Assessment Demonstration
What You Will Learn in This Chapter
This unit provides hands-on demonstrations of EEG assessment, from streamlined abbreviated Q recordings to comprehensive 19-channel evaluations. You will observe how clinicians collect, process, and interpret EEG data using a variety of tools and systems. Whether you work in a VA medical center, a hospital neurology department, or a private clinic, these skills form the foundation of effective neurofeedback practice.
Whether you are beginning your neurofeedback training or refining your assessment expertise, these demonstrations will guide you through the step-by-step process of transforming raw EEG recordings into clinically actionable information. By the end, you will understand how different assessment approaches serve different clinical needs.
BCIA Blueprint Coverage: This unit addresses VI. Patient/Client Assessment - D. Assessment Demonstration: Perform a basic EEG assessment, an abbreviated Q recording and/or attaching electrode cap and completing an abbreviated Q or 19-channel QEEG recording.
Learning Objectives
After completing this section, you will be able to:
Describe the purpose and procedure of an abbreviated Q recording.
Explain the difference between clinical databases and normative databases for EEG assessment.
Identify the key steps in conducting a 19-channel EEG recording with normative database comparison.
Describe the process of visual inspection, artifact rejection, and data extraction from EEG recordings.
Overview
This section covers the practical side of EEG assessment, building on the foundational concepts introduced in earlier units of Neurofeedback Tutor. You will encounter two broad approaches: abbreviated Q recordings that sample a subset of scalp sites, and full 19-channel evaluations that provide a comprehensive picture of brain electrical activity. Understanding when to use each approach, and what each can and cannot tell you, is a core clinical skill.
Dr. Ronald Swatzyna has generously permitted the authors to share the Houston Neuroscience Brain Center's client qEEG cap orientation video.
As discussed in previous units, every EEG assessment begins with a visual inspection of the raw recording. Clinicians use various montages, specific groupings of electrode comparisons (Thomas, 2007), to identify the EEG's basic characteristics and flag any abnormal patterns that may warrant a neurological referral. Once visual inspection is complete, the clinician may pursue a quantitative analysis, and this section demonstrates several examples of that process. This progression from visual inspection to quantitative analysis mirrors the way experienced clinicians think: first look at the data with your own eyes, then let the numbers refine your interpretation.
Neurofeedback Tutor describes and demonstrates an example of a 2-channel assessment that uses a series of three pairs of 10-20 system sites, with specific tasks assigned to each pair. This should not be confused with an EEG assessment that uses two channels at only two sites, which would have limited clinical usefulness; any particular complaint may be associated with deviations at different locations depending on the individual. Since Neurofeedback Tutor is equipment, software, and database agnostic, this unit illustrates its concepts with products from several manufacturers.

EEG assessment follows a logical progression: visual inspection first, then quantitative analysis. This unit demonstrates both abbreviated Q recordings, which sample selected scalp sites, and full 19-channel assessments, which provide comprehensive coverage. You will see examples from multiple manufacturers, reflecting the equipment-agnostic approach of Neurofeedback Tutor.
Abbreviated Q Recordings
NewQ
This section introduces abbreviated Q recordings, streamlined EEG assessments that sample a subset of scalp locations rather than the full 19-channel array. These tools offer clinicians a faster, more automated path from data collection to clinical interpretation. We will examine how they work, what distinguishes their databases from normative approaches, and why they have become popular in diverse practice settings.
