Definition
What You Will Learn
This unit introduces the foundational concepts of biofeedback and neurofeedback training. You will explore how these learning processes help individuals regulate their psychophysiology, understand the key definitions from major professional organizations, and learn to distinguish legitimate biofeedback from physiological monitoring, modulation, and pseudo-biofeedback devices. By the end of this unit, you will be able to explain neurofeedback to clients and describe its relationship to biofeedback training.
Biofeedback training (BFT) and neurofeedback training (NFT) involve the same learning processes we use to develop motor skills or master a videogame. An individual acts (breathes slowly and effortlessly), observes the results (heart rate variability increases), and repeats those two steps to develop a lasting habit (slow-paced breathing). Clients actively learn to regulate their psychophysiology (Thompson & Thompson, 2015).
Biofeedback also acts as a psychophysiological mirror, teaching individuals to monitor, understand, and change their physiology by making invisible processes visible (Peper, Shumay, & Moss, 2012). Biofeedback teaches clients to listen to their bodies. Although they initially use equipment to track their physiology, biofeedback training progressively replaces external with internal cues.

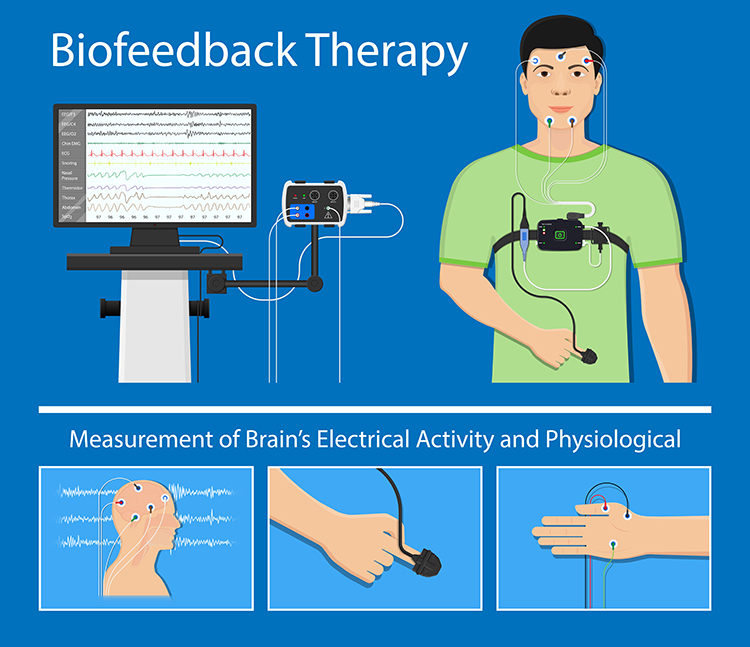
NFT is a branch of BFT that provides real-time displays of brain electrical activity using an electroencephalograph (EEG), as opposed to an electromyograph (EMG), heart rate variability (HRV), skin temperature, or other psychophysiological measures. An electroencephalograph monitors brain electrical activity (e.g., brainwaves), while an electromyograph detects muscle action potentials from skeletal muscles. These modalities differ in the signals they detect, process, and display (Collura, 2014).
The Process of Neurofeedback
Neurofeedback is the process of interacting with an electronic device that measures and feeds back information about brain electrical activity.
The goals of this process are to: (1) ensure healthy regulatory function in the brain's neuromodulating systems, (2) encourage global neuropsychophysiological change, (3) correct specific, distinct, identifiable disorders or barriers to optimal performance that result from underlying dysregulation, and (4) enhance performance by optimizing nervous system functioning.
What Neurofeedback Does
Neurofeedback provides accurate, timely, and helpful information to the client in the form of visual, auditory, or tactile feedback that responds to meaningful changes in monitored neuronal systems. Neurofeedback training promotes flexibility, resilience, and choice.
How Neurofeedback Works: The Operant Conditioning Loop
If neurofeedback is a learning process, what kind of learning is it? At its core, neurofeedback relies on operant conditioning, the principle that behavior followed by a reward becomes more likely to recur (Sherlin et al., 2011). Here, the "behavior" is a pattern of brain electrical activity, and the reward is the feedback itself.
The loop repeats in three steps. First, sensors detect a targeted EEG feature, such as the amplitude of activity in a chosen frequency band, and software compares that feature to a threshold the practitioner has set. Second, when the brain produces the desired pattern and crosses the threshold, the client earns a reward, perhaps a pleasant tone, a rising score, or a brightening movie. Third, this reinforcement makes the rewarded pattern slightly more likely a moment later, and across hundreds of trials the brain gradually shifts toward the target (Kerson et al., 2025).
Much of this learning is implicit, which means clients usually cannot put into words how they earned the reward, much as you cannot fully explain how you balance a bicycle (Sitaram et al., 2017). Classical conditioning contributes as well, because the trained brain state becomes paired with the calm, focused context of the session (Sherlin et al., 2011). This is why the motor-skill analogy from the start of this chapter fits so well: you act, you observe the result, and repetition turns a fragile new skill into a durable habit.
Click on the link to view Neurofeedback Overview, produced by ISNR. The society was called the International Society for Neurofeedback and Research from 2006 until 2019, when it took its present name, the International Society for Neuroregulation & Research, so older publications appear under the earlier name.

BFT may be more effective when training promotes mindfulness. A mindfulness approach teaches clients to focus on their immediate feelings, cognitions, and sensations in an accepting and non-judgmental way, to distinguish between what can and cannot be changed, and to change the things they can (Khazan, 2013).
Clients can become stuck when they focus on outcomes they cannot immediately control. For example, James, an undergraduate Psychology major, was diagnosed with ADHD. When he ruminated about his mistakes on daily quizzes, this undermined his motivation to study and resulted in lower scores. He could not study while he worried about his quiz performance.
When James learned to accept occasional mistakes without fear, his studying and course grade improved. James succeeded by changing what he could: his reaction to unavoidable errors.

BCIA Blueprint Coverage
This unit addresses I. Orientation to Neurofeedback - A. Definition of Neurofeedback (EEG Biofeedback).

