operant theory to determine which responses could be voluntarily controlled and which could not. For example, Kimble (1961) argued that although subjects could learn to consciously control skeletal muscle responses, autonomic processes (such as heart rate) were involuntary, could be only classically conditioned, and were forever outside of conscious control. This perspective ignored the almost 3,000-year-old yogic practice of autonomic control and research by Lisina (1958); Lapides, Sweet, and Lewis (1957); and Kimmel (1967) that demonstrated voluntary control of autonomic responses." (Peper & Shaffer, 2010, p. 143)
The Evolution of EEG Research and Practice
1800s to 1940s
Early EEG equipment was imprecise and only minimally helpful in studying neuroanatomy and neurophysiology.
1960 to 1985
Environmental artifacts readily contaminated clinical EEG biofeedback devices. Excessive expectations and media hype over alpha training contributed to the perception that EEG biofeedback was not a viable modality. Biofeedback shifted to autonomic and skeletal muscle biofeedback. The minority of professionals who continued investigating and clinically using EEG biofeedback operated within an often unsupportive and hostile scientific environment.
2005-Present
The development of affordable, powerful digital computer technology, micro-electronics, more accurate sensors, and normative databases has enabled the average trainer to provide neurofeedback training. The increased portability and turn-key operation of EEG systems have enabled their use in both clinic and home environments.
Contributors To EEG Research
Luigi Galvani (1791) reported electrical currents in animals (Swartz & Goldensohn, 1998).

This finding was confirmed by Giovanni Aldini (1794) and Freiherr (baron) von Humboldt (1797).
Ernst Fleischl von Marxow (1833) recorded visual cortical potentials (cortical potentials evoked by visual stimuli) but did not describe rhythmic oscillation (Niedermeyer, 1993).

Emil du Bois-Reymond (1849) reported electrical conduction in muscles and peripheral nerves (Niedermeyer & Schomer, 2011).

Theodore Fritsch and Julius Eduard Hitzig (1858) discovered that cortical stimulation elicits a localized motor response (Niedermeyer & Schomer, 2011).
_AB.1.0435_Hitzig_CROPPED.tif.jpg)
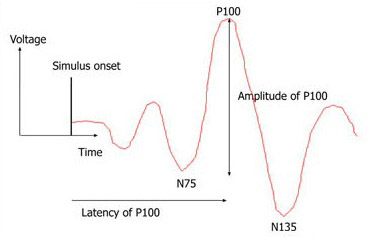
Richard Caton (1875) was an English physician who discovered electrical potentials in vivisected animals. He recorded spontaneous electrical potentials from the exposed cortical surface of monkeys and rabbits. He was the first to measure evoked potentials (EPs), which are EEG responses to stimuli (Niedermeyer & Schomer, 2011).
A visual evoked potential (VEP) is shown below.
He also reported the first observations of the shift of the cortical gradient to electro-negative during activation.
Vasili Yakovlevic Danilewsky (1877) published Investigations in the Physiology of the Brain, which explored the relationship between the EEG and states of consciousness (Brazier, 1959).

Adolf Beck (1891) published studies of spontaneous electrical potentials detected from the brains of dogs and rabbits. He was the first to document alpha blocking, where sensory stimulation blocks rhythmic oscillations (Coenen et al., 1998).

Sir Charles Sherrington (1906) introduced the terms neuron and synapse and published the Integrative Action of the Nervous System. He made significant contributions to understanding muscle action, movement, proprioception, reflexes, and spinal nerves (Niedermeyer & Schomer, 2011).

Sherrington proposed the "enchanted loom" metaphor for the human brain in a passage in the 1942 Man on His Nature, in which he poetically described the change in cortical activity as we awaken:
"The great topmost sheet of the mass, that where hardly a light had twinkled or moved, becomes now a sparkling field of rhythmic flashing points with trains of traveling sparks hurrying hither and thither. The brain is waking and with it the mind is returning. It is as if the Milky Way entered upon some cosmic dance. Swiftly the head mass becomes an enchanted loom where millions of flashing shuttles weave a dissolving pattern, always a meaningful pattern though never an abiding one; a shifting harmony of subpatterns." (p. 178)"
Current sleep research shows that the cortical networks are considerably more active during sleep than Sherrington imagined.
Vladimir Pravdich-Neminsky (1912) photographed dogs' EEG and event-related potentials, demonstrated a 12-14 Hz rhythm that slowed during asphyxiation, and introduced the term electrocerebrogram (Niedermeyer & Schomer, 2011).

Napolean Cybulsky and Jelenska-Maciesyna (1914) recorded experimental seizures (Swartz & Goldensohn, 1998).
Alexander Forbes (shown below) and David W. Mann (1920) reported replacing the string galvanometer with a vacuum tube to amplify the EEG. The vacuum tube became the de facto standard by 1936 (Swartz & Goldensohn, 1998).

Hans Berger (1929) was an Austrian neurologist and psychiatrist who published the first human EEG recording. He published fourteen scientific papers from 1929 to 1938 (Niedermeyer & Schomer, 2011).
He described a pattern of oscillating electrical activity recorded from his son Klaus' scalp (see published samples below).
Berger showed that these potentials were not due to scalp muscle contractions. Berger discovered the alpha rhythm, the first EEG rhythm, and called it the Berger rhythm. He identified sleep spindles, which are short bursts of 12-15 Hz activity during stage 2 sleep. Berger viewed the EEG as analogous to the ECG because it generates an electrical signal that can be amplified and displayed. He introduced the term elektenkephalogram. He believed that the EEG had diagnostic and therapeutic promise in measuring the impact of clinical interventions.
He demonstrated that alterations in state (sleep/wake, eyes open/closed, drug/no drug, and illness/health) are associated with changes in the EEG. He associated the beta rhythm with alertness. He described interictal activity (EEG potentials between seizures) and recorded a partial complex seizure (impaired awareness and repetitive behaviors called automatisms) in 1933. Finally, he performed the first qEEG, which measures the signal strength of component EEG frequencies (Hassett, 1978; Robbins, 2000; Swartz & Goldensohn, 1998).
Edgar Douglas Adrian (shown below) and Bryan Matthews (1934) confirmed Berger's findings by recording their EEGs using a cathode-ray oscilloscope. Their demonstration of EEG recording at the 1935 Physiological Society meetings in England led to its widespread acceptance (Niedermeyer & Schomer, 2011)
Adrian provided evidence supporting the all-or-none law: action potentials initiated at the axon hillock either occur or not. When they occur, they have the same amplitude and speed. He used himself as a subject and demonstrated the phenomenon of alpha blocking, where opening his eyes suppressed alpha rhythms.

Matthews (shown below) developed the oscillograph and differential amplifier, which is used in modern biofeedback and neurofeedback amplifiers

M. H. Fisher and H. Lowenback (1935) provided the first demonstration of epileptiform spikes (sharp EEG transients with a duration of less than 70 ms) (Swartz & Goldensohn, 1998).
Erna Gibbs, Fredric A. Gibbs, H. Davis, and William G. Lennox inaugurated clinical electroencephalography in 1935 by identifying abnormal EEG rhythms associated with epilepsy, including interictal spike waves and 3-Hz activity in absence seizures, which involve periods of less than 15 s during which a client blanks out (Brazier, 1959). Erna and Frederick Gibbs were married and closely collaborated on their research, including developing a scale for rating beta spindles.
Erna and Frederic Gibbs (top) and William Lennox (bottom) are pictured below.


Frederic Bremer (1935) used the EEG to show how sensory signals affect vigilance and studied the sleep-wake cycle. He divided the EEG into standard-bandwidth Bremer bands: delta (0-4 Hz), theta (4-8 Hz), alpha (8-12 Hz), and beta (12-32 Hz) (Niedermeyer & Schomer, 2011).

Fredric A. Gibbs and Herbert H. Jasper (1936) showed that the interictal spike was the defining indicator of epilepsy (Niedermeyer & Schomer, 2011).
W. G. Walter (1940s) named the delta and theta waves and the contingent negative variation (CNV). This slow cortical potential may reflect expectancy, motivation, intention to act, or attention (Niedermeyer & Schomer, 2011).
Walter (shown below) located an occipital lobe source for alpha waves and demonstrated that delta waves could help find brain lesions like tumors. In 1946, he described electrical responses to photic stimulation (visual stimulation at a specific flash frequency).

He improved Berger's electroencephalograph and pioneered EEG topography (Bladin, 2006). EEG topography maps electrical activity across the brain surface, as shown below.
The British EEG society was established in 1942, and the American EEG society began in 1947.
Nathaniel Kleitman (1953) has been recognized as the "Father of American sleep research" for his seminal work in sleep-wake cycle regulation, circadian rhythms, the sleep patterns of different age groups, and the effects of sleep deprivation. Kleitman described the basic patterns of sleep cycles and connecting transitional states (Niedermeyer & Schomer, 2011).

He discovered the phenomenon of rapid eye movement (REM) sleep with his graduate student Eugene Aserinsky. Below is a sample of brainwave activity during REM sleep.
William C. Dement (1950s), another of Kleitman's students, described the EEG architecture and phenomenology of sleep stages and the transitions between them in 1955, associated REM sleep with dreaming in 1957, and documented sleep cycles in another species, cats, in 1958, which stimulated basic sleep research. He established the Stanford University Sleep Research Center, the first international sleep laboratory, in 1970. He has contributed to research on sleep deprivation and the diagnosis and treatment of sleep disorders like apnea and narcolepsy (Niedermeyer & Schomer, 2011).

Kleitman and Dement advanced polysomnography by incorporating eye movement and the EEG during an entire night's sleep. These measurements enabled the study of sleep stages and behaviors like dreaming.
Per Andersen and S. A. Andersson (1968) proposed that thalamic pacemakers project synchronous 7-Hz alpha rhythms to the cortex via thalamocortical circuits and discovered the phenomenon of long-term potentiation (LTP). Per Anderson is shown below.
Neurofeedback Research
Joseph Kamiya (1960s) is considered the "Father of Neurofeedback." He demonstrated that the alpha rhythm in humans could be operantly conditioned. He published an influential article in Psychology Today that summarized research that showed that subjects could learn to discriminate when alpha was present or absent and that they could use feedback to shift the dominant alpha frequency by about 1 Hz. Almost half of his subjects reported experiencing a pleasant "alpha state" characterized as an "alert calmness." These reports may have contributed to the perception of alpha biofeedback as a shortcut to a meditative state. He also studied EEG activity during meditative states. Kamiya's research demonstrated a clinical application alpha-theta neurofeedback.
"Both the public and academic worlds recognize Joe Kamiya as the father of biofeedback. In 1966, while monitoring subjects' EEGs in his sleep lab at the University of Chicago, he performed a novel experiment by ringing a bell whenever an alpha burst occurred. He discovered that some subjects could discriminate when they produced alpha activity. His 1968 publication of 'Conscious Control of Brain Waves' in Psychology Today summarized research that showed that subjects could learn to discriminate when alpha was present or absent and that they could use feedback to shift the dominant alpha frequency about 1 Hz. Almost half of his subjects experienced a pleasant alpha state, which they characterized as an 'alert calmness.' Kamiya's article made biofeedback accessible to the public and made it exciting because it suggested that individuals can learn to control their own consciousness."
"Alpha biofeedback fit an emerging zeitgeist of self-exploration. American culture in the 1960s and 1970s was shaped by a confluence of forces: exploration of consciousness through drugs such as LSD (Timothy Leary and Richard Alpert) and Eastern meditative practices such as transcendental meditation (TM). Harvard physician Herbert Benson repackaged TM as the relaxation response without an overt spiritual dimension. Kamiya's work implied that a language of consciousness was possible and resulted in neurofeedback, one of the most promising areas of biofeedback." (Peper & Shaffer, 2010, p. 143)
Barbara Brown (1970s) demonstrated the clinical use of alpha-theta biofeedback. In research designed to identify the subjective states associated with EEG rhythms, she trained subjects to increase the abundance of alpha, beta, and theta activity using visual feedback. Brown recorded their subjective experiences when the amplitude of these frequency bands increased. She also helped popularize biofeedback by publishing a series of books, including New Mind, New body (1974), Stress and the Art of Biofeedback (1977), and Supermind (1980). Brown was a co-founder and first President of the Biofeedback Research Society, which became the Biofeedback Society of America and then the Association for Applied Psychophysiology and Biofeedback.

Thomas Mulholland and Erik Peper (1971) showed that occipital alpha increases with eyes open and not focused and is disrupted by visual focusing, a rediscovery of alpha blocking.
Elmer Green and Alyce Green (1969, 1970, 1977) investigated the voluntary control of internal states by individuals like Swami Rama and American Indian medicine man Rolling Thunder in India and at the Menninger Foundation. They brought portable biofeedback equipment to India and monitored practitioners as they demonstrated self-regulation. A film containing footage from their investigations was released as Biofeedback: The Yoga of the West (1974).
The Greens showed that, like the yogis they studied, ordinary individuals could learn self-regulation of "involuntary" physiological functions like blood pressure, the EEG, heart rate, skeletal muscle activity, and skin temperature.
They developed alpha-theta training at the Menninger Foundation from the 1960s to the 1990s. They hypothesized that theta states allow access to unconscious memories and increase the impact of prepared images or suggestions. Their alpha-theta research fostered Peniston's development of an alpha-theta addiction protocol.
They pioneered temperature biofeedback training for Raynaud's, migraine, and hypertension and wrote the classic Beyond Biofeedback (1977). They developed clinical biofeedback by applying these modalities to various disorders like hypertension and migraine.
Thomas Budzynski (1969, 1973) developed a twilight learning device that monitored left hemisphere EEG while a patient sleeps and played recorded educational content like language lessons and affirmations (positive statements) when theta was present. The premise of twilight learning is that affirmations have a greater impact when presented in a transitional state in which theta waves replace the alpha rhythm.

He studied the lateralization of brain function across the two cerebral hemispheres and the use of neurofeedback and audio-visual stimulation (brain brightening) to correct age-related cognitive decline.
M. Barry Sterman (1973) showed that cats and human subjects could be operantly trained to increase the amplitude of the sensorimotor rhythm (SMR) between 12-15 Hz recorded from the sensorimotor cortex.
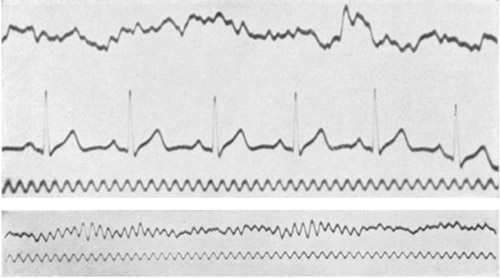
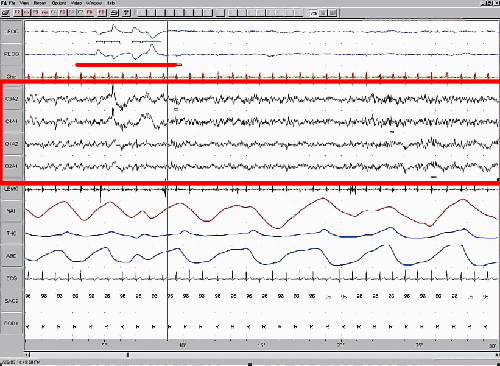
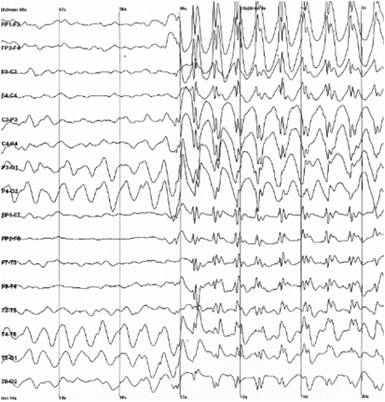
He demonstrated that SMR production protects cats against drug-induced generalized seizures (tonic-clonic seizures involving loss of consciousness) and reduces the frequency of seizures in humans diagnosed with epilepsy. He found that his SMR protocol, which uses visual and auditory EEG biofeedback, normalizes their EEGs (SMR increases while theta and beta decrease toward normal values) even during sleep. Generalized seizure activity is shown below.
Sterman conducted excellent research published in mainstream journals, which should have propelled SMR training into the forefront of seizure disorder treatment. Sterman also co-developed the Sterman-Kaiser (SKIL) qEEG database.
Joel Lubar (1970s) studied SMR biofeedback to treat attention disorders and epilepsy in collaboration with Sterman. He demonstrated that SMR training could improve attention and academic performance in children diagnosed with Attention Deficit Disorder with Hyperactivity (ADHD) at the University of Tennessee.
Lubar documented the importance of theta-to-beta ratios (the ratio of power in the theta and beta bands) in ADHD and developed theta suppression-beta enhancement protocols to decrease these ratios and improve student performance.
Erwin Roy John and Frank H. Duffy (1970s) collaborated in developing quantitative electroencephalography (qEEG) and its use in the assessment of disorders. John created neurometrics in which clients are compared to a normative database. Finally, John contributed to the study of memory and proposed that memory is distributed across the brain. John (left) and Duffy (right) are pictured below.
 |
 |
Jay Gunkelman's (Moss & Gunkelman, 2002) involvement in applied psychophysiology and biofeedback dates back to 1972 with the grant funding of the first state hospital-based biofeedback laboratory. Since the mid-1970s, he has specialized in the classical clinical EEG and is one of the world's most experienced EEG/qEEG specialists. He was instrumental in developing biofeedback and neurofeedback efficacy standards that have served as the foundation for the AAPB reference Evidence-Based Practice in Biofeedback and Neurofeedback. Jay has been one of the field's most influential educators and prolific authors.

Michael and Lynda Thompson (2015) have been "master teachers as well as superb clinicians and clinical researchers. Over the years, their clinic has acquired a much deserved international reputation with clients from other countries seeking their expertise. Somehow they also manage to teach workshops on biofeedback and neurofeedback to other professionals in the field." Thomas Budzynski, PhD.
 |
 |
They wrote The Neurofeedback Book: An Introduction to Basic Concepts in Applied Psychophysiology which has been the "bible" of neurofeedback didactic education. In 2016, AAPB awarded Michael and Lynda its Distinguished Scientist award.
Margaret Ayers (1975) was an early neurofeedback pioneer, established the first private clinical practice that exclusively provided neurofeedback, and published the first papers on neurofeedback for treating traumatic brain injury. She developed digital real-time EEG monitoring technology and investigated seizure control and treatment of coma patients with open head wounds. Her neurofeedback protocol down-trained slow-wave activity and uptrained 15-18 Hz activity.

Niels Birbaumer and colleagues (1970s) have studied operant conditioning of slow cortical potentials (SCPs; gradual changes in the membrane potentials of cortical dendrites that last from 300 ms to several seconds) since the late 1970s. They have demonstrated that subjects can learn to control these DC potentials and have studied the efficacy of SCP biofeedback in treating ADHD, epilepsy, and schizophrenia. They have shown that negative SCPs improve cognitive performance while positive SCPs increase the seizure threshold. Finally, they explored applications for brain-computer interfaces.
William N. Kuhlman and B. J. Kaplan (1979) identified the stabilizing 9-11-Hz mu rhythm in human subjects, which they considered separate from the SMR. They replicated Sterman's SMR research to inhibit generalized seizures.
Sue and Siegfried Othmer (1985) worked with Margaret Ayers to resolve their son's epilepsy. They proposed that protocols be chosen based on symptom patterns and pioneered computer games designed to modify the EEG. They investigated infra-low feedback (ILF) training of SCPs.
 |
 |
Eugene Peniston (1989) studied with the Greens at the Menninger Foundation. He developed the Peniston-Kulkosky Protocol, which uses alpha-theta training to treat alcoholism and post-traumatic stress disorder.

This multimodal protocol incorporated alpha-theta neurofeedback that uptrained alpha (8-13 Hz) and theta (4-8 Hz), autogenic training, constructed visualizations, diaphragmatic breathing, guided imagery, systematic desensitization, and temperature biofeedback. The diverse suggestion techniques utilized to potentiate alpha-theta training have influenced the use of guided imagery and behavior change scenarios in current alpha-theta neurofeedback.
Peniston and Kulkovsky reported that 8 of 10 experimental patients who received their alpha-theta protocol for alcoholism maintained abstinence from alcohol after 12-18 months compared with none of 10 controls. The two experimental patients who relapsed showed significantly reduced tolerance for alcohol. Peniston published seminal articles concerning alpha-theta training.
Vincent Monastra published early qEEG studies concerning the theta/beta ratio in ADHD and neurofeedback treatment of ADHD. Along with Lubar and Linden, he developed the statistical basis for using theta/beta power ratio measurement as a marker for ADHD.

Robert Thatcher (2010) developed a quantitative EEG database known as the lifespan database (NeuroGuide). He published the Handbook of QEEG and EEG Biofeedback. He developed 2- and 4-channel z-score training, 19-channel surface and LORETA z-score NF training, and BrainSurfer.

Juri Kropotov, who holds doctoral degrees in theoretical physics, philosophy, and neurophysiology, studied event-related potentials, developed EEG amplifiers (Mitsar 201 and 202), and is a prolific author, including his 2009 book Quantitative EEG: Event-Related Potentials and Neurotherapy. He is affiliated with the Human Brain Institute (HBI) and developed WinEEG software, using the HBI normative database for EEG and ERP analysis. He received the USSR State Prize in 1985 and the Copernicus Prize by the Polish Neuropsychological Society in 2009.

Roberto Pasqual Marqui has contributed to functional brain mapping using EEG and magnetoencephalography, and the study of functional connectivity in brain networks. He developed the three-dimensional Low Resolution Electromagnetic Tomography (LORETA).

