Key Studies
What You Will Learn in This Chapter
This unit surveys the research evidence supporting neurofeedback's clinical and performance applications. You will explore representative randomized controlled trials (RCTs) and quasi-experimental studies across major clinical conditions: ADHD, traumatic brain injury, substance use disorders, epilepsy, anxiety disorders, depression, and tinnitus. By the end of this chapter, you will be able to identify the key protocols, leading researchers, and efficacy ratings that define the neurofeedback evidence base.
BCIA Blueprint Coverage: This unit addresses IV. Research Evidence Base for Neurofeedback - B. Key Research Studies.
This unit covers the growing body of research supporting clinical and performance applications of neurofeedback. Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.) provides a comprehensive review of these studies. Here, we summarize representative randomized controlled trials (RCTs)—experiments that randomly assign participants to treatment or control conditions—and quasi-experimental studies, which compare groups without full randomization. Together, these designs provide the strongest available evidence of treatment efficacy.
BCIA Blueprint Coverage

This unit covers Attention Deficit Hyperactivity Disorder, Mild Closed Head Injuries and Traumatic Brain Injury, Substance Use Disorder, Epilepsy, Anxiety and Anxiety Disorders including Post-Traumatic Stress Disorder, Depression, and Tinnitus. It closes with modifiable biological contributors to consider when clients do not respond, and with cutting-edge topics in neurofeedback research.
Evidence-Based Practice (4th ed.)
We have updated the efficacy ratings for clinical applications covered in AAPB's Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.).

Attention Deficit Hyperactivity Disorder (ADHD)
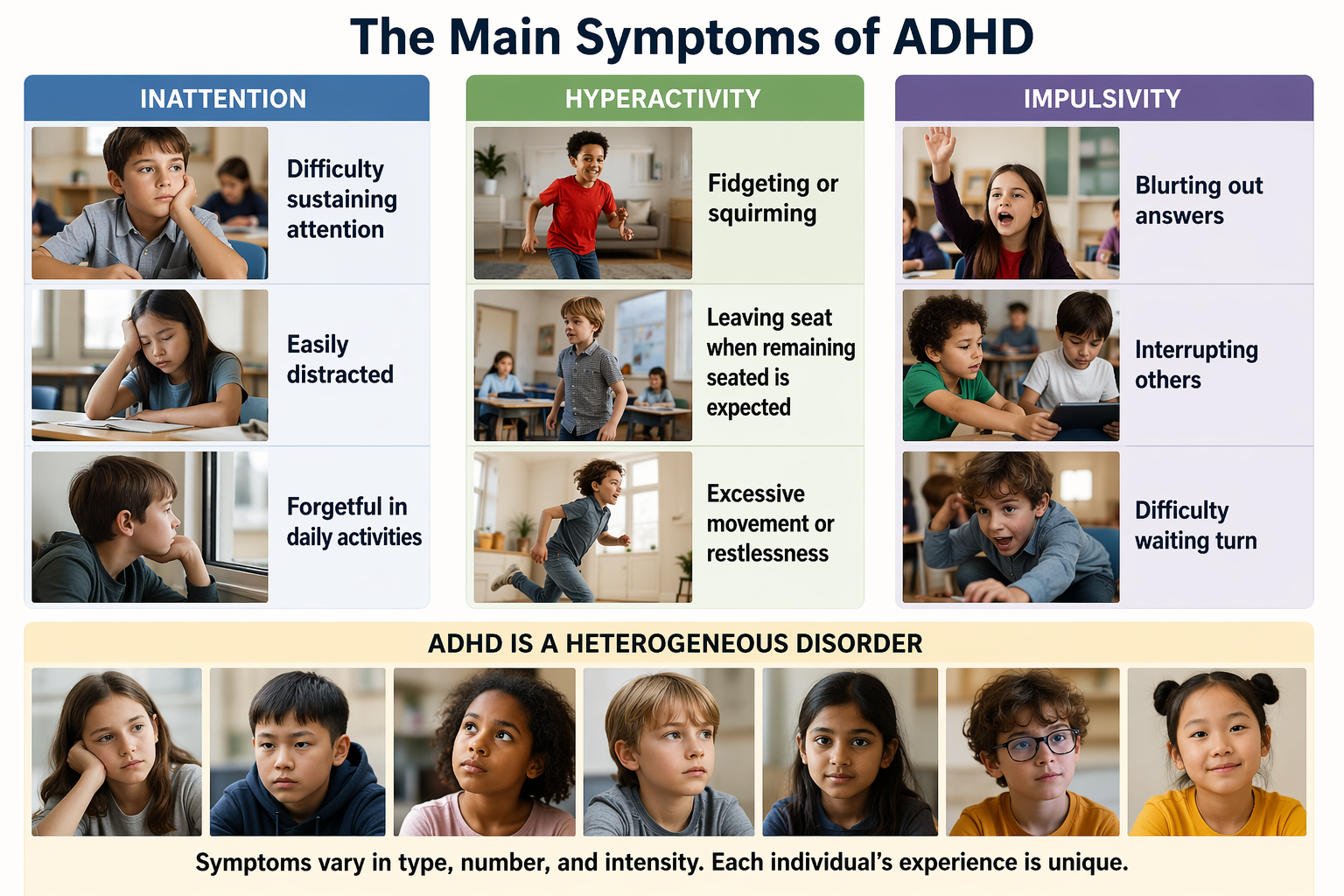
Attention Deficit Hyperactivity Disorder (ADHD) is characterized by a consistent pattern of inattention, hyperactivity, and impulsivity that disrupts daily functioning or development (American Psychiatric Association, 2013). ADHD is not simply being easily distracted or having high energy; it represents a fundamental difference in how the brain regulates attention and behavior. Most children diagnosed with ADHD carry some form of it into adolescence and adulthood, so this is not something most people simply "grow out of" (Spencer, Biederman, & Mick, 2007). Reported persistence rates vary enormously with the definition used rather than with the disorder's course, being highest for syndromatic remission and lowest for functional remission (Biederman, Mick, & Faraone, 2000), which is why any single percentage should be read alongside the criterion that produced it. Check out Dr. Russell Barkley's video ADHD is a Disorder of Impairment not Knowledge.
Attention Dysregulation Rather Than Attention Deficit
The disorder's name is a misnomer, and correcting it changes how you talk with clients and how you interpret what happens in the training room. A child who cannot stay with ten minutes of homework may spend six uninterrupted hours drawing characters from a favorite show or reading about black holes. That contradiction is not evidence that the attention is available on demand; it is evidence that its allocation is not under voluntary control. Most of attention is automated rather than deliberate, operating in the background to filter, prioritize, and suppress information much as breathing operates without conscious supervision (Anderson, 2021; Bishop, 2008). What we usually call "paying attention" is the small, effortful portion sitting on top of that automated system. In ADHD, the automated layer is chronically disrupted (Lin et al., 2015), so the difficulty is not a missing quantity of attention but unreliable control over when attention engages, where it settles, and how readily it releases. Atypical dopamine reward pathways, the neural circuits that assign motivational value to stimuli, appear to drive much of this unpredictability, which is why intrinsically rewarding material captures attention effortlessly while equally important but unrewarding material does not (Tripp & Wickens, 2024).
Because symptom expression depends heavily on environmental demand, the same child can look unimpaired in a highly structured classroom and profoundly impaired during an unstructured summer, and an adolescent who managed well with parental scaffolding may collapse academically during the first semester of college (Murray et al., 2019). Diagnosis typically occurs at the moment demands exceed capacity, which is why the Centers for Disease Control and Prevention (2013) found average diagnostic ages of 5 years for severe, 7 years for moderate, and 8 years for mild presentations. For the neurofeedback clinician, this variability carries three practical implications. First, a strong session followed by a poor one reflects the disorder rather than noncompliance, and framing it that way to families protects the therapeutic alliance. Second, an engaging feedback display can recruit attention that a dull display cannot, so in-session performance partly measures the screen rather than the client; varying displays and comparing performance across them guards against overinterpreting a single good run. Third, baseline and outcome assessments should sample more than one context, because a single clinic measurement taken in a quiet, novel, one-to-one setting is close to the best-case environment for a client with ADHD.
Persistence, Remission, and the Adult Client
The assumption that ADHD resolves with maturation shaped insurance coverage and treatment planning for decades, and it was wrong. Denworth (2024) summarizes evidence that roughly 2.5% to 3% of adults meet criteria compared with 5% to 6% of children, and that symptom-based estimates run considerably higher, approaching 9% in young adults. The DSM-5 lowered the adult symptom threshold and recognized that presentation changes with age: the child who climbed the furniture becomes the adult who cannot finish reports, sustain relationships, or pay bills on time. Full remission is uncommon. Reanalysis of longitudinal data by Sibley and colleagues found that only about 9% of people diagnosed in childhood showed no signs of ADHD in adulthood, and those cases tended to involve milder childhood symptoms and strong parental support (as reported in Denworth, 2024). The more typical course is fluctuation, with symptoms waxing and waning as environmental stress rises and falls.
