Signal Acquisition
What You Will Learn
This unit covers how clinicians record and interpret EEG activity using standardized electrode placement systems. You will learn the International 10-20 and expanded 10-10 systems, how montage selection shapes what you see in the EEG, and how software-based reformatting allows you to reanalyze session data by referencing electrodes to different sites or combinations of sites. These tools also enable computation of variables related to communication and network function within the central nervous system (CNS).
The quantitative EEG (qEEG) applies digital signal processing to the EEG to derive measures such as absolute and relative amplitude or power within selected frequency bands, together with connectivity measures like coherence and phase. A full-cap 21-channel recording (19 scalp sensors plus two ear sensors) and the resulting qEEG analysis can be especially valuable for designing treatment protocols in complex cases like Autism Spectrum Disorders or traumatic brain injury. EEG topography then displays these data on a scalp surface map, from which the spatial distribution of the underlying brain activity is inferred.
You will also learn to identify and manage artifacts, the noncerebral signals that contaminate EEG recordings. Both physiological artifacts (like muscle activity and eye blinks) and exogenous artifacts (like 60-Hz line noise) require careful precautions, visual inspection of the raw EEG, and systematic removal of contaminated epochs through a process called artifacting. Impedance tests and behavioral checks are essential safeguards for recording fidelity.
Finally, you will explore how to interpret EEG recordings in context, recognizing the effects of eye closure, age, time of day, alertness and drowsiness, medication, and relaxation on the signals you observe.
Graphic © Medical-R/Shutterstock.com.
BCIA Blueprint Coverage
This unit addresses III. Instrumentation and Electronics - B. Signal Acquisition.

The sections that follow cover the International 10-20 and 10-10 Systems, a Comparison of Neuroimaging Techniques, Using a Limited Number of Electrodes, Montage Options and Their Consequences, Recognizing and Correcting Signals of Noncerebral Origin, and Recognizing Normal EEG Patterns.
Listen to Lecture: Signal Acquisition (Part 1)
International 10-20 and 10-10 Systems
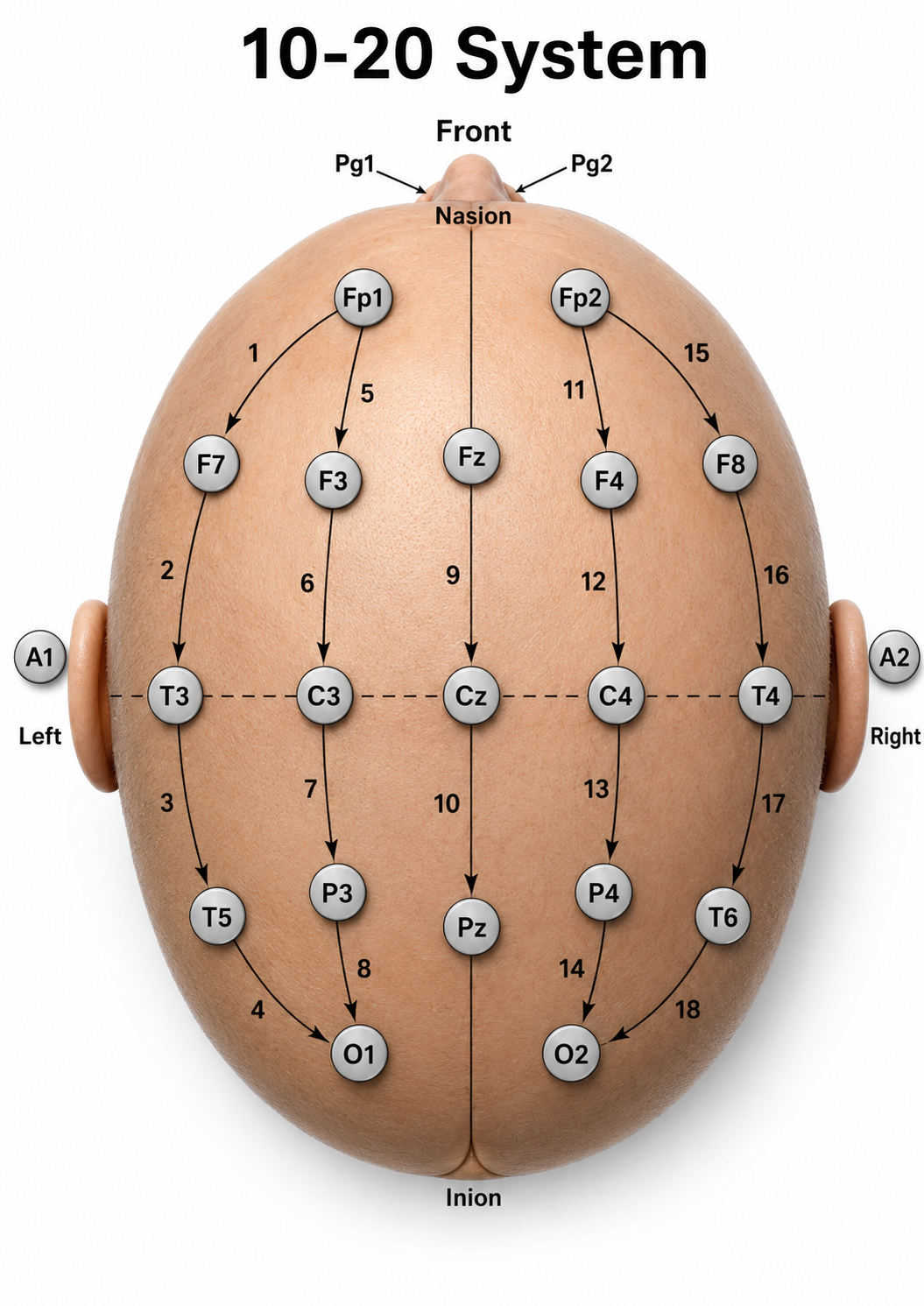
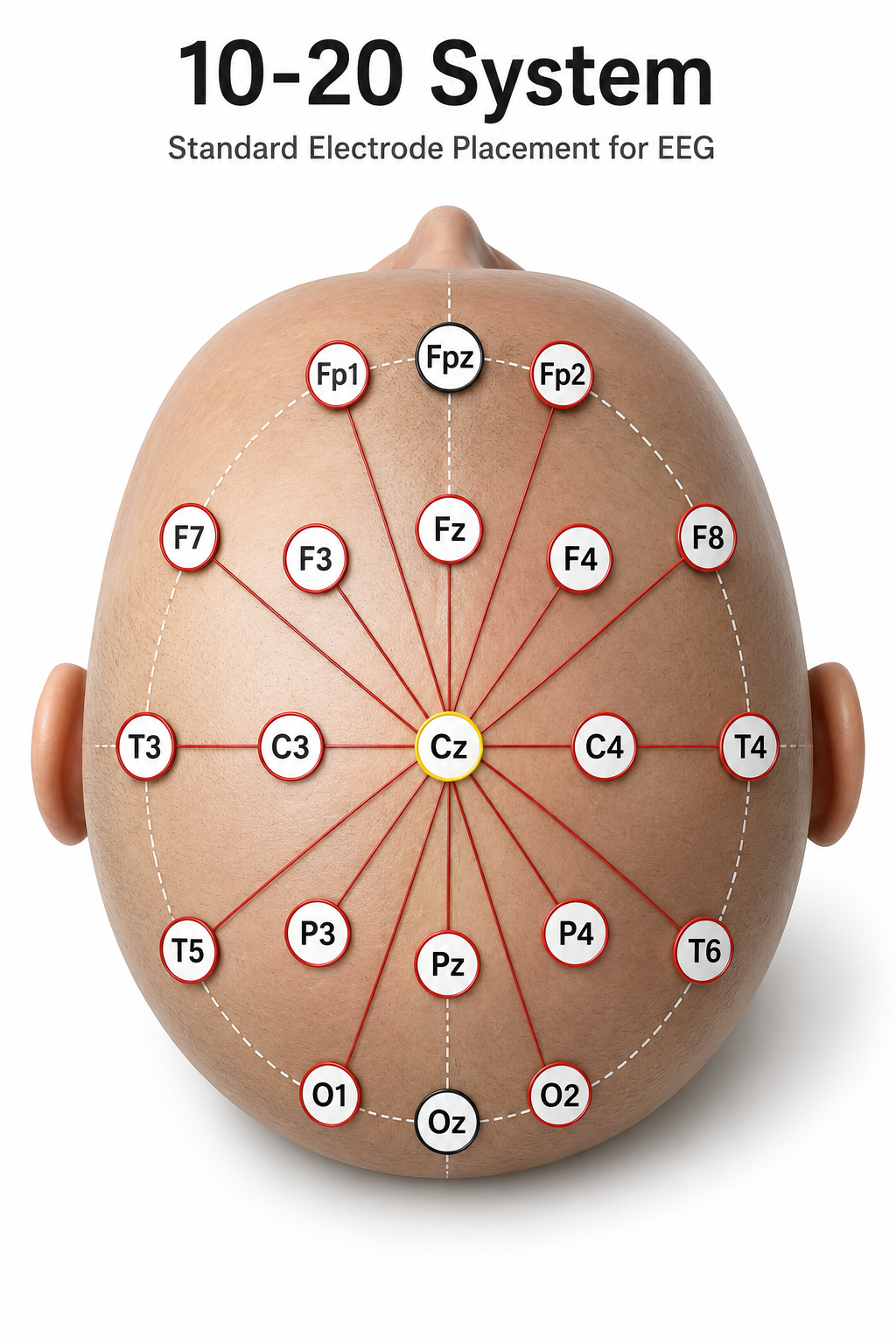
This section introduces the two standardized electrode placement systems you will use in clinical practice: the International 10-20 system and its expanded 10-10 counterpart. The International 10-20 system is a standardized procedure for positioning electrodes on 19 scalp sites plus reference and ground locations. Although the electrode itself contacts only a small patch of scalp—often compared to the size of a coin—the potential it records is not confined to that patch. Because the skull and scalp spread (volume-conduct) the underlying currents, each scalp electrode sums synchronous activity from several square centimeters of cortex, and the recorded maximum may not sit directly over the EEG generator (Nunez & Srinivasan, 2006).
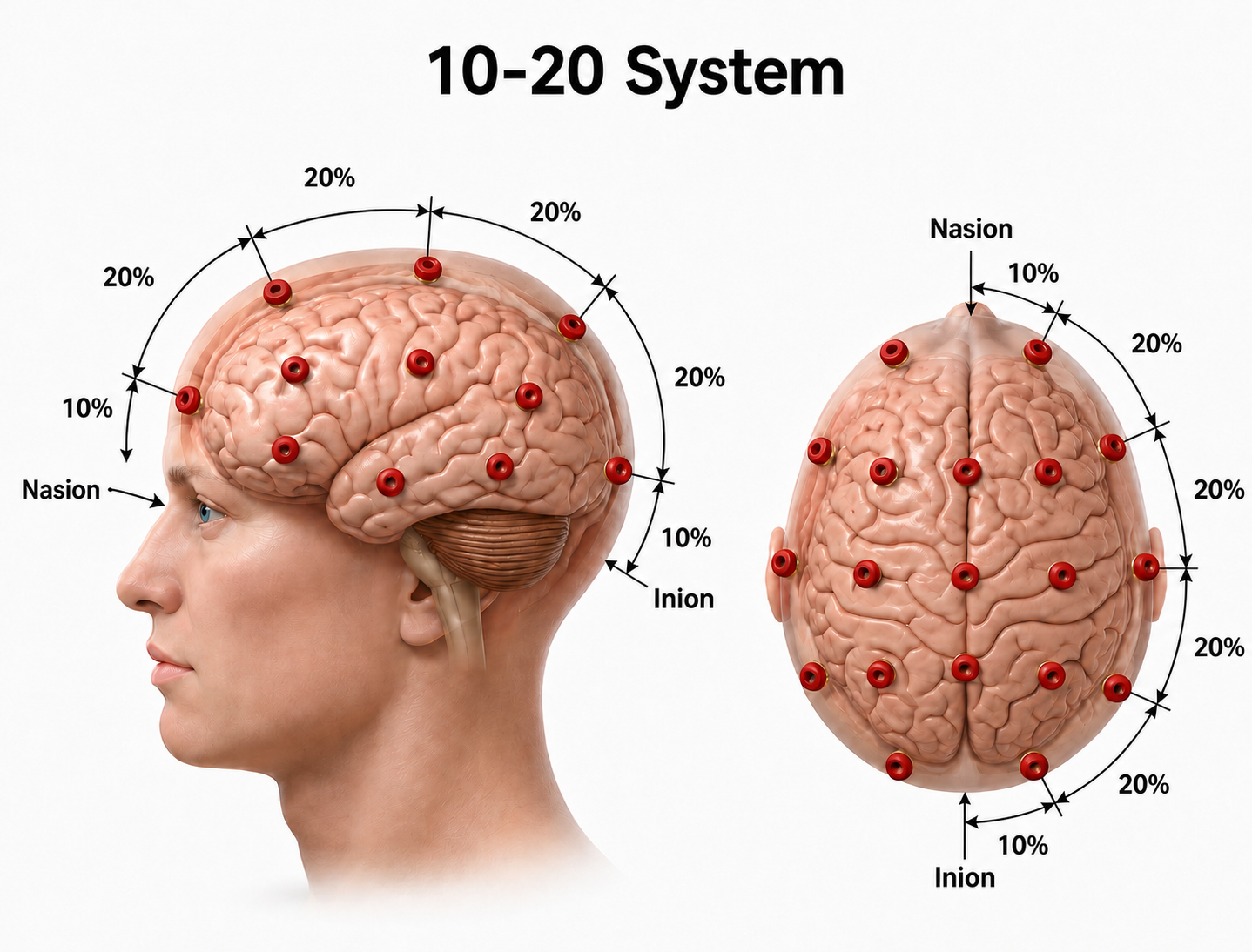
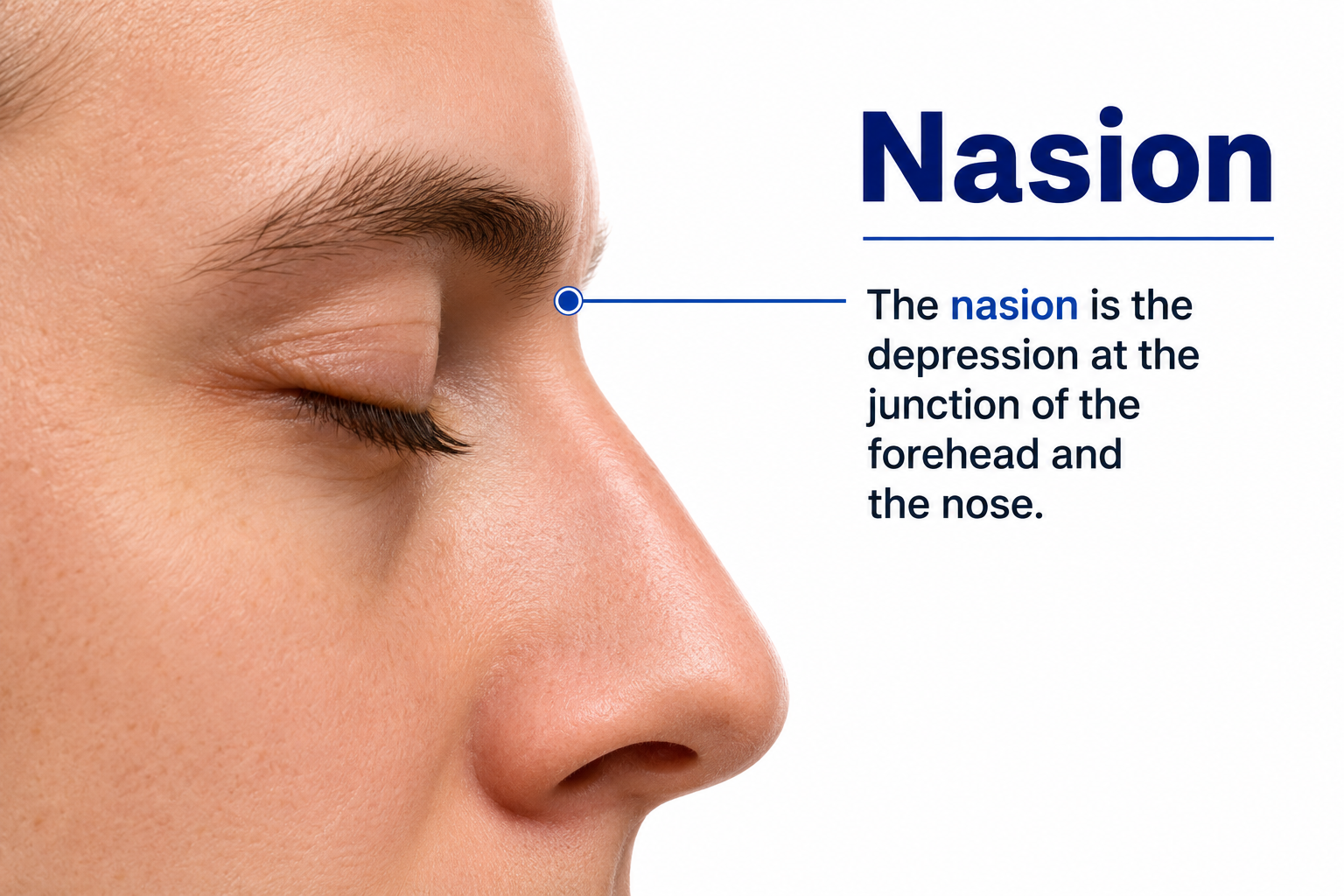
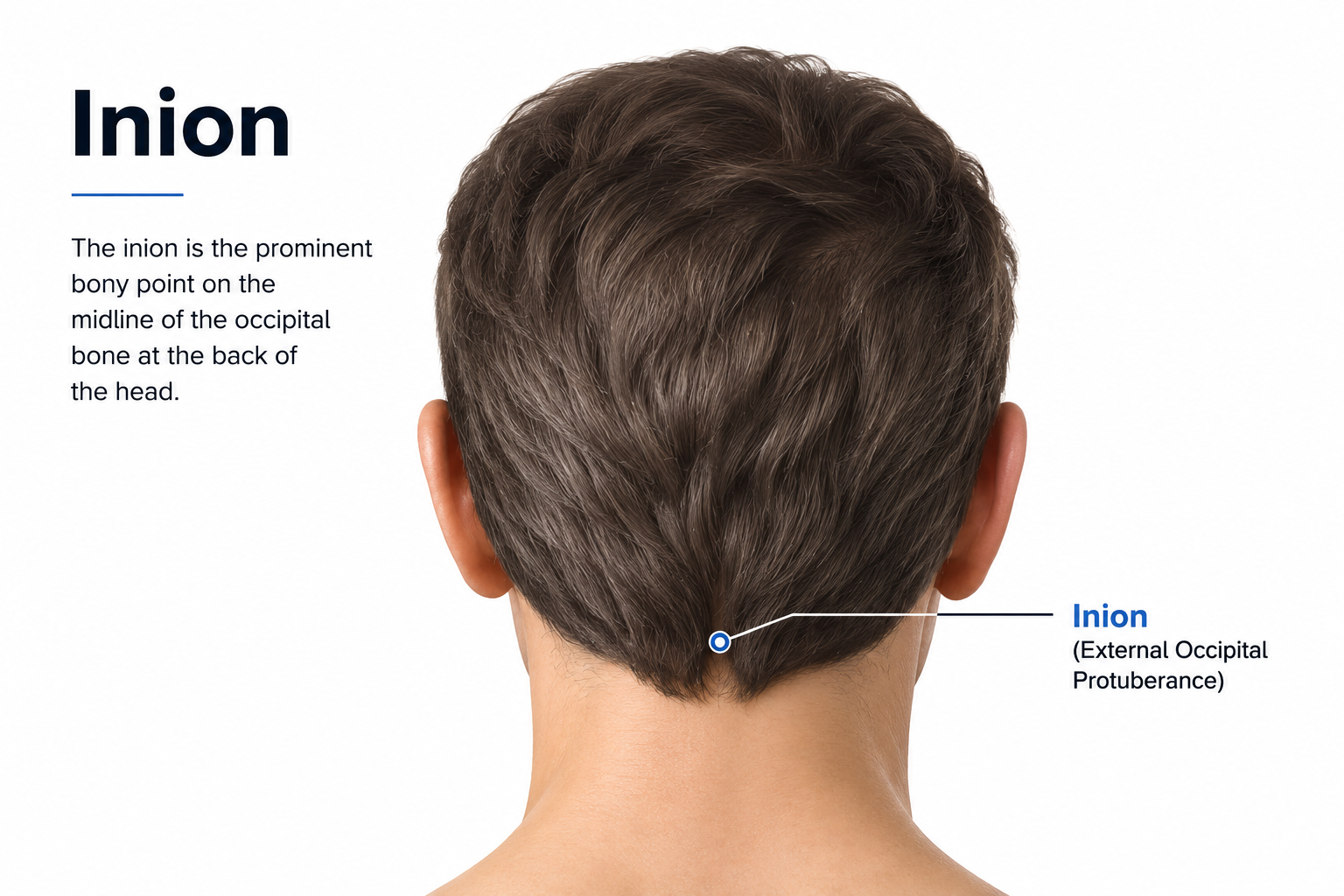
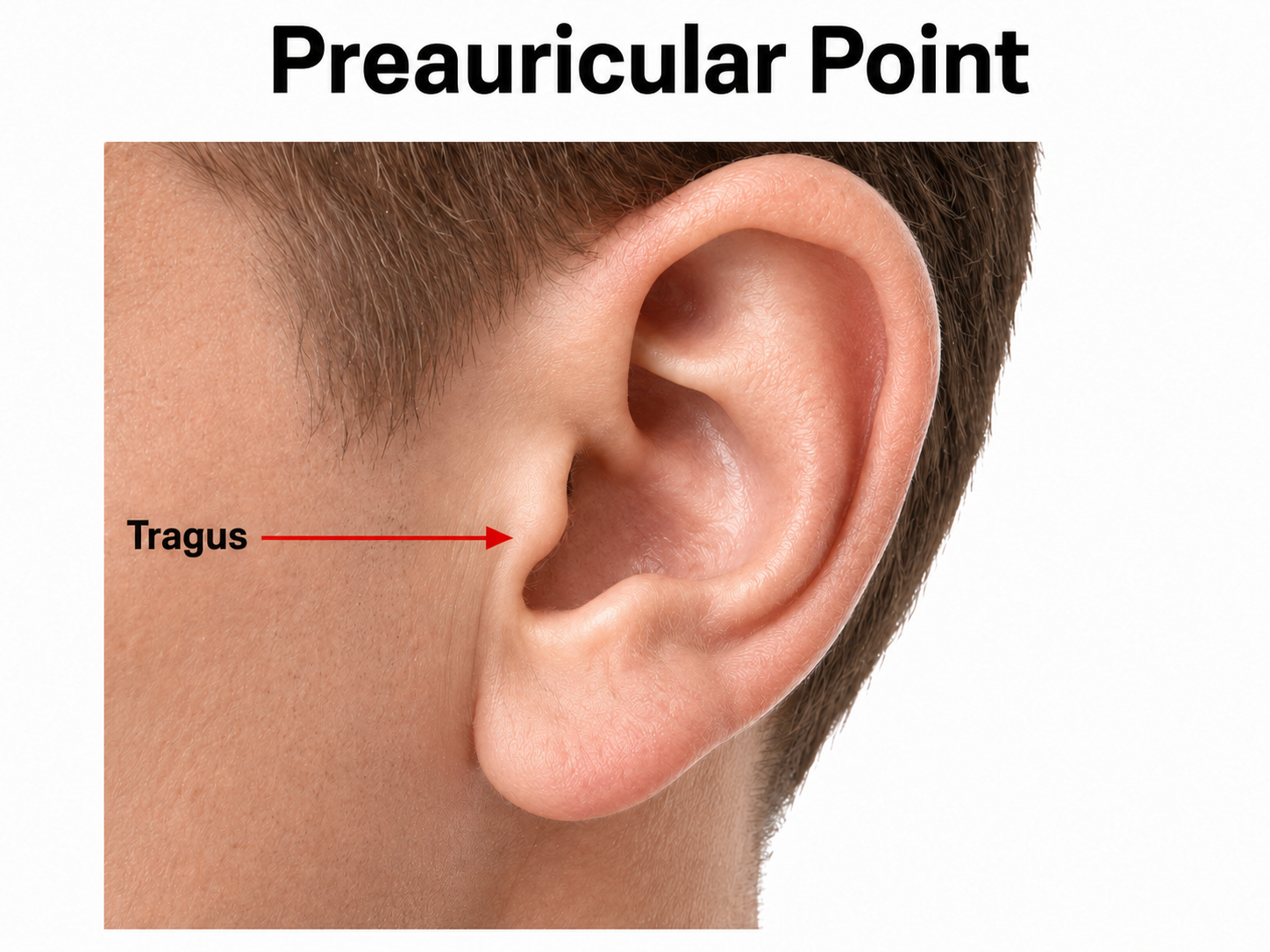
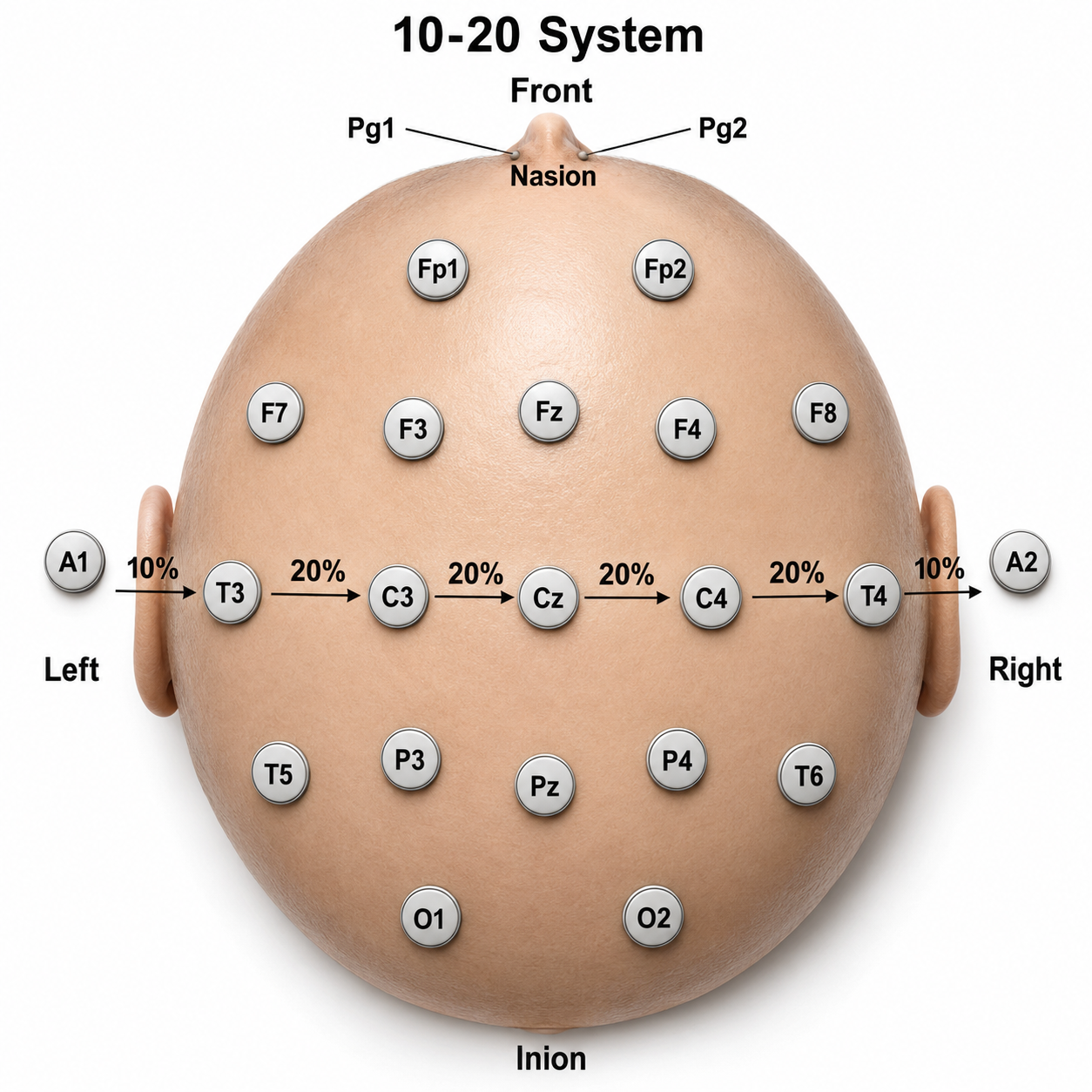
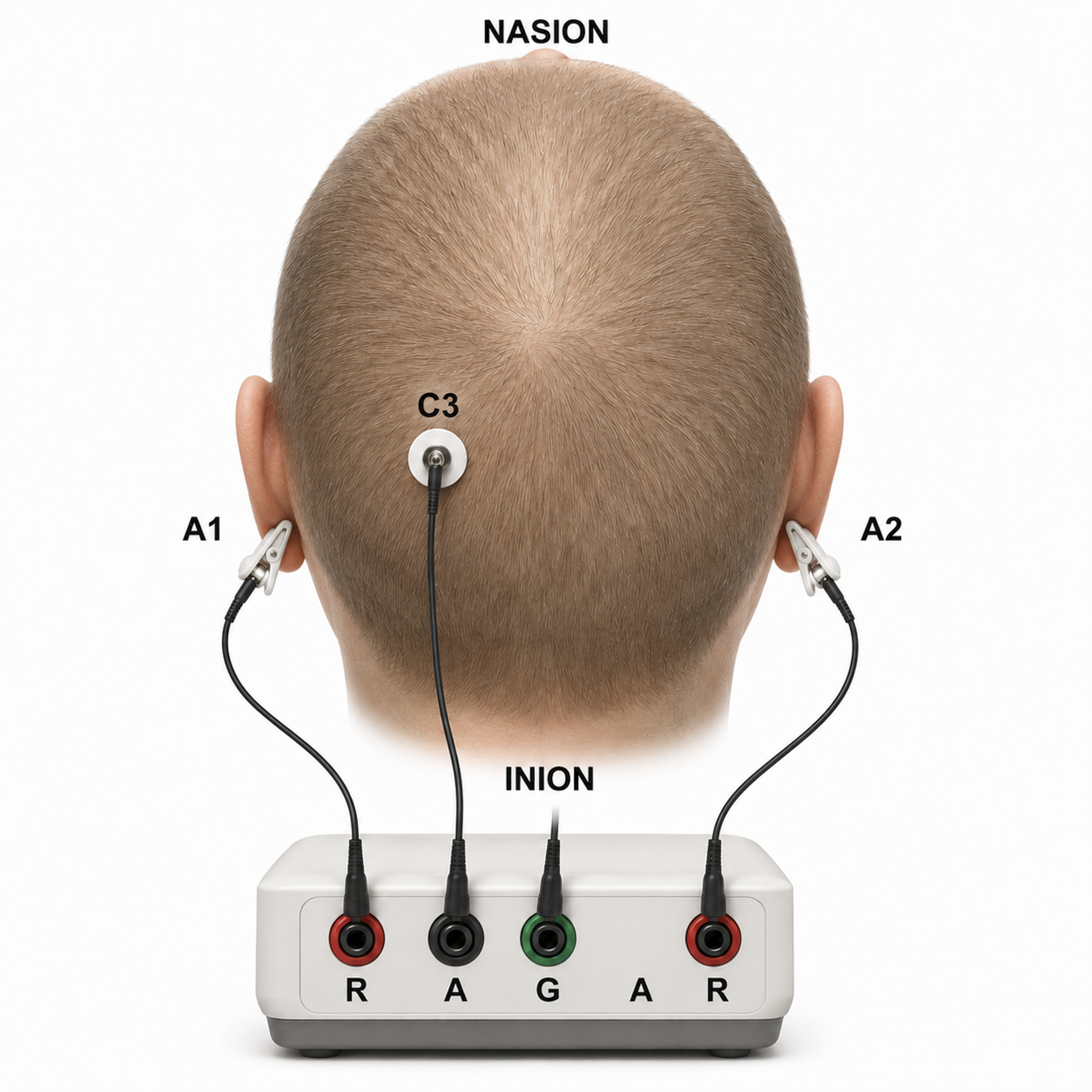
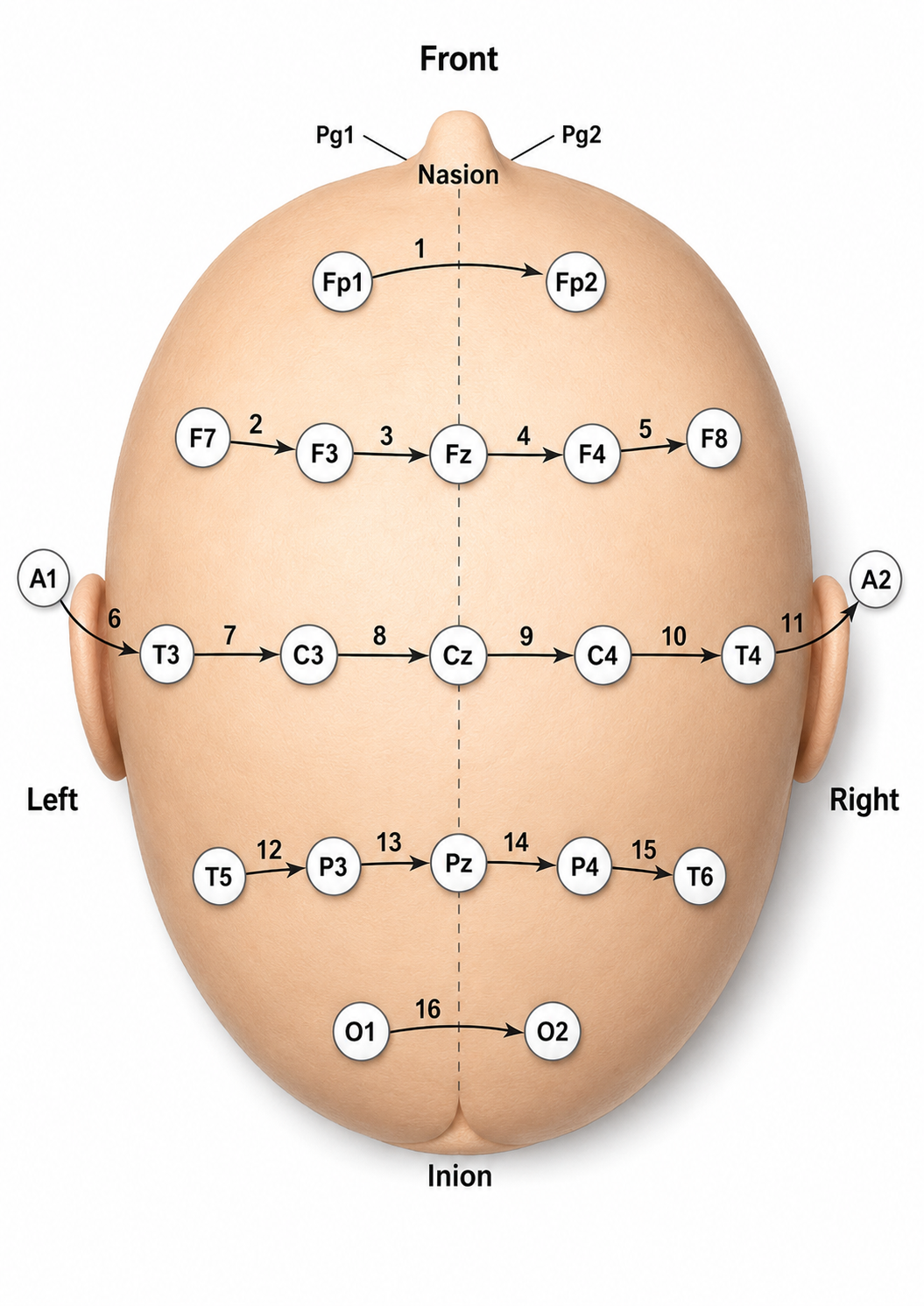
The system works by measuring two key distances on the head: from the nasion (the depression at the bridge of the nose) to the inion (the bony prominence on the back of the skull), and from the left preauricular point (the slight depression in front of the ear, above the earlobe) to the right. Electrode positions are then calculated at intervals of 10% or 20% along these distances. The flap at the opening of the ear is called the tragus, a useful landmark during setup. Check out the YouTube video The International 10-20 System for a visual walkthrough of these landmarks.
Graphic © Alila Medical Media/Shutterstock.com.
The nasion is the depression at the bridge of the nose.
The inion is the external occipital protuberance, the bony prominence at the midline on the back of the skull, along the superior nuchal (occipital) ridge.
The left and right preauricular points are slight depressions located in front of the ears and above the earlobe. The flap at the opening of the ear is called the tragus.
The vertex (Cz) sits at the intersection of two imaginary lines: one drawn from the nasion to the inion, and the other between the two preauricular points. Cz is located at the 50% mark along both lines, placing it at the very top of the head.
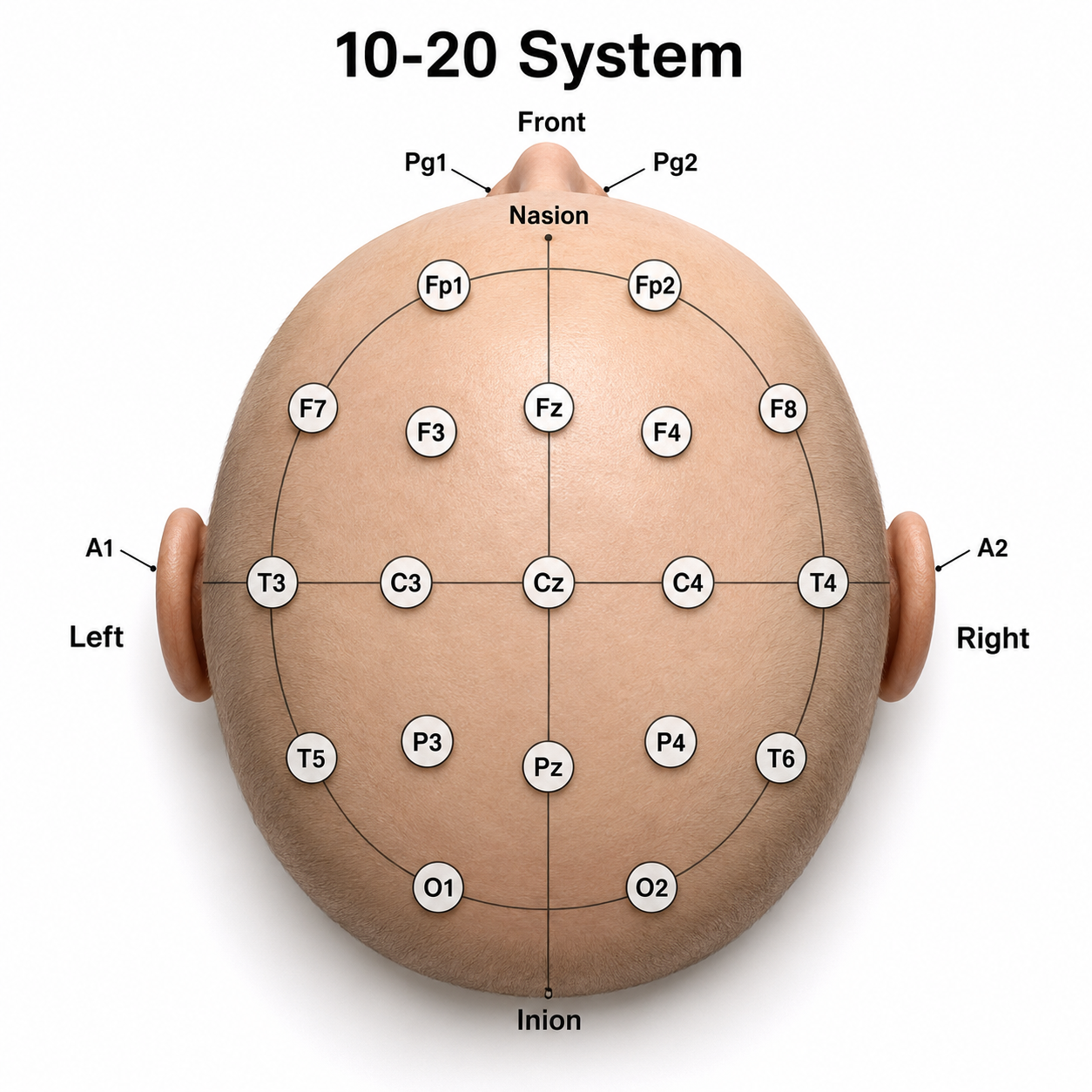
The system gets its "10-20" name because electrode sites are separated by either 10% or 20% of the distance between corresponding anatomical landmarks. In the graphic below adapted from Fisch (1999), each midline site is positioned at 10% or 20% of the nasion-to-inion distance.
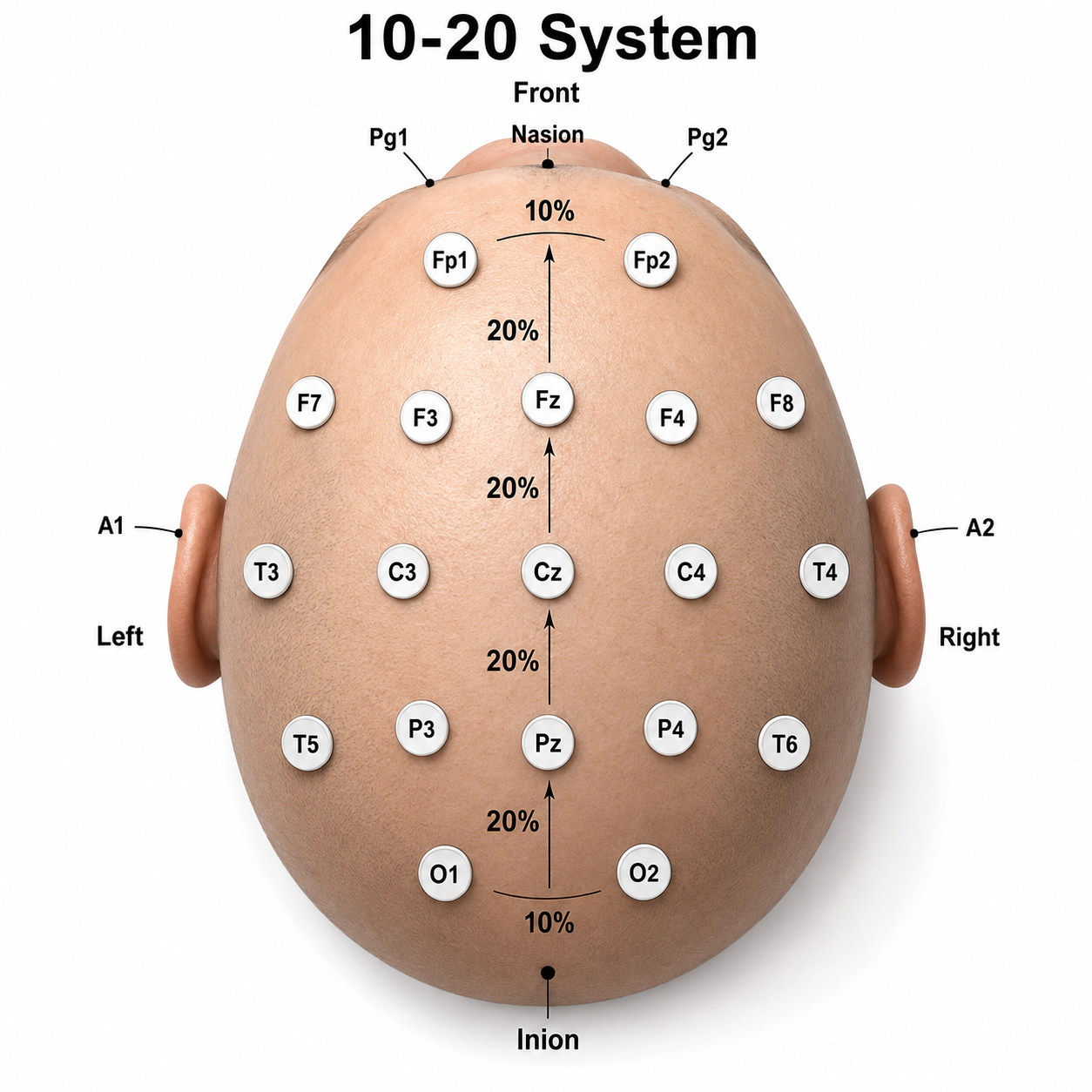
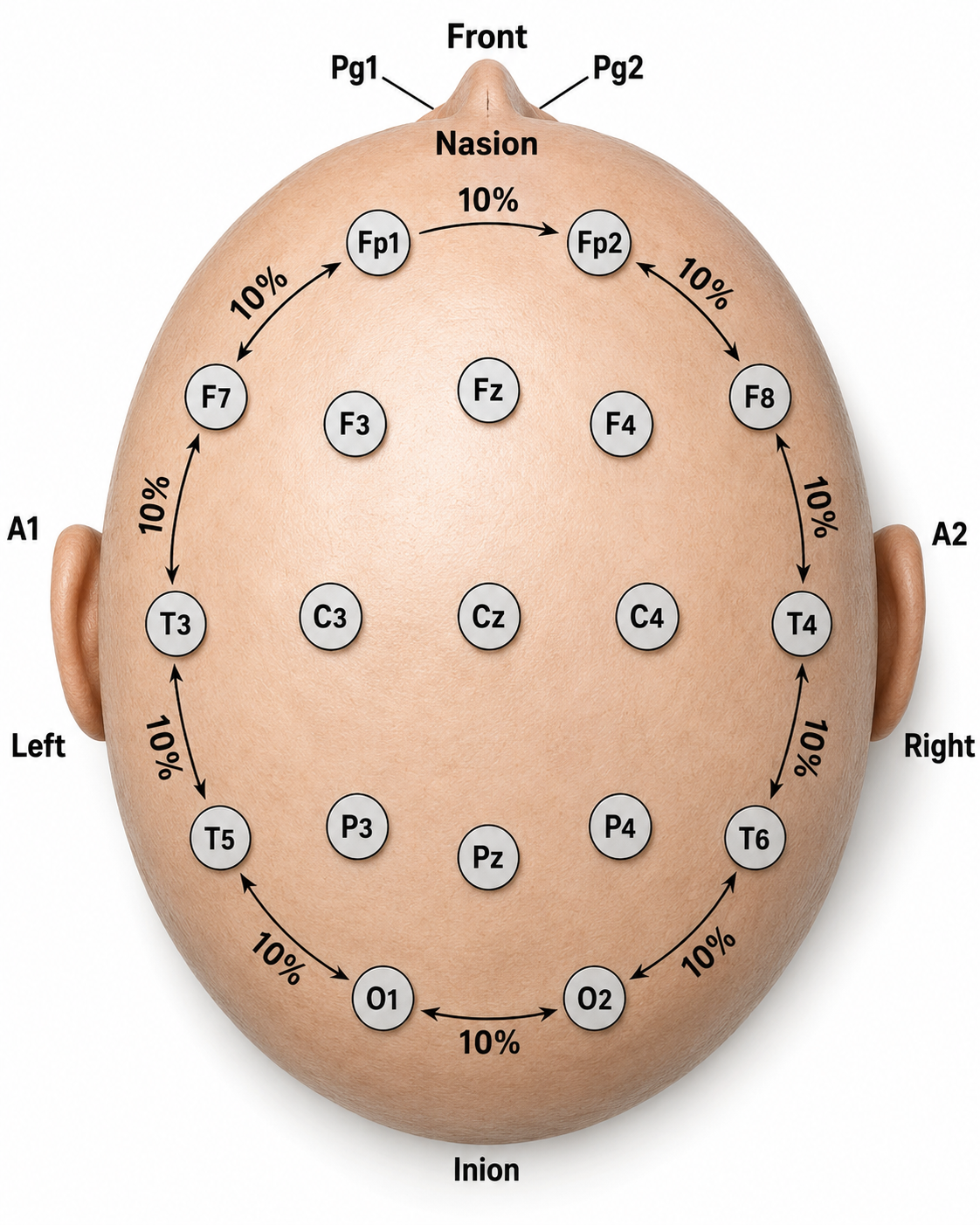
Each circumferential site is 10% of the total circumference, excluding Fpz or Oz.
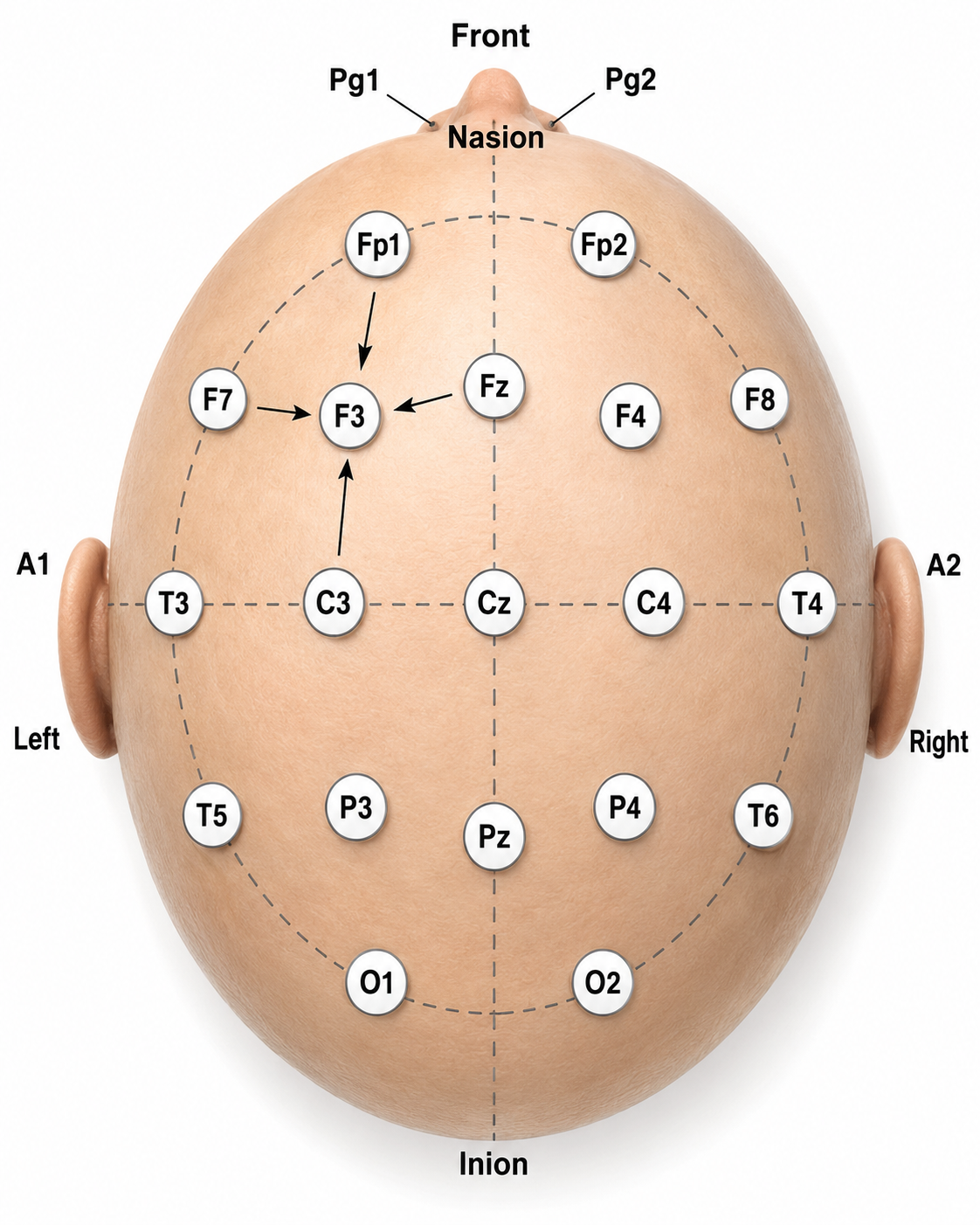
Intermediate sites are halfway between sets of adjacent sites.
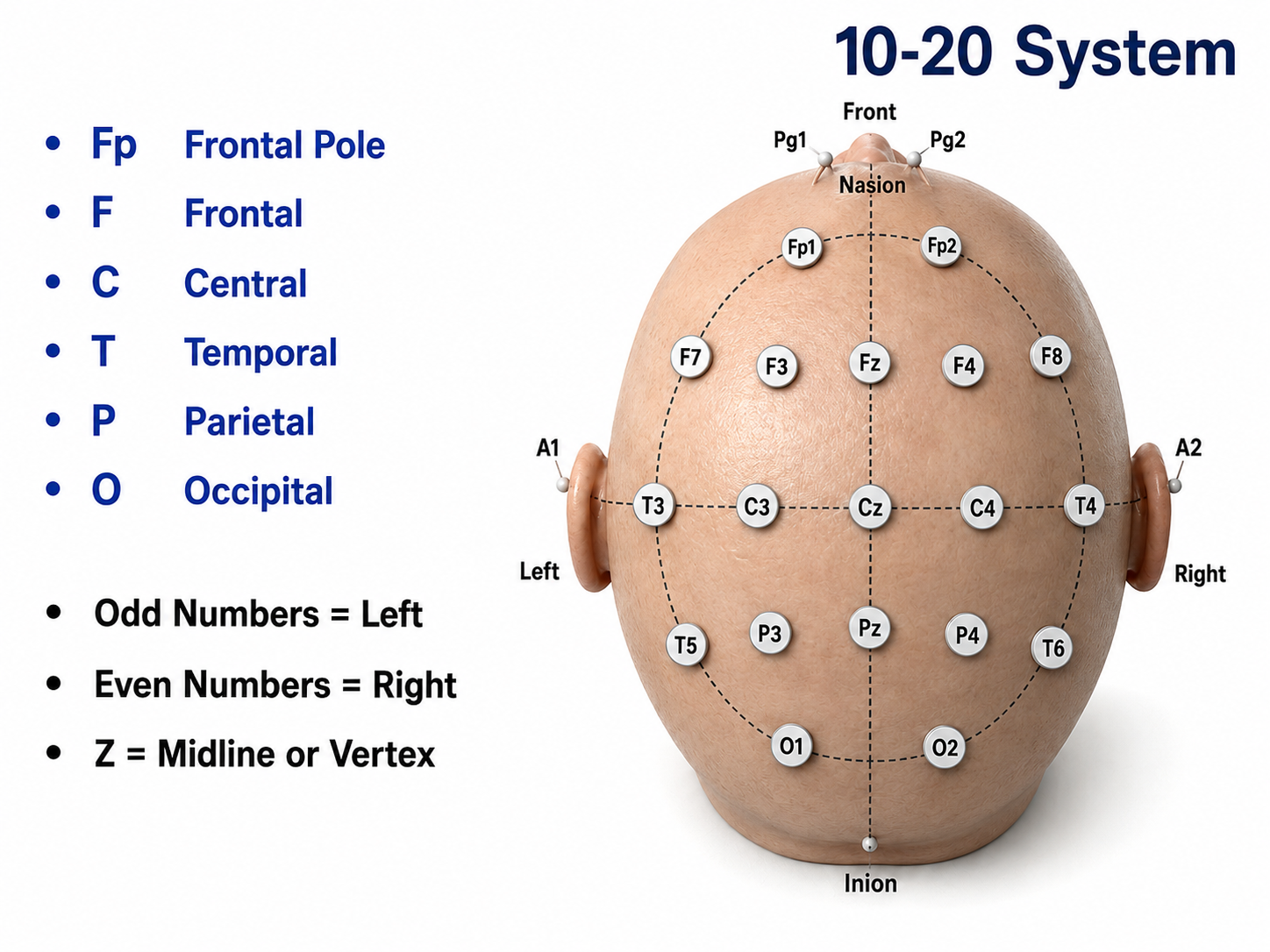
Each electrode is assigned a letter-and-subscript label that tells you exactly where it sits. The letters represent the underlying brain region: Fp (frontopolar or prefrontal), F (frontal), C (central), P (parietal), O (occipital), and A (auricular). A subscript of z indicates a midline placement along the central axis from nasion to inion.
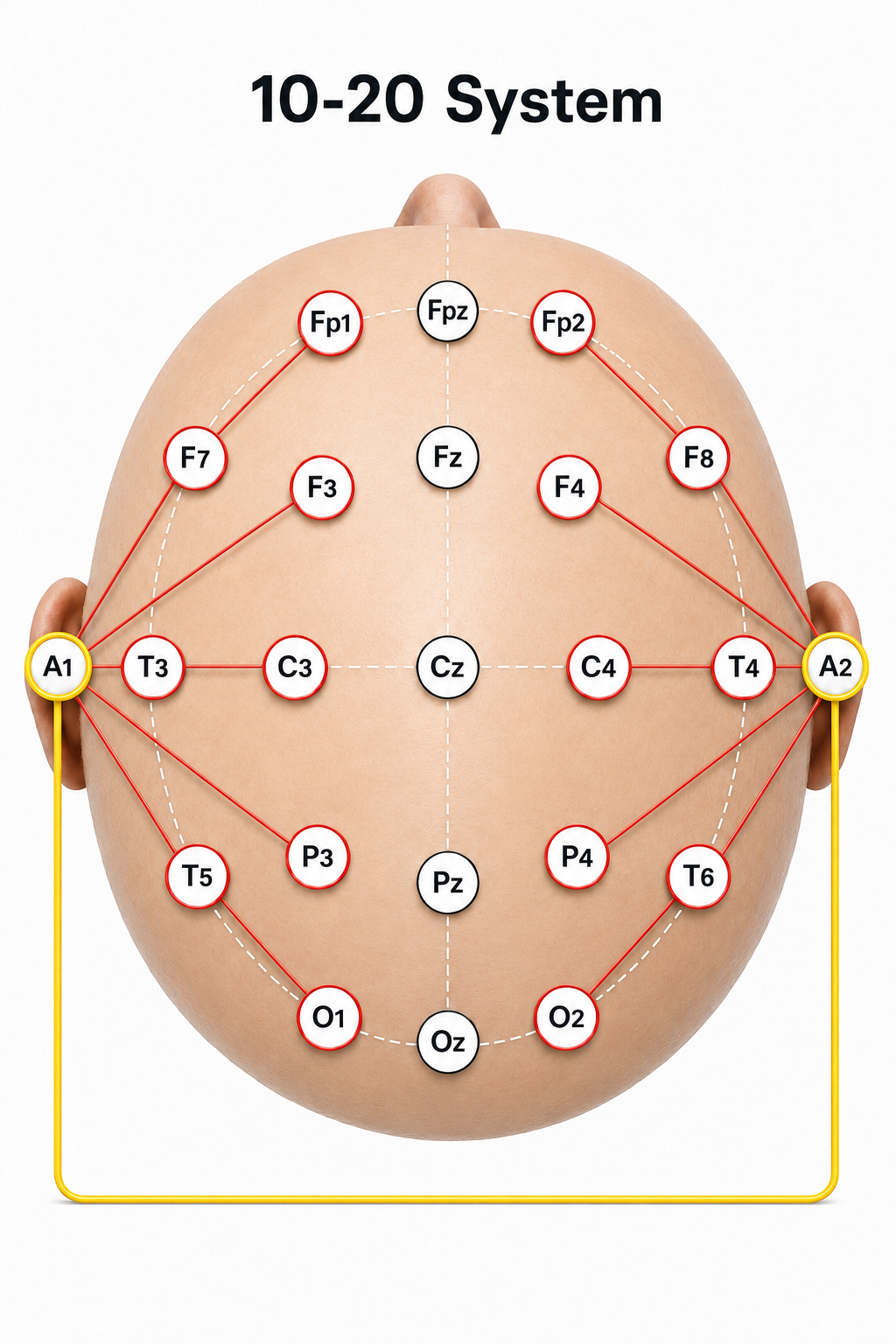
Numerical subscripts range from 1 to 8 and increase with distance from the midline. The 10-20 system assigns odd-numbered electrodes to the left hemisphere and even-numbered electrodes to the right, a convention worth memorizing since it applies throughout clinical EEG. Two ear electrodes (A1 and A2), which serve as reference sites in many montages, are typically placed on the earlobes.
You will notice this unit referring to both 19 and 21 electrodes, so it is worth reconciling the two counts. The standard clinical array uses 19 scalp recording sites (Fp1 through O2), and adding the two ear electrodes (A1 and A2) brings the total to the 21 electrode placements specified by the American Clinical Neurophysiology Society (Acharya et al., 2016). A separate ground electrode completes the setup. Whether A1 and A2 are described as recording or reference electrodes depends on the montage in use, which is why you will also see the array written as 19 scalp electrodes plus reference and ground. Keeping this distinction in mind will help you interpret electrode counts consistently as you work through the rest of the unit.
Modified Combinatorial Nomenclature
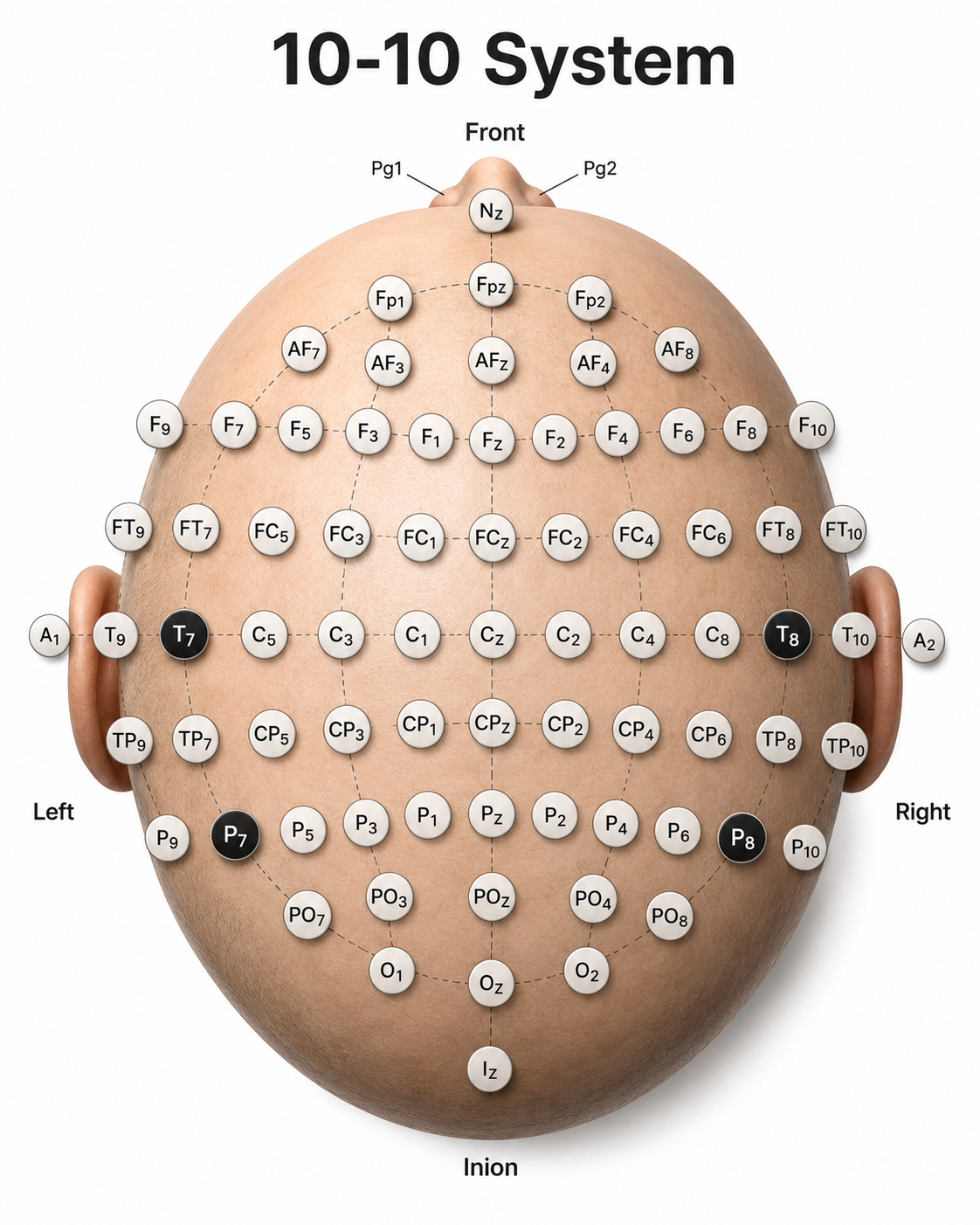
The American Clinical Neurophysiology Society (ACNS)—and, before its renaming, the American Electroencephalographic Society—published nomenclature guidelines that expand the 10-20 system to 75 electrode positions (ACNS Guideline 2; Acharya et al., 2016). This expanded system allows clinicians to define sites midway between standard 10-20 positions, better localize epileptiform activity, increase EEG spatial resolution (the ability to distinguish activity from different brain areas), and improve detection of localized evoked potentials. Adding electrodes improves spatial sampling; it does not overcome the blurring produced by volume conduction through the skull and scalp.
The modified combinatorial system also corrects inconsistent legacy designations, replacing T3/T4 and T5/T6 with the more logical T7/T8 and P7/P8. In the diagram below, black circles with white lettering depict these replacement sites. Also called the 10-10 system, this arrangement locates electrodes at every 10% along medial-lateral contours and adds new contours between those in the original 10-20 layout. Each electrode site sits at the intersection of a medial-to-lateral coronal line (designated by letters) and a longitudinal sagittal line (designated by numerical subscripts).
As with the 10-20 system, letters represent the underlying region: N (nasion), Fp (frontopolar or prefrontal), AF (anterior frontal), F (frontal), FT (frontotemporal), FC (frontocentral), A (auricular), T (temporal), C (central), TP (temporoparietal), CP (centroparietal), P (parietal), PO (parieto-occipital), O (occipital), and I (inion). Each two-letter label marks an intermediate contour: AF lies between Fp and F, FT and FC between F and T/C, TP and CP between T/C and P, and PO between P and O.
Please note that in this nomenclature the letter "P" designates a parietal site when its subscripted number is 6 or less (P3, P4, Pz), whereas P7 and P8 designate the posterior temporal sites formerly labeled T5 and T6.
A subscript of z again represents a midline placement. Numerical subscripts range from 1 to 10 and increase with distance from the midline, with odd numbers on the left and even numbers on the right, the same convention used in the 10-20 system.
Comparison of Neuroimaging Techniques
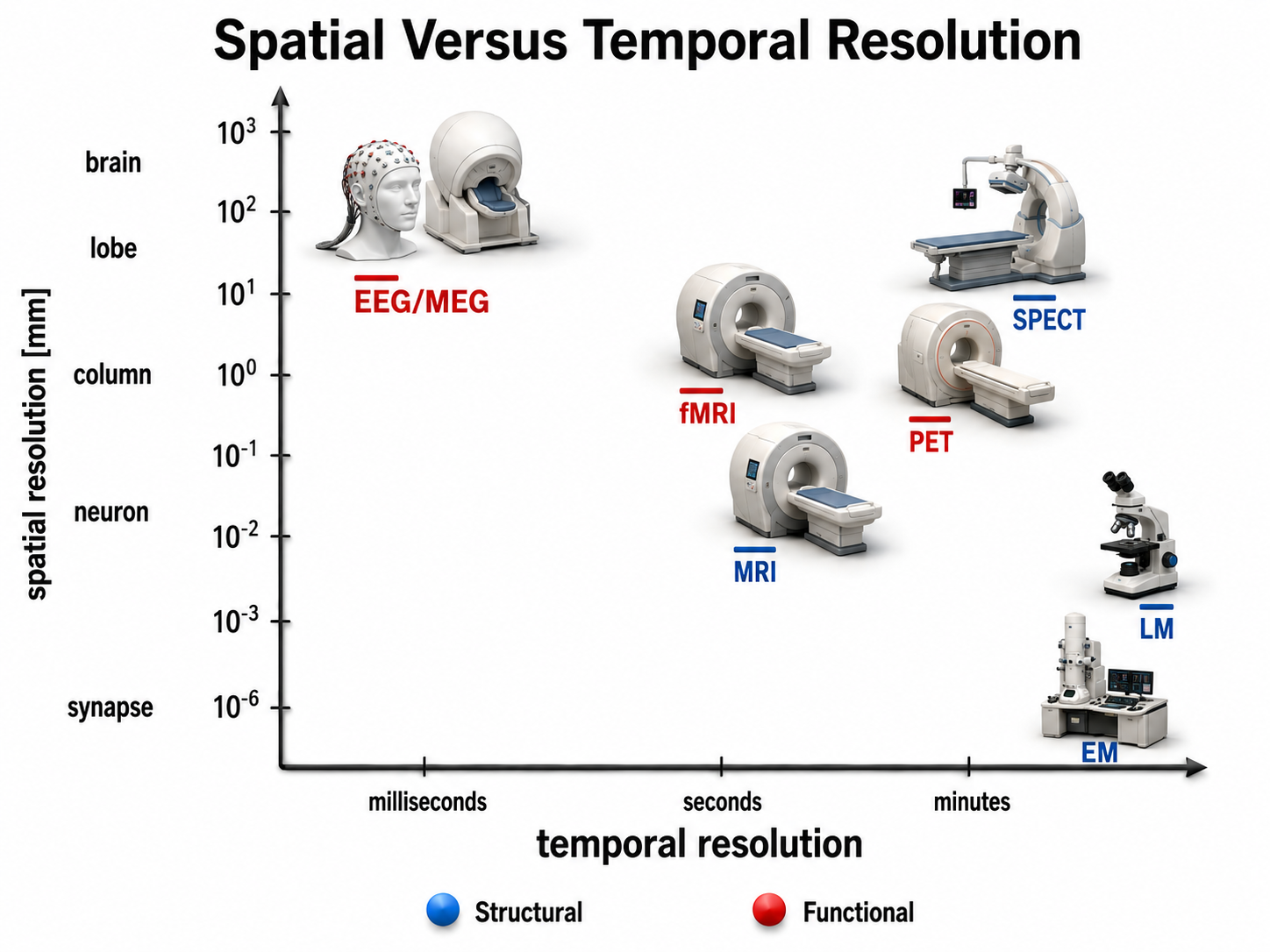
This section compares the major brain imaging methods, divided into structural techniques (which show anatomy) and functional techniques (which show activity). Understanding where EEG fits among these methods will help you appreciate both its strengths, particularly its excellent temporal resolution, and the complementary information that other modalities provide. Structural methods include CT and MRI, which present images of brain structures. Functional methods include EEG, MEG, fMRI, PET, and SPECT, each of which constructs images showing the location of differing levels of brain activity.
These functional techniques differ in the biological signals they measure. EEG detects brain electrical activity directly and MEG detects the magnetic fields that this activity generates; fMRI tracks blood oxygenation as an indirect marker of neural activity; PET uses positron-emitting radioisotopes attached to a tracer molecule, most commonly the glucose analog fluorodeoxyglucose (FDG), though many other tracers are used; and SPECT uses gamma-emitting radioisotopes. Because PET and SPECT usually require administering radioactive tracers and expose the patient to ionizing radiation, they are more invasive and carry greater risk for patients and research participants (Breedlove & Watson, 2023).
Each functional method can be evaluated on two dimensions: temporal resolution (how quickly it detects changes in function) and spatial resolution (how precisely it locates where those changes occur). EEG and MEG excel at temporal resolution, capturing neural events in milliseconds, but locating the sources of those events requires solving an inverse problem that has no unique solution, so their effective spatial resolution is generally coarser and less certain than fMRI's millimeter-level precision. This tradeoff is central to choosing the right imaging tool for a given clinical or research question.
Structural Techniques
The main structural imaging techniques are computerized axial tomography and magnetic resonance imaging.
Computerized Axial Tomography
Computerized Axial Tomography (CAT or CT) provides medium-resolution images of brain structure by moving an x-ray source along an arc surrounding the head (Breedlove & Watson, 2023). CT scans allow physicians to visualize structural abnormalities such as stroke damage and tumors, making them a valuable first-line diagnostic tool in emergency settings.

