Patient/Client Assessment
What You Will Learn in This Chapter
This unit walks you through the comprehensive process of intake assessment for neurofeedback. You will explore how practitioners gather, organize, and integrate information from interviews, questionnaires, rating scales, cognitive tests, and psychophysiological measures to build a clear picture of each client's presenting concerns. You will also see how EEG assessment findings combine with intake data to create a holistic formulation that drives treatment planning and informed consent.
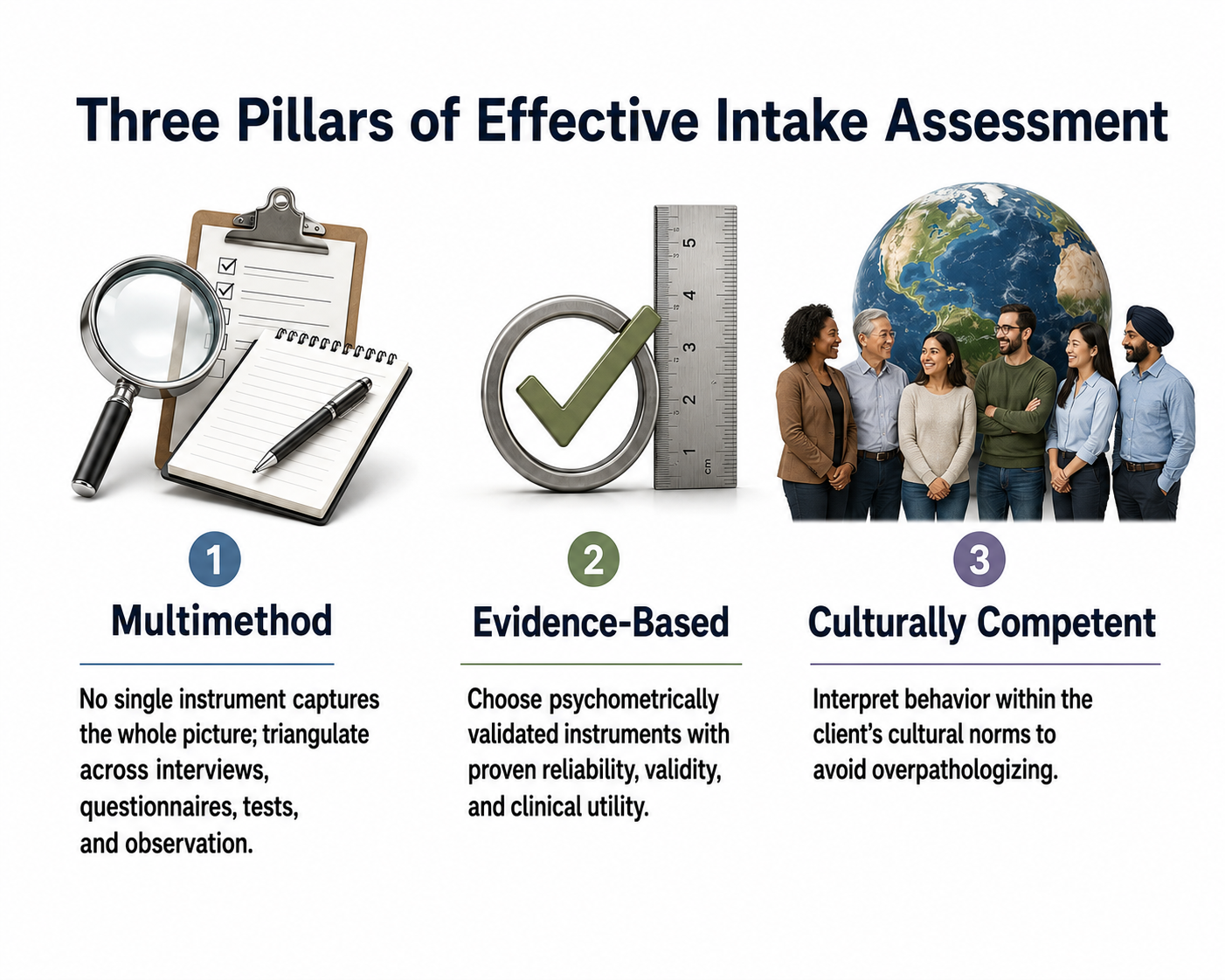
Effective assessment rests on three pillars: it should be multimethod, evidence-based, and culturally competent. Whether your client seeks relief from a clinical disorder or wants to sharpen athletic or military performance, a thorough intake lays the groundwork for successful neurofeedback training.
BCIA Blueprint Coverage: This unit addresses VI. Patient/Client Assessment - A. Intake Assessment and VI. Patient/Client Assessment - B. EEG Assessment.
Learning Objectives
After completing this section, you will be able to:
Describe the general purposes and methods of intake assessment for neurofeedback.
Explain the importance of multimethod, evidence-based, and culturally competent assessment.
Identify the types of quantitative and qualitative information gathered during an intake.
Describe how EEG assessment findings are integrated with intake information to guide treatment planning.
This section introduces three foundational principles that underpin every intake assessment: multimethod strategies, evidence-based instrument selection, and cultural competence. Together, these principles ensure that the information you collect is comprehensive, psychometrically sound, and sensitive to the diverse backgrounds of the clients you serve. Understanding these principles early will help you see why each subsequent step in the intake process matters.
Multimethod assessment means combining several evaluation tools because no single instrument can capture the full range of personality, behavior, and neurophysiological functioning relevant to a given client. Depending on your scope of practice and the client's presenting concerns, an intake may draw on questionnaires, interviews, objective personality tests, inventories, and behavioral observations (Pomerantz, 2020). Think of it as triangulation: each tool contributes a different angle on the same clinical picture, and the convergence of findings strengthens your confidence in the overall formulation.

Evidence-based assessment mirrors the broader movement toward evidence-based treatment. Practitioners should choose instruments that are psychometrically validated, meaning they demonstrate adequate reliability, validity, and clinical utility (Pomerantz, 2020). For example, the Beck Depression Inventory-II is widely used to measure the severity of depressive symptoms in adults precisely because decades of research support its reliability and validity. Its sensitivity and specificity as a screener depend on the cut score and the setting, so an elevated score calls for a clinical interview rather than standing on its own. Selecting well-validated tools is not merely an academic exercise; it directly affects the accuracy of your baseline data and the credibility of your treatment planning.
Culturally competent assessment requires sensitivity to how a given culture defines normality and abnormality. Providers who understand the cultural norms of the populations they serve are far less likely to engage in overpathologizing, the error of labeling culturally normal behavior as pathological because it is viewed through the provider's own cultural lens rather than the client's (Pomerantz, 2020). Dana (2005) went so far as to describe ignorance or insensitivity to cultural norms as cultural malpractice, a term that underscores the real-world harm that culturally uninformed assessment can inflict. In VA settings, military clinics, and diverse hospital systems alike, this principle is essential for accurate and equitable care.
BCIA Blueprint Coverage
This unit covers VI. Patient/Client Assessment - A. Intake Assessment and B. EEG Assessment.

This unit covers Intake Assessment, EEG Assessment for Neurofeedback, and their Integration.
Intake Assessment
Purposes of Intake Assessment
This section covers the core purposes of intake assessment: gathering information, sharing it with the client, and collaborative decision-making. It also addresses the specialized considerations that arise when working with performance-oriented clients. The overarching theme is that a well-conducted intake does more than collect data; it also builds the therapeutic relationship that sustains the entire course of neurofeedback training.
The general purposes of intake assessment are threefold: gathering information, sharing information, and supporting shared decision-making. Running in parallel with each of these is the essential goal of building a trusting working relationship that inspires the client's confidence that neurofeedback can help. The data collected during intake describe the presenting problem both qualitatively and quantitatively, and these measurements become the baseline against which all subsequent progress is judged.