Two features of this trajectory matter directly for neurofeedback practice. The first is the discontinuation cliff. Up to half of patients stop stimulant medication within the first year, and discontinuation peaks at age 18 as young adults move from pediatric to adult care, lose parental oversight, and absorb the cost themselves (Denworth, 2024). Many adults arrive at a neurofeedback clinic precisely at this transition, having lost a treatment that worked, and the durability evidence reviewed later in this unit is the most relevant thing you can offer them. The second is measurement. Because symptoms fluctuate with life circumstances independent of any intervention, a single pre-training and post-training comparison can easily capture a stressful semester rather than a training effect. Repeated measurement across the training course, documentation of concurrent life events, and follow-up assessment months after the final session all guard against attributing natural variation to your protocol.
Emotion Dysregulation as a Core Feature
Families frequently describe the presenting problem as temper rather than attention, and the research now supports taking that description seriously. Emotion dysregulation, meaning persistent difficulty managing emotional responses that produces heightened reactivity, prolonged distress, and reliance on maladaptive strategies such as suppression or rumination, appears in a systematic review by Soler-Gutiérrez, Pérez-González, and Mayas (2023) to be a core symptom of adult ADHD rather than a comorbid complication. Adults with ADHD score lower on emotion regulation measures with medium-to-large effect sizes relative to controls, and those deficits track strained relationships, workplace difficulty, and elevated rates of substance use. Emotion dysregulation is a transdiagnostic factor, a process that appears across many diagnoses including borderline personality disorder and depression, but in ADHD it is bound specifically to impulsivity and executive dysfunction, which distinguishes it from the same surface presentation in other conditions.
The neural account is one of impaired top-down control. Prefrontal cortex, which supports executive control; the anterior cingulate cortex, which integrates emotional and cognitive information and monitors conflict; the amygdala, which tags stimuli with emotional salience; and the orbitofrontal cortex, which links emotional information to personal goals, together fail to modulate emotional reactivity efficiently (Soler-Gutiérrez et al., 2023). Event-related potential studies show enlarged late positive potential (LPP) amplitudes in adults with ADHD, a sustained positive brain response to emotionally charged material that indexes how much processing an emotional stimulus is consuming. The enlargement suggests these clients are spending more neural effort to manage the same emotional load. Behaviorally, the signature is difficulty returning to baseline after a setback rather than an unusually large initial reaction.
This has immediate consequences for how you set up an ADHD case. Administer a standardized emotion regulation measure such as the Difficulties in Emotion Regulation Scale or the Emotion Regulation Questionnaire at intake and again at follow-up, because attention scores can improve while the complaint that brought the family in does not (Soler-Gutiérrez et al., 2023). Expect emotional reactivity inside the session as well, since a difficult trial or a missed reward threshold is exactly the kind of small setback these clients recover from slowly. Building in brief recovery pauses after failed trials, and coaching cognitive reappraisal rather than suppression as the client's in-session strategy, addresses the mechanism directly; suppression predicts slower emotional recovery and should be discouraged. Because the same review found medication and behavioral intervention to be synergistic for emotional outcomes, and because women with ADHD show greater emotion dysregulation on average, neurofeedback for these clients is usually best positioned as one component of a plan that also includes emotion-focused therapy, parent work, and, where appropriate, pharmacotherapy.
The Neurophysiological Basis of ADHD
Why do children with ADHD have trouble paying attention? The answer lies partly in their brainwave patterns. Children with ADHD often display an elevated theta/beta ratio (TBR), meaning they show too much slow-wave theta activity (4-8 Hz) and not enough fast-wave beta activity (13-21 Hz) over frontal and central brain regions (Wang, Wang, Wang, & Wong, 2024). To understand this, think of theta waves as the brain in a drowsy, daydreaming state, while beta waves represent the brain in an alert, focused mode. An elevated TBR suggests the brain is not revving up to full alertness when it should be.
This pattern may reflect cortical hypoarousal, a state where the cortex (the brain's outer layer responsible for higher functions) is not adequately activated. Imagine trying to concentrate while half-asleep: that is somewhat analogous to what children with ADHD experience. Their brains are not generating enough of the fast activity associated with sustained attention. The TBR may also reflect deficient cortical responses during mental effort or impaired top-down attention control, the ability to voluntarily direct attention where you want it, mediated by the dorsolateral prefrontal cortex (Bluschke et al., 2016; Wang et al., 2024).
Why TBR Seemed Like a Big Deal
The EEG theta/beta ratio (TBR) took off in ADHD because early studies often found that, on average, people with ADHD showed relatively more slow "theta" activity and/or less faster "beta" activity at rest—making TBR look like a simple, objective biomarker. But when researchers pooled results across many studies, the picture got messy. The grand mean effect was substantial (d = 0.62 across ages 6 to 18), yet effects varied a lot between samples and drifted downward over the years, and the drift came from rising TBR in the non-ADHD comparison groups rather than from any change in the ADHD groups. The authors' conclusion was that excessive TBR cannot be considered a reliable diagnostic measure, while a substantial subgroup of patients does deviate on it and may derive prognostic information from it (Arns et al., 2013).
The Core Problem: It's Not Specific Enough
TBR changes for plenty of reasons that aren't ADHD—like drowsiness, sleep loss, developmental stage, and medication effects—so a high value can't cleanly separate ADHD from non-ADHD. That overlap is why the American Academy of Neurology's practice advisory cautions that TBR should not be used to confirm ADHD (outside research) and warns about misdiagnosis risk if it's treated like a diagnostic test (Gloss et al., 2016).
ADHD Isn't One Brain Pattern
A key modern insight is that ADHD is heterogeneous: there may be a subgroup with elevated TBR, not the whole diagnosis. Large-sample work has reported evidence for a "high-TBR cluster" that represents only a minority of people with ADHD, which fits the broader view that multiple EEG profiles can exist under the ADHD umbrella (Bussalb et al., 2019; Bong & Kim, 2021).
So What's the Controversy, in One Line?
TBR can be an interesting research signal and sometimes an assessment aid, but overreliance turns a state-sensitive, non-specific ratio into a pseudo "brain test for ADHD"—a leap the evidence and guidelines don't support (Arns et al., 2013; Gloss et al., 2016).
Beyond Surface Power: Network and Connectivity Dysregulation
Surface power measures like TBR treat each electrode as an isolated report on local activity, but the brain regulates behavior by coordinating specialized regions into networks, distributed sets of structures that activate together to accomplish a task. Kerson and colleagues (2023) examined this coordination directly in the baseline EEG of 120 rigorously diagnosed children aged 7 to 10 from the ICAN trial, a multisite double-blind study of theta/beta neurofeedback. They analyzed coherence, a measure of how consistently the signals from two brain regions maintain their phase relationship and therefore an index of functional communication between them, along with phase relationships across every Brodmann area connection within five networks and across all major frequency bands. Brodmann areas (BAs) are numbered cortical regions defined by differences in cell architecture, each associated with characteristic functions. Because the resulting dataset held hundreds of possibilities per data point, the team used a Monte Carlo model, a machine learning method that repeatedly draws random samples and aggregates the results to establish confidence in patterns buried in complex data, comparing each child against an age-matched normative database.
The finding was hypocoherence, meaning reduced connectivity between regions rather than excessive connectivity, concentrated in three networks: the default mode network (DMN), which supports self-referential thought and mind-wandering; the salience network (SalN), which detects behaviorally relevant stimuli and switches processing toward them; and the attention dorsal network (AttDN), which directs and sustains goal-driven attention. Within those networks, Brodmann areas 7, 10, and 11 were the most dysregulated. BA 7 sits in superior parietal cortex and supports visuospatial attention, BA 10 occupies the frontal pole and supports higher-order planning, and BA 11 lies in orbital prefrontal cortex, part of the ventromedial prefrontal cortex tied to decision-making and emotion regulation. Secondary involvement appeared in areas serving language, object and face recognition, and visuomotor planning, including BAs 21, 30, 35, 37, 39, and 40 (Kerson et al., 2023).
Reduced connectivity in exactly the networks responsible for detecting what matters, switching toward it, and holding attention there is a coherent account of the disorganization families report, and it points toward training targets that a single Cz montage cannot reach. The dysregulated areas map onto familiar recording sites: BA 10 and BA 11 lie beneath the frontopolar sites Fp1 and Fp2, and BA 7 lies beneath the parietal sites P3, Pz, and P4. That correspondence is the practical rationale for connectivity training aimed at frontoparietal coherence in clients whose qEEG shows hypocoherent long-range connections, and for qEEG-guided site selection generally rather than a fixed protocol applied to every ADHD referral. Two cautions belong with that enthusiasm. Scalp coherence is degraded by volume conduction, the spread of electrical current through tissue from a single source to multiple electrodes, which can manufacture apparent connectivity where none exists; and the inverse problem means surface recordings can never uniquely identify which cortical generators produced them. Source-localized findings identify plausible targets, not certainties, and should inform protocol selection alongside the clinical picture rather than override it.