Glossary
absence seizure: a seizure usually lasting less than 15 s in which a client blanks out; also called petit mal seizures.
affirmations: positive statements like "Every day I am getting better in every way."
all-or-none law: action potentials either occur or not. When they occur, they have the same amplitude and speed.
alpha blocking: replacement of the alpha rhythm by low-amplitude desynchronized beta activity during movement, attention, mental effort like complex problem-solving, and visual processing.
alpha rhythm: the first EEG rhythm discovered by Berger that ranges from 8 to 12 Hz which appears in three-quarters of adults when they are calm, awake, and not actively processing information.
alpha-theta training: training to progressively slow the EEG, increasing alpha and then theta abundance, developed by Brown and the Menninger Foundation and then adopted by Peniston and Kulkovsky in treating alcoholics.
beta rhythm: the second EEG rhythm discovered by Berger, 12-16 Hz.
biofeedback: information about psychophysiological performance obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
complex partial seizure: a seizure in which awareness is impaired and repetitive behaviors called automatisms (e.g., lip smacking) may occur.
contingent negative variation (CNV): a steady, negative shift in potential (15 microvolts in young adults) detected at the vertex discovered by Walter. This slow cortical potential may reflect expectancy, motivation, intention to act, or attention. The CNV appears 200-400 ms after a warning signal (S1), peaks within 400-900 ms, and sharply declines after a second stimulus that requires the performance of a response (S2).
cortical gradient: the difference in electrical charge between cortical neurons and scalp electrodes. When cortical networks are activated, their neurons are positively charged, and scalp electrodes are negatively charged.
curare: a paralytic drug used by Miller and DiCara to prevent rats from "cheating" by using skeletal muscles during operant conditioning of heart rate, blood pressure, kidney blood flow, skin blood flow, and intestinal contraction.
cybernetic theory: Weiner proposed that living systems are controlled by monitoring their results.
delta rhythm: EEG rhythm named by Walter that ranges from 0.5 to 3.5 Hz and is increased in adult Stage 3 sleep, brain injury, brain tumor, and developmental disability.
dysponesis: Whatmore and Kohli's concept of misplaced effort. For example, bracing your shoulders when you hear a loud sound.
EEG topography: the display that maps EEG activity across the brain surface in color.
evoked potentials: brain electrical potentials that are elicited by sensory stimulation.
feedback: in cybernetic theory, orders to correct small errors to prevent larger future errors in a closed system.
feedforward: in cybernetic theory, orders to perform an action based on anticipated conditions in an open system.
generalized seizures: seizures characterized by a peculiar cry, loss of consciousness, falling, tonic-clonic convulsions of all extremities, incontinence, and amnesia for the episode. These were previously called grand mal seizures.
homeostasis: a steady internal state proposed by Bernard and Cannon.
instrumental learning: operant conditioning, an unconscious associative learning process that modifies the form and occurrence of voluntary behavior by manipulating its consequences.
interictal activity: EEG potentials between seizures.
manometric flame: a device developed by Koenig and studied by Alexander Graham Bell for teaching the deaf to speak that displayed sounds as patterns of light.
motor unit: alpha motor neuron and the skeletal muscle fibers it controls.
neuron: an excitable nervous system cell that processes and distributes information, chemically and electrically, and usually contains a soma (cell body), dendrites, and axon.
normative database: means and standard deviations for EEG variables such as amplitude, power, coherence, and phase that are calculated for single hertz bins, frequency bands, or band ratios based on the EEG data collected from healthy normal subjects who are grouped by age, eyes open or eyes closed conditions, and sometimes gender and task, which also allows for the specification of z-scores with a mean of 0 and standard deviation of 1 for the various combinations of EEG variables, frequency ranges, subject ages, eyes-open or eyes-closed conditions and other variables.
operant conditioning: an unconscious associative learning process that modifies the form and occurrence of an operant behavior (emitted behavior) by manipulating its consequences.
Peniston-Kulkovsky addiction protocol: a multimodal approach that incorporates visualization training, temperature biofeedback, rhythmic breathing techniques, autogenic training exercises, construction of personalized imagery, guided imagery, and 30 alpha-theta sessions.
phonautograph: a device developed by Leon Scott and studied by Alexander Graham Bell to teach the deaf to speak, translating sound vibrations into tracings on smoked glass to show their acoustic waveforms.
photic stimulation: visual stimulation at a specific flash frequency.
punisher: a consequence that weakens an operant behavior. For example, shoulder pain (punisher) following excessive exercise (operant behavior) may reduce exercise intensity.
punishment: in operant conditioning, the consequence of an operant behavior reduces its probability.
quantitative EEG (qEEG): digitized statistical brain mapping using at least a 19-channel montage to measure EEG amplitude within specific frequency bins.
reinforcement: in operant conditioning, the consequence of an operant behavior increases its probability.
reinforcer: a consequence that strengthens an operant behavior. For example, weight loss (reinforcer) following daily walks (operant) may increase the probability of walking.
self-regulation: the control of your behavior (voluntary hand-warming).
sensorimotor rhythm (SMR): EEG rhythm that ranges from 12-15 Hz and appears when you inhibit movement and relax your muscles.
setpoint: the system goal, for example, a thermostat setting of 75 degrees F (23.9 degrees C).
sleep spindles: short bursts of 12-15 Hz activity during stage 2 sleep.
slow cortical potentials (SCPs): gradual changes in the membrane potentials of cortical dendrites that last from 300 ms to several seconds. These potentials include the contingent negative variation (CNV), readiness potential, movement-related potentials (MRPs), and P300 and N400 potentials. SCPs modulate the firing rate of cortical pyramidal neurons by exciting or inhibiting their apical dendrites. They group the classical EEG rhythms using these synchronizing mechanisms.
spike: a sharp EEG transient with a duration of less than 70 ms.
stress: Selye's concept of a nonspecific response to stimuli called stressors.
synapse: specialized chemical and electrical junctions across which neurons communicate with each other and non-neural cells.
system variable: the variable that is controlled. For example, room temperature is the system variable for a thermostat.
thalamus: a forebrain structure above the hypothalamus that receives, filters, and distributes most sensory information. The thalamus contains neurons that can block or relay ascending sensory information. When these thalamic neurons rhythmically fire, this blocks the transmission of information to the cortex. When they depolarize in response to sensory information, this integrates and transmits this information to the cortex. Inputs to the thalamus determine whether these neurons block or relay sensory information.
theta rhythm: the EEG rhythm discovered by Walter that ranges from 4 to 7 Hz and is associated with drowsiness, the transition from wakefulness to sleep, rapid eye movement (REM) sleep, and the processing of information.
theta/beta training: a protocol that decreases theta amplitude and increases beta amplitude.
theta-to-beta ratio: the ratio of power in the theta and beta bands.
twilight learning: Budzynski's training paradigm in which recorded material is played when theta activity replaces alpha activity.
visual cortical potentials: brain electrical potentials evoked by visual stimuli like flashing lights.
z-score training: a strategy that attempts to normalize brain function with respect to mean values in a clinical database. EEG amplitudes that are 2 or more standard deviations above or below the database means are down-trained or uptrained to treat symptoms and improve performance.
REVIEW FLASHCARDS ON QUIZLET
Click on the Quizlet logo to review our chapter flashcards.
Assignment
From your perspective, which EEG researcher contributed most to the development of neurofeedback? Why?
References
Adrian, E. D., & Mathews, B. H. C. (1934). The Berger rhythm. Brain, 57, 355-385. https://doi.org/10.1093/brain/57.4.35
Andersen, P., Andersson, S. A. (1968). Physiological basis of alpha rhythm. Appleton-Century-Crofts.
Andreassi, J. L. (2007). Psychophysiology: Human behavior and physiological
response (5th ed.). Lawrence Erlbaum and Associates, Inc.
Ayers, M. E. (1995). EEG neurofeedback to bring individuals out of level 2 coma [Abstract]. Biofeedback and Self-Regulation, 20(3), 304-305.
Ayers, M. E. (1995). Long-term follow-up of EEG neurofeedback with absence seizures. Biofeedback & Self-Regulation, 20(3), 309-310.
Berger, H. (1920). Ueber das elektroenkephalogramm des menschen. Archiv für Psychiatrie und
Nervenkrankheiten, 87, 527-570.
Bernard, C. (1957). An introduction to the study of experimental medicine. Dover. (Originally
published, 1865.)
Birbaumer, N., Elbert, T., Lutzenberger, W., Rockstroh, B., & Schwarz, J. (1981). EEG and slow cortical potentials in anticipation of mental tasks with different hemispheric involvement. Biol Psychol, 13, 251–260. https://doi.org/10.1016/0301-0511(81)90040-5
Bladin, P. F. (2006). W. Grey Walter, pioneer in the electroencephalogram, robotics, cybernetics, artificial intelligence. Journal of Clinical Neuroscience, 13(2), 170-177. https://doi.org/10.1016/j.jocn.2005.04.010
Bokser, I. O. (1999). History of creation of the doctrine, equipment and methods of formation of biological feedback. Med Tekh, 4,
44-46.
PMID: 10464764
Brazier, M. A. B. (1959). The EEG in epilepsy: A historical note. Epilepsia, 1(1-5), 328-336. https://doi.org/10.1111/j.1528-1157.1959.tb04270.x
Brazier, M.A.B. (1961). A history of the electrical activity of the brain. The first half-century. Pitman.
Bremer, F. (1935). Cerveau isole et physiologie du sommeil. Com Ren Soc Bio (Paris), 118, 1235-1241.
Brown, B. (1974). New mind, new body. Harper & Row.
Brown, B. (1977). Stress and the art of biofeedback. Harper &
Row.
Brown, B. (1980). Supermind: The ultimate energy. Harper &
Row.
Bruce, R. V. (1973). Bell: Alexander Graham Bell and the conquest of solitude. Gollancz.
Caton, R. (1875). The electric currents of the brain. British Medical Journal, 2, 278.
Coenen, A. M. L., Zajachkivsky, O., & Bilski, R. (1998). Scientific priority of A. Beck in the neurophysiology.
Experimental and Clinical Physiology and Biochemistry, 1, 105-109.
Cybusky, N., & Jelenska-Macieszyna, X (1914). Action currents of the cerebral cortex [in Polish]. Bull Acad Sci Cracov, B, 776–781.
Dement, W. (2000). The promise of Sleep: A pioneer in sleep medicine explores the vital connection between
health, happiness, and a good night’s sleep. Random House.
Evans, J. R., & Abarbanel, A. (1999). Introduction to quantitative EEG
and neurofeedback. Academic Press.
Fahrion, S., Norris, P., Green, A., Green, E., & Snarr, C. (1986). Biobehavioral treatment of essential hypertension: A group outcome study. Biofeedback-and-Self-Regulation, 11(4), 257-277.
Flor, H. (2002). Phantom-limb pain: characteristics, causes, and treatment. The Lancet, Neurology, 1(3),
182-189. https://doi.org/10.1016/S1474-4422(02)00074-1
Goldensohn, E. S., Porter, R. J., & Schwartzkroin, P.A. (1997). The American Epilepsy Society: An historic perspective on 50 years of advances in research. Epilepsia, 38(1), 124–150. https://doi.org/10.1111/j.1528-1157.1997.tb01088.x
Green, E. E., Walters, E. D., Green, A. M., & Murphy, G. (1969). Feedback technique for deep relaxation.
Psychophysiology, 6 (3), 371-377.
https://doi.org/10.1111/j.1469-8986.1969.tb02915.x
Green, E., & Green, A. (1977). Beyond biofeedback. Delacorte Press.
Green, E., Green, A. M., & Walters, E. D. (1970). Self-regulation of
internal states. In J. Rose (Ed.), Progress of cybernetics:
Proceedings of the First International Congress of Cybernetics,
London, September 1969 (pp. 1299-1318). Gordon and Breach
Science Publishers.
Green, E., Green, A. M., & Walters, E. D. (1970). Voluntary control of
internal states: Psychological and physiological. Journal of
Transpersonal Psychology, 2, 1-26.
Kamiya, J. (1969). Operant control of
the EEG alpha rhythm. In C. Tart (Ed.), Altered states of
consciousness. Wiley.
Kleitman, N. (1960). Patterns of dreaming. Scientific American, 203(5), 82-88. https://doi.org/10.1038/scientificamerican1160-82
Lubar, J. F. (1989). Electroencephalographic biofeedback and
neurological applications. In J. V. Basmajian (Ed.), Biofeedback:
Principles and practice for clinicians (3rd ed.), pp. 67-90.
Williams and Wilkins.
Lubar, J. F. (1991). Discourse on the development of EEG diagnostics and
biofeedback treatment for attention-deficit/hyperactivity disorders.
Biofeedback and Self-regulation, 16, 201-225. https://doi.org/10.1007/bf01000016
Lubar, J. F., & Shouse, M. N. (1977). Use of biofeedback in the
treatment of seizure disorders and hyperactivity. In B. B. Lahey & A. E.
Kazdin (Eds.), Advances in clinical child psychology (pp.
203-265). NY: Plenum Press.
McKnight, J. T., & Fehmi, L. G. (2001). Attention and neurofeedback
synchrony training: Clinical results and their significance. Journal
of Neurotherapy, 5. https://doi.org/10.1300/J184v05n01_05
Miller, N. E. (1969). Learning of visceral and glandular responses.
Science, 163, 434-445. https://doi.org/10.1126/science.163.3866.434
Miller, N. E. (1978). Biofeedback and visceral learning. Annual
review of psychology, 29, 373-404. https://doi.org/10.1146/annurev.ps.29.020178.002105
Miller, N. E., & DiCara, L. (1967). Instrumental learning of heart rate changes in curarized rats: Shaping and specificity to discriminative stimulus. Journal of Comparative and Physiological Psychology,
63, 12-19. https://psycnet.apa.org/doi/10.1037/h0024160
Miller, N. E., & Dworkin, B. (1974). Visceral learning: Recent
difficulties with curarized rats and significant problems for human
research. In P. A. Obrist; A. H. Black, J. Brener, & L. V. DiCara (Eds.),
Cardiovascular psychophysiology (pp. 312-331). Aldine.
Moss, D., & Gunkelman, J. (2002). Task force report on methodology and empirically supported treatments: Introduction and summary. Applied Psychophysiology and Biofeedback, 27 (4), 261-262. https://doi.org/10.1023/a:1021009301517
Mulholland, T., & Peper, E. (1971). Occipital alpha and accommodative vergence, pursuit tracking, and fast eye movements. Psychophysiology, 8, 556-575. https://doi.org/10.1111/j.1469-8986.1971.tb00491.x
Niedermeyer, R., & Schomer, D. L. (2011). Historical aspects of EEG. In D. L. Schomer & F. Lopes da Silva (Eds.). Niedermeyer's Electroencephalography: Basic principles, clinical applications, and related fields (6th ed.). Lipincott Williams & Wilkins.
O’Leary, J. L., & Goldring, S. (1976). Science and epilepsy. Raven Press.
Peper, E., & Shaffer, F. (2010). Biofeedback history: An alternative view. Biofeedback, 38(4),
142-147.
https://doi.org/10.5298/1081-5937-38.4.03
Pravdich-Neminsky, V. V. (1913). Ein versuch der registrierung der elektrischen gehirnerscheinungen. Zbl Physiol
27, 951–960.
Robbins, J. (2000). A symphony in the brain. Atlantic Monthly Press.
Sherrington, C. S. (1906). The integrative action of the nervous system. Yale University
Press.
Sherrington, C.S. (1942). Man on his nature. Cambridge University Press.
Skinner, B. F. (1938). The behavior of organisms: An experimental analysis. Appleton-Century.
Sterman, M. B. (1973). Neurophysiologic and clinical studies of sensorimotor EEG biofeedback training: Some effects on epilepsy. Seminars in Psychiatry, 5, 507-524.
Swartz, B. E., & Goldensohn, E. S. (1998). Appendix: Time of the history of EEG and associated fields. Electroencephalography and Clinical Neurophysiology, 106, 173-176. PMID: 9741779
Thompson, M., & Thompson, L. (2016). The neurofeedback book: An introduction to basic concepts in applied
psychophysiology (2nd ed.). The Association for Applied Psychophysiology and Biofeedback.
Thorndike, E. (1911). Animal intelligence: Experimental studies. The Macmillan Company.
Walter, W. G. (1937). Electroencephalogram in cases of cerebral tumour. Proceedings of the Royal Society of
Medicine, 30, 579-578. PMID: 19991061
Walter, W. G. (1953). The living brain. Norton.
Walter, W. G., Cooper, R., Aldridge, V. J., McCallum, W. C., & Winter, A. L. (1964). Contingent negative variation: An electric sign of sensorimotor association and expectancy in the human brain. Nature, 203,
380-384. https://doi.org/10.1038/203380a0
Wiener, N. (1948). Cybernetics: Or control and communication in the animal and the machine.
MIT Press.
C. OVERVIEW OF PRINCIPLES OF HUMAN LEARNING AS THEY APPLY TO NEUROFEEDBACK
This unit covers Three Main Types of Learning, Classical Conditioning, Operant Conditioning, Nonassociative Learning, Observational Learning, and Critical Elements in Neurofeedback Training.
Learning
A movie plays when a child increases low beta and decreases theta activity (positive reinforcement). A score counter stops reversing when a child focuses on a reading selection after several minutes of distraction (negative reinforcement). The training goal becomes progressively more demanding as the child succeeds (shaping).

Sherlin et al. (2011) emphasized the importance of learning theory in neurofeedback: "It is our contention that future applications in clinical work, research, and development should not stray from the already-demonstrated basic principles of learning theory until empirical evidence demonstrates otherwise." (p. 292)

We can divide learning into three main categories: associative, nonassociative, and observational. Associative learning and observational learning are most relevant to neurofeedback. In associative learning, we create connections between stimuli, behaviors, or stimuli and behaviors. Associative learning aids our survival since it allows us to predict future events based on our experience. Learning that B follows A provides us with time to prepare for B. Two forms of associative learning are classical conditioning and operant conditioning (Cacioppo & Freberg, 2016).
Classical Conditioning
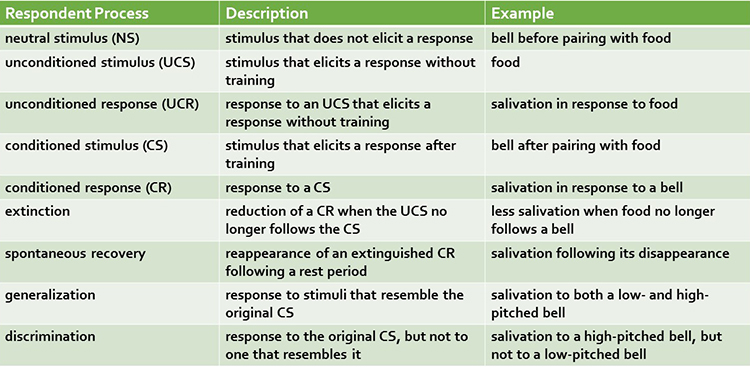
Pavlov demonstrated classical conditioning in 1927 based on his famous research with dogs. Due to faulty English translations, we now use the adjectives conditioned and unconditioned instead of conditional and unconditional. We will use the current terminology to minimize confusion.
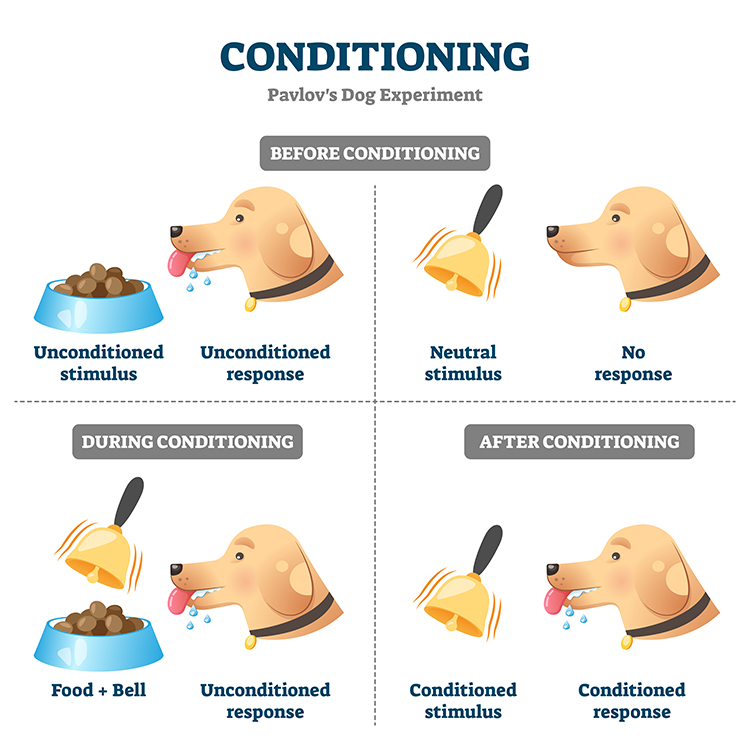
Classical conditioning is an unconscious associative learning process that builds connections between paired stimuli that follow each other in time. Through this learning process, a dog in Pavlov's laboratory learned that if A (a ringing bell) occurs, B (food) will follow. The ability to predict the future from experience is crucial to our survival since it gives us time to prepare.
Before learning to anticipate food in Pavlov's laboratory, dogs salivated (unconditioned response) when they saw food (unconditioned stimulus). An unconditioned response (UCR) follows an unconditioned stimulus (UCS) before conditioning. However, until the dogs learned to associate the sound of a bell with food delivery, the bell was a neutral stimulus (NS) that did not elicit salivation.
Through the repeated pairing of the bell with the arrival of food, Pavlov's dogs learned that the bell reliably signaled the arrival of food. The bell became a conditioned stimulus (CS) that elicited the conditioned response (CR) of salivation. Graphic © VectorMine/iStockphoto.com.
When the association between the CS and CR is disrupted because B no longer consistently follows A, the frequency of the CR may decline or the CR may disappear. This phenomenon is called extinction. In Pavlov's situation, repeated trials where food did not follow bell ringing reduced or eliminated salivation. The extinction of CRs allows us to adapt to changes in our experience. You learn to use passwords less predictable than "password" after becoming a victim of identity theft. You can to play with dogs, again, after you were bitten as a child.
Pavlov argued that extinction is not forgetting but evidence of new learning that overrides previous learning. The phenomenon of spontaneous recovery, where the CR (salivation) reappears after some time without exposure to the CS (bell), supports his position. Dogs who stopped salivating by the end of an extinction trial in which no food followed the bell resumed salivating during a break or the next session.
Generalization and discrimination are mirror images of each other. In generalization, the conditioned response is elicited by stimuli (low-pitched bell) that resemble the original conditioned stimulus (high-pitched bell). Generalization promotes our survival because it allows us to apply learning about one stimulus (lions) to similar predators (tigers) without experiencing them.
In contrast, in discrimination, the conditioned response (salivation) is elicited by one stimulus (high-pitched bell) but not another (low-pitched bell). When soldiers return to civilian life, they must distinguish between a CS that signals danger (gunfire) and one that is benign (fireworks). Discrimination is often impaired in soldiers diagnosed with post-traumatic stress disorder (PTSD).
Operant Conditioning
Edward Thorndike's (1913) law of effect proposed that the consequences of behavior determine its addition to your behavioral repertoire. From his perspective, cats learned to escape his "puzzle boxes" by repeating successful actions and eliminating unsuccessful ones.
Operant conditioning is an
unconscious associative learning process that modifies an operant behavior, voluntary behavior that operates on the environment to produce an outcome, by manipulating its
consequences (Miltenberger, 2016).
Operant conditioning differs from
classical conditioning in several respects. Where operant conditioning teaches the association of a voluntary behavior with its consequences, classical conditioning teaches the predictive relationship between two stimuli to modify involuntary behavior.
Neurofeedback teaches self-regulation of neural activity and related "state changes" using operant conditioning via the selective presentation of reinforcing stimuli, including visual, auditory, and tactile displays.
Operant conditioning occurs with a situational context. The identifying characteristics of a situation are called
its
discriminative stimuli and can include
the physical environment and physical, cognitive, and emotional cues. Discriminative stimuli teach us when to
perform operant behaviors.
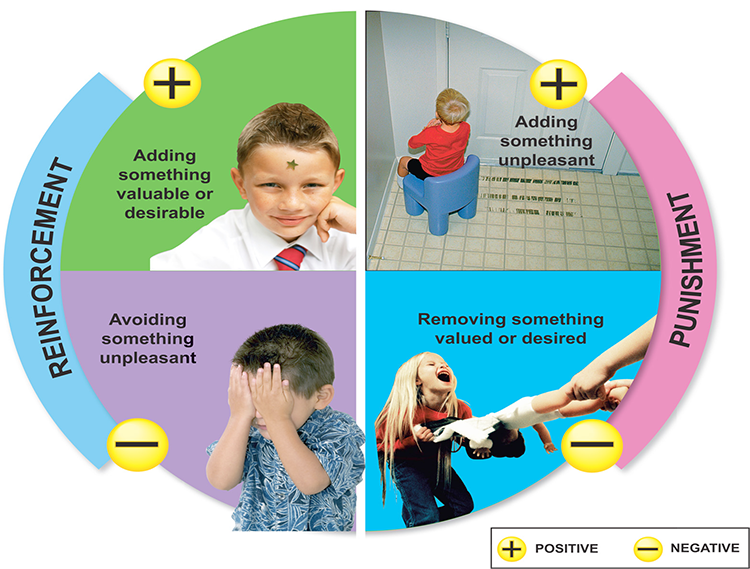
The consequences of operant behaviors can increase or decrease their frequency. Skinner proposed four types of consequences: positive reinforcement, negative reinforcement, positive punishment, and negative punishment. Where positive and negative reinforcement increase behavior, positive and negative punishment decrease it.
Due to individual differences, we cannot know in advance whether a consequence will be reinforcing or punishing since these are not intrinsic properties of a consequence. We can only determine whether a consequence is reinforcing or punishing by measuring how it affects the behavior that preceded it. In neurofeedback, a movie that motivates the best performance might be the most reinforcing for the client, regardless of the therapist's personal preference.
Positive reinforcement increases
the frequency of a desired behavior by making a desired outcome contingent on performing the action. For example, a movie plays when a client diagnosed with attention deficit hyperactivity disorder (ADHD) increases low-beta and decreases theta activity.
Negative reinforcement increases the frequency of a desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on performing the action. For example, an athlete's anxiety decreases by shifting from high beta to low beta.
Positive punishment decreases or eliminates an undesirable behavior by associating it with unwanted consequences. For example, a child's increased fidgeting dims a favorite movie and lowers the sound.
Negative punishment
decreases or eliminates an undesirable behavior by removing what is desired. For example, oppositional behavior could result in a clinician turning off a popular game.
Reinforcement Criteria
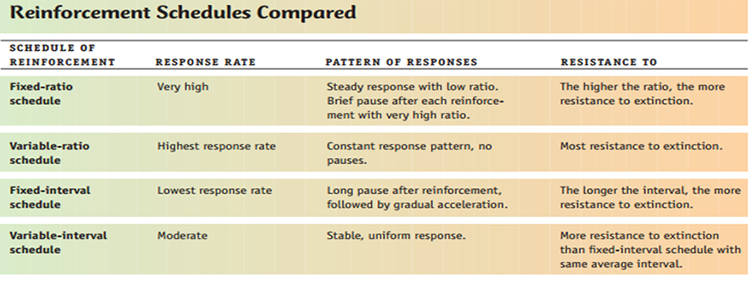
Current research is exploring the optimal reinforcement criteria for neurofeedback training. Client skill acquisition is markedly affected by changing parameters like reinforcement schedule, frequency of reward, reinforcement delay, conflicting reinforcements, conflicting expectations, and alteration of the environment.While continuous reinforcement, reinforcement of every desired behavior, is helpful during the early stage of skill acquisition, it is impractical as clients attempt to transfer the skill to real-world settings. Since reinforcement outside of the clinic is intermittent, partial reinforcement schedules, where the desired behavior is only reinforced some of the time, are important as training progresses. This reduces the risk of extinction, where failure to reinforce the desired behavior reduces the frequency of that behavior.
For neurofeedback, variable reinforcement schedules, where reinforcement occurs after a variable number of responses (variable ratio) or following a variable duration of time (variable interval) produce superior response rates than their fixed counterparts.
Sherlin et al. (2011) emphasized the importance of professionals understanding targeted brain rhythms and the underlying EEG neurophysiology. For example, the sensorimotor rhythm (SMR) consists of spindles with at least a 0.25-second duration. Use of criteria like "time above threshold" or "duration of sustained reward" tailors feedback to the SMR rhythm and results in superior outcomes compared to reinforcing any shift above an SMR amplitude threshold.
Sherlin et al. (2011) advised that: "For operant conditioning, it is very important to be aware of specifically 'what behavior' is being conditioned in order to achieve learning and to improve the specificity" (p. 300).
This is especially important in the context of EEG artifacts, which are false signals that masquerade as brain electrical activity. The EEG is vulnerable to diverse biological (electrocardiogram, eye movement, respiratory, skeletal muscle) and environmental (50/60-Hz, radiofrequency) artifacts. Neurofeedback systems should provide real-time artifact control and trainers should carefully monitor training to prevent "artifact-driven feedback." We don't want to inadvertently reward changes in the frequency of eye blinks or the degree of frontalis muscle contraction. Control of artifact avoids reinforcement of a coincidental response and increases training specificity and success (Sherlin et al., 2011).
Shaping
Shaping, the method of successive approximations, teaches clients new behaviors and increases the frequency of rarely performed behaviors. A trainer starts by reinforcing spontaneous voluntary behaviors that resemble the desired behavior and then progressively raises the criteria for reinforcement to achieve the training goal. For example, the trainer can gradually require lower theta-to-beta ratios for a movie to play.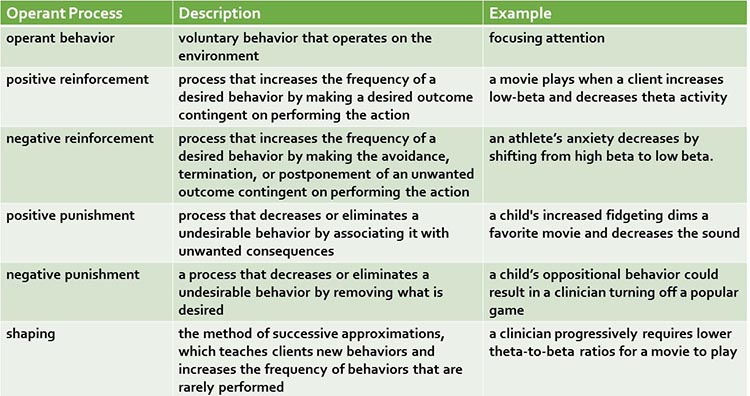
Sherlin et al. (2011) warn that shaping should not be performed using auto-thresholding because this approach rewards transient responses in the right direction, whether or not this shift involves an absolute change from baseline. Auto-thresholding can deliver reinforcement when clients are not producing the desired behavior and even when they are producing the opposite behavior. Finally, they observe that shaping is not applicable to slow cortical potential (SCP) neurofeedback since there are no normative values to shape towards; only the direction of deviation from baseline (positive or negative) is critical to training success.
Discrimination and Generalization
Discrimination and generalization are the ultimate goals of neurofeedback training. Discrimination teaches when the desired behavior will be reinforced. The initial discriminative stimuli include the cues provided by the training environment, like animations and tones. Following successful skill acquisition, a trainer may introduce a stressor to "raise the bar." Now, the stressor serves as another discriminative stimulus for performing the desired behavior. Discrimination teaches a client to identify and disarm symptom triggers in everyday life instead of unconsciously reacting to them.Generalization teaches the transfer of the desired behavior to multiple environments and in response to diverse stressors. This enables a client to respond adaptively to novel and unanticipated triggering stimuli. While the ability to perform the learned response in many situations contributes to flexibility, it is not always advantageous. Discrimination, based on an understanding of set and setting, helps determine when a response is required and which response is appropriate.
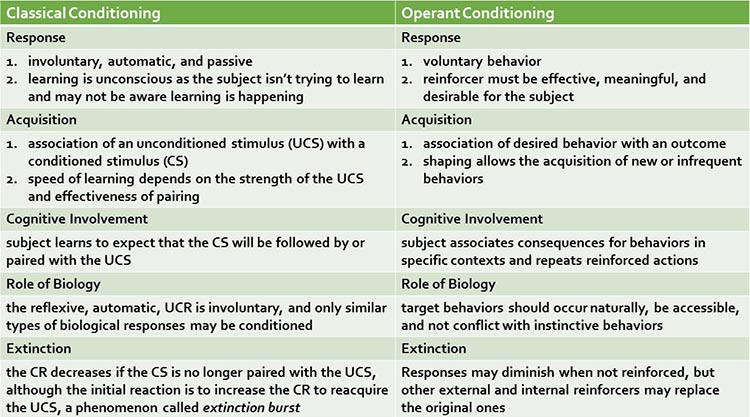
Check out the TED-Ed video, The Difference Between Classical and Operant Conditioning.
Nonassociative Learning
Nonassociative learning is a simple learning process in which the strength of the response to a stimulus changes with repeated exposure. Habituation and sensitization are nonassociative learning processes.
In habituation, our response to an unchanging harmless stimulus weakens with repeated exposure. This process can interfere with the transfer of training to the environment. Clients can quickly tune out reminders (colored dots) to practice self-regulation skills. One strategy to counter habituation is to change the color and shape of these prompts randomly.
In sensitization, our response to a range of stimuli strengthens following exposure to a single powerful stimulus. For example, following a traumatic experience (earthquake), your response to movement or noise might be exaggerated. Graphic © maroke/Shutterstock.com.

Observational Learning
Observational learning allows us to rapidly modify an existing skill or acquire a new one by observing others. This social learning process is highly efficient because it bypasses trial-and-error learning. We don't personally experience negative outcomes since others have done it for us.
Observational learning is interactive. For example, we listen to a teacher play a violin passage, we attempt to play the same notes, and then compare the two performances. We play the passage, again and again, until we "get it right." Feedback allows us to refine our playing until we can match the original sample.