Information from the intake also feeds into a clinical formulation, an explanatory model of why the problem occurs and what interventions are most likely to alleviate it. This formulation sets the stage for planning neurofeedback training and equips the client to give informed consent. In some practice settings, a further purpose of intake may be to establish a formal diagnosis.
Optimum Performance Assessment
Not every client comes to your office with a clinical disorder. Some practitioners focus their neurofeedback and biofeedback work on what is variously called peak performance, optimum performance, or simply performance training. These clients, who include athletes aiming to sharpen reaction time, musicians seeking better concentration under pressure, and military personnel training for sustained vigilance, do not generally view themselves as having a "presenting problem." Instead, their goal is to raise an already functional baseline to a higher level.
Despite this difference in framing, the assessment goals for performance clients closely mirror those for clinical clients. Identifying current levels of function and quantifying how they compare to normative benchmarks is just as important for guiding performance training as it is for treating a disorder. The desired outcomes are simply measured by different indicators: improved scores, higher ratings, better musical opportunities, or enhanced academic results specific to the client's pursuits.
A critical caution applies here. When working with performance clients, the assessment may reveal an underlying clinical issue, and communicating this finding requires tact and clinical judgment. Practitioners who are not licensed or registered health professionals may fail to recognize such issues altogether and could inadvertently select training protocols that worsen them. For this reason, practitioners working with optimum performance clients should apply the same comprehensive assessment techniques described throughout this section to ensure a thorough understanding and to avoid adverse outcomes.
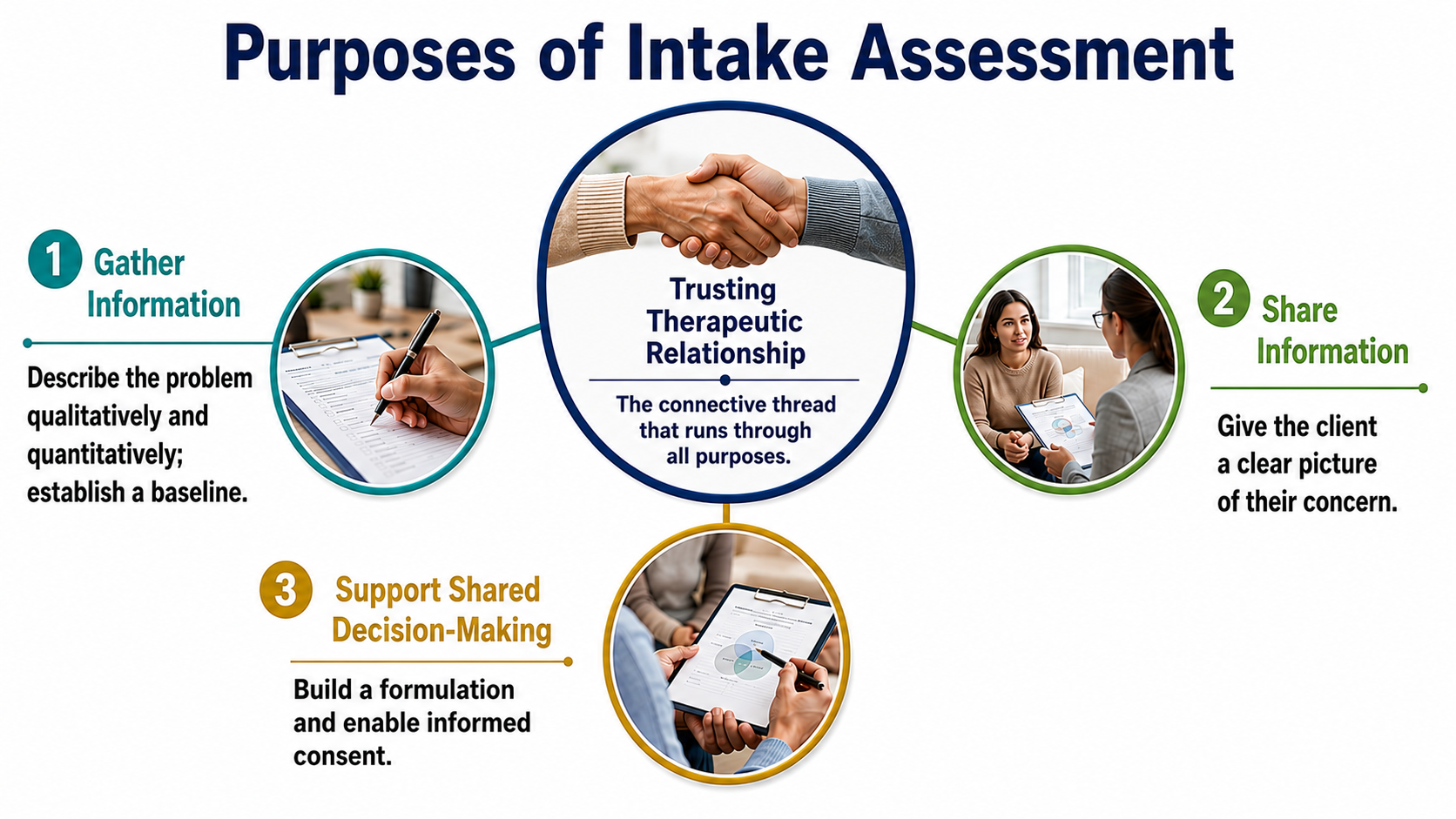
Intake assessment serves to gather and share information, support shared decision-making, and build a trusting therapeutic relationship. The results describe the problem qualitatively and quantitatively and establish a baseline for measuring progress. Performance clients require the same thorough assessment as clinical clients to avoid missing underlying issues that could be worsened by training.
Intake Assessment Methods
This section walks through the practical steps of the intake process, from the first phone call through the final review of outside reports. Each step is designed to collect a distinct type of information, and together they produce the comprehensive clinical picture that drives your treatment planning. Along the way, you will see how active listening and clear communication keep the client engaged and the data accurate.