Graphic © Tyler Olson/Shutterstock.com.
Graphic © Triff/Shutterstock.com.
Magnetic Resonance Imaging (MRI)
Magnetic resonance imaging (MRI) constructs higher-resolution images than CT scans by using powerful magnetic fields and radio wave pulses. Because MRI does not use ionizing radiation, it carries less cumulative risk with repeated use, although its strong magnetic field creates its own safety contraindications for patients with certain implants. MRI scans allow detailed examination of brain anatomy, including the location and volume of specific brain regions. Their superior spatial resolution can detect subtle abnormalities, such as the demyelination seen in multiple sclerosis, that CT scans would miss (Breedlove & Watson, 2023).

Graphic © Peastock/Shutterstock.com.
Graphic © MriMan/Shutterstock.com.
Functional Techniques
The functional techniques reviewed below include the EEG and qEEG, magnetoencephalography (MEG), functional magnetic resonance imaging (fMRI), positron emission tomography (PET), and single-photon computerized emission tomography (SPECT). See Lebby (2013) for an excellent overview of these techniques. Also, consult the McGill brain imaging tool module.
EEG
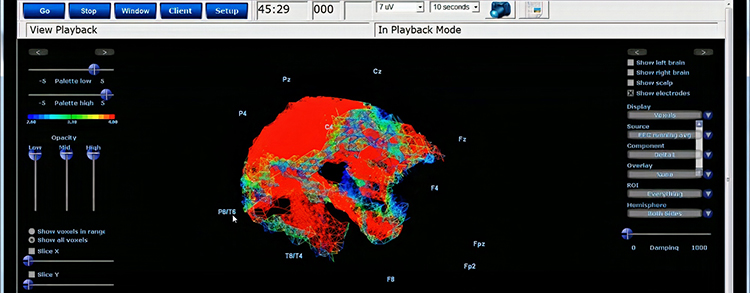
EEG and qEEG can be understood as functional imaging techniques in their own right, although a single-channel recording images the signal's frequency content rather than its anatomical source. Even a single-channel EEG displays microvolt amplitudes across adjacent 1-Hz bins or frequency bands, as in a 2D or 3D spectrogram. The 19-channel qEEG adds spatial information, mapping activity across the scalp using a 2D 10-20 layout, or estimating distributed sources in three dimensions with methods like LORETA (Low Resolution Brain Electromagnetic Tomography) and its variants sLORETA and eLORETA (Pascual-Marqui et al., 1994). As their name indicates, these are low-resolution source estimates constrained by modeling assumptions, not direct measurements of deep activity.
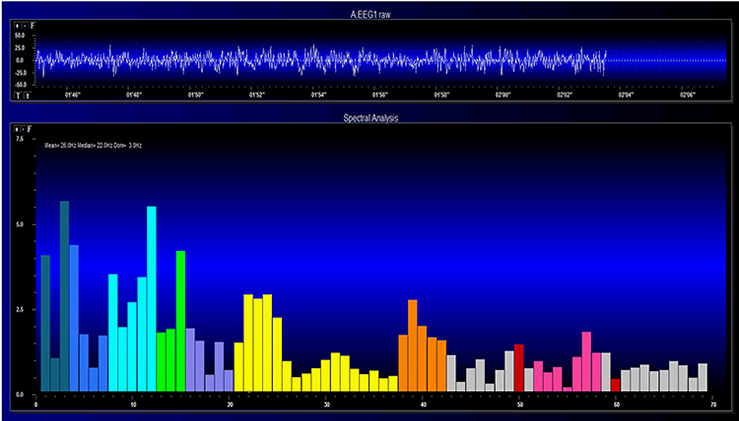
Graphic © John S. Anderson.
Graphic courtesy of BrainMaster Technologies.
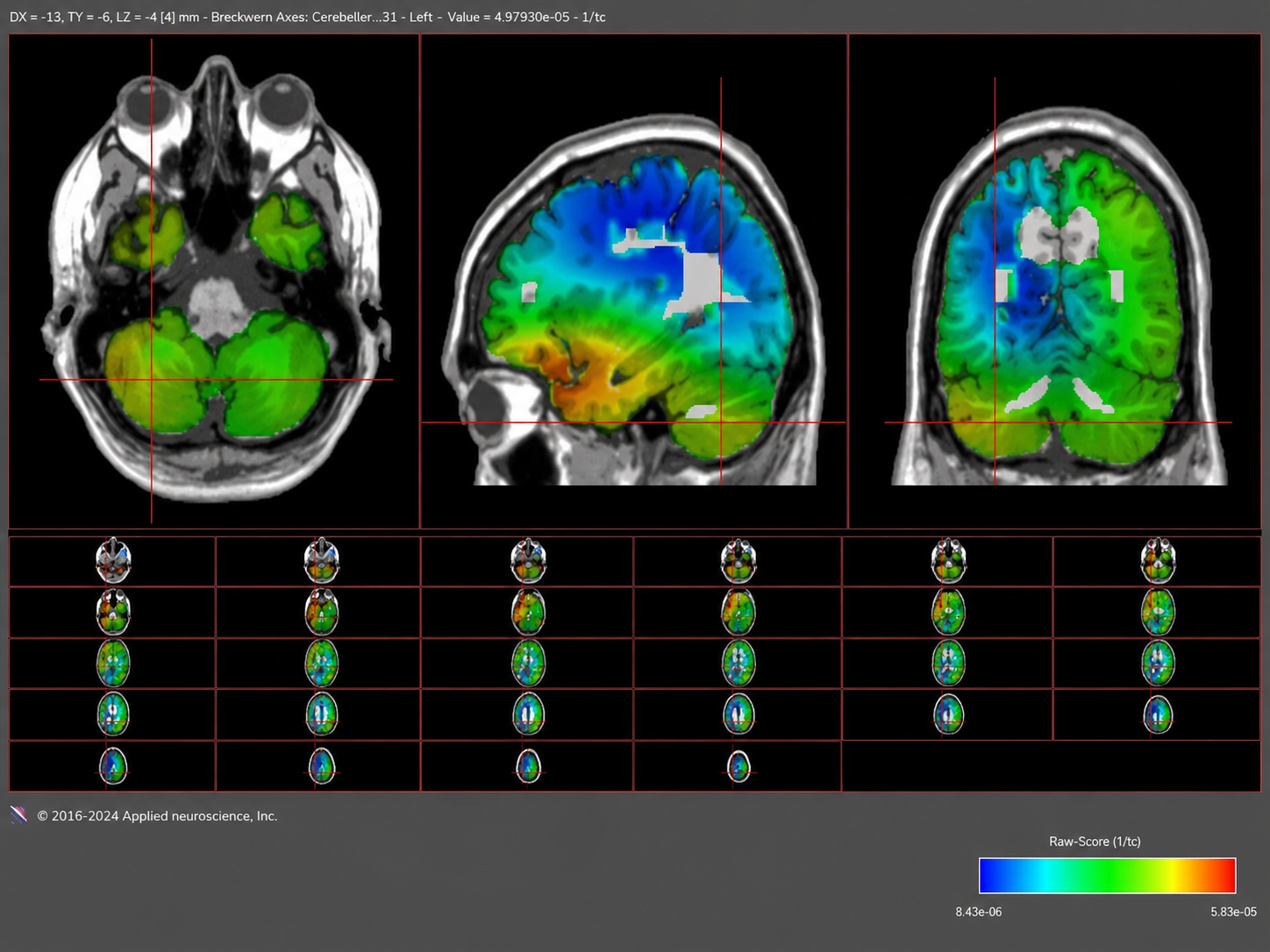
swLORETA graphic from Neuroguide - NeuroNavigator.
Magnetoencephalography
Magnetoencephalography (MEG) is a noninvasive functional imaging technique that has traditionally used SQUIDs (superconducting quantum interference devices), and increasingly uses optically pumped magnetometers (OPMs), to detect the weak magnetic fields generated by neuronal activity. Like EEG, MEG offers millisecond temporal resolution, allowing it to measure rapidly shifting patterns of cortical circuit activation (Breedlove & Watson, 2023). Because the skull distorts magnetic fields far less than electric fields, MEG generally localizes superficial cortical sources more accurately than scalp EEG—reported localization errors are often on the order of a few millimeters to about a centimeter—but its accuracy depends on source depth, orientation, and the head model used, and it remains less spatially certain than fMRI. Researchers sometimes combine MEG with MRI to better delineate the cortical structures generating the detected magnetic fields (Lin et al., 2004).

Magnetoencephalography Graphic © Image Source Trading ltd/Shutterstock.com.
Functional Magnetic Resonance Imaging (fMRI)
Functional Magnetic Resonance Imaging (fMRI) uses intense magnetic fields to detect the blood-oxygen-level-dependent (BOLD) signal, which reflects local changes in blood flow, blood volume, and the concentration of deoxygenated hemoglobin that accompany neural activity. Because blood flow increases more than oxygen consumption does, the BOLD signal is an indirect hemodynamic marker rather than a direct measure of oxygen use. Evidence from simultaneous recordings indicates that the signal corresponds more closely to local field potentials and synaptic input than to spiking output (Logothetis et al., 2001). A scanner's magnet strength, measured in teslas (T), strongly influences its spatial resolution, which is quantified in terms of voxel size, a three-dimensional pixel representing a specific volume of brain tissue. Higher magnet strength improves the signal-to-noise ratio, enabling finer voxel sizes and more detailed imaging. Most clinical and research scanning is done at 1.5 or 3.0 T; 7.0 T systems are now approved for clinical use, and ultra-high-field research scanners of 9.4 T and above exist at a small number of centers.

However, higher spatial resolution comes with a tradeoff: increased granularity can introduce more noise and potential artifacts, complicating the task of distinguishing true physiological signals from spurious data. Achieving the right balance between resolution and signal quality is crucial for accurate functional interpretations. Although fMRI is limited by the sluggishness of the hemodynamic response—which begins roughly 1 to 2 seconds after neural activity and peaks about 4 to 6 seconds later—it can reveal how networks contribute to cognitive performance. Compared to PET, fMRI offers both superior spatial resolution and superior temporal resolution, while PET retains the advantage of being able to image specific molecular targets (Breedlove & Watson, 2023).
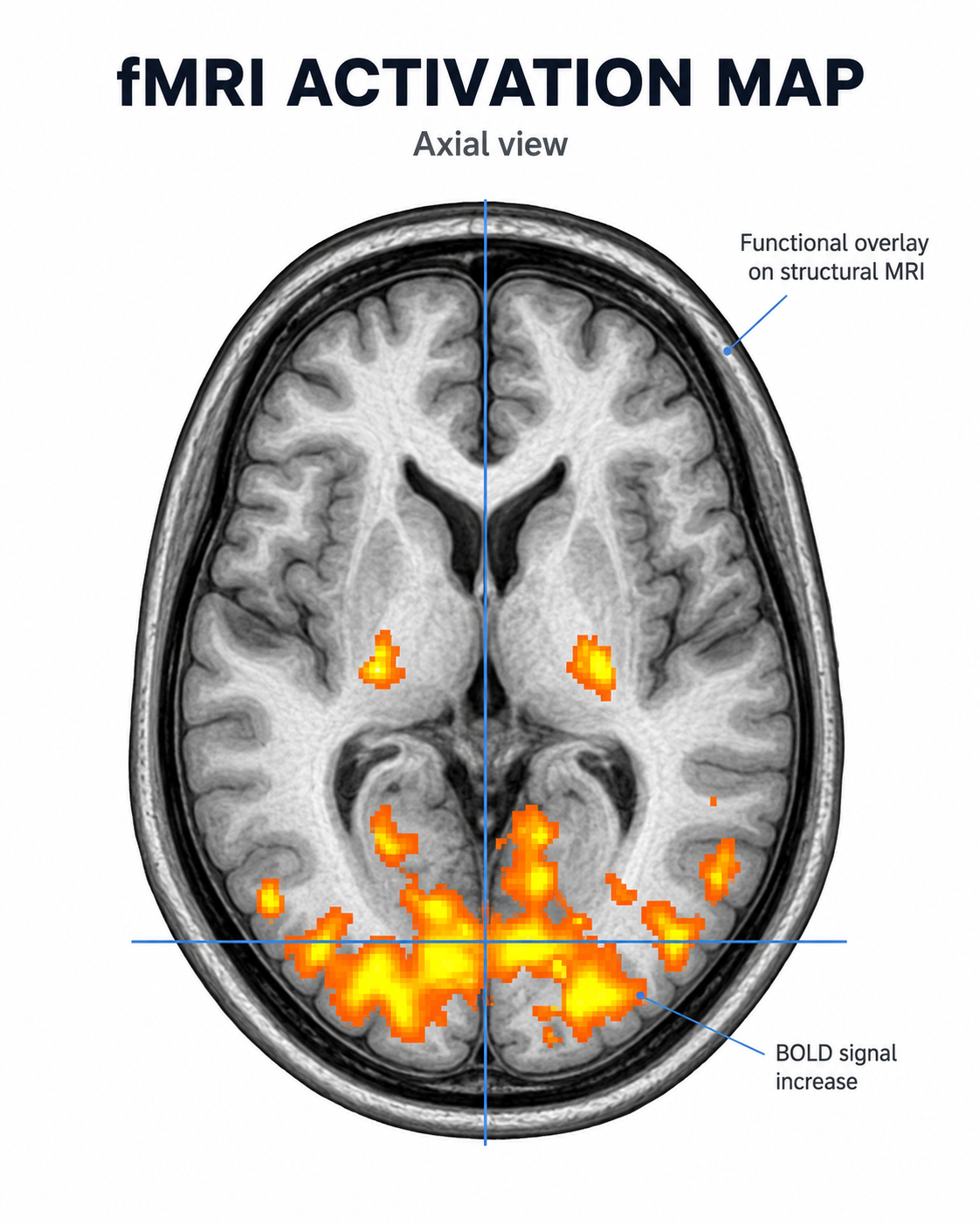
Axial fMRI activation map showing task-related BOLD signal increases overlaid on a structural MRI, with strongest activation in posterior cortical regions and smaller bilateral activation clusters in deeper cortical areas.
Positron Emission Tomography
Positron emission tomography (PET) is a functional imaging technique in which a radioactively labeled tracer is introduced into the bloodstream—usually by intravenous injection, sometimes by inhalation—and its distribution in the brain is imaged to measure metabolism, blood flow, or receptor binding (Breedlove & Watson, 2023). PET scans achieve low temporal resolution (tens of seconds to minutes) with moderate spatial resolution (roughly 4 to 6 mm on modern scanners), making them better suited for studying sustained metabolic and molecular processes than rapidly changing neural events.

PET scan graphic © Gorodenkoff/Shutterstock.com.
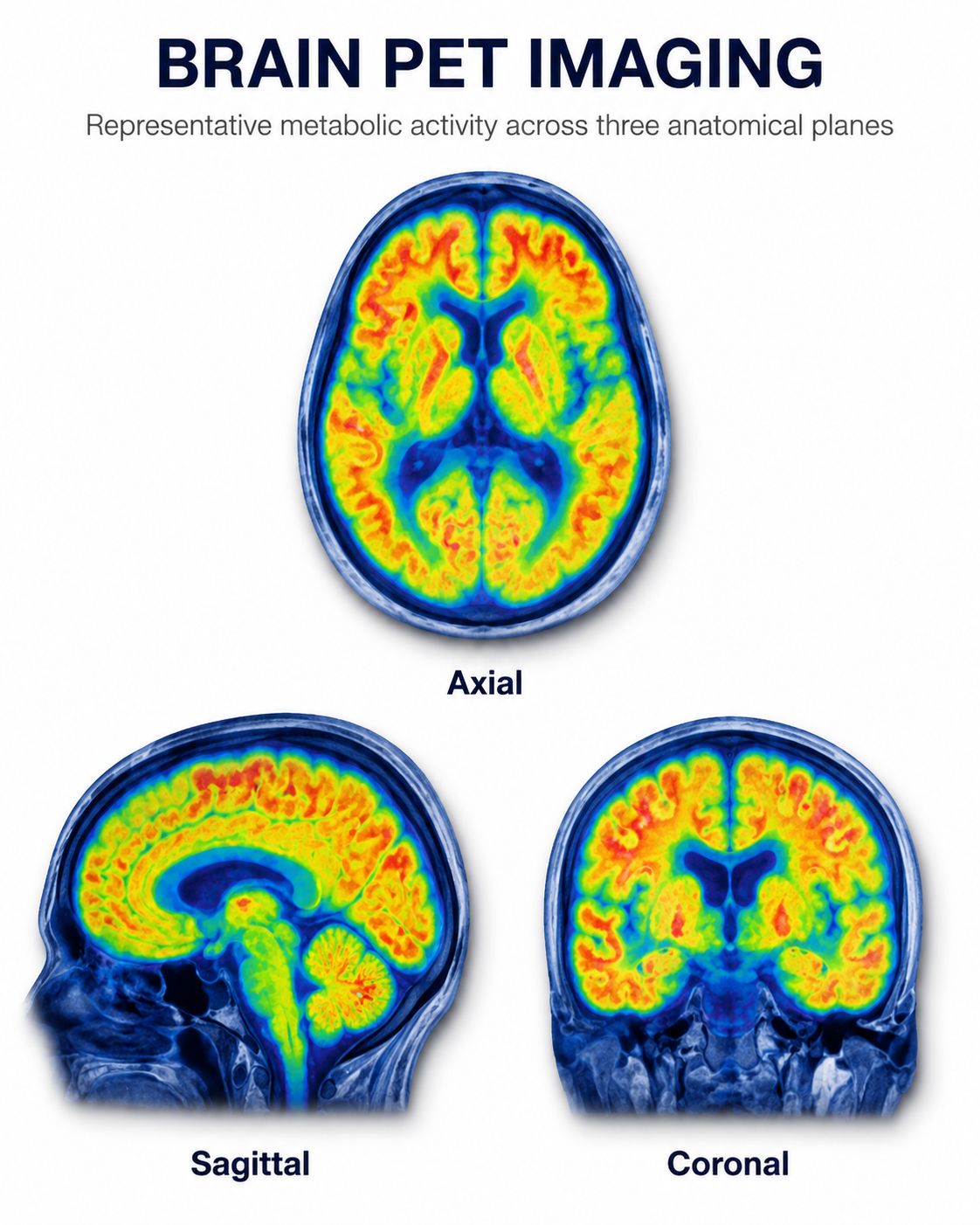
Brain PET imaging showing regional metabolic activity across axial, sagittal, and coronal planes, with warmer colors indicating higher tracer uptake and cooler colors indicating lower uptake.
Single-Photon Emission Computerized Tomography
Single-photon emission computerized tomography (SPECT) is a functional imaging technique that uses gamma rays to create three-dimensional and slice images of cerebral blood flow averaged over several minutes. SPECT achieves limited temporal resolution (minutes) and the coarsest spatial resolution of the functional methods discussed here—typically on the order of 1 cm—but it remains clinically useful for evaluating regional perfusion differences.