Critical Elements in Neurofeedback Training
Successful neurofeedback training incorporates readiness, repetition (exercise), reinforcement (effect), primacy, recency, intensity, freedom, and resources (requirement).
Readiness
Readiness means preparation for training and involves concentration and enthusiasm. "Individuals learn best when they are physically, mentally, and emotionally ready to learn, and do not learn well if they see no reason for learning" (Tracy, 2018). Graphic © Tom Wang/Shutterstock.com.
This requires adequate rest and nutrition and a positive and supportive environment. Client education that explains the training process clearly defines goals and outcomes, and links training to personally relevant benefits enhance readiness.
In contrast, poor client motivation, lack of understanding of potential benefits, and biopsychosocial impediments can impair readiness. Significant biopsychosocial constraints include a chaotic, disruptive, or traumatic environment, inadequate rest and nutrition, developmental delays, lack of resources, and traumatic brain injury or other medical problems.
Repetition (Exercise)
Exercises performed within and outside the clinic promote client engagement and transfer of training to everyday life. Successful training recognizes brain plasticity and the physiological requirements for skill acquisition and consolidation. Practice periods should range from 10-30 minutes and include a minimum of 20 repetitions. Graphic © PH888/Shutterstock.com.
Reinforcement (Effect)
Rewards must be personally desirable to the client. trainers can confirm this by observing the impact of reinforcers on engagement, motivation, and performance. Intrinsically reinforcing outcomes accelerate the development of mastery and improve retention. Clear evidence of success builds confidence and reduces frustration. Encouragement by staff and family is essential to sustain progress as a client experiences difficulty.
Sherlin et al. (2011) speculated that secondary reinforcement for achievement during neurofeedback (monetary rewards or points that can be redeemed for a prize) might accelerate learning self-regulation skills. They cautioned that secondary reinforcement should be delivered for EEG changes and not simple attendance.
Reinforcement must occur "immediately" to ensure that the brain correctly pairs this consequence with the desired behavior that preceded it. Early studies determined that the optimal delay between an operant behavior and reinforcement is less than 250 to 350 ms (Felsinger & Gladstone, 1947; Grice, 1948). The faster the delivery of reinforcement following the desired behavior, the less time required for skill acquisition. This means that shorter EEG filter response times are better (Sherlin et al., 2011, p. 298),
"The more immediate the delivery of the reinforcer after the behavior, the more effective the reinforcer" (Miller, 2006). (p. 233) Graphic © Nicky Rhodes/Shutterstock.com.

Egner and Sterman (2006) cautioned that neurofeedback training "should stress exercise rather than entertainment" because complex games might prevent clients from linking brain responses to reinforcement due to distraction produced by more salient game stimuli.
Primacy
Trainerss should approach neurofeedback training like a contractor building a house: start with a strong foundation. Graphic © Mary Rice/Shutterstock.com.
Client education should present the core principles that will set the foundation for future learning. Like home construction, skill acquisition should proceed in a stepwise fashion that builds upon previous experience. The successful acquisition of initial skills builds confidence and aids the mastery of more complex skills.
Recency
Clients more readily recall material that is learned most recently. The combination of recency and repetition improves the retention of self-regulation skills. The frequency of training sessions impacts learning since greater frequency reinforces skill acquisition as the pairing with skill practice and reinforcement occurs more recently. Graphic © Leah-Anne Thompson/Shutterstock.com.
Intensity
The brain is a difference and intensity detector. The brain allocates greater attention and processing power to events that are more intense and novel. This suggests that adjunctive experiential exercises can facilitate self-regulation skill retention. Graphic © Solis Images/Shutterstock.com.
Freedom
Active, willing participation facilitates learning, while coercion, compulsion, and forced participation inhibit it. Reward systems are only effective when they encourage active and engaged participation. Clients who adopt goals and outcomes as their own will develop improved self-motivation and perceived self-efficacy. Graphic © UbjsP/Shutterstock.com.
Resources (Requirement)
Neurofeedback professionals start with skills that are already in a client's repertoire and then progress from there. For example, heart rate variability biofeedback builds on a client's existing breathing skills and then shapes its mechanics and rate. Shaping, the gradual reinforcement of successive approximations of a target behavior, adds new skills to a client's repertoire. Graphic © Robert Kneschke/Shutterstock.com.
Olton and Noonberg (1980) proposed that performance goals should be raised when a client succeeds more than 70% of the time and lowered when a client succeeds less than 30% of the time. Neurofeedback systems incorporate algorithms that automatically revise goals based on the client's performance (e.g., time above threshold) to maintain motivation and ensure sufficient challenge.
Glossary
classical conditioning: an unconscious associative learning process that builds connections between paired stimuli that follow each other in time.
conditioned response (CR): in classical conditioning, a response to a conditioned stimulus (CS). For example, salivation in response to a bell.
conditioned stimulus (CS): in classical conditioning, a stimulus that elicits a response after training. For example, a bell after pairing with food.
discrimination (classical conditioning): response to the original CS, but not to one that resembles it. For example, salivation to a high-pitched bell, but not to a low-pitched bell.
discrimination (operant conditioning): performance of the desired behavior in one context, but not another. For example, increasing sensorimotor rhythm (SMR) activity at bedtime, but not during a morning commute.
discriminative stimuli: in operant conditioning, the identifying characteristics of a situation (the physical environment and physical, cognitive, and emotional cues) that teach us when to perform operant behaviors. For example, a traffic slowdown could signal a client to practice effortless breathing.
EEG artifacts: false signals that masquerade as brain electrical activity.
extinction (classical conditioning): reducing a CR when the UCS no longer follows the CS. For example, less salivation when food no longer follows a bell.
extinction (operant conditioning): a reduction in response frequency when the desired behavior is no longer reinforced. For example, a client practices less when the clinician ceases to praise this behavior.
generalization (classical conditioning): response to stimuli that resemble the original CS. For example, salivation to both a low- and high-pitched bell.
generalization (operant conditioning): performance of the desired behavior in multiple contexts. For example, increasing low-beta activity during both classroom lecture and golf practice.
habituation: nonassociative learning phenomenon in which responses to unchanging and harmless stimuli decrease.
learning: the process by which we acquire new information, patterns of behavior, or skills.
negative punishment: in operant conditioning, learning by observing others. For example, a child’s oppositional behavior could result in a clinician turning off a popular game.
negative reinforcement: in operant conditioning, a process that increases the frequency of the desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on acting. For example, an athlete’s anxiety decreases by shifting from high beta to low beta, rewarding this self-regulation.
neutral stimulus (NS): in classical conditioning, a stimulus that does not elicit a response. For example, a bell before pairing with food.
nonassociative learning: a simple learning process in which the strength of the response to a stimulus changes with repeated exposure.
observational learning: learning by observing others. For example, a fitness client learns to stretch by watching a personal trainer demonstrate the technique.
operant conditioning: an unconscious associative learning process that modifies an operant behavior, voluntary behavior that operates on the environment to produce an outcome by manipulating its consequences.
positive punishment: in operant conditioning, a process that decreases or eliminates an undesirable behavior by associating it with unwanted consequences. For example, a child's increased fidgeting dims a favorite movie and lowers the sound.
positive reinforcement: in operant conditioning, a process that decreases or eliminates an undesirable behavior by associating it with unwanted consequences. For example, a movie plays when a client increases low-beta and decreases theta activity.
sensitization: nonassociative learning phenomenon in which there is an exaggerated reaction to diverse stimuli following exposure to a single powerful stimulus.
spontaneous recovery: in classical conditioning, the reappearance of an extinguished CR following a rest period. For example, salivation following its disappearance.
stimulus discrimination: in classical conditioning, when a conditioned response (CR) is elicited by one conditioned stimulus (CS) but not by another. For example, your blood pressure increases during a painful dental procedure but not during an uncomfortable blood draw.
stimulus generalization: in classical conditioning, when stimuli that resemble a conditioned stimulus (CS) elicit the same conditioned response (CR). For example, when your blood pressure increases during a painful dental procedure and an uncomfortable blood draw.
unconditioned response (UCR): in classical conditioning, a response to an UCS that elicits a response without training. For example, salivation in response to food.
unconditioned stimulus (UCS): in classical conditioning, a stimulus that elicits a response without training. For example, food.
REVIEW FLASHCARDS ON QUIZLET
Click on the Quizlet logo to review our chapter flashcards.
Assignment
Now that you have completed this unit, which sounds do you prefer when you have succeeded during neurofeedback training? Which visual displays are more motivating for you?
References
Albino, R., & Burnand, G. (1964). Conditioning of the alpha rhythm in man. Journal of Experimental Psychology, 67(6), 539-544.
Cacioppo, J. T., & Freberg, L. A. (2016). Discovering psychology (2nd ed.). Cengage Learning.
Clemente, C. D., Sterman, M. B., & Wyrwicka, W. (1964). Post-reinforcement EEG synchronization during alimentary behavior. Electroencephalography Clinical Neurophysiology, 355-365.
Cooper, J., Heron, T., & Heward, W. (2019). Applied behavior analysis (3rd ed.). Pearson Education.
Durup, G., & Fessard, A. I. (1935). Blocking of the alpha rhythm, L'ann'ee Psychologique, 36(1), 1-32.
Felsinger, J. M., & Gladstone, A. I. (1947). Reaction latency (StR) as a function of the number of reinforcements (N). Journal of Experimental Psychology, 37(3), 214-228.
Grice, G. R. (1948). The acquisition of a visual discrimination habit following response to a single stimulus. Journal of Experimental Psychology, 38(6), 633-642,
Jasper, H., & Shagass, C. (1941). Conditioning the occipital alpha rhythm in man. Journal of Experimental Psychology, 28(5), 373-387.
Kamiya, J. (2011). The first communications about operant conditioning of the EEG, Journal of Neurotherapy, 15(1), 65-73.
Knott, J. R. (1941). Electroencephalography and physiological psychology: Evaluation and statement of problem. Psychological Bulletin, 38(10), 944-975.
Loomis, A. L., Harvey, E. N., and Hobart, G. (1936). Electrical potentials of the human brain. Journal of Experimental Psychology, 19, 249.
Malott, R. W., & Shane, J. T. (2013). Principles of behavior (7th ed.). Pearson Prentice Hall.
Miller, L. K. (2006). Principles of everyday behavior analysis (4th ed.). Wadsworth,
Miltenberger, R. G. (2016). Behavior modification: Principles and procedures. Cengage Learning.
Olton, D. S., & Noonberg, A. R. (1980). Biofeedback: Clinical applications in behavioral medicine. Prentice-Hall, Inc.
Pavlov, I. P. (1927). Conditioned reflexes. Oxford University Press.
Sherlin, L. H., Arns, M., Lubar, J., Heinrich, H., Kerson, C., Strehl, U., & Sterman, M. B. (2011). Neurofeedback and basic learning theory: Implications for research and practice. Journal of Neurotherapy, 15, 202-304. doi:10.1080/10874208.2011.623089
Sterman, M. B., LoPresti, R. W., & Fairchild, M. D. (1969). Electroencephalographic and behavioral studies of monomethyl hydrazine toxicity in the cat. Technical Report AMRL-TR-69-3, Wright-Patterson Air Force Base, Ohio, Air Systems Command.
Thorndike, E. L. (1913). Educational psychology: Briefer course. Teachers College.
Tracy, M. (2018). Personal communication regarding principles of learning.
Travis, L. E., & Egan, J. P. (1938), Conditioning of the electrical response of the cortex. Journal of Experimental Psychology, 22(6), 524-531.
Wyrwicka, W., & Sterman, M. B. (1968). Instrumental conditioning of sensorimotor cortex EEG spindles in the waking cat. Physiology and Behavior, 3(5), 703-707.
D. ASSUMPTIONS UNDERLYING NEUROFEEDBACK
This unit covers Concepts of Feedback and Control, Basic Psychophysiology of Stress, and Basic Physiology of Attention.
Biofeedback is a learning process like learning to play a musical instrument or a videogame. In biofeedback, an individual interacts with a device (usually electronic) that monitors and feeds back information about physiological activity. For example, a child uses a strategy (instructs the body to remain still), observes the results (SMR increases and high beta decreases), and repeats this action throughout the day.
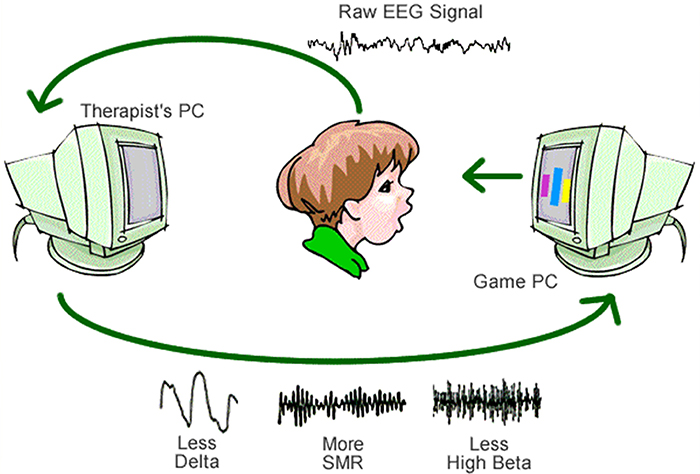
We can think of biofeedback as a "psychophysiological mirror" that teaches individuals to monitor, understand, and change their physiology (Peper, Shumay, & Moss, 2012).
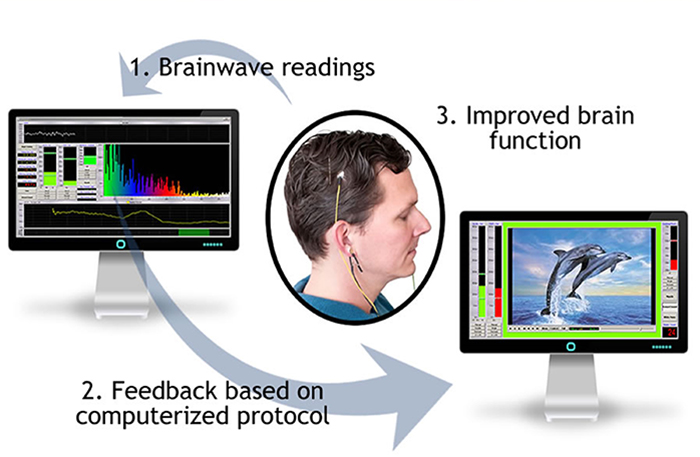
Biofeedback training aims to teach self-regulation, which is control of behavior without feedback.
For example, a client could use a mirror or a position sensor on their back (e.g., biofeedback) to practice keeping the chin level. When they have practiced sufficiently to achieve good posture without reminders, this shows that they have achieved self-regulation. Biofeedback training is a bridge to self-regulation. Graphic © fizkes/Shutterstock.com.
Biofeedback is information that can be used to guide and improve performance.
While biofeedback training is a powerful intervention in clinical disorders, it is increasingly used to promote optimal performance. Graphic © LDprod/Shutterstock.com.

Biofeedback training may be more effective when training promotes mindfulness. Mindfulness involves "paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally" (Kabat-Zinn, 1994). A mindfulness approach teaches clients to focus on their immediate feelings, cognitions, and sensations in an accepting and non-judgmental way, to distinguish between what can and cannot be changed, and to change the things they can (Khazan, 2013). Mindfulness guides the trial-and-error process underlying self-regulation by helping clients draw connections between their actions, internal feedback, and results. Graphic © fizkes/Shutterstock.com.

Clients can become stuck when they focus on outcomes they cannot immediately control. For example, Jane was diagnosed with elevated blood pressure. When she measured her pressure several times a day, her anxious attention increased these values and amplified her anxiety. Heightened anxiety, in turn, interfered with her practice of slow-paced breathing. She could not focus on his breathing while she worried about her hypertension. Her blood pressure gradually decreased when Jane learned to accept her high blood pressure without fear, reduce her measurement frequency to once a day, and focus entirely on healthy breathing. Jane succeeded by changing what she could; her breathing pattern. Graphic © Ivelin Radkov/Shutterstock.com.
A comprehensive view of health and optimal performance recognizes the importance of the interconnected domains of body, mind, and spirit. In this context, spirit can mean philosophical beliefs or soul. Graphic © Gustavo Frazao/Shutterstock.com.

Neurofeedback, which is also called EEG biofeedback, is the process of interacting with an electronic device that measures and feeds back information about brain electrical activity via brainwave information. This process aims to ensure effective regulation by the neuromodulating systems of the brain, encourage global neurophysiological change, and correct specific, distinct, and identifiable disorders due to underlying dysregulation.

What does neurofeedback do? Neurofeedback provides accurate, timely, and useful information to the client. This information is displayed using visual, auditory, or tactile feedback that corresponds to meaningful changes in the monitored systems. Neurofeedback training encourages flexibility, resilience, and choice.
Neuroplasticity, the ability of neurons and their networks to remodel themselves in response to experience, makes neurofeedback training possible (Breedlove & Watson, 2020). The learning mechanisms that underlie neurofeedback training depend on interrelated structural and functional changes. Neuroplasticity involves alterations in transmitter release and binding, modulation of transmitter release by interneurons, the formation and elimination of synapses, selecting among competing neural pathways, and strengthening and weakening the connectivity between brain regions.
BCIA Blueprint Coverage
This unit addresses I. Orientation to Neurofeedback - D. Assumptions underlying neurofeedback.
This unit covers Concepts of Feedback and Control, Basic Psychophysiology of Stress, and Basic Physiology of Attention.
Concepts of Feedback and Control
Both biofeedback and neurofeedback are based on concepts of feedback and control found in cybernetic theory. Two everyday examples of feedback and control are radar speed displays and handheld thermometers.
A radar speed display shows motorists how closely their speed matches the posted limit. This example illustrates the concept of biofeedback. The device displays information about an activity (speed) back to an individual (a driver) to (hopefully) change speeding behavior. A reward occurs when the display stops and shows the correct speed. Graphic ©Tada img/Shutterstock.com.

Handheld thermometers give you direct, bidirectional feedback (information) about your finger temperature, allowing you to practice increasing hand temperature.

Cybernetic Model
The cybernetic model proposes that "biofeedback is like a thermostat." The term biofeedback originated in cybernetic theory. Learning self-regulation requires accurate feedback about our physiology (Annett, 1969). Graphic © Maridav/Shutterstock.com.
The components of a thermostat system include a setpoint or goal (75° F/ 23.9° C), system variable or what is controlled (room temperature), negative feedback or corrective instructions (commands to change furnace output), and positive feedback or instructions to continue action (orders to continue furnace output).
The internal environment fluctuates around a setpoint and is never
stationary. This allows rapid adaptation to changing activity levels and
environmental conditions. Homeostasis is
a state of dynamic constancy achieved by stabilizing
conditions above and below a setpoint, which may change over time. From
the perspective of the cybernetic model, biofeedback training supplements
a client's proprioception to bring a malfunctioning biological system
variable (blood pressure) under better control (Fox, 2019).
Homeostasis depends on sensory systems (networks that monitor system
variables) to detect an actual or anticipated
change in physiological processes (temperature), an
integrating center,
which receives input from many sensors, and multiple effector systems
(control systems) to
adjust physiological processes.
The body maintains dynamic constancy through continuous negative feedback
loops amplified by positive feedback and antagonistic effectors.
Negative feedback loops produce corrective changes when a physiological
variable is outside an acceptable range. For example, we initiate
clotting to stop blood loss from a wound.
Positive feedback loops amplify the changes produced by negative feedback.
For example, activating one clotting factor activates others to create
a blood clot.
Push-pull control by effectors that produce antagonistic effects achieves
more precise control than turning a single effector on or off. For
example, a sympathetic nerve accelerates the heart while the
parasympathetic vagus nerve slows the heart.
BASIC PSYCHOPHYSIOLOGY OF STRESS
Stress can be confusing since it can refer to a stimulus, response, a transaction. The stress response is multidimensional, there are multiple stress responses, and individuals often show a characteristic response pattern. The conceptualization of the stress response as nonspecific is misleading since clients may have unique stress triggers (time pressure) and specific psychophysiological changes (blood pressure spikes).
While early theories of stress emphasized the role of stimuli, more recent theories focus on our cognitive appraisal of events and coping resources. The biopsychosocial model has replaced the aging biomedical model due to its greater comprehensiveness and support for interdisciplinary treatment of disorders. Likewise, the allostatic load model has replaced Selye's General Adaptation System framework for understanding the role of stress in disease. Graphic © Arseniy Krasnevsky/Shutterstock.com.

Chronic stress reduces heart rate variability (HRV). "HRV is the organized fluctuation of time intervals between successive heartbeats defined as interbeat intervals" (Shaffer, Meehan, & Zerr, 2020). We measure the time intervals between successive heartbeats in milliseconds. Graphic courtesy of Dick Gevirtz.
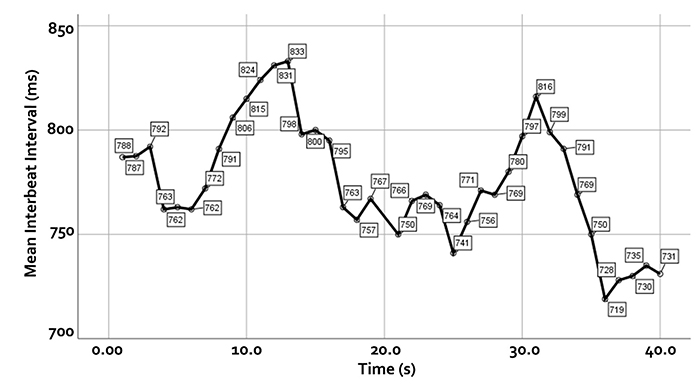
HRV is crucial to health, performance, and resilience. Low HRV is a marker for cardiovascular disorders, including hypertension, especially with left ventricular hypertrophy; ventricular arrhythmia; chronic heart failure; and ischemic heart disease (Bigger et al., 1995; Casolo et al., 1989; Maver et al., 2004; Nolan et al., 1992; Roach et al., 2004). Low HRV predicts sudden cardiac death, particularly due to arrhythmia following myocardial infarction and post-heart attack survival (Bigger et al., 1993; Bigger et al., 1992; Kleiger et al., 1987).
Reduced HRV may predict disease and mortality because it indexes reduced regulatory capacity, which is the ability to surmount challenges like exercise and stressors. Patient age may be an essential link between reduced HRV and regulatory capacity since both HRV and nervous system function decline with age (Shaffer, McCraty, & Zerr, 2014).
Stressors and Stress
Cannon (1939) studied how environmental stressors like cold temperatures and loss of oxygen trigger a fight-or-flight response. He conceptualized stress as the disruption of homeostasis when the body mobilizes the sympathetic nervous system and endocrine system to deal with external threats.

Selye (1956) also studied environmental challenges to homeostasis. He referred to stress (and strain) as emotional and physiological responses to stimuli called stressors.
Listen to a mini-lecture on Stressors and Stress © BioSource Software LLC.
Selye conceptualized stress as a nonspecific response.
Selye conceptualized these responses as nonspecific since many stimuli can produce the same physiological changes. He theorized that negative and positive stimuli could provoke stress responses requiring coping resources. He termed stress due to aversive stimuli, distress, and positive events, eustress (Moksnes & Espnes, 2016).The Yerkes-Dodson curve graphs the relationship between stressors and performance. The left side of the inverted U-curve depicts an underload where an individual is insufficiently challenged and bored. This phenomenon of low motivation and performance has been termed rust out and reminds us that we require stressors for motivation and creativity (O'Dowd, 1987). The middle region that ends with peak performance corresponds to eustress. An optimal level of challenge promotes focus, motivation, and creativity. The right side of the curve represents the worsening effects of excessive pressure, overload, and burn-out with anxiety, panic, and anger. Graphic © Olivier Le Moal/Shutterstock.com.
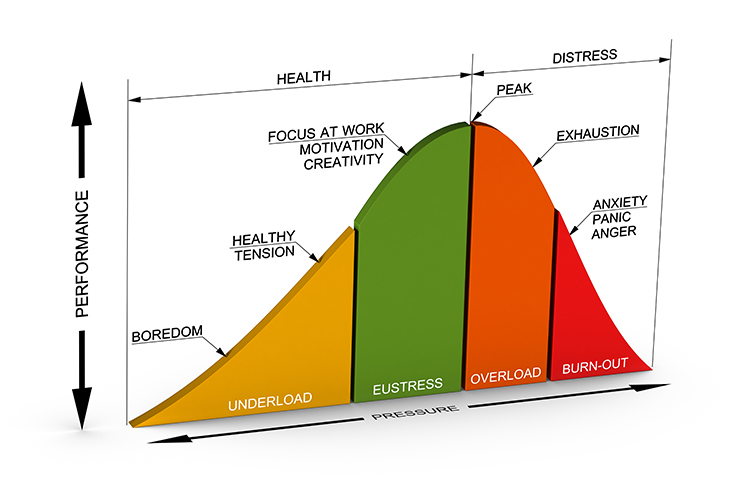
Evaluation
Selye's model excluded psychological factors like appraisal. His assumption that stress involves nonspecific physiological changes is incorrect. All stressors do not produce a uniform endocrine stress response. Instead, stressors can change multiple body systems in response to stressor intensity, biological predisposition, cognitive appraisal, perceived support, and emotional response (Mason, 1971, 1975; McEwen, 2005; Taylor, 2021). Finally, whereas Selye proposed that our stress responses attempt to maintain physiological processes within a narrow optimal range, current research focuses on adaptation (e.g., allostatic load model) instead of set points (Brannon et al., 2022).
The Stress Response Is Multidimensional
The human stress response is multidimensional and involves diverse systems, ranging from the central nervous system to the immune system. Each person uniquely responds to stressors. This individualized pattern is called response stereotypy. Individuals differ in the systems impacted, their activation or suppression, and how these changes affect health. While stressors can produce system-wide macroscopic changes like increased blood pressure, they can also cause epigenetic changes that alter DNA expression. Graphic © Sergey Nivens/Shutterstock.com.

Sympathetic and Parasympathetic Responders
Two modal patterns of autonomic response to stressors have been observed. A sympathetic responder may
increase blood pressure, heart rate, and sweat gland activity and decrease heart rate variability and peripheral
blood flow. These changes may result from increased sympathetic activation, decreased parasympathetic
activation called parasympathetic withdrawal, or a combination of both. Listen to a mini-lecture on Sympathetic and Parasympathetic Responders © BioSource Software LLC.
In contrast, a parasympathetic responder may increase digestive activity, constrict the lungs' alveoli, and faint from low blood pressure.
Individuals can react to stressors with elements of both autonomic patterns. For example, they can increase heart rate and blood pressure (sympathetic) while experiencing the gastrointestinal symptoms of diarrhea and gas (parasympathetic).
Hawks and Doves
Individuals differ in their behavioral activation when confronted by a stressor. While behavior is activated in the "fight-or-flight" response, it is suppressed in the "freeze-hide" response. The dazed young man illustrates passive parasympathetically-mediated freezing. Graphic © Dean Drobot/Shutterstock.com.
Evolutionary biologists have called active and passive responses "hawk" and "dove" strategies. Graphic © jimkruger/ iStockphoto.com.

Hawks are described as "proactive and bold," while doves are passive, reactive, nonaggressive, and cautious. Hawks appear to utilize the "fight-or-flight" response and activate the sympathetic-adrenomedullary (SAM) pathway. Doves, in contrast, activate the hypothalamic-pituitary (HPA) axis (Woolfolk et al., 2007).
Men and women may respond differently to stressors. Studies of hormonal secretion during sports competition (Kivlinghan et al., 2005) and children's reactions to threatening behavior by their mothers (David & Lyons-Ruth, 2005) support the hypothesis that men are more likely to flee while women prefer to affiliate. Graphic © lassedesignen/Shutterstock.com.