Preliminary Steps
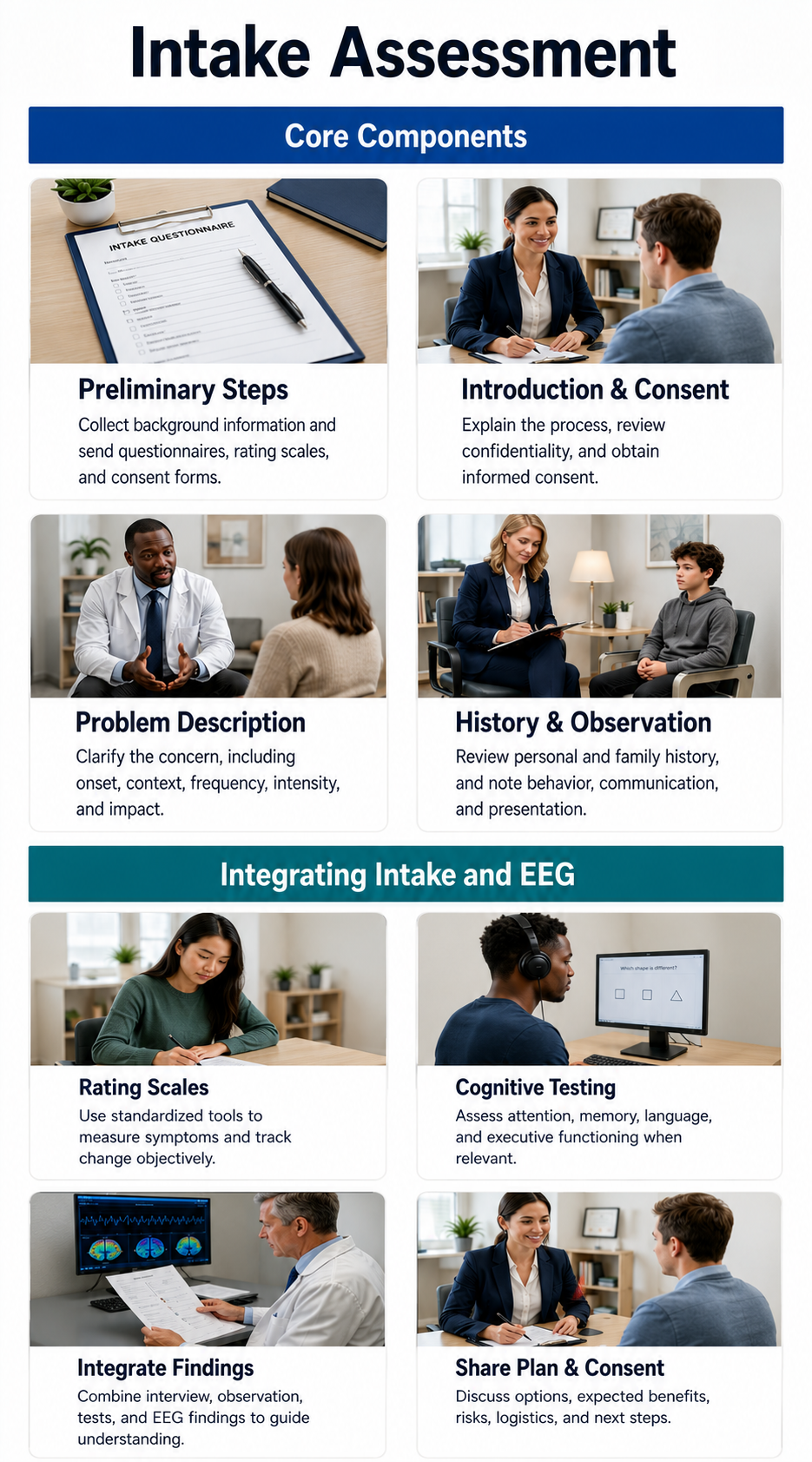
After the client or referral source makes initial contact, the practitioner can use that first conversation to collect basic background information, either by phone or by sending a questionnaire. If a background questionnaire is sent, it may be accompanied by standardized or non-standardized rating scales that the client is asked to complete before the first face-to-face meeting.
Alternatively, all background forms, questionnaires, and rating scales can be administered at the practitioner's office immediately before the intake interview. Some instruments can even be completed online in advance. When the client is a child, questionnaires and rating scales may be sent to a parent or another significant person in the child's life, such as a teacher. Consent forms can also be included with these preliminary materials.
Introduction and Consent
The first face-to-face meeting begins with the provider introducing themselves and outlining what the intake assessment will involve so the client knows what to expect. An essential early step is reviewing the limits of confidentiality and confirming that the client wishes to proceed; this consent should be documented. These initial moments set the tone for the entire professional relationship.
Throughout the intake, the provider should employ active listening and supportive communication skills to foster trust and credibility (Silverman et al., 2013). Clients who feel heard and respected are more likely to provide accurate, detailed information. If identifying details such as name, birthdate, address, and emergency contact information were not collected in advance, this is the time to gather them.
Problem Description
Following the introductory phase, the practitioner turns to the client's presenting problem and goal (Schwartz, 2016). A simple open-ended question, such as "Tell me what brings you in today," gives the client space to describe their concerns in their own words. A great deal can be learned in these first few minutes by listening without interruption; the practitioner can then follow up with targeted questions that flesh out the clinical picture.
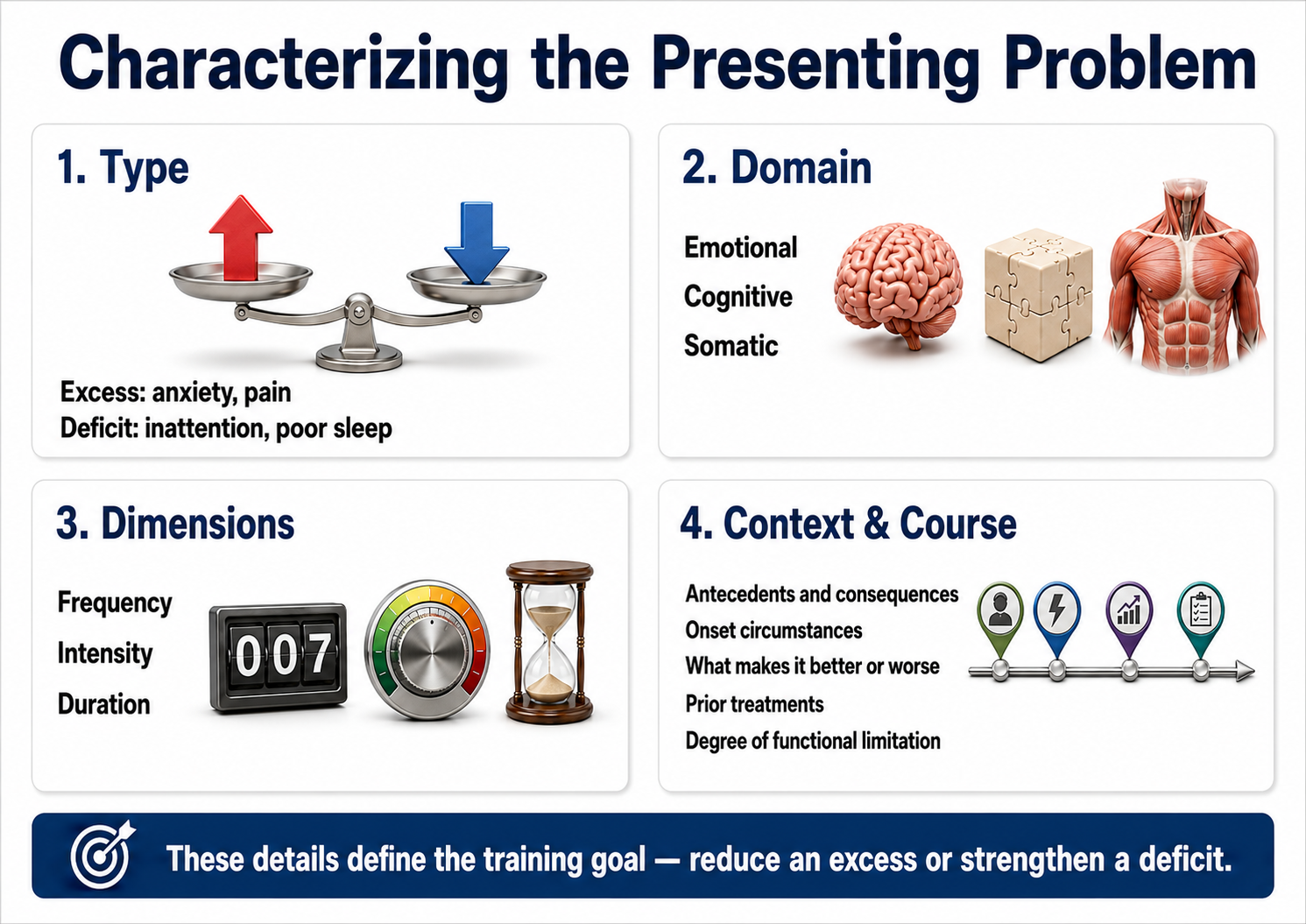
The goal of this inquiry is to construct a clear description of the primary concern. The problem may represent an excess (such as anxiety or pain) or a deficit (such as inattention or poor sleep) and may relate primarily to emotional, cognitive, or somatic functioning. Useful descriptors include the frequency, intensity, and duration of problem episodes. Context matters, too: the motivational conditions, antecedents, and consequences surrounding the behavior help explain when and why it occurs.
The clinical timeline is equally informative. When did the problem first appear, and what circumstances surrounded its onset? How has the symptom waxed and waned over time, and what factors make it worse or better? What has the client, or others, already tried to change the problem, and is the client receiving any concurrent treatment? Understanding the degree to which the issue limits daily functioning helps illustrate its severity and guides treatment intensity.