Graphic adapted from © rumruay/Shutterstock.com.
Using a Limited Number of Electrodes
This section examines the practical question of how many EEG channels you need for effective assessment and training. Peer-reviewed evidence indicates that increasing the number of electrodes improves spatial sampling and the accuracy with which independent sources can be separated from artifact; Lau et al. (2012), for example, found that source-separation accuracy in mobile EEG improved as channel count rose. It is important to distinguish that finding from the further claim that more channels produce better clinical or performance outcomes in neurofeedback, which has not been established by controlled trials. Although some practitioners conduct assessment and training with a single channel, multi-channel methods have become increasingly accessible as costs have decreased.
A full 19-channel EEG assessment, for example, not only provides amplitude and frequency data from every site in the 10-20 system but also enables computation of metrics such as coherence (the consistency of the common frequency content between two sites), phase (the timing relationship between signals at different sites) and co-modulation (the similarity in magnitude changes between two sites).
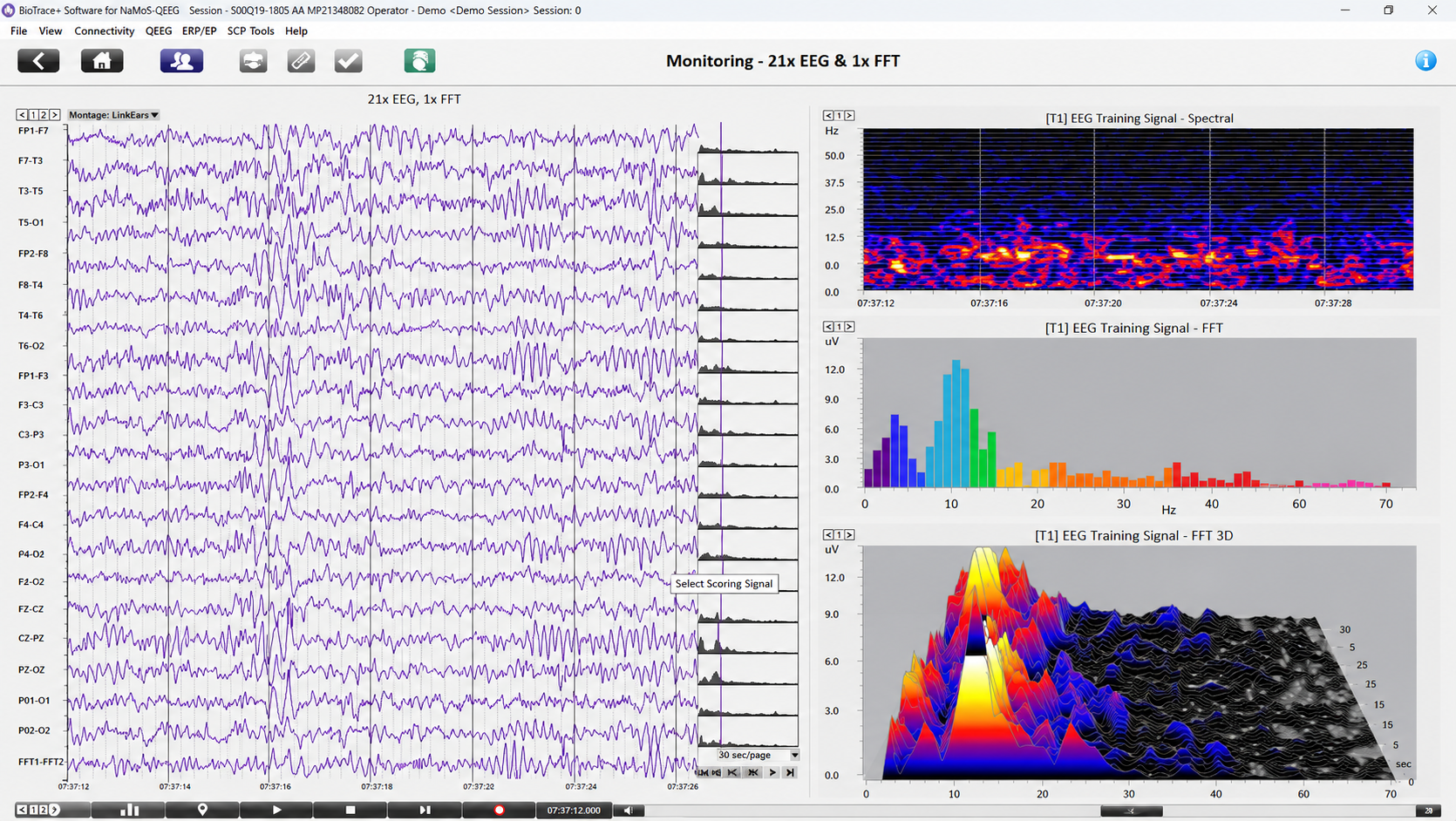
Raw Tracings and Multiple Spectral Displays from BioTrace - Mind Media
These connectivity metrics describe statistical relationships between the signals recorded at two sites, which are commonly interpreted as indexing communication between brain regions; a single channel cannot yield them at all. Because volume conduction and the choice of reference can inflate apparent connectivity, these measures require careful artifacting and cautious interpretation. Multi-channel data are particularly beneficial for complex symptom profiles like those associated with Autism Spectrum Disorders, epilepsy, and traumatic brain injury (Thompson & Thompson, 2015).
Graphic © Chaikom/Shutterstock.com.
A channel is an EEG amplifier output resulting from scalp electrical activity detected through three electrode connections: the active (positive) electrode, placed over a known EEG generator like Cz; the reference (negative) electrode, which may be located on the scalp, earlobe, or mastoid; and the ground electrode, also typically placed on an earlobe or mastoid (Thompson & Thompson, 2015). Terminology varies across textbooks and manufacturers. The two signal electrodes are more precisely described as input 1 (noninverting, +) and input 2 (inverting, −), and the third electrode is more precisely described as the amplifier's common or ground connection, which establishes the reference potential for the amplifier but contributes no signal of its own. The word "reference" is unfortunately used for both input 2 and this common connection, so read each source carefully.
Electrically, the two signal inputs are balanced and interchangeable; reversing them does not change the magnitude of the recorded difference, but it does invert the polarity of the displayed waveform. Some neurofeedback data acquisition systems nonetheless require that a specific sensor be designated the "reference," as in a linked-ears reference.
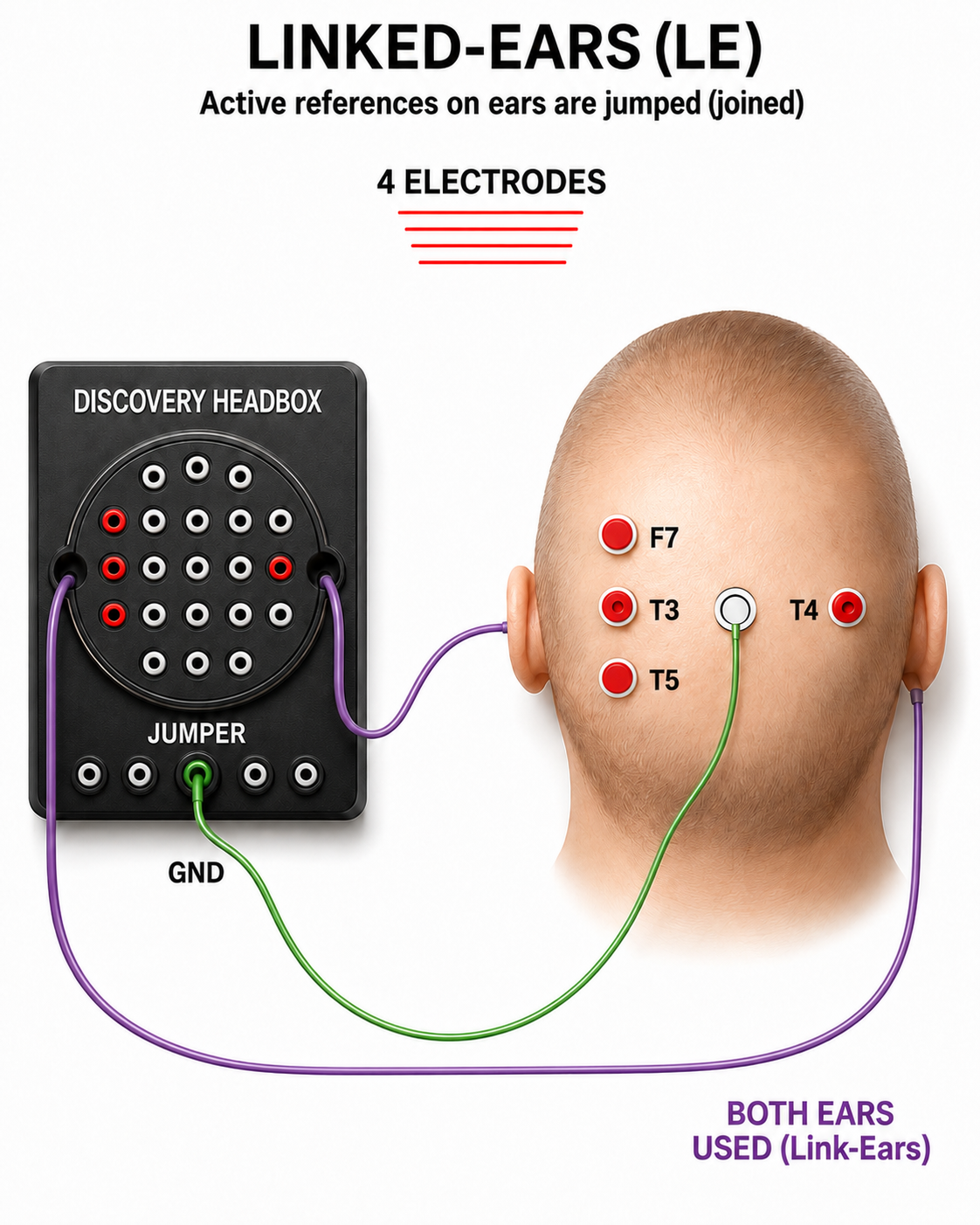
The graphic was adapted from John Demos' BCIA-recommended Getting Started with EEG Neurofeedback (2nd ed.). The ear references are connected as a common reference for the four active electrodes (F7, T3, T4, and T5).
A derivation is the assignment of two electrodes to an amplifier's inputs 1 and 2. For example, Fp1 to O2 means that Fp1 is placed in input 1 and O2 in input 2. A montage groups multiple derivations together to record EEG activity across several channels simultaneously (Thomas, 2007). Most modern digital amplifiers acquire every input relative to a single hardware reference—commonly Cz, FCz, CPz, or a mastoid, depending on the system—so montage changes are performed in software rather than by manually switching electrode connections.
All montages compare EEG activity between one or more pairs of electrode sites.
Montage Options and Their Consequences
Referential (Monopolar) Montage
A referential (monopolar) montage places one active electrode (A) on the scalp and a "neutral" reference (R) and ground (G) on the ear or mastoid. This montage assumes that the EEG activity displayed on your screen represents the active (+) site, because the reference (−) site is presumed to be electrically quiet. That assumption is never fully satisfied: no scalp or ear site is truly inactive, so the displayed waveform always reflects the difference between the two sites. The differential amplifier amplifies the difference between its two inputs while rejecting the portion common to both, a property called common-mode rejection, which attenuates noise and artifacts shared by both sites.
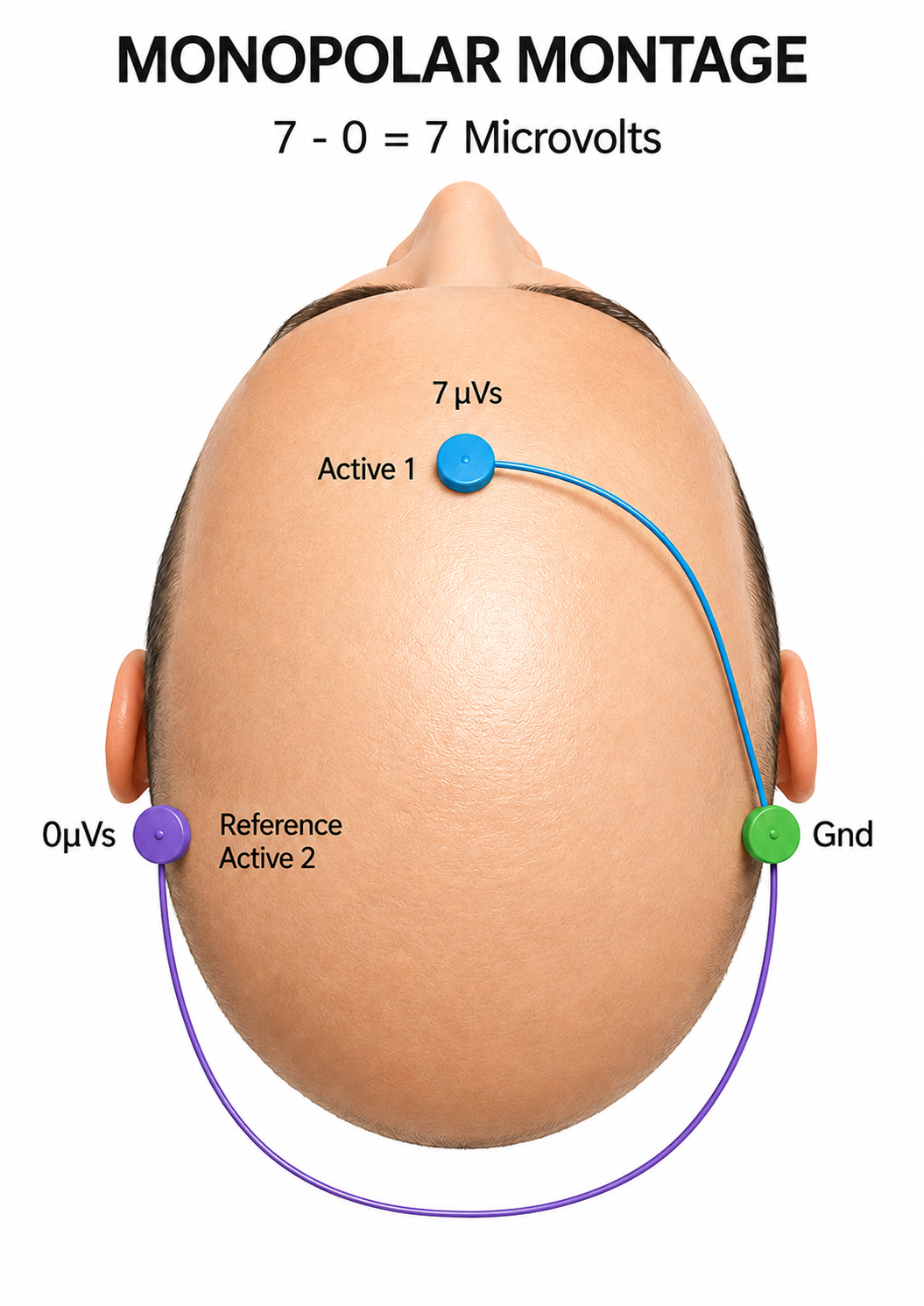
We adapted this graphic from John Demos' BCIA-recommended Getting Started with EEG Neurofeedback (2nd ed.). The active electrode "sees" 7 microvolts while the reference "sees" 0 microvolts, so the amplifier outputs their difference of 7 microvolts. This idealized example assumes a perfectly inactive reference.
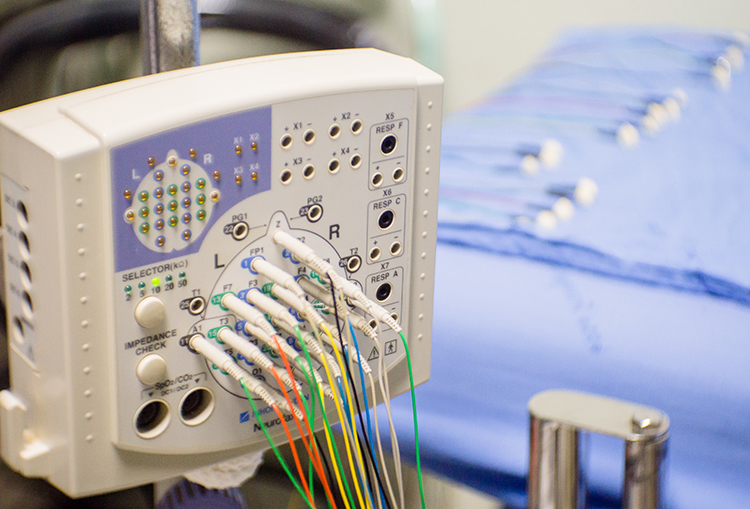
In the photograph below, the blue cable would be used for the active electrode, the yellow cable with an ear clip for reference, and the black cable with an ear clip for the ground.

However, this montage is vulnerable to artifacts from the contraction of facial muscles (Demos, 2019). The ear reference can also introduce reference contamination, where EEG signals picked up by the ear electrode are added to other channels through the differential amplifier, since the amplifier retains anything that differs between the active and reference inputs. This commonly results in alpha activity from posterior sources close to the ear appearing in channels where it does not belong.
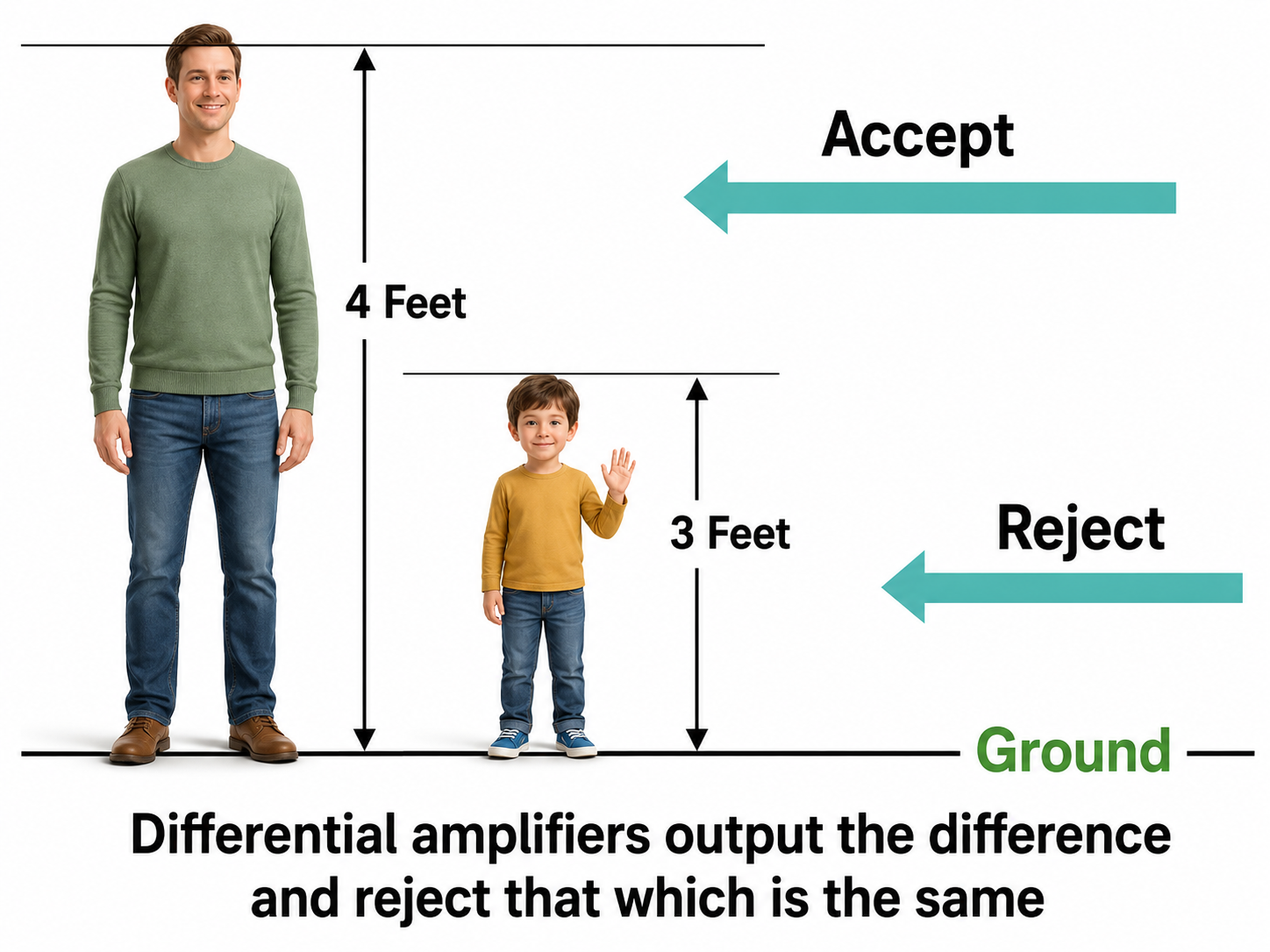
We adapted this graphic from John Demos' BCIA-recommended Getting Started with EEG Neurofeedback (2nd ed.). In this height analogy, a differential amplifier rejects the portion common to both inputs (e.g., 3 feet) and outputs only the difference (e.g., 4 feet). A single-ended amplifier outputs the entire value (e.g., 7 feet, artifact plus signal). The units here are illustrative only; actual EEG voltages are measured in microvolts.
Sequential (Bipolar) Montage
A sequential (bipolar) montage compares EEG activity between two scalp electrodes, both considered "active" sites, rather than referencing one to a presumed-neutral ear or mastoid. The positive (+) and negative (−) electrodes (often called "active" and "reference") are both attached to the scalp, while the ground (G) electrode is placed on the scalp, an earlobe, or over the mastoid process. Like the referential montage, this configuration detects the voltage difference between its two inputs, but now both inputs carry cerebral EEG signals.
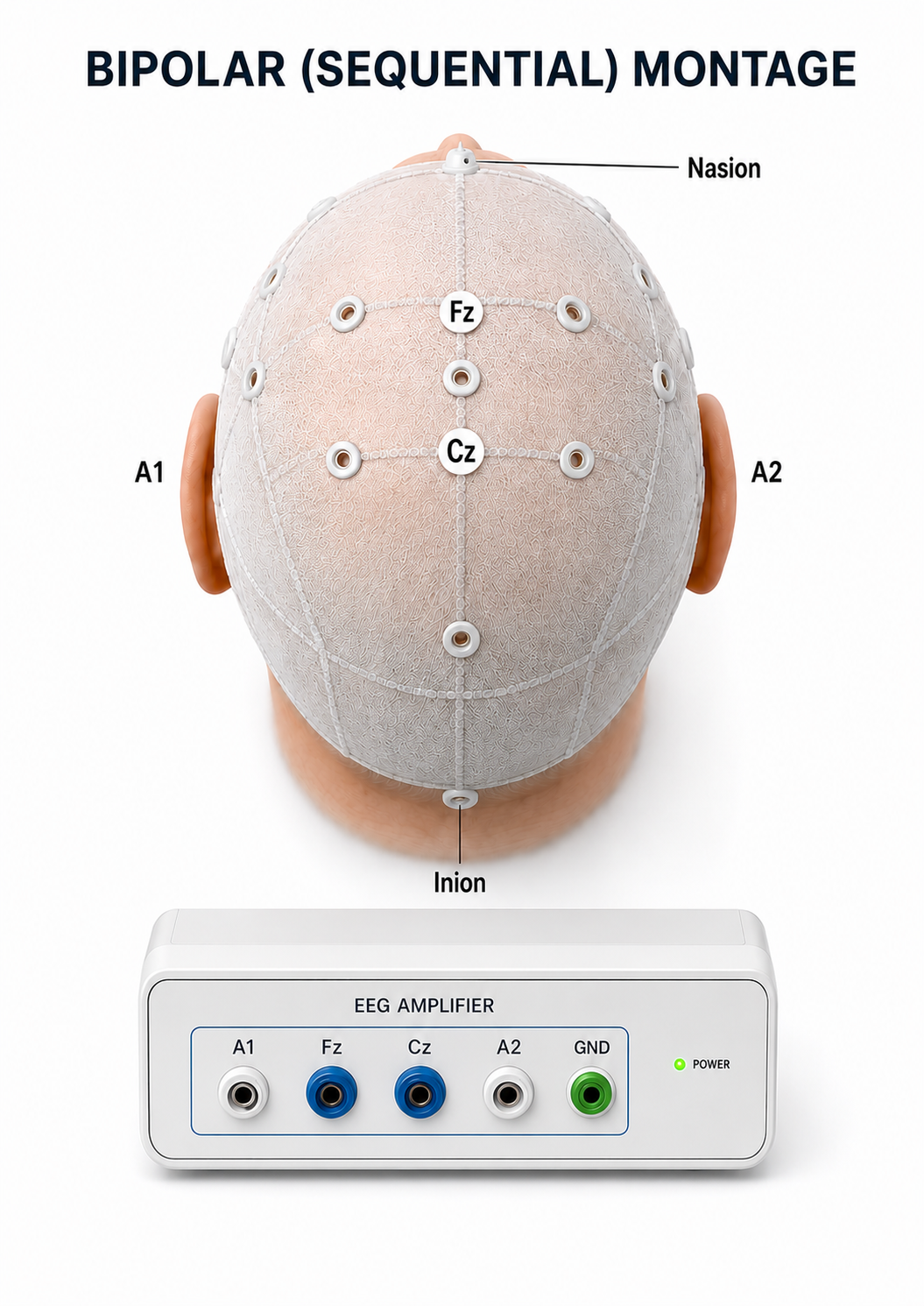
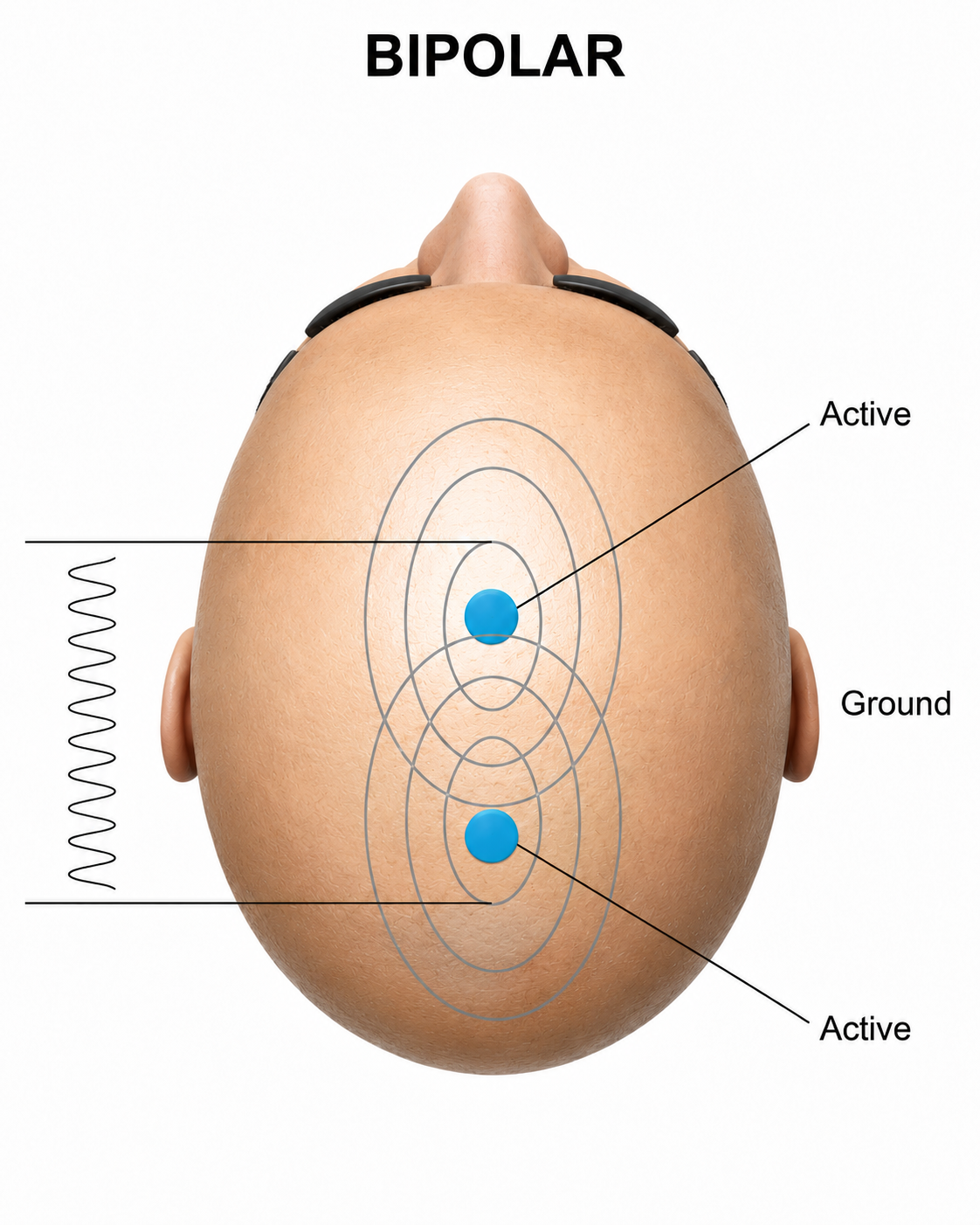
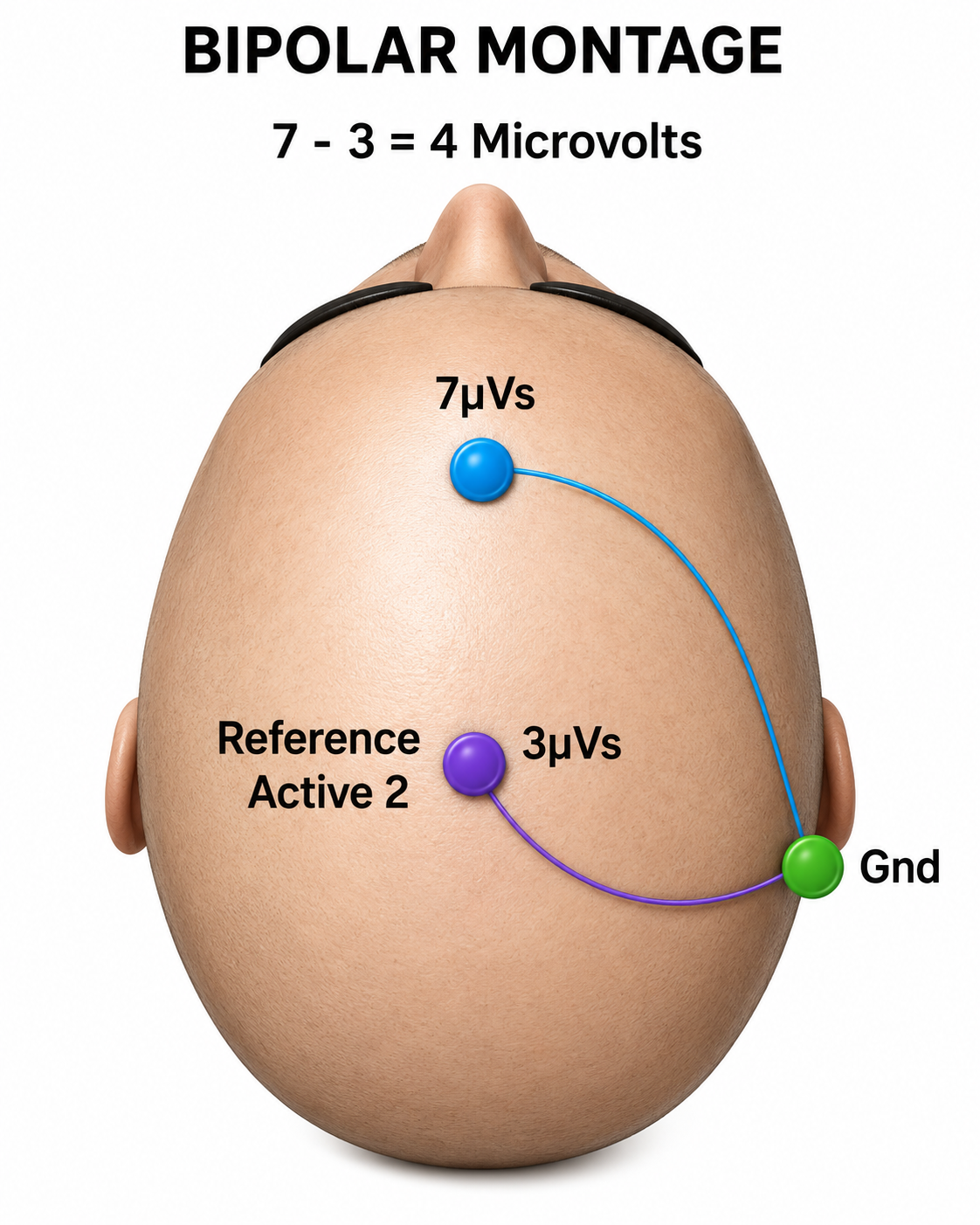
We adapted this graphic from John Demos' BCIA-recommended Getting Started with EEG Neurofeedback (2nd ed.). In the diagram on the right, the active "sees" 7 microvolts while the reference "sees" 3 microvolts. A differential amplifier subtracts these voltages, leaving 4 microvolts.
When 19 channels are used, this montage presents electrode pairs shown in sequence. Note that only the black cable for the ground has an ear clip in the photograph below. As a single channel, this montage does not localize EEG activity well because it shows only the difference between the A and R signals. However, when used as part of a 19-channel assessment, it excels at localizing EEG events related to epilepsy and can reduce artifacts when the A and R electrodes are relatively close together.
A sequential montage is frequently used in neurofeedback, where it trains the difference between EEG activity at the A and R electrodes. One important caveat: when training produces a change, it remains uncertain whether the change occurred at the A electrode, the R electrode, or both. The two signals are generally more similar when sensors are closer together and less similar when they are farther apart (e.g., Fp1-O2). When the two electrodes record nearly the same potential—as homologous frontopolar sites such as Fp1 and Fp2 often do—this montage may cancel genuine EEG activity along with the noise, a phenomenon sometimes called in-phase cancellation.
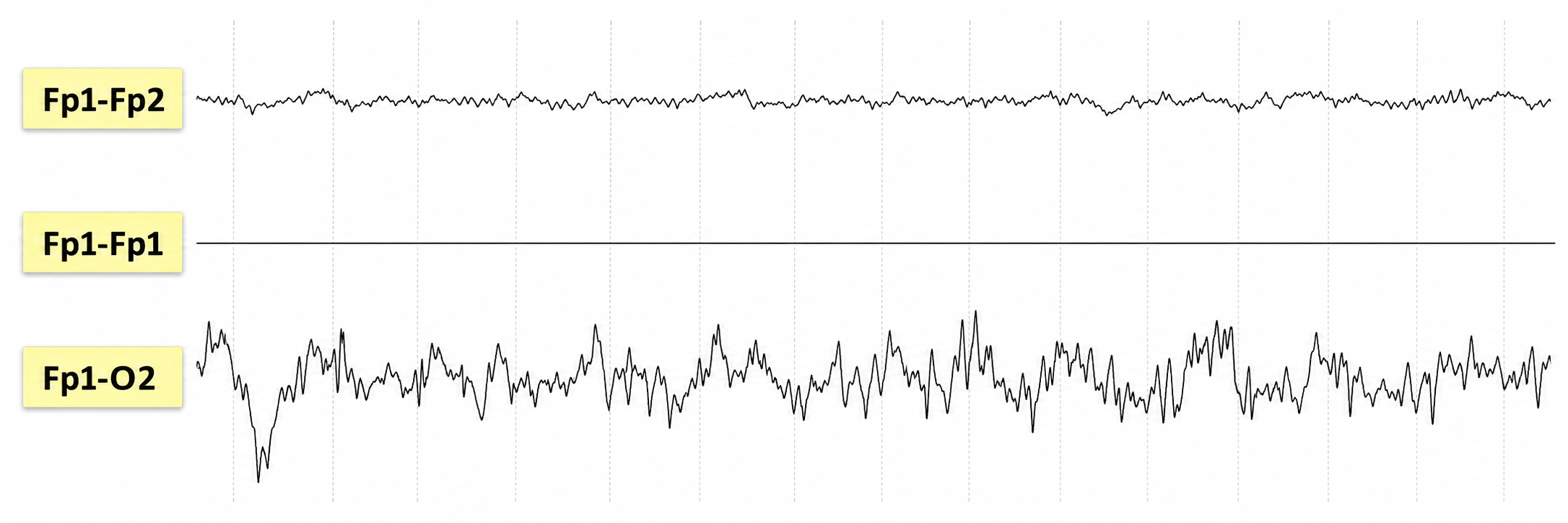
Graphic © John S. Anderson. Fp1–Fp2: low-amplitude, irregular mixed-frequency activity with no major frontal polar voltage difference. Fp1–Fp1: flat/isoelectric tracing, as expected because the same electrode is compared with itself. Fp1–O2: much higher-amplitude irregular slow activity, maximal in this wide anterior–posterior derivation; this suggests a large voltage gradient between Fp1 and O2.
Montages for 21 Recording Electrodes
All montages compare EEG activity between one or more pairs of electrode sites.
Listen to Lecture: Signal Acquisition (Montages)
This section examines the major montage configurations used in clinical EEG with 21 recording electrodes. The choice of montage does not alter the raw cortical electrical activity itself but rather filters, enhances, or diminishes specific aspects of it based on the spatial relationship between electrodes and the brain's dipolar sources, the electrical fields that produce opposing voltages detectable at the scalp. A montage defines how each EEG channel is constructed by determining which electrodes are compared to each other.
Broadly, montages fall into two categories. In a bipolar montage, each channel represents the voltage difference between two adjacent or anatomically aligned electrodes, emphasizing local voltage gradients. This configuration is especially useful for identifying focal abnormalities, such as epileptiform discharges, through phase reversals, points where waveform polarity inverts along a chain of electrodes, indicating the likely location of maximal voltage. The longitudinal bipolar ("double banana") montage arranges channels along the anterior-posterior axis, while the transverse montage organizes them across the coronal plane from left to right.
In contrast, a referential montage displays the voltage at each active electrode relative to a common reference point, which may be a single electrode, a pair of electrodes, or a mathematically computed value like the average of all electrodes. Referential montages are particularly suited for assessing global brain activity, hemispheric asymmetries, and background rhythms. Examples include the average reference, Cz reference, and linked ears montages. The Laplacian montage is often grouped with the referential montages because each electrode is compared to a computed value—a weighted average of its immediate neighbors—but it is more accurately described as a spatial filter, since it has no common reference site at all.
The sections that follow examine the structure, clinical utility, and interpretive implications of each montage. By understanding the distinction between bipolar and referential configurations, you can select the most appropriate montage for a given diagnostic question and use re-montaging, applying multiple montages to the same data set, for more comprehensive analysis.
Longitudinal Bipolar Montage
The longitudinal bipolar (double banana) montage is one of the most widely used configurations in clinical electroencephalography. It consists of bipolar derivations arranged in parallel chains, linking electrodes from the frontal to the occipital poles along the midline and lateral scalp. For example, one left-hemisphere chain includes the derivations Fp1-F3, F3-C3, C3-P3, and P3-O1, with a mirror chain on the right: Fp2-F4, F4-C4, C4-P4, and P4-O2.
Recording
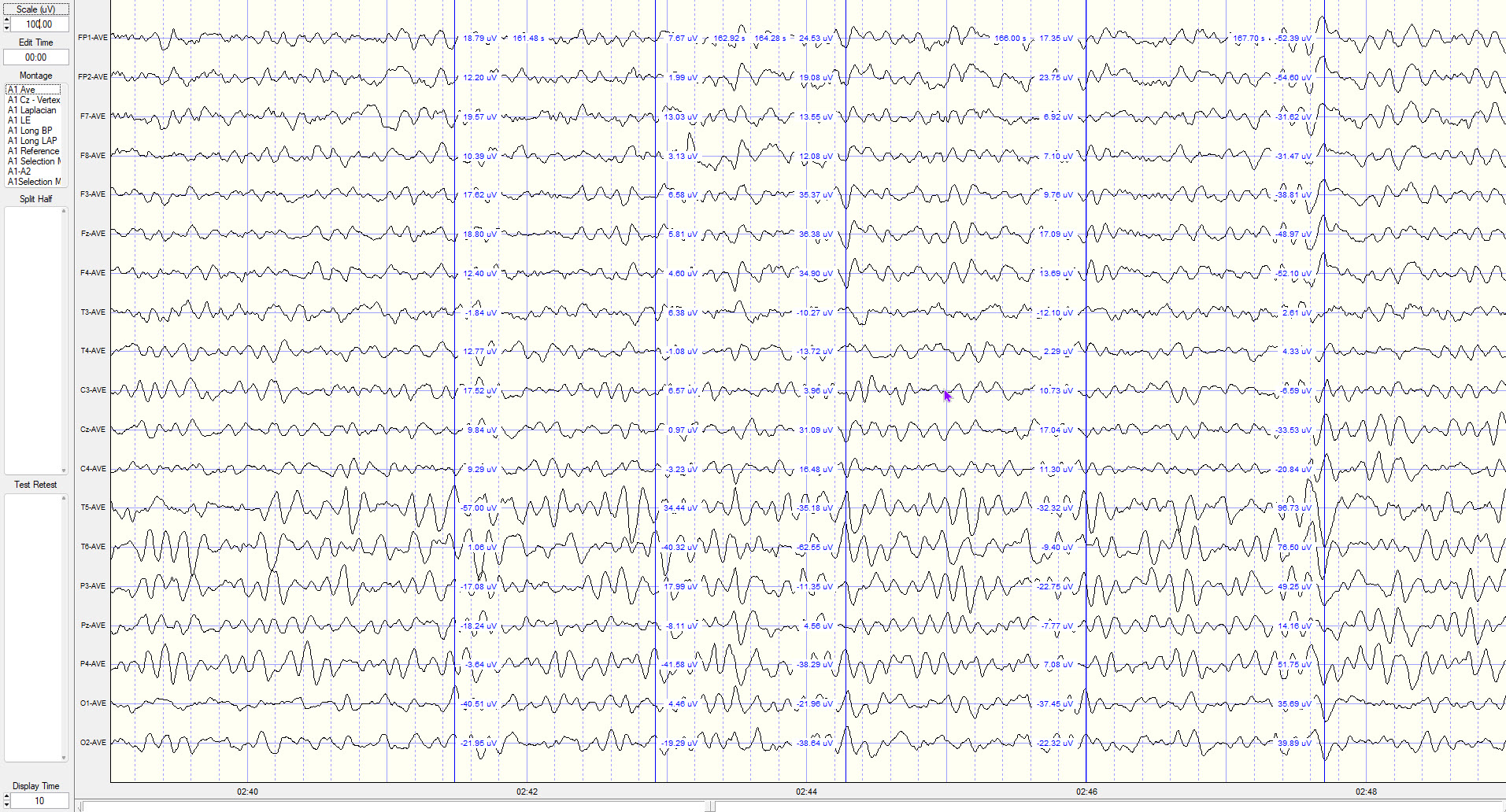
The images below show the same sample of EEG with different montages.
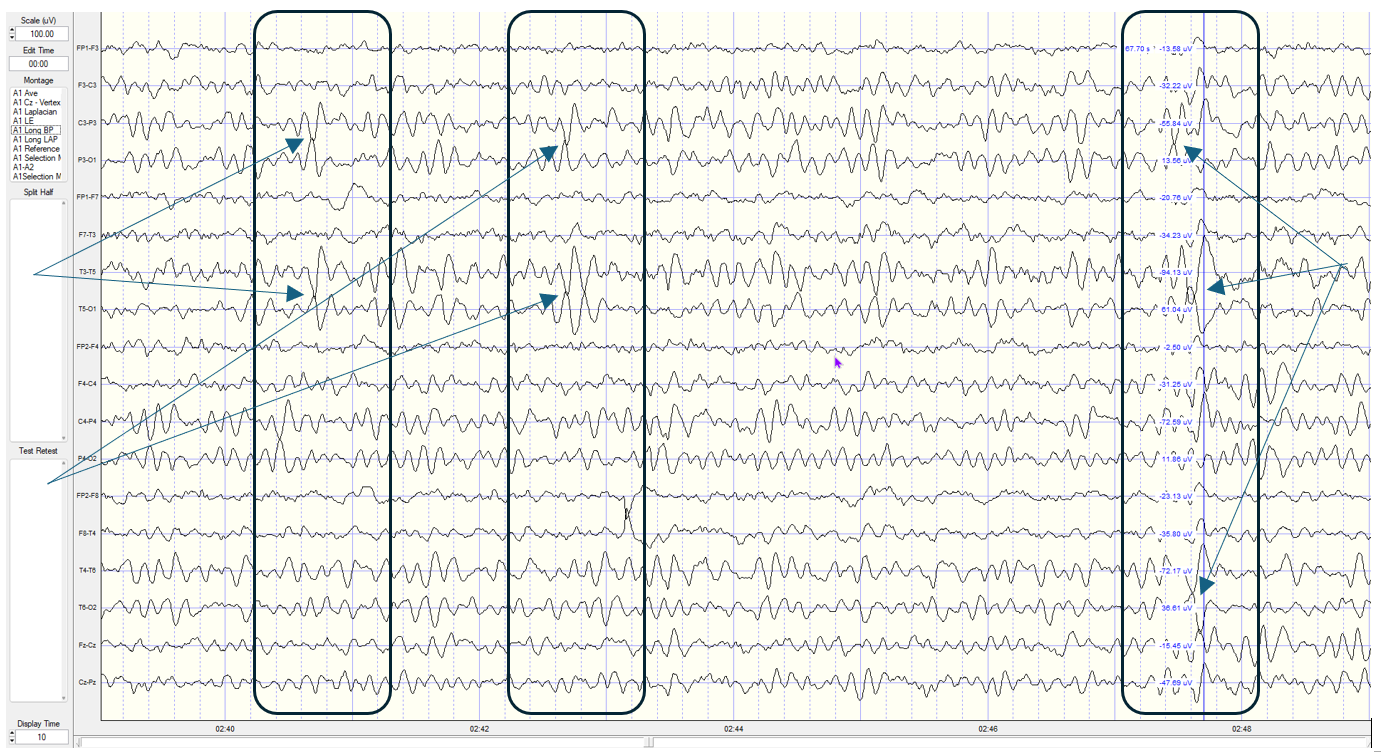
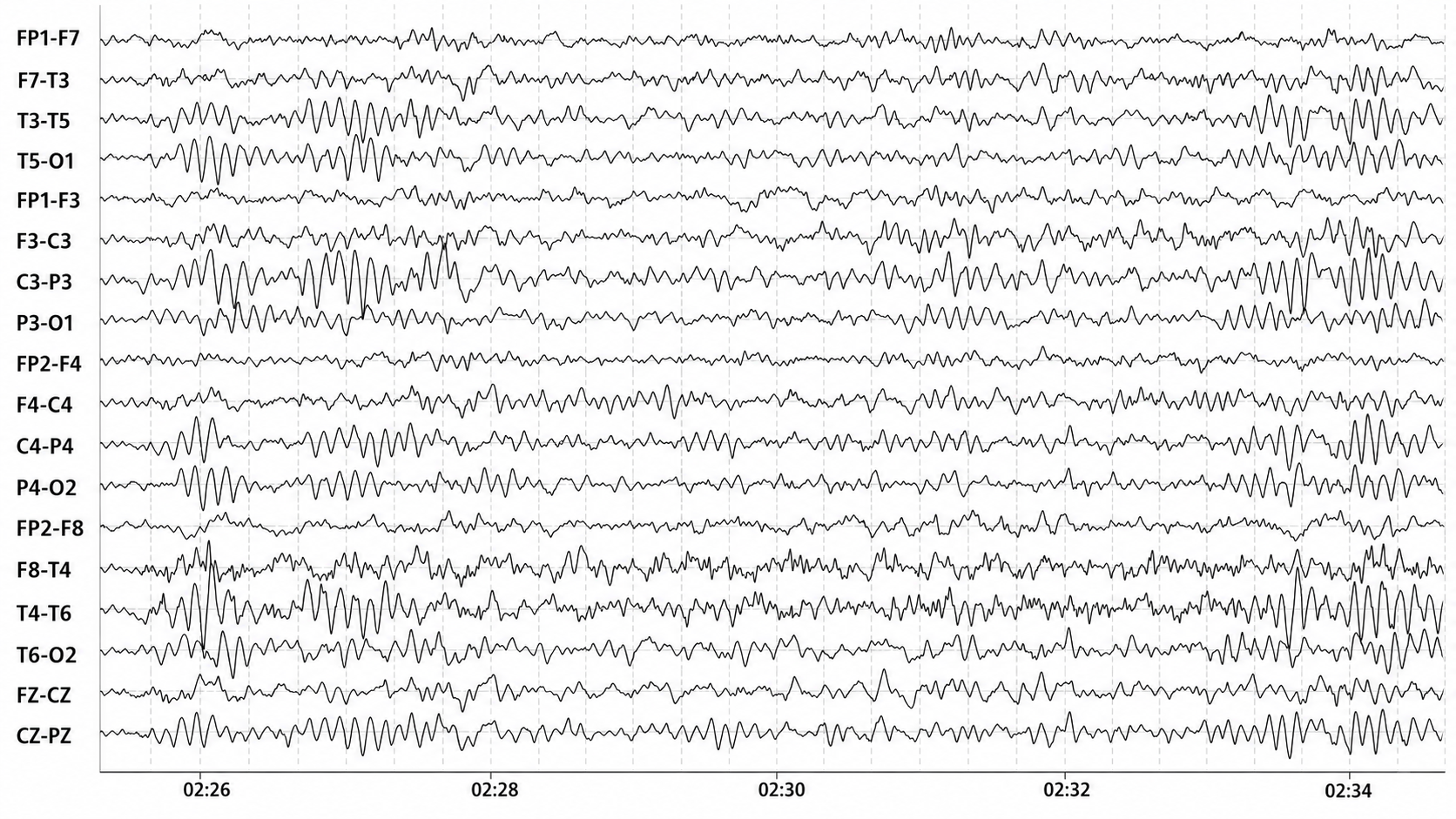
Longitudinal Bipolar Montage (Long BP) — Scale: 100 µV — 13-year-old male. The boxes mark sections of the recording where the phase reversals are clearest, and the arrows indicate the phase reversals themselves. This is a sequential montage—the longitudinal bipolar montage—in which a chain of electrode pairs is compared in order. Note that the first pairs, beginning with Fp1–F3 and followed by F3–C3, do not show the very high-amplitude 6 Hz activity (between 75 and 100 µV) that appears in the C3–P3 derivation and continues into the P3–O1 derivation. Observe that the waves in these two adjacent derivations point alternately toward and away from one another, indicating that the two are 180 degrees out of phase—that is, deflecting in opposite directions. This phase reversal locates the source of the high-amplitude activity beneath the electrode common to both derivations, in this case P3.
Below this, a second phase reversal appears between T3–T5 and T5–O1, localizing that source to T5. A similar but much lower-amplitude waveform is present at F3–C3 and F7–T3, reflecting a diminishing field in the derivations farther from the source.
Strengths
The primary strength of this montage is its capacity to reveal phase reversals, the inversion points of waveform polarity along the bipolar chain, which serve as a crucial diagnostic cue for localizing the maximum field of a focal discharge. This makes the montage particularly effective at detecting focal epileptiform activity organized along the sagittal plane (Niedermeyer & da Silva, 2005). The montage is also intuitive and standardized, which promotes consistent interpretation across clinical institutions.
Limitations
However, the longitudinal bipolar montage has notable limitations. Activity that is spatially generalized across adjacent electrode pairs may be attenuated or even canceled if it appears in phase across a chain. Activity oriented vertically or obliquely relative to the anteroposterior axis may also be poorly resolved due to the montage's directional bias. Additionally, this montage may be less sensitive to activity originating from deep cortical structures, such as mesial temporal regions.
Transverse Montage
The transverse (coronal bipolar) montage links electrodes across the coronal plane, from one hemisphere to the other. A typical frontal chain might include F7-F3-Fz-F4-F8, followed by T3-C3-Cz-C4-T4 at the central level, and T5-P3-Pz-P4-T6 through the parietal and temporal regions. This left-to-right orientation complements the front-to-back view of the longitudinal bipolar montage.
Recording