Stress-related disorders are more prevalent in women than men in the US (Gaidos, 2016).
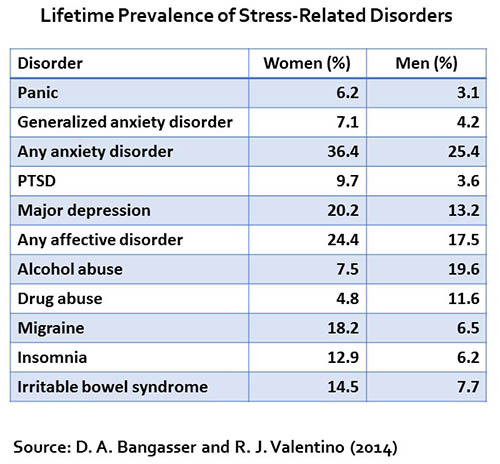
Biopsychosocial Model
Engel's (1977, 1980) biopsychosocial model proposes that the complex interplay of psychological, biological, and sociological factors results in health or illness.
In this model, stress is a psychological risk factor that affects and is influenced by an individual's biology and sociology. The biopsychosocial model challenges the biomedical model that illness is primarily due to biological abnormalities, which has influenced medical practice since the 1700s (Taylor, 2012). A clinician who adopts the biopsychosocial model assumes that health depends on all three factors. When treating illness, these factors must be assessed and addressed using an interdisciplinary approach (Schwartz, 1982).
The illustration below was adapted from Brannon et al. (2022).
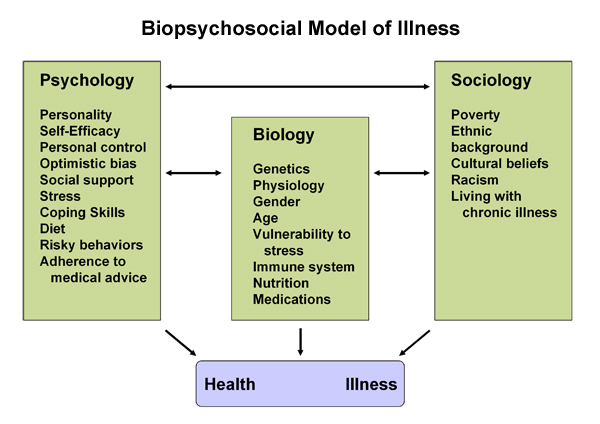
Evidence supporting the biopsychosocial model includes increased psychological and medical disorders in divorced and bereaved persons (Schneider, 1984).
Allostatic Load Model
Allostasis, which means achieving stability through change, involves matching type (sympathetic or parasympathetic) and intensity of physiological activation to situational demands (Brannon et al., 2022).
McEwen and Seeman's (1999) allostatic load model proposes that biological responses to stress (e.g., cortisol secretion or elevated glutamate transmission) can harm the body when stressors are acute or repeatedly occur. Over time, the stress response itself may overwhelm the body's adaptive capacity.

Caption: Bruce McEwen
Allostatic load can produce growing changes during childhood, increasing health risks across the life cycle (Wiley et al., 2016). It can prematurely age the body. Chronic stress may suppress cell-mediated immunity, reduce hippocampal control of cortisol during stress, lower heart rate variability (HRV), raise plasma epinephrine, increase the waist-to-hip ratio, reduce hippocampal volume, impair cognitive performance (e.g., memory), increase plasma fibrinogen, raise blood pressure, and increase the risk of illness and death (Juster et al., 2010; Karlamangla et al., 2006; McEwen & Gianaros, 2010). Table adapted from Seeman et al. (1997) and Taylor (2021).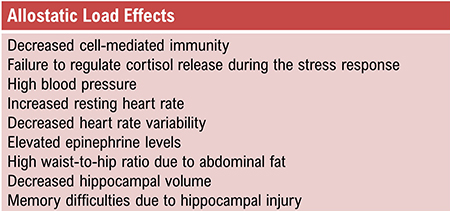
Researchers have linked high allostatic load to illness in children and the elderly (Johnston-Brooks et al., 1998; Seeman et al., 1997). The damage produced by allostatic load can be amplified by decreased healthy behaviors (e.g., exercise) and increased unhealthy behaviors (e.g., binge drinking and smoking) (Ng & Jefferey, 2003).
Check out Sapolsky's superb National Geographic YouTube video Stress, Portrait of a Killer.
Stress-Diathesis Model
The stress-diathesis model explains that stressors interact with our inherited or acquired biological vulnerabilities, diatheses, to produce medical and psychological symptoms. From this perspective, disease results when an individual is predisposed to disease and experiences stress. Life event scales like the SRRS and USQ may achieve low predictive validity because they only and incompletely assess stress; they do not evaluate illness vulnerability (Marsland et al., 2001).
The interrelationship among stress, insomnia, and depression illustrates the stress-diathesis model. Sleep reactivity, the tendency for sleep to be disrupted by stress, appears to be a shared vulnerability in insomnia and depression. Greater sleep reactivity produces insomnia, and insomnia contributes to depression. Chronic insomnia can also increase blood pressure, blood sugar levels, and weight (Drake et al., 2014).
System-Wide Effects of Stress
Stress and the Microbiome
The human body primarily comprises single-celled organisms, which outnumber our human cells 1.3-to-1 (Sender et al., 2016). Viruses vastly outnumber bacteria and could sharply increase microbe-to-human cell ratio (Saey, 2016). Most human bacteria are located in our gut. The human microbiome is the collection of microorganisms that reside in our bodies. Graphic © Kateryna Kon/Shutterstock.com.
Research using rodents suggests that the 40 trillion bacteria in our microbiome may influence brain development, neurotransmitter synthesis, emotions, pain thresholds, and response to stressors. In rodents, shifts in the microbiome's ecology can produce more exploratory or cautious behavior.
Listen to a mini-lecture on the Microbiome © BioSource Software LLC.
The relationship between the brain and gut biome appears to be bidirectional. While the brain and gut microbiome probably communicate using several pathways, the 100 million enteric system neurons which regulate the GI tract may prove to be a crucial nexus. Mild stress can reduce the number of beneficial bacteria. Severe chronic stress might contribute to the development of disease. While researchers struggle to define a healthy gut microbiome's characteristics, evidence suggests that disorders like anxiety and depression may be associated with abnormal microbiota (Carpenter, 2012).
Stress Accelerates Aging
Epel and colleagues (2004) studied 58 healthy women who cared for either healthy or chronically ill children. The researchers administered a brief questionnaire that assessed chronic stress during the previous month and obtained a blood sample to measure telomere (DNA and protein that cover the ends of chromosomes), length, and levels of telomerase (an enzyme that adds DNA to telomeres). Graphic © Designua/Shutterstock.com.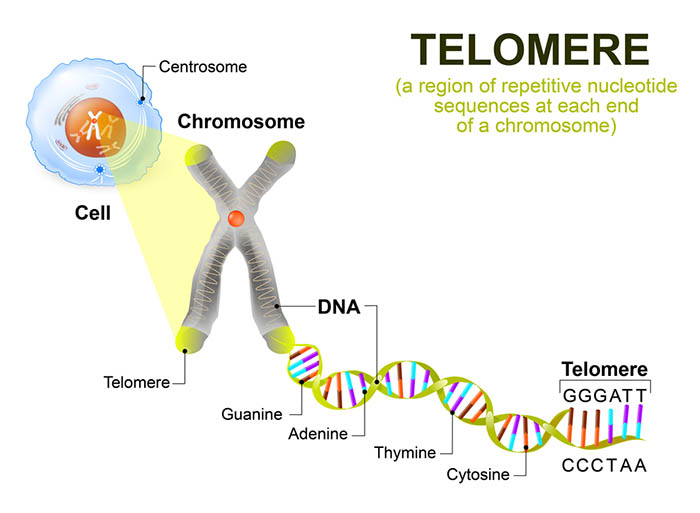
With repeated cell division, telomere DNA is lost, the telomere shortens, and eventually, cell division stops. When cells age, telomerase activity declines, and the telomere shortens. Graphic © koya979/ Shutterstock.com.
The researchers found that the mothers of chronically ill children reported higher chronic stress levels than mothers of healthy children. More years of caring for chronically ill children were correlated with shorter telomeres and lower telomerase levels. Perceived levels of chronic stress—and not a child's actual health status—predicted telomere length. The researchers calculated that the cells of high-stress mothers had aged 9 to 17 more years than those of the low-stress mothers.
Stress May Contribute to Mild Cognitive Impairment
Older adults enrolled in the Einstein Aging Study who reported high stress levels were twice as likely to exhibit the memory deficits associated with mild cognitive impairment (MCI), which may precede Alzheimer's (Katz et al., 2015).Stressful Life Events
Cataclysmic Events
Lazarus and Cohen (1977) described cataclysmic events as "sudden, unique, and powerful single life-events requiring major adaptive responses from population groups sharing the experience” (p. 91).Intentional and unintentional, these events can impact local communities (e.g., mass shootings), geographic regions (e.g., earthquakes, fires, hurricanes, and tsunamis), and the entire planet (e.g., the COVID-19 pandemic. These catastrophes can produce death, dislocation, fear, grief, trauma, and Post-Traumatic Stress Disorder. Graphic © Syda Productions/Shutterstock.com.

Many factors influence survivor response to these powerful stressful events, including perceived discrimination, resources, support, vulnerability to future harm, distance from the devastation, and media coverage. The stressfulness of an event is influenced by geographic proximity, its recency, and whether it was intended. Intentional events are more traumatic than natural disasters because the perpetrators targeted the victims and could do so again (Brannon et al., 2022).
Life Events
Cataclysmic events like a pandemic are so disruptive become they change our lives in various ways: education, employment, exercise, personal, family member, and friend illness, routines, sleep, social interaction, and working conditions.Life events differ from cataclysmic events in three ways. They affect fewer individuals. They require adjustment, whether positive (e.g., the birth of a child) or negative (e.g., the death of a loved one). Last, they can develop more slowly (e.g., divorce) or suddenly (e.g., injury in a car crash).
Holmes and Rahe (1967) measured major positive and negative life changes using their Social Readjustment Rating Scale (SRRS). The scale lists 43 events, each assigned a different Life Change Unit (LCU) value. They arranged these events in descending order from the death of a spouse (100 LCUs) to minor law violations (11 LCUs). Individuals select the events they have experienced within the last 6 to 24 months. Researchers calculate a stress score by summing the LCU value of the checked events.
Studies that combine prospective (subjects report current events) and retrospective methods (researchers examine subsequent health records) have reported increased illness and accidents following increased stressful events (Johnson, 1986; Rahe & Arthur, 1978). However, the correlation between SRRS scores and disease is around + 0.30 (Dohrenwend & Dohrenwend, 1984), which means that the SRRS accounts for only 9% of the variance in disease.
Listen to a mini-lecture on the Effects of Major Life Changes and Hassles © BioSource Software LLC.
The SRRS has received severe criticism, and its popularity has declined. Critics have argued that its positive events can reduce the risk of illness (Ray, Jefferies, & Weir, 1995). Many individuals who exceed 300 points in a year remain healthy. Scales like the SRRS underestimate African-American life stress (Turner & Avison, 2003). The SRRS assumes that an event impacts all people equally. The wording of some items is vague (e.g., "change in responsibilities at work"). Pessimism can distort recollections of life events (Brett et al., 1990). Finally, the scale does not consider whether an event has been resolved (Turner & Avison, 1992) or an event's controllability or probability (Gump & Matthews, 2000).
The Undergraduate Stress Questionnaire (USQ) developed by Crandall and colleagues (1992) instructs students to select events—mostly hassles—they have experienced during the past two weeks. Higher USQ scores are associated with increased use of health services.
The Perceived Stress Scale (PSS) developed by Cohen and colleagues (1983) measures perceived hassles, major life changes, and shifts in coping resources during the previous month using a 14-item scale. PSS items assess the degree to which respondents rate their lives as unpredictable, uncontrollable, and overloaded (p. 387). The PSS achieves good reliability and validity (Brannon et al., 2022). PSS scores predict cortisol levels (Harrell et al., 1996), fatigue, headache, sore throat (Lacey et al., 2000), and immune changes (Maes et al., 1997).
Hassles and Uplifts
A hassle is a minor stressful event like waiting in a checkout line or experiencing a traffic jam. Hassles can produce illness via several pathways. First, hassles can cause accumulating allostatic load. Second, hassles can amplify the effects of adverse life events and chronic stress (Marin et al., 2007; Serido et al., 2004; Taylor, 2021). Graphic © Dmitry Kalinvosky/Shutterstock.com.
Graig's (1993) concept of urban press illustrates how ever-present environmental stressors (e.g., alienation, crowding, fear of crime, noise, and pollution) acting in concert as daily hassles can increase death from heart attacks (Christenfeld et al., 1999). As with stressors in general, an individual's perception of daily hassles like noise and population density determines their effects on behavior, health, and performance (Brannon et al., 2022; Evans & Stecker, 2004; Schell & Denham, 2003). For example, crowding is our perception of density, influenced by our perceived degree of control. Graphic © Wachiwit/Shutterstock.com.

Discrimination experienced in the classroom, community, family, media, and workplace is another source of daily hassles. Discrimination based on age, biological sex, ethnicity, gender identity, and religion can disadvantage and physically endanger individuals and threaten their mental and physical health (Brannon et al., 2022; Pascoe & Richman, 2009; Troxel et al., 2003). Discrimination has elevated the risk of suicide in the bisexual, gay, lesbian, and transgender communities (Haas et al., 2011). Further, Anti-Asian hate has resulted in a wave of attacks against Asian Americans. Graphic © CNN.

The framework of intersectionality proposes that social identities (e.g., biological sex, class, gender identity, and race) interact to produce discrimination, disadvantage, or advantage. For example, a white woman with a disability may encounter sexism and ableism, while a Black transgender woman with the same disability may experience the former discrimination and transphobia. Their lived experiences will differ because their unique identities intersect, creating different patterns of discrimination and access barriers (Surrey Place-Staff, 2021). Graphic courtesy of Womankind Worldwide.
An uplift is a minor positive event like receiving an unexpected call from a friend or playing with new puppies. Graphic © Orientgold/Shutterstock.com.

Kanner and colleagues (1981) developed a 117-item Hassles Scale and 138-item Uplifts Scale to measure negative and positive daily experiences. Respondents selected the hassles and uplifts they experienced during the previous month. Next, they rated the degree to which they experienced each selected item on a 3-point scale to assess their perception of each stressor. They found a moderate correlation between hassles and major life changes. Lazarus (1984) reported that the Hassles Scale better predicted psychological health than major life changes.
DeLongis and colleagues (1988) replaced the Hassles and Uplifts Scales with a 53-item revised Hassles and Uplifts Scale. Respondents selected the items they experienced that day and rated each item using a 4-point scale (none to a great deal). The revised Hassles Scale better predicted headache frequency and intensity (Fernandez & Sheffield, 1996) and inflammatory bowel disease frequency (Searle & Bennett, 2001) than the Social Readjustment Rating Scale. Consistent with Lazarus's emphasis on the appraisal of events, the perceived intensity of hassles better predicted headache symptoms than the number of hassles.
The interaction between hassles and chronic stress is complex. Hassles may increase the psychological distress produced by chronic stress (Serido et al., 2004). Conversely, chronic stress may reduce the effects of hassles by placing them in perspective (McGonagle & Kessler, 1990).
Hardiness
Some individuals do not experience illness or psychological distress when exposed to adverse life events and hassles. Although they may experience brief distress, they generally recover (Lehrer, 2021). Researchers use the concept of hardiness to explain these outliers (Maddi, 2017; Maddi et al., 2017; Pitts et al., 2016; Stoppelbein et al., 2017). Graphic ©lassedesignen/Shutterstock.com.
The hardiness concept emerged from a 12-year study of manager stress responses at the Illinois Bell Company (Maddi, 1987). Halfway through the study, their parent company's reorganization eliminated half their employees within a year. Two-thirds of the managers experienced severe stress reactions (e.g., heart attacks, depression, and suicide), and one-third thrived. The investigators concluded that the hardy managers were protected by attitudes of commitment (strong involvement), control (internal locus of control), and challenge (learning from experience and accepting change).
Hardiness involves biological (McVicar et al., 2014; Oken et al., 2015; Parkash et al., 2017) and social factors (Kuzman & Konopak, 2016; Zeer et al., 2016). Longitudinal studies suggest that infants' autonomic and emotional reactivity predicts later emotional reactivity (Berry et al., 2012; Cohen, 1989; Raby, 2016; Wagner et al., 2017). Less reactive infants may become more resilient. In addition, cohesiveness and social support (actual and perceived) may buffer hardy individuals against stressors. Graphic © Nina Buday/Shutterstock.com.

Psychological Factors in Stress
Traumatic Stress and Post-Traumatic Stress Disorder (PTSD)
Traumatic stress is produced by a highly intense stressor that disrupts coping and endangers ourselves or others. Post-Traumatic Stress Disorder (PTSD) is a severe and long-lasting trauma and stressor-related disorder that often develops within three months of a traumatic event. DSM-5 (APA, 2013) divides its symptoms into four clusters: intrusion, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity. Graphic © John Gomez/Shutterstock.com.
The exposure can also be second-hand, such as witnessing domestic violence or learning about a family tragedy (Crider, 2004; Lamprecht & Sack, 2002). The lifetime prevalence of adult PTSD in the United States is about 6.8% (Kessler et al., 2005).
While the earliest model of PTSD focused on trauma during combat, subsequent research has shown that crime, domestic violence, natural disasters, sexual assault, and terrorism can precipitate PTSD symptoms. Since women are more likely than men to experience these stressful events, it should not be surprising that they are more often diagnosed with this disorder (Stein et al., 2000). Children and adolescent victims and witnesses of violence also share an elevated risk of PTSD (Silva et al., 2000).
A single traumatic event can reshape synapses and increase electrical activity in the amygdala 10 days later. The N-methyl-D-aspartate receptor (NMDA-R) protein, which plays a central role in long-term memory, mediates these changes (Yasmin et al., 2016). Amygdala graphic © Kateryna Kon/ Shutterstock.com.
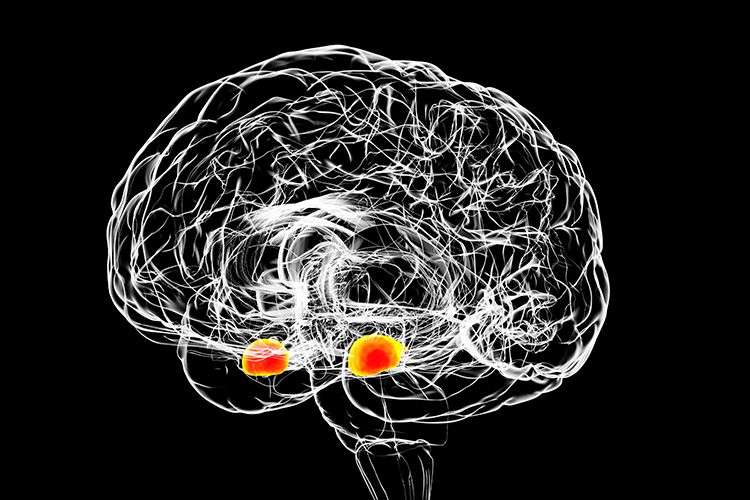
Children with depression experience trauma (35 percent) and bullying (29 percent) (Advokat, Comaty, & Julien, 2014). Graphic © fasphotographic/Shutterstock.com.

Intentional acts may produce more widespread distress than natural disasters because they threaten future and more devastating attacks. The impact of a catastrophic event depends on your distance from the event, the time interval since the event, and the perpetrators' perceived intentions (Brannon et al., 2022).
PTSD can permanently damage the systems that regulate our stress response, particularly the amygdala and hypothalamic-pituitary-adrenal (HPA) axis. Patients experience increased cortisol level fluctuation and persistent epinephrine, norepinephrine, testosterone, and thyroxin elevation (Taylor, 2006).
PTSD may promote medical illness through persistent immunosuppression (Kawamura et al., 2001). Military veterans diagnosed with PTSD have a greater risk of developing severe diseases following discharge than veterans without PTSD (Deykin et al., 2001). PTSD may also exacerbate pre-existing health problems. PTSD resulting from the September 11, 2001, World Trade Center attacks may have helped worsen asthmatic symptoms in New York residents (Fagan et al., 2003).
Negative Affect States and Affectivity
From a mindfulness perspective, we should not consider emotional responses like depression as negative but as difficult emotions. A clinician would encourage clients to accept depressed feelings as part of themselves without judgment and to focus on specific behaviors that can be changed (Khazan, 2013).Stressors can trigger complex adjustments, including challenging affective states (anxiety) and corresponding psychophysiological changes (decreased HRV). Barrett and Russell's (1998) structural model represents each affective state within a circumplex based on its degrees of affective valence (unpleasant to pleasant) and affective intensity (activation to deactivation). Affective states fall inside or along the surface of this circular structure. Diagram adapted from Russell and Barrett (1999).
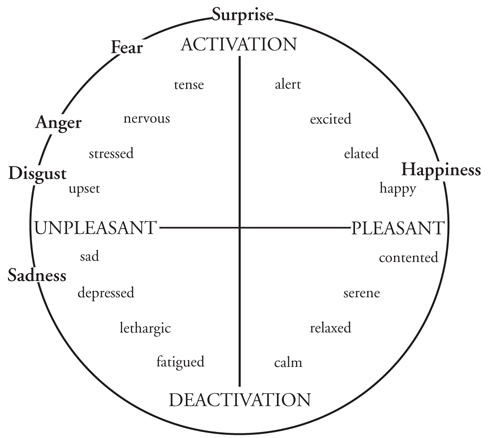
Negative states (sad) are located in the left hemisphere, and positive states (contented) are located in the right hemisphere. Activated states (tense) are placed in the top hemisphere and deactivated states (fatigued) are placed in the bottom hemisphere. While adjacent affective states (stressed and nervous) most resemble each other, those 180° apart (stressed and relaxed) are opposites. After clinicians identify their clients' position within the circumplex, they may intervene to shift them to a more appropriate affective state, like relaxed instead of nervous.
Researchers have reported psychophysiological correlates of the affective valence and activation dimensions. Surface EMG (SEMG) and EEG can help assess affective valence. SEMG measurements of the zygomatic (smiling) and corrugator (frowning) muscles are correlated with positive and negative affect (Lang et al., 1993). Higher left/right prefrontal cortex activation ratios are correlated with positive affect, while reverse ratios are correlated with negative affect (Sutton & Davidson, 1997). Sympathetic nervous system modalities like electrodermal activity are associated with affective intensity (Crider, 2004; Lang et al., 1993).
Negative affectivity (neuroticism) is a predisposition toward distress and dissatisfaction. Individuals rated high on this trait negatively perceive themselves, others, and the environment and have a pessimistic perspective. They rank more events as stressful, report more intense stress, complain more frequently about health problems, and report more severe symptoms when physically ill than those with lower negative affectivity (Cohen et al., 1995; Gunthert et al., 1999). Negative affectivity may increase vulnerability to stressors and health conditions like anxiety and depressive disorders they exacerbate (Brannon et al., 2022).
The Type D (distressed) personality combines high levels of negative affectivity and social inhibition. Individuals rated high on this dimension cannot communicate their distress with others. Researchers have studied the relationship between negative emotionality and social inhibition and the Five-Factor Model of Personality. Negative emotionality is positively correlated with Neuroticism, whereas social inhibition is negatively correlated with Conscientiousness and Agreeableness (De Fruyt & Denollet, 2002). Five-Factor Model of Personality adapted from Sarafino et al. (2020).
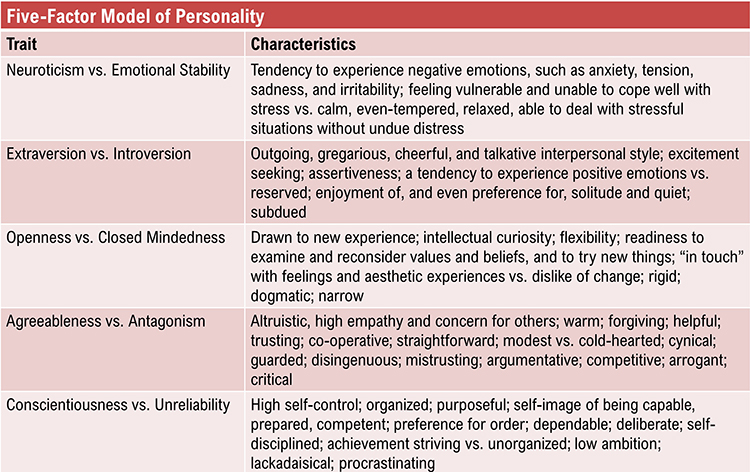
The Type D personality better predicted arterial plaque buildup than the Type A behavior pattern (Lin et al., 2018). However, although initial studies suggested that Type-D coronary artery disease patients have poorer prognoses, later studies (Bishop, 2016; Meyer et al., 2014) have not consistently supported this association.
Anxiety
A Framingham study report by Markovitz et al. (1993) showed that men with elevated anxiety had twice the risk of middle-age hypertension as men with lower anxiety. This increased risk was not found for women. A prospective study by Kawachi et al. (1994) revealed that men diagnosed with phobic anxiety had a three times greater risk of sudden cardiac death. Albert et al. (2005) found that women diagnosed with phobic anxiety had a 59% greater risk of sudden cardiac death and a 31% greater risk of fatal coronary heart disease than women who scored low. These increased risks were associated with risk factors such as diabetes, hypertension, and high cholesterol. Graphic © Malochka Mikalai/ Shutterstock.com.
Depression
Pratt et al. (1996) reported that depressed individuals had a four times greater risk of a heart attack in the next 14 years than non-depressed individuals. Frasure-Smith et al. (1995) found that depressed heart attack patients had a four times greater risk of another heart attack in the next 18 months than non-depressed heart attack patients. Carney et al. (2005) discovered that depressed heart attack patients were almost three times more likely to die over 30 months than non-depressed heart patients. Decreased heart rate variability accounted for a significant share of the increased risk of death.Jonas and Mussolino (2000) found in a 16-year longitudinal study that participants diagnosed with depression had a 70% greater risk of stroke mediated by ethnicity. Stroke risk was higher for depressed European American men than women and depressed African Americans than European Americans. Everson et al. (1998) reported that depressed individuals had a greater risk of death from stroke than nondepressed participants. Graphic © MeganAlter/Shutterstock.com.

Type A-B Continuum
Friedman and Rosenman (1974) proposed the Type A-B continuum of risk for coronary artery disease. They described extreme Type A’s as competitive, concerned with numbers and acquisition, hostile, and time-pressured. In contrast, Type B's are less motivated and do not usually exhibit Type A behaviors. Their study of 3,000 men over 8.5 years showed that Type A behavior doubled the risk of a heart attack. The National Heart Lung and Blood Institute (1981) concluded that Type A behavior is an independent risk for heart disease.Despite early hopes that the global Type A behavior pattern could independently predict heart disease, current research has not consistently supported this association (Brannon et al., 2022; Espnes & Byrne, 2016).
Hostility
Hostility is a negative attitude about others, not an emotion. Hostility is the toxic component of the Type A behavior pattern. In contrast, anger is a difficult emotion associated with physiological arousal. Longitudinal studies suggest a modest predictive relationship between hostility and hypertension (Yan et al., 2003) and cardiovascular disease (CVD; Chida & Steptoe, 2009).Anger and Cardiovascular Reactivity
Hostility is a negative attitude towards individuals—not an emotion—and may persist for long. Taylor (2012) proposed that cardiovascular reactivity (changes in cardiovascular function due to physical or psychological challenge) and hostility in conflict situations might promote heart disease through changes in blood vessels and catecholamine levels, sympathetic nervous system release of lipids into circulating blood, and blood platelet activation.Anger is a difficult emotion that involves physiological arousal and persists for a brief period. Siegman and colleagues (1987) proposed that the expression of anger—and not our experience of it—could result in heart disease. Examples of expressed anger include raising your voice during arguments and temper tantrums (Brannon et al., 2022). Graphic © Oliyy/Shutterstock.com.