EEG Biomarkers Beyond the Theta/Beta Ratio
Because TBR alone cannot carry diagnostic weight, attention has shifted to other electrophysiological features that add information beyond behavioral observation. Alpha power, the magnitude of oscillations in the 8 to 12 Hz band traditionally associated with relaxed wakefulness and cortical inhibition, is one of them. Adults with ADHD show attenuated relative alpha at baseline, which the authors interpret as cortical hyperactivation, and after a session of neurofeedback targeting alpha desynchronization, resting alpha rebounded partway toward control values, with the size of that rebound correlating within individuals with fewer commission errors on a Go/No-go task, the standard laboratory measure of response inhibition in which participants must withhold a prepared response (Deiber et al., 2019). Note that this cuts against the hypoarousal account offered earlier, and the tension is real rather than apparent. Different bands index different things: elevated theta and an elevated theta/beta ratio support a hypoarousal reading, while reduced alpha indexes greater activation in that band, and spindling excessive beta has itself been read as a hypoarousal pattern despite being a beta excess. The field's resolution is that ADHD is electrophysiologically heterogeneous, so hypoarousal describes one subgroup rather than the disorder, and arousal claims should always be tied to a specific band and a specific subtype. That combination is notable because it links a trained EEG change to a behavioral change in the deficit of interest. In children the picture is less uniform: some show subtypes with elevated alpha, and elevated alpha is more common when depression is comorbid, which limits its specificity (Byeon et al., 2020; Poil et al., 2014). More consistent is impaired alpha modulation during cognitive work. Children with ADHD show weaker alpha decreases while encoding information into working memory, and the magnitude of that failure correlates with poorer executive function and reading comprehension (Lenartowicz et al., 2018).
Event-related potentials (ERPs), voltage changes in the ongoing EEG that are time-locked to a specific stimulus or response and therefore index discrete stages of information processing, offer the most mature alternative. The P300, a positive deflection peaking roughly 300 to 600 ms after a task-relevant stimulus, is reduced in amplitude and delayed in latency in ADHD, reflecting deficient allocation of attentional resources. The contingent negative variation (CNV), a slow negative shift that builds during the interval between a warning signal and an expected imperative stimulus, is smaller and less sustained, reflecting impaired preparation. Meta-analysis places these differences at moderate effect sizes and locates them primarily in later, cognitive components rather than early sensory ones (Banaschewski & Brandeis, 2007; Kaiser et al., 2020). Error-processing components differ as well: the error-related negativity (ERN), a sharp negative deflection appearing within about 100 ms of a mistake, and the error positivity (Pe), the later positive deflection associated with conscious error awareness, both index the performance monitoring that ADHD disrupts (Groom et al., 2010). Combining ERP measures with Go/No-go performance produced a diagnostic index that separated children with ADHD from typically developing peers with large effect sizes and replicated in an independent sample (Häger et al., 2021).
None of these are diagnostic tests, and the honest summary is that they offer incremental validity over behavioral observation alone rather than a replacement for it. Their practical value in a neurofeedback practice lies in outcome measurement and protocol selection. An ERP paradigm recorded before and after a training course gives you a mechanism-level outcome that parent rating scales cannot supply, and a client whose primary abnormality is a flattened CNV is a candidate for slow cortical potential training on theoretical grounds in a way that a client with elevated resting TBR is not.
Screening for Refractory Features Before Training
The most actionable EEG findings in ADHD may be the ones that have nothing to do with power ratios. Reviewing routine clinical EEG in 1,233 treatment-refractory psychiatric patients, Swatzyna and colleagues (2024) identified four recurring features. Focal slowing, localized low-frequency activity indicating regional cerebral dysfunction often tied to old injury or lesion, appeared in 53.4% of the sample. Spindling excessive beta (SEB), frontocentral beta activity in the 15 to 35 Hz range with a spindle-like morphology, appeared in 25.1% of refractory cases and in about 12% of a broader psychiatric sample; a replication study confirmed that patients with SEB show more impulse-control problems (d = 0.87) and more false-positive errors (d = 0.55), though it failed to replicate the proposed link to sleep problems (Arns et al., 2015; Krepel et al., 2021). Encephalopathy, diffuse slowing and amplitude attenuation reflecting toxic, metabolic, or hypoxic compromise, appeared in 10.9%. Isolated epileptiform discharges (IEDs), brief abnormal waveforms indicating cortical hyperexcitability, appeared in 24.3% of the refractory sample overall, and a systematic review found them in more than a quarter of ADHD cohorts, well above the roughly 1% to 3% reported in healthy children (Swatzyna et al., 2020, 2024). These are refractory-sample rates; do not read them as base rates for ADHD generally.
Critically, none of this is predictable from the diagnosis. Swatzyna and colleagues (2015) found only about 6% alignment between formal DSM diagnoses and specific EEG abnormalities across 386 refractory cases, which means a symptom-based referral tells you almost nothing about whether one of these features is present. The clinical consequences are concrete. Epileptiform activity is frequently subclinical and invisible to behavioral observation, yet both stimulants and antidepressants can lower seizure thresholds, so its detection changes medication decisions and warrants referral to a neurologist before training proceeds. Spindling excessive beta argues against reflexive beta up-training over frontocentral sites, since the standard Lubar approach would reward activity that is already excessive. Focal slowing raises the question of an unreported head injury and may redirect the case toward the protocols discussed in the traumatic brain injury section of this unit. Capturing any of this requires reviewing the raw, artifact-inspected EEG in eyes-open and eyes-closed conditions rather than reading a spectral summary alone, which is the single most useful habit a neurofeedback clinician can adopt at intake.
Key Concept
Understanding the neurophysiology of ADHD helps explain why telling a child with ADHD to "just pay attention" is rarely effective. Their brain is not generating the neural activity patterns needed for sustained focus. Neurofeedback trains the brain to produce these patterns, addressing the root cause rather than just managing symptoms.
Assessment Before Training: Sample Drift and Diagnostic Confidence
Every assessment instrument carries a quiet assumption that the client in front of you resembles the people it was built on. Diagnostic validity statistics are not properties of a disorder; they are properties of a test applied to a particular derivation sample, the population from which criteria, norms, and accuracy figures were originally generated. Sensitivity, the probability that a test is positive when the condition is present, and specificity, the probability that it is negative when the condition is absent, describe how an instrument performed in that sample under those conditions. The DSM-5 ADHD criteria and most rating scale norms were refined on samples that were disproportionately young, school-age, male, white, and clinic-referred (Barkley, 2015). The further a client departs from that profile, the less those numbers can be trusted, a phenomenon best described as sample drift.
College students illustrate the problem cleanly. Lefler and colleagues (2021) note that students are older than the derivation samples, lack the teacher informants that child-normed instruments assume, and become their own primary informant at precisely the moment when motivation to over-report may be elevated by accommodation-seeking or stimulant access. The requirement that symptoms be present before age 12 rests almost entirely on recall, which is vulnerable to bias in both directions, and the clinically important distinction between late-onset ADHD, in which symptoms genuinely first appear in adulthood and are more often attributable to another condition, and late-identified ADHD, in which longstanding symptoms were simply never recognized, is frequently collapsed in practice. Girls and women present a parallel case: the overt hyperactivity and disruptive classroom behavior that anchored the original criteria map more closely onto male presentation, while inattentive symptoms and internalizing comorbidities are more easily misattributed to anxiety (Quinn & Madhoo, 2014). Racial and ethnic minority youth are similarly underrepresented in normative samples, and referral bias compounds the effect, with Black children more likely to be referred for disruptive behavior and less likely to receive an ADHD diagnosis than white peers with comparable symptom profiles (Epstein et al., 2005).
One finding from this literature bears directly on how neurofeedback outcomes are measured. Continuous performance tests such as the TOVA appear throughout the studies reviewed in this unit and throughout everyday practice, yet a meta-analysis pooling 19 studies of commercially available continuous performance tests found their standalone diagnostic accuracy to be modest, with sensitivities from 0.59 to 0.75 and specificities from 0.66 to 0.74 across subscales (Arrondo et al., 2024). A high score neither confirms ADHD nor does a normal score exclude it. The useful distinction is between classification and change: these tasks are weak at separating one person from another but remain reasonable for tracking the same client against their own baseline, provided you administer them under consistent conditions and interpret a single score cautiously. Alongside them, gather collateral information from a parent, partner, or roommate, obtain historical records such as report cards and prior evaluations, and use validated impairment scales. Lefler and colleagues (2021) recommend that no diagnosis rest on self-report alone regardless of symptom severity, and that recommendation applies with equal force to the referral diagnosis you inherit before beginning training.