Transverse Bipolar Montage (Trans BP) — Here the phase reversals are less well defined, because this source is best revealed in the anterior–posterior derivations of the longitudinal bipolar montage. Overall power is also lower: each channel displays the difference between its two electrodes, and in this transverse montage the side-to-side differences are smaller than those along the anterior–posterior derivations.
Strengths
The transverse montage is especially valuable when lateralization is of clinical concern. It is often used alongside the longitudinal bipolar montage in epilepsy evaluations, as it can reveal whether a discharge is restricted to one hemisphere, crosses the midline, or is more pronounced on a particular side. This configuration is also well-suited for highlighting hemispheric asymmetries in background rhythm and interictal epileptiform activity.
Limitations
This montage is less commonly used, which means it may require greater interpretive skill and spatial visualization. The absence of anterior-posterior connections can obscure phase reversals along that axis, reducing effectiveness for localizing discharges from midline or parasagittal regions. The reliance on lateral electrodes also introduces greater sensitivity to artifact from facial and temporal muscle activity.
Average Reference Montage
The average reference montage takes a fundamentally different approach from bipolar configurations. Each active electrode is referenced to the arithmetic mean of all scalp electrode potentials, with the underlying assumption that the sum of all scalp-recorded potentials approximates zero, creating a theoretically neutral reference. Mathematically, the signal displayed for each electrode is recalculated as the difference between that electrode's voltage and the averaged signal from the full array.
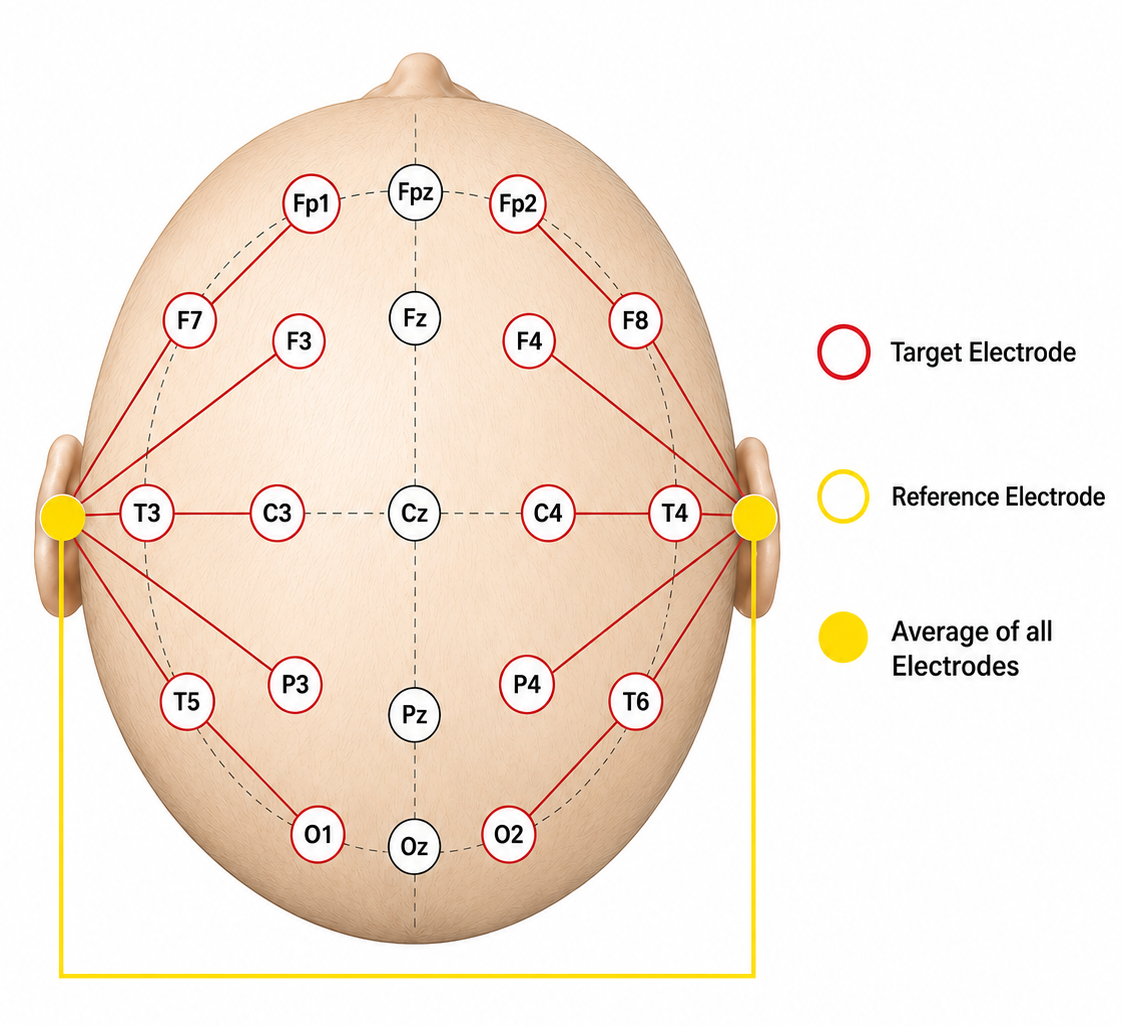
The image was adapted from López et al. (2016). In most cases, the midline electrodes are also included in these calculations.
Recording
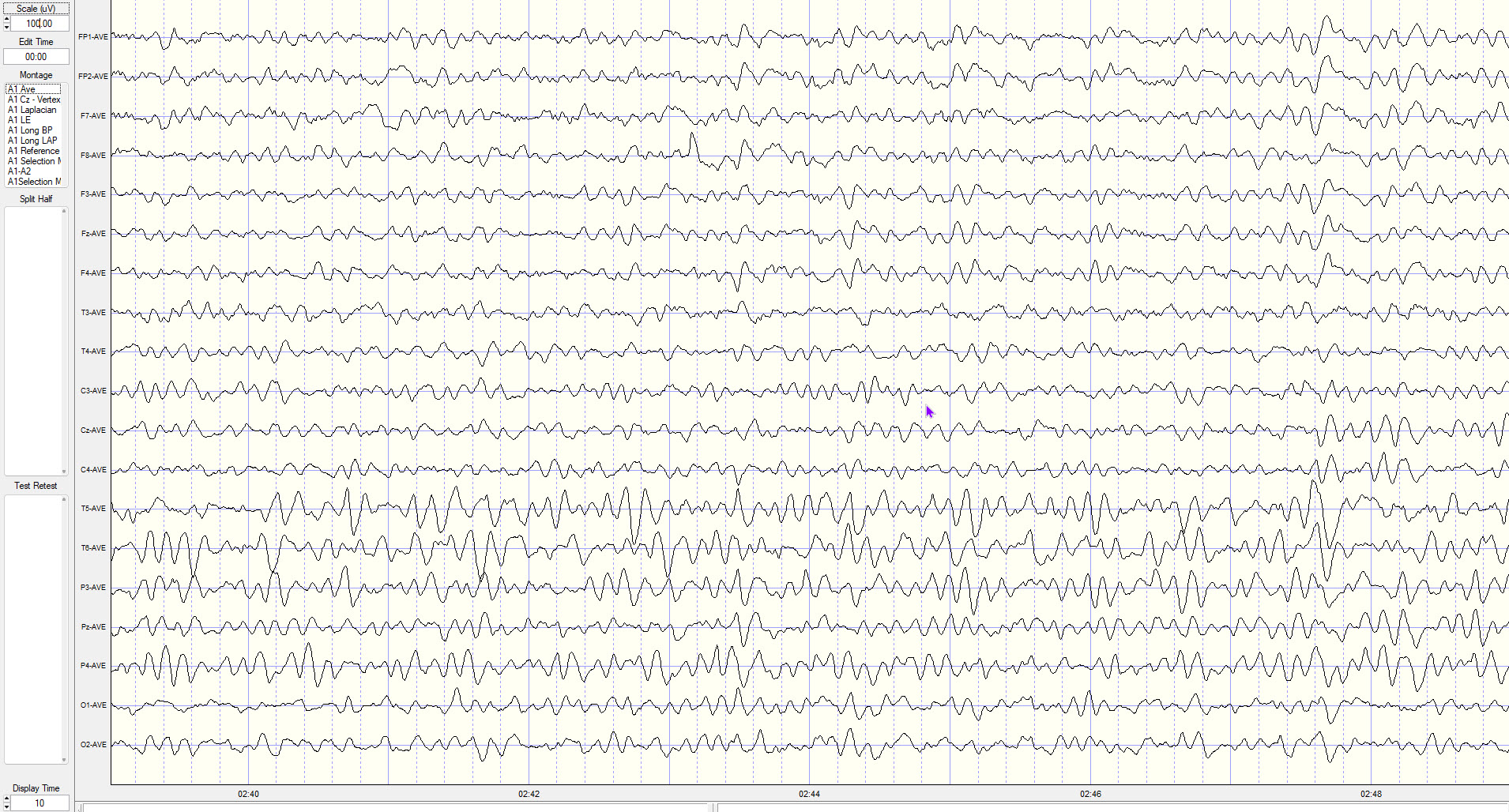
Average Reference Montage (Ave Ref) — This view shows clear anterior–posterior differences in location, along with reduced power compared with the longitudinal bipolar montage owing to the montage's averaging effect.
Strengths
The main advantage of this montage is that it replaces a single physical reference site—which is never electrically silent—with a computed, spatially distributed one, providing approximate spatial neutrality. It is not truly "reference-free"; the average itself is a reference, and its neutrality depends on the assumptions described above. It is particularly useful for visualizing diffuse, low-amplitude cerebral activity, including generalized spike-wave discharges, slow-wave abnormalities, and subtle background fluctuations. Because every electrode is displayed against the same computed reference, spatial comparisons across channels are more direct, making this montage highly valuable in qEEG and source localization studies (Fisch, 1999).
Limitations
However, this montage is highly susceptible to contamination by a single noisy electrode. If one electrode produces a high-amplitude artifact (from muscle activity or movement, for example), it shifts the computed average and distorts every channel in the display. The zero-sum assumption is also only approximately valid, and it degrades further when electrodes are unevenly distributed or confined to the upper head surface, as they are in the 10-20 array, or when cortical activity is spatially unbalanced (Nunez & Srinivasan, 2006).
Cz Reference Montage
The Cz reference montage is a referential (monopolar) configuration in which every scalp electrode is referenced to a single, fixed electrode at the vertex (Cz). This straightforward setup provides consistent spatial orientation for each channel and is used in event-related potential (ERP) research and in some pediatric recordings, where ease of interpretation and temporal clarity are priorities. Note that clinical sleep staging follows a different convention: the American Academy of Sleep Medicine specifies mastoid-referenced derivations (F4-M1, C4-M1, O2-M1), not a Cz reference.
We adapted this image from López et al. (2016). In most cases, the midline electrodes are also included in these calculations.
Recording
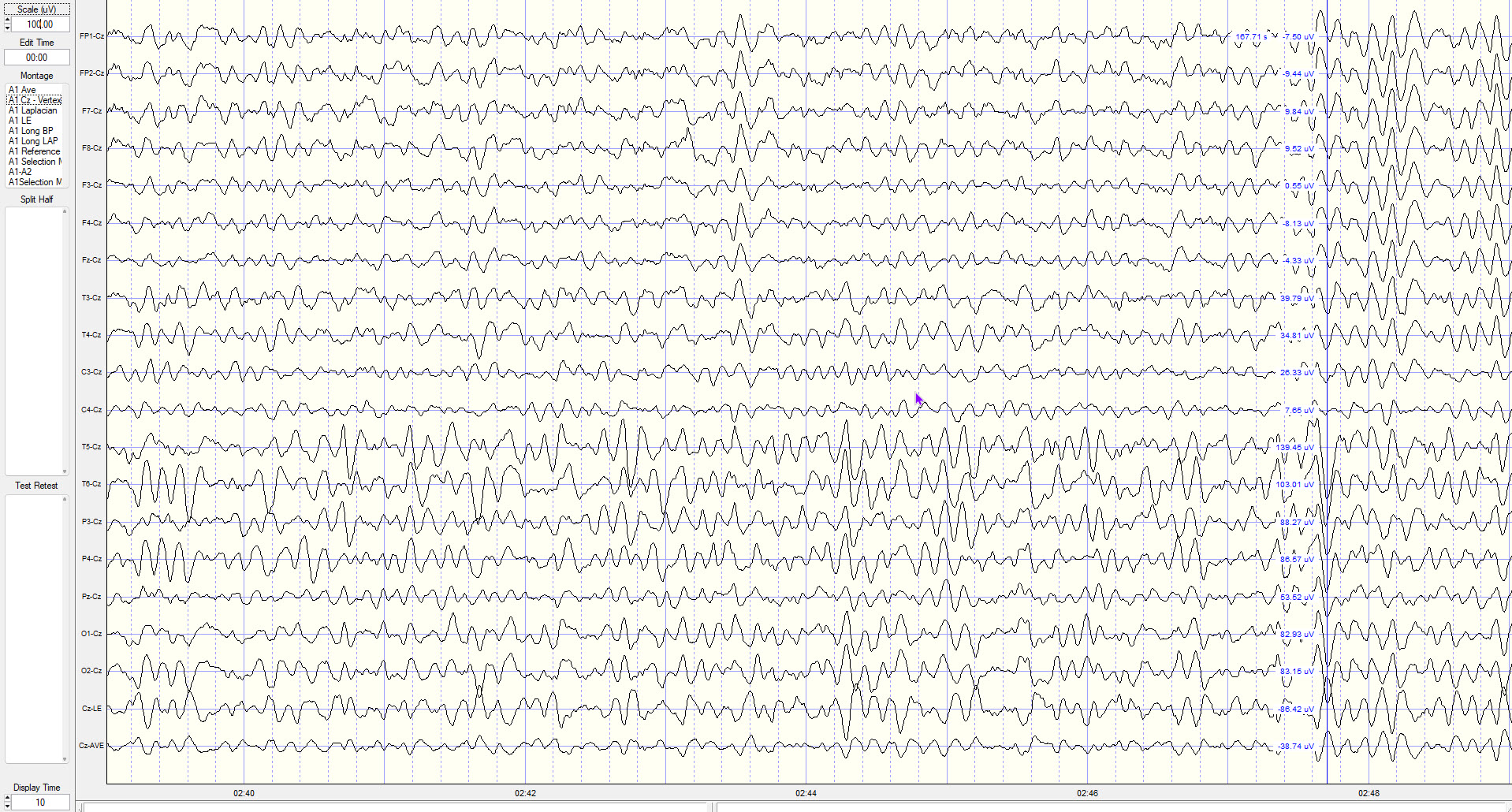
The Cz or Vertex Montage (Cz) also does not show phase reversals, since those are identified across adjacent electrode pairs. However, this montage shows larger voltage differences for electrode locations further from the Cz reference. This is particularly true for the T5 and T6 electrodes, which at the indicated point show 139.45 µV and 103.01 µV respectively. This illustrates differential amplification: what survives is whatever differs between the two inputs, while activity shared by both is rejected. The further an electrode is from a fixed reference like Cz, the less activity it shares with that reference and the more is retained.
Strengths
Because Cz is equidistant from both hemispheres, lateralized discharges produce strong voltage differences and clear waveforms. The fixed reference also facilitates temporal alignment of discharges, which is useful for assessing spike timing, propagation patterns, and hemispheric synchrony.
Limitations
Cz is a problematic reference for activity that originates near the vertex itself, such as discharges from the supplementary motor area, parasagittal cortex, or midline regions. When the reference is physically close to the source, the recorded potential difference may be minimal or absent, leading to false negatives. This limitation is particularly relevant when interpreting generalized or midline spike-wave complexes or high-frequency sleep spindles that originate near central sites (Niedermeyer & da Silva, 2005).
Linked Ears Reference (A1-A2 reference or LE) Montage
The linked ears reference montage references all scalp electrodes to the average of the left (A1) and right (A2) earlobe electrodes. These electrodes are presumed to be relatively inactive compared with cerebral sources, providing a convenient common baseline for assessing cortical activity. This montage has been widely used in routine clinical EEG and in quantitative EEG because of its simplicity and because most normative databases were collected with it (Niedermeyer & da Silva, 2005).
Two cautions apply. Physically shorting A1 and A2 together with a jumper lowers the impedance across the head and can shunt and distort genuine interhemispheric asymmetries; for this reason most modern systems compute the linked-ears reference mathematically as the average of the two separately recorded ear channels rather than wiring them together. And, as the recordings below illustrate, the ears are not silent, so the linked-ears reference introduces reference contamination into every channel.
Recording
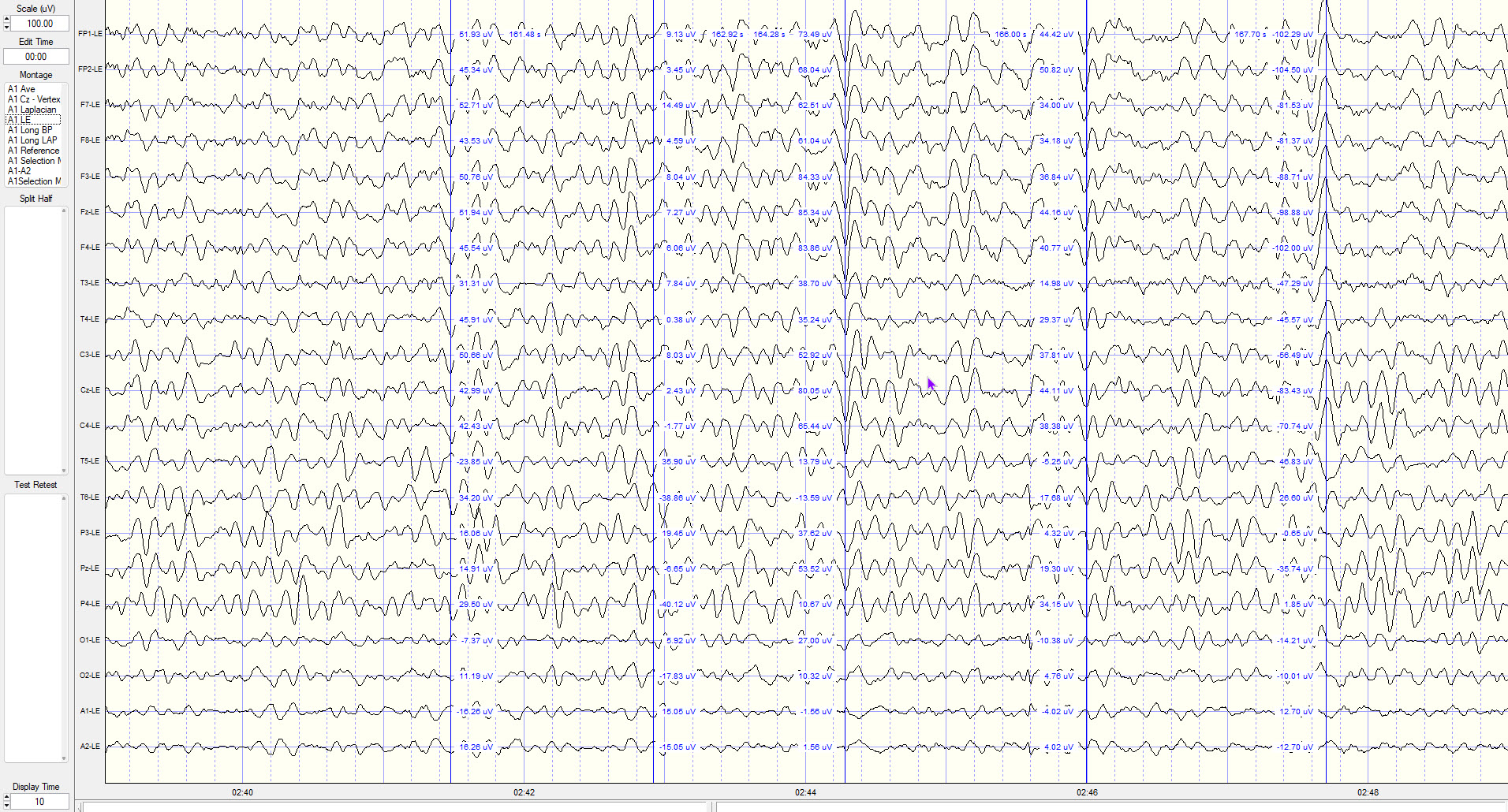
Linked Ears Montage – Scale 100uV, Display time 10 seconds. This montage shows significant synchronous activity due to reference contamination.
Notice the two reference tracings across the bottom of the image contain what appear to be EEG waveforms. These tracings represent the reference electrodes A1 and A2 (auricular left and right respectively) compared to the linked ears reference, which is the average of the two reference electrode channels: ChannelLE = channelraw − [(A1 + A2) ÷ 2].
Because the reference value is subtracted from every channel, any cerebral activity present in the ears is injected into all of them with inverted polarity. Where the scalp site carries little of that activity (mostly frontal), it appears added; where the scalp site already carries it (mostly parietal and occipital), it is partly cancelled. This is a consequence of differential subtraction, not of common-mode rejection working as intended.
Note in the image above that the prefrontal or frontal pole Fp1 and Fp2 electrodes have the highest amplitude and that O1 and O2 have the lowest. In the Average Reference Montage image below the posterior temporal, parietal and occipital sensors show the highest voltage while frontal, central and temporal show lower values.
In this Average Reference Montage image, the posterior temporal, parietal and occipital sensors show the highest voltage while frontal, central and temporal show lower values.
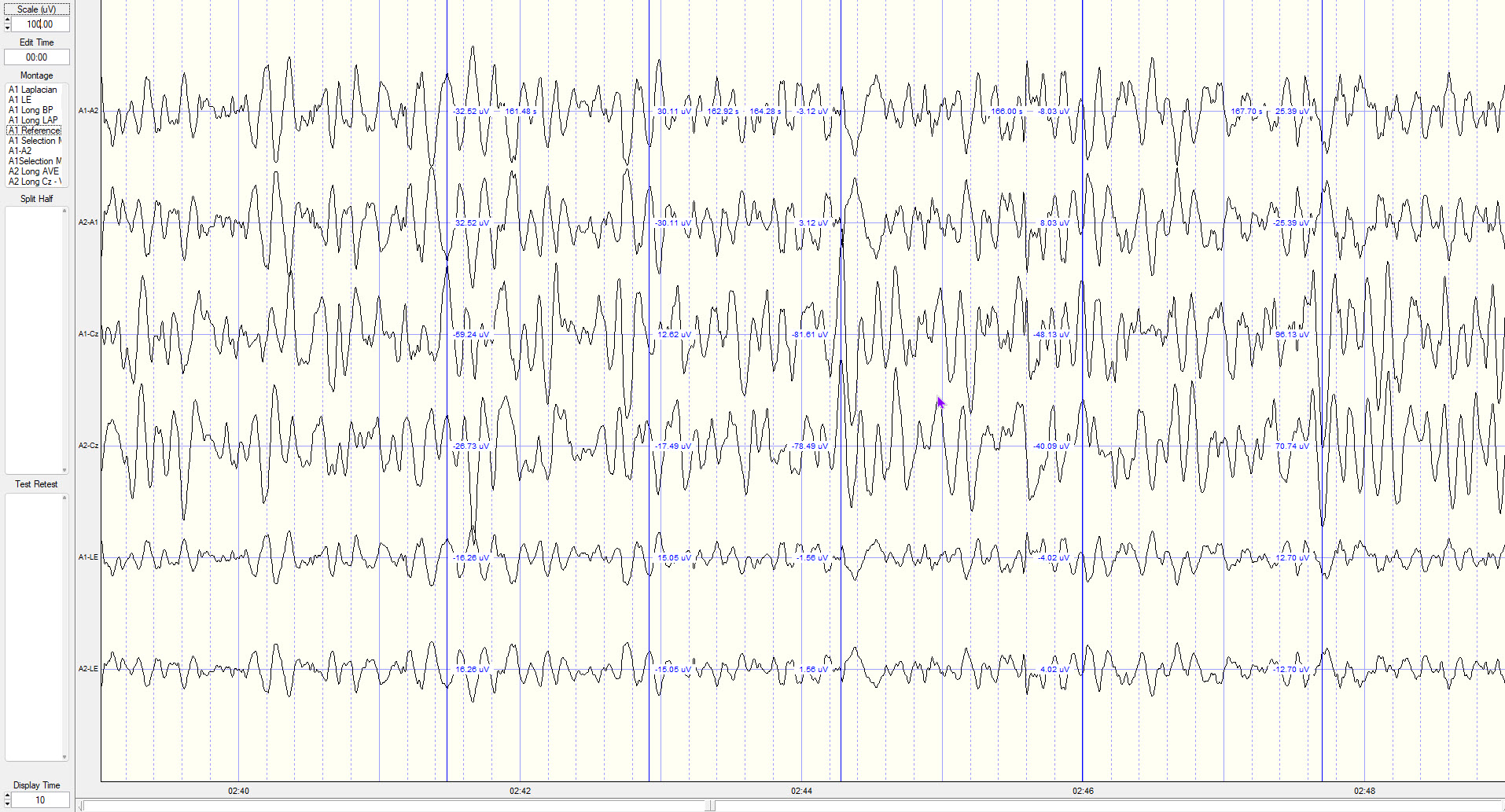
This is a created montage showing the ear references in differing combinations, e.g., A1-A2, A2-A1, A1-Cz, A2-Cz and finally A1-LE and A2-LE.
Note that the first two tracings have reverse polarity – the waves are waving in the opposite direction – as would be expected with that comparison. The initial blue vertical voltage indicator shows the first A1-A2 tracing with the right side A2 electrode as more electrically negative and the second voltage indicator for that same tracing shows the left side A1 electrode as more electrically negative. This shows the "alternating current" nature of the EEG recording.
The second two tracings show waveforms with some phase similarity but it appears from visual inspection that the voltage is somewhat higher on the left (A1-Cz).
The final two tracings show A1 and A2 compared to the average of the two electrode values and clearly show they are exactly opposite in phase as would be expected from the formula.
However, the bottom line is that the reference channels and the derivative LE linked ears channel contain EEG waveforms that will be propagated into every channel as noted above.
Strengths
The primary strength of the linked ears montage is its relative ease of interpretation and its ability to provide clear visualization of regional asymmetries. Because all electrodes share a common reference point, focal abnormalities such as interictal epileptiform discharges are often well-demarcated, especially when lateralized. Placing the reference off the scalp proper also avoids projecting vertex-region cerebral activity into every channel, as a Cz reference does, and it is the reference used by most qEEG normative databases (Nuwer, 1997).
Limitations
However, the assumption that the earlobes are electrically inactive is not valid. The ears routinely pick up cerebral activity—especially temporal and posterior activity, and particularly during high-amplitude discharges—which is then injected into the reference and, through the differential amplifier, into every channel (Gloor, 1985). Because the earlobes sit close to the temporalis and posterior neck muscles, they are also a common entry point for EMG contamination. Asymmetry in earlobe impedance or local artifact can produce lateralized distortions that mimic or obscure true cerebral asymmetries, and the reference may underrepresent midline or deep sources.
Laplacian Montage
The Laplacian montage enhances the localization of cortical activity by referencing each electrode to a weighted average of its surrounding electrodes. This approach approximates the second spatial derivative of the potential field, emphasizing signals originating directly beneath each electrode while attenuating distant or volume-conducted signals (Nunez & Srinivasan, 2006). Think of it as a spatial "sharpening filter" for EEG data.
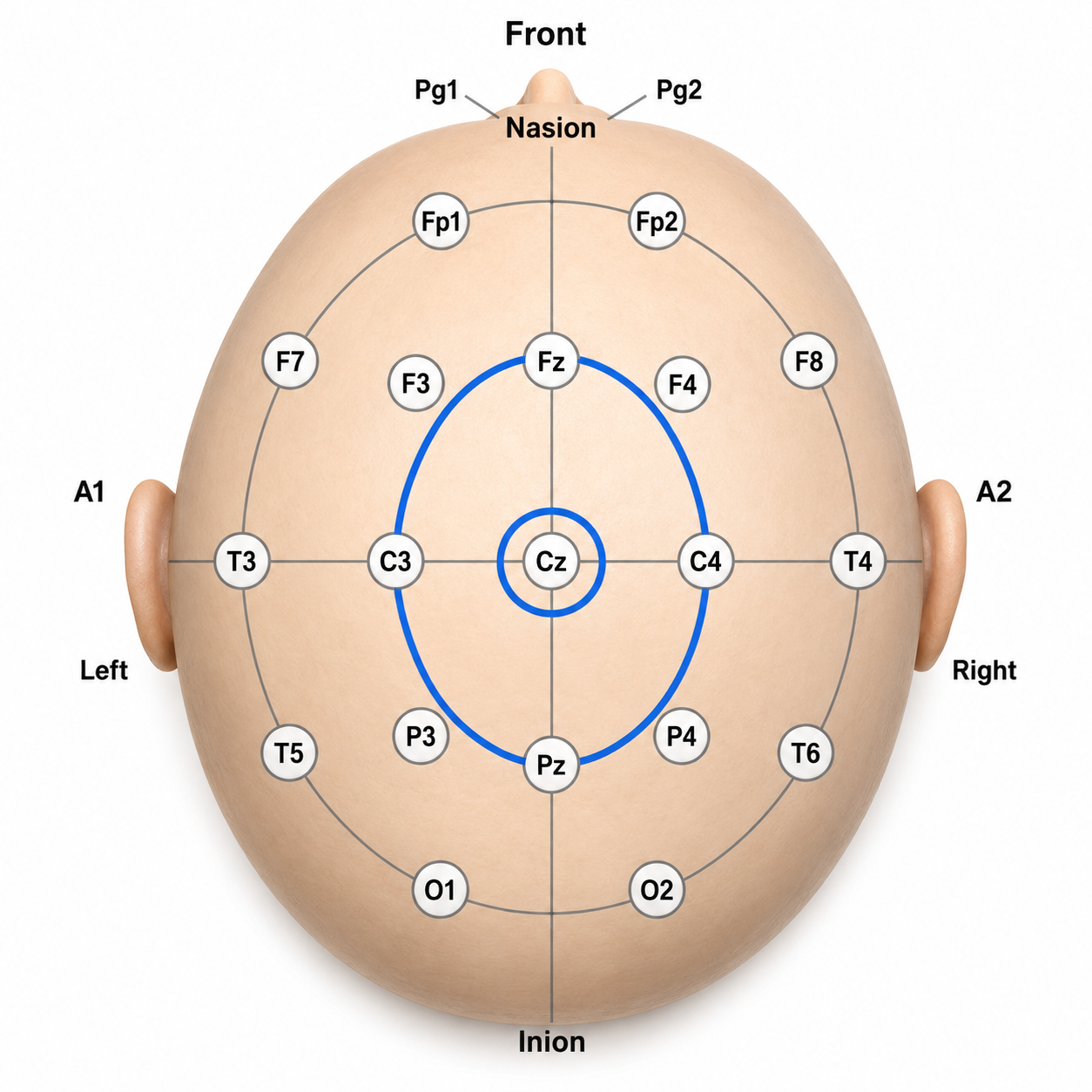
In a Laplacian montage, the signal at a target electrode is compared with the activity of surrounding electrodes to estimate local scalp potential and reduce broad, volume-conducted activity. The small blue circle around Cz identifies it as the central target electrode. The larger blue oval identifies the neighboring electrodes used as the surrounding reference field, chiefly Fz, C3, C4, and Pz. Cz is emphasized, while more diffuse activity shared across nearby electrodes is subtracted out. This makes focal central activity easier to see and helps improve spatial localization compared with a conventional referential montage.
Recording
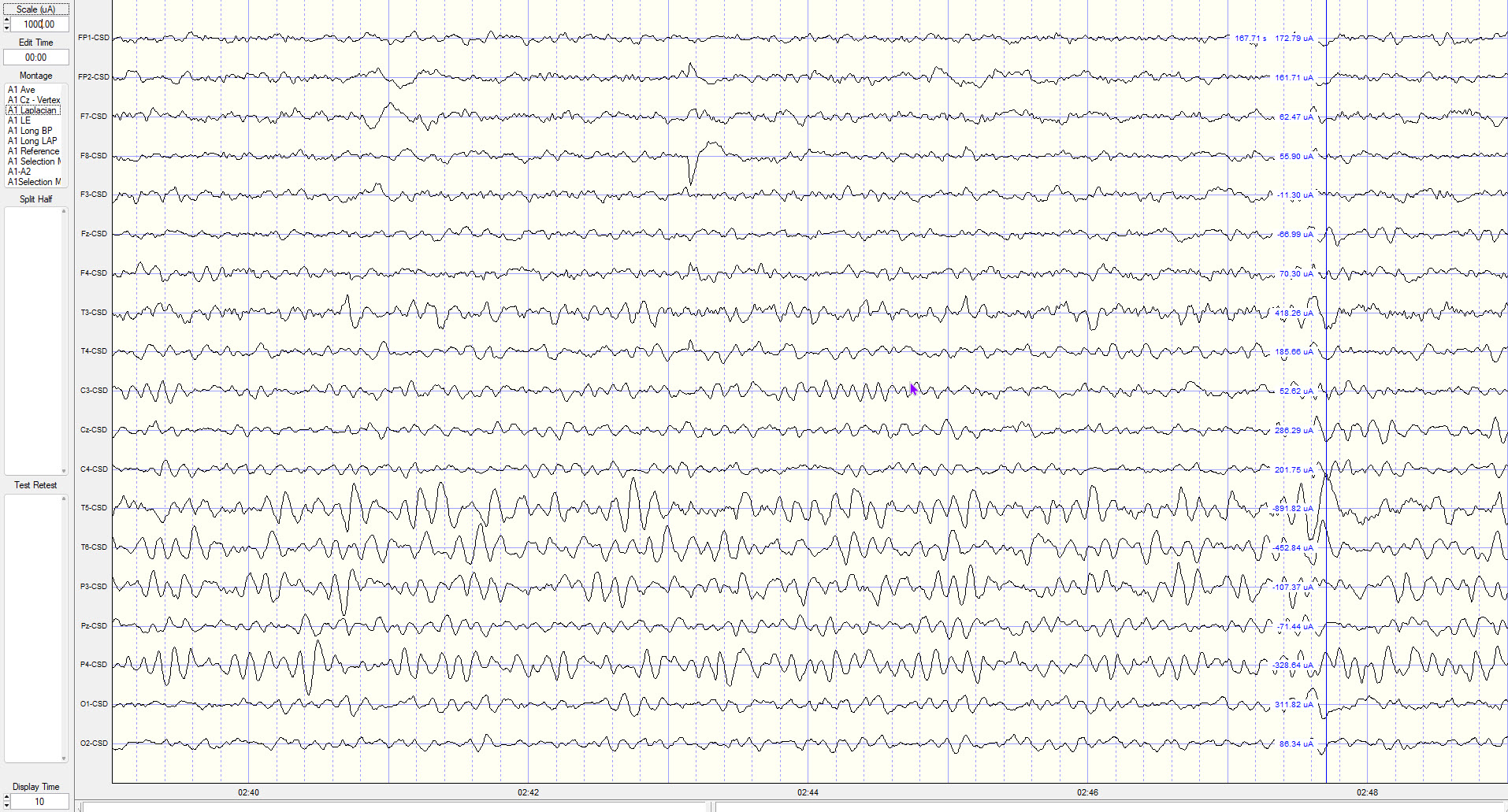
The Laplacian Montage (LAP) displays an estimate of current source density (CSD) rather than voltage. Strictly speaking, the surface Laplacian has units of potential per unit area (commonly µV/cm²); some software labels the axis in current units such as µA, which should be read as a software convention rather than a literal current measurement. This montage, too, does not show phase reversals in the conventional sense.
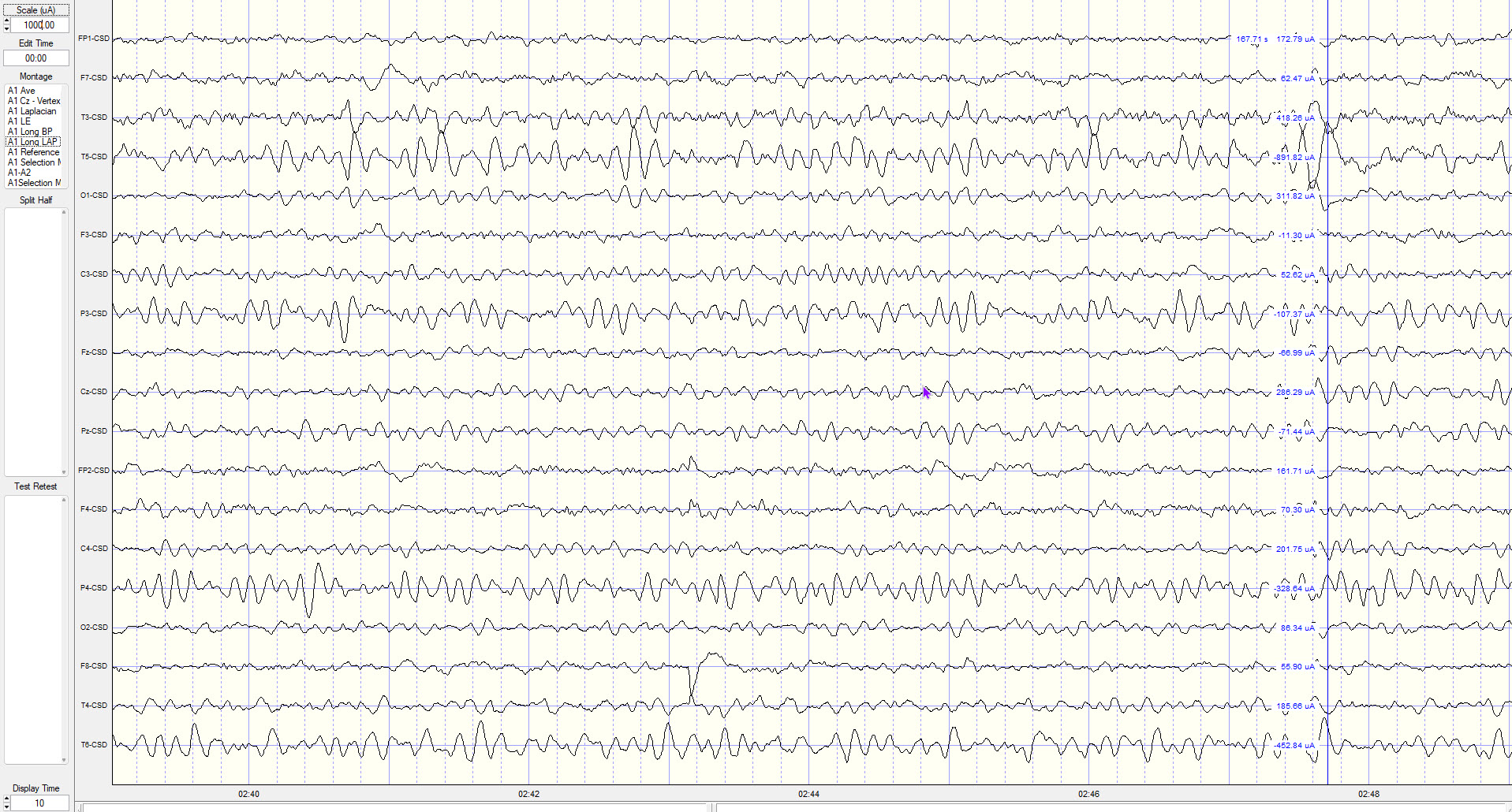
However, in this non-traditional view that applies an anterior–posterior electrode-chain approach similar to the Long BP montage, comparable phase-reversal information appears to be present—between T3-CSD and T5-CSD, and between T5-CSD and O1-CSD.
Strengths
The Laplacian montage offers significant advantages for localizing focal cortical activity with high spatial precision. Unlike referential montages that rely on ear or mastoid electrodes, this configuration excludes distant references, minimizing the risk of artifact from electrically active or asymmetrically placed reference sites. It is particularly effective for detecting focal epileptiform discharges, localized slowing, and sensorimotor rhythms, especially when applied in high-density EEG systems (McFarland et al., 1997). While not typically used as a primary montage, it serves as a valuable supplementary tool for refining diagnostic accuracy in complex cases.
Limitations
The Laplacian montage's accuracy depends on high-density, evenly spaced electrode arrays, making it less reliable in standard low-density systems like the 10-20 configuration. A key concern is the edge effect: electrodes at the scalp periphery (such as Fp1, Fp2, F7, F8, O1, and O2) lack surrounding electrodes on all sides, reducing the precision of spatial averaging in these regions. Additionally, the spatial filtering inherent to this method attenuates slow or widespread activity, limiting its sensitivity to generalized abnormalities such as diffuse slowing or generalized spike-wave discharges (Gordon & Rzempoluck, 2004; Srinivasan et al., 1996).
Montage Selection Strategy
When viewing the EEG, your goal is to identify areas that deviate from typical patterns, correlate those differences with client symptoms, and design training protocols to address them. Each montage reveals different aspects of the same data. The longitudinal bipolar and transverse montages are most effective at demonstrating focal abnormalities, with clear localization, polarity, and sharp morphology, making them essential for identifying epileptiform discharges and mapping their spatial distribution.
The average reference montage, while less sensitive to focal events, contributes significantly to assessing hemispheric symmetry and background rhythm integrity, particularly in diffuse or generalized processes. The Cz reference montage provides a reliable lateralized perspective for differentiating left versus right hemispheric activity, though it lacks optimal resolution for midline sources. The linked ears reference offers consistency in visualizing lateralized abnormalities but can introduce asymmetry and contamination, especially with poor electrode impedance.
The Laplacian montage offers superior spatial resolution for identifying focal cortical sources by emphasizing activity local to each electrode and suppressing distant or volume-conducted activity. Understanding the comparative strengths and limitations of each montage enables more nuanced and precise interpretation of EEG findings, enhancing diagnostic accuracy and supporting informed clinical decision-making.
Re-Montaging
In clinical electroencephalography, the montage used to display data fundamentally shapes how brain activity is visualized and interpreted. An essential feature of modern digital EEG is that clinicians are not limited to a single display: they can apply different montages to the same epoch of data. This process, known as re-montaging, allows for a more complete understanding of the recorded activity.
Modern EEG visualization software also allows clinicians to create custom montages that highlight selected electrodes, use alternative electrode arrangements, or follow non-standard sequences. For example, grouping all frontal electrodes at the top of the page makes eye artifact easier to identify, while grouping temporal electrodes together facilitates EMG artifact detection.
The narrated video below © John S. Anderson displays the same 21-channel recording viewed using different montages with a 60-Hz notch filter on and off.
Re-montaging enables clinicians to re-express the same underlying electrical signals in different spatial contexts. A spike that shows a clear phase reversal in a longitudinal bipolar montage may appear attenuated in an average reference montage. Conversely, a sharply contoured waveform seen in a bipolar montage can be cross-checked in a referential montage to determine whether it reflects true cortical activity or a muscle artifact. This comparative approach is essential for avoiding misinterpretation, particularly when benign variants or technical artifacts could be mistaken for pathologic activity.
Re-montaging also improves localization. By switching between longitudinal and transverse configurations, you can more precisely triangulate the source of epileptiform discharges and determine whether a waveform is confined to one hemisphere or crosses the midline. In suspected encephalopathy, re-montaging into an average reference montage may better demonstrate diffuse slowing or triphasic waves. Following the average reference, the Laplacian montage can help zero in on areas of interest, while the linked ears montage should be consulted to identify likely reference contamination affecting downstream evaluations such as topographic z-score maps, coherence, and network analyses.
Digital EEG systems have made re-montaging straightforward and immediate. The American Clinical Neurophysiology Society recommends the use of both bipolar and referential montages and encourages at least 16 recording channels with the full complement of 10-20 system electrodes. When you identify an EEG feature, such as slowed alpha, elevated frontal theta, excess fast activity, or an atypical alpha response, in one montage, always verify and validate that finding using additional montages.
Use Consistent Settings
One important consideration for viewing the EEG is to use consistent display settings. In clinical EEG, the conventional standards are a sensitivity of 7 μV/mm and a "chart speed" of 30 mm per second; neurofeedback software often expresses the vertical axis instead as a fixed scale marker, commonly 50 or 100 μV. In the era of paper recording, tracings were drawn by pens on moving chart paper at 30 mm/s for routine adult and pediatric recordings, with slower speeds such as 15 mm/s used for neonatal and sleep studies. Modern digital systems replicate this format so that waveforms appear consistently the same each time they are viewed and can be compared to reference sources.
Most modern EEG software expresses display time in seconds rather than chart speed equivalents. At 30 mm/s, a standard page corresponds to 10 seconds of data, which is the setting to select in programs such as NeuroGuide; note that in some display modes the vertical scale adjusts automatically to the highest voltage in the recording, which will change the apparent amplitude from page to page unless it is fixed.
Best Practices from the American Clinical Neurophysiology Society Guideline 3 (2016)
The Committee reaffirms the statements pertaining to montages set forth previously in the Guidelines of the American Clinical Neurophysiology Society (ACNS) and that are paraphrased as follows:
(a) that no less than 16 channels of simultaneous recording be used, and that a larger number of channels be encouraged,
(b) that the full 21 electrode placements of the 10-20 system be used,
(c) that both bipolar and referential montages be used for clinical interpretation,
(d) that the electrode derivations of each channel be clearly identified at the beginning of each montage,
(e) that the pattern of electrode connections be made as simple as possible, and that montages should be easily comprehended,
(f) that the electrode pairs (bipolar) preferentially should run in straight (unbroken) lines and the interelectrode distances kept equal,
(g) that tracings from the more anterior electrodes be placed above those from the more posterior electrodes on the recording page, and,
(h) that it is very desirable to have some of the montages comparable for all EEG laboratories.
2.2 The Committee recommends a "left above right" order of derivations, i.e., on the recording page, left-sided leads should be placed above right-sided leads for either alternating pairs of derivations or blocks of derivations. This recommendation coincides with the prevailing practice of most EEG laboratories, at least in North America and in many other areas.
Recognizing and Correcting Signals of Noncerebral Origin
This section covers one of the most practical skills in clinical EEG: recognizing and managing artifacts. EEG artifacts are noncerebral electrical signals that contaminate the recording. They fall into two broad categories. Physiological artifacts originate from the body and include electromyographic (muscle), electro-ocular (eye blink and movement), cardiac (pulse), sweat (skin impedance), drowsiness, and evoked potential artifacts. Exogenous artifacts come from external sources and include movement, 60 Hz and field effect, and electrode-related (impedance, bridging, and electrode pop) artifacts.
Listen to Lecture: Signal Acquisition (Part 2)
The movie features a 19-channel BioTrace+ /NeXus-32 display of EEG artifacts © Mary Tracy.
Electromyographic (EMG) Artifact
EMG artifact is interference in EEG recording caused by volume-conducted signals from skeletal muscles. This artifact appears as a high-frequency "buzz" during muscle contraction and shows up as elevated beta and gamma activity in the qEEG. Surface EMG power is distributed across roughly 20 to 500 Hz, with most of the energy concentrated between about 50 and 150 Hz. Critically, the low end of that distribution overlaps the EEG beta band, so EMG cannot be separated from cerebral fast activity by frequency alone.
The graphic below shows how the choice of high-frequency filter (HFF), a filter that attenuates frequencies above a specified cutoff, affects contamination by this artifact. All channels on the left side of the tracing show EMG artifact admitted by a 55-Hz high-frequency filter. The right tracing appears clean because its 15-Hz filter attenuates the higher frequencies where most of this artifact resides. Note that filtering changes only the appearance of the tracing; the contamination remains in the underlying data and will still affect quantitative measures computed from it.
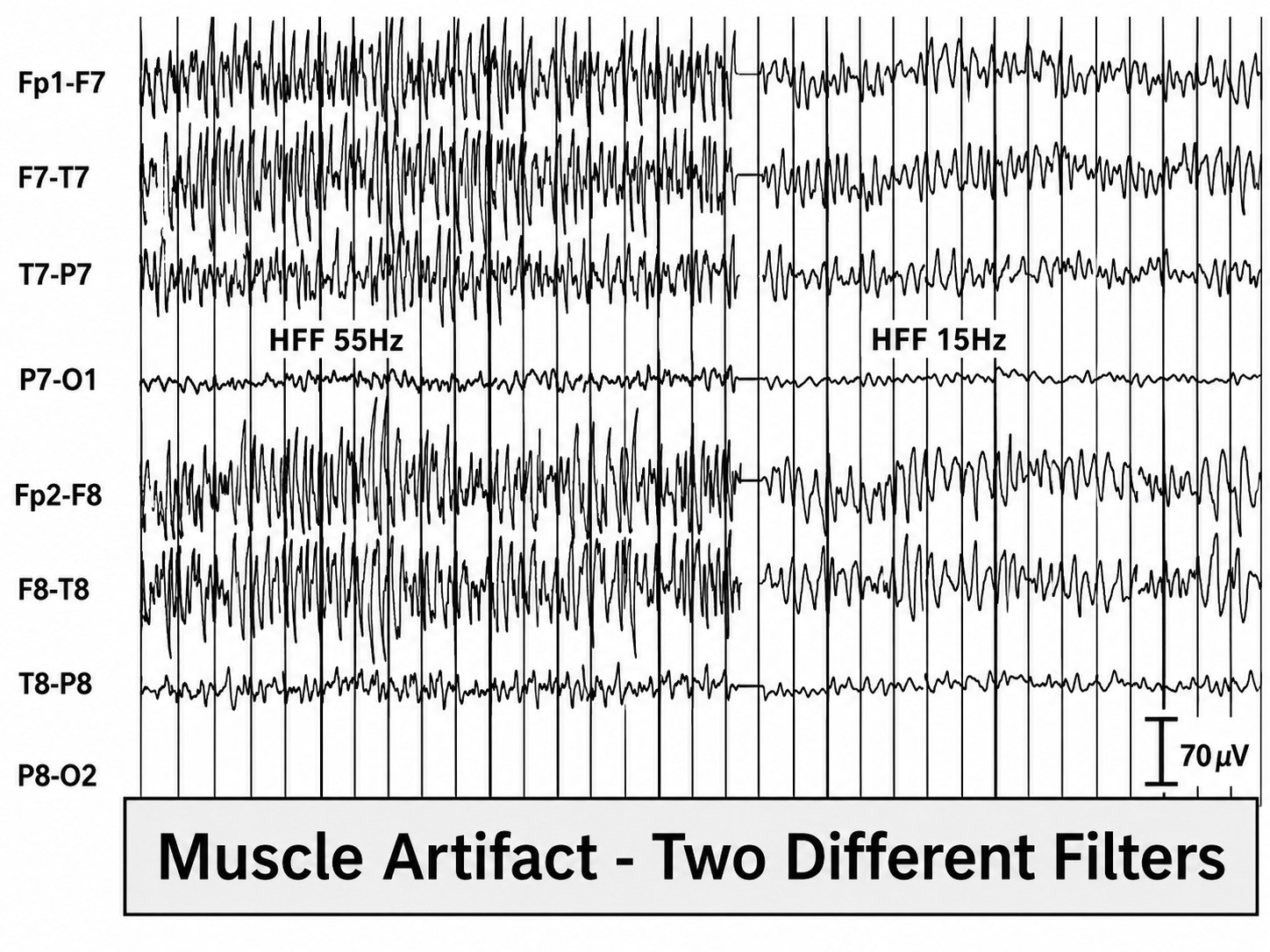
This image contrasts the same EEG segment under two filter conditions: HFF 55 Hz on the left and HFF 15 Hz on the right. The higher filter setting preserves more high-frequency EMG activity, while the lower setting attenuates it. The longitudinal bipolar temporal EEG channels show prominent, irregular high-frequency activity consistent with myogenic artifact when the high-frequency filter is set to 55 Hz. Reducing the high-frequency filter to 15 Hz markedly attenuates and smooths the fast activity, demonstrating how filtering can suppress the visual appearance of muscle artifact without removing the underlying contamination from the recording.
The next graphic shows how gum chewing can generate EMG artifact by contracting the muscles of mastication. While strong muscular contraction can contaminate every frequency band, including the alpha range near 10 Hz, the beta band (roughly 13–30 Hz) and the gamma range above 30 Hz are most affected. This means EMG artifact may create the appearance of greater beta activity than is actually present, a critical consideration when interpreting qEEG maps.
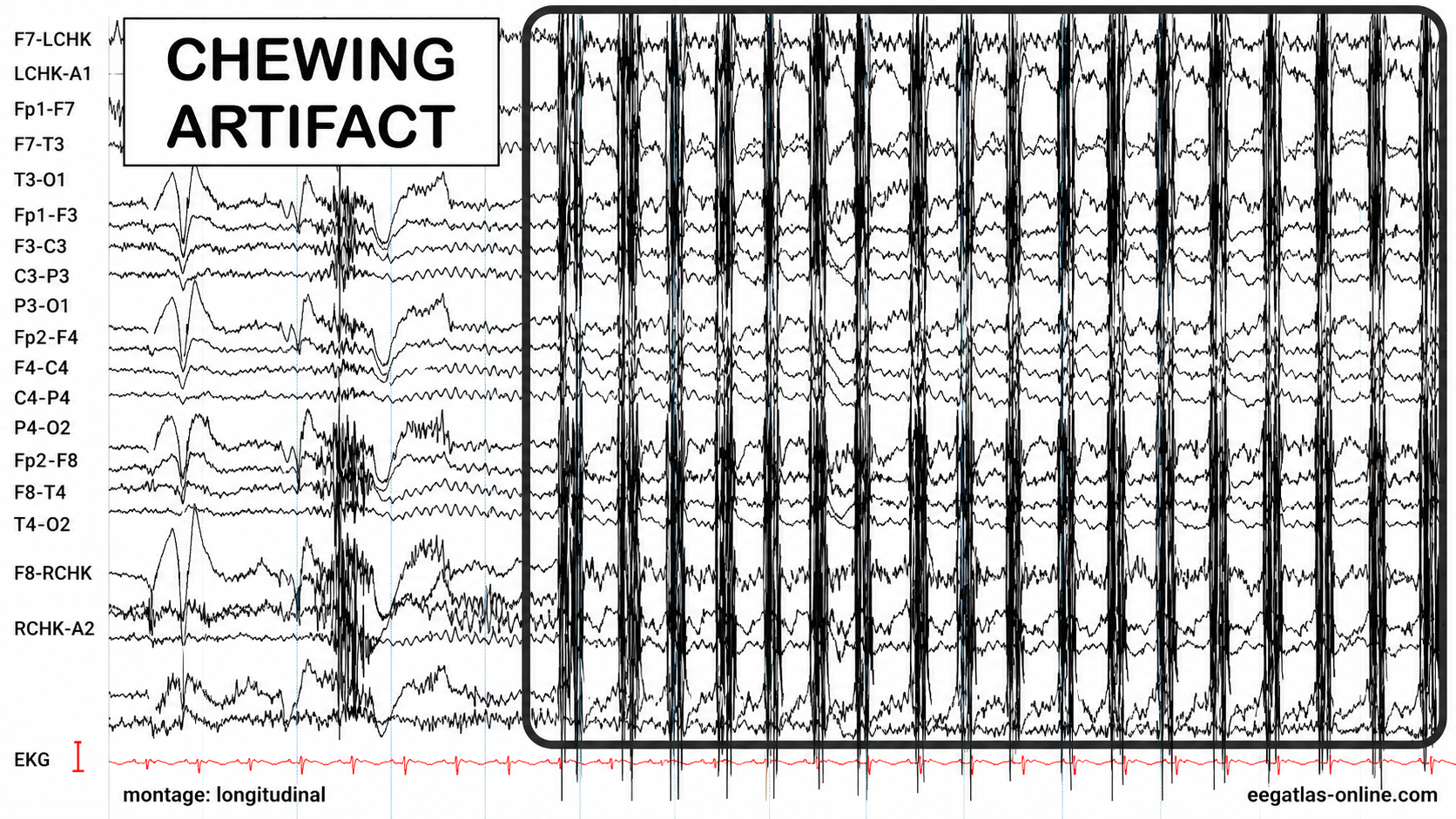
Graphic adapted from © eegatlas-online.com. This EEG recording captures chewing artifact in a longitudinal bipolar EEG montage, showing rhythmic, high-amplitude EMG bursts from jaw muscle activity that obscure the underlying cerebral signal, especially across anterior and temporal leads.
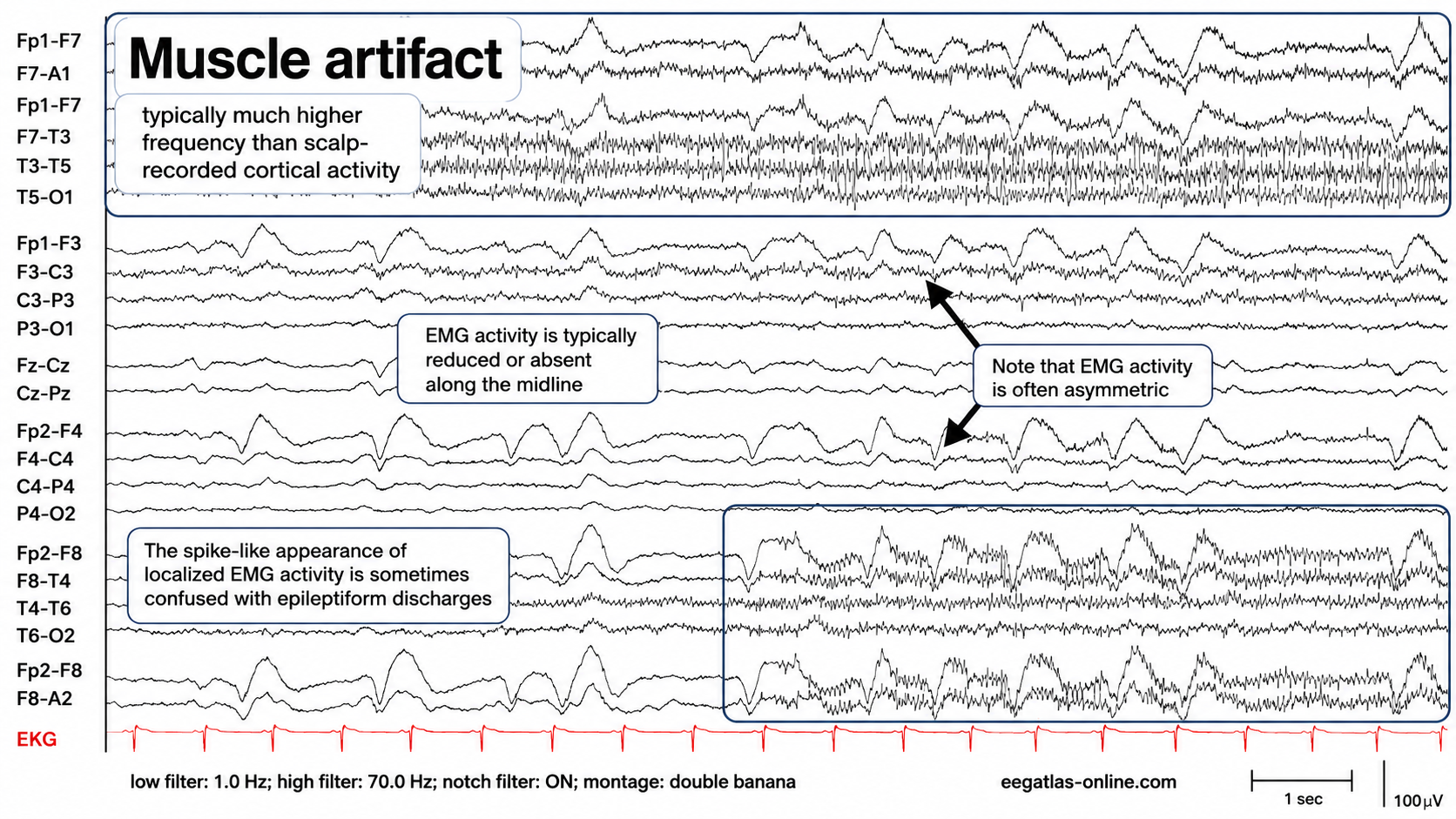
Graphic adapted from © eegatlas-online.com. This recording illustrates muscle artifact in a double-banana EEG montage. This tracing demonstrates irregular, high-frequency EMG activity superimposed on scalp-recorded EEG, most prominent over the anterior and temporal derivations and relatively reduced along the midline. The artifact is asymmetric, intermittent, and sharply contoured in places, producing spike-like waveforms that may be mistaken for epileptiform discharges if interpreted without attention to frequency content, distribution, field, and temporal context. The preserved high-frequency components are emphasized by the 70 Hz high-frequency filter setting, while the red EKG channel provides cardiac timing for comparison. Overall, the pattern is consistent with myogenic contamination rather than primary cortical activity.
Below is a BioGraph ® Infiniti EMG artifact display. Note how the amplitude of the EEG spectrum increases with each contraction.
Thompson and Thompson (2015) observed that EMG artifact is often readily detected because it may affect only one or two channels, particularly at T3 and T4 at the periphery, and less often at O1, O2, Fp1, and Fp2. Generalized tension, however, can contaminate the entire array, so a focal distribution should be treated as a helpful clue rather than a defining feature. You can identify EMG artifact by visually inspecting the raw signal, as shown in the next graphic using a 70-Hz high-frequency filter.
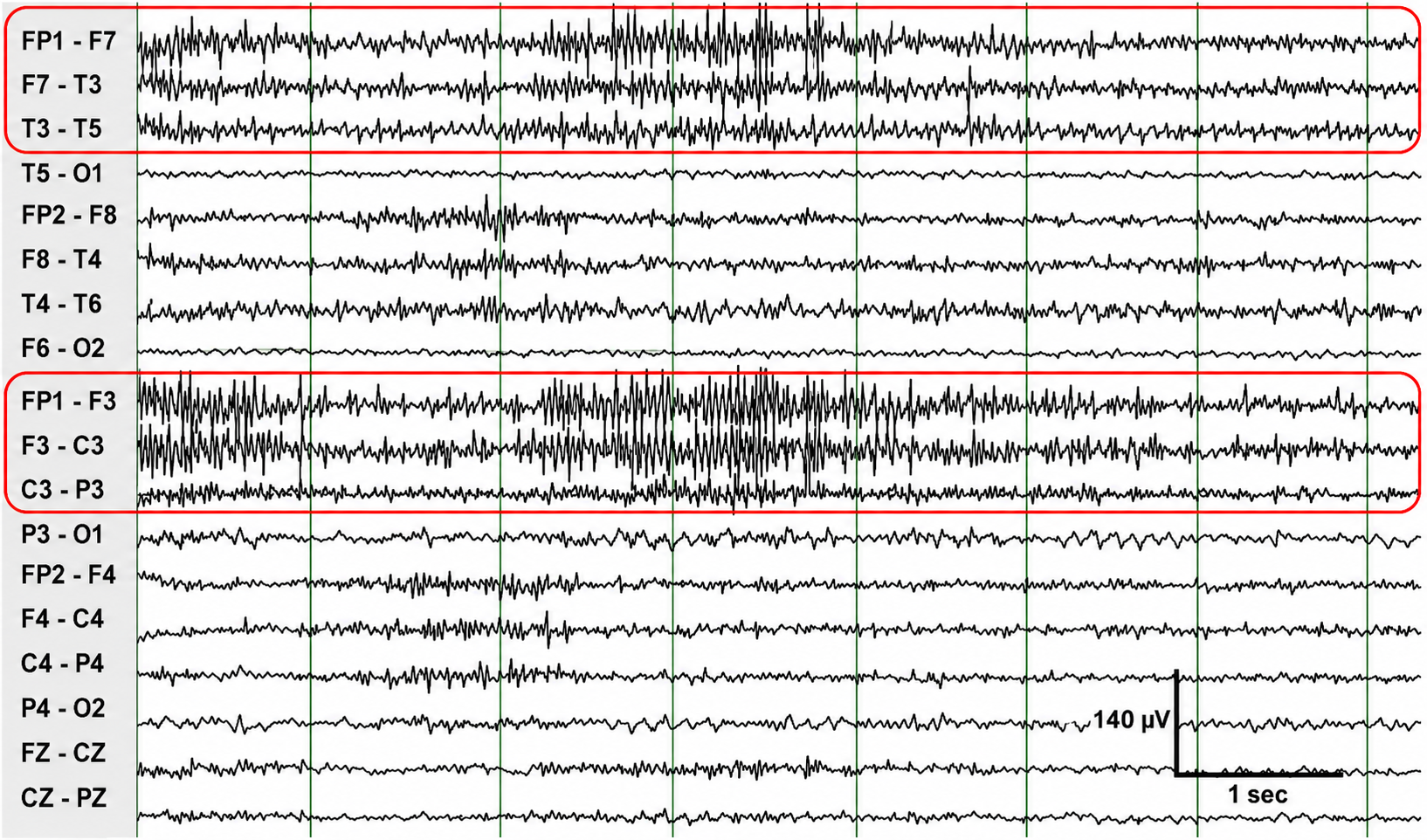
Graphic adapted from © eegatlas-online.com. This graphic illustrates focal EMG artifacts contaminating a longitudinal bipolar EEG montage. The red-outlined regions highlight irregular, high-frequency muscle activity superimposed on the EEG, most prominent in the left anterior temporal and left parasagittal derivations, including FP1–F7, F7–T3, T3–T5, FP1–F3, F3–C3, and C3–P3. The activity is asymmetric, anteriorly weighted, and relatively reduced in posterior and midline channels, a distribution consistent with focal myogenic contamination from scalp, facial, temporalis, or jaw muscle activity. The sharply contoured bursts and fast rhythmic components may obscure the underlying cerebral background and can be mistaken for pathologic fast activity or spike-like transients if interpreted without considering artifact morphology, spatial distribution, and lack of a consistent physiologic cortical field. Calibration markers indicate a 1-second time base and 140 µV amplitude scale.
Electro-Ocular Artifact
Electro-ocular artifact contaminates EEG recordings with potentials generated by eye blinks, eye flutter, and other eye movements. For example, anxious patient eyelid flutter may cause deflections at Fp1 and Fp2 (Klass, 1995). This artifact arises because the eye acts as an electrical dipole—the corneoretinal potential, electropositive at the cornea and electronegative at the retina—whose orientation relative to the frontal electrodes changes when the eye rotates. Eyelid movement across the cornea contributes as well. Bell's phenomenon refers to the upward and outward rotation of the eye during lid closure, which drives the corneal positivity toward the frontopolar electrodes and produces a large frontal deflection.
Both types of eye artifact can mimic meaningful EEG patterns, particularly for untrained readers, and may distort assessment results when using normative database comparisons. Slow lateral eye movements during an eyes-closed recording can be mistaken for delta activity, since they produce deflections in the delta range of roughly 0.5–4 Hz or slower. Blink artifact can resemble the sharp spike-and-wave patterns associated with seizure activity, especially when repetitive, as with eye flutter.
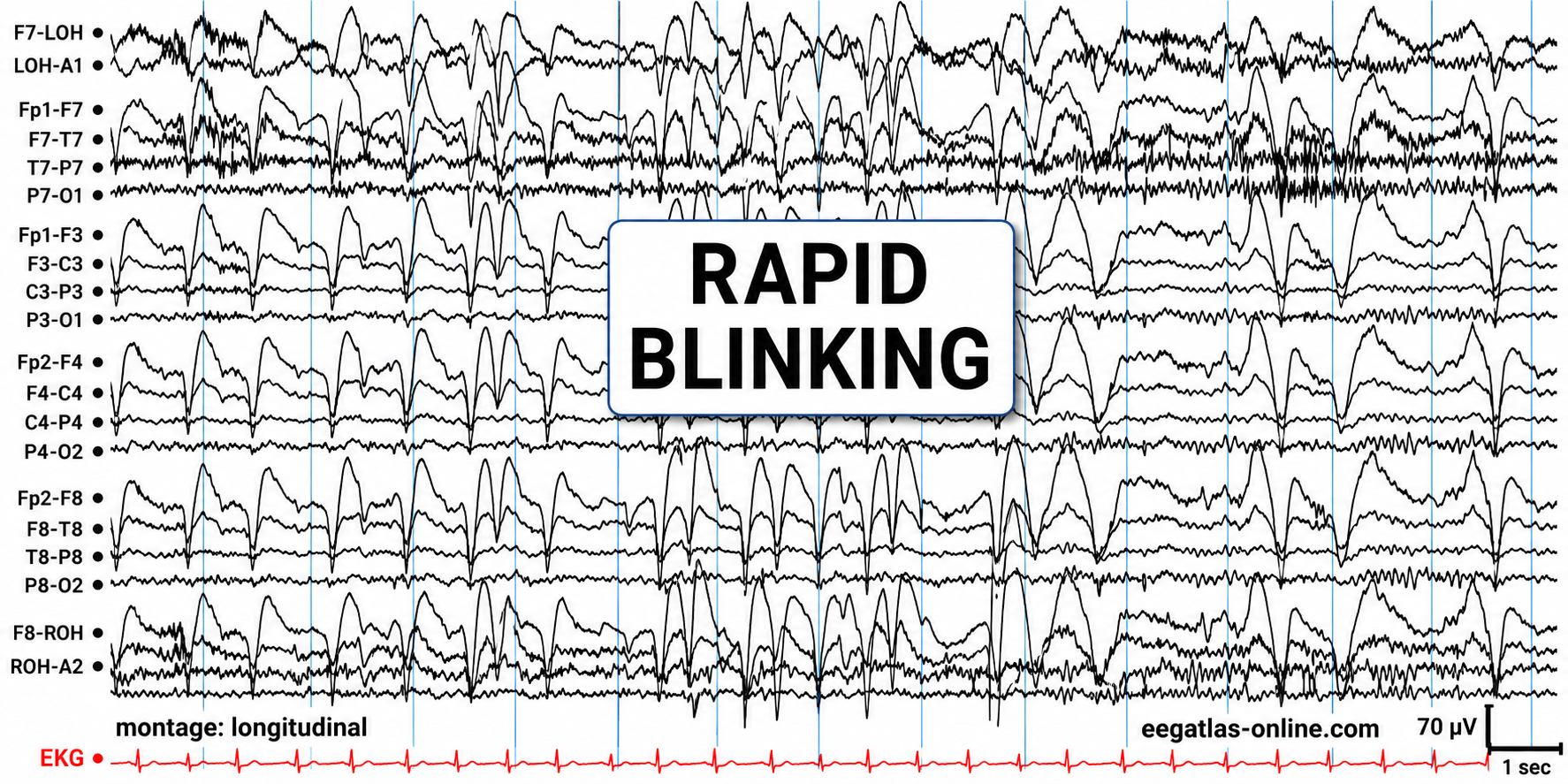
Graphic adapted from © eegatlas-online.com. This graphic captures rapid blinking artifact in a longitudinal bipolar EEG montage. This tracing shows repeated, high-amplitude, sharply contoured anterior slow transients occurring in rapid succession, maximal in the frontal and frontopolar derivations and spreading posteriorly with decreasing amplitude. The pattern is broadly synchronous across anterior chains and is time-locked to repeated eyelid movements, consistent with rapid blinking artifact. Although eyelid and facial muscle activity may contribute high-frequency EMG components, the dominant waveform morphology reflects ocular/blink artifact rather than cerebral activity. The artifact obscures the underlying EEG background, especially in FP1–F7, FP1–F3, FP2–F4, and FP2–F8 channels, and could be mistaken for frontal rhythmic or sharply contoured activity if interpreted without attention to its stereotyped anterior distribution, repetitive blink timing, and lack of a physiologic cortical field. The EKG channel is displayed separately at the bottom, with calibration markers indicating 1 second and 70 µV.
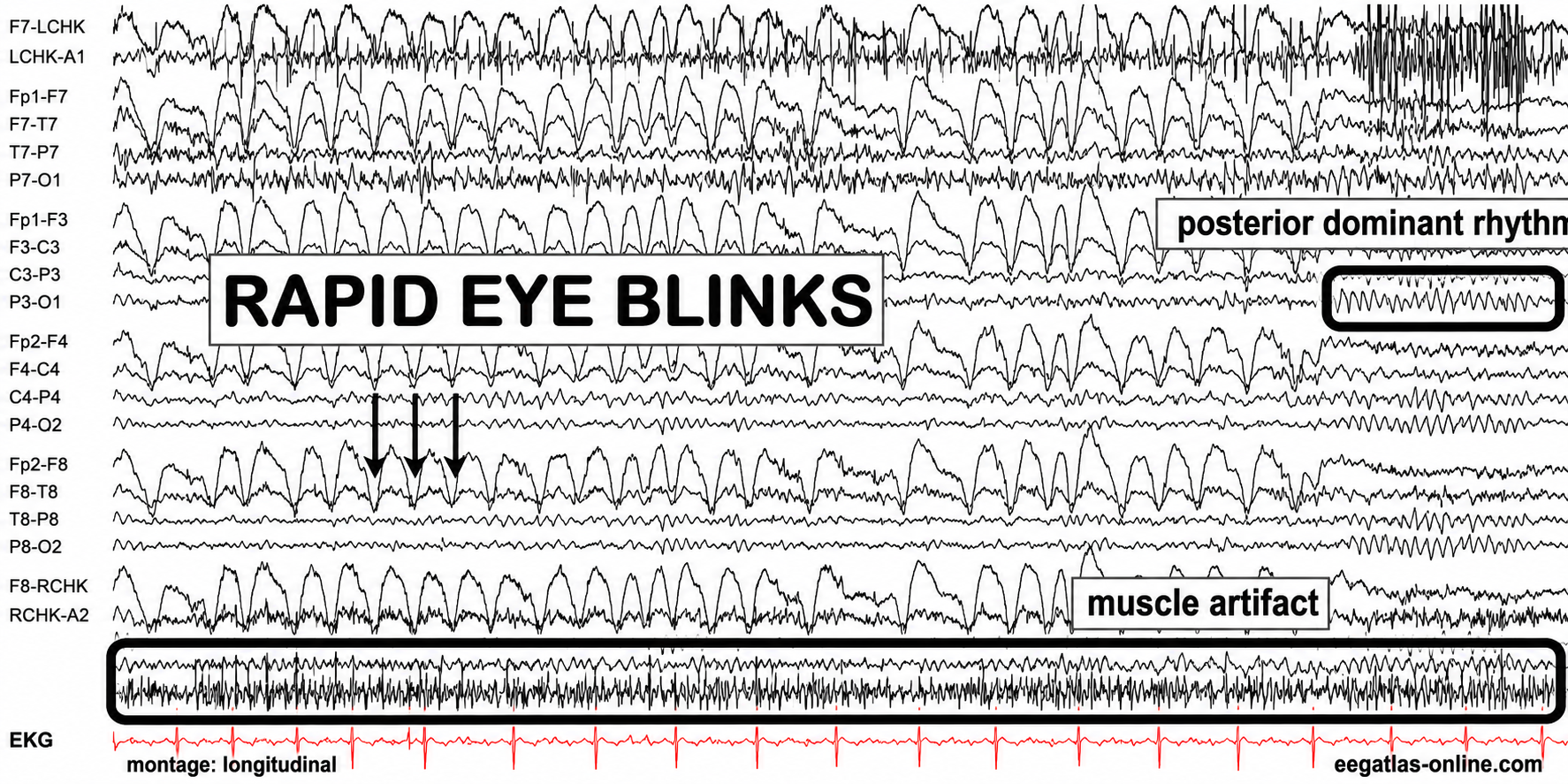
Graphic adapted from © eegatlas-online.com. This recording captures rapid eye-blink artifact with superimposed muscle artifact in a longitudinal bipolar EEG montage. The tracing shows repetitive, high-amplitude, sharply contoured anterior transients produced by rapid blinking, maximal in the frontopolar and frontal derivations and diminishing posteriorly. These stereotyped blink waveforms recur in close succession and obscure the underlying EEG background, particularly across FP1–F7, FP1–F3, FP2–F4, and FP2–F8 chains. A separate band of irregular high-frequency activity labeled muscle artifact is visible near the lower portion of the recording, consistent with concurrent facial, scalp, or jaw EMG contamination. In contrast, the labeled posterior dominant rhythm is seen over posterior channels as a more regular occipital rhythm, helping distinguish physiologic cerebral activity from ocular and myogenic artifact. The EKG channel at the bottom provides cardiac timing and is not time-locked to the blink or muscle bursts.
The next graphic shows eye blinks, sharp lateral eye movement, and slow lateral eye movement.
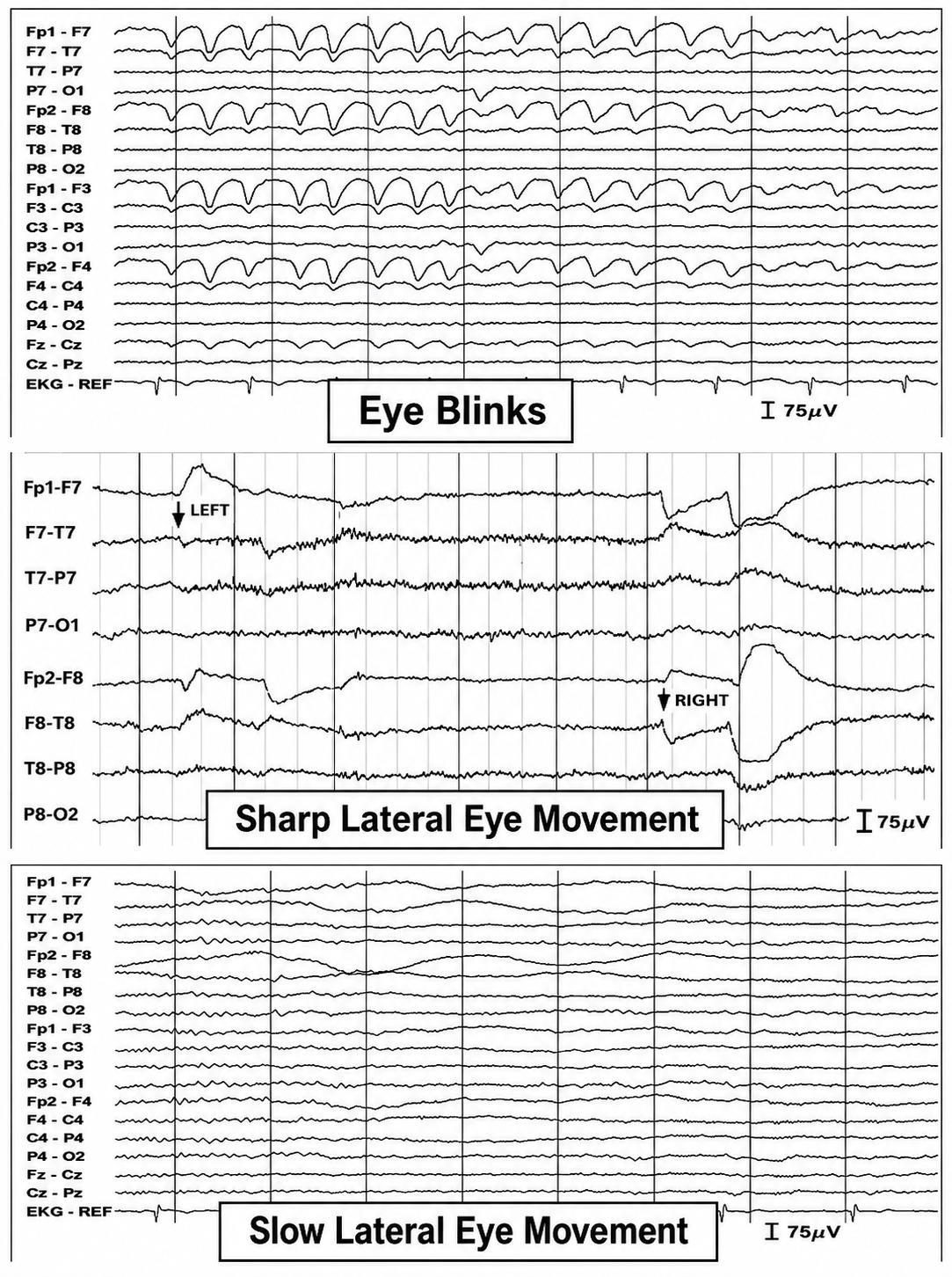
This recording captures eye blinks and lateral eye movements. This longitudinal bipolar EEG graphic contrasts three common ocular artifacts. The upper panel shows repeated eye-blink artifacts, appearing as large, stereotyped, frontally maximal slow deflections that are most prominent in FP1–F7, FP2–F8, FP1–F3, and FP2–F4, with attenuation posteriorly. The middle panel demonstrates sharp lateral eye movements, with asymmetric frontal-temporal deflections corresponding to leftward and rightward gaze shifts. The lower panel shows slow lateral eye movement, producing broader, lower-frequency drifting potentials across anterior derivations. Although eyelid and periocular muscle activity may add small fast components, the dominant pattern is ocular rather than primary EMG artifact, reflecting corneoretinal and eyelid-movement potentials that can obscure or mimic frontal cerebral activity. Calibration markers indicate 75 µV amplitude scaling.
Below is a BioGraph ® Infiniti EEG display of eye movement artifact.
Below is a NeXus display of eye blink and EMG © John S. Anderson.An upward eye movement makes Fp1 and Fp2 electrically positive, while a downward movement makes them electrically negative. Remember that clinical EEG is displayed with negative-up polarity, so a frontal positivity appears as a downward pen deflection. In a longitudinal sequential montage, the artifact appears most prominently in the frontopolar derivations (Fp1-F3, Fp2-F4, Fp1-F7, and Fp2-F8). A leftward eye movement carries the positive cornea toward F7, producing a positivity at F7 and a corresponding negativity at F8 (Thompson & Thompson, 2015). Rapid eye flutter may closely resemble seizure activity.
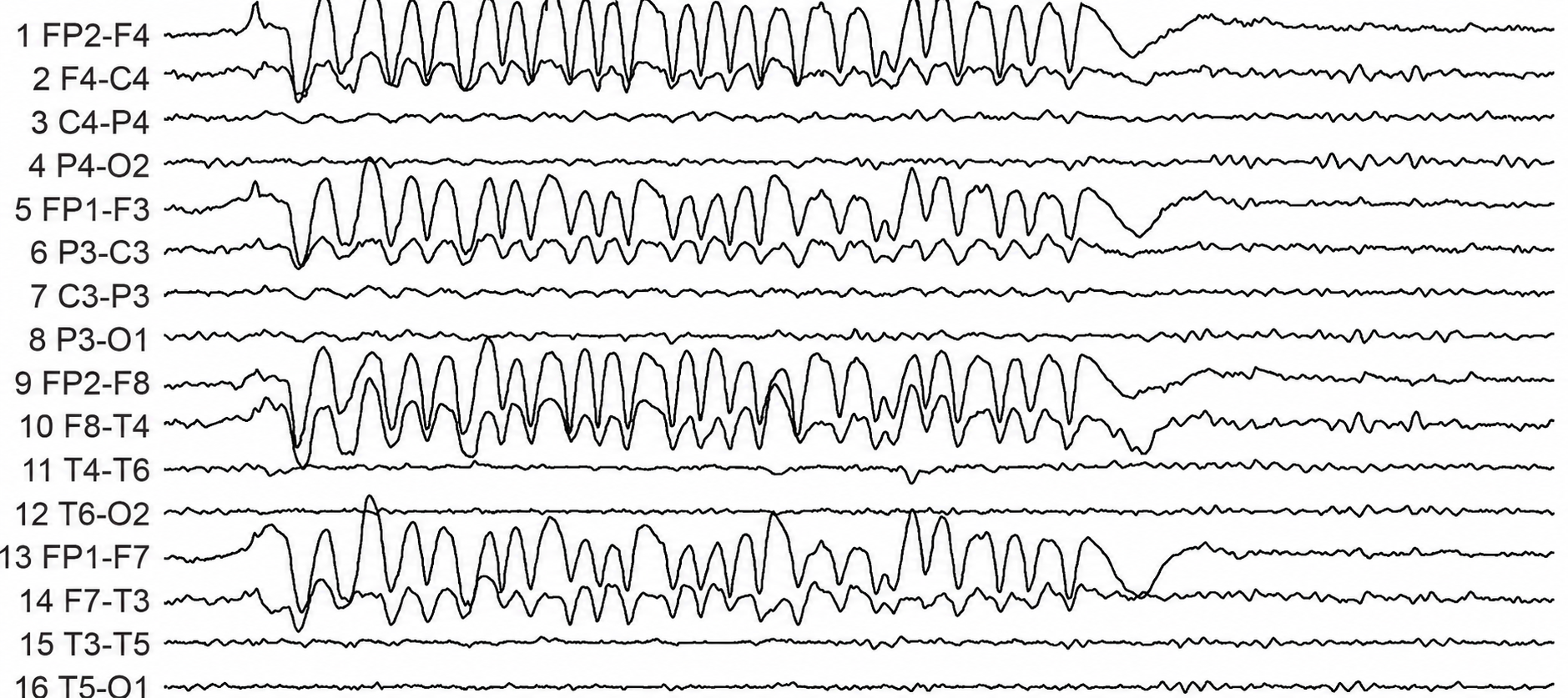
This recording captures rapid blinking artifact in a bipolar EEG montage. This tracing shows a burst of repetitive, high-amplitude anterior deflections maximal in the frontopolar and frontal derivations, including FP2–F4, FP1–F3, FP2–F8, and FP1–F7. The waveforms are stereotyped, rhythmic, and sharply contoured, with clear attenuation in central, parietal, temporal-posterior, and occipital channels. The morphology and distribution are most consistent with rapid eye-blink artifact, reflecting ocular potentials with possible superimposed periocular muscle activity, rather than primary cortical activity. Because the repeated frontal transients are large and sharply contoured, they may obscure the underlying EEG and could be misread as frontal rhythmic slowing or epileptiform-appearing activity unless their anterior predominance, blink-like repetition, and lack of a physiologic cortical field are recognized.
Cardiac and Pulse Artifacts
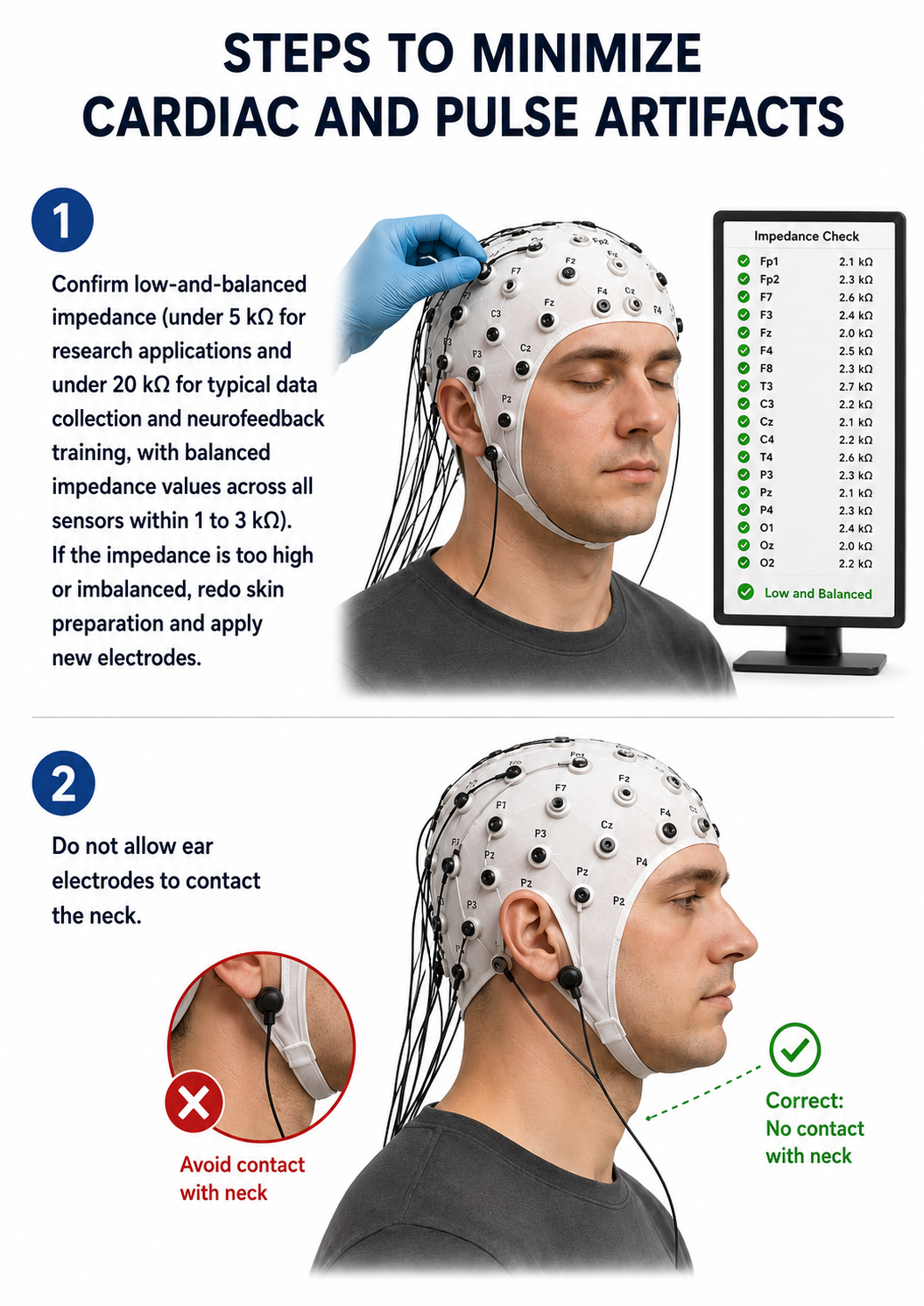
Cardiac artifact occurs when the ECG signal appears in the EEG (Jiang et al., 2019). This artifact may be produced when electrode impedance is imbalanced or too high, or when an ear electrode contacts the neck. It is also more common in patients with short, wide necks. The ECG signal spans roughly 0.05–100 Hz, so its artifact can contaminate the delta through beta bands, although the sharp QRS complex contributes most of its distinctive appearance. Because multiple electrodes detect this artifact simultaneously and in near-perfect time-lock, it can create the false appearance of elevated coherence, a particularly misleading finding when evaluating brain connectivity.
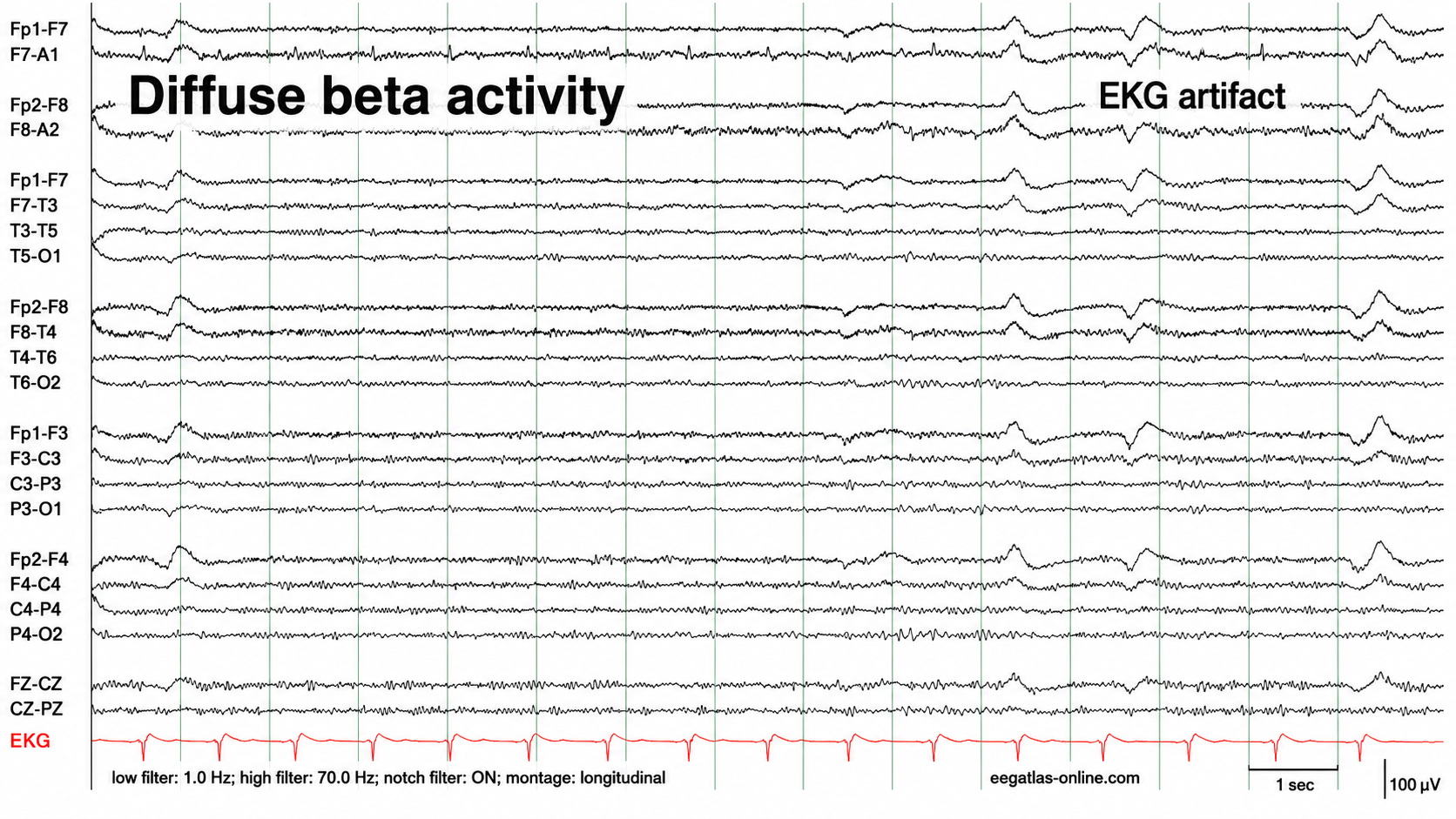
Graphic adapted from © eegatlas-online.com. This EEG segment is displayed in a longitudinal bipolar montage with a low-frequency filter of 1.0 Hz, a high-frequency filter of 70.0 Hz, the notch filter turned on, and a simultaneous EKG channel recorded at the bottom. Historically, fast beta activity has been understood in clinical EEG as a low-amplitude, high-frequency background feature that is often most visible over frontal and central scalp regions. It is generally interpreted cautiously because it is highly sensitive to patient state, medication effects, muscle activity, and recording conditions. Cardiac artifact has an equally long-standing role in EEG interpretation as an extracerebral signal that can project into scalp channels and mimic sharply contoured cerebral transients if the EKG channel is not reviewed carefully.
The dominant feature in this tracing is diffuse beta activity. The fast activity is low in amplitude, broadly distributed, and present across multiple bilateral derivations rather than being confined to a single focal region. It appears most conspicuous in frontal, frontotemporal, and central chains, but it is not limited to one hemisphere or one electrode pair. The activity does not show a focal phase reversal, does not organize into an evolving rhythmic discharge, and does not have the morphology of a definite epileptiform pattern in this isolated sample. In clinical terms, this would be described as diffuse excessive beta or diffuse fast activity, while recognizing that the finding is nonspecific.
You can detect cardiac artifacts by inspecting chart recorder, data acquisition, or oscilloscope displays of the raw EEG waveform. Cardiac artifact appears as a sharp, regularly repeating wave recurring at the heart rate—roughly once per second at a resting rate of about 60 beats per minute (Thompson & Thompson, 2015). ECG artifacts are most easily recognized when a separate ECG tracing is available for direct comparison, and they are observed best in referential montages using earlobe electrodes A1 and A2 or mastoid electrodes M1 and M2.
Below is a BioGraph ® Infiniti ECG artifact display.
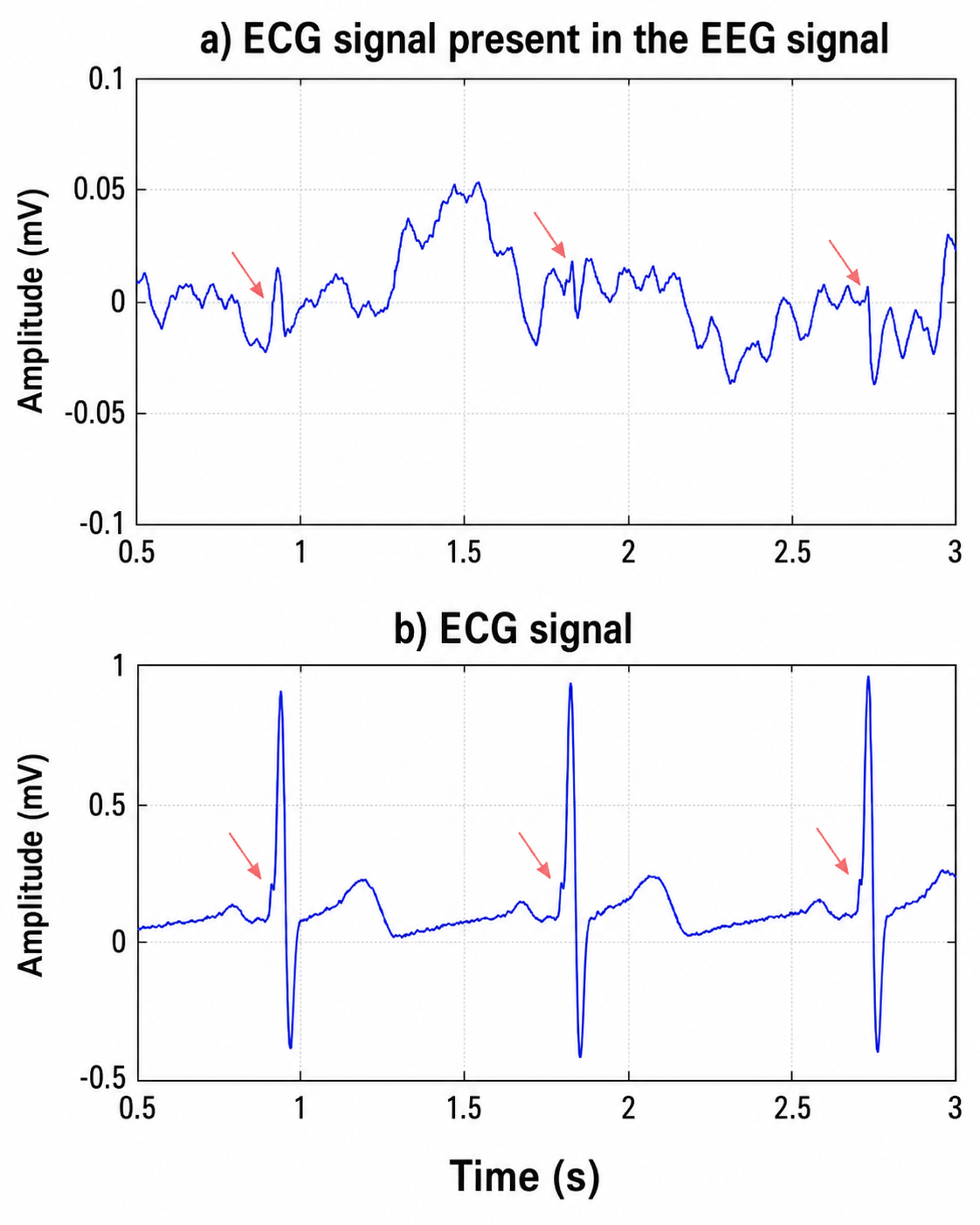
We adapted an ECG artifact graphic by Garces et al. (2007). The upper trace is labeled as an EEG signal containing ECG activity. Its amplitude is much smaller than the ECG trace, ranging approximately from −0.1 to +0.1 mV, which corresponds to about −100 to +100 µV. Across the 0.5-to-3.0 second epoch, the signal shows an irregular low-amplitude EEG background with superimposed deflections. The red arrows identify small waveform components in the EEG trace that occur at the same times as cardiac events in the lower ECG trace. These deflections are not large compared with the background, but their repeated temporal alignment with the ECG complexes makes them suspicious for cardiac artifact rather than independent cerebral activity.
The lower trace is the ECG signal itself. It has a larger amplitude range, extending roughly from −0.5 to +1.0 mV, and shows three prominent cardiac complexes over the displayed interval, occurring at approximately 0.95, 1.82, and 2.73 seconds. Each complex has a steep, high-amplitude QRS morphology, followed by slower recovery components. The red arrows point to earlier portions of the cardiac cycle immediately preceding the large QRS peaks. These same time points correspond to subtle deflections in the upper EEG trace, demonstrating that components of the cardiac signal are being transmitted into, or recorded by, the EEG channel.
Another cardiac-related artifact is the pulse artifact, which occurs when an EEG electrode is placed directly over a blood vessel. The mechanical movement of the electrode as the vessel expands and contracts with each heartbeat produces a slow-wave pattern that can be mistaken for delta activity. Pulse artifact in particular tends to appear in topographic EEG maps as excess delta at the affected site, leading to false positive findings; ECG artifact, being sharper, contributes across a wider range of bands. Both are time-locked to the cardiac cycle, which is why a simultaneous ECG channel is the most reliable way to identify them.
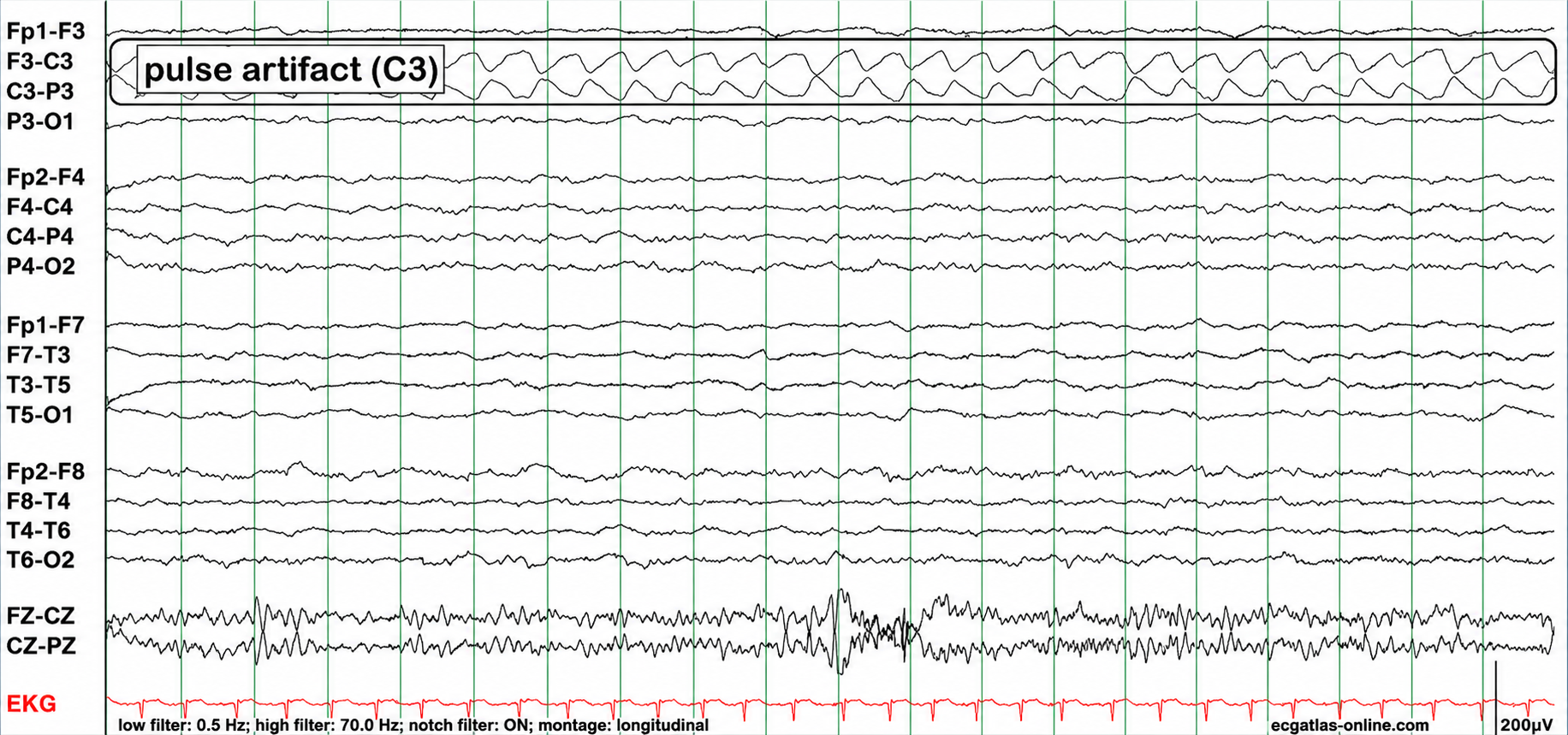
Graphic adapted from © eegatlas-online.com. This EEG segment is displayed in a longitudinal bipolar montage with a low-frequency filter of 0.5 Hz, a high-frequency filter of 70 Hz, the notch filter turned on, and a simultaneous EKG channel shown in red at the bottom. The calibration marker indicates 200 µV, so the prominent activity in the upper left parasagittal channels is relatively high in amplitude compared with much of the remaining background. Historically, this is the type of recording in which careful montage-based reasoning is essential, because a localized electrode artifact can produce a striking apparent abnormality unless one asks whether the waveform is generated by cortex or by a single contaminated electrode.
The most conspicuous abnormal-looking activity is the rhythmic waveform labeled pulse artifact (C3). It is confined almost entirely to the two bipolar derivations that share the C3 electrode, namely F3-C3 and C3-P3. The waveform has a repetitive, rounded, mechanical quality rather than the morphology of a cerebral rhythm. It recurs at a fairly regular interval and appears in opposite polarity across the two adjacent channels, creating a phase-reversal-like pattern at C3. In a true cerebral discharge, a phase reversal can sometimes help localize a cortical voltage maximum, but in this case the localization to a single electrode shared by two channels, the regular pulse-like repetition, and the absence of a physiologic field into neighboring left parasagittal or homologous right-sided channels strongly favor artifact.
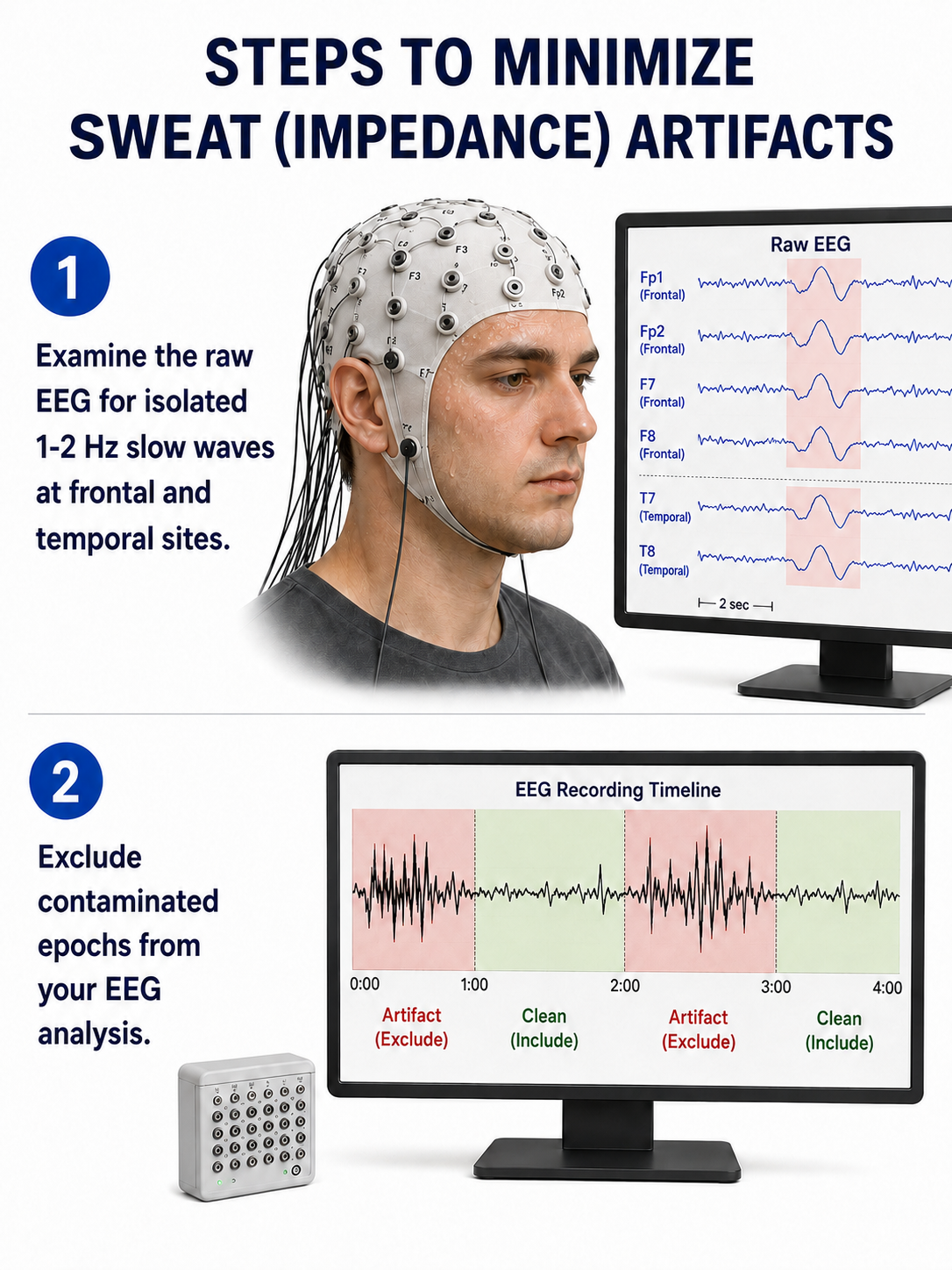
Sweat (Skin Potential) Artifact
Sweat artifact arises from two related mechanisms: the sodium chloride in perspiration alters the electrical properties of the skin under and near the electrode, and sweat gland activity generates its own very slow skin potentials. Sweat artifact and bridging artifact are related but distinct: heavy perspiration can create a conductive path between neighboring electrodes and so cause bridging, but the two produce different appearances and are treated separately below.
The classic sweat artifact is a large, very slow, rolling undulation of the baseline—typically below 0.5–1 Hz, and therefore slower than delta activity—appearing across several channels, most often frontal and temporal sites. Because these undulations are so slow, they are attenuated by raising the low-frequency filter cutoff, although the underlying skin condition should be corrected rather than filtered. Sweating may be provoked by anxiety, a warm room, or abrupt unexpected stimuli (Thompson & Thompson, 2015). See the Impedance Artifact section below for an illustration of the electrode-interface instability that heavy sweating can produce.
Bridging Artifact
Bridging artifact (also called a salt bridge) occurs when a low-resistance conductive path forms between adjacent electrodes—typically from excessive electrode paste or gel, heavy perspiration, or a wet scalp—so that the two electrodes record nearly the same potential. Bridged electrodes produce nearly identical tracings in a referential montage and a flat or markedly attenuated channel in a bipolar montage, because there is almost no voltage difference left for the differential amplifier to display. The Fp1-F3 channel's reduced amplitude and frequency in the graphic below illustrate this artifact.
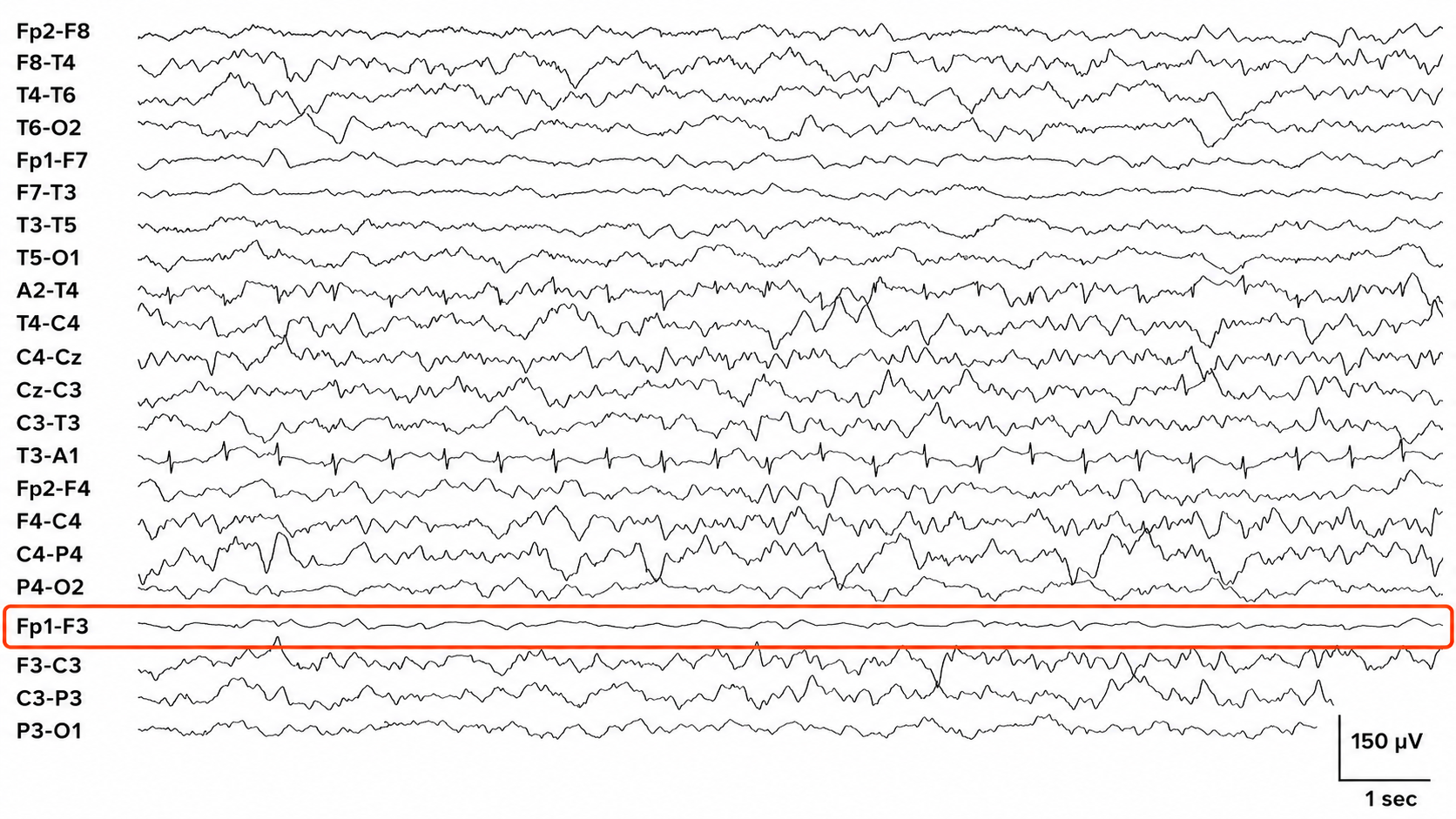
This EEG segment demonstrates a bridging artifact involving the left anterior frontal electrodes, most clearly seen in the highlighted Fp1-F3 derivation. Historically, bridging artifact has been recognized as an important technical pitfall in scalp EEG because it can make two nearby electrodes behave as though they are electrically shorted together. When conductive paste, sweat, saline, gel spread, or another low-resistance pathway connects two electrodes, the voltage difference between them becomes artificially reduced. In a bipolar montage, this can produce an abnormally flat or attenuated channel between the bridged electrodes, even while surrounding channels continue to show normal or artifact-contaminated EEG activity.
In this tracing, the highlighted Fp1-F3 channel is strikingly low in amplitude compared with adjacent and homologous derivations. It appears relatively flat and featureless across the displayed epoch, while the neighboring F3-C3, C3-P3, and P3-O1 channels show substantially larger mixed-frequency activity. This pattern is not physiologically plausible as an isolated absence of cerebral activity only between Fp1 and F3. Instead, it suggests that Fp1 and F3 are recording nearly the same electrical potential, leaving little voltage difference for the bipolar amplifier to display in the Fp1-F3 channel.
Drowsiness Artifact
Drowsiness artifact appears when drowsiness or stage N1 or N2 sleep intrudes into the EEG recording. Drowsiness is not an artifact in the strict sense—it is a normal physiologic state change, not a noncerebral signal—but it is treated as one here because it contaminates a recording intended to sample waking activity. This is most likely during eyes-closed conditions, though clients may drift into sleep even during an ostensibly "awake" recording. Recognizing drowsiness matters because it changes the EEG in ways that can be mistaken for pathology or that render portions of the recording unrepresentative of the client's waking brain state.
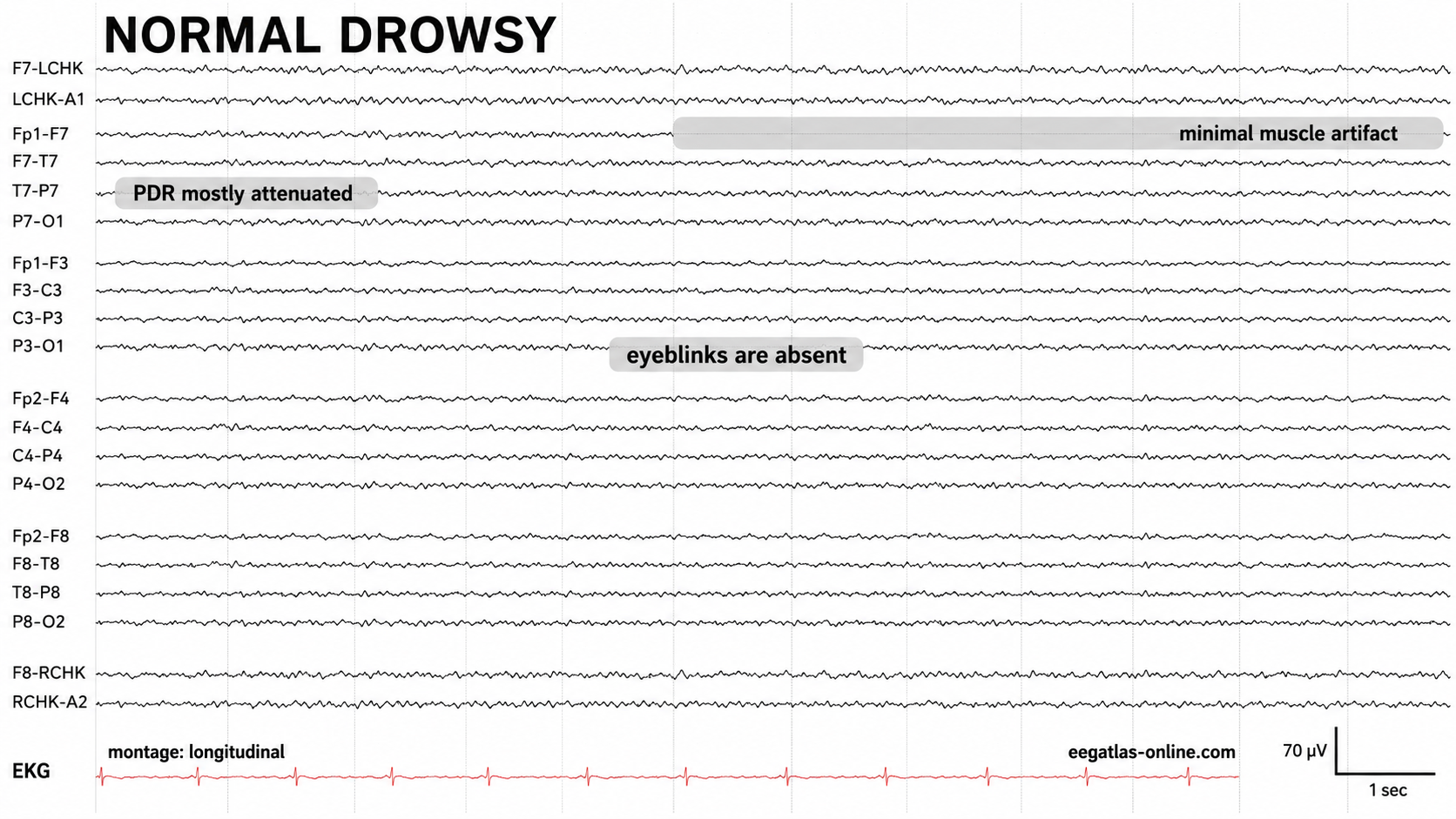
Graphic adapted from © eegatlas-online.com. This EEG segment shows a physiologic drowsy state in a longitudinal montage, with an EKG channel recorded at the bottom and a calibration of approximately 70 µV with a 1-second time marker. In the historical development of clinical EEG interpretation, drowsiness became important because the transition from relaxed wakefulness into stage N1 sleep changes the background in predictable ways: the posterior dominant rhythm loses persistence, eye blinks diminish or disappear, muscle activity often decreases, and the tracing becomes lower in sustained alpha organization with more mixed low-amplitude activity.
The most important feature in this recording is the attenuation of the posterior dominant rhythm. In a fully awake, relaxed, eyes-closed adult, one would expect a more sustained posterior alpha rhythm, usually maximal over the posterior head regions. In this segment, the posterior rhythm is mostly attenuated, especially across the posterior temporal and occipital derivations, consistent with the transition away from relaxed wakefulness. The tracing is not flat or suppressed; rather, it shows a low-amplitude mixed background in which the organized posterior alpha rhythm is no longer prominent.
The first example below shows a brief episode of drowsiness lasting about 5 seconds, with a dropout of the alpha rhythm (the posterior dominant rhythm, or PDR) followed by its return. The second example shows the end of a longer period of light sleep with a K-complex indicated in the F3-C3 derivation, followed by a return to a typical alpha rhythm.
This EEG recording is most consistent with a normal drowsy state. The tracing is shown in a longitudinal bipolar montage with a simultaneous EKG channel at the bottom, and the overall appearance is that of a low-amplitude, relatively symmetric background during the transition from relaxed wakefulness toward early sleep. In clinical EEG interpretation, drowsiness is recognized not as a pathologic state but as a physiologic change in background organization. As the patient becomes drowsy, the posterior dominant rhythm that is usually most evident during relaxed eyes-closed wakefulness becomes less sustained or attenuates, eye blinks diminish or disappear, and muscle activity often decreases as facial and scalp tone relax.
In this segment, the posterior dominant rhythm is mostly attenuated. The posterior derivations do not show a robust, continuous alpha rhythm, and instead the tracing contains lower-amplitude mixed-frequency activity distributed across the scalp. This is an expected feature of drowsiness, especially during the transition from wakefulness into stage N1 sleep. The background does not appear globally suppressed; rather, it has lost the organized posterior alpha pattern typical of fully alert relaxed wakefulness.
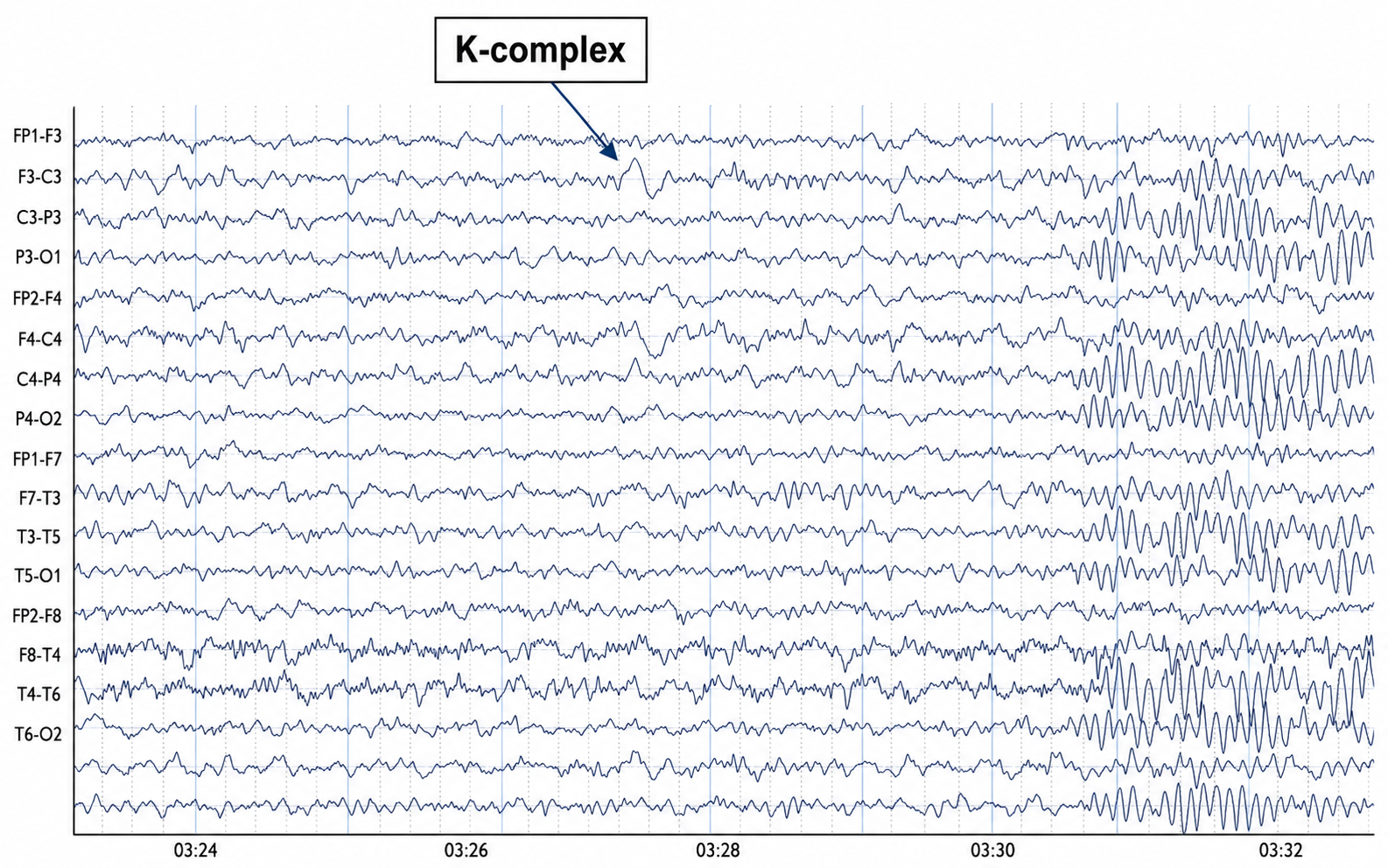
This EEG segment shows a normal sleep-transition pattern with clear features of drowsiness progressing into stage N2 sleep. The recording is displayed in a longitudinal bipolar montage, with bilateral anterior-posterior chains that allow comparison of frontal, central, temporal, parietal, and occipital regions. Historically, drowsiness in EEG was recognized by attenuation of the posterior dominant rhythm and the emergence of low-amplitude mixed-frequency activity, while stage N2 sleep became defined by the appearance of characteristic graphoelements such as K-complexes and sleep spindles. This image contains both the subdued, mixed background expected with reduced wakefulness and more specific stage N2 features.
The most conspicuous labeled event is a K-complex near the middle of the displayed epoch, around 03:27. It appears as a relatively high-amplitude, sharply contoured slow complex with a broad field, most evident over the frontocentral derivations. Its morphology is consistent with a normal sleep-related K-complex rather than an epileptiform discharge, because it is broad, state-dependent, not followed by an evolving ictal rhythm, and occurs in a background that otherwise shows sleep architecture. The field is not restricted to one electrode or one channel, which argues against a focal electrode artifact.
Later in the segment, beginning around 03:30 and continuing toward 03:32, there are prominent rhythmic waxing-and-waning bursts consistent with sleep spindles. These are most apparent over central and parasagittal derivations, with bilateral expression and a frequency visually compatible with the sigma range, typically around 12–14 Hz. Their morphology is regular and spindle-like, with gradual buildup and decline rather than abrupt onset and termination. This is a normal physiologic sleep pattern and supports classification as stage N2 sleep rather than simple quiet wakefulness.
Stage 1 (N1) sleep is a subtle, drowsy state that clients often fail to recognize. Alpha amplitude—especially over occipital sites—decreases markedly, while theta activity increases. Slow, rolling eye movements are accompanied by reductions in EMG amplitude, and the onset of sleep may bring sharply contoured transients known as vertex sharp waves (V-waves), which are maximal at the vertex and are a normal finding rather than epileptiform activity.
Graphics © John S. Anderson. The two images above each contain raw EEG tracings from two scalp electrodes: A (EEG1) shows P3–A1, and B (EEG2) shows P4–A2. The raw tracings are displayed with a 0–60 Hz bandpass and a 50 µV vertical scale. Below each set of raw tracings are compressed spectral arrays (CSA) presenting the same information as a three-dimensional image: frequency on the x-axis (here 0–40 Hz), power on the y-axis (0–12.0 in units of µV², which this software labels picowatts), and time on the z-axis (10 seconds).
Note that the top image, recorded during the initial eyes-closed period, shows an active posterior rhythm of about 10 Hz; the spectral display clearly renders bright yellow (higher-amplitude) peaks at 10 Hz. The lower image shows a much slower pattern in the raw tracing, with clear lateral eye-movement artifacts along with some theta and delta activity. The CSA reflects the same change, including the loss of the 10 Hz posterior rhythm. Together, these two images detail the transition from an awake, eyes-closed EEG to a drowsy, Stage 1 pattern.
When you detect drowsiness artifact during a training session, suspend recording and instruct your clients to move their hands and legs to increase wakefulness. To reduce the likelihood of this artifact, ask clients to obtain a full night's sleep—7 to 9 hours for most adults—before the recording, and schedule sessions away from the post-lunch dip when possible (Thompson & Thompson, 2015).
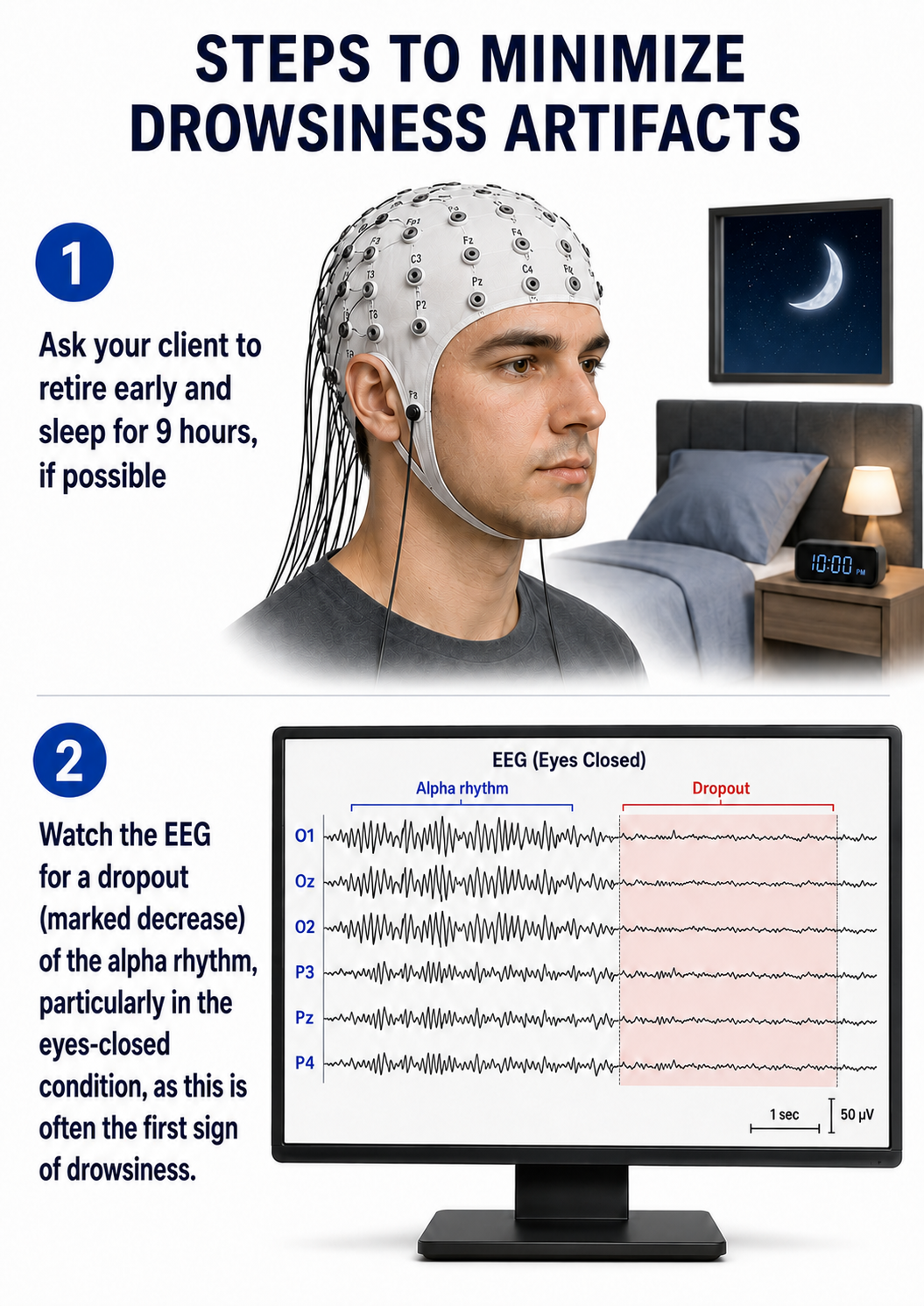
Evoked Potential
Evoked potential artifact (also called event-related potential artifact) consists of somatosensory, auditory, and visual signal processing-related transients that may contaminate multiple channels of an EEG record. While evoked potentials increase recording variability and reduce its reliability, they minimally affect averaged data (Thompson & Thompson, 2015).
Watch BPM Biosignals' YouTube video EEG: Visually evoked potentials (VEP).
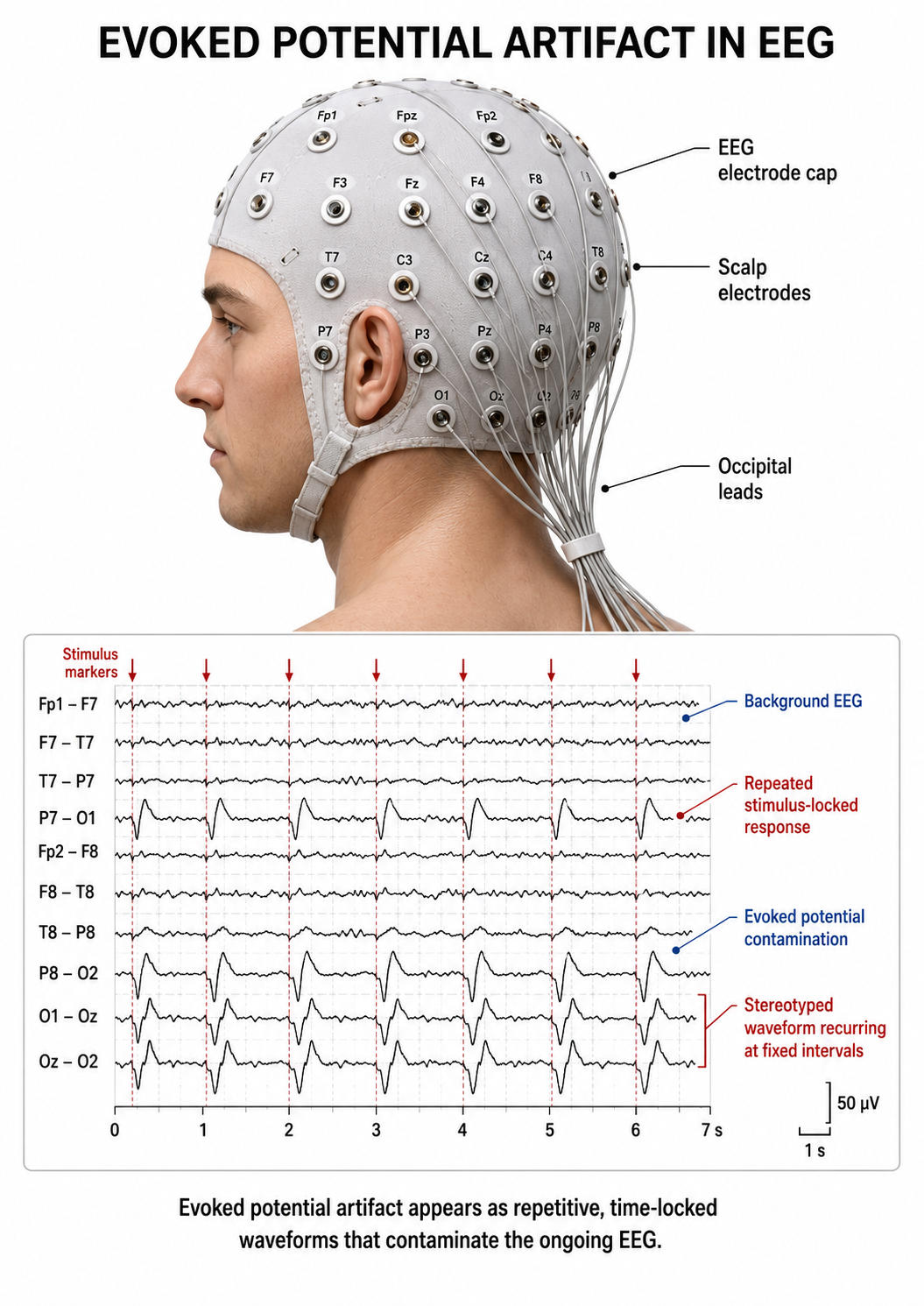
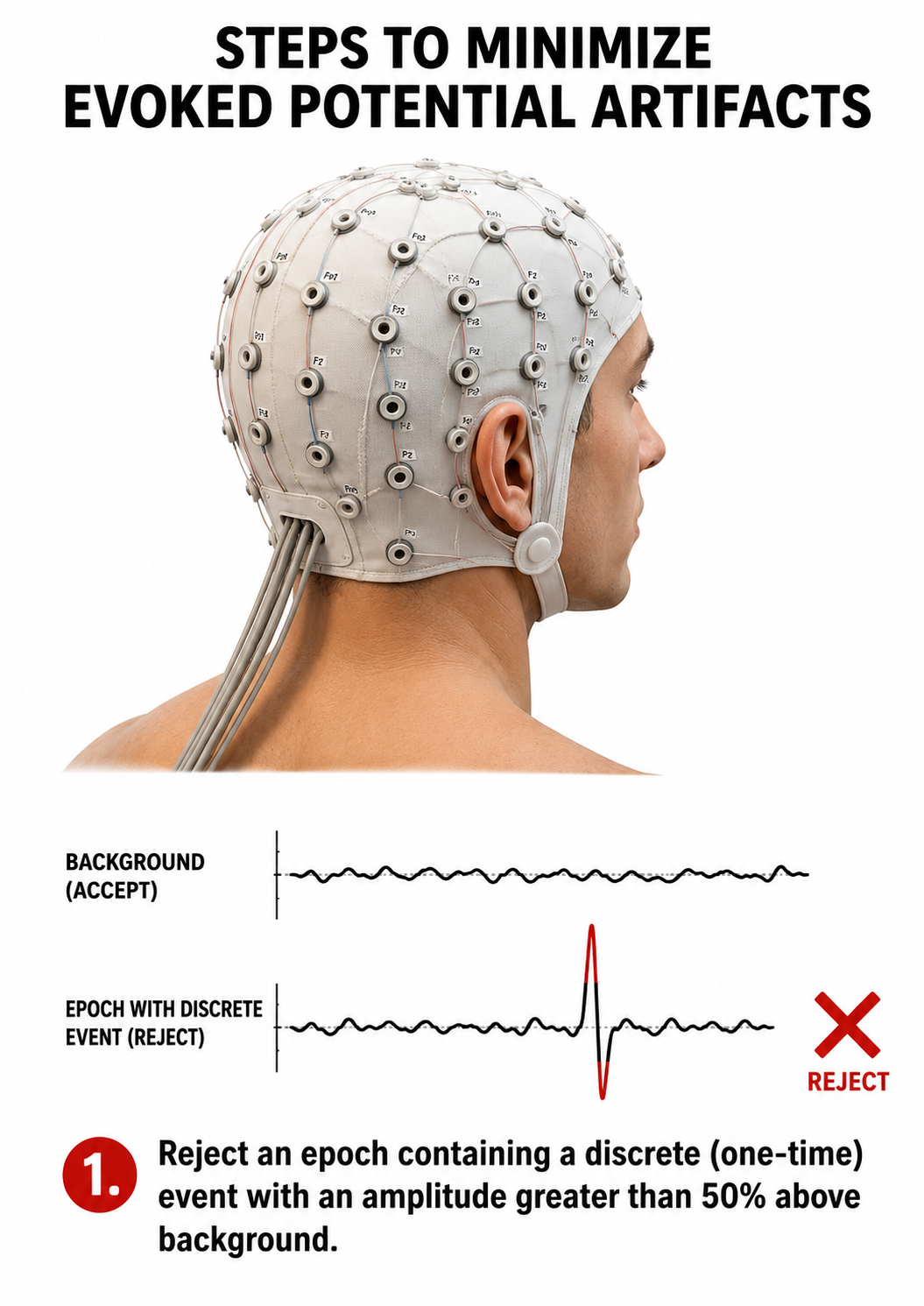
Movement Artifact
Movement artifact is caused by client movement or the movement of electrode wires by other individuals. Most of these artifacts result from brief changes in the electrode-skin surface connection. Cable movement is specifically called cable sway. Movement artifacts can produce high-amplitude voltages that are difficult to distinguish from genuine EEG and EMG signals on a single channel, although their abrupt onset, nonphysiologic morphology, and simultaneous appearance across many channels usually give them away. While the delta band is most affected, this artifact may also contaminate the theta band (Thompson & Thompson, 2015).
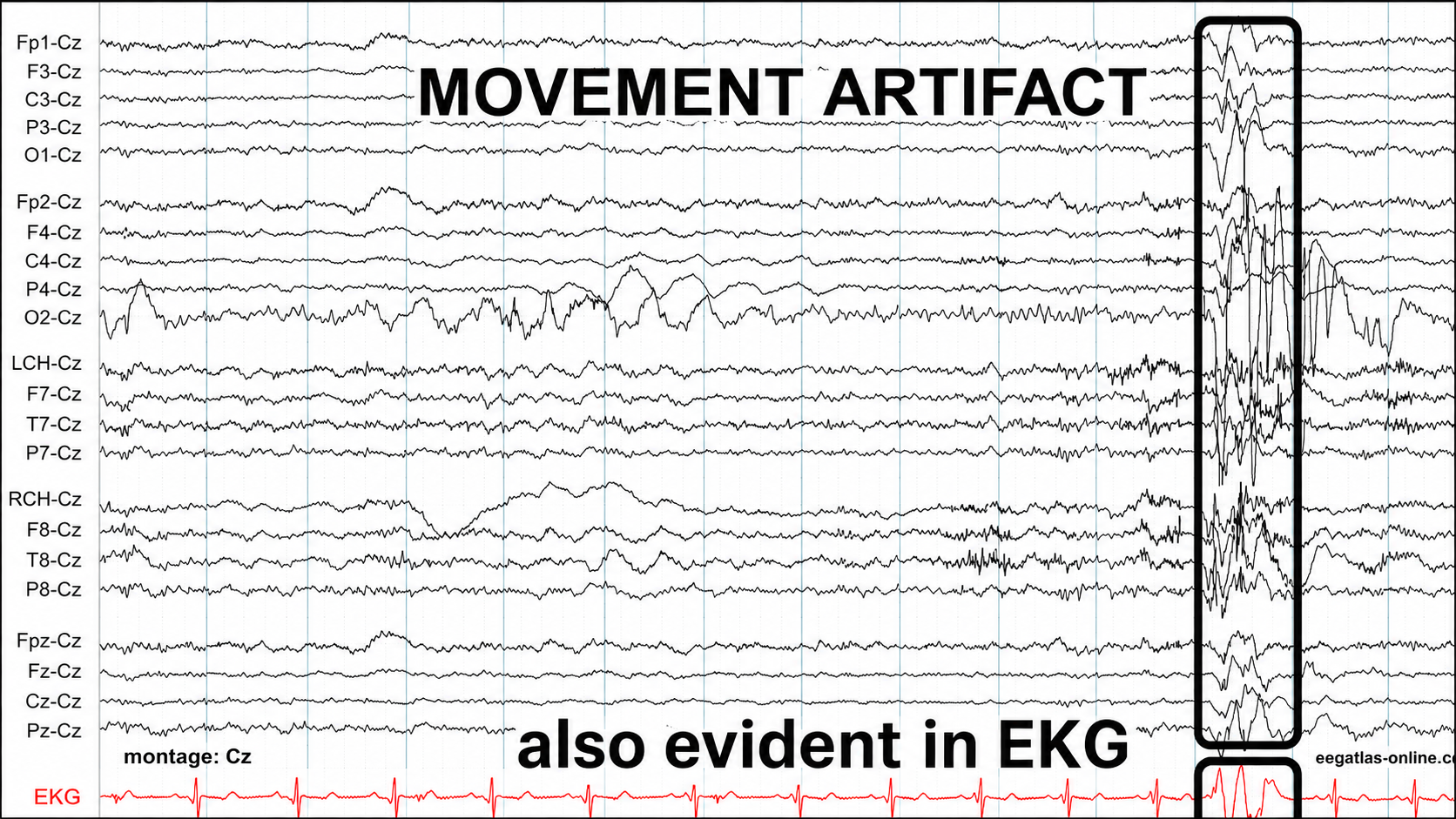
Graphic adapted from © eegatlas-online.com. This EEG segment shows a prominent movement artifact in a Cz-referential montage, with the most obvious contaminated interval highlighted near the right side of the tracing. The recording shows multiple scalp derivations referenced to Cz, with a simultaneous EKG channel at the bottom. Before the highlighted event, the EEG background consists of relatively lower-amplitude mixed-frequency activity with intermittent slower fluctuations. During the highlighted interval, however, there is an abrupt, large-amplitude, irregular disturbance that appears nearly simultaneously across many EEG channels.
The artifact has the typical appearance of movement contamination: the waveforms are large, abrupt, jagged, and nonphysiologic, with sudden baseline shifts and superimposed irregular faster components. The activity does not resemble a normal cerebral rhythm, a focal epileptiform discharge, or an evolving seizure pattern. Instead, it appears as a broad mechanical disruption of the recording. The morphology varies from channel to channel, but the timing is shared across much of the montage, which suggests movement of the patient, electrodes, leads, or reference pathway rather than a localized cortical generator.
The simultaneous disturbance in the EKG channel is especially important. The red EKG tracing at the bottom shows a clear disruption during the same interval as the EEG artifact, with large noncardiac deflections superimposed on or replacing the usual cardiac rhythm. When a large EEG disturbance is also evident in the EKG channel, the finding strongly supports a non-cerebral source, because true cortical activity would not be expected to produce a simultaneous large artifact in the cardiac lead. This temporal correspondence indicates that the event likely reflects body movement, cable movement, electrode displacement, or generalized mechanical disturbance affecting multiple recording channels.
The graphic below shows movement artifacts due to head movement (left), respiration (center), and tongue movement (right).
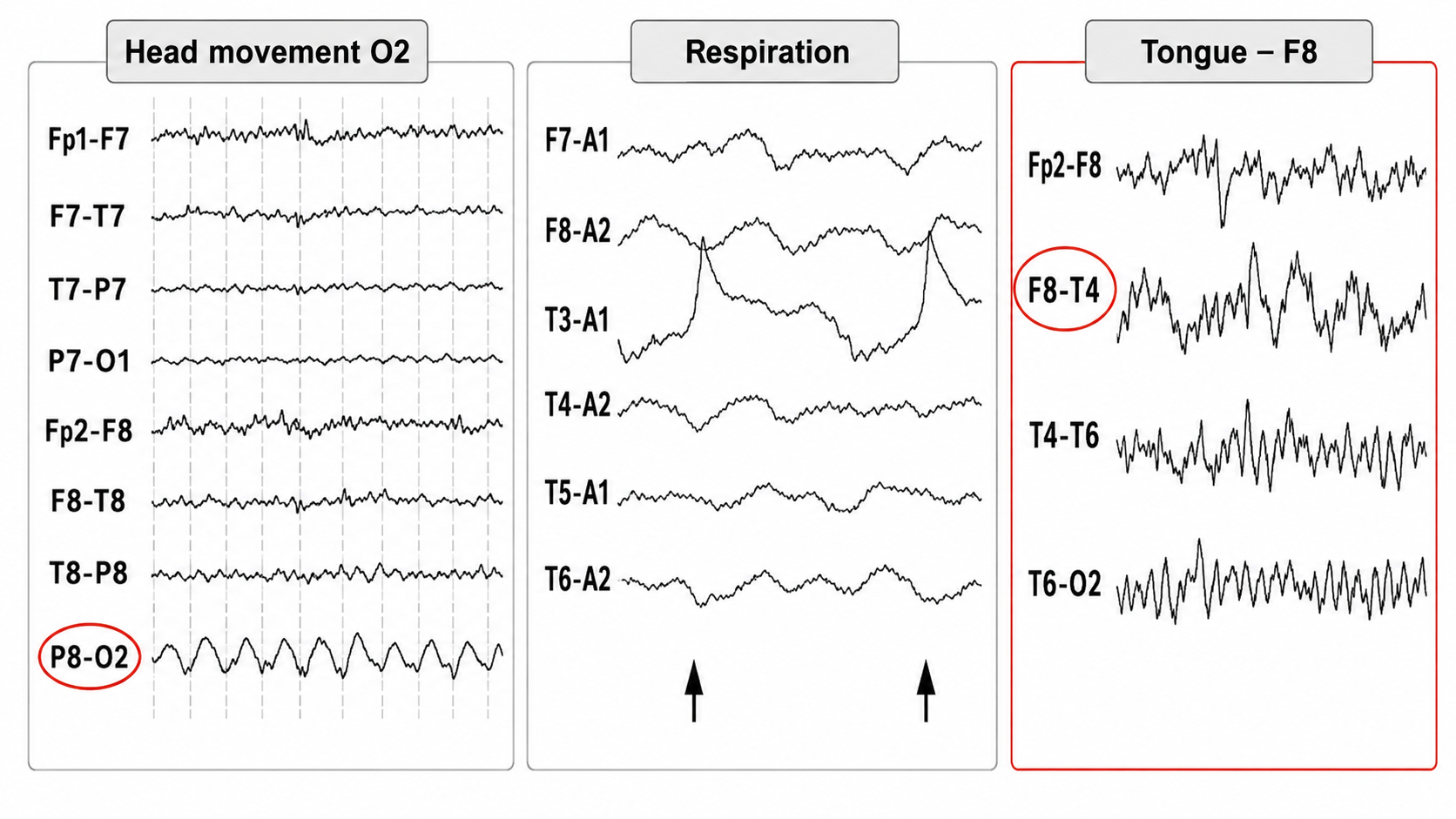
In the left panel, labeled “Head movement O2,” the most conspicuous abnormality is in the P8-O2 derivation. This channel shows a repetitive, relatively large-amplitude, slow rhythmic waveform that is not seen with comparable amplitude in the neighboring right temporal or left-sided channels. Because the affected channel includes O2, the pattern suggests movement or mechanical instability involving the right occipital electrode region. The waveform has a smooth, repetitive, mechanical quality rather than the spatially distributed field expected from a physiologic posterior rhythm. Its confinement to a posterior derivation and its regular movement-like morphology favor head movement or electrode motion near O2 rather than a focal occipital cerebral discharge.
The middle panel, labeled “Respiration,” shows slower rhythmic baseline fluctuations that correspond to breathing-related movement. The arrows mark respiratory cycles, and several channels show broad, slow deflections that rise and fall in a pattern compatible with chest, neck, head, or cable movement during respiration. This type of artifact may be more prominent in temporal or referential derivations, depending on electrode placement, wire tension, body position, and reference configuration. Unlike cerebral rhythmic activity, respiratory artifact tends to have a slow, periodic cadence tied to the breathing cycle, often with broad baseline shifts rather than organized cortical waveforms.
The right panel, labeled “Tongue – F8,” demonstrates a more irregular movement and muscle-related artifact, maximal in the F8-T4 derivation. The highlighted channel contains high-amplitude, jagged, irregular activity, with additional contamination in adjacent right anterior and temporal channels such as Fp2-F8 and T4-T6. This distribution suggests a source near the right anterior temporal/frontotemporal region, compatible with tongue movement, jaw activation, or nearby facial muscle activity affecting the F8 electrode region. The waveform is not sinusoidal or physiologically organized; instead, it is abrupt, uneven, and sharply irregular, which is typical of orofacial movement or electromyographic contamination.
Below is a BioGraph ® Infiniti cable movement artifact display. Note the two voltage spikes at the beginning of the recording.
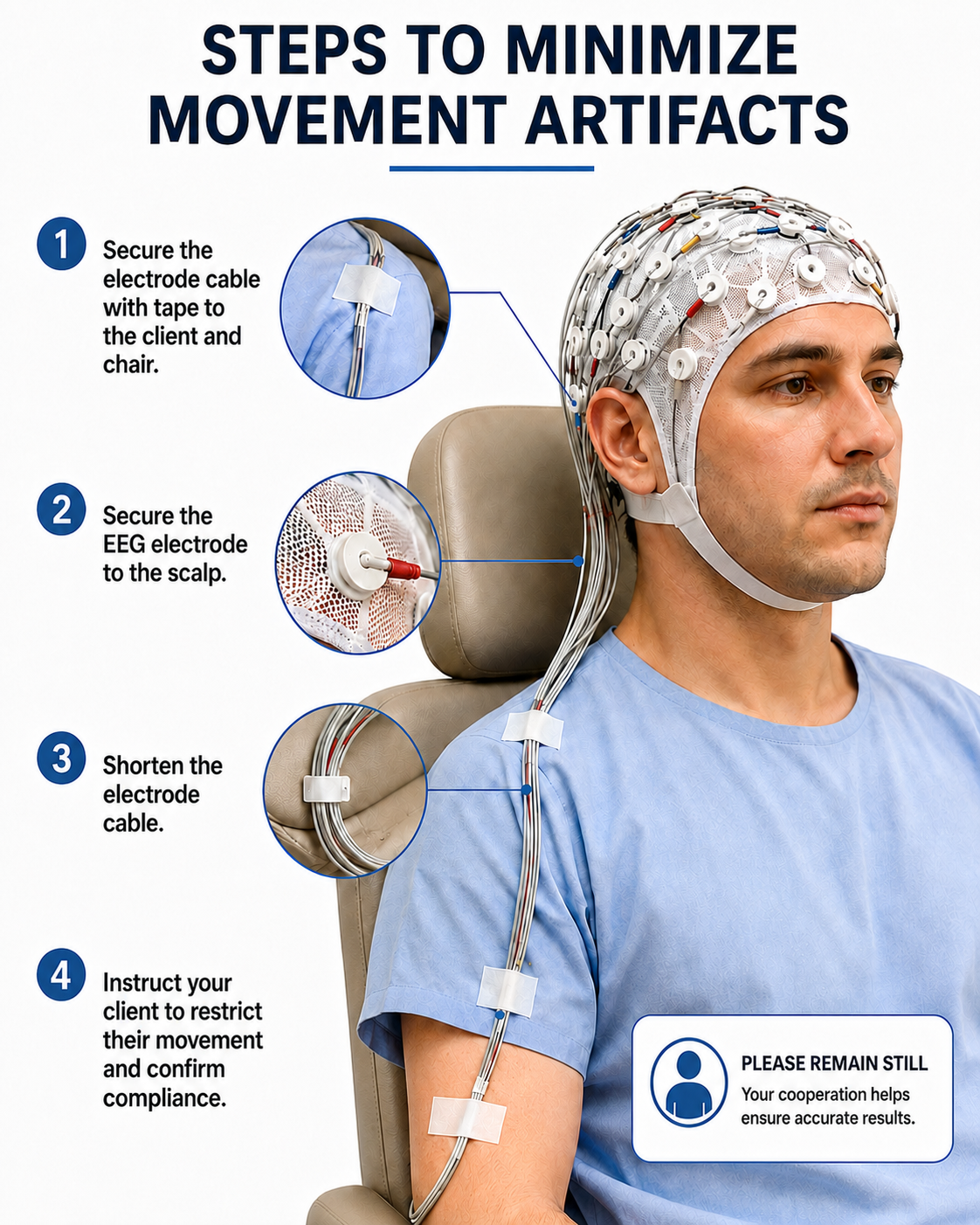
50/60 Hz and Field Artifacts
Both 50/60 Hz and field artifacts are external artifacts transmitted by nearby electrical sources such as power adapters for laptop computers or other electronic devices. While 60-Hz artifact is the primary concern in North America where AC voltage is transmitted at 60 Hz, 50-Hz artifact is the equivalent problem in regions that generate power at 50 Hz. Their fundamental frequency is 50 or 60 Hz, with harmonics at 100/120 Hz, 150/180 Hz, and 200/240 Hz.
An important complication is that a notch filter (a filter that suppresses a narrow band of frequencies) does not eliminate the problem. A notch centered at 50 or 60 Hz attenuates the fundamental but leaves the harmonics at 100/120 Hz and above untouched unless additional notches are applied, and the filter itself removes genuine cerebral activity within its stopband and can distort the phase and amplitude of nearby frequencies. Sharp notch filters can also produce ringing artifacts around abrupt transients. Separately, if the sampling rate and anti-aliasing filter are inadequate, line noise and its harmonics can be aliased down into lower frequencies where they masquerade as beta or even alpha activity. What a linear amplifier does not do is generate true subharmonics at half or a quarter of the line frequency; contamination reported at 25 Hz or 30 Hz is better explained by aliasing, intermodulation, or filter artifacts than by subharmonic generation. Because imbalanced electrode impedances defeat common-mode rejection, they increase an amplifier's vulnerability to line noise, which is why the durable fix is good, balanced electrode contact and removal of the interference source rather than reliance on the notch filter.
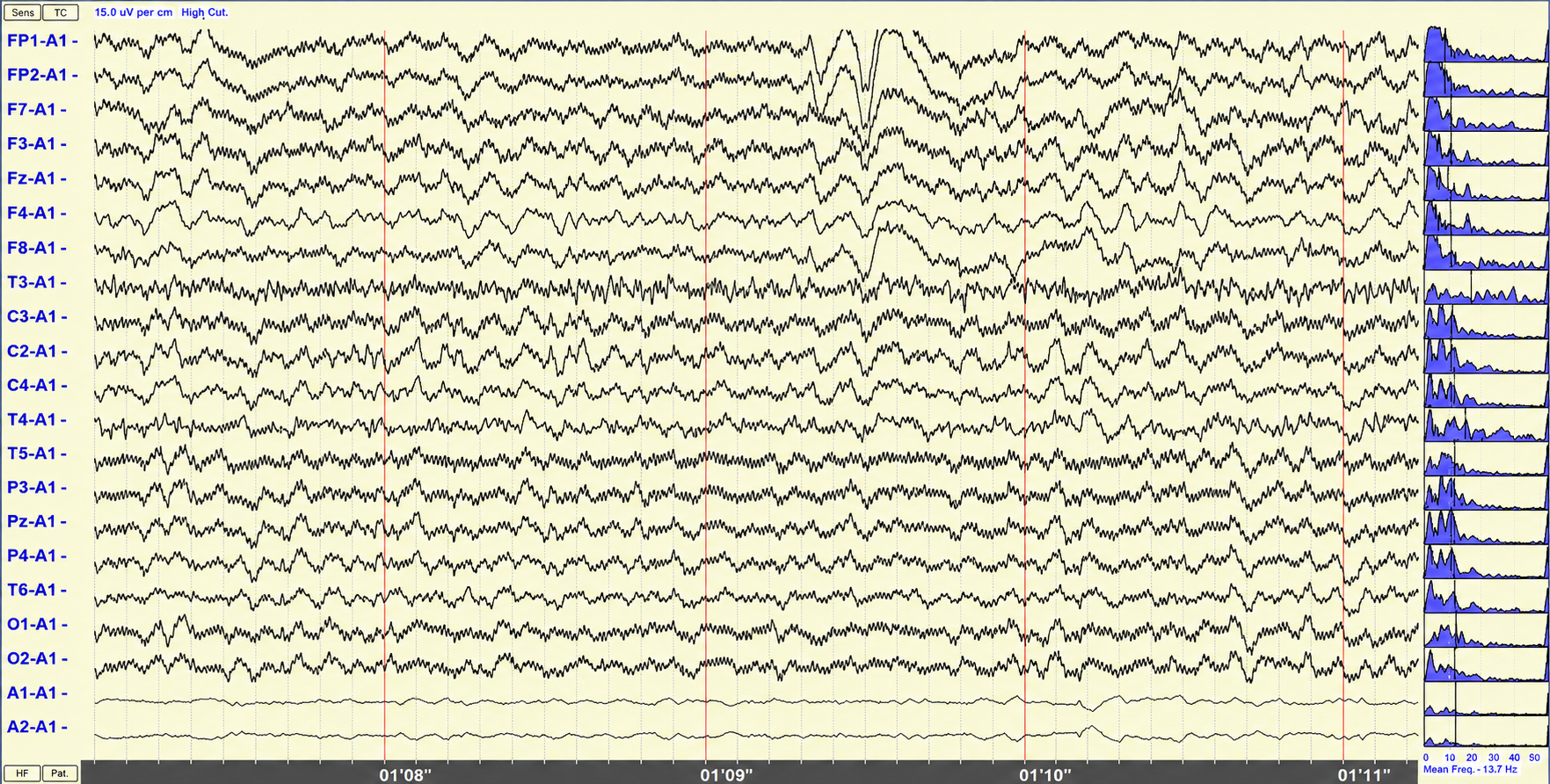
The 60-Hz artifact graphic © John S. Anderson. This EEG segment is shown in a referential montage in which the scalp electrodes are referenced primarily to A1, with a sensitivity of 15 µV/cm. The recording is heavily contaminated by a widespread, regular, high-frequency signal consistent with 60-Hz line-frequency artifact. The artifact appears as a fine, tightly spaced, nearly sinusoidal oscillation riding on top of the slower EEG background across many channels. Its uniformity and persistence distinguish it from physiologic beta activity, which is usually less mechanically regular, more variable over time, and more dependent on state, medication, or regional scalp muscle activity.
The contamination is broadly distributed across the montage rather than limited to one physiologic field. Channels from frontal, central, temporal, parietal, and occipital regions all show varying degrees of this fast regular activity. Because the montage is referential, a problem involving the reference, ground, electrode impedance balance, environmental electrical interference, or amplifier shielding can project the artifact widely across the recording. The A1-referenced layout is important because contamination affecting the reference pathway can make a technical problem appear generalized.
A BioGraph ® Infiniti display of 60-Hz artifact is shown below in red. Note the cyclical voltage fluctuations and 60-Hz peak in the power spectral display.
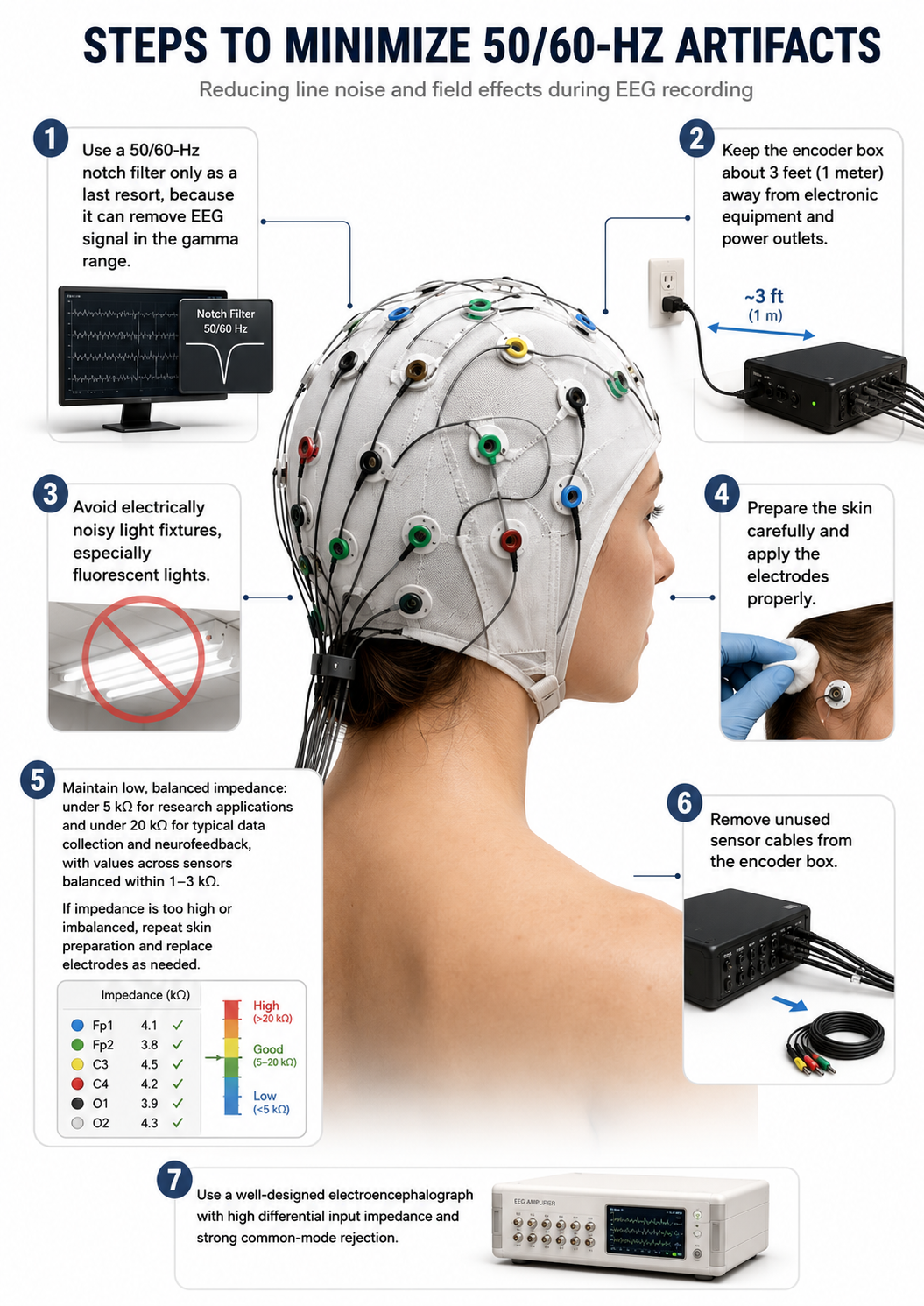
Radiofrequency Artifact
Radiofrequency (RF) artifact is contamination from external electromagnetic sources. The classic teaching that it radiates outward in a cone from the front of a display describes cathode-ray-tube televisions and monitors, which are now rare; contemporary LCD and LED displays do not emit in this way. In a modern clinic the practical RF sources are mobile phones and their transmitters, cordless phones, Wi-Fi and Bluetooth devices, wireless microphones, elevator and HVAC motors, and nearby medical equipment. The artifact typically appears and disappears abruptly, is mechanically regular, and does not respect physiologic fields, as the recording below illustrates.
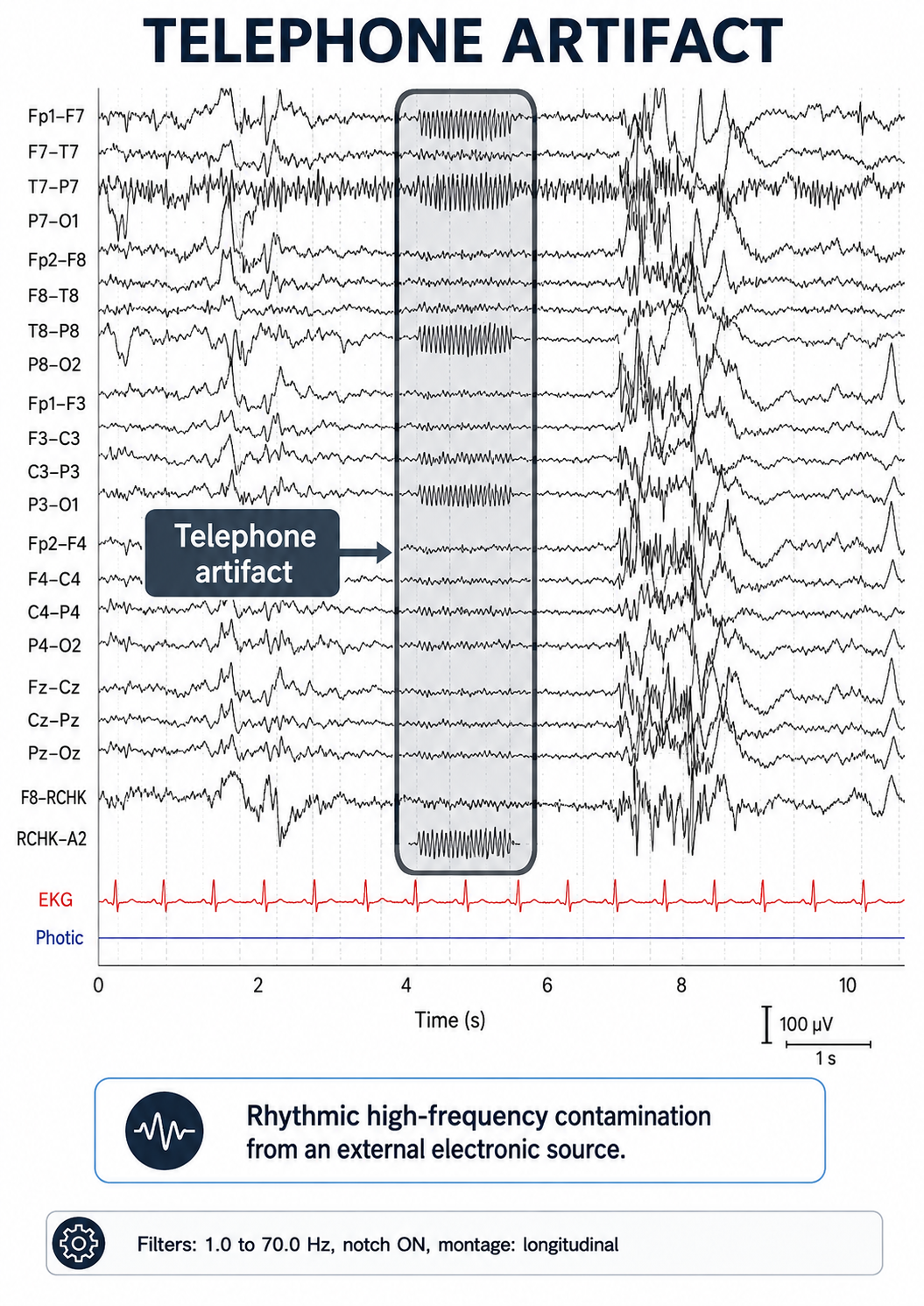
Graphic adapted from © eegatlas-online.com. This EEG segment demonstrates radiofrequency contamination, labeled here as a telephone artifact, in a longitudinal bipolar montage. The recording uses filters from 1.0 to 70.0 Hz with the notch filter turned on, and includes simultaneous EKG and photic channels. The artifact is most clearly visible in the boxed interval between approximately 4 and 6 seconds, where a rhythmic, tightly packed, high-frequency oscillation appears abruptly in several channels. Its sudden onset, nearly mechanical regularity, and abrupt disappearance strongly favor contamination from an external electronic source rather than physiologic cerebral activity.
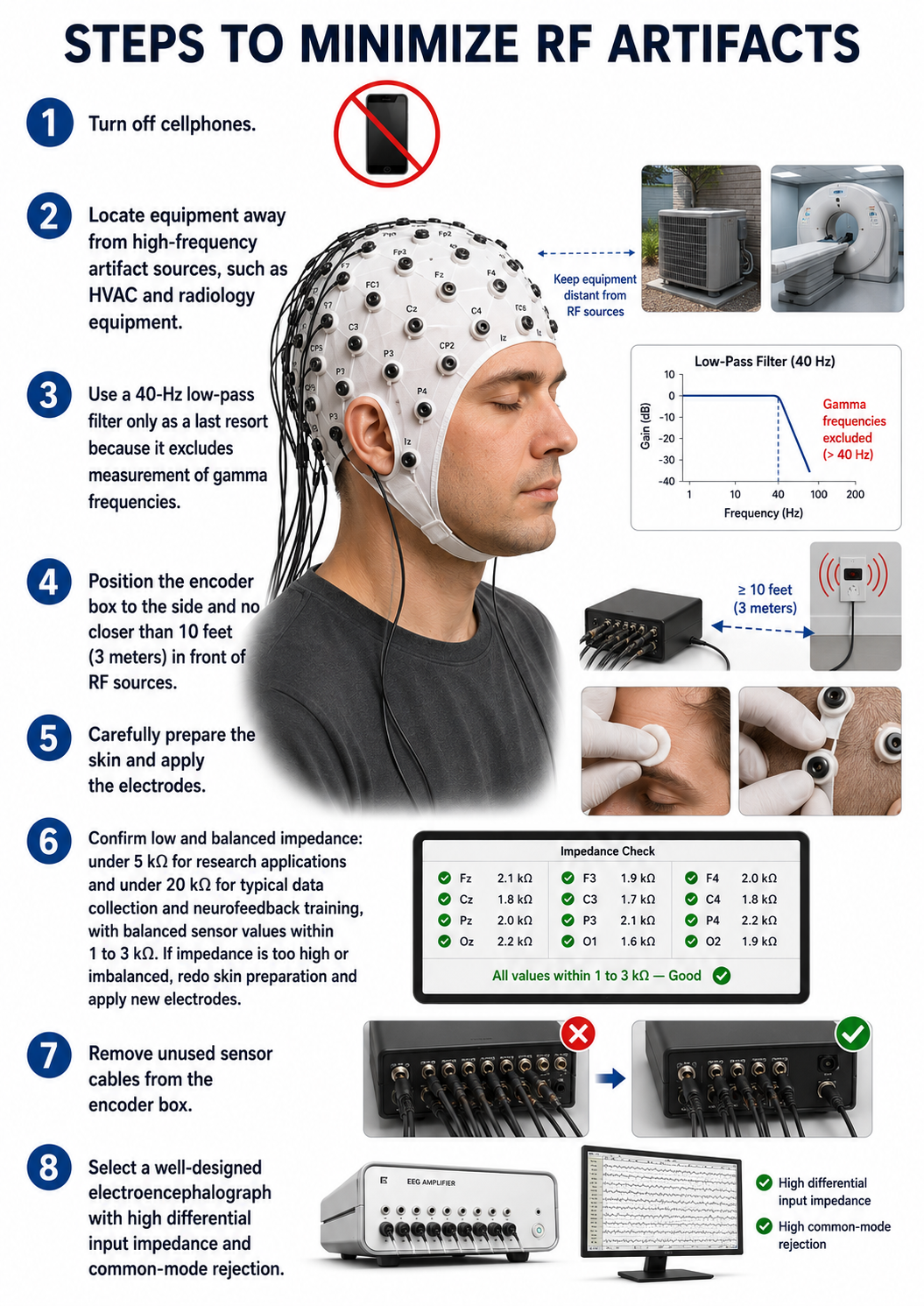
Electrode Artifacts
EEG recordings can be contaminated by several sources of electrode artifact. Even with proper care, electrode surfaces corrode and leads and connectors sustain damage over time. Electrodes are also subject to polarization, a chemical process at the electrode–electrolyte interface in which separated regions of positive and negative charge build up and reduce ion exchange. Polarization occurs at the electrode, not in the amplifier; what reaches the amplifier is a shifting DC offset and an unstable, elevated impedance. Using two different metals for the two inputs of a channel compounds the problem, because dissimilar metals have different half-cell potentials and generate a standing DC voltage difference that the differential amplifier cannot reject. Silver–silver chloride electrodes are preferred precisely because they are relatively nonpolarizing.
A common source of this problem is electrodes built on a base substrate—such as 3-D-printed plastic, brass, or copper—that is then electroplated with gold, silver, or a silver–silver chloride coating. Once repeated use and cleaning wear the coating through, the exposed circuit contains dissimilar metals (copper, brass, gold, silver, and so on), producing circuit and impedance problems (Kaveh et al., 2022).
Impedance Artifact
Unless skin-electrode impedance (the frequency-dependent opposition to an AC signal, measured in ohms and conventionally reported in kilohms) is low and balanced across sites, artifacts such as 50/60 Hz interference and movement can contaminate the EEG signal, as seen in the P3 and Pz electrodes in the graphic below. Published targets differ by application: ACNS Guideline 1 for clinical EEG specifies impedances between 100 Ω and 5 KΩ, research and evoked potential work commonly aims for under 5 KΩ, and neurofeedback practice guidance often accepts up to about 10–20 KΩ with modern high-input-impedance amplifiers, provided the values are matched within roughly 1–3 KΩ between sites. Regular impedance checks during setup and again at the end of a session ensure consistent contact quality.
It helps to understand why this balance matters, not just the target values. Recall that the differential amplifier removes shared noise such as 50/60 Hz interference through common-mode rejection, but it can do so only when the active and reference inputs present nearly identical impedances. When the two impedances differ, the same line noise produces slightly different voltages at each input, and that difference survives as a signal the amplifier treats as though it were genuine EEG (Demos, 2019). Low absolute impedance reduces overall noise pickup, while balanced impedance preserves the amplifier's ability to cancel it, which is why both conditions appear in the targets above. This mechanism is what the impedance question in the Assignment at the end of this unit asks you to explain.
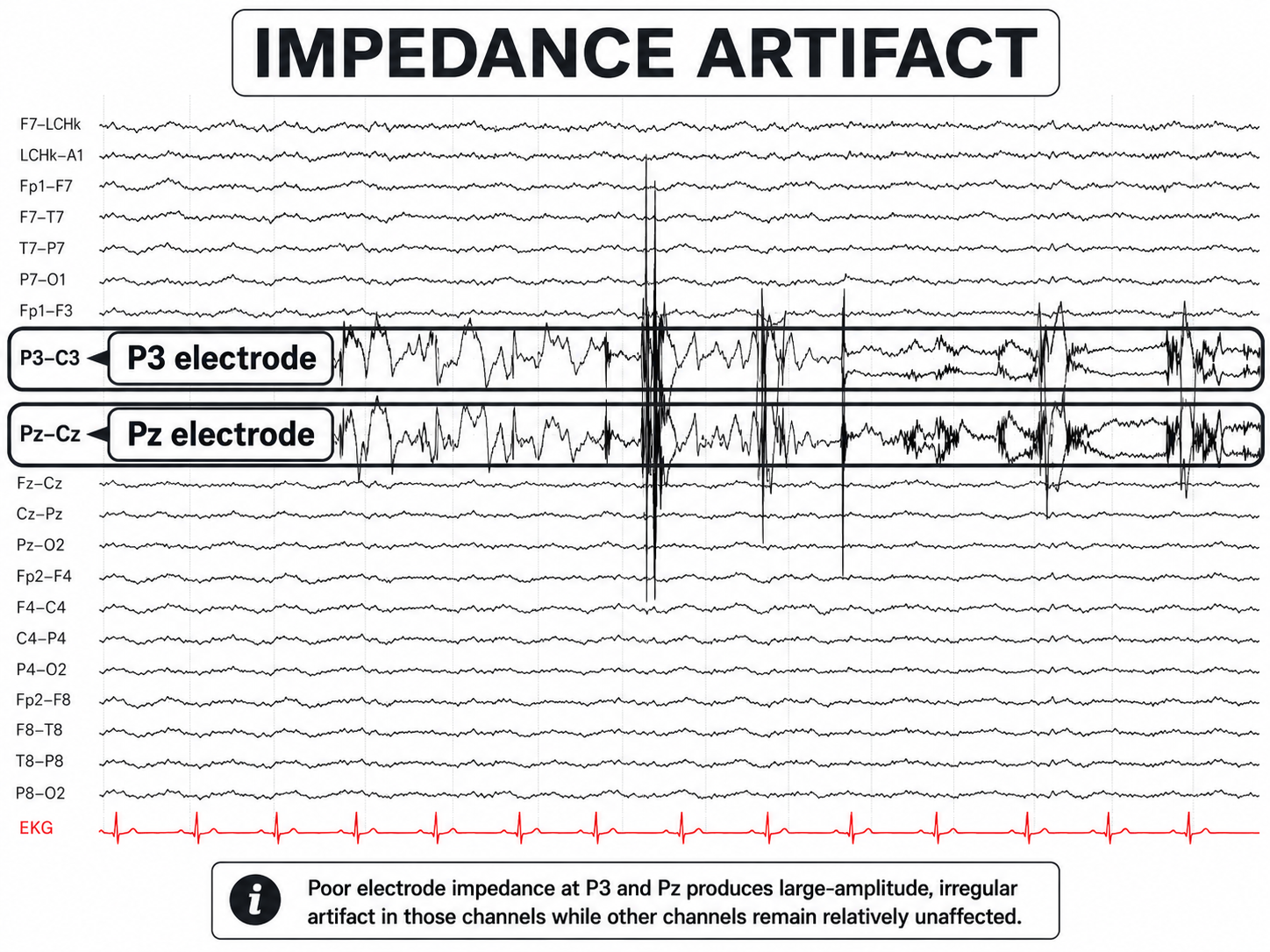
Graphic adapted from © eegatlas-online.com. The recording is displayed in a longitudinal bipolar arrangement with an EKG channel at the bottom. The red EKG tracing is regular and does not account for the large irregular activity in the highlighted EEG channels. The key abnormal-looking activity appears in the P3-C3 derivation and the Pz-Cz derivation, where the waveforms are much larger, more irregular, and more sharply unstable than the surrounding EEG background. These discharges fluctuate abruptly, with jagged high-amplitude deflections and intermittent vertical transients. Their morphology is not consistent with a normal cerebral rhythm, an evolving seizure pattern, or a reproducible epileptiform field.
Using abrasive gels or prepping the skin to reduce impedance is important, particularly in long-duration studies where skin conditions may change over time. However, infection control procedures must be enhanced whenever electrode attachment methods breach intact skin, due to the risk of disease transmission from bodily fluids. Modern high-input-impedance amplifiers have reduced the need for vigorous abrasion in many applications, but they have not eliminated the need for careful skin preparation: high absolute impedance still increases noise pickup, and impedance imbalance still defeats common-mode rejection regardless of how high the amplifier's input impedance is.
Electrode Pop Artifact
Even when impedance is low and balanced, mechanical disturbance can produce a distinctive artifact. Electrode pop artifact is a sudden, large deflection—classically a steep upstroke followed by a slower return to baseline—confined to the channels sharing a single electrode. It reflects an abrupt change in the electrode–electrolyte–skin junction, such as a loose or partially detached electrode, a bubble or void in the gel or paste, drying paste, or a tug on the lead wire. The defining feature is that the junction's standing potential shifts suddenly; despite the name, no spark or electrical discharge occurs. Its diagnostic hallmark is the complete absence of a physiologic field: the deflection appears only in derivations containing the offending electrode and does not spread to neighboring sites.
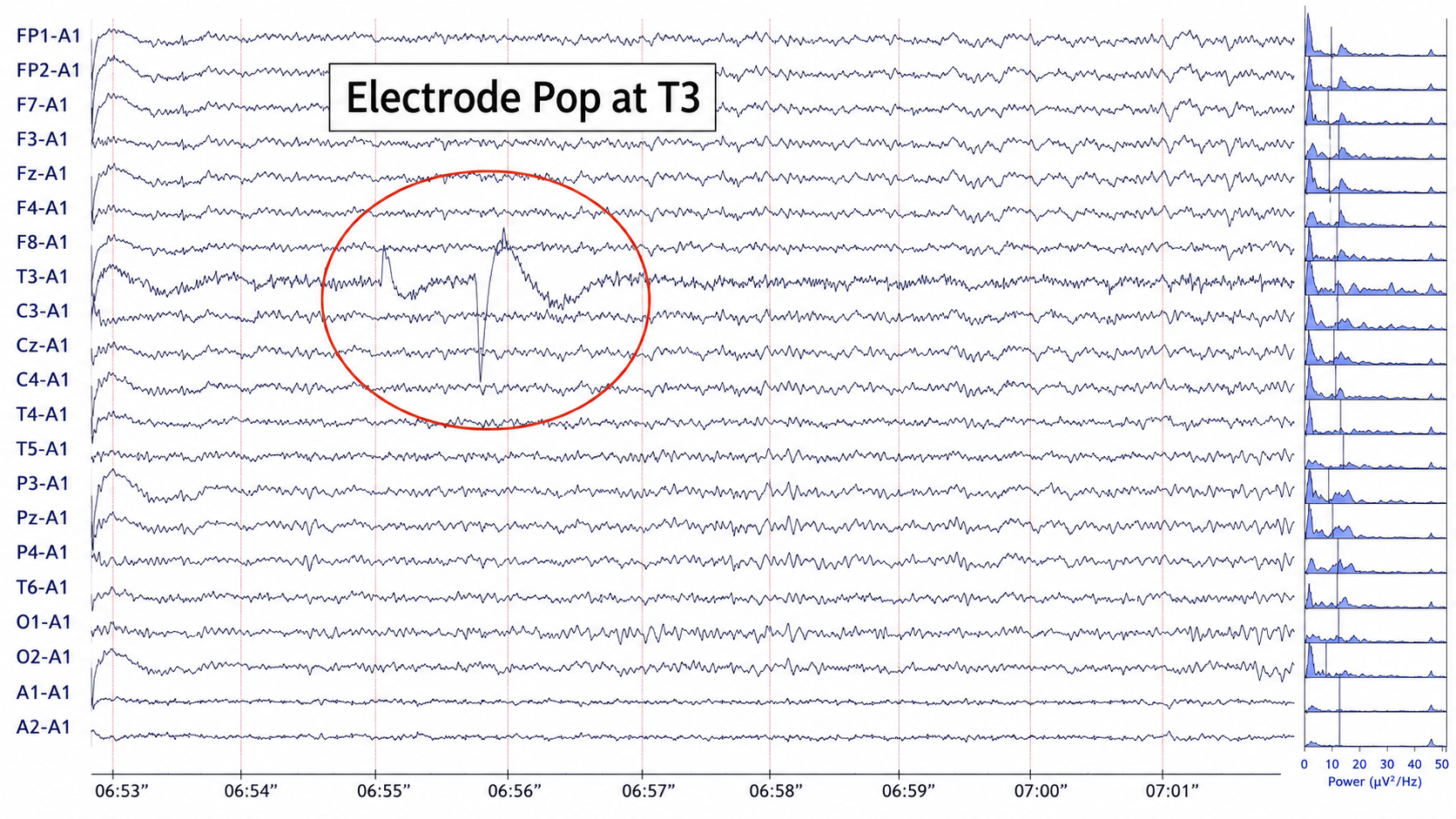
Graphic © John S. Anderson. This EEG segment shows an electrode-pop artifact localized to the T3 electrode, displayed in a referential montage with most channels referenced to A1. The circled event occurs around 06:55 to 06:56 and is most conspicuous in the T3-A1 channel, where there is an abrupt, high-amplitude, sharply contoured voltage excursion followed by slower baseline recovery. Historically, this type of artifact has been recognized as a common technical pitfall in EEG because sudden changes at the electrode–scalp interface can create waveforms that look strikingly sharp or paroxysmal, yet are not generated by cerebral cortex.
The morphology is typical of an electrode pop. The waveform begins suddenly, has a steep vertical component, and is followed by a slower, irregular return toward baseline. This combination of an abrupt transient and subsequent baseline drift suggests a sudden impedance change or intermittent loss and recovery of electrode contact. Common technical causes include drying conductive paste, a loose electrode, tugging on the lead wire, sweat or motion at the electrode site, or a brief mechanical shift at the scalp–electrode interface. Because the affected electrode is T3, the artifact appears most prominently in the T3-A1 derivation.
Recognizing Normal EEG Patterns
This section covers normal EEG patterns, including the posterior dominant rhythm, the effects of eyes-open and eyes-closed conditions, developmental changes in the EEG across the lifespan, and diurnal influences. Understanding what "normal" looks like is essential, because you cannot identify pathology or training targets without first recognizing the healthy baseline.
Normal EEG Patterns
The healthy adult EEG is a cerebral symphony composed of delta, theta, alpha, sensorimotor rhythm, beta, and gamma activity. Delta predominates in deep sleep and is normal there, although prominent waking delta in an adult is abnormal. These rhythms correlate with behavioral states (attentiveness, sleeping, waking, seizures, and coma), occur in distinct frequency ranges, and are characterized by synchrony and desynchrony. Synchrony means that pools of neurons coordinate their firing through pacemakers and mutual coordination. Desynchrony means that pools of neurons fire independently, driven by stimulation of specific sensory pathways up to the midbrain and high-frequency stimulation of the reticular formation and nonspecific thalamic projection nuclei.