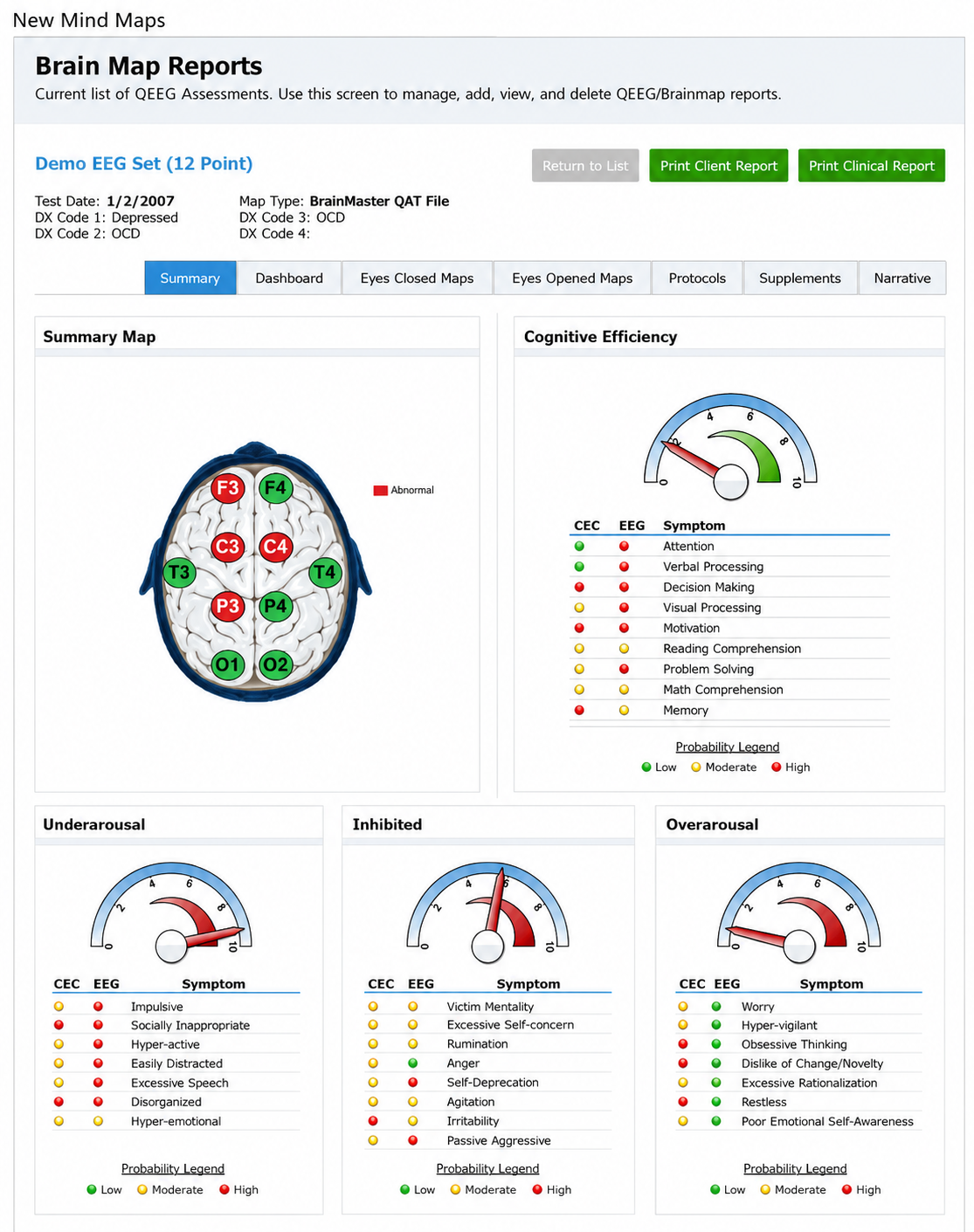
The first example is the NewQ, a six-location assessment that samples selected sites from the International 10-20 system, the standardized electrode placement grid used across clinical EEG practice. Similar tools include New Mind Maps, The Learning Curve (TLC), the Clinical Q, and others. Some are designed for specific hardware and software platforms, while others work across multiple systems. As a class, these tools offer a degree of automation in collecting, processing, and interpreting EEG information that benefits both beginners and experienced practitioners by incorporating expert decision-support systems into the assessment process.
A shared feature of these abbreviated approaches is their reliance on a clinical database, a collection of EEG metrics linked to known clinical findings rather than to the statistical norms of a healthy population (Swingle, 2014). Swingle argues that clinical databases are superior to normative databases (for a survey of database use in qEEG evaluation, see Johnstone & Gunkelman, 2003) because they connect EEG patterns directly to clinical observations, such as the typical voltage of alpha activity (8–12 Hz rhythms associated with relaxed wakefulness) in a particular region during specific tasks. Each clinical database reflects its developer's years of education, training, and clinical experience, allowing other practitioners to leverage that accumulated expertise.