Distinguishing ADHD from Oppositional Defiant Disorder
Referrals for "attention problems" often arrive describing a child who argues, refuses, and loses their temper, and separating the two disorders that can produce that description changes what training can reasonably accomplish. Oppositional defiant disorder (ODD) is characterized by a persistent pattern of angry and irritable mood, argumentative or defiant behavior, and vindictiveness directed at authority figures. Its dysfunction lies in emotional regulation and social interaction rather than attention, and it is more closely associated with environmental and familial stressors than with the executive deficits that define ADHD (Forssman et al., 2012). Clinicians routinely fall into a diagnostic halo effect, in which the visibility of one symptom cluster colors the perception of another, so that impulsivity reads as defiance or defiance reads as inattention. Three questions usually separate them in practice: whether the behavior appears across settings or mainly with particular adults, whether it emerged early in development or situationally, and whether it looks unintentional or deliberate. ADHD symptoms are cross-situational, early, and unintentional; ODD behaviors are situational, emotionally reactive, and most pronounced with authority figures (Kaźmierczak-Mytkowska et al., 2022; Seppä et al., 2024).
Two consequences follow for neurofeedback. First, children with comorbid ADHD and ODD respond less well to methylphenidate than children with ADHD alone (D'Aiello et al., 2024), which means a substantial share of the families arriving at a neurofeedback clinic after medication disappointment are carrying an unrecognized ODD component. Their expectation that training will succeed where medication failed needs to be met with an honest account of what attention training addresses. Second, ODD shows up inside the training room as refusal to wear the cap, arguing about session length, and negotiating the reward criteria. That behavior is not resistance to neurofeedback specifically and will not resolve as attention improves; it requires behavioral parent management work and an explicit contingency plan established before training begins rather than improvised in session six.
Neurofeedback Protocols for ADHD
The Lubar ADHD protocol emerged from Joel Lubar and his colleagues' pioneering research with ADHD children at the University of Tennessee. The basic protocol trains clients to inhibit (reduce) theta activity (4-8 Hz) while increasing beta activity (13-21 Hz) over approximately 40 sessions, with each session using 30-minute training periods. The logic is straightforward: if the problem is too much slow activity and not enough fast activity, train the brain to shift that balance.
For electrode placement, the active electrode is typically placed at CZ (the top-center of the head) for most patients, with reference to the left ear and a ground on the right ear. Clinicians may adjust placement based on individual needs: C3 (left-center) for those who need to increase frontal activation, and C4 (right-center) for those with right-hemisphere deficits.
Landmark Research Studies
Lubar and Shouse (1976) published the first single-case experimental demonstration of neurofeedback for hyperkinesis (the earlier term for ADHD). Their elegant design followed one 11-year-old boy, medicated with methylphenidate throughout, across five sequential phases: no drug, drug only, drug plus training to increase SMR (sensorimotor rhythm) while suppressing theta, drug plus a reversed contingency that decreased SMR while increasing theta, and finally a return to the original training. Hyperkinetic behavior and sustained schoolwork improved under the SMR increase/theta decrease contingency, deteriorated toward pretraining levels when the contingency was reversed, and improved again when it was reinstated. That within-subject reversal is what makes the demonstration persuasive, since it is difficult to explain by placebo response or by time spent with clinicians. Shouse and Lubar (1979) extended the design to four children, three of whom showed contingent EEG change tied to improved classroom behavior; the fourth never acquired the response and did not improve.
Lubar and Lubar (1984) trained 6 children with attention deficit disorders twice weekly for 10 to 27 months, with a gradual phase-out, combining EEG biofeedback with academic support. All six improved on grades or achievement measures, and none remained on medication for hyperkinetic behavior at the end of treatment. The paper reports no long-term follow-up, and the 8-year follow-up figure sometimes attributed to it does not appear there.
The intelligence and continuous-performance findings often folded into that study belong to a separate, larger one. Lubar, Swartwood, Swartwood, and O'Donnell (1995) trained 23 clients aged 8 to 19 in an intensive summer program and found that those who successfully reduced theta over the training sessions showed roughly a 12-point gain in WISC-R IQ and significant improvement on the Test of Variables of Attention (TOVA), while those who did not reduce theta showed neither. That conditional relationship is the more interesting finding, because it ties the behavioral change to the trained EEG change rather than merely to time in treatment.
Lubar (1995) followed 52 patients treated with neurofeedback for as long as 10 years. Their improvement on the Conners scale, a standard measure of attention and ADHD symptoms, remained stable at follow-up. This durability distinguishes neurofeedback from medication, which typically stops working as soon as it is discontinued.

Dr. Joel Lubar, pioneer of neurofeedback treatment for ADHD.
Rossiter and La Vaque (1995) conducted a head-to-head comparison, matching subjects on age, IQ, gender, and diagnosis and assigning them to either Ritalin (the most common ADHD medication) or neurofeedback. Both groups improved comparably on TOVA measures of inattention, impulsivity, information processing, and response variability. This finding challenged the assumption that medication was the only effective treatment for ADHD. Note the design limit, which the authors' later replication states plainly: assignment followed patient and parent preference rather than randomization, so this is a matched quasi-experiment and cannot by itself establish equivalence.
Thompson and Thompson (1998) reported treating 98 children and 13 adults over 40 fifty-minute sessions using Lubar's ADHD protocol. The percentage of children using Ritalin declined from 30% at the start of the study to just 6% post-treatment, suggesting many children no longer needed medication after completing neurofeedback. Theta/beta ratios significantly declined for children but not for adults, and participants achieved impressive gains on intelligence tests, the TOVA, and the Wide Range Achievement Test.

Drs. Lynda and Michael Thompson, pioneers in neurofeedback research and clinical practice.
Monastra, Monastra, and George (2002) compared 49 children in a 1-year multimodal program (Ritalin, parent counseling, and academic consultation) with 51 children who received the same program plus neurofeedback (weekly 30 to 40-minute sessions training SMR or beta while suppressing theta at the vertex, with points exchangeable for a $15 cash reward). Assignment followed parental preference rather than randomization, which is the study's principal limitation.
Here is the critical finding: both groups significantly improved on the TOVA and the Attention Deficit Disorders Evaluation Scale when medicated with Ritalin, but only the group that received neurofeedback maintained performance gains when unmedicated. A qEEG scan confirmed that reduced cortical slowing occurred only in children who received neurofeedback. In other words, medication improved performance temporarily, but neurofeedback produced lasting brain changes. Parenting style moderated behavioral symptoms at home but not in the classroom, highlighting the importance of parent involvement.

Dr. Vincent Monastra, researcher in neurofeedback treatment for ADHD.
Gevensleben and colleagues (2009) conducted a multisite randomized controlled study of 102 children diagnosed with ADHD, of whom 94 were analyzed. The neurofeedback group received training that combined blocks of theta/beta training and slow cortical potential neurofeedback, while the control group received computer-based attention skills training. The combined neurofeedback group outperformed the control group on parent and teacher ratings, and both neurofeedback protocols produced comparable changes. Effect sizes on the primary parent-rated outcome were 0.60, with 0.64 for teacher ratings. Importantly, these gains were maintained at a 6-month follow-up, where the effect size was 0.71 (Gevensleben et al., 2010), suggesting the training produced lasting improvements; note that only 61 of the 94 analyzed children contributed follow-up data.
One evidence rating is often quoted in this field and is worth stating precisely, because it is frequently misattributed. PracticeWise, the company that produces the Blue Menu of Evidence-Based Psychosocial Interventions distributed with American Academy of Pediatrics materials, has since 2012 assigned biofeedback a Level 1, Best Support rating for attention and hyperactivity behaviors, and the current edition still does (PracticeWise, 2026). Three qualifications belong with that fact. The rating is PracticeWise's rather than the Academy's; the table names biofeedback rather than neurofeedback, although the trials underlying it used EEG biofeedback; and Level 1 requires only two randomized trials by independent teams using manuals, so biofeedback shares the category with six other interventions rather than standing above them. Most importantly, the Academy's own clinical practice guideline reaches a different conclusion: Wolraich and colleagues (2019) place EEG biofeedback among interventions with too little evidence to recommend. Report the PracticeWise rating accurately, and do not present it as an Academy endorsement.
A NeXus-10 BioTrace+ caterpillar game. The three caterpillars represent the theta, SMR, and beta frequency bands.
Executive Function Outcomes and the Question of Dose
The landmark studies above established that neurofeedback changes ADHD symptoms. A more recent question is whether it changes the underlying self-regulatory machinery. Executive function refers to the family of higher-order processes that allow a person to inhibit impulses, hold information in mind, and shift flexibly between tasks, and roughly half of children with ADHD show measurable deficits in it (Diamond, 2013; Zhong et al., 2025). Zhong and colleagues (2025) addressed the question with a preregistered systematic review and meta-analysis in Scientific Reports pooling 17 randomized and controlled trials of children aged 6 to 17, comprising 939 participants, with total training time ranging from 119 to 2,400 minutes. Control conditions included no treatment, treatment as usual, physical activity, cognitive training, electromyographic biofeedback, behavior therapy, and medication. Because outcomes were measured on different scales, results were expressed as the standardized mean difference (SMD), an effect size that converts each study's result into common units so they can be combined.