Jain and colleagues (1995) monitored patients using an electronic stethoscope. When they were angry, they observed declines in the heart's ejection fraction (the ratio of blood pumped by the left ventricle during a contraction compared to its total filling volume). Bhat and Bhat (1999) demonstrated that an intervention to manage anger using biofeedback significantly increased their patients' ejection fraction.
Expressed anger may contribute to heart disease by increasing cardiovascular reactivity (CVR), often revealed as increased blood pressure and heart rate in response to social stressors like a provocation.
Dujovne and Houston (1991) linked expressed hostility with increased total cholesterol and low-density lipoprotein (LDL) in men and women. Goldman (1996) reported that individuals classified with high anger had a 2.5 times greater chance of re-clogging arteries after angioplasty. Siegman and colleagues (1992) found that training to slow speech rate and lower speech volume reduced CVR.
Researchers have shown that provocation can increase cardiovascular reactivity.
Smith and Brown (1991) found that women showed less CVR than men when provoked. While husbands increased their heart rate and systolic blood pressure while trying to control their wives, they did not experience these changes when trying to control their husbands. The wives' systolic blood pressure only increased when their husbands expressed cynical hostility.
After provoking male undergraduates, Siegman, Anderson, Herbst, Boyle, and Wilkinson (1992) observed increased heart rate and blood pressure (diastolic and systolic). The subjects reported experiencing considerable anger following their provocation.
Fredrickson et al. (2000) asked adult men and women to re-experience earlier anger experiences. More hostile participants produced larger and longer-duration blood pressure increases than less hostile individuals. Also, African Americans showed greater CVR than European Americans.
Bishop and Robinson (2000) studied Chinese and Indian men in Singapore who performed a difficult task either with or without harassment. The harassed participants showed greater CVR than those who were not provoked.
Smith et al. (2004) reported that high-hostile husbands experienced greater cardiovascular reactivity during stressful interactions with their wives than low-hostile husbands.
Suppressed Anger
Diamond (1982) hypothesized an anger-in dimension, which is the tendency to withhold the expression of anger, even when anger is warranted. Dembroski and colleagues (1985) reported that anger suppression could contribute to heart disease. Siegman (1994) recommended that patients develop an awareness of their anger but express it using a quiet, slow voice.Acute and Chronic Stress Responses
Acute Stress
Cannon's fight-or-flight response focuses on sympathetic nervous system responses to an acute stressor and describes the sympathetic-adrenomedullary (SAM) pathway that releases the hormones epinephrine and norepinephrine. Selye's General Adaptation Syndrome (GAS) describes our prolonged response to a chronic stressor across three stages. The GAS summarizes changes in the hypothalamic-pituitary-adrenal (HPA) axis, which releases the hormones CRH, ACTH, and cortisol, and explains how chronic stress can produce disease and death.
The Fight-or-Flight Response
Cannon (1932) described the fight-or-flight response, in which an individual confronts or flees a stressor. During an acute stress response, which corresponds to the end of Selye's alarm stage, we activate the sympathetic nervous system (SNS), increasing respiration, cardiac output, blood flow to skeletal muscles, and metabolism while decreasing digestion and the reproductive system activity. The SNS, in turn, activates the hard-wired sympathetic-adrenomedullary (SAM) pathway, resulting in the release of the hormones epinephrine and norepinephrine by the adrenal medulla (inner adrenal gland).Listen to a mini-lecture on the SAM Pathway © BioSource Software LLC. The acute stress response is illustrated © Designua/Shutterstock.com.
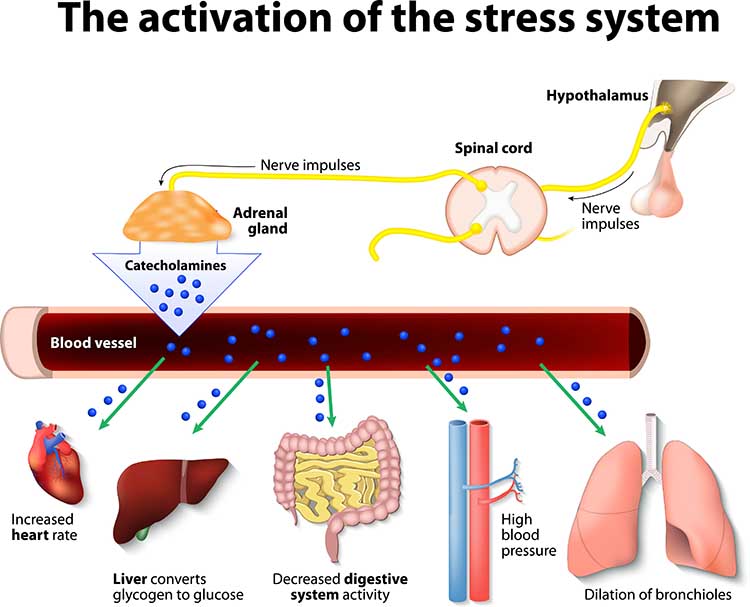
The adrenal medulla releases epinephrine and norepinephrine in a 4:1 ratio (Fox, 2019). The adrenal medulla is the inner region of the adrenal glands located at the top of each kidney. Graphic © Designua/Shutterstock.com.
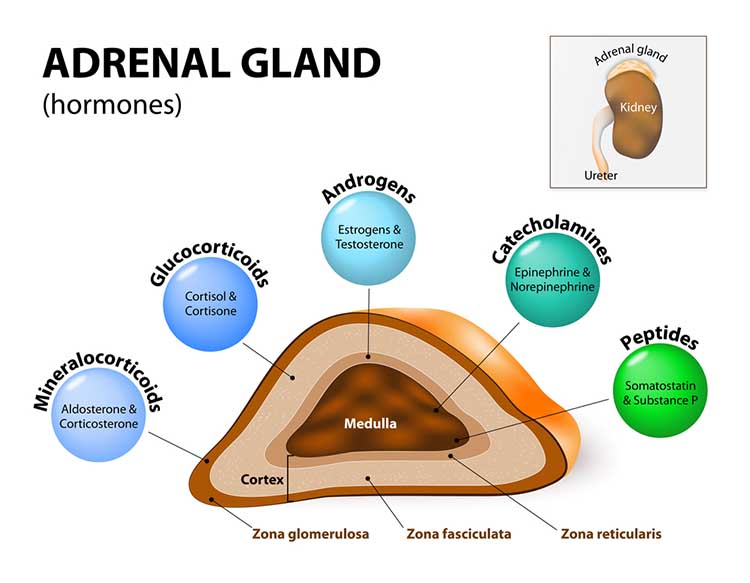
The catecholamines epinephrine and norepinephrine mobilize blood glucose and fatty acids to provide energy for skeletal muscle contraction. They increase blood flow to the muscles by increasing cardiac output and blood pressure. They dilate coronary blood vessels and the bronchioles of the lungs and increase respiratory rate. Increased delivery of oxygen to the brain heightens alertness. As part of fight or flight, they increase metabolic rate, activate fibrinogen to accelerate clotting, constrict skin blood vessels to reduce blood loss, and release endorphins to suppress pain (McEwen, 2002). Epinephrine levels are higher when we are fearful, and norepinephrine levels are higher when angry (Ward et al., 1983).
SAM activation is adaptive when its intensity and duration enable us to cope with an external threat. Low SAM activation facilitates athletic and cognitive performance, while intense SAM activation allows us to overcome physical threats. However, intense SAM activation is maladaptive in panic attacks or anticipatory anxiety, where there is neither an external threat nor active coping.
Intense SAM activation can threaten health and produce medical complaints.
Listen to a mini-lecture on the Effects of Intense SAM Activation © BioSource Software.
Anger can constrict coronary arteries and reduce cardiac output in cardiac patients (Committee on Health and Behavior, 2001) and are a risk factor for heart attacks and sudden cardiac death (Williams et al., 2000). Anxiety and acute grief, which can also produce intense SAM activation, are risk factors for sudden cardiac death (Engel, 1971; Kawachi et al., 1994). SAM activation also underlies common symptoms of chest pain, dizziness, and shortness of breath that can be confused with coronary insufficiency (Crider, 2004).
While Cannon emphasized sympathetic activation, stressors can also suppress parasympathetic activation and reduce HRV, consisting of changes in the time intervals between consecutive heartbeats (Task Force, 1996). Reduced parasympathetic tone can decrease restorative stage 3 sleep, contribute to illness, and increase mortality (Hall et al., 2004).
The Hypothalamic-Pituitary-Adrenal (HPA) Axis
The hypothalamic-pituitary-adrenal (HPA) axis is the second stage of the body's defense. The HPA axis is the foundation of allostasis and its failure, allostatic overload (McEwen, 2002). The HPA axis releases the hormones CRH, ACTH (corticotropin), and cortisol. This cascade starts with signals from the amygdala to the hypothalamus and ultimately targets the adrenal glands located at the top of each kidney.Listen to a mini-lecture on the HPA Axis © BioSource Software.
The adrenal cortex, which is the adrenal gland's outer region, produces the hormones aldosterone and cortisol. Cortisol is the most important glucocorticoid. Cortisol levels peak from 20-40 minutes following a stressor (Brannon et al., 2022). View the Blausen Adrenal Cortex Anatomy and Secretion of Cortisol animation.
This pathway is regulated by negative feedback as rising cortisol levels inhibit hormone secretion by the hypothalamus and anterior pituitary. Graphic © Designua/Shutterstock.com.
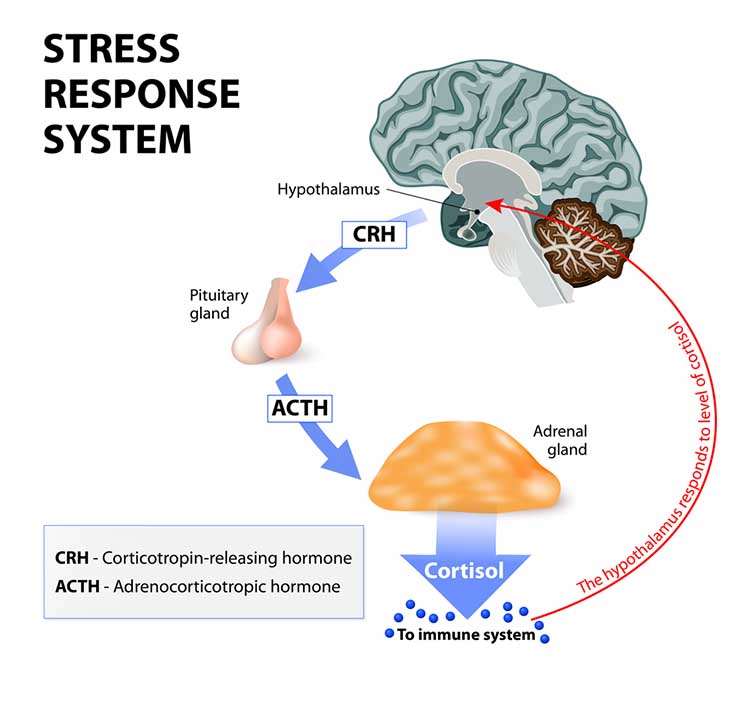
Sustained elevated cortisol levels can affect mood and produce system-wide damage. Graphic © medicalstocks/Shutterstock.com.
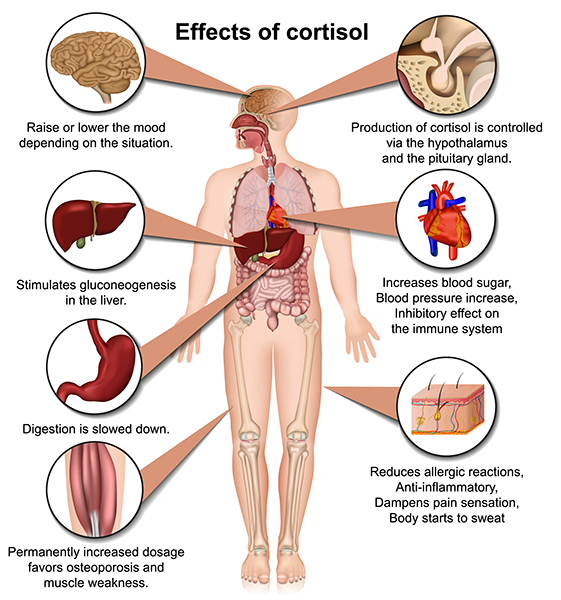
CRH
In response to stressful stimuli, the central nucleus of the amygdala activates the paraventricular nucleus (PVN) of the hypothalamus, resulting in increased CRH release to the pituitary gland.Chronic, elevated CRH levels in the bloodstream may enhance learning classically conditioned fear responses, heighten arousal and attention to increase readiness to respond to a stressor, intensify the startle response, and reduce appetite and body weight, sexual behavior, and growth.
ACTH
When CRH binds to the pituitary gland, it releases corticotropin (ACTH). ACTH triggers cortisol release by the adrenal cortex (outer part) and helps resist infection.Cortisol
Cortisol exerts widespread effects on critical body organs (Kemeny, 2003) and cortisol levels in the blood index stress, peaking 20 to 40 minutes following a stressor (Brannon et al., 2022).Listen to a mini-lecture on Cortisol © BioSource Software LLC.
Cortisol increases our activity and appetite. It helps convert fat and protein to glucose. Cortisol has short-term and long-term effects on immunity. At first, cortisol directs white blood cells to sites of infection or wounds, increases their stickiness and adherence to blood vessels and damaged tissue, and communicates when immune activity is sufficient. Cortisol's long-term effect, however, is impaired immune function (McEwen, 2002).
In healthy individuals, cortisol levels are highest in the early morning, when they help wake us up, and are lowest at night. In severely depressed individuals, the cortisol rhythm is suppressed, and its levels remain moderately high over 24 hours. Chronically elevated cortisol levels in the bloodstream adversely affect many organs, including the brain.
Allostatic load can result in hyperglycemia (elevated blood sugar), insulin insensitivity (prevents insulin from transporting glucose into skeletal muscles), increased gastric acid secretion, and ulcer. Muscle protein is converted to fat. Fat storage in the abdomen increases, which endangers health more than storage in the hips and thighs. Bone mass is reduced due to the loss of minerals (McEwen, 2002).
Cortisol release can affect gene transcription, thus producing long-term and immediate effects on the body and setting the stage for several physical and psychological disorders (panic, PTSD, and somatization).
While we've seen how allostatic load can result in chronically elevated HPA axis release of cortisol, the opposite pattern, underproduction of cortisol, also occurs. Cortisol suppresses the immune system, which reduces inflammation and swelling and moderates chronic pain. Low cortisol levels can result in allergies, asthma, autoimmune disorders like rheumatoid arthritis and multiple sclerosis, and chronic pain syndromes like fibromyalgia (McEwen, 2002).
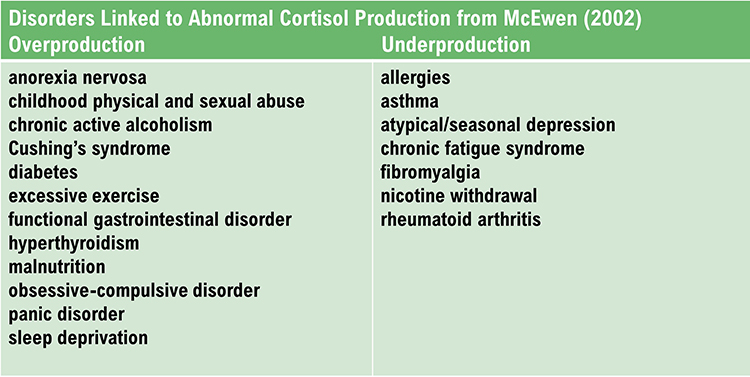
Cortisol binding to the amygdala increases CRH and ACTH. Cortisol release amplifies the fear response, increases our ability to store implicit memories about stressful stimuli, and increases the amygdala’s ability to escape the prefrontal cortex’s regulation of emotional behavior.
Cortisol binding to the hippocampal formation disrupts the medial temporal lobe memory system’s creation of explicit (conscious) memories. Cortisol interferes with hippocampal regulation of the PVN of the hypothalamus. Chronically elevated cortisol levels harm and kill hippocampal neurons. Cortisol suppresses neuronal repair by BDNF and interferes with creating new neurons. The elderly are more vulnerable to cortisol's harmful effects because they shut down their stress response more slowly. Their cortisol negative feedback loop functions less efficiently compared with younger individuals (McEwen, 2002).
Two pathways from the raphe system terminate in the hippocampus: an anxiogenic anxiety-producing pathway, and an anxiolytic, or anxiety-reducing pathway. Elevated cortisol levels suppress the anxiolytic pathway and facilitate the anxiogenic pathway. These changes heighten anxiety in a chronically stressed individual.
Cortisol binding to the dorsolateral and ventromedial prefrontal cortex injures and kills neurons as in the hippocampus. Cortisol disrupts executive functions like attention and decision-making, increasing anxiety and fear.
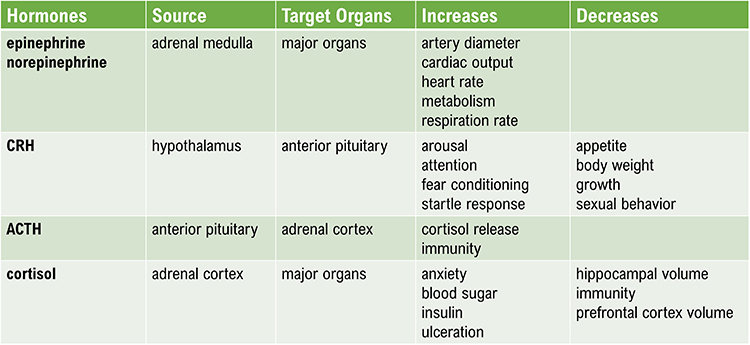
Men and Women Respond Differently to Stressors
Taylor and colleagues argue that men's and women's behavioral and neuroendocrine responses to stressors differ, largely because of oxytocin. The posterior pituitary releases oxytocin when we encounter stressors. Researchers have associated oxytocin, which is affected by estrogen, with social bonding.Although they share the same nervous system reactions to stressors, men tend to react with fight-or-flight while women respond with tend-and-befriend. Taylor and colleagues (2000) theorize that a tend-and-befriend response is an alternative reaction to stressors. They believe that tending, nurturing behavior, and befriending, seeking, and providing social support may better characterize women. The tend-and-befriend response may protect their safety and the lives of their offspring.
Their higher oxytocin levels cause women to seek and provide greater support when distressed than men (Bodenmann et al., 2015; Tamres et al., 2002; Taylor et al., 2000). Supporting this view, women reporting relationship stress have higher blood oxytocin levels (Taylor et al., 2006; Taylor, Saphire-Bernstein, & Seeman, 2010). An interaction may mediate this response between oxytocin and estrogen and endogenous opioids. Graphic © YAKOBCHUK VIACHESLAV/Shutterstock.com.

Chronic Stress
General Adaptation Syndrome (GAS)
The General Adaptation Syndrome (GAS) was Selye’s (1956) three-stage model of chronic autonomic and endocrine system responses to stressors.Listen to a mini-lecture on the General Adaptation Syndrome © BioSource Software LLC.
Selye argued that diverse stressors produce a three-stage response (alarm, resistance, and exhaustion) in all subjects. In this model, a cold stressor is interchangeable with a shock stressor because they produce the same autonomic and endocrine responses. Whereas Cannon showed that acute stress could change the functions of our internal organs, Selye mainly demonstrated using animal models that chronic stress can change their structure (Crider, 2004).
Alarm is the first stage of Selye’s GAS and consists of shock and countershock phases. The shock phase includes reduced body stress resistance and increased autonomic arousal and hormone release (ACTH, cortisol, epinephrine, and norepinephrine) that comprise the fight-or-flight response. In the countershock phase, resistance increases due to local defenses.
Resistance is the second stage of Selye’s General Adaptation Syndrome. Local defenses have made the generalized stress response unnecessary. Both cortisol output and stress symptoms, like adrenal gland enlargement, decline. While the person appears to be normal, adaptation to the stressor places mounting demands on the body, leading to diseases of adaptation like hypertension as adaptation energy is depleted. Local defenses will break down if stressors persist. McEwen calls these adjustments allostatic load.
Recovery or Exhaustion is the third stage of Selye’s General Adaptation Syndrome. We recover when a stressor has ended, and we can restore homeostasis. In exhaustion, increased endocrine activity depletes body resources and raises cortisol levels, resulting in suppressed immunity and stress syndrome symptoms. Selye believed that these changes could cripple immunity and cause bronchial asthma, cardiovascular disease, depression, hypertension, hyperthyroidism, peptic ulcer, ulcerative colitis, and possibly death (Brannon et al., 2022).
While Selye conceptualized stress as the outcome of the three-stage GAS, stress may occur at any time. Individuals may experience stress-related changes in anticipation of an event or after it has ended. Chronic resistance appears to produce more significant harm than exhaustion (Taylor, 2021).
Graphic adapted from Biostrap.
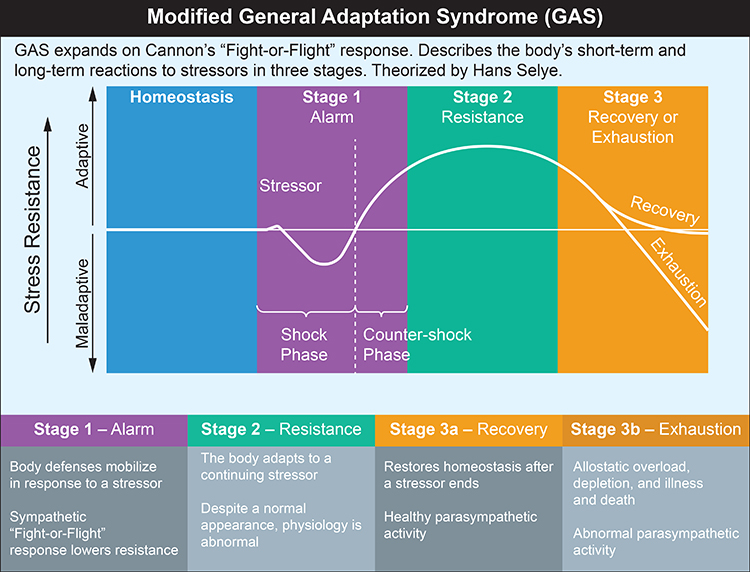
While Selye made a landmark contribution to our understanding of the role of chronic stress and glucocorticoid-mediated damage in disease, critics have challenged his characterization of the stress response as nonspecific and his conceptualization of stressors. Critics have questioned the GAS on four issues.
First, since most of Selye's research subjects were nonhuman animals, this may have caused him to essentially overlook the role of human emotion and cognitive appraisal in the chronic stress response.
Second, since Selye focused on stressors instead of human characteristics like biological predispositions and personality, he mistakenly assumed a uniform response to stressors. Stressors can produce different hormonal responses (Kemeny, 2003).
Third, while Selye emphasized the role of exhaustion in disease, there is more substantial evidence that chronic resistance may produce more significant harm (Taylor, 2012).
Fourth, while Selye conceptualized stress as the outcome of the GAS, both the anticipation of an event and coping with it during the resistance stage can disrupt performance and produce suffering (Taylor, 2012).
Brain Structures Involved in Stress
The amygdala, hypothalamus, hippocampus, and prefrontal cortex are the four brain structures most important to the stress response.The amygdala is part of the limbic system and participates in evaluating whether stimuli are threatening, establishing unconscious emotional memories, learning conditioned emotional responses, and producing anxiety and fear responses. The animation below is courtesy of Wikipedia.
The hypothalamus lies beneath the thalamus in the forebrain. It helps the body maintain a dynamic homeostatic balance by controlling the autonomic nervous system, endocrine system, survival behaviors (four F’s), and interconnections with the immune system. The animation below is courtesy of Wikipedia.
The Hypothalamus Receives Information About Stressors
Much of the information about stressors is relayed to the PVN. This hypothalamic nucleus organizes behavior to respond to changes in internal body states. The PVN receives input from the limbic system and cerebral cortex, other parts of the hypothalamus, and brainstem structures (nucleus of the solitary tract, tegmentum and reticular formation, periaqueductal gray, locus coeruleus, and raphe system). Graphic © Alila Medical Media/Shutterstock.com.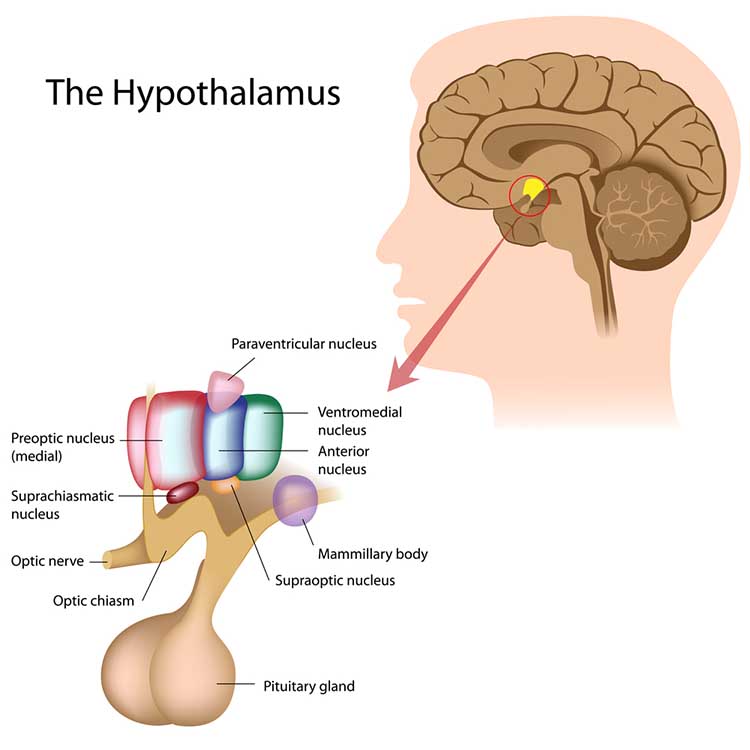
When the PVN is excited, it releases several chemical substances, including CRH, oxytocin, arginine-vasopressin, thyrotropin-releasing hormone, growth hormone-releasing hormone, somatostatin, dopamine, enkephalin, cholecystokinin, and angiotensin.
This large variety of hormones enables the individual to respond to a wide range of stressors. Since stressful events may simultaneously present many stressors, these chemical substances allow the individual to respond completely and appropriately.
The hippocampus is part of the medial temporal lobe memory system and helps form declarative memories, allows us to navigate our environment, and prevents excessive hypothalamic CRH release. Graphic © decade3d - anatomy online/Shutterstock.com.
The prefrontal cortex (PFC) is the most anterior region of the frontal lobes. The PFC contains the orbitofrontal and ventromedial, dorsolateral prefrontal cortex, and anterior and ventral cingulate cortex. The PFC is responsible for the brain’s executive functions, including planning, guiding decisions using emotional intelligence, working memory, allocation of attention, and emotional experience. The PFC inhibits emotional behavior triggered by the amygdala. Graphic © 2003 by Josephine F. Wilson.
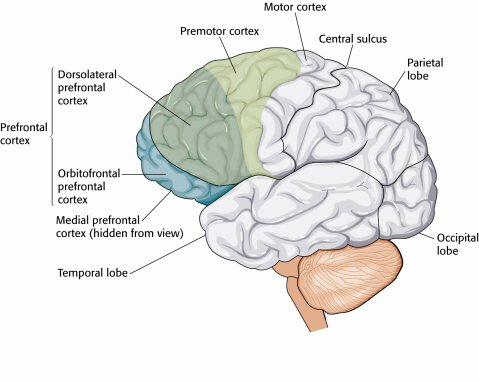
Psychoneuroimmunology (PNI)
Nonspecific and Specific Immune Mechanisms
The human body utilizes nonspecific and specific immune mechanisms to protect itself against invading organisms, damaged cells, and cancer.The main nonspecific, or innate, mechanisms are relatively rapid in response and include anatomical barriers (skin and mucous membranes) and phagocytosis (ingestion of microorganisms) by macrophages and neutrophils. Natural killer cells and neutrophils destroy infectious agents. Nonspecific mechanisms release antimicrobial agents (hydrochloric acid, interferons, and lysozymes) and signal to other immune responders. Local inflammatory responses confine microbes, allowing white blood cells and other immune cells to attack them.
In contrast, specific or adaptive immune mechanisms are slower and aim to target invaders and diseased cells selectively. The specific immune response involves the production and proliferation of antibodies by B cells, targeted destruction of foreign material by T cells, and preparation for future infiltrations of the same antigen (Shaffer & Mannion, 2016). In the illustration below, macrophages arrive to protect endangered cells. Graphic © UGREEN 3S/Shutterstock.com.
We develop specific immunity after birth through exposure to microorganisms and vaccinations, and it employs an antigen-antibody reaction to protect us against specific microorganisms and their toxins. Antigens are foreign molecules (proteins or polysaccharides) that stimulate antibody production. Antibodies are cellular proteins that combine with antigens to neutralize them.
Humoral and cell-mediated immunity are two types of specific immune responses. In humoral immunity, B lymphocytes rapidly produce antibodies that counter bacteria into the blood, neutralize toxins, and prevent reinfection by viruses. The illustration below shows lymphocytes (white) attacking bacteria. Graphic © dreamerb/Shutterstock.com.