Importantly, a clinical database assessment does not produce a formal diagnosis like those found in the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR). Instead, it flags possible clinically relevant findings related to the client's presenting symptoms. This distinction matters in practice: the assessment guides your clinical reasoning and protocol selection without overstepping the boundaries of what the EEG data alone can establish.
The following video describes the NewQ as an example of an abbreviated Q assessment. A subsequent demonstration walks through the complete process of collecting, processing, and interpreting the data. While this video features one specific tool, the workflow is representative of the broader category. Some tools assess additional sites, some collect data simultaneously rather than sequentially, and some use individual sensors while others employ an EEG "cap," an elastic fabric cap that holds sensors at fixed 10-20 positions, as shown in the image below.

Video © J. S. Anderson.
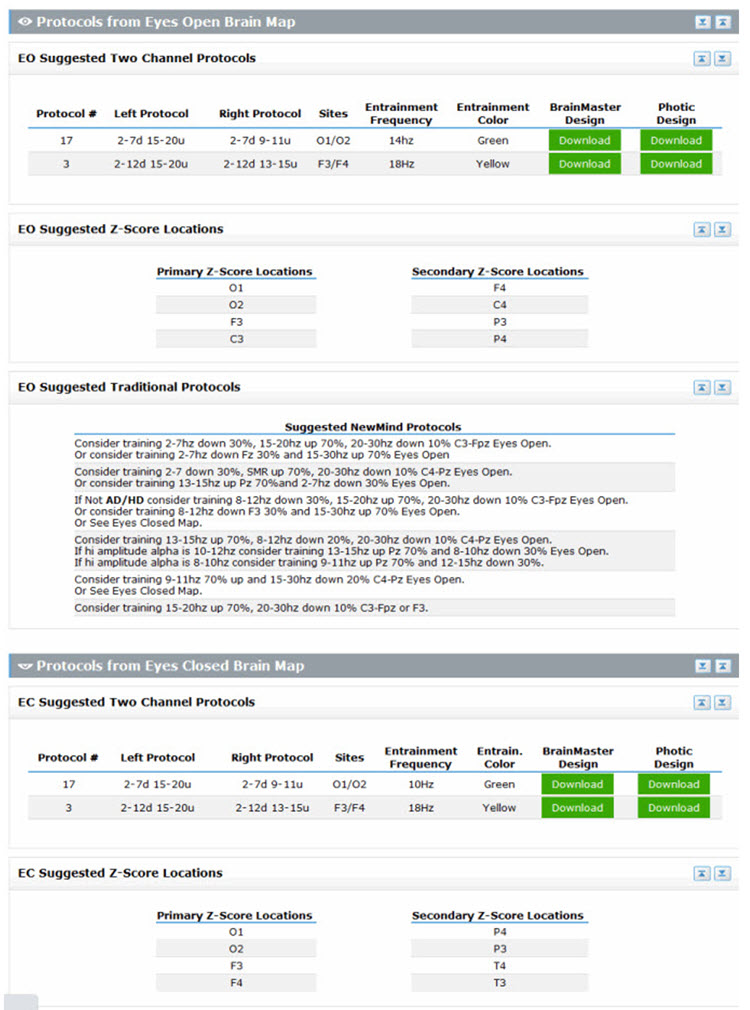
In summary, abbreviated Q assessments provide clinically useful information in a time-efficient format. They help validate and explain client symptoms, support training protocol selection, and can be readily repeated to monitor progress, making them practical tools for busy clinical settings. Two additional report examples appear below.