Two domains improved. Inhibitory control, the capacity to suppress an impulsive or inappropriate response, improved across 12 studies and 640 participants with an SMD of 0.36 and low variability across studies. Working memory, the ability to hold and manipulate information briefly, improved across seven studies and 370 participants with an SMD of 0.37, though variability here was high, signaling that not all protocols delivered equally. Global executive function measured by the Behavior Rating Inventory of Executive Function, a standardized parent and teacher questionnaire on which lower scores indicate better everyday functioning, favored neurofeedback across the three studies that used it. Cognitive flexibility, the ability to shift between mental sets or strategies, could not be pooled because too few trials assessed it, which remains a real gap in the evidence (Zhong et al., 2025).
The most clinically useful finding concerns dose. Splitting the trials at the median of 1,260 minutes of total training, roughly 21 hours, changed the picture entirely. Below that threshold, neither inhibitory control nor working memory improved significantly. Above it, both did, with inhibitory control at an SMD of 0.30 and working memory at 0.44 (Zhong et al., 2025). Treat those subgroup values as approximate: both fall below the overall pooled estimate for inhibitory control, which cannot be true of a proper subgroup decomposition, so the published subgroup figures appear internally inconsistent even though the qualitative dose pattern stands. Set against the classic Lubar protocol of approximately 40 sessions using 30-minute training periods, which yields about 1,200 minutes of actual training, that threshold is a warning rather than a reassurance: a course delivered at the low end of conventional practice sits just below the point at which executive gains became detectable in this analysis. Session count is the wrong unit. What accumulates is active training time, and a 45-minute session that contains 20 minutes of actual feedback is not the same dose as one containing 35. Tracking cumulative training minutes rather than session numbers, and telling families at the first appointment that meaningful executive change is a multi-month commitment, sets expectations that the evidence can actually support.
Durability partly justifies that demand. Six to twelve months after training ended, working memory gains remained robust with an SMD of 0.63, while inhibitory control showed a marginally sustained effect, a pattern consistent with earlier evidence that neurofeedback effects on attention and impulsivity outlast the training period (Van Doren et al., 2019; Zhong et al., 2025). Gains that persist after the equipment is put away suggest lasting neural adaptation rather than practice on a task, and that distinction is worth explaining to a family weighing a demanding protocol. The candid limitations belong in the same conversation. Effect sizes were small to moderate, working memory results were heterogeneous, and the authors detected publication bias specifically within the long-duration subgroup analyses, where positive trials may be overrepresented. An earlier meta-analysis of 10 trials found no significant benefit for response inhibition, sustained attention, or working memory as assessed by neuropsychological tests, although more sessions trended toward better response inhibition (Louthrenoo et al., 2022). Neurofeedback earns its place here as an adjunct with durable, modest effects, not as a cure.
What Changes and What Does Not: Evidence from the ICAN Trial
If theta/beta training works by lowering theta, then theta should fall in the children who improve. Enriquez-Geppert and colleagues (2024) tested that assumption directly using EEG data from the multicenter, double-blind ICAN randomized controlled trial. Their sample comprised 142 children aged 7 to 10 with ADHD and elevated TBR of at least 4.5 at Fz or Cz, randomized in a 3:2 ratio to real neurofeedback (n = 84) or sham neurofeedback (n = 58), a control condition in which feedback is generated from prerecorded EEG rather than the child's own brain activity. Both groups completed 38 sessions over 14 weeks, and both received coaching, lifestyle recommendations, and rewards; medication was withheld for five days before each assessment. The team measured resting-state EEG across two minutes each of eyes open and eyes closed, and task-related theta during an oddball task, in which participants respond to infrequent target tones amid frequent standard tones. They separated global theta, averaged across electrode sites, from frontal-midline theta, which arises from medial prefrontal regions during cognitive control, and compared clinical remitters, children showing meaningful symptom reduction on standardized behavioral assessment, with non-remitters.
Resting theta did not change. Global theta shifted by a mean of −0.013 and frontal-midline theta by −0.012, with no significant differences between the real and sham groups and none between remitters and non-remitters. During error processing on the oddball task, however, the groups diverged sharply: remitters showed increased global theta after training while non-remitters showed a decrease, and a significant three-way interaction emerged for frontal-midline theta. Task accuracy and reaction time were unchanged (Enriquez-Geppert et al., 2024). Weigh those subgroup results against their samples: the resting-state analysis rests on 68 children and the error-processing analysis on 30, so the remitter and non-remitter divergence is suggestive rather than settled. The parent trial itself found no benefit on its primary outcome (Arnold et al., 2021).
Three practical lessons follow. The first is a measurement lesson: do not use resting TBR or resting theta as your marker of progress. In a large, well-controlled trial they failed to move even in the children who improved clinically, so a flat resting spectral profile at session 20 is not evidence that training is failing, and a favorable one is not evidence that it is working. Behavioral rating scales completed by multiple informants and task-based measures remain the defensible outcome metrics. The second is a mechanism lesson: the changes that tracked clinical improvement appeared during error processing, when the brain was actively monitoring its own performance, which points toward protocols and training tasks that engage cognitive control rather than passive rest, and toward more selective targeting of theta-band networks than a broadband down-training of theta can achieve. The third is a humility lesson: the divergence between remitters and non-remitters occurred regardless of whether children received real or sham feedback, a reminder that coaching, structure, reward contingencies, and lifestyle change are doing real work inside every neurofeedback protocol. That is not an argument against the training; it is an argument for delivering those bundled components deliberately rather than treating them as incidental to the screen.
Clinical Efficacy
Based on six randomized controlled trials, Stefanie Enriquez-Geppert and colleagues rated neurofeedback for ADHD level 5, efficacious and specific in Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.). This is the highest possible rating, indicating strong evidence of effectiveness with well-controlled studies demonstrating superiority over credible placebo treatments.
Neurofeedback produces larger effects on inattention than hyperactivity/impulsivity (Chen et al., 2022; Van Doren et al., 2019). Think of neurofeedback like a workout for specific brain rhythms. The two protocols researchers have studied most, theta/beta ratio training and SMR enhancement, place sensors on the top of the head (at sites called Cz and Fz) and train the brain waves that control how alert, focused, and mentally "online" a person feels (Arns et al., 2014; Enriquez-Geppert et al., 2019).
When someone learns to dial down slow theta waves and crank up faster beta waves at the front of the scalp, the biggest changes show up in the medial and inferior frontal parts of the brain, the same regions that help you stay on task and catch yourself before making a mistake (Bluschke et al., 2016). SMR training seems to work through a slightly different route: it strengthens the thalamocortical circuits that generate sleep spindles, which in turn sharpens daytime vigilance and drives improvements in attention (Arns & Kenemans, 2014).
Hyperactive movement, though, is a different beast. It is generated deep in the brain by the basal ganglia and striatum, structures buried far below the scalp where surface electrodes simply cannot reach. So when neurofeedback reduces fidgeting and restlessness, it is probably doing so indirectly, by letting the cortex keep a tighter leash on motor output, or through the general benefits of sitting still and practicing self-control for an hour at a time (Solanto, 2002).
Research comparing different protocol variations found that beta upregulation, whether alone or combined with theta training, produced the most consistent improvements in response inhibition and conflict control (Enriquez-Geppert, Smit, Pimenta, & Arns, 2019). This suggests that enhancing fast brain activity may be particularly important for improving the cognitive control deficits central to ADHD.
Reviewing the same protocols for Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.), Enriquez-Geppert and colleagues (2023) emphasize that the efficacy rating attaches to personalized delivery rather than to a generic procedure. Established protocols show medium-to-large effect sizes with benefits that outlast medication over time, and that advantage is enhanced when protocol selection is guided by EEG subtyping rather than applied uniformly to everyone carrying the diagnosis.
Personalizing the Session for the Client with ADHD
Efficacy established in a trial has to survive contact with a restless nine-year-old in a chair for 45 minutes. Personalization is not a luxury here. Counting the ways the DSM-5 criteria can be satisfied gives some sense of the heterogeneity: with nine inattention and nine hyperactivity-impulsivity symptoms and a threshold of six in a domain, there are 116,220 qualifying symptom profiles for a child, and 196,608 once the adult threshold of five is applied (Silk et al., 2019). A large state space does not by itself mean that no two clients are alike, since symptoms cluster rather than combine at random, but it does mean that a single protocol applied to a diagnostic label will fit some clients much better than others. Meanwhile the traditional therapeutic frame of sustained sitting, focused engagement, and quiet cooperation asks precisely what these clients cannot easily give. A former young adult client described the internal experience this way:
Looking back, I felt like I was thinking through mud. The teacher would explain an assignment and I would try to write down what she said but I'd get lost along the way and if I raised my hand to ask her to repeat, she would complain that I wasn't paying attention… After doing neurofeedback, I can now organize things and make my way through step-by-step processes. I'm still not at a typical level but I'm so much better that everyone notices and remarks on the changes. I still often feel like I'm trying to think through mud, it's just that the mud is quite a bit thinner than it used to be.
Several adjustments follow directly from the symptom picture. Hyperactive-impulsive behavior degrades physiological measurement as much as it disrupts conversation, so fidgeting, squirming, and talking during acquisition contaminate the very signal you are training; addressing movement artifact through seating, brief movement breaks, and realistic session length is a data-quality intervention, not merely a behavioral one. Frequent brief pauses help substantially, and a common practical rhythm is roughly ten seconds of rest every three minutes, which lets the client discharge restlessness on a predictable schedule rather than at random. Advance prompts about transitions, such as announcing that two minutes remain before switching tasks, reduce the frustration that abrupt changes provoke (Barkley, 2015).