Activated B cells differentiate into plasma cells, which secrete antibodies (immunoglobulins), and memory B cells, which are transformed into antigen-specific plasma cells when they reencounter the original antigen. Humoral immunity is most effective in countering bacterial infections and preventing new viral infections. The illustration below shows lymphocytes (white) attacking bacteria. Graphic © Designua/Shutterstock.com.
Cell-mediated immunity provides a slower cellular response that utilizes cytotoxic and helper T cells from T lymphocytes provided by the thymus gland. Cytotoxic T (TC) cells release toxins to destroy specific virally infected cells. Helper T (TH) cells release cytokines like interleukin-2 to aid TC and B cells' action and macrophages. TH cell cytokines can also suppress immune responses. Cell-mediated immunity is most effective in controlling cancer, foreign tissue, fungal and viral infections, and parasites.
Two-Way Brain-Immune System Communication
Nervous and immune system communication is bidirectional. From the nervous system side, adrenal cortical release of glucocorticoids suppresses immunity, including cell-mediated mechanisms like phagocytosis. At the start of the COVID-19 pandemic, admitted patients with higher cortisol levels were more likely to die from this infection (Tan et al., 2020).From the immune system side, increased proinflammatory cytokine release can signal the nervous system, resulting in feelings of depression, fatigue, loss of energy, and reduced pleasure (Anisman et al., 2005; Brannon et al., 2022; Dantzer et al., 2008). Acute and prolonged brain fog due to COVID-19 has been attributed to elevated cytokine levels (Theoharides et al., 2021). Graphic © Designua/Shutterstock.com.
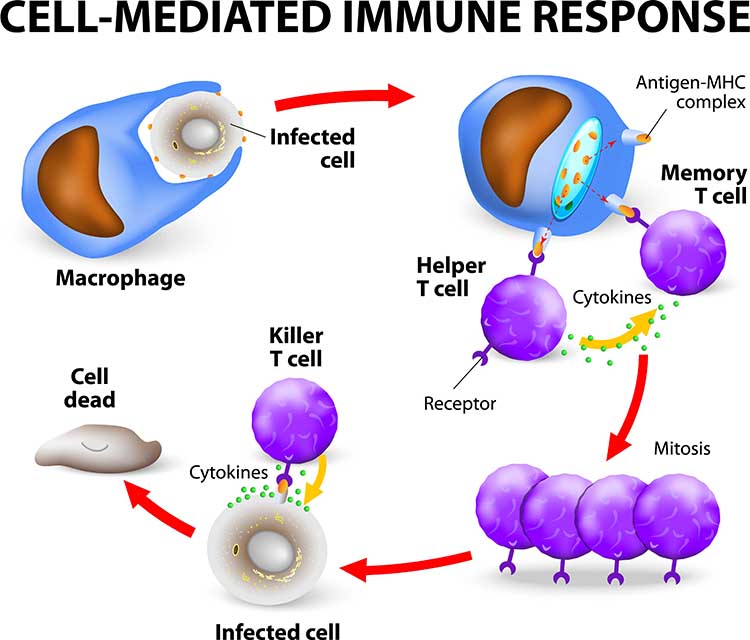
Check out Professor Gillian Griffiths' video Killer T Cell: The Cancer Assassin.
The Immune System Is Interconnected with the Nervous System
The classical model of the immune system is that it operates independently of the nervous system and psychological processes. However, researchers have demonstrated complex interactions among the nervous, endocrine, and immune systems, consistent with Green and Green's psychophysiological principle. Psychological processes like expectancies (placebo effect) and learning (classical conditioning) can affect all three systems, and the immune system can affect psychological functioning (drowsiness from a fever). Psychoneuroimmunology is a multidisciplinary field that studies the interactions between behavior and these three systems.After Solomon and Moos (1964) introduced the term psychoneuroimmunology in a journal article, Ader and Cohen's (1975) demonstration of classical conditioning in a rat's immune system helped establish this field's scientific legitimacy.
Ader and Cohen trained rats to associate a conditioned stimulus (a saccharine and water solution) with an unconditioned stimulus (the immunosuppressive drug cyclophosphamide). This resulted in a conditioned response (CR) of immune suppression, which resulted in rat fatalities. Following conditioning, rats who drank only sweetened water (CS) died due to conditioned immunosuppression. Successful replication of these findings helped overcome resistance to the controversial view that the nervous system and immune system can interact.
The mechanisms underlying these complex interactions include HPA axis hormones (ACTH, cortisol, CRH, epinephrine, and norepinephrine), immune cell chemical messengers called cytokines (interleukins), additional hormones (androgens, estrogens, progesterone, and growth hormone), and neuropeptides. Neuropeptides are chains of amino acids, like beta-endorphins, that neurons use for communication.
Stress and Immunity
There is persuasive evidence that stressful life events can reduce immunity and that behavioral interventions can enhance or maintain it. Bereavement can reduce lymphocyte (lymphatic white blood cell) proliferation (Schleifer et al., 1983). Academic exams, marital conflict, negative affect associated with stress, clinical and subclinical depression, and negative daily mood can suppress immunity (Herbert & Cohen, 1993; Kiecolt-Glaser et al., 2002; Stone et al., 1994).The stress of living near the Three Mile Island nuclear plant when it experienced a significant accident reduced residents' B cell, T cell, and natural killer cell counts compared with control subjects (McKinnon et al., 1989).
A study of Alzheimer's caregivers showed lowered immunity and longer wound healing times, and worse psychological and physical health than controls who were not caregivers (Kiecolt-Glaser, 1999). The Alzheimer's patients' deaths did not improve caregiver immunity or psychological functioning (Robinson-Whelen et al., 2001).
Finally, laboratory stressors produced more significant discomfort and immunosuppression in chronically-stressed young males than those not chronically stressed (Pike et al., 1994). Exposure to chronic stress may have intensified their subjects' response to acute laboratory stressors.
Behavioral Interventions Can Strengthen Immunity
Behavioral interventions can increase immunocompetence. Miller and Cohen's (2001) meta-analytical study of behavioral interventions showed modest increases in immunity. Hypnosis increased immune function more than relaxation and stress management.A stress management program that incorporated relaxation training reduced symptoms and increased salivary antibodies and psychological functioning in children diagnosed with frequent upper respiratory infections (Hewson-Bower & Drummond, 2001).
College students who wrote journal entries about highly stressful experiences increased lymphocyte proliferation and made fewer health center visits (Pennebaker et al., 1988). Smyth et al. (1999) asked asthma and rheumatoid arthritis patients to write journal entries about highly stressful experiences or planned daily activities. At a 4-month follow-up, 50% of the Pennebaker journal group who wrote about stressful experiences and 25% of the control group achieved clinically significant improvement in their immune-related disorders (Crider, 2004).
Dental and medical students who received hypnosis training maintained immune function while a control group showed declines in immunity (Kiecolt-Glaser et al., 2001). This finding suggests that behavioral interventions may be more effective in maintaining normal immunity than boosting immunity (Brannon et al., 2022).
Cognitive Appraisal of Stressors and Coping
Lazarus and Folkman's (1984) Transactional Model of Stress has more strongly influenced psychologists than Selye's General Adaptation Syndrome.
Caption: Richard Lazarus
Whereas Selye's stimulus model theorized that events determine stress, Lazarus' cognitive model proposed that stress is determined by our perception of the situation and emphasizes person-environment
fit (Taylor, 2012).
Coping is central to the Transactional Model of Stress. Lazarus and Folkman defined it as "constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person” (1984, p. 141). Coping is an effortful learned process whose goal is to manage a situation (Brannon et al., 2022).
![]()
Listen to a mini-lecture on the Transactional Model of Stress © BioSource Software LLC.
In primary appraisal, we categorize the consequences of events as positive, neutral, or negative and determine whether an event is relevant, negative, or potentially negative. We evaluate these events for their possible harm, threat, or
challenge.
Harm is damage that has
already occurred. For example, a person who experiences a heart attack
may perceive harm as damage to the heart muscle.
Threat means damage that could arise in the future. The
heart attack survivor may anticipate restricted physical activity and
reduced income. The perception of an event as a threat has physiological
consequences and can result in elevated blood pressure.
Challenge is the potential to cope
with the event and gain from this opportunity. The heart attack survivor
may reframe this health crisis as an opportunity to make a career
change. The perception of an event as a challenge can increase perceived
self-efficacy and positive emotion while lowering blood pressure (Maier et al.,
2003).
The Chinese pictogram wei ji,
representing danger and opportunity, illustrates the negative and
positive possibilities considered during primary appraisal.
During
secondary appraisal, we evaluate whether our coping abilities and resources can surmount an event's harm, threat, or challenge. Lazarus and
Folkman (1984) listed health and energy, positive belief,
problem-solving skills, social skills, social support, and material
resources as necessary coping resources. Again, perception of our coping
abilities and resources is more important than their actual existence.
The balance between primary and secondary appraisal determines how we
subjectively experience the event. We experience the most stress when
perceived harm or threat is high and perceived coping skills and
resources are low. Stress is reduced when we perceive that our coping
abilities and resources are high (Taylor, 2012).
Secondary appraisal can lead to our use of direct action, reappraisal,
and palliation.
Direct action can take different
forms depending on the nature of the threat. We may use aggression and escape behaviors from Cannon's fight-or-flight response for violent threats to our survival. We may use problem-solving for medical or psychological threats, define the problem, identify options, and test these options until we succeed. A cardiac patient may enroll
in a cardiac rehabilitation program to increase exercise tolerance and
reduce the risk of artery narrowing.
Reappraisal may reduce stress when
direct action is impractical or unsuccessful. Reappraisal modifies our
perception of a threat. When individuals are overwhelmed by traumatic
stress, they may initially use ineffective strategies like denial and
rationalization. As they cope with the crisis, they may progress with
more successful strategies like reframing
in which they place the stressful situation in perspective and focus on
available opportunities. For example, a cardiac patient may decide that his heart
attack allowed him to spend more time with his
grandchildren.
Palliation consists of efforts to
reduce our stress response rather than attack the stressor. Trainers
may use biofeedback and adjunctive techniques like effortless breathing
to teach cardiac patients to control their anxiety. While this does not
correct the cause of the stress response, it is often superior to
medications like anxiolytics that risk side effects, tolerance, physical
dependence, and withdrawal effects. Successful clinical interventions
for chronic problems like anxiety, depression, and pain incorporate
effective palliation since complete remission may be unlikely. The diagram below was adapted from Crider
(2004).
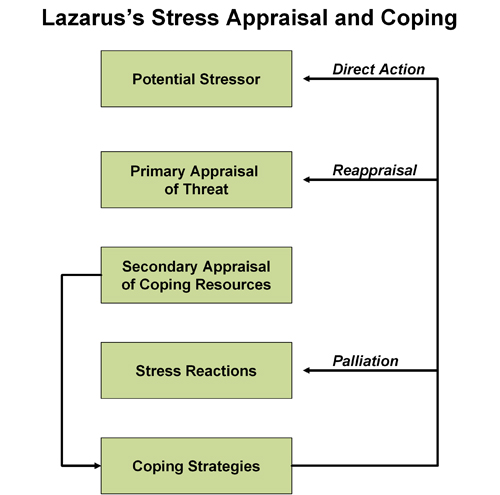
Evaluation
The Transactional Model of Stress encompasses cognitive appraisal, missing from the General Adaptation Syndrome. Research supports this model. For example, performance is better when we perceive an event as challenging instead of threatening (Moore et al., 2012).Lazarus and Folkman's model recognizes that we constantly change as we cope with stressors and that our coping successes and failures influence our appraisals of future events (Brannon et al., 2022).
The Effect of the Perception that Stress Impacts Health
Cannon (1942) studied voodoo deaths in shamanistic cultures and published speculation about how beliefs can produce lethal cascades of system failure in the American Anthropologist. Graphic © Fer Gregory/Shutterstock.com.
Keller et al. (2012) conducted a regression analysis of the 1998 National Health Interview Survey and prospective National Death Index data from 28,753 adults. Both elevated levels of reported stress and the perception that stress negatively impacted health independently and jointly predicted poor physical and psychological health outcomes. While neither variable independently predicted premature death, subjects who reported high levels of stress and the perception that stress impacts health experienced a 43% greater risk of early death.
Listen to a mini-lecture on the Effect of the Perception That Stress Harms Health © BioSource Software LLC.
Check out Kelly McGonigal's TED Talk How to Make Stress Your Friend. McGonigal proposes that we train clients to reframe sympathetic activation as evidence of our courage to rise to a challenge instead of the body injuring itself.

Personality Dimensions
Mastery
Mastery overlaps with the concepts of locus of control, perceived control, and self-efficacy. Mastery is the relatively stable expectancy that we can control personal outcomes. Graphic © pamspix/iStockphoto.com.
Mastery affects our appraisal and coping with stressors. Individuals with high levels of mastery expect to succeed when challenged by stressors, cope more effectively, and report lower levels of depression and stress than people with low levels of mastery (Gurung, 2019).
In Weiss’ (1977) replication of the Brady “executive monkey” study, the "executive” rat could switch off the tail shock by turning the wheel. Because it had control over the shock, it was no more likely to develop ulcers than an unshocked control rat. The "subordinate" rat received the same shocks as the "executive" rat. Because the "subordinate" rat had no control over the shocks, it was more likely to develop ulcers than the "executive" rat.
Impulsiveness
Distress can increase impulsive behavior that produces immediate relief or pleasure, sometimes at the cost of personal health (Tice et al., 2001). Graphic © YouraPechkin/iStockphoto.com.
Examples include binge drinking, suspending medication and physical exercise, consuming unhealthy meals, and defaulting on responsibilities like attending class or work. Substance abuse may reduce an individuals' motivation and capacity to meet their commitments.
Hopelessness
Hopelessness is a depressive symptom that might be an independent heart attack risk factor. Compared with middle-aged Finnish men scoring low in hopelessness, those scoring high were two to three times more vulnerable to a heart attack over the ensuing 6 years and three to four times more likely to die (Everson et al., 1996). Graphic © microcosmos/Shutterstock.
Optimism
Optimism is a generalized expectancy of positive future outcomes. Optimists focus on a situation's positive dimensions, minimizing daily hassles (Nelson et al., 1995). Graphic © hidesy/iStockphoto.com.
Optimism aids health by encouraging more effective problem-focused coping strategies instead of avoidant coping strategies. These strategies result in better stress management and practice of health-promoting behaviors like barrier protection during sex. Optimists show good psychological health, effective natural killer (NK) cell response during stress, and slower AIDS progression. In the context of the Transactional Model of Stress, optimists diverge from pessimists in secondary appraisal, actions, and personal adjustment (Gurung, 2019).
A prospective study showed that the 25 percent most optimistic women had about a 30 percent lower mortality risk than the 25 percent least optimistic women. Dispositional optimism was associated with reduced mortality due to cancer, heart disease, infection, respiratory disease, and stroke. While attenuated, these results held up after controlling socioeconomic status, depression, health conditions, and health-related behaviors (Kim et al., 2016).
Pessimism
Pessimism, a generalized expectancy of future adverse outcomes, is also a heart attack risk factor. A Harvard School of Public Health team found pessimistic adult men had a doubled risk of developing heart disease over 10 years (Kubzansky et al., 2001).
Alexithymia
Wickramasekera (1988) described alexithymics as low in hypnotic ability and awareness of internal cues and feelings associated with illness. Alexithymia is prevalent in patients with multiple psychosomatic complaints and may delay seeking and receiving medical attention.Reactivity
Eliot's (1992) hot reactors cannot be identified by their overt behavior but risk sudden death due to pathological acute and chronic responses to stressors. Hot reactors show an acute increase in catecholamine secretion, which increases the risk of cardiac arrhythmia due to excessive myocardial fiber contraction and clot formation. When they are challenged by long-term stressors and experience fear, uncertainty, and loss of control, they also show a chronic increase in glucocorticoid secretion, which raises total cholesterol while lowering protective HDL-C.African Americans start to show greater reactivity than their European American counterparts by childhood (Murphy et al., 1995), perhaps due to stressors associated with their ethnicity. This difference may help explain their higher prevalence of cardiovascular disease.
Everson et al. (2001) discovered that the risk of stroke was more significant for men with higher systolic blood pressure reactivity.
Resources to Buffer Stress
Social Support
Social support consists of received support (support provided) and perceived support (expected support) from individuals and organizations. Both forms of social support include informational, material, and psychological assistance from others. The value of each kind of social support depends on an individual's specific needs. Graphic © Yuri/iStockphoto.com.
Social networks and social contacts both concern the number and kinds of interpersonal relationships. A social network is a social structure consisting of nodes (individuals or organizations) tied together. Social contacts are the nodes (individuals or organizations) comprising a person’s social network.
Patients with a high level of social support participate in an extensive social network consisting of numerous social contacts. Those with low social support have a limited social network with few social connections.
High levels of social support are associated with better health, faster recuperation, less psychological distress, lower depression risk, and lower mortality than low levels of social support (Gurung, 2019). Graphic © Ljupco Smokovski/Shutterstock.com.

The Alameda County Study (Berkman & Syme, 1979) documented a relationship between social contacts and longevity. Adults with the fewest social connections had 2-4 times the risk of death than those with the most social contacts. Gender and age moderated the effect of social connection. Males' highest relative risk of death (3.2) was from age 50-59, whereas women's highest relative risk (4.6) was from age 30-49 (Brannon et al., 2022).
Listen to a mini-lecture on the importance of social contact © BioSource Software LLC. Graphic © Ljupco Smokovski/Shutterstock.com.

Hawkley and colleagues (2006) reported that loneliness is an independent risk factor for hypertension comparable to obesity and a sedentary lifestyle. They studied 229 participants aged 50 to 68 years and measured their perceived degree of loneliness, as well as previously established cardiovascular and psychosocial risk factors. Even after statistically controlling for other negative emotional states (e.g., depression, hostility, or stress), lonely older participants had systolic blood pressures up to 30 mmHg higher than their non-lonely counterparts. They discovered that loneliness and stress raised blood pressure via different mechanisms and produced an additive effect. Furthermore, the impact of loneliness on blood pressure increased with age.
Prosocial Behavior
A prospective study of 846 adults by Poulin et al. (2013) showed that providing tangible assistance to friends or family members in the previous year buffered the effects of stress on mortality over 5 years. In contrast, stress predicted mortality for participants who did not help others.Follow-up data from the longitudinal National Survey of Midlife Development in the U.S. (MIDUS II) of 1054 middle-aged adults found that women who perceived that they supported others in positive social relationships had lower IL-6 levels, a marker for inflammation (Jiang et al., 2021). Elevated IL-6 levels are linked to an increased risk for serious diseases.
Listen to a mini-lecture on the importance of prosocial behavior © BioSource Software LLC.
Graphic © Monkey Business img/Shutterstock.com.

Aerobic Exercise
A sedentary lifestyle marked by prolonged sitting and TV-viewing time was linked to chronic health conditions and all-cause mortality in a meta-analysis of data from over 1 million middle-aged men and women. Individuals who engaged in moderate-intensity exercise 60-75 minutes per day eliminated the increased risk of death due to sitting but only attenuated the risk associated with TV-viewing time (Ekelund et al., 2016). Graphic © racornShutterstock.com.
Mildly depressed college women who participated in an aerobic exercise program showed markedly reduced depression compared with those who did relaxation exercises or received no treatment (McCann & Holmes, 1984). Graphic © Maksim Toome/Shutterstock.com.

A study that compared exercise with drug treatment or a combination of exercise and drug treatment found that exercise improved mood and the other two conditions. When treatment was discontinued, participants who continued to exercise were less likely to relapse than those who had received drug treatment (Babyak et al., 2000).
The positive impact of exercise on mood may be mediated by reduced cardiovascular reactivity (Perkins et al., 1986), and increased involvement (Estabrooks & Carron, 1999), self-efficacy (McAuley et al., 2003), and self-esteem (Sonstroem, 1997).