Clinical Q Assessment Report
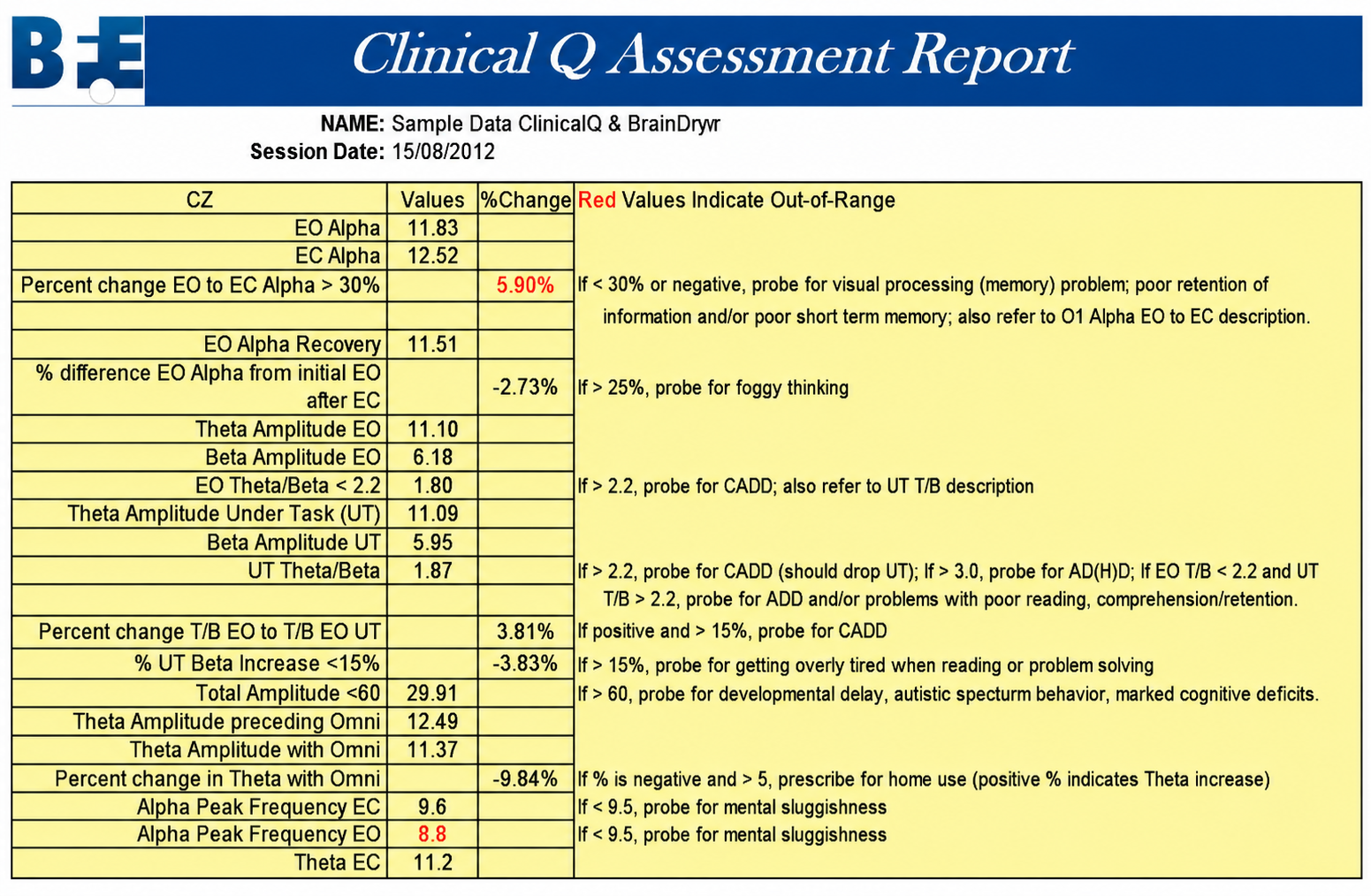
Abbreviated Q recordings like the NewQ use a subset of 10-20 scalp locations to produce clinically useful analyses in less time than a full 19-channel assessment. Their reliance on clinical databases, which link EEG patterns to observed clinical findings rather than population norms, allows clinicians to identify relevant patterns and select appropriate training protocols. These tools do not produce formal diagnoses but instead guide clinical reasoning and support treatment planning.
19-Channel Recordings
This section explores the full 19-channel EEG recording with normative database comparison, the most comprehensive of the assessment approaches covered in this unit. Where abbreviated Q recordings offer speed and clinical specificity, 19-channel assessments provide a detailed, whole-brain picture of electrical activity. We will walk through the recording process, the critical steps of artifact rejection and visual inspection, and how the resulting data are compared to normative values to guide treatment planning.