This unit covers Definitions of Biofeedback and Neurofeedback, Physiological Monitoring and Modulation Are Not Biofeedback, and Quantum Biofeedback and LenyosysTM.
Definitions of Biofeedback and Neurofeedback
Since neurofeedback is a specialized application of biofeedback, we will start with the Biofeedback Alliance and Nomenclature Task Force definition (Schwartz, 2010).
Biofeedback Alliance and Nomenclature Task Force (2008)
Biofeedback is a process that enables an individual to learn how to change physiological activity for the purposes of improving health and performance. Precise instruments measure physiological activity such as brainwaves, heart function, breathing, muscle activity, and skin temperature. These instruments rapidly and accurately "feed back" information to the user. The presentation of this information, often in conjunction with changes in thinking, emotions, and behavior, supports desired physiological changes. Over time, these changes can endure without continued use of an instrument.
The main elements of this definition are that (1) biofeedback is a learning process that teaches an individual to control her physiological activity, (2) biofeedback training aims to improve health and performance, (3) instruments rapidly monitor an individual's performance and display it back to her, (4) the individual uses this feedback to produce physiological changes, (5) changes in thinking, emotions, and behavior often accompany and reinforce physiological changes, and (6) these changes become independent of external feedback from instruments.
The Biofeedback Certification International Alliance (BCIA) emphasized that neurofeedback is a form of biofeedback in its Blueprint of Knowledge.
Biofeedback Certification International Alliance (2016) Definition of Neurofeedback
Neurofeedback is employed to modify the electrical activity of the CNS, including EEG, event-related potentials, slow cortical potentials and other electrical activity either of subcortical or cortical origin. Neurofeedback is a specialized application of biofeedback of brainwave data in an operant conditioning paradigm. The method is used to treat clinical conditions as well as to enhance performance.
The International Society for Neuroregulation & Research (ISNR) maintains the field's most detailed definition of neurofeedback. Its Board of Directors edited and ratified the current version on July 28, 2024, replacing an earlier statement that had circulated for more than a decade.
International Society for Neuroregulation & Research (2024) Definition of Neurofeedback
Neurofeedback (NFB) is a therapeutic intervention utilizing a brain-computer interface (BCI). An individual's brainwave activity is tracked in real-time (with a sensor), is interpreted (with a decoder), and then information is used to encourage the individual to modulate specific brainwave activity via "feedback" (effector). Through behavior modification and learning processes self-regulation of brain and central nervous system (CNS) function is taught.
The goal of NFB is to address reported symptoms, improve health and well-being, or improve human performance.
Three features of this definition are worth pausing over, because each one changes how you explain neurofeedback to a client or a referring physician.
First, ISNR now frames neurofeedback as a brain-computer interface (BCI), a system that reads a neural signal and returns information derived from it. The three components named in the definition are the sensor that tracks brainwave activity, the decoder that interprets it, and the effector that delivers the feedback. That vocabulary places neurofeedback in the same engineering family as the assistive BCIs used by people with severe motor impairment, while keeping the distinction that matters clinically: a neurofeedback BCI is used to teach self-regulation rather than to operate a device.
Second, the definition locates the learning explicitly. Change occurs "through behavior modification and learning processes," which is the same operant framework described earlier in this unit. ISNR draws the boundary of the field on exactly this basis, stating that electrical neuromodulation methods "do not employ operant conditioning nor instrumental learning, so they are separate and distinct from all forms of biofeedback." This is a sharper criterion than the one the society used previously, and it is the criterion this unit applies in the section on modulation and entrainment devices below.
Third, the goal statement is deliberately broad. Neurofeedback may aim to address symptoms, to improve health and well-being, or to improve performance, and the three are not the same undertaking. A performance-optimization client and a client seeking symptom relief warrant different assessment, different outcome measures, and different conversations about what success looks like.
ISNR also states that neurofeedback "is considered safe," while noting that temporary discomforts such as fatigue or headache may occur, and describes it as "considered an evidence-based intervention." Both statements are a professional society's characterization of its own field rather than an independent appraisal, and the strength of the evidence differs substantially by condition. For the current efficacy ratings and the criteria behind them, see the Efficacy Criteria and Key Studies units and the field's standard reference (Khazan et al., 2023). The safety statement is examined in the Perspective section that follows.
Perspective
Two claims in the ISNR definition deserve a closer look: where it locates neurofeedback's target, and what it says about safety.
First, the definition says that neurofeedback teaches "self-regulation of brain and central nervous system (CNS) function." Read casually, that invites the familiar shorthand in which NFT is top-down and biofeedback training (BFT) is bottom-up. A more nuanced explanation is that both NFT and BFT involve top-down interventions and bottom-up interventions. The differentiation between body-centered and central nervous system (CNS) interventions is largely arbitrary, and it reflects an incomplete understanding of the interconnections between these systems.
For example, the CNS is instrumental in modifying behaviors like respiration, and changes in respiration modulate CNS activity. Hyperventilation leading to hypocapnia causes a general slowing of the EEG (Shafi & Westover, 2018).
Therefore, NFT and BFT share components like breathing, education about the training process, mindfulness, and problem-solving, all of which involve the brain and central nervous system. Likewise, since the central nervous system and peripheral nervous system cooperate through complex feedback and feedforward loops, we can conceptualize them as one complex integrated system.
Clinicians who treat ADHD may begin treatment with heart rate variability biofeedback, which displays beat-to-beat heart rate and coaches slow breathing at the client's resonance frequency to increase the amplitude of heart rate oscillations. Whereas attention involves brainstem, subcortical, and cortical networks, successful HRVB training (which is often characterized as bottom-up) may significantly increase continuous attention and make NFT unnecessary or may facilitate improved outcomes when followed by NFT for this condition.
Second, ISNR states that neurofeedback "is considered safe" and notes that temporary discomforts may occur. That is better calibrated than the society's earlier language, which said trainees generally do not experience negative side effects at all, but it still leaves the practitioner to judge what "temporary" covers. Hammond and Kirk (2008) assembled accounts supplied by practitioners, together with anecdotal reports, indicating that when applied incorrectly neurofeedback can be associated with adverse reactions like anxiety, depression, emotional lability, explosiveness, incontinence, OCD, and sedation. Their evidence base is clinical and anecdotal rather than experimental; they did not review randomized controlled trials.
Hammond and Kirk did not rigorously evaluate the anecdotal reports supplied by clinicians for length or severity of disruption resulting from NFT. In most cases, such effects are temporary unless reinforced by continuing incorrect training approaches (J. S. Anderson, personal communication, June 6, 2016).
Rogel et al. (2015) randomized 30 healthy undergraduates to a modified SMR protocol, an upper alpha protocol, or sham feedback across ten sessions. Most participants in every group reported some side effects. The authors separated non-specific effects, which appeared under sham as well and are therefore not attributable to any particular protocol, from protocol-specific effects, and concluded that the SMR protocol was the most sensitive to side effects. The practical lesson is that reported side effects are common and that a sham condition is needed before any of them can be attributed to the training itself.
Core Elements of Neurofeedback
The client-practitioner relationship is the foundation of BFT and NFT. Neurofeedback is most effective when clients and providers are mindful because this promotes self-awareness and a sense of agency. Neurofeedback promotes self-regulation when a practitioner provides effective coaching (Khazan, 2019).