Synchrony graphic revised from Bear, Connors, and Paradiso (2002).
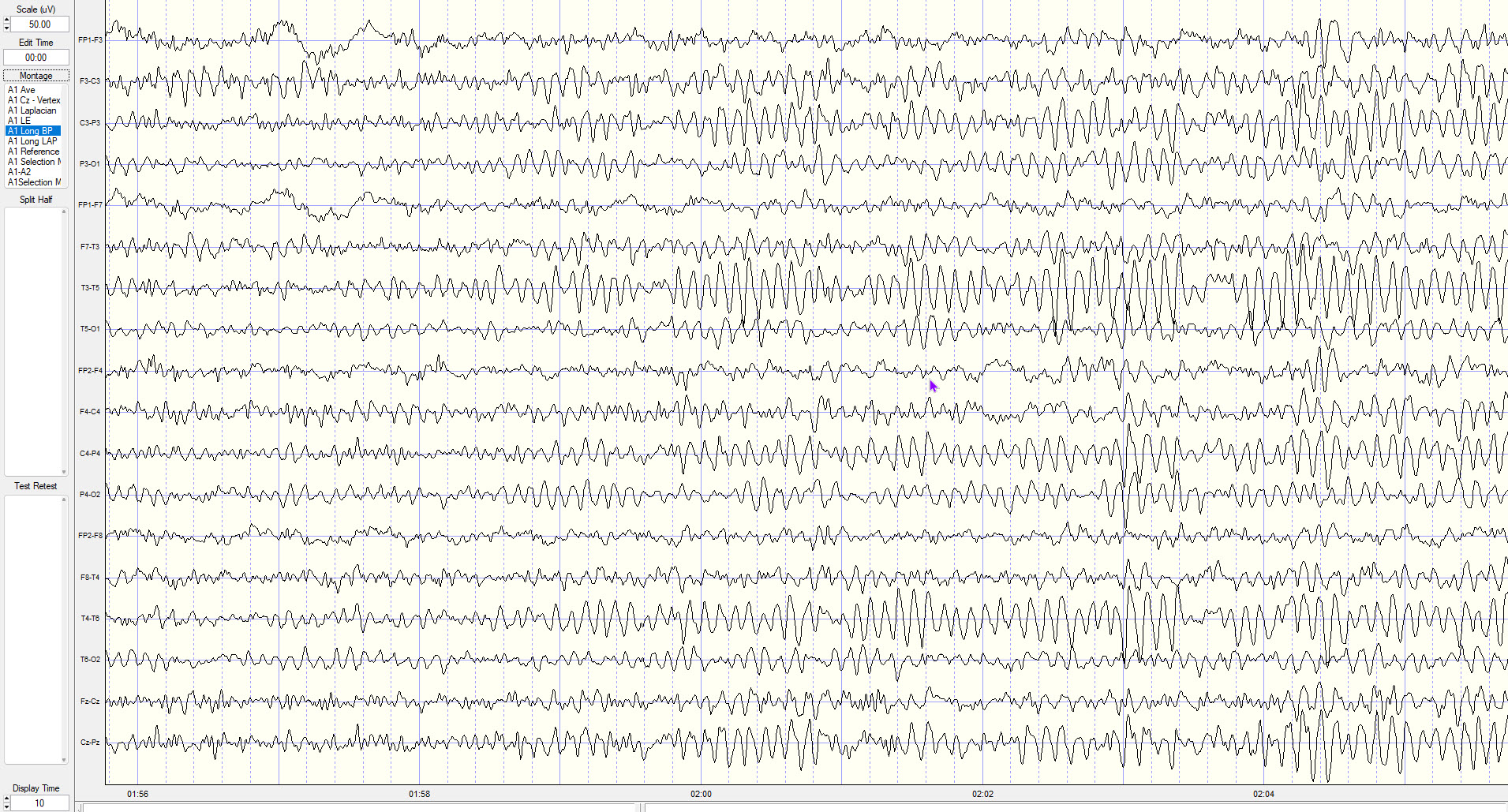
Synchronized EEG graphic © John S. Anderson.
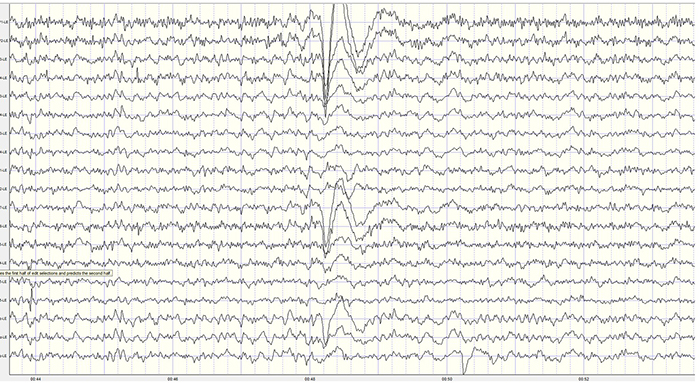
Desynchronized EEG graphic © John S. Anderson.
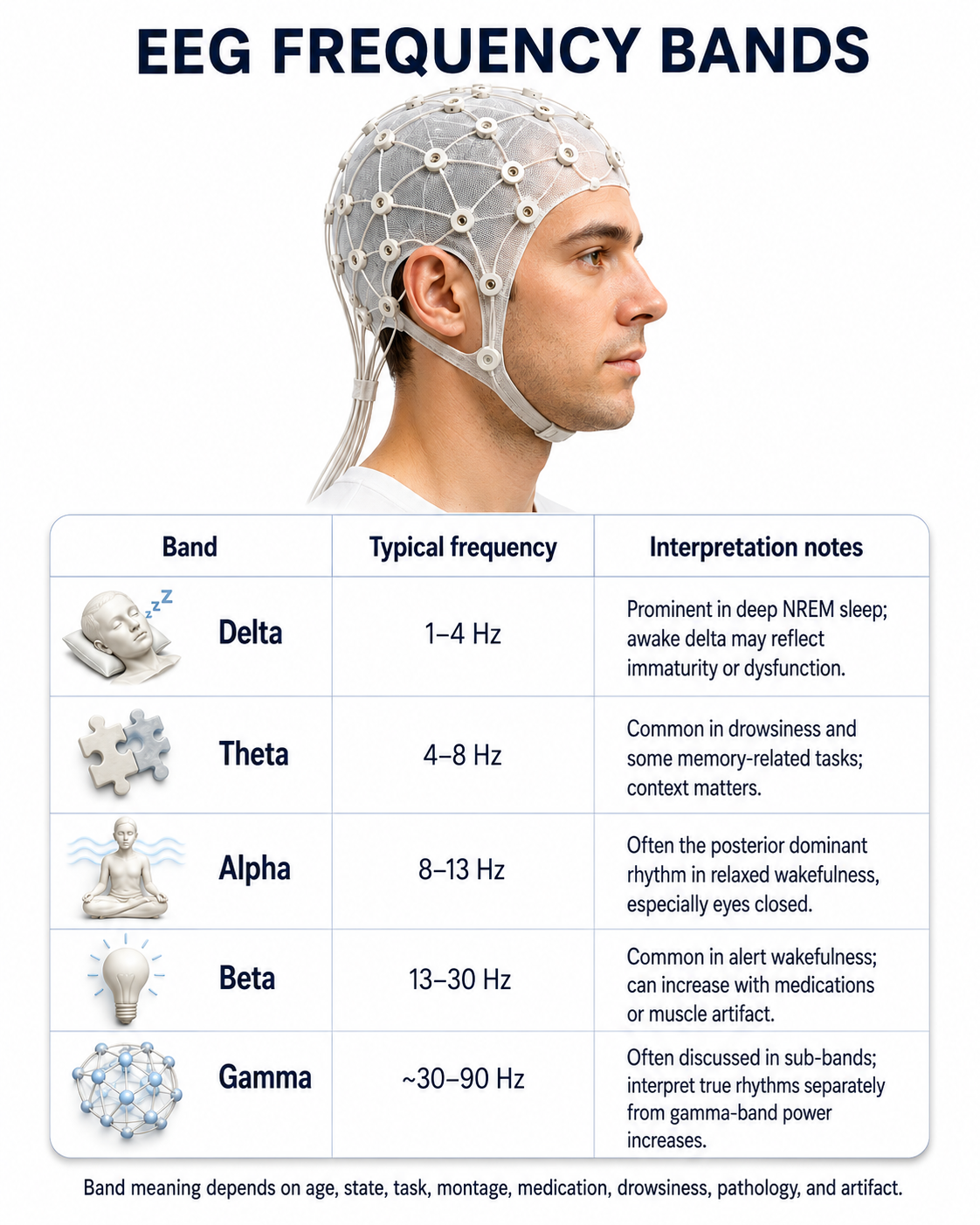
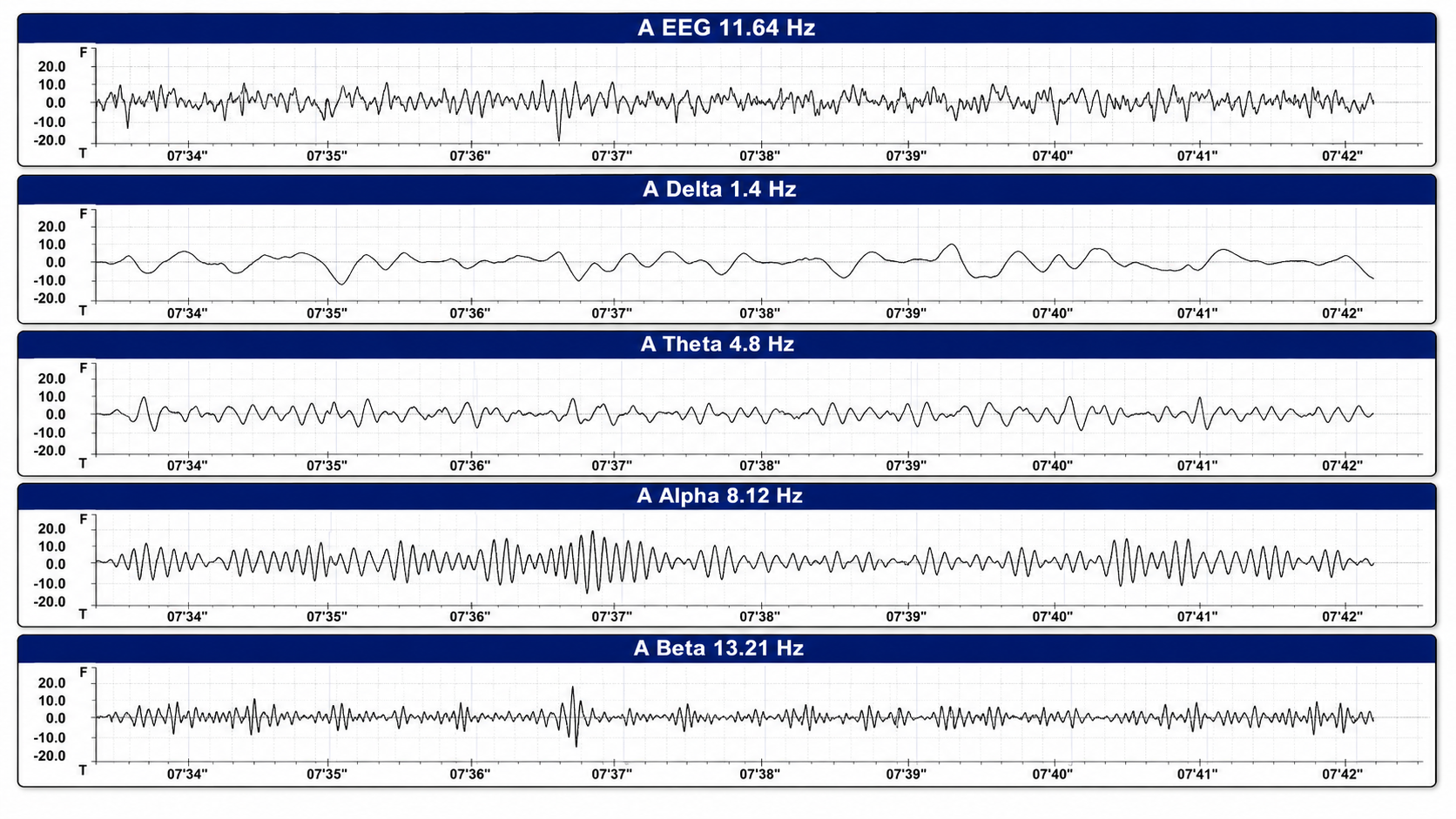
This EEG display illustrates how a raw EEG waveform is composed of multiple frequency components. The raw trace is not interpreted by frequency alone; rather, its appearance reflects the combined contribution of slow delta activity, intermediate theta activity, organized alpha activity, and faster beta activity. The alpha band appears especially organized in this example, while delta and theta provide slower background fluctuations and beta contributes smaller faster activity. There is no clear seizure evolution, spike-and-wave discharge, or definite epileptiform pattern visible in this band-separated display.
Effect of Eyes Open and Closed Conditions on the EEG
The alpha rhythm is strongly modulated by visual input. Opening the eyes blocks or attenuates the posterior alpha rhythm, a phenomenon Hans Berger first described in his 1929 report and now called alpha-blocking or the Berger effect, in which the alpha rhythm gives way to low-amplitude, desynchronized faster activity during movement, attention, mental effort, or visual processing. In contrast, alpha is most prominent during relaxed, drowsy-free wakefulness with the eyes closed (Thompson & Thompson, 2015). This alpha reactivity is one of the first things clinicians look for when evaluating an EEG, because a reduced or absent response can indicate neurological dysfunction.
The movie below is a 19-channel BioTrace+ /NeXus-32 display of eyes open and closed EEG © John S. Anderson. Note the appearance of alpha activity with eyes closed at about 14 seconds and alpha-blocking with eyes open at about 45 seconds.
The graphic below illustrates alpha-blocking and was uploaded to ResearchGate by the author, Byoung-Kyong Min. The two trials show alpha-blocking during eyes-open conditions.
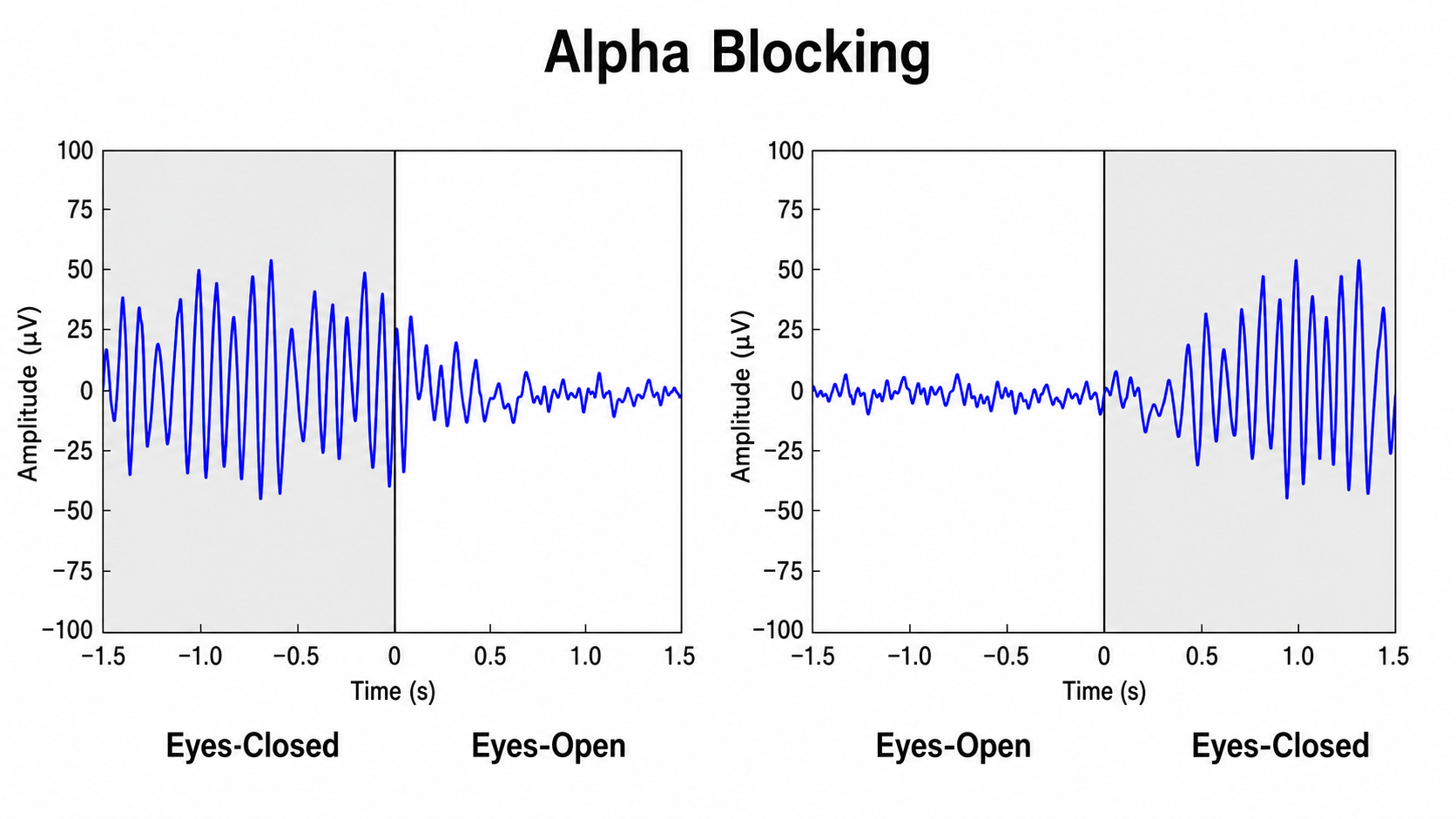
This figure demonstrates alpha blocking, also known historically as the Berger effect, in which the posterior alpha rhythm attenuates when the eyes open or when visual attention increases. The display contains two time-domain examples with amplitude shown in microvolts and time centered at zero seconds. In the left panel, the subject begins in an eyes-closed condition, shown by a prominent rhythmic alpha activity with relatively regular oscillations reaching roughly 40–50 µV. At the vertical transition line marking eye opening, the alpha rhythm rapidly attenuates, becoming lower in amplitude and more irregular. This is the classic alpha-blocking response: a synchronized posterior rhythm present during relaxed eyes-closed wakefulness is suppressed by eye opening and visual engagement.
The right panel shows the reciprocal pattern. During the eyes-open condition before zero seconds, the tracing is low amplitude and relatively desynchronized, with no sustained alpha rhythm. After the eyes close, a rhythmic alpha pattern gradually emerges, increasing in amplitude and regularity over the next several hundred milliseconds. This illustrates alpha reactivity rather than abnormal slowing. The rhythm does not appear abruptly as an epileptiform event, does not evolve like a seizure pattern, and does not have spike-and-wave morphology. Instead, it reflects a normal state-dependent shift in cortical rhythm organization.
Posterior Dominant Rhythm
The posterior dominant rhythm (PDR) is the dominant, reactive rhythm recorded over the posterior head regions during relaxed, eyes-closed wakefulness, and it must attenuate with eye opening to qualify as the PDR. Two different standards are in circulation, and it is important not to confuse them. In clinical electroencephalography, the normal adult PDR falls between 8 and 13 Hz, and a frequency below 8 Hz in an awake adult is the accepted criterion for abnormal slowing (Niedermeyer & da Silva, 2005). Some neurofeedback authors use a narrower window of interest, treating values outside roughly 9 to 11 Hz as clinically noteworthy and worth correlating with medication use or symptoms such as anxiety (Demos, 2019). A PDR of 8.5 Hz is therefore within normal limits clinically, even though a neurofeedback practitioner might flag it for follow-up.
In clinical settings, the presence, frequency, reactivity, and symmetry of the PDR are key indicators of neurological health. A slower PDR frequency is a nonspecific finding that can accompany drowsiness, medication effects, metabolic disturbance, or cognitive decline including Alzheimer's disease, so it should never be interpreted in isolation. Evidence linking a higher-than-average PDR frequency to heightened arousal is weaker; PDR frequency is relatively stable within an individual and is influenced substantially by age and heredity. The symmetry of the PDR across hemispheres is another important consideration, as a persistent amplitude asymmetry greater than about 50 percent, or any frequency asymmetry, may indicate structural abnormalities such as stroke, tumor, or traumatic brain injury.
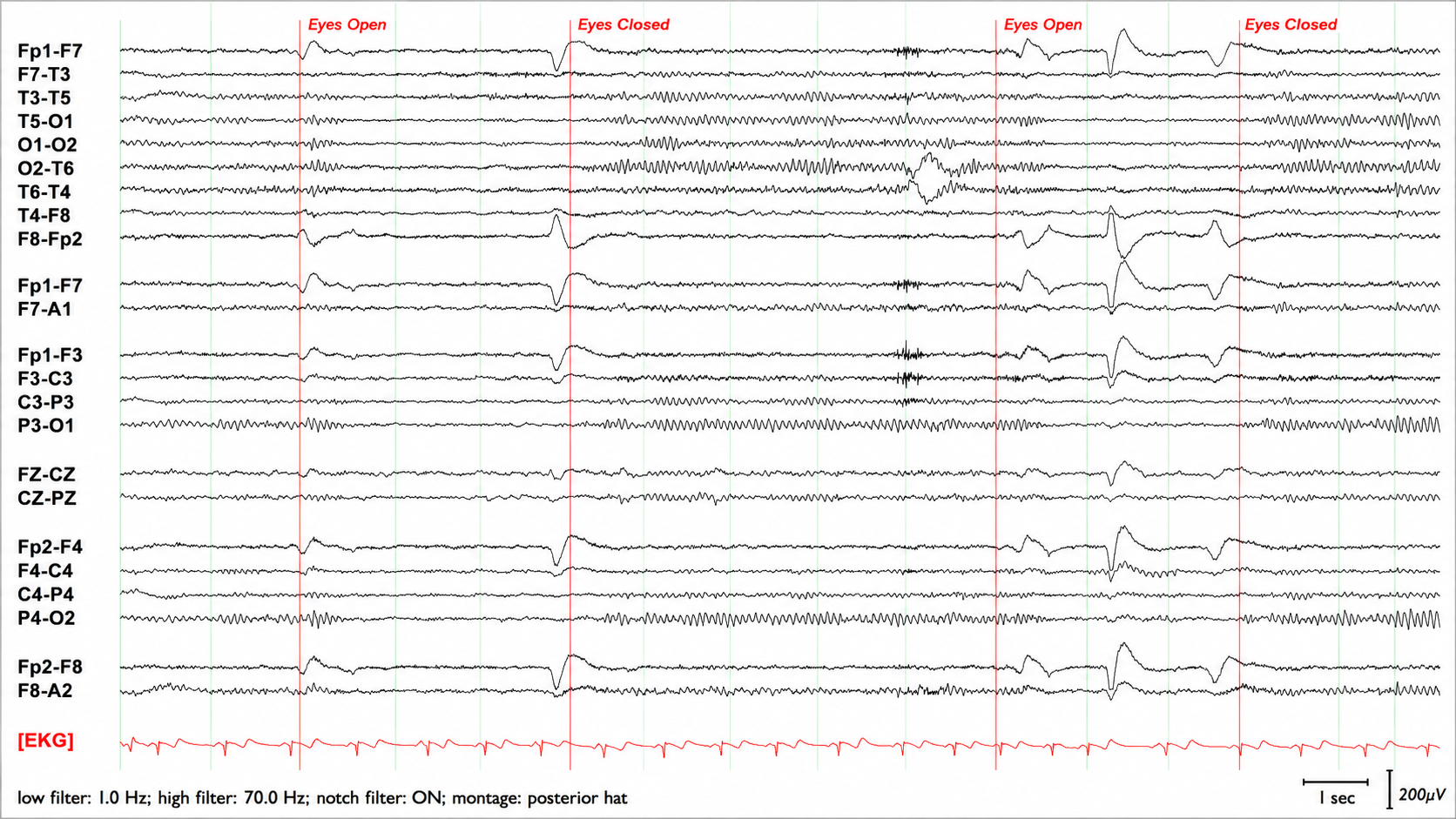
Graphic adapted from © eegatlas-online.com. This EEG recording demonstrates a posterior dominant rhythm, or PDR, with clear reactivity to eye opening and eye closure. The tracing is displayed in a posterior-oriented montage with a low-frequency filter of 1.0 Hz, a high-frequency filter of 70.0 Hz, the notch filter turned on, and a simultaneous EKG channel at the bottom. The red vertical markers indicate changes in eye state, alternating between eyes open and eyes closed. Historically, the PDR has been one of the foundational features of routine EEG interpretation because it provides a visual marker of wakeful background organization, especially over the occipital and posterior parietal regions during relaxed eyes-closed wakefulness.
During the eyes-closed portions of the recording, a rhythmic alpha-frequency pattern becomes prominent over the posterior derivations. It is most evident in channels involving the occipital and posterior temporal regions, including T5-O1, O1-O2, O2-T6, P3-O1, P4-O2, and related posterior chains. The rhythm appears regular, sinusoidal, and sustained, with a visually estimated frequency in the alpha range, approximately 8–12 Hz. Its posterior predominance and reproducible appearance after eye closure support interpretation as the PDR rather than generalized rhythmic artifact or epileptiform activity.
During the eyes-open portions, the posterior alpha rhythm attenuates substantially. The posterior channels become lower in amplitude and less rhythmically organized, showing relative desynchronization compared with the eyes-closed state. This attenuation with eye opening is the expected alpha-blocking response, sometimes historically referred to as the Berger effect. The repeated alternation in this recording is important: when the eyes close, the PDR reappears; when the eyes open, it suppresses. This state-dependent reproducibility supports a physiologic reactive posterior rhythm.
Developmental Aspects of the EEG
The EEG changes dramatically across the lifespan, reflecting the progressive maturation of brain structures. Slow activity predominates in infancy and early childhood, and the dominant background frequency rises steadily through childhood into adolescence, reaching adult values around 10 Hz by the early teens. This progression mirrors the maturation of thalamocortical circuits, which play a key role in generating rhythmic brain activity.
These developmental shifts reflect the increasing differentiation of cortical and subcortical structures, the growth of longer-distance network connections, and enhanced communication between brain regions as each area begins to specialize for processing sensory input, executive tasks, and other functions. Peak alpha frequency declines modestly during later adulthood (Thompson & Thompson, 2015). Published developmental milestones for the PDR vary somewhat by source; Demos (2019) gives approximately 6 Hz at 1 year, 8 Hz at 8 years, 9 Hz at 10–12 years, and 10 Hz at 13–14 years, while the standard clinical neurophysiology literature places the 8 Hz milestone earlier, at about age 3, with 9 Hz reached near age 9 (Niedermeyer & da Silva, 2005). Use the norms that accompany whichever database or reference text you are working from, and do not treat a single milestone table as definitive.
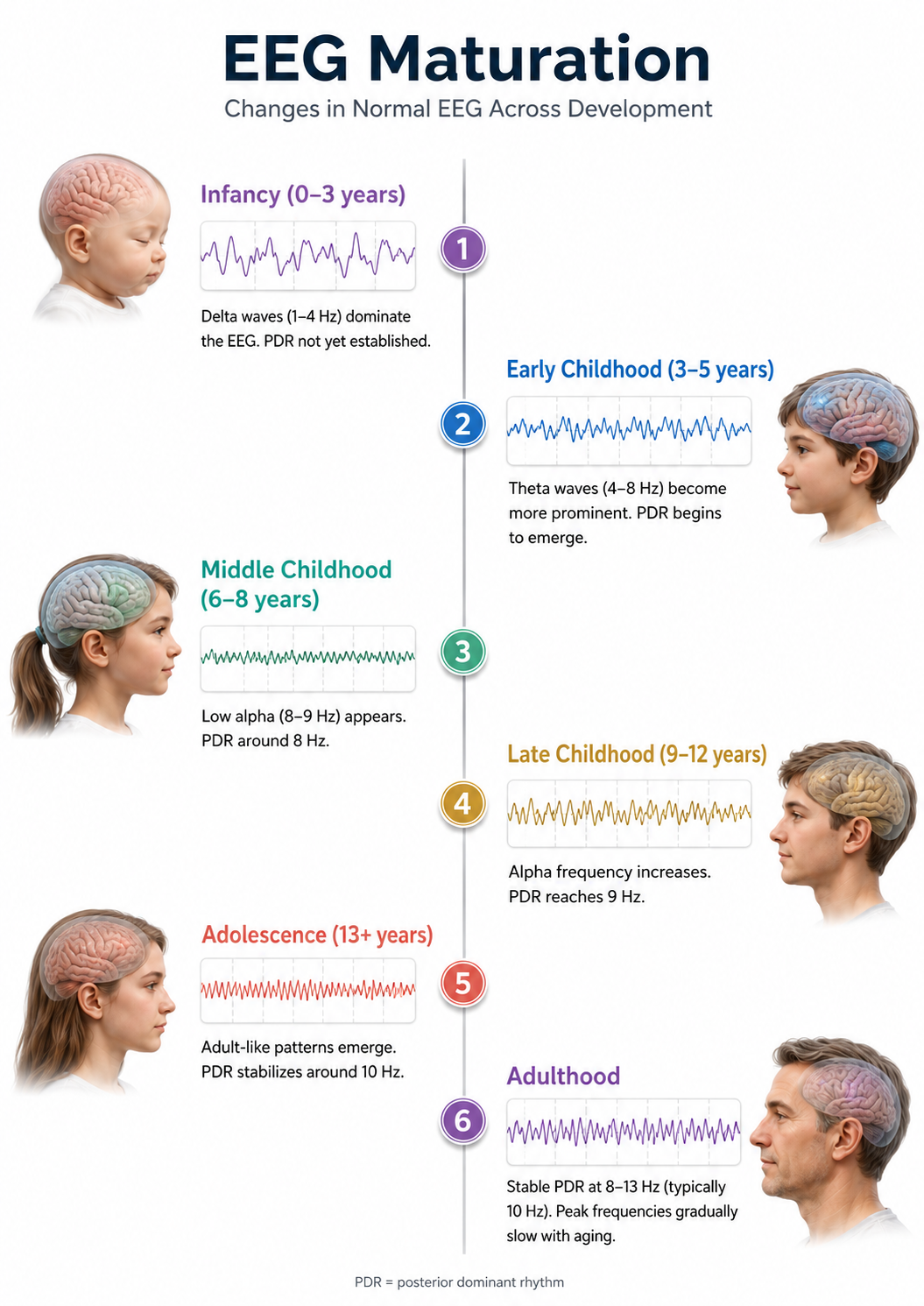
Diurnal Influences on the EEG
Alpha and theta amplitudes vary across the day. Thompson and Thompson (2015) report the highest values near 11 am, 1 pm, and 3 pm and note that fatigue and individual differences shape the magnitude and timing of these changes. Treat these specific clock times as illustrative rather than fixed: the underlying literature is small, and peak times depend on each person's sleep schedule and circadian phase. The practical implication is robust regardless of the exact hours—serial assessments should be conducted at the same time of day so that diurnal fluctuation is not mistaken for treatment effect.
Evaluation of Subject Variables During Acquisition
Subject variables are crucial to the interpretation of EEG measurements. This section examines the importance of alertness-drowsiness, physical relaxation, and anxiety. The effects of eyes closed/eyes open were covered above, and medication effects are addressed in the Psychopharmacology unit. As a reminder, benzodiazepines, which enhance GABAergic inhibitory neurotransmission, characteristically produce prominent frontocentral beta activity while attenuating and destabilizing the posterior alpha rhythm; they do not increase PDR amplitude. Caffeine likewise tends to reduce alpha power. Understanding these pharmacological effects is essential for accurate EEG interpretation in medicated patients.
Alertness-Drowsiness
A client's age determines how drowsiness is expressed in the EEG. Many children present with hypnagogic hypersynchrony as they fall asleep. This is the abrupt appearance of high-amplitude (commonly 100–350 µV), rhythmic, sinusoidal 3–5 Hz theta and delta activity, maximal frontocentrally, and it is a normal finding despite being mistaken for epileptiform activity by inexperienced readers. It appears from roughly 3 months of age, is most common between about 6 months and 6 years, and becomes rare after age 12. Note that it consists of high-amplitude slow bursts, not low-amplitude spikes. Beta activity between 20 and 25 Hz also appears maximally at central and posterior sites in drowsy infants and young children. When older children and adults become drowsy or enter stage N1 and N2 sleep, frontocentral beta may be activated (Fisch, 1999).
Adult EEG drowsiness patterns increasingly appear by age 10. Slow lateral eye movements are associated with 1-Hz (or slower) waveforms detectable with greatest amplitude and reverse polarity at F7 and F8. Continued drowsiness may produce 1–2 Hz slowing of the alpha rhythm, making it crucial to confirm client wakefulness when assessing alpha rhythm frequency (Fisch, 1999). From ages 10 to 20, drowsiness is often accompanied by rhythmic frontal theta (Fisch, 1999).