The primary alternative to abbreviated Q assessments is the full 19-channel recording, which captures data from all standard International 10-20 system scalp locations simultaneously. The data are then compared to a normative database, a collection of EEG metrics from a representative sample of healthy individuals recorded under standardized resting and active-task conditions. This comparison reveals where a client's brain electrical activity falls relative to age-matched norms, expressed as z-scores (standard deviations from the database mean; Thatcher, 1998; Thatcher et al., 2019). The following video demonstrates the complete recording process. Video © J. S. Anderson.
EEG Recording, Testing, and Protocol Development
We encourage you to view the following two-hour video in stages, as it provides a comprehensive overview of the full assessment-to-treatment workflow. The recording covers 19-channel EEG data collection, protocol selection, treatment implementation, and qEEG-guided neurofeedback. This end-to-end demonstration shows how assessment findings translate directly into clinical decisions, the bridge from data to practice that defines effective neurofeedback. Video © J. S. Anderson.
Clean Data Extraction and Comparison to a Normative Database
Before quantitative analysis can begin, the raw EEG must be carefully cleaned, a process that connects directly to the artifact rejection skills covered in earlier units. Visual inspection starts with the standard 19-channel recording referenced to linked ears. The clinician then extracts segments for each recording condition (for example, eyes open and eyes closed), inspects the data using multiple montages, different electrode comparison configurations that reveal different aspects of brain activity, and selects only clean, artifact-free epochs. These artifact-free segments are the foundation of a reliable quantitative comparison to the normative database. Video © J. S. Anderson.
The rigor of this data-cleaning process directly affects the quality of your assessment results. Artifacts, false signals from sources like muscle tension, eye blinks, or electrical interference, can distort quantitative values and lead to inaccurate comparisons with the normative database. Taking time to carefully reject contaminated epochs is what separates a clinically trustworthy assessment from a misleading one.

Full 19-channel recordings with normative database comparisons offer the most comprehensive of the EEG assessment approaches covered in this unit. The process follows a structured sequence: recording from all standard scalp locations, visual inspection using multiple montages, careful artifact rejection, extraction of clean data, and statistical comparison to age-matched norms. The quality of the final assessment depends directly on the rigor of each preceding step, making meticulous data cleaning essential to accurate clinical interpretation.
Check Your Understanding
- What is the difference between a clinical database and a normative database in EEG assessment?
- Why might a 2-channel assessment using only two sites have limited clinical usefulness?
- What are the key steps involved in processing a 19-channel EEG recording for normative database comparison?
- How can abbreviated Q assessments like the NewQ assist clinicians in selecting training protocols?
- Why is visual inspection of the raw EEG an important first step before quantitative analysis?
Assignment
Now that you have completed this unit, explain why the visual inspection of raw EEG waveforms is important.
Glossary
A (auricular): International 10-20 system earlobe reference placement.
abbreviated Q recording: an EEG assessment that samples a subset of International 10-20 system scalp sites, usually against a clinical database, in place of a full 19-channel recording.
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with relaxed wakefulness. Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
amplitude: the strength of the EEG signal, measured in microvolts (μV) and seen in the peak-to-trough height of EEG waves. Amplitude is not power: picowatts are a unit of power and are never a unit of amplitude.
artifact: false signals like 50/60Hz noise produced by line current.
artifact rejection: the removal of epochs contaminated by noncerebral signals before quantitative analysis.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
bipolar (sequential) montage: a recording method in which each channel compares two active electrodes rather than an active electrode and a shared reference. In a sequential montage, channels are chained so that each shares one electrode with the next.
bridging artifact: a short circuit between adjacent electrodes due to excessive application of electrode paste or a client sweating excessively or arriving with a wet scalp.