Together, these details allow the provider and client to define a training goal, such as decreasing a problematic excess or strengthening a deficient function. The EEG assessment results, discussed later in this unit, further refine this goal-setting process.
Personal and Family History
Understanding the broader context of the presenting problem requires a review of personal and family history (Stucky & Bush, 2017). Personal history topics typically include medication use, substance use, diet and exercise, sleep patterns, medical conditions, psychiatric history, family and social relationships, education, work experiences, legal matters, and military service. For each of these areas, it is helpful to ask about any prior treatment, specialized training, or accommodations the client has received.
Establishing the client's typical level of functioning provides an important reference point. The relevant domains include personal care, household management, socialization, community involvement, education or work, and leisure. Family history covers parents, siblings, and potentially other relatives, though it is usually more focused than the personal history, concentrating on issues directly relevant to the client's presenting problem, such as a family pattern of mood disorders or attention difficulties.
Diagnostic Interviewing
For registered or licensed health professionals, the information gathered during intake may contribute to a formal diagnosis. Several semi-structured interview formats exist to systematically elicit the information needed for psychiatric differential diagnosis. Medical practitioners may similarly arrive at a diagnosis by combining interview data with findings from physical examinations and laboratory or imaging tests.
Barriers, Strengths, and Client Perspective
A thorough intake goes beyond describing the problem; it also maps the personal, social, and material resources available for resolution. These resources might include high motivation, a supportive family, reliable transportation, or internet access for remote sessions. Equally important is identifying barriers, whether personal, social, or practical, that could impede progress. The client's own understanding of what causes the problem and what it will take to remedy it is a valuable point of inquiry, because treatment adherence improves when the provider and client share a coherent explanatory framework.
Behavioral Observation and Mental Status Examination
From the moment the client walks in, their manner of moving and speaking offers clinically relevant information. Gait, posture, eye contact, speech rate, and emotional expressiveness all contribute to the overall picture. In some clinical settings, the practitioner may administer a more formal mental status examination, a structured format for briefly assessing mental functioning that covers speech, emotion and affect, thought content and form, perceptual disturbances, cognition, reasoning, insight, and judgment (Sadock et al., 2017).
Collateral Interview
When clients may be unable to provide fully reliable information because of age, cognitive impairment, or limited insight into their own symptoms, an interview with a close relative or someone with significant direct experience with the client can be invaluable. Collateral information refers to these third-party reports from family members, friends, or other healthcare professionals. Such interviews may fill in gaps, introduce new information, and reveal inconsistencies that point to potential client deficits not captured in the primary interview.
Reports
Several types of existing reports may be relevant to the intake assessment, including medical and psychiatric records, academic transcripts, and vocational evaluations. If the client was referred by another professional, that referral report can shed valuable light on the reason for referral, attainable goals, and the likely predisposing, precipitating, and perpetuating factors behind the problem.
Although referral reports are often written, a direct phone conversation with the referral source can be especially informative for clarifying nuance. The client's consent should always be obtained before requesting any outside records.
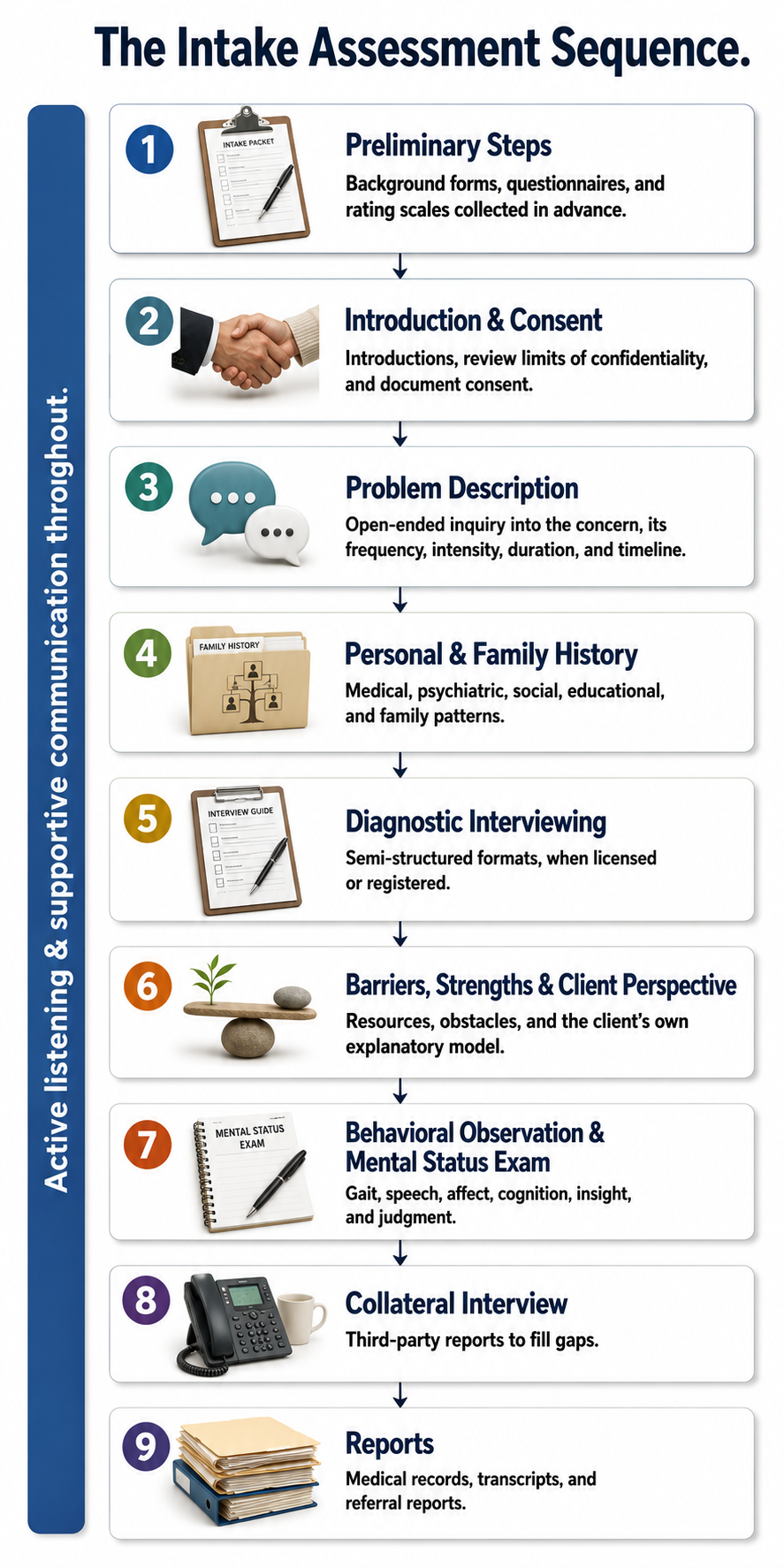
Intake methods span a structured sequence: preliminary data collection, an introductory meeting with consent review, detailed problem description, personal and family history, diagnostic interviewing when appropriate, identification of barriers and strengths, behavioral observation and mental status examination, collateral interviews, and review of relevant reports. Active listening and supportive communication build the therapeutic relationship throughout each step.
Questionnaires and Rating Scales
This section examines the specific instruments practitioners use to quantify and contextualize a client's presenting concerns: questionnaires, rating scales, cognitive tests, and psychophysiological measures. Each tool contributes a different type of data, whether qualitative, quantitative, or physiological, and together they form the evidence base against which neurofeedback training outcomes will later be measured.