Interoception: Your Body's Inner Sense
Appreciation
Dr. Nate Ewigman inspired and contributed to this section.

Right now, without checking a pulse, can you feel your own heartbeat? Can you tell whether your stomach is full or whether your shoulders are tense? That inward sense is called interoception, the process your nervous system uses to detect, interpret, and regulate signals coming from inside your body, such as heartbeat, breathing, hunger, temperature, and muscle tension (Chen et al., 2021; Craig, 2002). It is the inward-facing partner of exteroception, which is how you sense the outside world through sight, sound, touch, and smell. Interoception helps keep your internal conditions stable, a balance called homeostasis, and it supports allostasis, your body's habit of adjusting in advance to meet demands before they fully arrive (Barrett & Simmons, 2015; Khalsa et al., 2018).
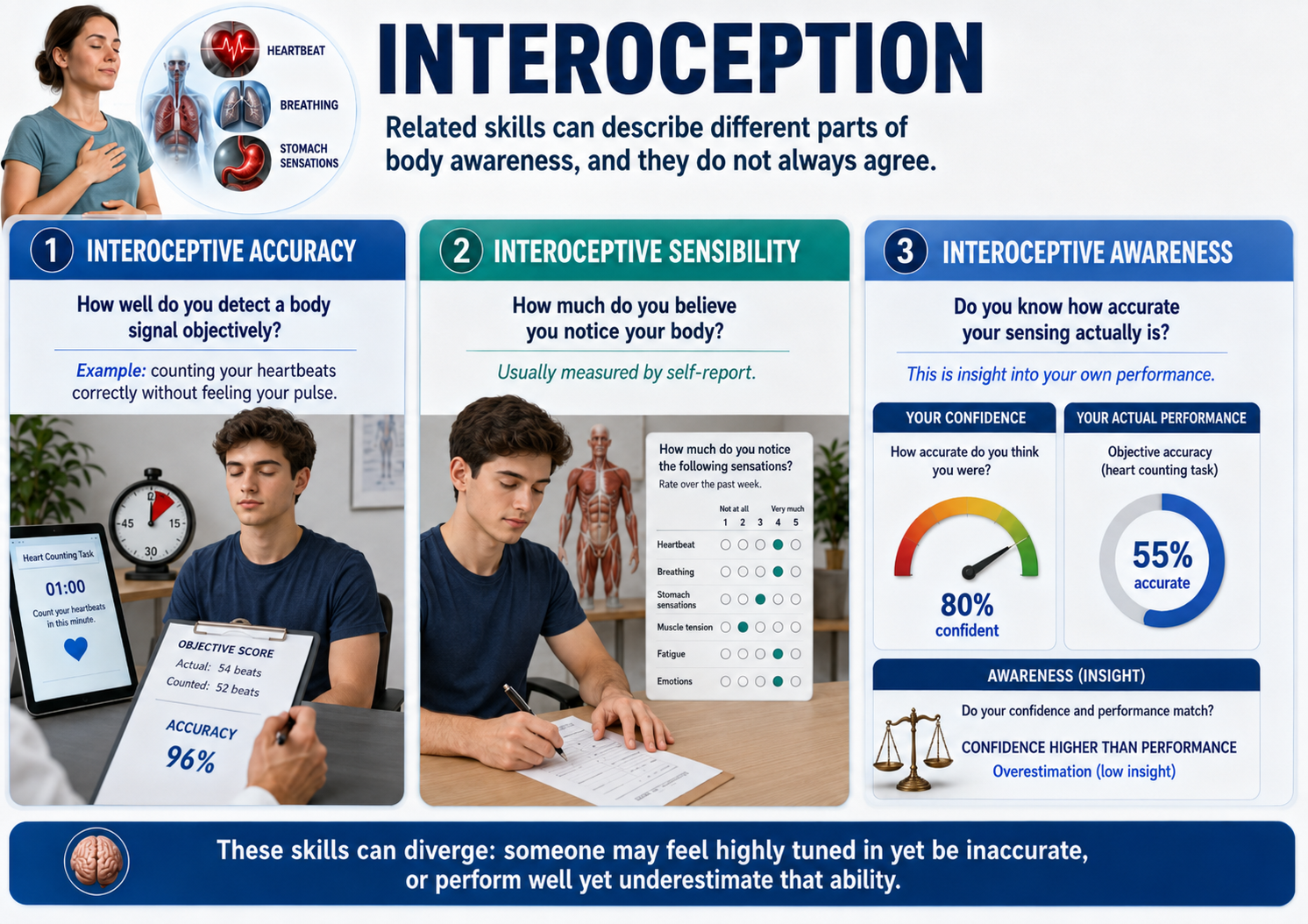
Interoception turns out to be not one skill but several, and they do not always agree. Interoceptive accuracy is how well you objectively detect a body signal, such as counting your heartbeats correctly without feeling your pulse. Interoceptive sensibility is how much you believe you notice your body, measured by your own self-report. Interoceptive awareness goes one level higher, because it is knowing how accurate your sensing actually is (Garfinkel et al., 2015). Since these can come apart, someone may feel deeply tuned in to their body yet score poorly on an objective test.
So how does the brain create this inner sense? Many signals from your organs travel up sensory fibers of the vagus nerve, called vagal afferents, to the brainstem, then by way of the thalamus to a region folded deep in the brain called the insula, which converts raw body signals into felt experience (Craig, 2009; Khalsa et al., 2018). The front portion, the anterior insula, works with the salience network, the circuitry that decides what is worth your attention. Importantly, the brain does not wait passively; it constantly predicts what your body will feel next and corrects itself when reality differs, a process known as predictive coding (Barrett & Simmons, 2015). This helps explain why anxiety, panic, chronic pain, and trauma can each distort interoception differently, sometimes muting a signal, sometimes amplifying it, and sometimes attaching alarm to signals that are perfectly accurate.
Here is where biofeedback and neurofeedback rejoin the story, because both make hidden body signals easier to feel. When you watch your heart rate rise and fall on a screen during slow breathing, you are practicing interoception with training wheels. Heart rate variability biofeedback works best when you breathe at your personal resonance frequency, an individually ideal slow pace that makes the heart-rhythm changes large and easy to notice (Lehrer & Gevirtz, 2014). A recent systematic review reported that this kind of training can measurably sharpen interoception across behavioral, physiological, and brain measures (Wareing et al., 2024).