Religious and Spiritual Activity
In a national health survey financed by the U.S. Centers for Disease Control and Prevention, religiously active people had longer life expectancies (Hummer et al., 1999). McCullough and colleagues (2000) performed a meta-analysis that assigned greater weights to studies that controlled confounding variables like age, gender, health, and social support. They found that religious involvement was linked to a slightly lower mortality rate and that this was not due to social support. Graphic © LincolnRogers/ iStockphoto.com.
BASIC PHYSIOLOGY OF ATTENTION
Brain Organization and Dynamics
The brain is organized into interactive functional distributed networks with spatial, temporal, and content-based relationships.
These networks interact through feedback loops and transiently organized aggregates of neurons, all mediated by rhythmic, oscillatory electrical discharges that ultimately produce the EEG.
This process is further controlled/informed by selective attention to specific categories of interest.
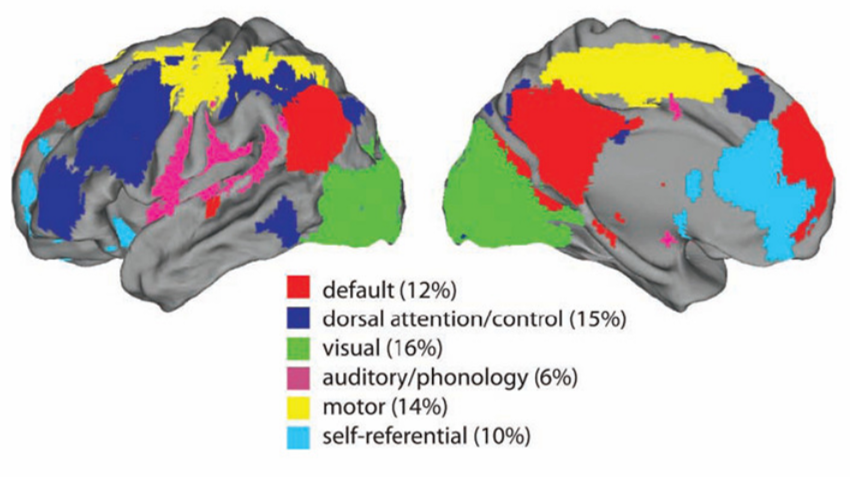
Each type of local cognitive, sensory processing, or emotional network produces oscillatory activity and contains internal stabilizing characteristics. These local networks exist within a global dynamic network
system that links and provides an interactive capacity to the smaller networks, also operating within an oscillatory framework.
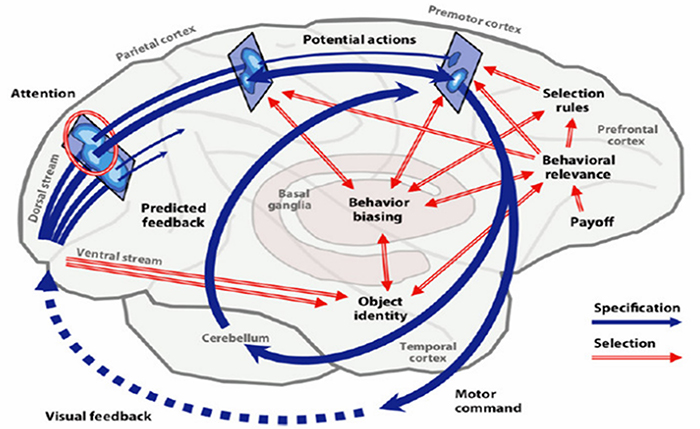
The central nervous system processes incoming content. Separate regions process specialized content (e.g., auditory, kinesthetic, tactile, visual). Content is shared, integrated, compared to previous content, and analyzed. Decisions are made regarding memory and responses. All of this central nervous system activity occurs within interacting networks linked by electrical/chemical signals. Electrical discharges from network activity are recorded from the scalp surface as the EEG.
Network Overview
The networks most relevant to attention include the executive, affective, motor, oculomotor, and social circuits.
Executive Network
The dorsolateral prefrontal cortex plays a critical role in executive functions, which Kropotov (2009) described as "the coordination and control of motor and cognitive actions to attain specific goals." Executive functions include allocation of attention, cognitive inhibition, behavioral inhibition, working memory, and cognitive flexibility. The executive network focuses and maintains continuous attention. The diagrams below were adapted from Alexander et al. (1986) and Thompson and Thompson (2016).
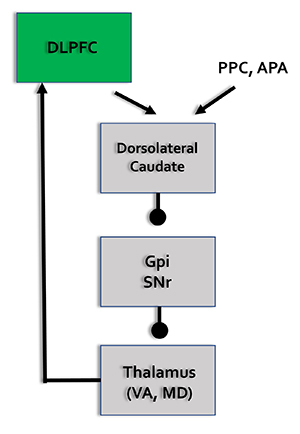
DLPC = dorsolateral prefrontal cortex, PPC = posterior parietal cortex, APA = arcuate premotor area, GPi = globus pallidus internal segment, SNr = substantia nigra, pars reticulata, VA = ventral anterior nucleus of the thalamus, MD = medial dorsal nucleus of the thalamus.
Affective Network
The pre- and subgenual areas of the anterior cingulate cortex (ACC) participate in affective circuits triggered when we make mistakes. The dorsal rostral cingulate zone monitors cognitive activity to predict when errors are likely, and greater executive control may be needed (Thompson & Thompson, 2016).
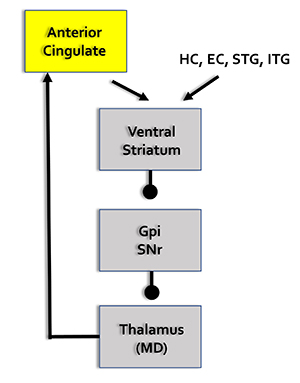
HC = hippocampal cortex, EC = entorhinal cortex, STG = superior temporal gyrus, ITG = inferior temporal gyrus, posterior parietal cortex, GPi = globus pallidus internal segment, SNr = substantia nigra, pars reticulata, MD = medial dorsal nucleus of the thalamus.
Motor Network
The supplementary motor area (SMA), in concert with the premotor cortex, primary motor cortex, sensorimotor cortex, and cerebellum, plans, initiates, and inhibits voluntary movements and muscle contractions (Breedlove & Watson, 2020; Thompson & Thompson, 2016).
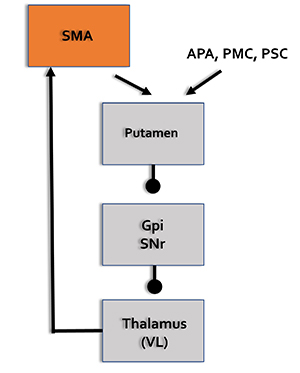
SMA = supplementary motor area, APA = arcuate premotor area, PMC = primary motor cortex, PSC = primary somatosensory cortex, GPi = globus pallidus internal segment, SNr = substantia nigra, pars reticulata, VL = ventral lateral nucleus of the thalamus.
Oculomotor Network
The frontal eye field (FEF), in concert with the dorsolateral prefrontal cortex, posterior parietal cortex, basal ganglia, and thalamus, programs and initiates voluntary eye movements, inhibits eye movements toward distracting stimuli, and allows us to return our focus to locations we've experienced in the past (Thompson & Thompson, 2016).
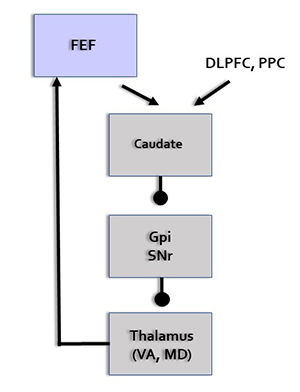
FEF = frontal eye field, DLPFC = dorsolateral prefrontal cortex, PPC = posterior parietal cortex, GPi = globus pallidus internal segment, SNr = substantia nigra, pars reticulata, VA = ventral anterior nucleus of the thalamus, MD = medial dorsal nucleus of the thalamus.
Social Network
The orbitofrontal cortex (OFC), along with the basal ganglia and thalamus, orchestrates the highest level of emotional processing in the nervous system. The social network is responsible for socially responsible behavior, empathy, behavioral inhibition, emotional regulation, and sound judgment (Thompson & Thompson, 2016).
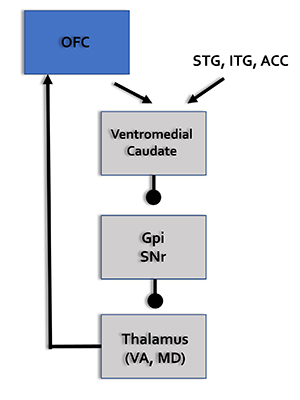
OFC = orbitofrontal cortex, STG = superior temporal gyrus, ITG = inferior temporal gyrus, ACC = anterior cingulate cortex, GPi = globus pallidus internal segment, SNr = substantia nigra, pars reticulata, VA = ventral anterior nucleus of the thalamus, MD = medial dorsal nucleus of the thalamus.
Attentional Processes
Attention is the selection of sensory information or cognition for enhanced processing. We can overtly or covertly attend to stimuli. In overt attention, our attentional focus and sensory orientation coincide. For example, you parse this sentence as you focus your gaze on it. In covert attention, we shift our attentional focus from our sensory orientation. For example, you attend to a reminder on the corner of your screen while you gaze at this sentence. While the midbrain superior colliculus is mainly implicated in overt attention, it may also regulate covert attention (Breedlove & Watson, 2020).
Attention is more selective than arousal, which is our overall level of alertness (Breedlove & Watson, 2020).
Research using divided attention tasks, where subjects simultaneously process multiple stimuli, shows that attentional resources are finite. The challenge of attending to more than one target at a time increases when they occupy different spatial locations. When we attend to a stimulus, we shift our attentional spotlight (focus) to select a stimulus for enhanced analysis (Bee & Micheyl, 2008).
Perceptual load (stimulus processing demands) determines the level at which an attentional bottleneck (stimulus selection) occurs. Complex stimuli, which involve a high perceptual load and monopolize processing resources, result in early selection where we filter out lower priority competing stimuli before preliminary perceptual and semantic analysis. Conversely, simple stimuli, which involve a low perceptual load and leave free processing resources, result in late selection where we filter out competing stimuli after performing extensive analysis (Lavie et al., 2004).
The Pulvinar Mediates Attentional Shifts
The pulvinar nucleus, which comprises the posterior quarter of the human thalamus, processes visual information and directs attention. The pulvinar plays a pivotal role in processing visual information and shares widespread connections with the cingulate, parietal cortex, and superior colliculus. The pulvinar is crucial for orienting, shifting attention, and filtering out irrelevant stimuli. Tasks that present subjects with more distracting stimuli increase pulvinar activation, as shown by functional MRI (fMRI) (Buchsbaum et al., 2006).
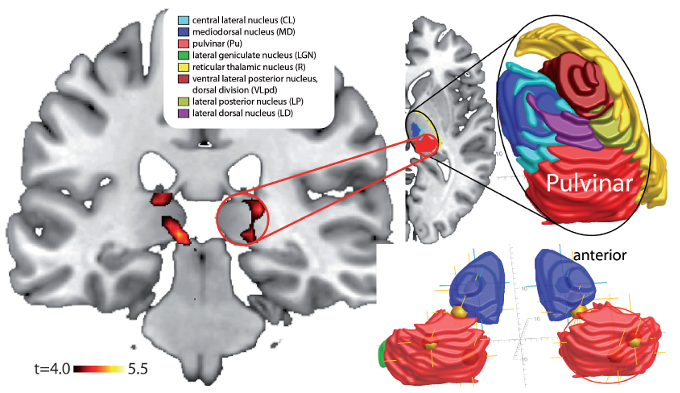
Overall, the pulvinar guides the processing of relevant information in wide-ranging cortical networks based on dynamically changing attentional priorities (Breedlove & Watson, 2020; Saalmann et al., 2012).
Cortical Regions That Guide Attention
The dorsal frontoparietal system, which is comprised of the intraparietal sulcus and frontal eye field, is responsible for top-down direction of attention (Breedlove & Watson, 2020). The intraparietal sulcus (IPS), located in the parietal lobe, provides voluntary top-down steering of attention (Corbetta & Shulman, 1998).
The frontal eye field (FEF), found in the premotor region of the frontal lobes, directs gaze towards targets selected by the IPS (Paus et al., 1991). Target selection is guided by cognitive goals (top-down processing) rather than stimulus characteristics (bottom-up processing). The dorsal frontoparietal system is shown below in gold.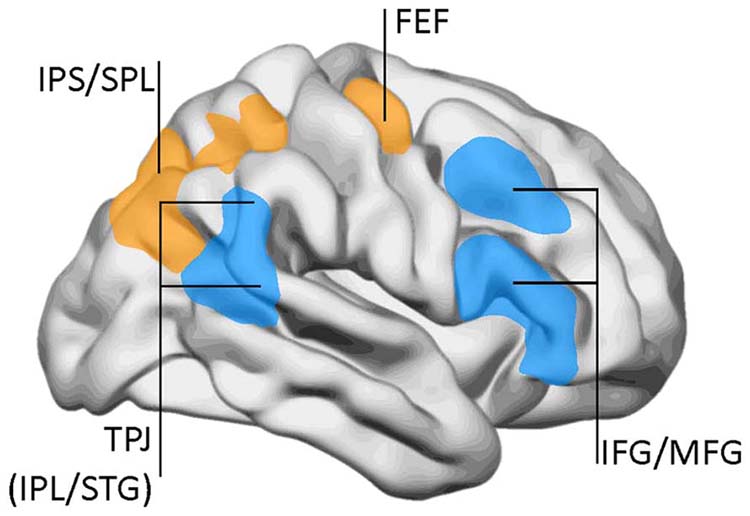
In contrast, the temporoparietal junction (TPJ), where the superior temporal gyrus and inferior parietal lobe intersect, mediates bottom-up shifts in attention in response to stimulus attributes (Corbetta & Shulman, 2002). The TPJ functions like a circuit breaker by overruling immediate attentional priorities and reallocating attentional resources to a new target (Breedlove & Watson, 2020). The bottom-up system is shown above in blue. IPL stands for inferior parietal lobe, STG for superior temporal gyrus, IFG for inferior frontal gyrus, and MFG for middle frontal gyrus.
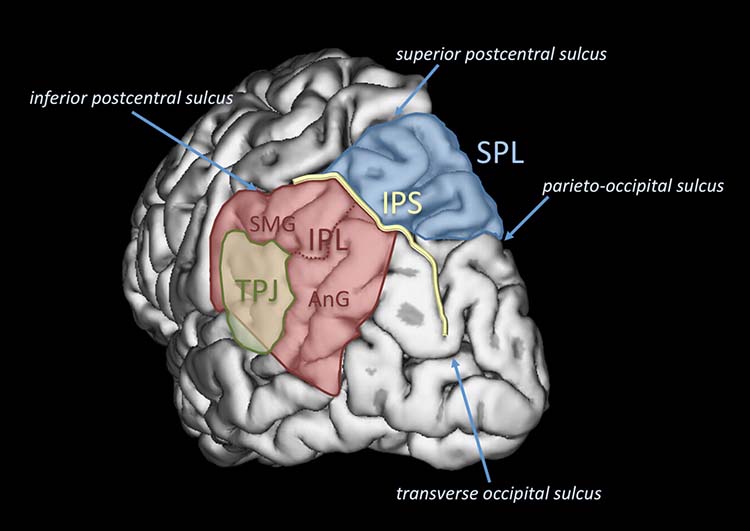
Two Cortical Networks Regulate Attention
Two cortical networks cooperatively regulate subcortical and cortical systems to produce a coherent perceptual experience (Breedlove & Watson, 2020). A dorsal frontoparietal system provides top-down control of endogenous attention (voluntary attention), directing the attentional spotlight to support cognitive system priorities. A right temporoparietal system provides bottom-up control of exogenous attention (involuntary reflexive attention), which redirects attention based on the novelty or importance of incoming stimuli.
Extensive interconnections between the two networks allow us to fluidly redirect attention from stimuli that are forebrain priorities (IPS) to those that are unexpected.
Salience Network
The salience network comprises structures that seek to monitor our external and internal environments to determine which of these inputs are essential and require further processing and attention. The insula, primarily the anterior insula, is a crucial component of this network because it facilitates bottom-up access to the brain’s attentional and working memory resources (Menon & Uddin, 2010). The cingulate gyrus, particularly the right dorsal anterior cingulate cortex, is another crucial component (Thompson & Thompson, 2016). Graphic © 2012 JAMA Psychiatry.
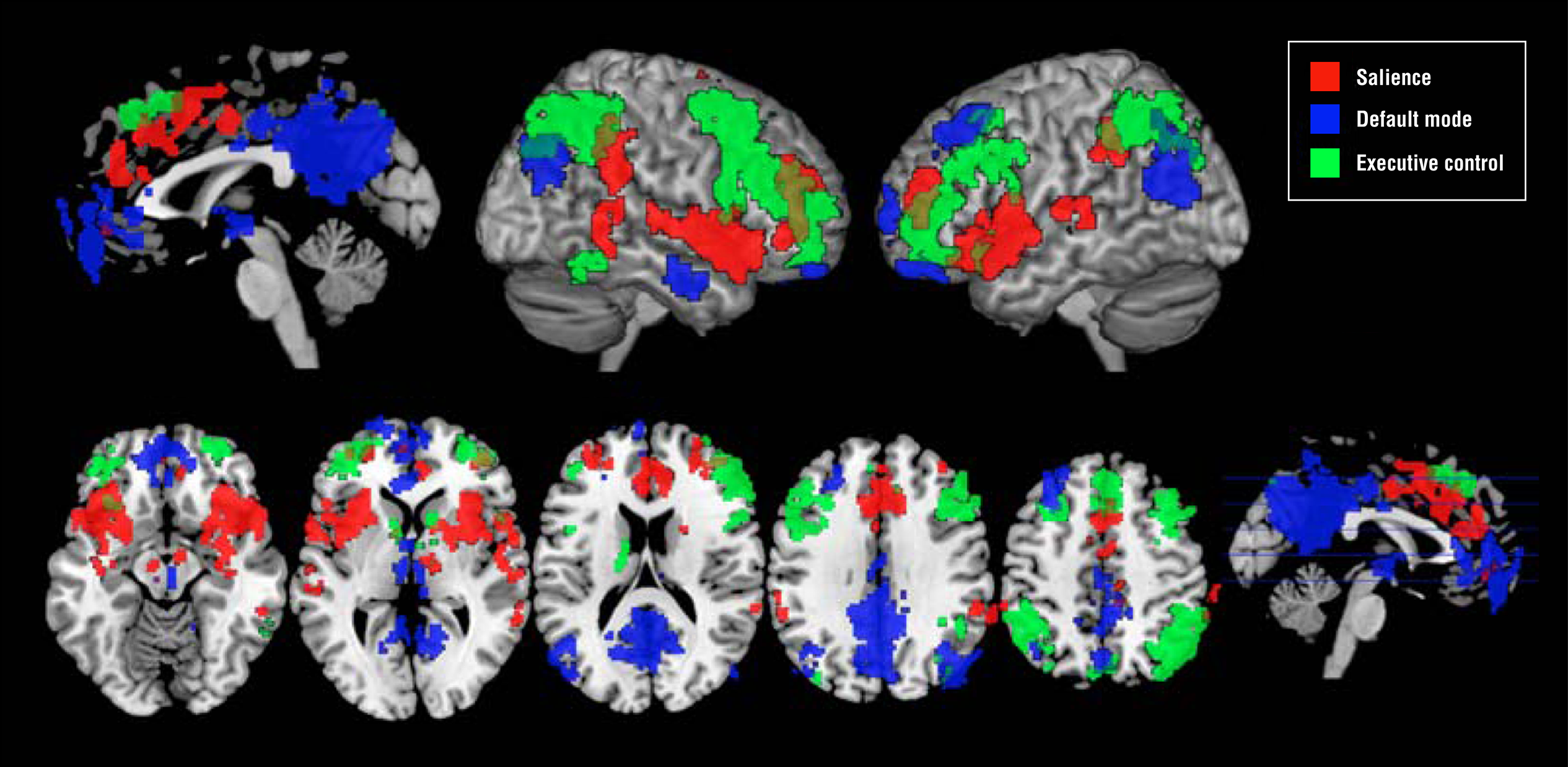
The insula, which is a cortical region located within the lateral sulcus, functions as an integrative and organization hub for the salience network. The insula integrates interoceptive awareness, emotional experience, and external perception to facilitate an individual's global perception of the world and its relationship. The insula directs specific networks in processing salient stimuli and the generation of appropriate responses to stimuli (Wiebking & Northoff, 2014).
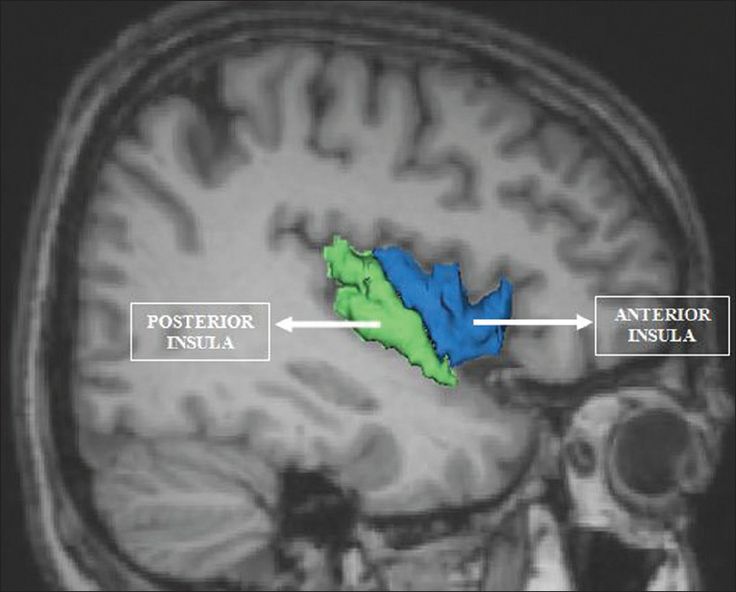
The insula appears to provide an interface between the human brain's cognitive, homeostatic, and affective systems. It, therefore, provides a link between the areas of the brain involved in monitoring internal signals and those engaged in watching incoming external sensory streams. The insula detects salient events via afferent pathways and switches between other large-scale networks when these events are recognized to guide attention and working memory.
The anterior and posterior insula interact to regulate autonomic responses to salient stimuli. Interactive communication between the insula and anterior cingulate cortex facilitates access to the motor system (Menon & Uddin, 2010).
This network appears to help us switch between task-oriented (executive) and default mode (attention) networks (Seeley et al., 2007; Shirer et al., 2012).
The graphic below from Menon and Uddin (2010) shows the salience network (right anterior insula and anterior cingulate cortex), central executive network (right dorsolateral prefrontal cortex and right posterior parietal cortex), and default mode network (ventromedial prefrontal cortex and posterior cingulate cortex).
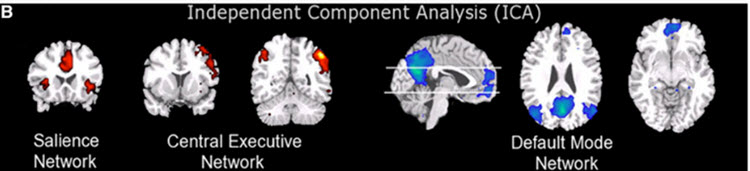
Default Mode Network (DMN)
Brain regions are selectively active when we are conscious (Breedlove & Watson, 2020). The default mode network (DMN) consists of frontal, temporal, and parietal lobe circuits active during spontaneous cognition like introspection, daydreaming, and streams of consciousness. The DMN appears to contribute flexible memory retrieval and idea generation, which are critical elements of creativity. The DMN is relatively inactive when pursuing external goals (Andrews-Hanna et al., 2010).
The DMN may contribute to creative fluency, generating innovative ideas like alternative uses for everyday objects. A study of neurosurgical patients showed that left DMN stimulation reduced the number of uses but not their originality (Shofty et al., 2022).
Understanding Ourselves
The posterior cingulate cortex (PCC) and precuneus combine bottom-up attention with information from memory and perception. The ventral (lower) part of the PCC activates in all tasks which involve the DMN, including those related to the self or others, remembering the past, thinking about the future, processing concepts, and spatial navigation. The dorsal (upper) part of PCC mediates involuntary awareness and arousal. The precuneus is concerned with visual, sensorimotor, and attentional information.The medial prefrontal cortex (mPFC) participates in decisions about the self, such as personal information, autobiographical memories, future goals and events, and decision-making regarding those close to us like family members. The ventral (lower) part is involved in positive emotional information and reward.
The angular gyrus connects perception, attention, spatial cognition, and action and helps us recall episodic memories.
Understanding Others
The major functional hubs include the PCC, mPFC, and angular gyrus. The dorsal medial prefrontal cortex (dmPFC) analyzes others' objectives. The temporoparietal junction (TPJ) constructs theories of mind, which are models of others' cognitive processes, emotions, knowledge, and motivation. The lateral temporal cortex is concerned with short-term verbal memory, naming, and reading. Finally, the anterior temporal pole is part of a bilateral semantic system representing object concepts and a left hemisphere-dominant network concerned with naming and understanding object names.Autobiography and Future Simulations
The major functional hubs include the PCC, mPFC, and angular gyrus. The hippocampus forms new declarative memories. The parahippocampal cortex (PHC) mediates spatial memory, navigation, and high-level visual processing like facial recognition. The retrosplenial cortex (RSC) is involved in episodic memory, navigation, predicting future events, and analyzing visual scenes. Finally, the posterior inferior parietal lobe (pIPL) integrates sensory information and participates in top-down attentional orienting.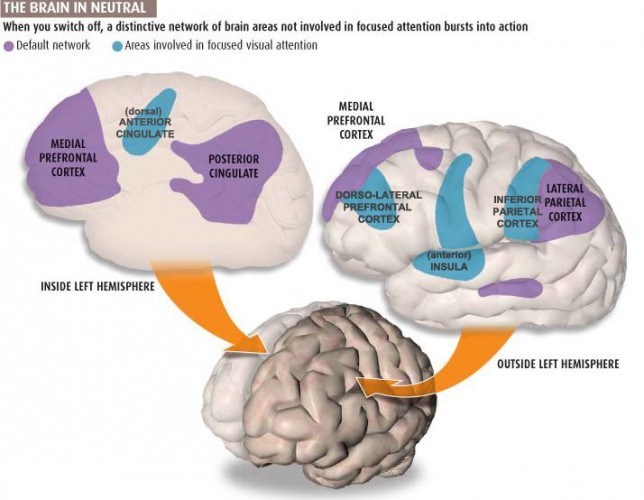
Glossary
acute stress response: autonomic changes that occur at the end of Selye’s alarm stage, for example, increased heart rate.
adaptation energy: in Selye’s General Adaptation Syndrome, the capacity of local organs to respond to the demands created by stressors. Depletion of adaptation energy theoretically results in local adaptation syndromes like muscle fatigue and tissue inflammation.
adrenal cortex: the outer region of the adrenal gland that produces the hormone cortisol.
adrenal medulla: the inner region of the adrenal gland that produces the hormones epinephrine and norepinephrine.
affective intensity: in Barrett and Russell’s structural model, a dimension that ranges from activated to deactivated states.
affective network: a network that is triggered when we make mistakes and that monitors cognitive activity to predict when errors are likely, and greater executive control may be needed. The affective network includes the anterior cingulate cortex, hippocampal cortex, entorhinal cortex, superior temporal gyrus, inferior temporal gyrus, posterior parietal cortex, globus pallidus internal segment, substantia nigra, pars reticulata, and medial dorsal nucleus of the thalamus.
affective valence: in Barrett and Russell’s structural model, a dimension that ranges from unpleasant to pleasant affective states.
alarm: the first stage of Selye’s General Adaptation Syndrome that consists of shock and countershock phases.
allostasis: the maintenance of stability through change by mechanisms that anticipate challenge and adapt through behavior and physiological change.
allostatic load model: McEwen and Seeman’s hypothesis that when stressors are acute or repeatedly occur, biological responses to stress can harm the body.
amygdala: limbic system structure that participates in evaluating whether stimuli are threatening, establishing unconscious emotional memories, learning conditioned emotional responses, and producing anxiety and fear responses.
arousal: overall level of alertness.
attention: the selection of sensory information or cognition for enhanced processing.
attentional bottleneck: a filter that limits enhanced processing to only the highest priority stimuli.
attentional spotlight: a shift of selective attention to choose stimuli for enhanced processing.
biofeedback: (1) learning process that teaches an individual to control her physiological activity, (2) biofeedback training aims to improve health and performance, (3) instruments rapidly monitor an individual's performance and display it back to her, (4) the individual uses this feedback to produce physiological changes, (5) changes in thinking, emotions, and behavior often accompany and reinforce physiological changes, and (6) these changes become independent of external feedback from instruments. Information about psychophysiological performance is obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
biopsychosocial model: Engel’s perspective that the complex interplay of psychological, biological, and sociological factors results in health or illness.
catecholamines: chemical compounds containing catechol and amine groups, like dopamine, epinephrine, and norepinephrine, derived from the amino acid tyrosine.
central executive network: structures including the dorsolateral prefrontal cortex, anterior cingulate cortex, and orbitofrontal cortex responsible for cognitive regulation of behavior.
central nucleus of the amygdala: the region of the amygdala that orchestrates the amygdala’s response to stressors. For example, it activates the paraventricular nucleus (PVN) of the hypothalamus, resulting in increased CRH release to the pituitary gland.
challenge: in Lazarus and Folkman’s Transactional Model of stress, an individual’s assessment during primary appraisal of her potential to cope with an event and gain from this opportunity.
cingulate cortex: cortex which lies above the corpus callosum that is responsible for the motivation dimension of attention, like pain due to physical injury and social rejection.
conditioned response (CR): in classical conditioning, a response (blood pressure rise) elicited by a conditioned stimulus (criticism).
conditioned stimulus: in classical conditioning, a stimulus (dentist's office), that in association with an unconditioned stimulus (pain), elicits an unconditioned response (anxiety) like the original unconditioned response.
corticotropin (ACTH): the hormone released by the pituitary gland following CRH binding that triggers cortisol release by the adrenal cortex.
corticotropin releasing hormone (CRH): the hormone released by the hypothalamus that triggers ACTH release by the pituitary gland.
cortisol: a glucocorticoid produced by the adrenal cortex that helps convert fat and protein to glucose and reduces inflammation.
countershock phase: the last part of Selye’s alarm stage of the General Adaptation Syndrome during which resistance increases due to increased activity by local defenses.
covert attention: an attentional focus independent of sensory orientation.
creative fluency: generating creative ideas like alternative uses for everyday objects.
default mode network: frontal, temporal, and parietal lobe circuits that are active during introspection and daydreaming and relatively inactive when we pursue external goals.
diathesis: inherited or acquired biological vulnerability. For example, obesity is a diathesis for diabetes.
diseases of adaptation: in Selye’s General Adaptation Syndrome, depletion of adaptation energy theoretically results in adaptation syndromes like atrial tachycardia.
distress: Selye’s term for stress due to negative stimuli.
divided attention tasks: situations where subjects must simultaneously process two or more stimuli.
dorsal frontoparietal system: the network comprised of the intraparietal sulcus and frontal eye field responsible for the top-down direction of attention.
dorsolateral prefrontal cortex: the left dorsolateral prefrontal cortex is concerned with approach behavior and positive affect. It helps us select positive goals and organizes and implements behavior to achieve these goals. The right dorsolateral prefrontal cortex organizes withdrawal-related behavior and negative affect and mediates threat-related vigilance. It plays a role in working memory for object location.
dove strategy: passive, reactive, nonaggressive, and cautious response to stressors.
early selection: filtering out lower-priority competing stimuli before preliminary perceptual and semantic analysis.
endogenous attention: voluntary attention that directs the attentional spotlight to support cognitive system priorities.
epinephrine: adrenal medulla hormone that increases muscle blood flow, converts stored nutrients into glucose for use by skeletal muscles, and initiates cardiac muscle contraction when it binds to β1 receptors.
eustress: Selye’s term for stress due to positive stimuli.
executive network: a network responsible for allocating attention, cognitive inhibition, behavioral inhibition, working memory, and cognitive flexibility. The executive network includes the dorsolateral prefrontal cortex, posterior parietal cortex, arcuate premotor area, globus pallidus internal segment, substantia nigra, pars reticulata, ventral anterior nucleus of the thalamus, and medial dorsal nucleus of the thalamus.
exhaustion: the third stage of Selye’s General Adaptation Syndrome during which increased endocrine activity depletes body resources and raises cortisol levels resulting in suppressed immunity, stress syndrome symptoms, and possible hospitalization and death.
exogenous attention: involuntary reflexive attention that redirects attention based on the novelty or importance of incoming stimuli.
fight-or-flight response: Cannon’s response of confronting or fleeing a threat that occurs at the end of Selye’s alarm stage.
frontal eye field (FEF): region of the premotor cortex that directs gaze towards targets selected by the IPS.
General Adaptation Syndrome (GAS): Selye proposed that diverse stressors produce a three-stage (alarm, resistance, and exhaustion) autonomic and endocrine response in all subjects.
harm: in Lazarus and Folkman's Transactional Model of Stress, damage that has already occurred. For example, a heart attack survivor may perceive harm as damage to the heart muscle.
hassle: minor stressful event, for example, waiting in a checkout line.
Hassles and Uplifts Scale: DeLongis, Folkman, and Lazarus’s revised 53-item scale measured hassle frequency and intensity. This scale better predicted headache frequency and intensity and inflammatory bowel disease frequency than the Social Readjustment Rating Scale (SRRS).
Hassles Scale: Kanner and colleagues’ 117-item scale that measures negative daily experiences.
hawk strategy: a proactive and bold response to stressors.
heart rate variability (HRV): beat-to-beat changes in heart rate, including changes in the RR intervals between consecutive heartbeats.
hippocampal formation: the limbic structure involved in controlling the endocrine system’s response to stressors, formation of explicit memories, and navigation. Cortisol binding to this structure disrupts these functions, interferes with creating new neurons, and harms and kills hippocampal neurons.
hypothalamic-pituitary-adrenal (HPA) axis: the hormonal cascade that starts with signals from the amygdala to the hypothalamus and ultimately targets the adrenal glands, releasing the hormones CRH, ACTH (corticotropin), and cortisol.
hypothalamus: a forebrain structure located below the thalamus that dynamically maintains homeostasis by controlling the autonomic nervous system, endocrine system, survival behaviors, and interconnections with the immune system.
insula: the cortical region located within the lateral sulcus of the frontal, parietal, and temporal lobes that functions as an integrative and organization hub for the salience network.
intraparietal sulcus (IPS): the region of the parietal lobe that provides voluntary top-down steering of attention.
late selection: filtering out competing stimuli after performing extensive analysis.
locus of control: Rotter’s concept of a continuum of control of outcomes where internals attribute outcomes to their efforts and externals attribute them to external events. This concept overlaps with the concepts of mastery, perceived control, and self-efficacy.
mastery: the relatively stable expectancy that we can control our personal outcomes. This concept overlaps with the concepts of locus of control, perceived control, and self-efficacy.
microbiome: the collection of the microorganisms that reside in the human body.
motor network: the network that plans, initiates and inhibits voluntary movements and muscle contractions. The motor network includes the supplementary motor area, premotor cortex, primary motor cortex, primary somatosensory cortex, cerebellum, arcuate premotor area, globus pallidus internal segment, substantia nigra, pars reticulata, and ventral lateral nucleus of the thalamus.
myelinated vagus: in Porges' polyvagal theory, the phylogenetically newer ventral vagal complex that rapidly adjusts cardiac output and promotes social engagement.