Graphic © fizkes/Shutterstock.com.
Physical Relaxation
The human stress response is multidimensional, involving diverse systems from the central nervous system to the immune system. Each person responds uniquely to stressors, a phenomenon called response stereotypy. Individuals differ in which physiological systems are activated or suppressed, the degree of these changes, and the impact on their health.
Because clients show widely different response patterns, assessment should monitor multiple physiological channels, including blood volume pulse (BVP) for heart rate and heart rate variability, electromyography (EMG), a respirometer for respiration rate and pattern, skin conductance (SC), and skin temperature. A capnometer, which measures end-tidal CO2, can complement a respirometer by detecting CO2 reductions due to overbreathing, a more subtle process than overt hyperventilation (Khazan, 2019). Normative values for these measures can be found in Moss and Shaffer's (2019) Physiological Recording Technology and Applications in Biofeedback and Neurofeedback.
Stress responses that affect physiologic activity outside the CNS can generate artifacts in EEG recordings. When client distress produces excessive artifact, a professional may need to coach the client to relax using one or more biofeedback modalities before proceeding. Clients should be monitored in a comfortable but upright position.
Anxiety
Anxious clients are frequently described as showing decreased alpha and increased beta activity, with some neurofeedback sources citing bands as narrow as 19–21 Hz or 20–23 Hz (Thompson & Thompson, 2015). Treat these narrow bands as clinical observations rather than established findings: there is no validated EEG biomarker for anxiety, the reported band limits differ across sources, and increased beta is difficult to separate from scalp EMG, which anxious clients produce in abundance. Conversely, anxious adults diagnosed with ADHD may show increased alpha activity, a reminder that anxiety's EEG signature is not uniform. Even without perceptible sweating, anxious patients may present with intermittent biphasic slow-wave activity of skin-potential origin (Picton & Hillyard, 1972). Clients who experience panic may exhibit paroxysmal EEG activity (Thompson & Thompson, 2015).