Consider Maya, a college sophomore who panics before exams. Her heart pounds, she reads that pounding as proof that something is terribly wrong, and the panic snowballs. Using heart rate variability biofeedback, she practices watching the same heartbeat on a screen while breathing slowly, gradually relabeling the sensation as ordinary information rather than danger. Clinicians call this kind of practice interoceptive exposure, and over time it helps Maya build a calmer, more accurate relationship with her own body (Khalsa et al., 2018).
Neurofeedback takes the same idea straight to the brain by showing neural activity back to a person in real time (Sitaram et al., 2017). The most developed interoception research uses real-time fMRI neurofeedback, which lets people watch and gradually learn to control activity in their own anterior insula, and some studies show that focusing on the heartbeat improves this control (Caria et al., 2010; Zhang et al., 2023). Electroencephalography is also being explored through the heartbeat-evoked potential, a brainwave response timed to each heartbeat, although this approach is younger and harder to measure cleanly (Coll et al., 2021; Pollatos & Schandry, 2004). Before reaching for any device, clinicians often gauge a person's interoceptive style with a questionnaire called the Multidimensional Assessment of Interoceptive Awareness, which helps separate healthy body-listening from anxious body-monitoring (Mehling et al., 2012; Mehling et al., 2018).
The goal of all this work is not to make you fixate on every twinge. Instead, the aim is a safer and more flexible relationship with your body's signals, so that biofeedback and neurofeedback become ways to recalibrate trust rather than machines that regulate you from the outside (Khalsa et al., 2018; Wareing et al., 2024).
Newer work suggests that even a single session of real-time fMRI neurofeedback can improve how accurately healthy adults perceive their own heartbeats. The effect varies from person to person, a useful reminder that controlling your own brain activity is a learnable skill rather than a guaranteed result (Haruki et al., 2025).
Inter-Brain Synchrony
Therapy provides a structured environment where patients can repeatedly experience and strengthen inter-brain synchrony (Meehan, 2025; Sened et al., 2022). In inter-brain synchrony, the neural activity of two individuals becomes aligned during social interactions. This synchrony is observed in therapeutic settings when a therapist and a patient engage in shared emotional and cognitive processes, such as maintaining eye contact, mirroring expressions, and synchronizing speech rhythms.
This mutual alignment of brain activity, often termed neural coupling, facilitates a deeper interpersonal connection and effective communication. Over time, this repeated neural coupling can lead to lasting neurobiological adaptations, reinforcing healthier emotional and cognitive frameworks.