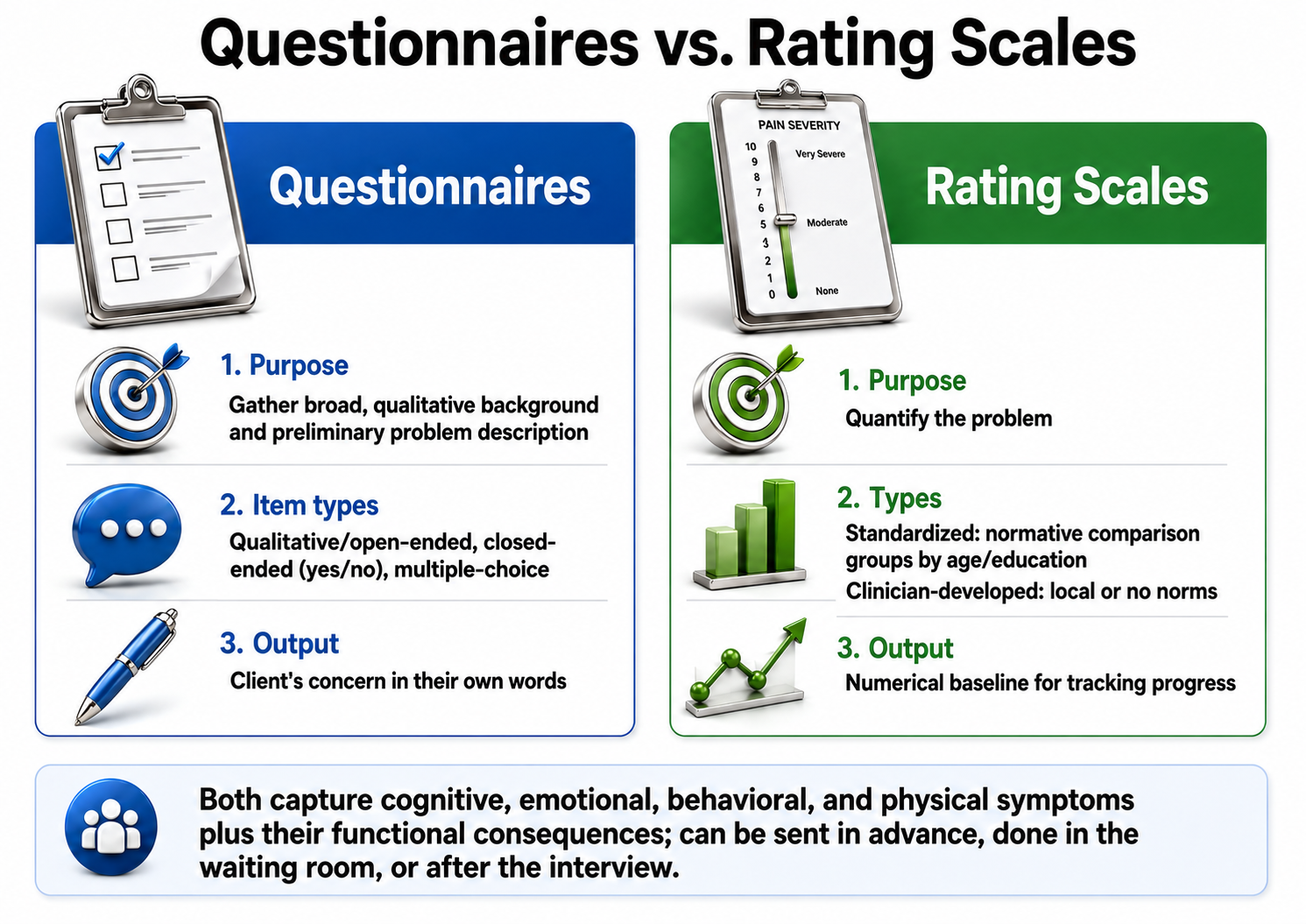
Questionnaires typically consist of checklists and open-ended items that allow clients to describe their concerns in their own words. Items may be qualitative (e.g., "Describe your primary concern"), closed-ended (e.g., "Have you ever had a seizure?"), or multiple-choice (e.g., "Check each type of caffeinated beverage you consume"). This flexibility makes questionnaires an efficient way to gather broad background information and a preliminary problem description.
Rating scales, by contrast, are designed to quantify a problem (Baer & Blais, 2010). Some are standardized instruments with normative data that compare the client's scores to those of matched reference groups based on variables such as age or education. Others are clinician-developed tools tailored to a specific practice setting and may or may not have local norms. Both questionnaires and rating scales can capture information about cognitive, emotional, behavioral, and physical symptoms, as well as the functional consequences of those symptoms, that is, the effect they have on practical, real-world ability and social adjustment (Psychology Tools, n.d.).
From a practical standpoint, information from questionnaires helps describe the presenting problem in qualitative terms and reveals how the client perceives it, while rating scales (together with later EEG results) provide the numerical baseline for tracking progress once training begins. These instruments can be sent in advance, completed in the waiting room, or administered after the interview, and collecting data beforehand makes the interview itself more focused and efficient (Pomerantz, 2020). Some questionnaires and rating scales are proprietary, while others are freely available in the public domain; informant versions also exist for gathering collateral perspectives.
Cognitive Tests
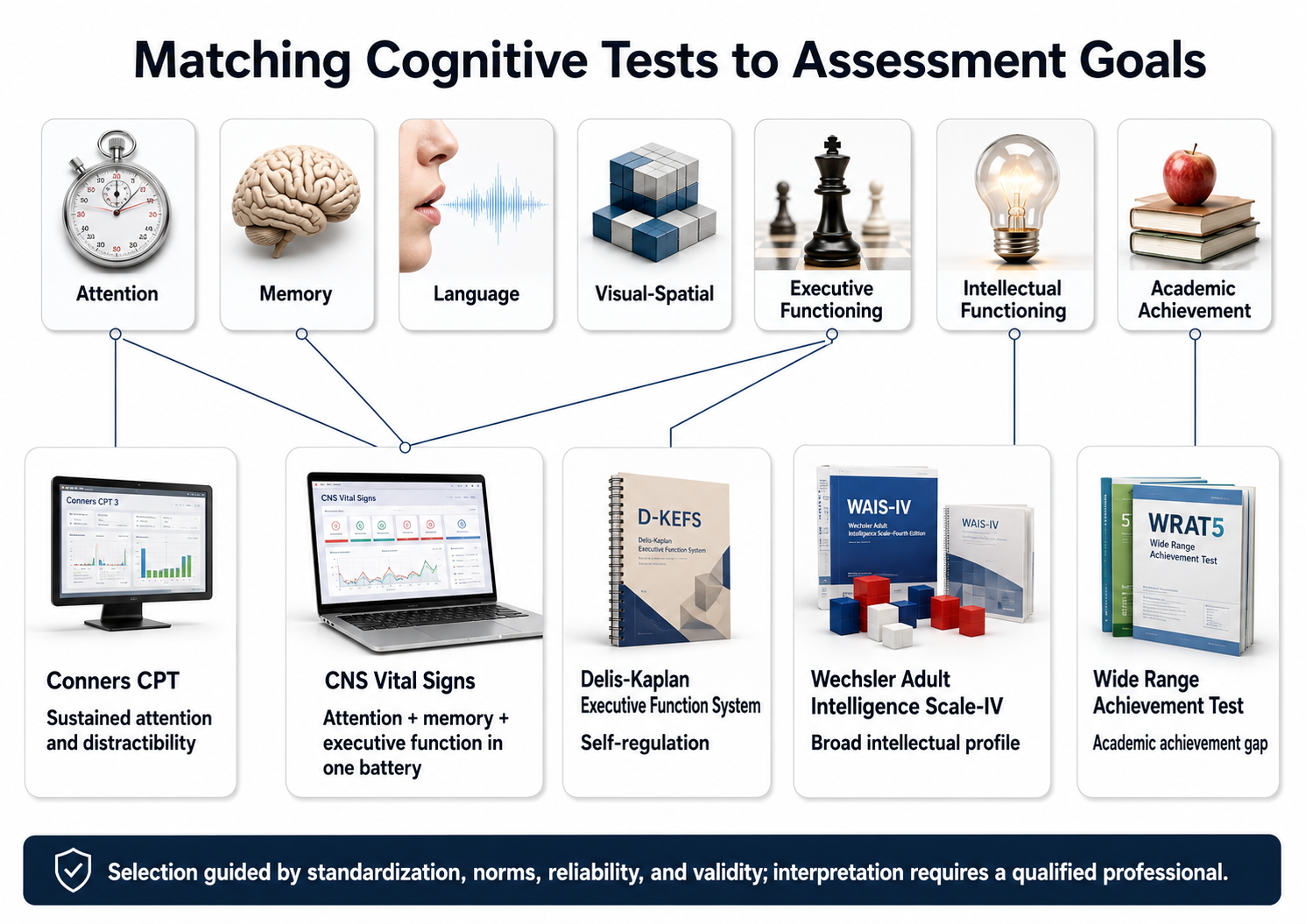
In both research and clinical settings, practitioners frequently administer tests of thinking and cognition to establish a more precise profile of the client's strengths and weaknesses (Lezak et al., 2012). Depending on the neurofeedback goals for a particular client, domains assessed may include attention, memory, language, visual-spatial perception and construction, and executive functioning. Intellectual functioning, academic performance, sensorimotor ability, and effort or performance validity may also be evaluated.