Graphic © Peshkova/Shutterstock.com.
Glossary
50/60 Hz: external artifacts transmitted by nearby electrical sources.
active electrode: an electrode placed over a site that is a known EEG generator like Cz.
alpha-blocking (Berger effect): the attenuation of the alpha rhythm and its replacement by low-amplitude desynchronized faster activity during eye opening, movement, attention, mental effort such as complex problem-solving, and visual processing.
amplitude: the strength of the EEG signal, measured in microvolts (µV). Power, a related but distinct measure, is proportional to amplitude squared and is expressed in µV² (which some software labels picowatts).
artifact: any signal in an EEG recording that does not originate from cerebral activity, whether physiological (muscle, eye, cardiac, sweat) or exogenous (line noise, movement, electrode problems).
artifacting: the systematic review of the raw EEG and removal or exclusion of contaminated epochs before quantitative analysis.
asynchronous waves: neurons depolarize and hyperpolarize independently.
average reference montage: an EEG referencing technique in which each electrode is referenced to the arithmetic mean of all scalp electrode potentials; it replaces a single physical reference with a computed one and is well suited to assessing diffuse activity and hemispheric symmetry, but it is distorted by any single noisy electrode.
Bell's phenomenon: the upward and outward rotation of the eye during lid closure, which carries the positive cornea toward the frontopolar electrodes and produces a large frontal deflection.
bipolar montage: a montage in which each EEG channel represents the voltage difference between two adjacent scalp electrodes.
bridging artifact (salt bridge): a low-resistance conductive path between adjacent electrodes, caused by excessive electrode paste or gel, heavy sweating, or a wet scalp, that leaves nearly no voltage difference between the bridged sites.
cable sway: movement artifact caused specifically by the movement of electrode cables.
cardiac artifact: the contamination of the EEG by the ECG signal.
channel: an EEG amplifier output that is the result of scalp electrical activity from three electrode/sensor connections to the scalp.
coherence: the consistency of the phase and amplitude relationship between two sites within a frequency band; often interpreted as an index of communication between brain regions, but inflatable by volume conduction, reference contamination, and artifact.
common-mode rejection: the differential amplifier's attenuation of signals present at both inputs, which reduces noise and artifacts common to the two sites; its effectiveness depends on the two inputs presenting closely matched impedances.
computerized axial tomography (CAT or CT): the creation of medium-resolution images of brain structure by moving an x-ray source along an arc surrounding the head.
Cz: the central midline electrode in the 10-20 system, often used as a common reference point in unipolar montages.
derivation: the assignment of two electrodes to an amplifier's inputs 1 and 2.
desynchrony: pools of neurons fire independently due to stimulation of specific sensory pathways up to the midbrain and high-frequency stimulation of the reticular formation and nonspecific thalamic projection nuclei.
differential amplifier (balanced amplifier): a device that boosts the difference between two inputs: the active (input 1) and reference (input 2).
dipolar sources: brain-generated electrical fields that produce opposing voltages detectable at the scalp; critical in EEG localization.
dipole: an electrical source with separated regions of positive and negative charge; for example, the eye is electropositive at the front and electronegative at the back.
drowsiness artifact: the intrusion of drowsiness or light sleep into a recording intended to sample wakefulness. In adults it begins with attenuation of the posterior dominant rhythm and slow rolling lateral eye movements, which appear as 1-Hz or slower waveforms of greatest amplitude and opposite polarity at F7 and F8, and it may progress to 1–2 Hz slowing of the alpha rhythm.
edge effect: the reduced precision of spatial averaging at scalp-periphery electrodes (such as Fp1, Fp2, F7, F8, O1, and O2) that lack neighboring electrodes on all sides.
EEG artifacts: noncerebral electrical activity in an EEG recording can be divided into physiological and exogenous artifacts.
electro-ocular artifact: contamination of EEG recordings by potentials generated by eye blinks, eye flutter, and eye movements.
electrode: a specialized conductor that converts biological signals like the EEG into currents of electrons.
electrode pop artifact: a sudden, steep deflection followed by a slower baseline return, confined to channels sharing one electrode, caused by an abrupt change at the electrode–electrolyte–skin junction; it shows no physiologic field.
EMG artifact: interference in EEG recording by volume-conducted signals from skeletal muscles, with power spread across roughly 20–500 Hz and concentrated between about 50 and 150 Hz, overlapping the EEG beta band at its low end.
epoch: a time segment of EEG recording, usually lasting a few seconds, used to examine waveform characteristics within a specific interval.
evoked potential artifact (event-related potential artifact): somatosensory, auditory, and visual signal processing-related transients that may contaminate multiple channels of an EEG record.
exogenous artifacts: noncerebral electrical activity generated by movement, 50/60 Hz and field effect, bridging, and electrode (electrode "pop" and impedance) artifacts.
field artifacts: external artifacts transmitted by nearby electrical sources.
focal activity: EEG signals that originate from a localized area of the brain, as opposed to generalized activity.
frequency (Hz): the number of complete cycles that an AC signal completes in a second, usually expressed in hertz.
functional magnetic resonance imaging (fMRI): an imaging technique to detect brain regions' oxygen use during specific tasks indirectly.
ground electrode: a sensor placed on an earlobe, mastoid bone, or the scalp that is grounded to the amplifier.
hertz (Hz): unit of frequency measured in cycles per second.
high-frequency filter (HFF): a filter that attenuates frequencies above a cutoff frequency.
hypnagogic hypersynchrony: a normal drowsiness pattern in children consisting of the abrupt appearance of high-amplitude (about 100–350 µV) rhythmic 3–5 Hz activity, maximal frontocentrally, that can be mistaken for epileptiform activity in an otherwise normal record.
impedance (Z): the frequency-dependent opposition to an AC signal, measured in ohms and conventionally reported in kilohms.
impedance meter: device that uses an AC signal to measure impedance in an electric circuit, such as between active and reference electrodes.
impedance test: automated or manual measurement of skin-electrode impedance.
inion: the external occipital protuberance, the midline bony prominence on the back of the skull.
International 10-10 system: a modified combinatorial system for electrode placement that expands the 10-20 system to 75 electrode positions to improve spatial sampling, aid localization of epileptiform activity, and improve detection of localized evoked potentials.
International 10-20 system: a standardized procedure for placing 19 scalp recording electrodes plus two ear electrodes (A1 and A2)—21 placements in all, per ACNS—and a separate ground electrode.
Laplacian montage: a spatial filter, often grouped with the referential montages, in which each electrode is compared with a weighted average of its immediately surrounding electrodes. This emphasizes activity local to each electrode while suppressing distant or volume-conducted signals, improving spatial resolution. Its accuracy depends on dense, evenly spaced arrays, and peripheral electrodes are subject to the edge effect.
linked ears reference montage: a referential EEG configuration in which all scalp electrodes are referenced to the average of the left (A1) and right (A2) earlobe electrodes. It assumes the earlobes are relatively inactive—an assumption that does not fully hold, so it introduces reference contamination—and is the reference used by most qEEG normative databases.
localization: the process of determining the origin of EEG activity within the brain, often aided by montage selection and waveform characteristics.
longitudinal bipolar montage: a bipolar montage where electrodes are connected front-to-back along the anterior-posterior axis; also known as the "double banana" montage.
magnetic resonance imaging (MRI): a noninvasive imaging technique that uses strong magnetic fields and bursts of RF energy to construct highly detailed images of the living brain.
magnetoencephalography (MEG): a noninvasive functional imaging technique that uses SQUIDs (superconducting quantum interference devices), or increasingly optically pumped magnetometers, to detect the weak magnetic fields generated by neuronal activity.
mastoid bone: the bony prominence behind the ear.
microvolt (μV): the unit of amplitude (signal strength) that is one-millionth of a volt.
monopolar recording: a recording method that uses one active electrode and one reference electrode, plus a ground.
montage: a grouping of electrodes (combining derivations) to record EEG activity.
motor unit: an alpha motor neuron and the skeletal muscle fibers it innervates.
movement artifact: voltages caused by client movement or the movement of electrode wires by other individuals.
nasion: the depression at the bridge of the nose.
notch filter: a filter that suppresses a narrow band of frequencies, such as those produced by line current at 50/60 Hz.
ohm (Ω): the unit of impedance or resistance.
phase: the timing relationship between the signals recorded at two different sites.
phase reversal: a change in polarity between adjacent electrodes in a bipolar montage, indicating the likely location of maximal voltage and aiding in source localization.
physiological artifacts: noncerebral electrical activity that includes electromyographic, electro-ocular (eye blink and eye movement), cardiac (pulse), sweat (skin impedance), drowsiness, and evoked potential.
polarity: the direction of waveform deflection (positive or negative) in EEG, relevant for determining the source and direction of electrical activity.
polarization: chemical reactions at the electrode–electrolyte interface that produce separated regions of positive and negative charge, reducing ion exchange and producing an unstable DC offset. Silver–silver chloride electrodes are relatively nonpolarizing.
positron emission tomography (PET): a functional imaging technique in which a positron-emitting tracer is introduced into the bloodstream and its distribution imaged to measure metabolism, blood flow, or receptor binding.
posterior dominant rhythm (PDR): the dominant, reactive rhythm recorded over the posterior head regions during relaxed eyes-closed wakefulness, which attenuates with eye opening; normally 8–13 Hz in awake adults.
preauricular point: the slight depression located in front of the ear and above the earlobe.
pulse artifacts: noncerebral voltages due to mechanical movement of an electrode in relation to the skin surface due to the pressure wave of each heartbeat.
quantitative EEG (qEEG): the digital analysis of EEG—typically from a 19-channel array—to derive amplitude or power within specific frequency bands or bins along with connectivity measures such as coherence and phase, often compared against a normative database.
radiofrequency (RF) artifact: contamination from external electromagnetic sources such as mobile and cordless phones, Wi-Fi and Bluetooth devices, motors, and nearby equipment; the classic "cone from the front of the screen" description applies to cathode-ray-tube displays rather than modern LCD and LED screens.
reference contamination: EEG signals picked up by the reference electrode that are added to other channels through the differential amplifier.
reference electrode: an electrode placed on the scalp, earlobe, or mastoid.
referential (monopolar) montage: the placement of one active electrode (A) on the scalp and a neutral reference (R) and ground (G) on the ear or mastoid.
re-montaging: the process of re-displaying EEG data using a different montage configuration, allowing clinicians to view the same recorded electrical activity from alternative spatial perspectives to enhance interpretation, localization, and artifact differentiation.
response stereotypy: a person's unique response pattern to stressors of identical intensity.
sequential (bipolar) montage: placement of active (A) and reference (R) sensors on active scalp sites and the ground (G) to an earlobe or mastoid.
single photon emission computerized tomography (SPECT): a functional imaging technique that uses gamma rays to create three-dimensional and slice images of cerebral blood flow averaged over several minutes.
spatial resolution: how precisely an imaging or recording method localizes where activity arises; for EEG, the ability of a montage and electrode array to distinguish activity arising from different areas of the brain.
subharmonic: a frequency component at an integer fraction of a fundamental (e.g., 30 Hz from 60 Hz). Linear amplification does not generate subharmonics; apparent low-frequency residue after notch filtering is better explained by aliasing, intermodulation, or filter artifacts.
sweat artifact: very slow (typically below 0.5–1 Hz) rolling baseline undulations produced when perspiration alters the electrical properties of the skin at and near the electrode and when sweat gland activity generates slow skin potentials. Heavy sweating can also cause bridging, but sweat artifact and bridging artifact are distinct phenomena.
synchrony: the coordinated firing of pools of neurons due to pacemakers and mutual coordination.
temporal resolution: how quickly an imaging method detects changes in brain function.
tragus: the flap at the opening of the ear.
transverse montage: a bipolar EEG montage that links electrodes horizontally across the head, providing sensitivity to lateralized and horizontal propagation of activity.
vertex (Cz): the intersection of imaginary lines drawn from the nasion to inion and between the two preauricular points in the International 10-10 and 10-20 systems.
voxel: a three-dimensional pixel representing a specific volume of brain tissue, used to measure and analyze brain activity and structure.
Test Yourself on ClassMarker
Click on the ClassMarker logo below to take a 10-question exam over this entire unit. There is no password.