Further evidence suggests that synchrony strengthens emotional bonds and improves cognitive flexibility. When neural coupling occurs, it facilitates better communication between brain regions associated with decision-making, problem-solving, and emotional processing. Researchers have proposed that this may help explain why higher therapist-client synchrony has been associated with better therapeutic outcomes, although the association is correlational and the direction of the effect is not established. Understanding and intentionally fostering this synchrony can, therefore, be a powerful tool in therapeutic practice, enhancing the overall efficacy of interventions.
For therapists, these findings underscore the importance of fostering therapeutic synchrony as an active component of treatment. Beyond verbal communication, nonverbal cues such as body language, tone of voice, and paced responsiveness contribute significantly to inter-brain synchrony. Therapists who practice mindfulness, attunement, and embodied presence may enhance their ability to facilitate neural synchrony with clients, potentially amplifying the effectiveness of therapy.
Moreover, this perspective encourages therapists to view relational healing not only as a psychological process but also as a neurobiological one. Clients who struggle with attachment issues, social difficulties, or trauma may particularly benefit from interventions that emphasize relational presence, attunement, and co-regulation.
Relational presence refers to the therapist's capacity to fully engage with the client, establishing an environment of genuine connection and trust where the client feels seen and valued. Attunement is the process by which the therapist accurately perceives and sensitively responds to the client's emotional signals, thereby fostering a therapeutic interaction that validates the client's internal experience. Co-regulation involves a collaborative dynamic in which the therapist supports the client in managing and modulating their emotional states, ultimately aiding the client in developing effective self-regulation skills. Collectively, these processes help create a secure relational framework essential for healing and developing adaptive emotional responses.
Research on inter-brain plasticity suggests that repeated neural synchrony between therapist and client may produce lasting neurobiological adaptations. This emerging field highlights how the therapeutic relationship itself can reshape neural pathways, potentially explaining the mechanisms underlying successful psychotherapy outcomes (Sened et al., 2022).
Biofeedback and neurofeedback are learning processes that teach self-regulation. BCIA defines neurofeedback as a specialized application of biofeedback of brainwave data in an operant conditioning paradigm, and ISNR's 2024 definition frames it as a brain-computer interface that teaches self-regulation of brain and CNS function through learning, which is what separates it from neuromodulation. Both top-down and bottom-up components contribute to effective training, and the therapeutic relationship forms a crucial foundation for positive outcomes. Interoception, the brain's sense of the body's internal state, helps explain why these methods work, since both biofeedback and neurofeedback teach clients to notice and recalibrate their own body signals.
Physiological Monitoring and Modulation Are Not Biofeedback
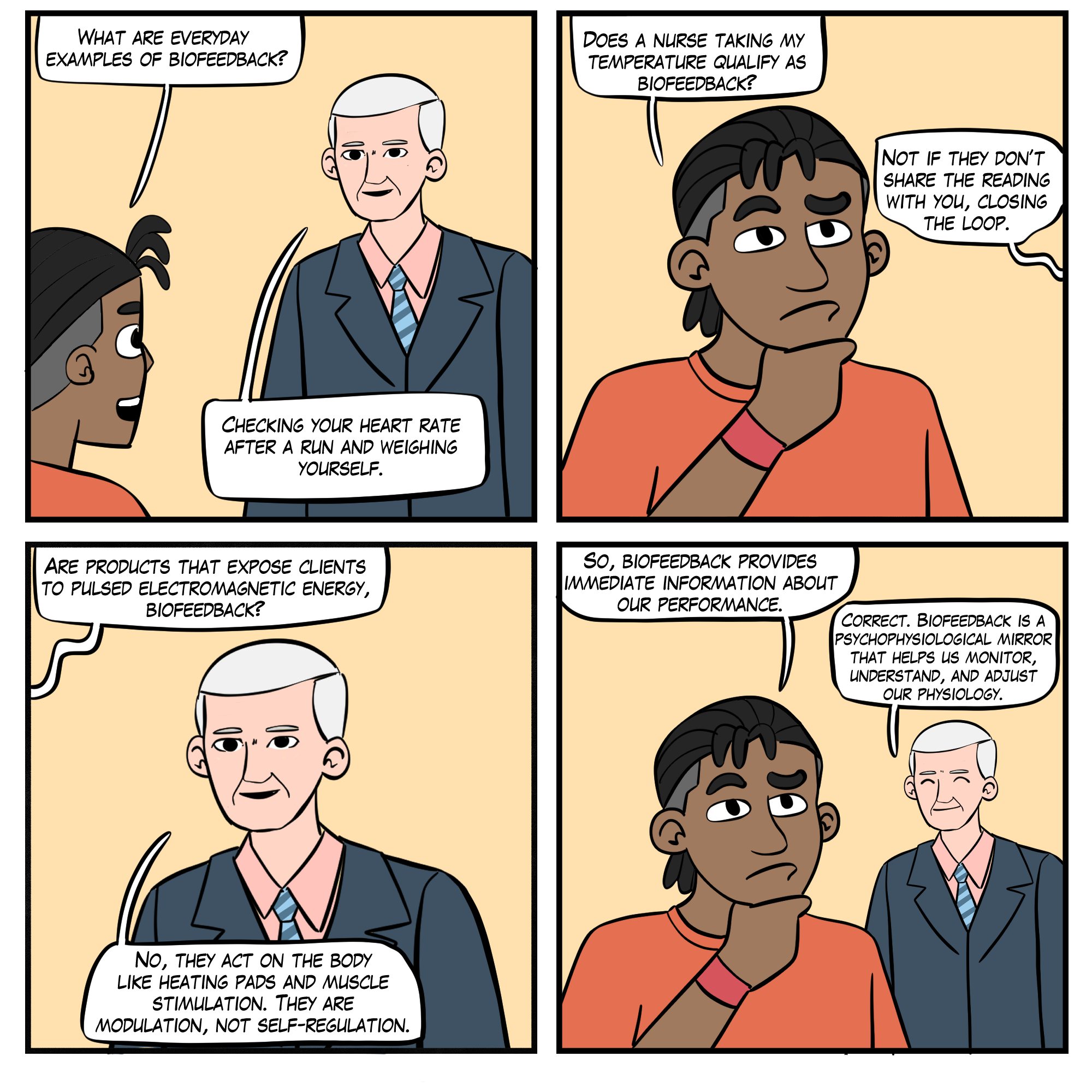
Physiological monitoring, detecting biological activity like blood pressure, is only one biofeedback component. When nurses measure your blood pressure, this is physiological monitoring. Nurses provide biofeedback when they report these values to you because this gives you information about your biological performance. When your nurse announces that your blood pressure was 120/70, the information returns to you, which is the ingredient monitoring alone lacks. Full biofeedback goes further: the information must be rapid enough and repeated often enough for you to link what you did to what changed, which is what turns feedback into a learning process.