negative affective states: in Barrett and Russell’s structural model, unpleasant states like sadness are located in the left hemisphere.
negative affectivity: a predisposition toward distress and dissatisfaction. Individuals who are rated high on this trait negatively perceive themselves, others, and the environment and have a pessimistic perspective.
neurofeedback: information about EEG activity obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
neuroplasticity: the ability of neurons and their networks to remodel themselves in response to experience.
norepinephrine: an adrenal medullary hormone that increases muscle blood flow and converts stored nutrients into glucose for skeletal muscles.
nucleus (PVN) of the hypothalamus: when activated by the central nucleus of the amygdala, this nucleus releases CRH to the pituitary gland.
oculomotor network: a network that programs and initiates voluntary eye movements, inhibits eye movements toward distracting stimuli, and allows us to return our focus to locations we've experienced in the past. The oculomotor network includes the frontal eye field, dorsolateral prefrontal cortex, posterior parietal cortex, caudate, globus pallidus internal segment, substantia nigra, pars reticulata, ventral anterior nucleus of the thalamus, and medial dorsal nucleus of the thalamus.
overt attention: the agreement between attentional focus and sensory orientation.
oxytocin: a hormone and neurotransmitter that may contribute to social bonding, anxiety following exposure to stressors, and the milk letdown reflex.
palliation: in Lazarus and Folkman’s Transactional Model of Stress, secondary appraisal can lead to efforts to reduce our stress response rather than attack the stressor.
parasympathetic responder: a response stereotypy in which an individual may increase digestive activity, constrict the lungs' alveoli, and faint from low blood pressure when challenged by stressors.
perceived control: an individual’s expectancy that she can influence her outcomes. This concept overlaps with the concepts of locus of control, mastery, and self-efficacy.
Perceived Stress Scale (PSS): Cohen and colleagues’ scale that measures perceived hassles, major life changes, and shifts in coping resources during the previous month using a 14-item scale. PSS items assess the degree to which respondents rate their lives as unpredictable, uncontrollable, and overloaded.
perceptual load: stimulus processing demands.
pituitary gland: the endocrine gland found at the base of the skull that is divided into the anterior pituitary, which secretes the tropic hormones adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, and growth hormone (GH), and the posterior pituitary that releases oxytocin or vasopressin produced by the hypothalamus.
polyvagal theory: Porges' theory that the unmyelinated vagus (dorsal vagus complex) and newer myelinated vagus (ventral vagal complex) mediate competing adaptive responses.
positive states: in Barrett and Russell’s structural model, pleasant states like contentment are located in the right hemisphere.
posttraumatic stress disorder (PTSD): severe and long-lasting trauma and stressor-related disorder that often develops within three months of a traumatic event and may include re-experiencing a traumatic event, avoidance of stimuli associated with the trauma, numbing of responsiveness, and hyperarousal.
prefrontal cortex: the most anterior region of the frontal lobes divided into orbitofrontal and ventromedial, dorsolateral prefrontal cortex, and anterior and ventral cingulate cortex subdivisions, and is responsible for the brain’s executive functions.
primary appraisal: in Lazarus and Folkman’s Transactional Model of Stress, the first stage of our response to an event during which we categorize the consequences of events as positive, neutral, or negative and determine whether an event is relevant and negative, or potentially harmful. We evaluate these events for their possible harm, threat, or challenge.
psychoneuroimmunology: Solomon and Moos’ term for a multidisciplinary field that studies the interactions between behavior and the nervous system, endocrine system, and immune system.
pulvinar nucleus: the posterior region of the thalamus that processes visual information and directs attention.
raphe system: a network of serotonergic neurons located in the brainstem that includes anxiety-producing and anxiety-reducing pathways that terminate on the hippocampus.
reappraisal: in Lazarus and Folkman’s Transactional Model of Stress, secondary appraisal can modify our perception of a threat when direct action is impractical or unsuccessful.
resistance: the second stage of Selye’s General Adaptation Syndrome where local defenses have made the generalized stress response unnecessary. Both cortisol output and stress symptoms, like adrenal gland enlargement, decline.
response stereotypy: a person’s unique response pattern to stressors of identical intensity.
salience network: structures including the insula and anterior cingulate cortex that seek to monitor our external and internal environments to determine which of these inputs are salient and require further processing and attention.
secondary appraisal: in Lazarus and Folkman’s Transaction Model of Stress, the second stage of our response to an event during which we evaluate whether our coping abilities and resources can surmount an event's harm, threat, or challenge.
self-efficacy: an individual’s expectancy that they can influence her outcomes. This concept overlaps with the concepts of locus of control, mastery, and perceived control.
shock phase: the first part of Selye’s alarm stage of the General Adaptation Syndrome that includes the reduced body stress resistance and increased autonomic arousal and hormone release (ACTH, cortisol, epinephrine, and norepinephrine) that comprise the “fight-or-flight” response.
social network: the network that mediates socially responsible behavior, empathy, behavioral inhibition, emotional regulation, and sound judgment. The social network includes the orbitofrontal cortex, superior temporal gyrus, inferior temporal gyrus, anterior cingulate cortex, caudate, globus pallidus internal segment, substantia nigra, pars reticulata, ventral anterior nucleus of the thalamus, and medial dorsal nucleus of the thalamus.
Social Readjustment Rating Scale (SRRS): Holmes and Rahe measured major positive and negative life changes using their Social Readjustment Rating Scale (SRRS), which lists 43 events, each assigned a different Life Change Unit (LCU) value.
stress: Selye’s term for a nonspecific response to stimuli called stressors.
stress-diathesis model: the view that stressors interact with our inherited or acquired biological vulnerabilities, diatheses, to produce medical and psychological symptoms.
stressors: Selye’s term for stimuli that elicit the stress response.
structural model: Barrett and Russell's representation of affective states within a circumplex (circular structure) based on its degrees of affective valence (unpleasant to pleasant) and affective intensity (activation to deactivation).
superior colliculus: the dorsal midbrain structure composed of gray matter that processes visual information, directs visual gaze and visual attention to selected stimuli, and participates in overt and covert attention.
sympathetic nervous system (SNS): autonomic nervous system branch that regulates activities that expend stored energy, such as when we are excited.
sympathetic responder: a response stereotypy in which an individual may increase blood pressure, heart rate, and sweat gland activity and decrease heart rate variability and peripheral blood flow pressure when challenged by stressors.
sympathetic-adrenomedullary path (SAM) pathway: during an acute stress response, the sympathetic nervous system directs the release of the hormones epinephrine and norepinephrine by the adrenal medulla.
telomerase: an enzyme that adds DNA to telomeres. Telomerase levels decline with chronic stress and cellular aging.
telomere: DNA and protein that cover the ends of chromosomes. Telomeres shorten with chronic stress and cellular aging.
temporoparietal junction (TPJ): the intersection of the superior temporal gyrus and inferior parietal lobe that mediates bottom-up shifts in attention in response to stimulus attributes.
tend-and-befriend response: Taylor and colleagues’ proposition that women may tend (nurture others) and befriend (seek and provide social support) in response to stressors.
threat: in Lazarus and Folkman’s Transactional Model of Stress, we evaluate events for the damage they could inflict in the future during primary appraisal.
Transactional Model of Stress: Lazarus and Folkman’s cognitive model proposed that stress is determined by our perception of the situation.
traumatic stress: stress produced by a highly intense stressor that disrupts coping and endangers ourselves or others.
unmyelinated vagus: in Porges' polyvagal theory, the phylogenetically older dorsal vagus complex that responds to threats through immobilization, feigning death, passive avoidance, and shutdown.
uplift: a minor positive event like receiving an unexpected call from a friend.
vagal withdrawal: the inhibition of the myelinated vagus, often by daily stressors.
ventromedial prefrontal cortex: region of the prefrontal cortex may play a role in calculating risk and the emotional responses of anxiety and fear. Cortisol binding to this structure increases anxiety and fear and disrupts and kills neurons.
Yerkes-Dodson curve: an inverted U-curve that illustrates the relationship between pressure and performance.
REVIEW FLASHCARDS ON QUIZLET
Click on the Quizlet logo to review our chapter flashcards.
Assignment
Now that you have completed this module, how has it changed your understanding of stress? Explain how the top-down and bottom-up attentional systems work together to direct our focus.
References
Alexander, G. E., DeLong, M. R., & Strick, P. L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual Review of Neuroscience, 9, 357-381. https://doi.org/10.1146/annurev.ne.09.030186.002041
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author.
Andreassi, J. L. (2000). Psychophysiology: Human behavior and physiological response. Lawrence Erlbaum Associates, Publishers.
Andrews-Hanna, J. R., Reidler, J. S., Huang, C., & Buckner, R. L. (2010). Evidence for the default network's role in spontaneous cognition. J Neurophysiol., 104, 1664-1671. https://doi.org/10.1152/jn.00830.2009
Asterita, M. F. (1985). The physiology of stress. Human Sciences Press, Inc.
Bangasser, D. A. (2013). Sex differences in stress-related receptors: 'Micro' differences with 'macro' implications for mood and anxiety disorders. Biology of Sex Differences, 4(1), 2. https://doi.org/10.1186/2042-6410-4-2
Bangasser, D. A., & Valentino, R. J. (2014). Sex differences in stress-related psychiatric disorders: Neurobiological perspectives. Frontiers in Neuroendocrinology, 35(3), 303-319. https://doi.org/10.1016/j.yfrne.2014.03.008
Barrett, L. F., & Russell, J. A. (1998). Independence and bipolarity in the structure of current affect. Journal of Personality and Social Psychology, 74, 967-984. https://doi.org/10.1037/0022-3514.74.4.967
Bee, M. A., & Micheyl, C. (2008). The cocktail party problem: What is it? How can it be solved? And why should animal behaviorists study it? Journal of Comparative Psychology, 122(3), 235-251. https://doi.org/10.1037/0735-7036.122.3.235
Brannon, L., Updegraff, J. A., & Feist, J. (2022). Health psychology (10th ed.). Wadsworth, Cengage Learning.
Breedlove, S, M., & Watson, N. V. (2020). Behavioral neuroscience (9th ed.). Sinauer Associates, Inc.
Brett, J. F., Brief, A. P., Burke, M. J., George, J. M., & Webster, J. (1990). Negative affectivity and the reporting of stressful life events. Health Psychology, 9, 57-68. https://doi.org/10.1037//0278-6133.9.1.57
Buchsbaum, M. S., Buchsbaum, B. R., Chokron, S., Tang, C., Wei, T. C., & Byne, W. (2006). Thalamocortical circuits: fMRI assessment of the pulvinar and medial dorsal nucleus in normal volunteers. Neuroscience Letters, 404(3), 282-287. https://doi.org/10.1016/j.neulet.2006.05.063
Cannon, W. (1932). The wisdom of the body. Norton.
Carney, R. M., Blumenthal, J. A., Freedland, K. E., Stein, P. K., Howells, W. B., Berkman, L. F., Watkins, L. L., Czajkowski, S. M., Hayano, J., Domitrovich, P. P., & Jaffe, A. S. (2005). Low heart rate variability and the effect of depression on post-myocardial infarction mortality. Archives of Internal Medicine, 165, 486-1491. https://doi.org/10.1001/archinte.165.13.1486
Carpenter, S. (2012). That gut feeling. Monitor on Psychology, 43(8), 50.
Cohen, S., Doyle, W. J., Skoner, D. P., Rabin, B. S., Gwaltney, J. M., & Newson, J. T. (1995). State and trait negative affect as predictors of objective and subjective symptoms of respiratory viral infections. Current Directions in Psychological Science, 5, 86-90. https://doi.org/10.1037//0022-3514.68.1.159
Corbetta, M., & Shulman, G. I. (1998). Human cortical mechanisms of visual attention during orienting and search. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences, 353(1373), 1353-1362. https://doi.org/10.1098/rstb.1998.0289
Corbetta, M., & Shulman, G. I. (2002). Control of goal-directed and stimulus-driven attention in the brain. Nature Reviews: Neuroscience, 3(3), 201-215. https://doi.org/10.1038/nrn755
Crandall, C. S., Preisler, J. J., & Aussprung, J. (1992). Measuring life event stress in the lives of college students: The Undergraduate Stress Questionnaire (USQ). Journal of Behavioral Medicine, 15, 627-662. https://doi.org/10.1007/BF00844860
David, D. H., & Lyons-Ruth (2005). Differential attachment responses of male and female infants to frightening maternal behavior: Tend or brief versus fight or flight? Infant Mental Health Journal, 26, 1-18. https://doi.org/10.1002/imhj.20033
DeLongis, A., Folkman, S., & Lazarus, R. S. (1988). The impact of daily stress on health and mood. Psychological and social resources as mediators. Journal of Personality and Social Psychology, 54, 486-495. https://doi.org/10.1037/0022-3514.54.3.486
Dohrenwend, B. S., & Dohrenwend, B. P. (1984). Life stress and illness: Formulation of the issues. In B. S. Dohrenwend & B. P. Dohrenwend (Eds.). Stressful life events and their contexts (pp. 1-27). Rutgers University Press.
Engel, G. L. (1971). Sudden and rapid death during psychological stress. Folklore or folk wisdom? Annals of Internal Medicine, 74, 771-782. https://doi.org/10.7326/0003-4819-74-5-771
Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196, 129-136. https://doi.org/10.1126/science.847460
Engel, G. L. (1980). The clinical application of the biopsychosocial model. American Journal of Psychiatry, 137, 535-544. PMID: 7369396
Ferguson, E., Williams, L., O'Connor, R. C., Howard, S., Hughes, B. M., Johnston, D. W., Allan, J. L., O'Connor, D. B., Lewis, C. A., Grealy, M. A., & O'Carroll, R. E. (2009). A taxometric analysis of Type-D personality. Psychosomatic Medicine, 71(9), 981-986. https://doi.org/10.1097/PSY.0b013e3181bd888b
Fox, I., & Rompolski, K. (2022). Human physiology (16th ed.). McGraw Hill.
Frasure-Smith, N., Lesperance, F., & Talajic, M. (1995). Depression and 18-month prognosis after myocardial infarction. Circulation, 91(4), 999-1005. https://doi.org/10.1161/01.cir.91.4.999
Gaidos, S. (2016). He stress, she stress: Scientists puzzle over why men and women react differently to pressure. Science News, 189(2), 18-21.
Gunthert, K. C., Cohen, L. H., & Armeli, S. (1999). The role of neuroticism in daily stress and coping. Journal of Personality and Social Psychology, 77, 1087-1100. https://doi.org/10.1037//0022-3514.77.5.1087
Harrell, E. H., Kelly, K., & Stutts, W. A. (1996). Situational determinants of correlations between serum cortisol and self-reported stress measures. Psychology: A Journal of Human Behavior, 33, 22-25.
Holmes, T. H., & Rahe, R. H. (1967). The Social Readjustment Rating Scale. Journal of Psychosomatic Research, 11, 213-218. https://doi.org/10.1016/0022-3999(67)90010-4
Johnson, J. H. (1986). Life events as stressors in childhood and adolescence. Sage.
Johnston-Brooks, C. H., Lewis, M. A., Evans, G. W., Whalen, C. K. (1998). Chronic stress and illness in children: The role allostatic load. Psychosomatic Medicine, 60, 597-603. https://doi.org/10.1097/00006842-199809000-0001
Kanner, A. D., Coyne, J. C., Schaefer, C., & Lazarus, R. S. (1981). Comparison of two modes of stress measurement: Daily hassles and uplifts versus major life events. Journal of Behavioral Medicine, 4, 1-39. https://doi.org/10.1007/bf00844845
Karlamangla, A. S., Singer, B. H., & Seeman, T. E. (2006). Reduction in allostatic load in older adults is associated with lower all-cause mortality risk: MacArthur studies of successful aging. Psychosomatic Medicine, 68, 500-507. https://doi.org/10.1097/01.psy.0000221270.93985.82
Katz, M. J., Derby, C. A., Wang, C., Sliwinski, M. J., Martin, J., Ezzati, A., . . . Lipton, R. B. (in press). Influence of perceived stress on incident amnestic mild cognitive impairment: Results from the Einstein Aging Study. Alzheimer Disease & Associated Disorders. https://doi.org/10.1097/WAD.0000000000000125
Kawamura, N., Kim, Y., & Asukai, N. (2001). Suppression of cellular immunity in men with a past history of posttraumatic stress disorder. American Journal of Psychiatry, 158, 484-486. https://doi.org/10.1176/appi.ajp.158.3.484
Keller, A., Litzelman, K., Wisk, L. E., Maddox, T., Cheng, E. R., Creswell, P. D., & Witt, W. P. (2012). Does the perception that stress affects health matter? The association with health and mortality. Healthy Psychology, 31(5), 677-684. https://doi.org/10.1037/a0026743.
Kemeny, M. E. (2003). The psychobiology of stress. Current Directions in Psychological Science, 12, 124-129. https://doi.org/10.1111/1467-8721.01246
Kessler, R. C., Berglund, P., Delmer, O., Jin, R., Merikangas, K. R., & Walters, E .E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593-602. https://doi.org/10.1001/archpsyc.62.6.593
Khazan, I. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. John Wiley & Sons, Ltd.
Kivlinghan, K. T., Granger, D. A., & Booth, A. (2005). Gender differences in testosterone and cortisol response to competition. Psychoneuroendocrinology, 30, 58-71. https://doi.org/10.1016/j.psyneuen.2004.05.009
Kroptov, J. D. (2009). Quantitative EEG, event-related potentials and neurotherapy. Academic Press, Elsevier.
Lacey, K., Zaharia, M. D., Griffiths, J., Ravindran, A. V., Merali, Z., & Anisman, H. (2000). A prospective study of neuroendocrine and immune alterations associated with the stress of an oral academic examination among graduate students. Psychoneuroendocrinology, 25, 339-356. https://doi.org10.1016/s0306-4530(99)00059-1
Lavie, N., Hirst, A., de Fockert, J. W., & Viding, E. (2004). Load theory of selective attention and cognitive control. Journal of Experimental Psychology: General, 133(3), 339-354. https://doi.org/10.1037/0096-3445.133.3.339
Lazarus, R. S. (1984). Puzzles in the study of daily hassles. Journal of Behavioral Medicine, 7, 375-389. https://doi.org/10.1007/BF00845271
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
Mason, J. W. (1971). A reevaluation of the concept of "nonspecificity" in stress theory. Journal of Psychiatric Research, 8, 323-333.
McEwen, B. S. (2000). Allostasis and allostatic load: Implications for neuropsychopharmacology. Neuropsychopharmacology, 22,108-124.
McEwen, B. S. (2002). The end of stress as we know it. Joseph Henry Press.
McEwen, B. S. & Seeman, T. (1999). Protective and damaging effects of mediators of stress: Elaborating and testing the concepts of allostasis and allostatic load. In Adler, N. E., Marmot, M., McEwen, B. S. & Stewart, J. (Eds.). Socioeconomic Status and Health in Industrial Nations: Social, Psychological and Biological Pathways. Ann NY Acad Sci, 896.
McEwen, B. S. & Seeman, T. (2003). Stress and affect: Applicability of the concepts of allostasis and allostatic load. In R. J. Davidson, K. R. Scherer, & H. H. Goldsmith (Eds.) Handbook of affective sciences. Oxford University Press.
McEwen, B. S., & Stellar, E. (1993). Stress and the individual: Mechanisms leading to disease. Archives of Internal Medicine, 153, 2093-2101. PMID: 8379800
McGonagle, K. A., & Kessler, R. C. (1990). Chronic stress, acute stress, and depressive symptoms. American Journal of Community Psychology, 18, 681-706. https://doi.org/10.1007/BF00931237
Menon, V., & Uddin, L. Q. (2010). Saliency, switching, attention and control: A network model of insula function. Brain Struct Function, 214(5-6), 655-667. https://doi.org/10.1007/s00429-010-0262-0
Ng, D. M., & Jefferey, R. W. (2003). Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychology, 22, 638-642. https://doi.org/10.1037/0278-6133.22.6.638
O'Dowd, T. C. (1987). To burn out or to rust out in general practice. J R Coll Gen Pract, 37(300), 290-291. PMID: 3449629
Paus, T., Kalina, M., Patocková, L., Angerová, Y., Cerný, R., Mecir, P., Bauer, J., & Krabec, P. (1991). Medial vs lateral frontal lobe lesions and differential impairment of central-gaze fixation maintenance in man. Brain, 114, 2051-2067. https://doi.org/10.1093/brain/114.5.2051
Rahe, R. H., & Arthur, R. J. (1978). Life change and illness studies: Past history and future directions. Journal of Human Stress, 4, 3-15. https://doi.org/10.1080/0097840X.1978.9934972
Ray, C., Jefferies, S., & Weir, W. R. (1995). Life-events and the course of chronic fatigue syndrome. British Journal of Medical Psychology, 68, 323-331. https://doi.org/10.1080/0097840X.1978.9934972
Ross, C. E., & Mirowsky, J. (1979). A comparison of life-event-weighting schemes: Change, undesirability, and effect-proportional indices. Journal of Health and Social Behavior, 20, 166-177. PMID: 479528
Russell, J. A., & Barrett, L. F. (1999). Core affect, prototypical emotional episodes, and other things called emotion: Dissecting the elephant. Journal of Personality and Social Psychology, 76(5), 805-819. https://doi.org/10.1037//0022-3514.76.5.805
Saalmann, Y. B., Pinsk, M. A., Wang, L., Li, X., & Kastner, S. (2012). The pulvinar regulates information transmission between cortical areas based on attention demands. Science, 337(6095), 753-756. https://doi.org/10.1126/science.1223082
Saey, T. H. (2016). Body's bacteria don't outnumber human cells so much after all: New calculations suggest roughly equal populations, not 10-to-1 ratio. Science News. Retrieved from https://www.sciencenews.org
Schwartz, G. E. (1982). Testing the biopsychosocial model: The ultimate challenge facing behavioral medicine? Journal of Consulting and Clinical Psychology, 50, 1040-1053.
Seeley, W. W., Menon, V., Schatzberg, A. F., Keller, J., Glover, G. H., Kenna, H., . . . Greicius, M. D. (2007). Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci, 27(9), 2349-2356. doi:10.1523/JNEUROSCI.5587-06.2007
Seeman, T. E., Singer, B. H., Rowe, J. W., Horwitz, R. I., & McEwen, B. S. (1997). Price of adaptation—allostatic load and its health consequences. Archives of Internal Medicine, 157, 2259-2268. PMID: 9343003
Selye, H. (1956). The stress of life. McGraw-Hill.
Selye, H. (1974). Stress without distress. Lippincott.
Selye, H. (1976). Stress in health and disease. Butterworth.
Sender, R., Fuchs, S., & Milo, R. (2016), Revised estimates for the number of human and bacteria cells in the body. BioRxiv. Posted online January 6, 2016.
Serido, J., Almeida, D. M., & Wethington, E. (2004). Chronic stress and daily hassles: Unique and interactive relationships with psychological distress. Journal of Health and Social Behavior, 45, 17-33. https://doi.org/10.1177/002214650404500102
Shirer, W. R., Ryali, S., Rykhlevskaia, E., Menon, V., Greicius, M. D. (2012). Decoding subject-driven cognitive states with whole-brain connectivity patterns. Cereb Cortex, 22. https://doi.org/158–165.10.1093/cercor/bhr099
Shofty, B., Gonent, T., Bergmann, E., Mayseless, N., Korn, A., Shamay-Tsoory, S., Grossman, R., Jalon, I., & Ram, Z. (2022). The default network is causally linked to creative thinking. Molecular Psychiatry. https://doi.org/10.1038/s41380-021-01403-8
Silva, R. P., Alpert, M., Munoz, D. M., Singh, S., Matzner, F., & Dummit, S. (2000). Stress and vulnerability to posttraumatic stress disorder in children and adolescents. Journal of Psychiatry, 157, 1229-1235. https://doi.org/10.1176/appi.ajp.157.8.1229
Sonstroem, R. J. (1997). Physical activity and self-esteem. In W. P. Morgan (Ed.), Physical activity and mental health (pp. 127-143). Taylor & Francis.
Stein, M. B., Walker, J. R., & Forde, D. R. (2000). Gender differences in susceptibility to posttraumatic stress disorder. Behavior Research and Therapy, 38, 619-628. https://doi.org/10.1016/s0005-7967(99)00098-4
Sutton, S. K., & Davidson, R. J. (1997). Prefrontal brain asymmetry: A biological substrate of the behavioral approach and inhibition systems. Psychological Science, 8, 204-210. https://doi.org/10.1111/j.1467-9280.1997.tb00413.x
Taylor, S. E., Klein, L. C., Lewis, B. P., Gruenewald, T. L., Gurung, R. A. R., & Updegraff, J. A. (2000). Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107, 411-429. https://doi.org10.1037/0033-295x.107.3.411
Thompson, M., & Thompson, L. (2015). The neurofeedback book (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Tice, D. M., Bratslavsky, E., & Baumeister, R. F. (2001). Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! Journal of Personality and Social Psychology, 80, 53-67. PMID: 11195891
Turner, R. J., & Avison, W. R. (1992). Innovations in the measurement of life stress: Crisis theory and the significance of event resolution. Journal of Health and Social Behavior, 33, 36-50. https://doi.org/10.2307/2136856
Turner, R. J., & Avison, W. R. (2003). Status variations in stress exposure: Implications for the interpretation of research on race, socioeconomic status, and gender. Journal of Health and Social Behavior, 44, 488-505. PMID: 15038145
Wiebking, C., & Northoff, G. (2014). Interoceptive awareness and the insula - Application of neuroimaging techniques in psychotherapy. GSTF International Journal of Psychology, 1(1), 53-60. https://doi.org/10.5176/0000-0002_1.1.8
Woolfolk, R. L., Lehrer, P. M., & Allen, L. A. (2007). Conceptual issues underlying stress management. In P. M. Lehrer, R. L. Woolfolk, & W. E. Sime (Eds.). Principles and practice of stress management (3rd ed.). The Guildford Press.
TEST YOURSELF ON CLASSMARKER
Click on the ClassMarker logo below to take a 10-question exam over this entire unit. There is no password.