Review Flashcards on Quizlet
Click on the Quizlet logo to review our chapter flashcards.

Visit the BioSource Software Website
BioSource Software offers Physiological Psychology, which satisfies BCIA's Neuroanatomy requirement, and the Neurofeedback100 Testing Service, which provides extensive multiple-choice testing over the Neurofeedback Blueprint.

Assignment
Now that you have completed this module, explain why low-and-balanced skin-electrode impedances are important in neurofeedback training. Describe the precautions you take to achieve acceptable impedance values. How do you measure impedance with your neurofeedback system?
References
Acharya, J. N., Hani, A. J., Thirumala, P. D., & Tsuchida, T. N. (2016). American Clinical Neurophysiology Society Guideline 3: A proposal for standard montages to be used in clinical EEG. Journal of Clinical Neurophysiology: Official Publication of the American Electroencephalographic Society, 33(4), 312-316. https://doi.org/10.1097/WNP.0000000000000317
Andreassi, J. L. (2000). Psychophysiology: Human behavior and physiological response. Lawrence Erlbaum and Associates, Inc.
Basmajian, J. V. (Ed.). (1989). Biofeedback: Principles and practice for clinicians. Williams & Wilkins.
Bear, M. F., Connors, B. W., & Paradiso, M. A. (2002). Neuroscience: Exploring the brain (2nd ed.). Lippincott Williams & Wilkins.
Breedlove, S. M., & Watson, N. V. (2023). Behavioral neuroscience (10th ed.). Sinauer Associates, Inc.
Cacioppo, J. T., & Tassinary, L. G. (Eds.). (1990). Principles of psychophysiology. Cambridge University Press.
Carvalhaes, C., & Acacio de Barros, J. (2015). The surface Laplacian technique in EEG: Theory and methods. International Journal of Psychophysiology, 97(3), 174-188. https://doi.org/10.1016/j.ijpsycho.2015.04.023
Collura, T. F. (2014). Technical foundations of neurofeedback. Taylor & Francis.
Demos, J. N. (2019). Getting started with EEG neurofeedback (2nd ed.). W. W. Norton & Company.
Fisch, B. J. (1999). Fisch and Spehlmann's EEG primer (3rd ed.). Elsevier.
Floyd, T. L. (1987). Electronics fundamentals: Circuits, devices, and applications. Merrill Publishing Company.
Garces, A., Laciar, E., Patiño, H., & Valentinuzzi, M. (2007). Artifact removal from EEG signals using adaptive filters in cascade. Journal of Physics: Conference Series, 90(1), 012081. https://doi.org/10.1088/1742-6596/90/1/012081
Gloor, P. (1985). EEG analysis and the localization of epileptic foci. In D. Daly & T. Pedley (Eds.), Current practice of clinical electroencephalography (pp. 139-174). Raven Press.
Gordon, R., & Rzempoluck, E. J. (2004). Introduction to Laplacian montages. American Journal of Electroneurodiagnostic Technology, 44(2), 98-102. PMID: 15328706.
Halford, J. J., Sabau, D., Drislane, F. W., Tsuchida, T. N., & Sinha, S. R. (2016). American Clinical Neurophysiology Society Guideline 4: Recording clinical EEG on digital media. Journal of Clinical Neurophysiology, 33(4), 317-319. https://doi.org/10.1080/21646821.2016.1245563
Hugdahl, K. (1995). Psychophysiology: The mind-body perspective. Harvard University Press.
Hughes, J. R. (1994). EEG in clinical practice (2nd ed.). Butterworth-Heinemann.
Iber, C., Ancoli-Israel, S., Chesson, A. L., & Quan, S. F. (2007). The AASM manual for the scoring of sleep and associated events: Rules, terminology and technical specifications. American Academy of Sleep Medicine.
Jiang, X., Bian, G.-B., & Tian, Z. (2019). Removal of artifacts from EEG signals: A review. Sensors, 19(5), 987. https://doi.org/10.3390/s19050987
Kaveh, R., Tetreault, N., Gopalan, K., Maravilla, J., Lustig, M., Muller, R., & Arias, A. (2022). Rapid and scalable fabrication of low impedance, 3D dry electrodes for physiological sensing. Advanced Materials Technologies, 7, Article 2200342. https://doi.org/10.1002/admt.202200342
Khazan, I. Z. (2019). Biofeedback and mindfulness in everyday life: Practical solutions for improving your health and performance. W. W. Norton & Company.
Klass, D. W. (1995). The continuing challenge of artifacts in the EEG. American Journal of EEG Technology, 35(4), 239-269. https://doi.org/10.1080/00029238.1995.11080524
Kubala, T. (2009). Electricity 1: Devices, circuits, and materials (9th ed.). Cengage Learning.
Lau, T. M., Gwin, J. T., & Ferris, D. P. (2012). How many electrodes are really needed for EEG-based mobile brain imaging? Journal of Behavioral and Brain Science, 2(3), 387-393. https://doi.org/10.4236/jbbs.2012.23044
Lebby, P. C. (2013). Brain imaging: A guide for clinicians. Oxford University Press.
Libenson, M. H. (2010). Practical approach to electroencephalography. Saunders Elsevier.
Lin, F., Witzel, T., Hamalainen, M. S., Dale, A. M., Belliveau, J. W., & Stufflebeam, S. M. (2004). Spectral spatiotemporal imaging of cortical oscillations and interactions in the human brain. NeuroImage, 23(2), 582-595. https://doi.org/10.1016/j.neuroimage.2004.04.027
Logothetis, N. K., Pauls, J., Augath, M., Trinath, T., & Oeltermann, A. (2001). Neurophysiological investigation of the basis of the fMRI signal. Nature, 412(6843), 150-157. https://doi.org/10.1038/35084005
López, S., Gross, A., Yang, S., Golmohammadi, M., Obeid, I., & Picone, J. (2016). An analysis of two common reference points for EEGs. IEEE Signal Processing in Medicine and Biology Symposium, 2016. https://doi.org/10.1109/SPMB.2016.7846854
McFarland, D. J., McCane, L. M., David, S. V., & Wolpaw, J. R. (1997). Spatial filter selection for EEG-based communication. Electroencephalography and Clinical Neurophysiology, 103(3), 386-394. https://doi.org/10.1016/S0013-4694(97)00022-2
Montgomery, D. (2004). Introduction to biofeedback. Module 3: Psychophysiological recording. Association for Applied Psychophysiology and Biofeedback.
Moss, D., & Shaffer, F. (Eds.). (2019). Physiological recording technology and applications in biofeedback and neurofeedback. Association for Applied Psychophysiology and Biofeedback.
Niedermeyer, E., & da Silva, F. L. (2005). Electroencephalography: Basic principles, clinical applications, and related fields (5th ed.). Lippincott Williams & Wilkins.
Nilsson, J. W., & Riedel, S. A. (2008). Electric circuits (8th ed.). Pearson Prentice-Hall.
Nunez, P. L., & Srinivasan, R. (2006). Electric fields of the brain: The neurophysics of EEG (2nd ed.). Oxford University Press.
Nuwer, M. R. (1997). Assessment of digital EEG, quantitative EEG, and EEG brain mapping. Report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology, 49(1), 277-292. PMID: 9222191.
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49-65. https://doi.org/10.1016/0167-8760(84)90014-X
Peek, C. J. (2016). A primer of traditional biofeedback instrumentation. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: A practitioner's guide (4th ed.). The Guilford Press.
Pfister, H., Kaynig, V., Botha, C. P., Bruckner, S., Dercksen, V. J., Hege, H.-C., & Roerdink, J. B. T. M. (2014). Visualization in connectomics. In C. D. Hansen, M. Chen, C. R. Johnson, A. E. Kaufman, & H. Hagen (Eds.), Scientific visualization: Uncertainty, multifield, biomedical, and scalable visualization (pp. 221-245). Springer. https://doi.org/10.1007/978-1-4471-6497-5_21
Picton, T. W., & Hillyard, S. A. (1972). Cephalic skin potentials in electroencephalography. Electroencephalography and Clinical Neurophysiology, 33(4), 419-424. https://doi.org/10.1016/0013-4694(72)90122-8
Srinivasan, R., Nunez, P. L., & Silberstein, R. B. (1996). Spatial filtering and neocortical dynamics: Estimates of EEG coherence. IEEE Transactions on Biomedical Engineering, 43(7), 683-693. https://doi.org/10.1109/10.502603
Stern, R. M., Ray, W. J., & Quigley, K. S. (2001). Psychophysiological recording (2nd ed.). Oxford University Press.
Thomas, C. (2007). What is a montage? EEG instrumentation. American Society of Electroneurodiagnostic Technologists, Inc.
Thompson, M., & Thompson, L. (2015). The biofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Return to Top