Mini-Lecture: Physiological Monitoring and Modulation
Likewise, modulation, stimulating the nervous system to produce psychophysiological change, is not biofeedback because it acts on your body instead of providing you with information about its performance.
For example, a physical therapist might treat back pain through a modality called muscle stimulation. A current delivered to postural muscles fatigues them so that they cannot produce painful spasms. After muscle stimulation brings spasms under control, a physical therapist can initiate surface electromyographic (SEMG) biofeedback to teach the patient to increase awareness and control of postural muscle contraction.

Similarly, various devices that input signals into the central nervous system are not biofeedback devices but are generally known as entrainment devices. These include Audio-Visual Entrainment (AVE), Cranial Electrotherapy Stimulation (CES), repetitive Transcranial Magnetic Stimulation (rTMS), transcranial Direct Current Stimulation (tDCS), pulsed ElectroMagnetic Field therapy (PEMF), and others.
These interventions may be useful and may provide an effective adjunct to biofeedback. However, since they do not provide information directly to the individual in a learning paradigm, they are not biofeedback. They represent treatment, not training. For this reason, providers should confirm that the use of these modalities falls within their scope of practice. The David Delight Pro, an AVE device, is shown below.

Physiological monitoring only becomes biofeedback when information is fed back to the individual. Modulation and entrainment devices stimulate the nervous system but do not teach self-regulation because they do not provide performance feedback. These distinctions are important for understanding scope of practice.
Quantum Biofeedback and LenyosysTM
Slawecki (2009) cautioned consumers in her report for BCIA, How to Distinguish Legitimate Biofeedback/Neurofeedback Devices.
The Seattle Times published an exposé on pseudo-biofeedback devices on November 18, 2007: "Miracle Machines: The 21st-Century Snake Oil."
Appending biofeedback to a product's name does not make it biofeedback. Exposing clients to electromagnetic fields is modulation. Since biofeedback provides clients with real-time performance information to guide self-regulation, Quantum Biofeedback and LenyosysTM devices fall outside this definition.
Quantum Biofeedback
Quantum Biofeedback (EPFX / SCIO / XRROID / QXCI) devices do not provide individuals with immediate information regarding their performance. Marketers advertise that these instruments monitor, diagnose, and correct cellular abnormalities at a quantum level without providing peer-reviewed data. Critics claim that treatment with these devices may result in false diagnoses and delay effective treatment for medical disorders.

The following information was retrieved from the Empowering Change in You site on December 27, 2009. Note the disclaimer about "curing" medical conditions and explanation that it produces changes through stress management:
The function of the Quantum Biofeedback/EPFX is similar to a virus-scan on a computer. It focuses on your energetic body, which offers a more complete view of each facet of your health. Based on Quantum Physics, it runs a comprehensive test that measures the body's frequencies. The system then contributes frequencies designed to resonate within the body, thus creating balance. The human body is composed of a biochemical structure and an electromagnetic field. It performs best when these functions are balanced with one another and in complete harmony. Unfortunately, the daily stresses of life that confront each and every one of us takes its toll on the human body. Stress reduction is essential for wellness. This energy work is non-invasive. It is important to remember that energetic medicine does not "cure" health problems. It addresses them specifically by making energetic corrections and rebalancing the system through stress management.
LenyosysTM
LenyosysTM describes its pulsed electromagnetic technology as a "body-biofeedback modality":
Ideal as a complement to neurofeedback and biofeedback therapy, BRT is a body-biofeedback modality that helps to address the physical and somatic symptoms of both simple and complex health issues including digestive problems, systemic inflammation, muscle and joint aches, drug and alcohol addiction, allergies and hypersensitivities, stress, trauma and chronic illness. Whether used before, right after or in between sessions, BRT works in tandem with neurofeedback and biofeedback to create synergies that relax the client, enhance the therapy session and improve end results.

Pulsed electromagnetic treatment is modulation, not biofeedback. Instead of providing double-blind studies of their product's effectiveness, the marketers provide references for the application of Pulsed Electromagnetic Field Therapy (PEMF) and magnetism for specific applications.
Legitimate biofeedback provides real-time performance information to guide self-regulation. Quantum biofeedback and similar devices that expose clients to electromagnetic fields without providing feedback are modulation devices, not biofeedback. Consumers and practitioners should verify claims with peer-reviewed research.
Check Your Understanding
- What are the six main elements of the Biofeedback Alliance and Nomenclature Task Force definition of biofeedback?
- How does neurofeedback differ from neuromodulatory approaches like AVE and rTMS?
- Why is physiological monitoring alone not considered biofeedback?
- What distinguishes legitimate biofeedback devices from pseudo-biofeedback devices like Quantum Biofeedback?
- How do inter-brain synchrony and therapeutic attunement contribute to effective neurofeedback outcomes?
Glossary
adverse reactions: iatrogenic effects like anxiety and sedation associated with BFT and NFT.
allostasis: the body's anticipatory adjustment of its physiology to meet expected demands and stay stable through change.
anterior insula (AI): the front part of the insula that blends internal body signals with emotion, attention, and conscious feeling.
attunement: the process by which a therapist accurately perceives and responds to a client's emotional state.
biofeedback: (1) learning process that teaches an individual to control her physiological activity, (2) the aim of biofeedback training is to improve health and performance, (3) instruments rapidly monitor an individual's performance and display it back to her, (4) the individual uses this feedback to produce physiological changes, (5) changes in thinking, emotions, and behavior often accompany and reinforce physiological changes, and (6) these changes become independent of external feedback from instruments. Information about psychophysiological performance is obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