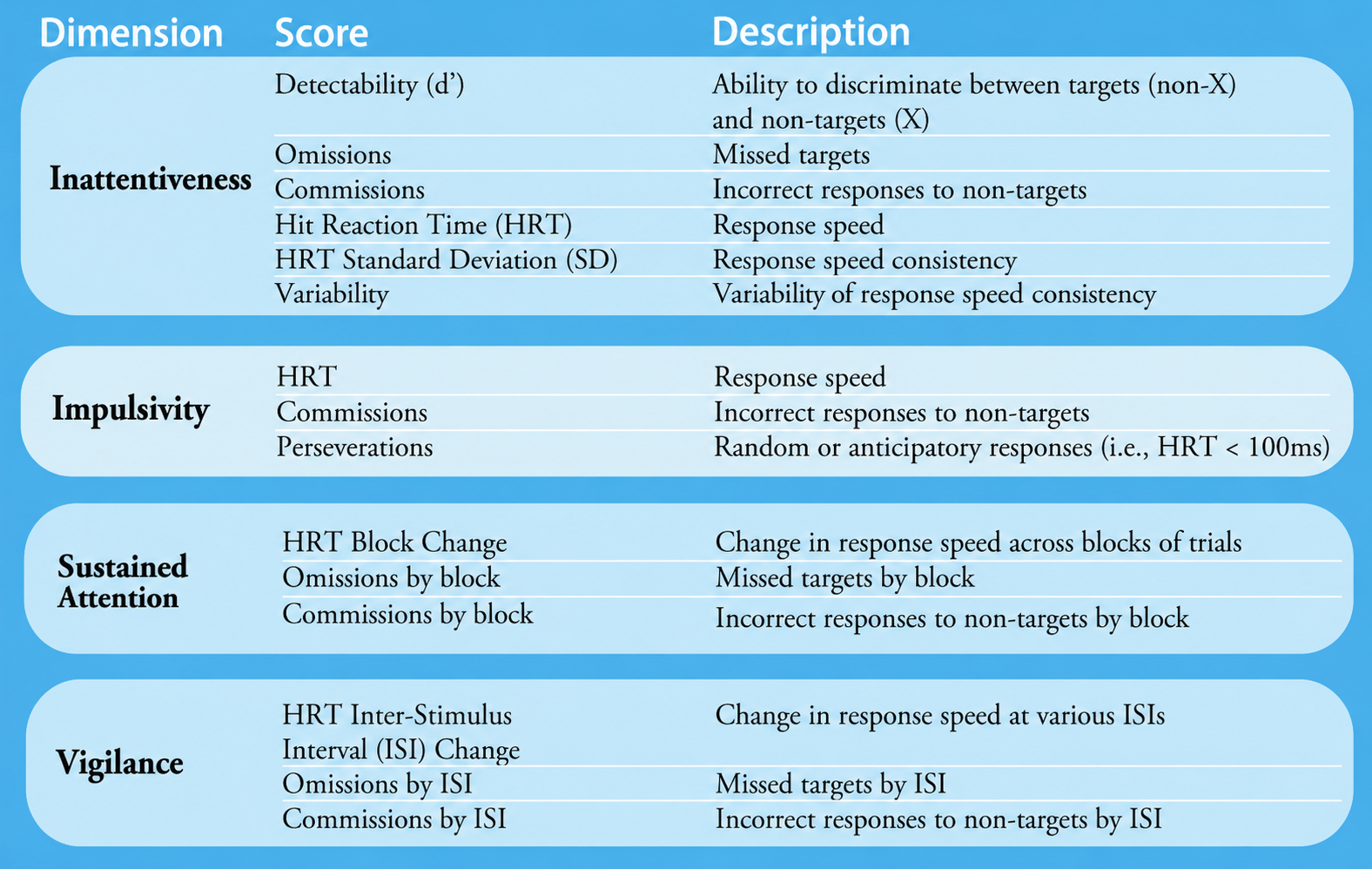
Consider a client whose primary reason for seeking neurofeedback is difficulty sustaining attention. A continuous performance test such as the Conners Continuous Performance Test (Conners, 2014) yields standardized, norm-referenced indices of attentional performance that complement the client's self-report, including omission and commission errors, response speed, and response-speed variability. They are an adjunct within a comprehensive evaluation rather than a stand-alone basis for diagnostic conclusions about attention.
Alternatively, if improved academic performance is the goal, an educational screening instrument such as the Wide Range Achievement Test (Wilkinson & Robertson, 2017) helps quantify the gap between current and expected achievement levels.
Other instruments target different facets of cognitive functioning. A measure of intelligence such as the Wechsler Adult Intelligence Scale-IV (Wechsler, 2008) provides a broad cognitive profile, while the Delis-Kaplan Executive Function System (Delis et al., 2001) zeroes in on executive functioning, the cognitive processes that regulate goal-directed behavior. Comprehensive cognitive test batteries like CNS Vital Signs (Gualtieri & Johnson, 2006) assess representative domains, including attention, memory, and executive function, within a single administration, offering an efficient overview of the client's cognitive landscape.
Regardless of which test is chosen, selection should be guided by the instrument's standardization methods, normative groups, reliability, and validity. Many tests are restricted to professionally qualified health practitioners, while others have fewer purchasing requirements. Traditional paper-and-pencil or object-manipulation tests typically require a trained examiner, whereas computer-administered tests reduce clinician time for both administration and scoring. In either case, a practitioner with appropriate professional background should interpret results to ensure they have validity and genuine value for the client.
Psychophysiological Assessment
Some practitioners integrate neurofeedback with other treatment modalities, which may include counseling or psychotherapy, medication management, audiovisual entrainment, brain stimulation, or peripheral biofeedback. When peripheral biofeedback is part of the treatment plan, psychophysiological assessment identifies which physical system to target, such as muscle tension, skin conductance, or respiration, and provides a baseline for judging the effectiveness of training (Khazan, 2013; Peper et al., 2008). This connection between intake assessment and biofeedback underscores a key point: the quantitative data collected during intake, whether from rating scales, cognitive tests, or physiological measures, all serve as reference points against which training outcomes will be evaluated.
Questionnaires and rating scales gather qualitative and quantitative information about symptoms and their functional consequences. Cognitive tests assess specific domains like attention, memory, and executive functioning to create a precise baseline profile. Psychophysiological assessment identifies peripheral systems to target when biofeedback is part of the treatment plan. Together, all quantitative data from intake serve as the reference points against which training progress is measured.