C (central): sites in the International 10-20 system that overlie the sensorimotor strip and, through volume conduction, also detect frontal, parietal-occipital, and temporal EEG activity.
channel: one differential amplifier input, formed by comparing two electrodes (active and reference). A single ground electrode is shared across all channels rather than belonging to any one channel.
clinical database: qEEG metrics linked to clinical findings and to a developer's accumulated clinical experience, rather than to the statistical norms of a symptom-free reference sample.
delta rhythm: 1-4 Hz oscillations with at least two generators, thalamocortical neurons and the cortex itself; delta is most prominent in stage 3 sleep but is not confined to it. Some sources set the lower edge at 0.5 Hz.
drowsiness artifact: in adults, 1-Hz (or slower) waveforms can be detected with the greatest amplitude, and reverse polarity at F7 and F8 may progress to 1-2 Hz slowing of the alpha rhythm.
EEG artifacts: noncerebral electrical activity in an EEG recording can be divided into physiological and exogenous artifacts.
electro-ocular artifact: contamination of EEG recordings by potentials generated by eye blinks, eye flutter, and eye movements.
electrode pop artifact: sudden large deflections in at least one channel when an electrode abruptly detaches from the scalp.
EMG artifact: interference in EEG recording by volume-conducted signals from skeletal muscles.
epoch: a defined segment of EEG selected for visual inspection or quantitative analysis.
exogenous artifacts: noncerebral electrical activity generated by movement, 50/60 Hz and field effect, bridging, and electrode (electrode "pop" and impedance) artifacts.
F (frontal): sites in the International 10-20 system that detect frontal lobe EEG activity.
Fp (frontopolar or prefrontal): sites in the International 10-20 system that detect prefrontal cortical EEG activity.
hertz (Hz): a unit of frequency measured in cycles per second.
impedance (Z): the complex opposition to an AC signal, measured in ohms and conventionally reported in kilohms (kΩ) for EEG.
impedance meter: a device that uses an AC signal to measure impedance in an electric circuit, such as between active and reference electrodes.
impedance test: automated or manual measurement of skin-electrode impedance.
inion: a bony prominence on the back of the skull.
International 10-20 system: a standardized procedure for 21 recording and one ground electrode on adults.
low resolution electromagnetic tomography (LORETA): Pascual-Marqui's (1994) mathematical inverse solution to identify the cortical sources of quantitative data acquired from 19 or more scalp electrodes.
mastoid bone: bony prominence behind the ear.
microvolt (μV): a unit of amplitude (signal strength) that is one-millionth of a volt.
montage: a grouping of electrodes (combining derivations) to record EEG activity.
movement artifact: voltages caused by client movement or the movement of electrode wires by other individuals.
nasion: the depression at the bridge of the nose.
normative database: qEEG metrics obtained from a representative sample of participants during resting and active-task conditions.
notch filter: a filter that suppresses a narrow band of frequencies, such as those produced by line current at 50/60Hz.
O (occipital): sites in the International 10-20 system that detect occipital lobe EEG activity.
ohm (Ω): a unit of impedance or resistance.
P (parietal): sites in the International 10-20 system that detect parietal lobe EEG activity.
physiological artifacts: noncerebral electrical activity that includes electromyographic, electro-ocular (eye blink and eye movement), cardiac (pulse), sweat (skin impedance), drowsiness, and evoked potential.
posterior dominant rhythm (PDR): the highest-amplitude frequency detected at the posterior scalp when eyes are closed.
power: amplitude squared, expressed in microvolts squared (μV²). μV² is numerically equal to picowatts only under the convention of a 1-ohm reference resistance, and that convention must be stated whenever picowatts appear. Because power is amplitude squared, amplitude-based and power-based thresholds and ratios are not interchangeable.
preauricular point: the slight depression located in front of the ear and above the earlobe.
protocol: a rigorously organized plan for training.
pulse artifacts: noncerebral voltages due to mechanical movement of an electrode in relation to the skin surface due to the pressure wave of each heartbeat.