bottom-up interventions: training that directly targets peripheral nervous system networks.
brain-computer interface (BCI): a system that records a neural signal, interprets it, and returns information derived from it. ISNR's 2024 definition describes neurofeedback as a BCI whose purpose is to teach self-regulation rather than to operate an external device.
central nervous system: the division of the nervous system that includes the brain, spinal cord, and retina.
classical conditioning: unconscious associative learning process that modifies reflexive behavior and prepares us to respond to future situations rapidly.
co-regulation: the process through which one person helps another regulate their emotional state through interaction and connection.
decoder: in a brain-computer interface, the component that interprets the recorded signal and determines what will be fed back.
effector: in a brain-computer interface, the component that delivers the feedback to the individual, such as a tone, a score, or a changing display.
electroencephalograph: an instrument that measures brain electrical activity.
electromyograph: an instrument that measures skeletal muscle action potentials.
entrainment devices: instruments that input signals such as light, sound, or electricity into the central nervous system.
exteroception: sensing information from outside the body, such as sights, sounds, touch, and smells.
feedback: in cybernetic theory, orders to act to correct small errors to prevent larger future errors in a closed system.
feedforward: in cybernetic theory, orders to perform an action based on anticipated conditions in an open system.
heart rate variability biofeedback: training that displays beat-to-beat changes in heart rate, usually derived from the intervals between consecutive heartbeats, and coaches breathing at the client's resonance frequency to increase the amplitude of those oscillations.
heartbeat-evoked potential (HEP): an EEG response timed to each heartbeat that serves as a marker of how the brain processes heart-related signals.
homeostasis: a state of dynamic constancy achieved by stabilizing conditions about a setpoint, whose value may change over time. Claude Bernard described the underlying idea in 1865 as the milieu intérieur, the stable internal environment an organism actively defends; Walter Cannon coined the term homeostasis in 1926 and developed it for a general readership in his 1932 book The Wisdom of the Body.
insula: a brain region folded deep within the lateral sulcus that turns internal body signals into felt experience.
inter-brain plasticity: the capacity of the brain to adapt and change based on repeated neural synchrony with another person.
inter-brain synchrony: the synchronization of brain activity between two individuals during social or therapeutic interactions.
interoception: the nervous system process of sensing, interpreting, and regulating signals from inside the body, such as heartbeat, breathing, hunger, and temperature.
interoceptive accuracy: objective performance in detecting internal body signals, such as correctly counting one's own heartbeats.
interoceptive awareness: metacognitive insight into how accurate one's own body sensing actually is.
interoceptive exposure: deliberate, supported contact with internal sensations so they can be reinterpreted as tolerable information rather than danger.
interoceptive sensibility: a person's self-reported tendency to notice and pay attention to internal body signals.
mindfulness: accepting and non-judgmental focus of attention on the present on a moment-to-moment basis.
modulation: stimulating the nervous system to produce psychophysiological change.
Multidimensional Assessment of Interoceptive Awareness (MAIA): a self-report questionnaire that measures several dimensions of body awareness and related self-regulation.
neural coupling: the alignment of one person's neural activity with another's during communication, such as the coupling between a speaker's and a listener's brain. It is the mechanism most often invoked to explain inter-brain synchrony.
neurofeedback: information about EEG activity obtained by noninvasive monitoring and used to help individuals achieve self-regulation through a learning process that resembles motor skill learning.
operant conditioning: an unconscious associative learning process that modifies the form and occurrence of voluntary behavior by manipulating its consequences.
peripheral nervous system: nervous system subdivision that includes autonomic and somatic branches.
physiological monitoring: measurement of biological activity like EEG activity.
predictive coding: a model in which the brain constantly predicts upcoming sensory input and updates those predictions when new evidence arrives.
real-time fMRI neurofeedback (rt-fMRI-NF): neurofeedback that displays live functional MRI signals from a targeted brain region so a person can learn to regulate it.
reinforcement: in operant conditioning, a consequence that increases the likelihood that the preceding behavior, such as a targeted brainwave pattern, will recur.
relational presence: a therapist's ability to be fully engaged and attuned to a client in a way that fosters connection and trust.
resonance frequency: an individually ideal slow breathing rhythm that maximizes heart rate oscillations and baroreflex engagement.
reward: the feedback (such as a tone, point, or brightening image) delivered when the brain meets the training threshold, serving as reinforcement in neurofeedback.
salience network: interacting brain regions, usually including the anterior insula and anterior cingulate cortex, that detect what is important and direct attention.
self-regulation: control of your behavior (e.g., voluntary increase in low-beta amplitude).
sensor: in a brain-computer interface, the component that tracks the individual's brainwave activity in real time.
therapeutic synchrony: the alignment of emotional and cognitive processes between therapist and client that enhances the therapeutic process.
threshold: the criterion value of a targeted EEG feature that the brain must reach to earn a reward during neurofeedback training.
top-down interventions: training that directly targets central nervous system frontal, parietal, and limbic networks.
vagal afferents: sensory fibers of the vagus nerve that carry information from internal organs toward the brain.
Test Yourself on ClassMarker
Click on the ClassMarker logo below to take a 10-question exam over this entire unit. There is no password.