EEG Assessment for Neurofeedback
This section covers how EEG data are collected and analyzed during intake, ranging from straightforward single-site recordings to complex 19-channel assessments with source localization. You will see how quantitative EEG measures such as amplitude, power, z-scores, ratios, coherence, and phase contribute to the clinical picture and connect with the intake data discussed earlier.
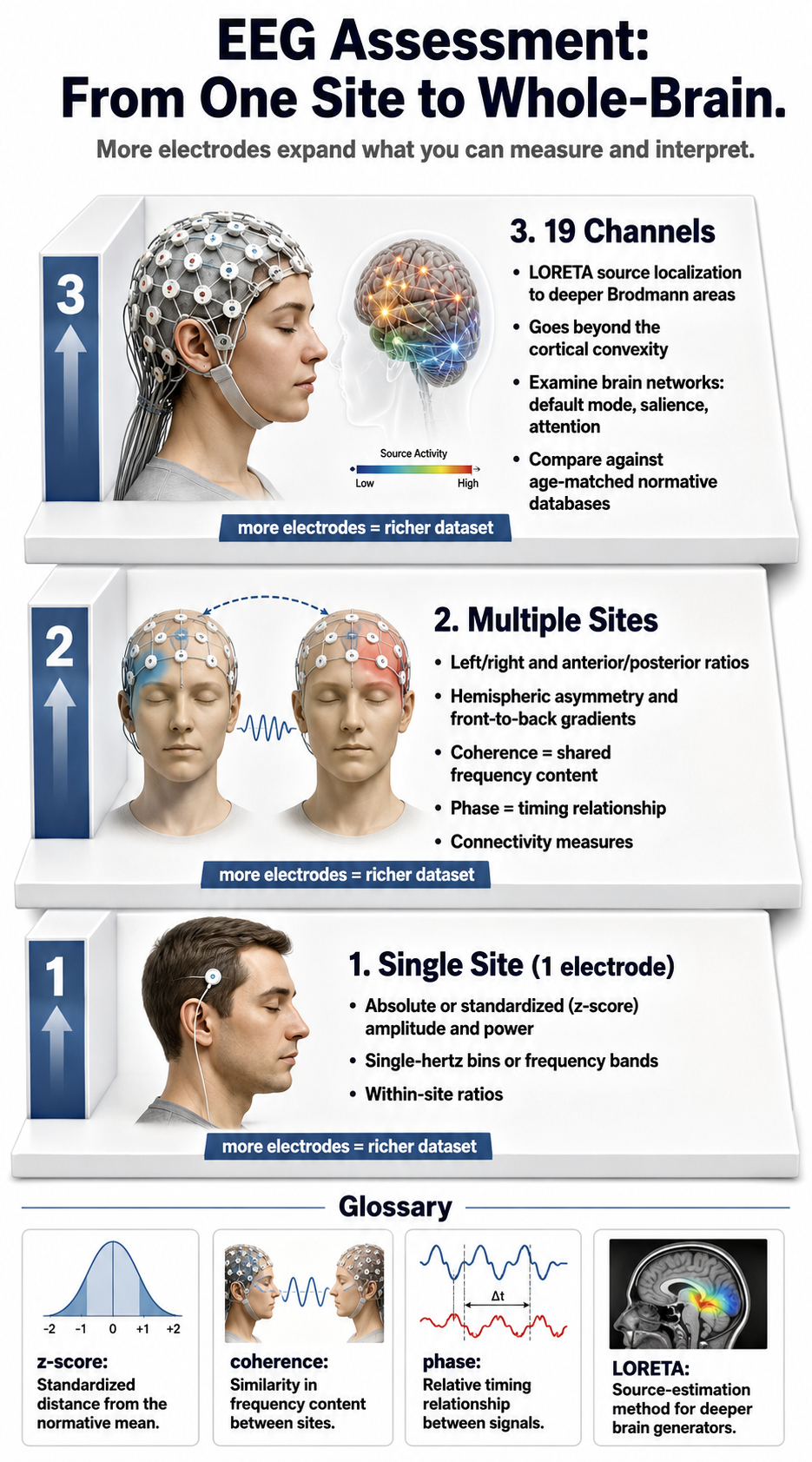
The complexity of initial EEG assessment depends on the presenting problem, the client's goals, and the practitioner's training. In typical neurofeedback practices, the number of electrode sites used ranges from 1 to 19, and more sites yield a richer dataset. Beyond visually examining the analog EEG waveform for artifacts and notable patterns, the practitioner can evaluate several variables quantitatively. Data from single sites may be expressed as absolute or standardized values (i.e., z-scores, measures of how far a value falls from the population mean in standard deviation units) of amplitude or power, calculated in single-hertz bins or across broader frequency bands. Power values may also be expressed as ratios that compare one frequency band to another, helping to characterize the relative dominance of different rhythms at a given site.
Dr. Ronald Swatzyna has generously permitted the authors to share the Houston Neuroscience Brain Center's client orientation video.
When more than one electrode is used, additional analytic possibilities emerge. Different ratios can be calculated by comparing left and right prefrontal sites or anterior and posterior sites, revealing patterns of hemispheric asymmetry or front-to-back gradients. Sites can also be compared using coherence (the consistency of the phase and amplitude relationship between two signals at a given frequency, computed as the normalized cross-spectrum and scaled from 0 to 1) and phase (the position of an oscillation within its cycle; in connectivity analysis, the quantity of interest is the phase difference between two sites at a given frequency). These inter-site measures add a connectivity dimension to the assessment that single-site data alone cannot provide.
When 19-channel recordings are obtained, the practitioner can perform LORETA (low resolution electromagnetic tomography) analyses, a mathematical technique developed by Pascual-Marqui et al. (1994) that estimates the cortical sources of scalp-recorded EEG activity. Unlike surface measures confined to the cortical convexity (the outer curve of the cerebrum immediately beneath the skull), LORETA estimates the distribution of source activity within the modeled brain volume, including deeper Brodmann areas, the cytoarchitectural zones of the cerebral cortex originally defined by histological staining, of which 43 are delineated in the human brain. Because the EEG inverse problem has no unique solution, these are blurred, low-resolution estimates rather than direct measurements of activity at a given site. This capability lets the practitioner examine functioning within specific brain networks, such as the default mode, salience, and attention networks. Normative databases are used alongside these analyses to compare the client's EEG patterns to a healthy age-matched reference group.
Both qualitative and quantitative EEG findings are interpreted to generate hypotheses that are then integrated with information from the other components of the intake assessment. Quantitative approaches to EEG assessment span a range of methodologies described by Collura (2014), Demos (2019), Kaiser (2008), Soutar and Longo (2011), Swingle (2015), Thatcher (2016), Thompson and Thompson (2015), and Van Deusen (Ribas et al., 2016).
EEG assessment ranges from simple single-site evaluations to complex 19-channel recordings with LORETA source localization. Quantitative measures include amplitude, power, z-scores, frequency-band ratios, coherence, and phase comparisons. These findings generate clinical hypotheses that are integrated with other intake information to guide treatment planning.
Integration of Intake and EEG Assessments
This section describes how all the threads of the intake process come together: the practitioner synthesizes assessment data with EEG findings to create a formulation, shares it with the client, and guides the client through informed consent. This integrative step is where data becomes clinical understanding and where the therapeutic relationship established earlier pays dividends.
The intake assessment concludes with the practitioner summarizing the critical information gathered from the various assessment methods and validating that summary with the client, asking whether anything needs to be corrected or added. The practitioner then integrates this information with EEG findings and with their own scientific and clinical knowledge. The result is a formulation: a coherent explanation of the problem that the client can consider, respond to, and ask questions about.
Building on this shared understanding, the provider presents how neurofeedback training protocols may address the identified concerns, along with the strength of the scientific evidence supporting those protocols. Practical details help the client know what to expect: a description of the neurofeedback equipment, what the provider will do during sessions, what the client will do, and what the training experience typically feels like. Possible side effects and the plan for managing them should be reviewed, as should the likely duration and cost of training, how and when progress will be monitored, and the expected durability of successful outcomes.