Goal setting deserves equal care. Break the training course into achievable steps and set thresholds the client can actually reach, since a criterion that yields reward on 20% of trials teaches helplessness rather than self-regulation (DuPaul & Stoner, 2014). Immediate, consistent, reward-based feedback improves behavioral and academic outcomes in this population, and rewards can be tangible or intangible, from stickers to praise to extra playtime (Chronis et al., 2004; Pelham & Fabiano, 2008). One of the genuine advantages of any biofeedback modality is that progress is visible in real time, within a session, and across sessions; showing a client their own trend line converts an abstract commitment into visible accomplishment and helps sustain the extended dose the outcome literature requires. Structure outside the session supports the same goal, since consistent routines, visual schedules, checklists, timers, and planners measurably reduce inattention and hyperactivity (Evans et al., 2014).
Finally, involve the parents deliberately. Behavioral parent training programs significantly improve behavior and reduce symptoms on their own (Chronis et al., 2004), and the clinic is a natural place to model the strategies parents will use at home. Inviting a parent to observe how you prompt transitions, set reachable thresholds, and praise effort rather than outcome gives them a concrete method rather than an instruction. It also addresses the emotional context that surrounds most of these families, in which a child accumulates corrections and reminders far faster than praise and internalizes a message of inadequacy that criticism itself can worsen (American Psychological Association, 2016; Peris & Miklowitz, 2015). Reframing the family's question from "why aren't they trying harder" to "what structure is missing" is part of the treatment, not a preamble to it.
Integrating Neurofeedback into a Multimodal Plan
The evidence assembled in this section points consistently toward integration rather than substitution. Executive gains were strongest when neurofeedback complemented cognitive training, cognitive-behavioral therapy, behavioral parent work, or medication rather than standing alone (Zhong et al., 2025). Emotion dysregulation responds to combined pharmacological and behavioral approaches with synergistic effects that neither achieves separately (Soler-Gutiérrez et al., 2023). Comorbid ODD requires its own behavioral intervention regardless of what happens to attention (D'Aiello et al., 2024). And the ICAN findings suggest that the coaching and contingency components bundled with training carry real weight of their own (Enriquez-Geppert et al., 2024).
This integrative stance also answers a broader critique. Writing in The New York Times Magazine, Tough (2025) argued that the field has leaned too heavily on a medical model of inherent biological deficiency, citing failures to replicate neuroimaging and genetic findings and the long-term outcomes of the Multimodal Treatment of ADHD study, in which the initial advantage of stimulant medication faded over time (Swanson et al., 2017). The critique lands where it concerns diagnostic inflation and overreliance on medication, and it is a useful corrective to any claim that a single EEG number defines the disorder. It overreaches when it dismisses neurobiological contributions altogether, because doing so would discard the refractory-case features, ERP differences, and connectivity findings reviewed above, along with the families whose children carry pronounced neurocognitive impairment that environmental adjustment alone does not resolve. The defensible position for a neurofeedback clinician sits between the two: ADHD is heterogeneous, its biological markers are real but distributed unevenly across the population carrying the label, and the most effective plans combine biological, psychological, and environmental approaches tailored to the individual profile in front of you.
Key Takeaways
Neurofeedback for ADHD is rated level 5 (efficacious and specific), the highest evidence rating. The Lubar protocol trains clients to inhibit theta and increase beta over approximately 40 sessions. Children with ADHD often show elevated theta/beta ratios, reflecting cortical hypoarousal (an underactivated brain state) and impaired attention. Through operant conditioning, theta/beta training aims to normalize this imbalance. Research consistently shows improvements comparable to stimulant medication, with the crucial advantage that neurofeedback gains persist even when medication is discontinued.
ADHD is better understood as dysregulated attention than absent attention, and emotion dysregulation is a core feature rather than a comorbid complication. Beyond surface power, the disorder involves hypocoherence in the default mode, salience, and dorsal attention networks and dysregulation of Brodmann areas 7, 10, and 11, while refractory cases frequently show focal slowing, spindling excessive beta, or epileptiform discharges that a spectral summary will miss. Meta-analytic evidence shows small but durable gains in inhibitory control and working memory that emerge mainly after roughly 1,260 minutes of cumulative training, so dose should be tracked in training minutes rather than session counts. Resting theta may not change even in children who improve clinically, making behavioral rating scales and task-based measures the defensible outcome metrics. Session design, family involvement, and integration with behavioral and pharmacological care are part of the intervention, not accessories to it.
Check Your Understanding
- What are the three main symptoms that characterize ADHD, and how does neurofeedback address each?
- Describe the Lubar ADHD protocol, including electrode placement, frequency targets, and typical session parameters.
- How did the Monastra, Monastra, and George (2002) study demonstrate the lasting effects of neurofeedback compared to medication alone?
- What efficacy rating did neurofeedback for ADHD receive in Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.)?
- Which three large-scale networks showed hypocoherence in the ICAN cohort, and which Brodmann areas were most dysregulated within them?
- Why did Enriquez-Geppert and colleagues (2024) conclude that resting theta is a poor index of treatment progress, and what should you measure instead?
- What total training dose did Zhong and colleagues (2025) identify as the threshold for executive function gains, and how does that compare with a conventional 40-session course?
- Which four EEG features recur in refractory cases, and how does each alter your treatment planning?
- Why does a continuous performance test serve better as a within-person change measure than as a diagnostic classifier?
- How would you distinguish ADHD from oppositional defiant disorder during intake, and why does the distinction matter for what neurofeedback can achieve?
Mild Closed Head Injuries and Traumatic Brain Injury (TBI)
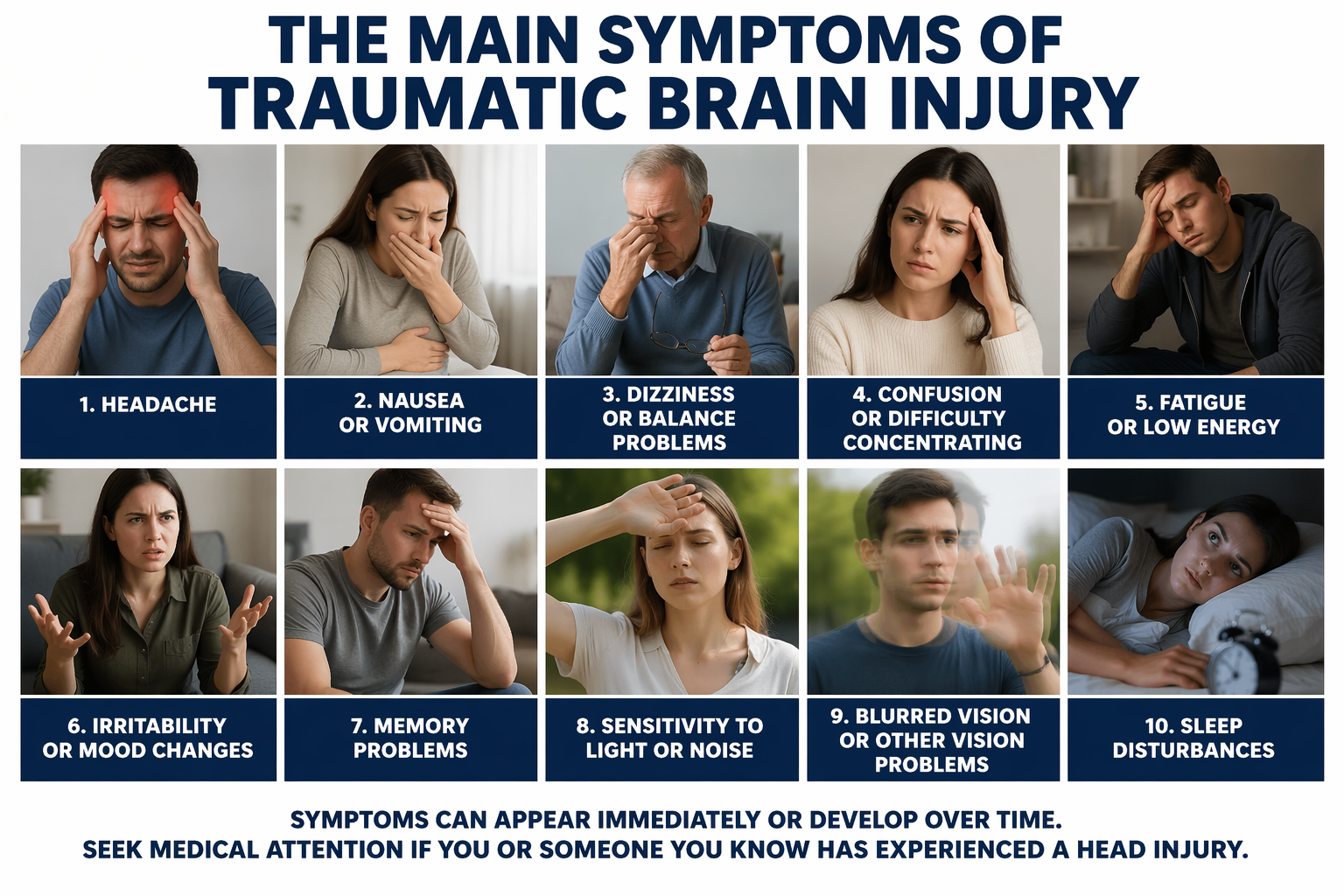
Traumatic brain injury (TBI) results when an external force produces intracranial injury through acceleration (the brain sloshing inside the skull) or direct impact. Unlike a stroke, which damages a specific blood vessel territory, TBI can disrupt brain function through both structural damage and altered neural connectivity across widespread regions. Check out Siddharthan Chandran's TED Talk Can the Damaged Brain Repair Itself?