Review Flashcards on Quizlet
Click on the Quizlet logo to review our chapter flashcards.

Visit the BioSource Software Website
BioSource Software offers Physiological Psychology, which satisfies BCIA's Neuroanatomy requirement, and the Neurofeedback100 Testing Service, which provides extensive multiple-choice testing over the Neurofeedback Blueprint.

Assignment
Now that you have completed this unit, how would you explain neurofeedback to a client? How would you explain the relationship between biofeedback and neurofeedback training?
References
Barrett, L. F., & Simmons, W. K. (2015). Interoceptive predictions in the brain. Nature Reviews Neuroscience, 16(7), 419-429. https://doi.org/10.1038/nrn3950
Biofeedback Certification International Alliance. (2016). Blueprint of knowledge statements for board certification in neurofeedback. http://www.bcia.org/files/public/EEGBlueprint.pdf
Caria, A., Sitaram, R., Veit, R., Begliomini, C., & Birbaumer, N. (2010). Volitional control of anterior insula activity modulates the response to aversive stimuli: A real-time functional magnetic resonance imaging study. Biological Psychiatry, 68(5), 425-432. https://doi.org/10.1016/j.biopsych.2010.04.020
Chen, W. G., Schloesser, D., Arensdorf, A. M., Simmons, J. M., Cui, C., Valentino, R., Gnadt, J. W., Nielsen, L., St Hillaire-Clarke, C., Spruance, V., Horowitz, T. S., Vallejo, Y. F., & Langevin, H. M. (2021). The emerging science of interoception: Sensing, integrating, interpreting, and regulating signals within the self. Trends in Neurosciences, 44(1), 3-16. https://doi.org/10.1016/j.tins.2020.10.007
Coll, M.-P., Hobson, H., Bird, G., & Murphy, J. (2021). Systematic review and meta-analysis of the relationship between the heartbeat-evoked potential and interoception. Neuroscience & Biobehavioral Reviews, 122, 190-200. https://doi.org/10.1016/j.neubiorev.2020.12.012
Collura, T. F. (2014). Technical foundations of neurofeedback. Routledge.
Craig, A. D. (2002). How do you feel? Interoception: The sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655-666. https://doi.org/10.1038/nrn894
Craig, A. D. (2009). How do you feel - now? The anterior insula and human awareness. Nature Reviews Neuroscience, 10(1), 59-70. https://doi.org/10.1038/nrn2555
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2015). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65-74. https://doi.org/10.1016/j.biopsycho.2014.11.004
Hammond, D. C., & Kirk, L. (2008). First, do no harm: Adverse effects and the need for practice standards in neurofeedback. Journal of Neurotherapy, 12(1), 79-88. https://doi.org/10.1080/10874200802219947
Haruki, Y., Yang, Y., Suzuki, K., Imamizu, H., & Ogawa, K. (2025). Real-time fMRI neurofeedback boosts heartbeat perception by modulating insula activation pattern during interoceptive attention. Imaging Neuroscience, 3, Article IMAG.a.142. https://doi.org/10.1162/IMAG.a.142
International Society for Neuroregulation & Research. (2024). What is neurofeedback? Edited and ratified by the ISNR Board of Directors, July 28, 2024. https://isnr.org/what-is-neurofeedback
Kerson, C., Sherlin, L. H., & Davelaar, E. J. (2025). Neurofeedback, biofeedback, and basic learning theory: Revisiting the 2011 conceptual framework. Applied Psychophysiology and Biofeedback. https://doi.org/10.1007/s10484-025-09756-4
Khalsa, S. S., Adolphs, R., Cameron, O. G., Critchley, H. D., Davenport, P. W., Feinstein, J. S., Feusner, J. D., Garfinkel, S. N., Lane, R. D., Mehling, W. E., Meuret, A. E., Nemeroff, C. B., Oppenheimer, S., Petzschner, F. H., Pollatos, O., Rhudy, J. L., Schramm, L. P., Simmons, W. K., Stein, M. B., ... Paulus, M. P. (2018). Interoception and mental health: A roadmap. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 3(6), 501-513. https://doi.org/10.1016/j.bpsc.2017.12.004
Khazan, I. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. John Wiley & Sons, Ltd.
Khazan, I. (2019). Biofeedback and mindfulness in everyday life: Practical solutions for improving your health and performance. W. W. Norton & Company.
Khazan, I., Shaffer, F., Moss, D., Lyle, R. R., & Rosenthal, S. (Eds.). (2023). Evidence-based practice in biofeedback and neurofeedback (4th ed.). Association for Applied Psychophysiology and Biofeedback.
Lehrer, P. M., & Gevirtz, R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 5, Article 756. https://doi.org/10.3389/fpsyg.2014.00756
Meehan, Z. M. (2025). 5-min science: Inter-brain plasticity can enhance psychotherapy. https://www.biosourcesoftware.com/post/5-min-science-inter-brain-plasticity-can-enhance-psychotherapy
Mehling, W. E., Acree, M., Stewart, A., Silas, J., & Jones, A. (2018). The Multidimensional Assessment of Interoceptive Awareness, Version 2 (MAIA-2). PLOS ONE, 13(12), Article e0208034. https://doi.org/10.1371/journal.pone.0208034
Mehling, W. E., Price, C., Daubenmier, J. J., Acree, M., Bartmess, E., & Stewart, A. (2012). The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLOS ONE, 7(11), Article e48230. https://doi.org/10.1371/journal.pone.0048230
Peper, E., Shumay, D. M., & Moss, D. (2012). Change illness beliefs with biofeedback and somatic feedback. Biofeedback, 40(4), 154-159. https://doi.org/10.5298/1081-5937-40.4.05
Pollatos, O., & Schandry, R. (2004). Accuracy of heartbeat perception is reflected in the amplitude of the heartbeat-evoked brain potential. Psychophysiology, 41(3), 476-482. https://doi.org/10.1111/1469-8986.2004.00170.x
Rogel, A., Guez, J., Getter, N., Keha, E., Cohen, T., Amor, T., & Todder, D. (2015). Transient adverse side effects during neurofeedback training: A randomized, sham-controlled, double blind study. Applied Psychophysiology and Biofeedback, 40(3), 209-218. https://doi.org/10.1007/s10484-015-9289-6
Schwartz, M. S. (2010). A new improved universally accepted official definition of biofeedback: Where did it come from? Why? Who did it? Who is it for? What's next? Biofeedback, 38(3), 88-90. https://doi.org/10.5298/1081-5937-38.3.88
Sened, H., Zilcha-Mano, S., & Shamay-Tsoory, S. (2022). Inter-brain plasticity as a biological mechanism of change in psychotherapy: A review and integrative model. Frontiers in Human Neuroscience, 16, 955238. https://doi.org/10.3389/fnhum.2022.955238
Shafi, M. M., & Westover, M. B. (2018). EEG activation methods. In D. L. Schomer & F. H. Lopes da Silva (Eds.), Niedermeyer's electroencephalography: Basic principles, clinical applications, and related fields (7th ed.). Oxford University Press.
Sherlin, L. H., Arns, M., Lubar, J., Heinrich, H., Kerson, C., Strehl, U., & Sterman, M. B. (2011). Neurofeedback and basic learning theory: Implications for research and practice. Journal of Neurotherapy, 15(4), 292-304. https://doi.org/10.1080/10874208.2011.623089
Sitaram, R., Ros, T., Stoeckel, L., Haller, S., Scharnowski, F., Lewis-Peacock, J., Weiskopf, N., Blefari, M. L., Rana, M., Oblak, E., Birbaumer, N., & Sulzer, J. (2017). Closed-loop brain training: The science of neurofeedback. Nature Reviews Neuroscience, 18(2), 86-100. https://doi.org/10.1038/nrn.2016.164
Slawecki, T. M. (2009). How to distinguish legitimate biofeedback/neurofeedback devices. Biofeedback Certification International Alliance.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Wareing, L., Readman, M. R., Longo, M. R., Linkenauger, S. A., & Crawford, T. J. (2024). The utility of heartrate and heartrate variability biofeedback for the improvement of interoception across behavioural, physiological and neural outcome measures: A systematic review. Brain Sciences, 14(6), Article 579. https://doi.org/10.3390/brainsci14060579
Zhang, Y., Zhang, Q., Wang, J., Zhou, M., Qing, Y., Zou, H., Li, J., Yang, C., Becker, B., Kendrick, K. M., & Yao, S. (2023). "Listen to your heart": A novel interoceptive strategy for real-time fMRI neurofeedback training of anterior insula activity. NeuroImage, 284, Article 120455. https://doi.org/10.1016/j.neuroimage.2023.120455
Return to Top