Alternatives to neurofeedback should also be discussed, including the option of no intervention or behavioral and lifestyle changes alone. In some cases, the intake data may suggest that neurofeedback is unlikely to be beneficial at present, and the provider has a responsibility to share that clinical judgment. The characterization of the presenting problem, the scientific evidence, the provider's expertise, and the client's own preferences and available resources all feed into this comprehensive discussion, which enables the client to give truly well-informed consent for neurofeedback. The provider may then conclude the assessment by determining whether a written report should be sent to a referring professional, obtaining consent to do so, scheduling a follow-up appointment, and summarizing any interim tasks (e.g., the client self-monitoring symptoms between sessions).
Summary
The practitioner uses a variety of methods during the intake assessment and organizes the resulting information into a coherent summary that describes and explains the client's problems and goals while guiding subsequent steps, including neurofeedback training. Data collected through interviews, questionnaires, rating scales, cognitive tests, psychophysiological measures, and EEG assessment all converge to help the client make a confident and well-informed decision about whether to proceed.
Integration involves synthesizing all assessment data, combining it with EEG findings and clinical knowledge to formulate a coherent understanding of the problem, and sharing this formulation with the client. The provider discusses training protocols, supporting evidence, costs, alternatives, and expected outcomes so the client can give well-informed consent for neurofeedback.
Telehealth and Remote Intake Assessment
The rapid expansion of telehealth has transformed how practitioners conduct intake assessments. Secure videoconferencing platforms now allow providers to complete interviews, administer questionnaires, and review consent forms remotely. Research suggests that remote intake can be as effective as in-person assessment for many client populations, while improving access for individuals in rural or underserved areas. Practitioners should ensure that their telehealth platforms comply with privacy regulations and that clients have adequate technology and a private environment for the session.
Digital Phenotyping and Passive Data Collection
Emerging research explores the use of smartphone-based passive data collection, sometimes called digital phenotyping, to supplement traditional intake methods. Patterns in sleep, physical activity, social interaction, and device usage may provide objective behavioral data that complements self-report measures. While still in early stages, these approaches hold promise for creating richer baseline profiles and tracking real-world functioning over time.
Check Your Understanding
- What are the general purposes of intake assessment, and why is building a trusting relationship essential?
- How do multimethod, evidence-based, and culturally competent assessment principles guide the intake process?
- What types of quantitative and qualitative information do questionnaires, rating scales, and cognitive tests provide?
- Describe how EEG assessment findings are integrated with intake information to create a treatment formulation.
- What information should a provider share with a client to support well-informed consent for neurofeedback?
Assignment
Now that you have completed this unit, summarize the potential benefits of collateral interviews. What can psychophysiological assessment contribute to client evaluation?
Glossary
Brodmann areas: cytoarchitectural zones of the cerebral cortex mapped by Brodmann on the basis of Nissl staining; the numbering runs from 1 to 52, but only 43 are delineated in the human brain (areas 12–16 and 48–51 were defined in non-human species).
coherence: the consistency of the phase and amplitude relationship between two EEG signals at a given frequency, computed as the normalized cross-spectrum and scaled from 0 to 1.
collateral information: reports from family members, friends, and healthcare professionals.
cortical convexity: the curve of the cerebrum immediately beneath the skull.
cultural malpractice: assessment and treatment decisions biased by cultural insensitivity and ethnocentrism.
culturally competent assessment: assessment that is informed by and sensitive to the meaning of actions, beliefs, and feelings within a client's culture.
evidence-based assessment: client evaluation using instruments that are reliable, valid, and possess clinical utility.
low resolution electromagnetic tomography (LORETA): Pascual-Marqui et al.'s (1994) mathematical inverse solution used to estimate the cortical sources of 19-electrode quantitative data acquired from the scalp.
mental status examination: a structured format for briefly assessing mental functioning, covering speech, emotion and affect, thought content and form, perceptual disturbances, cognition, reasoning, insight, and judgment.
multimethod assessment: evaluation using multiple assessment tools.
overpathologizing: labeling culturally normal behavior as abnormal.
phase: the position of an oscillation within its cycle, expressed in degrees or radians; in connectivity analysis, the quantity of interest is the phase difference between two sites at a given frequency.
psychophysiological assessment: evaluation of peripheral physiological systems, such as muscle tension, skin conductance, and respiration, to identify training targets and establish a baseline for judging the effectiveness of biofeedback.
z-score: a standardized value expressing how far a measurement falls from the reference-group mean in standard deviation units.
z-score training: neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Baer, L., & Blais, M. A. (Eds.). (2010). Handbook of clinical rating scales and assessment in psychiatry and mental health. Humana Press.
Collura, T. F. (2014). Technical foundations of neurofeedback. Routledge.
Conners, C. K. (2014). Conners Continuous Performance Test (3rd ed.). Multi-Health Systems.
Dana, R. H. (2005). Multicultural assessment: Principles, applications, and examples. Erlbaum.
Delis, D. C., Kaplan, E., & Kramer, J. H. (2001). Delis-Kaplan Executive Function System. The Psychological Corporation.
Demos, J. N. (2019). Getting started with EEG neurofeedback (2nd ed.). W. W. Norton & Company.
Gualtieri, C. T., & Johnson, L. G. (2006). Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology, 21(7), 623–643. https://doi.org/10.1016/j.acn.2006.05.007
Kaiser, D. A. (2008). Functional connectivity and aging: Comodulation and coherence differences. Journal of Neurotherapy, 12(2–3), 123–139. https://doi.org/10.1080/10874200802398790
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. Wiley-Blackwell.
Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel, D. (2012). Neuropsychological assessment (5th ed.). Oxford University Press.
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49–65. https://doi.org/10.1016/0167-8760(84)90014-X
Peper, E., Tylova, H., Gibney, K. H., Harvey, R., & Combatalade, D. (2008). Biofeedback mastery: An experiential teaching and self-training manual. Association for Applied Psychophysiology and Biofeedback.
Pomerantz, A. M. (2020). Clinical psychology: Science, practice, and diversity (5th ed.). Sage Publications.
Psychology Tools. (n.d.). Psychological assessment tools for mental health. Retrieved March 9, 2021, from https://www.psychologytools.com/download-scales-and-measures/
Ribas, V. R., Ribas, R. de M. G., & Martins, H. A. de L. (2016). The learning curve in neurofeedback of Peter Van Deusen: A review article. Dementia & Neuropsychologia, 10(2), 98–103. https://doi.org/10.1590/S1980-5764-2016DN1002005
Sadock, B. J., Sadock, V. A., & Ruiz, P. (2017). Kaplan and Sadock's concise textbook of clinical psychiatry (4th ed.). Wolters Kluwer.
Schwartz, M. S. (2016). Intake and preparation for intervention. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: A practitioner's guide (4th ed., pp. 217–232). Guilford Press.
Silverman, J., Kurtz, S., & Draper, J. (2013). Skills for communicating with patients (3rd ed.). CRC Press.
Soutar, R., & Longo, R. (2011). Doing neurofeedback: An introduction. ISNR Research Foundation.
Stucky, K. J., & Bush, S. S. (2017). The neuropsychology fact-finding casebook: A training resource. Oxford University Press.
Swingle, P. G. (2015). Adding neurotherapy to your practice: Clinician's guide to the ClinicalQ, neurofeedback, and braindriving. Springer.
Thatcher, R. W. (2016). Handbook of quantitative electroencephalography and EEG biofeedback (2nd ed.). ANI Publishing.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Wechsler, D. (2008). Wechsler Adult Intelligence Scale (4th ed.). Pearson.
Wilkinson, G. S., & Robertson, G. J. (2017). Wide Range Achievement Test (5th ed.). Pearson.
Return to Top