Defining Mild TBI and Why It Is So Easy to Miss
Injuries divide along two axes that matter clinically. Open injuries involve something penetrating the skull; closed injuries occur when the head and a hard object meet forcefully or when rapid acceleration and deceleration throw the brain against the inside of the skull, as in a motor vehicle collision or a fall. Damage may be diffuse, spread across tissue, or localized to a particular region, and localized damage is very unlikely after a mild injury. Mild traumatic brain injury (mTBI) is conventionally defined as loss of consciousness of up to 30 minutes, altered mental status for up to 24 hours, or post-traumatic amnesia lasting up to 24 hours; when any of these persists longer, or when structural imaging reveals intracranial pathology, the injury is classified as moderate or severe. Concussion is the everyday term for the same event.
The clinical difficulty is that mild injury is largely invisible to the instruments most clients have already encountered. Computed tomography and magnetic resonance imaging are usually normal after mTBI, and diffusion tensor imaging (DTI), which maps white matter tracts by measuring how water diffuses along them, has proved inconclusive in this population (Rosenfeld et al., 2013). Susceptibility-weighted imaging (SWI), an MRI sequence that exploits magnetic differences between tissues to reveal microhemorrhages and small veins, adds some sensitivity beyond DTI (Beauchamp et al., 2013), but most mTBI is still diagnosed by careful clinical assessment of the injured person and any witnesses as close to the time of injury as possible. Neuropsychological testing, questionnaires, and symptom tracking become useful two to three months later if symptoms have not resolved on their own. Measurable cognitive deficits are in fact uncommon several months after a single mild injury and, when present, are often attributable to non-cerebral causes such as pain, sleep disruption, or mood (Belanger et al., 2018).
Repetition may change that picture, though by less than is often claimed. The meta-analytic evidence from these same authors is sobering in the other direction: pooling eight studies of 614 people with multiple mTBIs against 926 with a single mTBI, the overall effect on neuropsychological functioning was minimal and nonsignificant (d = 0.06), with follow-up analyses detecting poorer performance only on delayed memory and executive function (Belanger et al., 2010, 2018). Repeated injury is a reason for closer attention, not a basis for predicting deficit. Cumulative exposure is nonetheless easy to underestimate: helmet-mounted sensors recorded a mean of 652 head impacts per high school football season, ranging from 372 for receivers and secondary players to 868 for linemen (Broglio et al., 2011), while collegiate players sustained a median of 257 to 438 impacts per season with individual players reaching nearly 1,500 (Crisco et al., 2010). Roughly 28,000 military service members sustained a TBI each year at the height of the post-2001 deployments, most classified as mild but frequently repetitive (Peskind et al., 2013); Department of Defense surveillance recorded 18,376 in 2024, of which 81.5% were mild. The practical consequence for intake is that asking whether a client has "had a concussion" is the wrong question. Ask instead how many impacts, over how many years, in what sports, what vehicles, and what deployments, and count events including those never medically evaluated. Two clients with identical presenting complaints and identical normal MRIs may differ enormously in cumulative burden, and that difference should shape both your expectations and how you explain the client's situation to them. Many arrive demoralized by a negative scan they were told meant nothing was wrong; explaining that structural imaging is not sensitive to the changes that follow mild injury is often the first genuinely useful thing a clinician can offer.
Neurophysiological Changes Following TBI
TBI produces characteristic EEG abnormalities, including increased theta activity (slow waves) and decreased beta activity (fast waves), reflecting disrupted neural communication between brain areas (Chen et al., 2023). Axonal injury, damage to the long fibers connecting neurons, interferes with connectivity between brain regions. This leads to deficits in learning, memory, attention, and information processing speed, not because any single area is destroyed, but because the regions can no longer coordinate their activity effectively.
These dysregulated EEG patterns, abnormal brainwave signatures that deviate from healthy functioning, correlate strongly with neurocognitive impairments and provide targets for neurofeedback intervention.
What produces them at the cellular level is mechanical strain rather than gross destruction. Even low-speed impacts and acceleration-deceleration events deform brain tissue, and Geddes-Klein and colleagues (2006) showed that the resulting strain is complex and becomes more pronounced when forces arrive from multiple directions, as when a vehicle strikes more than one object in a single crash or several players converge on one during a tackle. That strain has downstream consequences. Mechanical stretching drives accumulation of amyloid beta, the peptide implicated in Alzheimer's disease, by disrupting axonal transport (Chaves et al., 2021), and even very mild repetitive stretch causes axonal growth cones to collapse and cytoskeletal proteins to mislocalize (Yap et al., 2017). None of this registers on CT, MRI, fMRI, or DTI, which is precisely why so many clients report persistent cognitive difficulty that their imaging cannot corroborate.
Injury Is Local, Reorganization Is Brain-Wide
A focal injury does not produce a focal problem. Frankowski and colleagues (2022) mapped what happens to inhibitory circuitry after experimental TBI in mice using whole-brain imaging combined with rabies virus tracing, a technique that labels the neurons projecting onto a target cell so that its inputs can be counted. Their focus was somatostatin (SST) interneurons, a class of inhibitory neuron that regulates how much input local networks receive and how much output they produce. After injury, SST interneurons in the hippocampus received substantially more local input from nearby neurons while losing long-range input from distant structures such as the entorhinal cortex. The same reorganization appeared in regions the trauma never touched, including the prefrontal cortex. Transplanted interneuron progenitors survived, integrated into the injured tissue, and formed both local and long-distance connections, showing that the injured brain retains the capacity to rebuild long-range circuitry.
Local hyperconnectivity paired with long-range disconnection is a compact description of what qEEG coherence studies find after TBI, and it has three consequences for practice. It explains why abnormalities frequently appear at sites remote from the point of impact, which means whole-head assessment rather than recording over the impact site is the only defensible approach. It supports connectivity-oriented training over purely local amplitude training, because the deficit being corrected is a failure of long-distance integration rather than a local excess or shortage of one rhythm. And it offers a legitimate mechanism for the durability of gains, since the demonstration that new long-range connections can form after injury is exactly the neuroplastic capacity that neurofeedback claims to recruit.
Traumatic brain injury can result from direct impact or acceleration forces, causing cognitive, physical, and psychosocial deficits.
Demographics
TBI is far more common than most people realize. The 2023 National Health Interview Survey found that approximately 3% of Americans, representing nearly 10 million people, reported a TBI in the past year (Waltzman, Black, Daugherty, Peterson, & Zablotsky, 2025). There were approximately 214,110 TBI-related hospitalizations in 2020 and 69,473 TBI-related deaths in 2021 in the United States, averaging more than 586 hospitalizations and about 190 deaths per day (Centers for Disease Control and Prevention [CDC], 2023).
qEEG Assessment After Head Injury
Because structural imaging reports anatomy while the qEEG reports function and communication, quantitative EEG occupies a position after mild injury that no other accessible measure fills. The distinction matters because persisting cognitive symptoms and fatigue appear to reflect reduced efficiency of neural communication rather than tissue loss (Levine et al., 2008). The qEEG measures most consistently associated with TBI are therefore communication metrics rather than amplitude alone: coherence, and phase, the timing relationship between signals recorded at two sites, which indexes how quickly information travels between them (Thatcher et al., 1989). Localized findings do appear with more severe injury, and while moderate to severe closed TBI typically involves frontotemporal regions, localized damage is heterogeneous enough that no standard pattern can be assumed.
Two clinical illustrations show what the qEEG adds and what it demands of the clinician. In the first, a person struck in the face by a closed fist was recorded four days after the assault; LORETA, or low-resolution electromagnetic tomography, a method that estimates three-dimensional cortical sources from scalp recordings, revealed 2 Hz delta activity more than two standard deviations above age-matched norms in right posterior temporal, parietal, and occipital cortex, consistent with a contrecoup injury in which the brain rebounds against the skull opposite the point of impact. A recording two months later at the same frequency and threshold showed complete resolution, with no intervention beyond rest and leave from work (M. Tracy, personal communication). In the second, a client with multiple concussions and additional attentional and behavioral problems showed excess delta, theta, and alpha on topographic statistical maps, much of which had resolved after ten neurofeedback sessions (Koberda, 2015).