Quantitative EEG (qEEG): digitized statistical analysis of the EEG, comparing measures such as amplitude, power, coherence, and phase within specific frequency bins against a database. Topographic brain mapping typically uses 19 or more channels, but abbreviated and single-channel applications exist, such as the theta/beta ratio at Cz.
reference electrode: an electrode placed on the scalp, earlobe, or mastoid.
rhythmic midtemporal theta of drowsiness (RMTD): a benign drowsiness variant, not an epileptiform pattern. Notched rhythmic theta waveforms are localized to the midtemporal regions, some sharply contoured, and are often bitemporal with a shifting amplitude asymmetry.
sensorimotor rhythm (SMR): the 12-15 Hz spindle-shaped sensorimotor rhythm detected from the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
standardized LORETA (sLORETA): a refinement of LORETA that estimates a standardized current density at each voxel and partitions the intracerebral volume into 6,239 voxels at 5-mm spatial resolution.
surface Laplacian (SL) analysis: a family of mathematical algorithms that provide two-dimensional images of radial current flow from cortical dipoles to the scalp.
swLORETA: a more precise and accurate iteration of the LORETA source localization method.
theta/beta ratio (T/B ratio): the ratio between 4-8 Hz theta and 13-21 Hz beta, measured most typically along the midline. It was developed and normed on a single channel at the vertex (Cz).
theta rhythm: 4-8-Hz rhythms generated by a cholinergic septohippocampal system that receives input from the ascending reticular formation and a noncholinergic system that originates in the entorhinal cortex, which corresponds to Brodmann areas 28 and 34 at the caudal region of the temporal lobe.
tragus: the flap at the opening of the ear.
transient: isolated waveforms or complexes that can be distinguished from background activity.
vertex (Cz): the intersection of imaginary lines drawn from the nasion to inion and between the two preauricular points in the International 10-10 and 10-20 systems.
z-score: the number of standard deviations by which a client's value differs from the mean of a normative database.
z-score training: a neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Fein, G., Galin, D., Johnstone, J., Yingling, C. D., Marcus, M., & Kiersch, M. E. (1983). EEG power spectra in normal and dyslexic children. I. Reliability during passive conditions. Electroencephalography and Clinical Neurophysiology, 55(4), 399-405. https://doi.org/10.1016/0013-4694(83)90127-x
Hardt, J. V., & Kamiya, J. (1978). Anxiety change through electroencephalographic alpha feedback seen only in high anxiety subjects. Science, 201(4350), 79-81. https://doi.org/10.1126/science.663641
John, E. R., Ahn, H., Prichep, L., Trepetin, M., Brown, D., & Kaye, H. (1980). Developmental equations for the electroencephalogram. Science, 210(4475), 1255-1258. https://doi.org/10.1126/science.7434026
Johnstone, J., & Gunkelman, J. (2003). Use of databases in QEEG evaluation. Journal of Neurotherapy, 7(3-4), 31-52. https://doi.org/10.1300/J184v07n03_02
Kamiya, J. (1968). Conscious control of brain waves. Psychology Today, 1, 56-60.
Nuwer, M. R., & Coutin-Churchman, P. (2014). Brain mapping and quantitative electroencephalogram. In Encyclopedia of the Neurological Sciences (2nd ed.). Elsevier.
Rogala, J., Jurewicz, K., Paluch, K., Kublik, E., Cetnarski, R., & Wróbel, A. (2016). The do's and don'ts of neurofeedback training: A review of the controlled studies using healthy adults. Frontiers in Human Neuroscience, 10, 301. https://doi.org/10.3389/fnhum.2016.00301
Soutar, R., & Longo, R. (2022). Doing neurofeedback: An introduction (2nd ed.). Foundation for Neurofeedback and Neuromodulation Research.
Swingle, P. G. (2014, Spring). Clinical versus normative databases: Case studies of Clinical Q assessments. NeuroConnections.
Thatcher, R. W. (1998). Normative EEG databases and EEG biofeedback. Journal of Neurotherapy, 2(4), 8-39. https://doi.org/10.1300/J184v02n04_02
Thatcher, R. W., Lubar, J. F., & Koberda, J. L. (2019). Z-Score EEG biofeedback: Past, present, and future. Biofeedback, 47(4), 89-103. https://doi.org/10.5298/1081-5937-47.4.04
Thomas, C. (2007). What is a montage? In EEG instrumentation. American Society of Electroneurodiagnostic Technologists, Inc.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Return to Top