Read together, those two cases carry a warning that is easy to overlook. Spontaneous recovery after a single mild injury is common and can be substantial within weeks, so a qEEG recorded days after an injury is a poor pre-treatment baseline: improvement measured against it will confound natural healing with training effects. When the injury is recent and the client is not deteriorating, the defensible options are to document the early recording explicitly as an acute measurement, to establish the treatment baseline after the natural recovery window has passed, or to be candid in your reporting that early gains cannot be attributed to training. When the injury is remote and symptoms have persisted for months, that ambiguity largely disappears and the baseline is interpretable.
Neurofeedback Studies
Ayers (1995) reported treating 32 level-two coma patients, individuals who had been comatose for more than 2 months, noninvasively with neurofeedback, and described 25 of the 32 emerging from coma after only 1 to 6 treatments. The protocol involved inhibiting 4-7 Hz activity (slow waves) while reinforcing 15-18 Hz activity (faster waves). This report is widely repeated and should be handled with corresponding care: it is a two-page abstract from the Association for Applied Psychophysiology and Biofeedback annual meeting rather than a peer-reviewed study, so no methods, diagnostic criteria, outcome definitions, or statistics are available for scrutiny, and no independent replication exists. The closest subsequent attempt trained three patients in unresponsive wakefulness and reported EEG change without emergence, describing itself as the first evidence that neurofeedback can be applied in this population (Keller et al., 2015). Cite Ayers as a clinical anecdote worth following up, not as evidence of efficacy.
Walker, Norman, and Weber (2002) treated 26 patients with persistent symptoms after mild closed head injury and reported that 88% achieved more than 50% improvement in EEG coherence, a measure of how well different brain regions communicate, with a mean improvement of 72.7%. All patients who had been previously employed reported returning to work after completing their training, a particularly meaningful outcome given that TBI often ends careers. The study was an uncontrolled open trial with self-reported vocational outcomes, and the 88% figure describes change in the trained measure rather than in symptoms or function.
Clinical Efficacy
Anne Ward Stevens and Kori Trotter rated neurofeedback for concussion as level 3, probably efficacious in Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.).
Reviewing the same literature for the traumatic brain injury chapter of that volume, Foster, Foster, and Gross reached the same level 3 rating on the basis of four controlled trials, among them Keller's (2001) comparison of beta uptraining in 12 patients against 9 matched controls receiving computerized training, and a 20-participant pilot trial comparing focused attention meditation with meditation plus mobile neurofeedback for persistent symptoms after mild to moderate injury (Polich et al., 2020). Both are small, and Keller's used matched rather than randomized controls, so the rating rests on a thin evidence base. Their central conclusion is one of protocol philosophy rather than effect size: because TBI is so heterogeneous, neurofeedback succeeds to the degree that it addresses the particular symptoms of the particular client, and qEEG together with other functional neuroimaging is what allows presenting complaints to be matched to specific network anomalies (Foster et al., 2023).
Neurofeedback for TBI works through neuroplasticity, the brain's remarkable capacity to reorganize neural pathways and form new connections. Just as physical therapy helps the body compensate for injury by strengthening alternative pathways, neurofeedback helps the brain develop new patterns of activity. Training typically involves inhibiting slow-wave activity (4-7 Hz) and rewarding faster frequencies (15-18 Hz) at sites showing abnormality on qEEG assessment.
Customizing the Protocol: Z-Score and LORETA Training
What TBI degrades is efficiency rather than capacity, and the distinction shapes protocol design. Processing slows and attention fragments across its several forms, which include focused, sustained, selective, alternating, and divided attention. Because higher functions such as language, visuospatial construction, and reasoning are built from these more basic operations, an attentional bottleneck propagates outward into domains that appear unrelated to it. A useful analogy is a highway reduced from many lanes to one or two by construction: nothing is destroyed, but flow becomes halting, accordion-like, and prone to minor collisions. Clients describe this from the inside as mental effort where effort used to be unnecessary, with tasks that were once overlearned and automatic now requiring deliberate work, and with cognitive and emotional strain arriving together.
Three technical developments allow training to be matched to that profile. Z-score training applies operant conditioning against real-time comparisons with a normative database, so the reward criterion follows the client's specific deviations rather than a fixed frequency target. Training several measures concurrently, such as inhibiting 4 to 7 Hz while rewarding 15 to 18 Hz, addresses the multi-dimensional nature of post-injury dysregulation rather than one band at a time. LORETA extends both by moving the training target from the scalp toward the estimated cortical source, permitting greater specificity when the qEEG localizes the problem to a particular region or network (Foster et al., 2023; Koberda, 2015). Together these answer the customization question that the heterogeneity of TBI raises: rather than choosing a protocol for the diagnosis, you choose training targets for the deviations this client actually shows.
One caution belongs alongside this enthusiasm. Neurofeedback is efficacious and specific for ADHD, a condition defined by attentional and executive dysfunction, and the resemblance between post-injury attentional complaints and ADHD is close enough to make borrowing the ADHD protocol tempting. Similar symptoms, however, do not guarantee similar mechanisms, and the mechanism of action in mTBI may well differ from the mechanism in ADHD. Let the client's qEEG rather than the symptom label determine the protocol. For outcome measurement, supplement symptom report with attention measures administered before and after training, such as a continuous performance test, an n-back task, the Auditory Consonant Trigrams test, or the Paced Auditory Serial Addition Test, chosen so that the measure reflects the specific attentional subtype the client reports losing (Foster et al., 2023).
Psychiatric Vigilance After Head Injury
Head injury changes psychiatric risk, not only cognition. Trivedi and colleagues (2024) analyzed the 2017 National Inpatient Sample, isolating more than 26,000 individuals hospitalized with a TBI and matching them by age and sex to an equal number without one. Non-mood psychotic disorders, meaning conditions such as schizophrenia and delusional disorder in which psychosis is not driven primarily by mood change, were diagnosed in nearly 11% of the TBI group compared with fewer than 5% of controls. After adjustment for demographic, medical, and psychiatric variables, TBI remained an independent predictor associated with more than a twofold increase in odds, with the association strongest among younger patients and those carrying comorbid bipolar disorder, substance use, anxiety, intellectual disability, or personality disorders. The design imposes an important limit: because the data are cross-sectional hospital records, they cannot establish whether the psychotic disorder preceded or followed the injury.
The mechanisms the authors propose are familiar from earlier sections of this unit. TBI disrupts frontal–subcortical circuits and limbic-cortical pathways that support executive function, emotion regulation, and reality testing, the same networks implicated in psychotic illness. Microstructural and functional changes in prefrontal cortex, hippocampus, and amygdala produce aberrant connectivity and altered dopaminergic signaling, particularly along the mesolimbic pathway whose dysregulation is a long-standing account of psychosis, with neuroinflammation, white matter damage, and oxidative stress plausibly compounding the effect. This is the logic of the second hit hypothesis, in which a genetic or developmental vulnerability constitutes the first hit and a later environmental insult such as head injury constitutes the second, disrupting maturation during a sensitive period and accelerating a trajectory that might otherwise never have completed. Injury-related attentional and organizational deficits may also strip away the coping capacity that would ordinarily let early symptoms be compensated or concealed.
For a neurofeedback clinician this translates into a specific monitoring responsibility. Clients training for post-concussive symptoms, especially younger clients and those with the psychiatric comorbidities listed above, warrant periodic screening for emerging paranoia, perceptual disturbance, and unusual beliefs, with a referral pathway established before it is needed rather than improvised during a crisis. It also guards against a serious misattribution. When such symptoms surface during a training course, the reflex is to treat them as an adverse response to the protocol and adjust reward thresholds; the evidence here argues that psychiatric evaluation, not protocol titration, is the correct first move. The comorbidity pattern additionally links this section to the one that follows, since substance use both amplifies the risk observed here and frequently accompanies the head injuries that bring clients to a neurofeedback practice in the first place.
Key Takeaways
Neurofeedback for concussion is rated level 3 (probably efficacious). TBI affects nearly 10 million Americans annually, with symptoms including memory deficits, attention problems, and impaired decision-making. Neurofeedback protocols typically involve inhibiting theta (4-7 Hz) and rewarding beta (15-18 Hz) activity. Research shows improvements in attention, memory, cognitive function, and return-to-work rates, working through the brain's neuroplastic capacity to form new connections.
Mild injury is largely invisible to CT, MRI, and DTI, so intake should count cumulative impacts across a lifetime rather than ask about a single concussion; the risk of lasting deficit rises steeply beyond five episodes. Mechanical strain drives amyloid accumulation and axonal disruption too subtle for structural imaging to detect, and inhibitory circuits reorganize brain-wide after a focal injury, gaining local connections while losing long-range input. That pattern justifies whole-head assessment and connectivity-oriented training. Because spontaneous recovery is substantial in the first weeks, a qEEG recorded soon after injury makes a poor treatment baseline. Z-score and LORETA training allow protocols to follow the individual's deviations rather than the diagnosis, and hospitalized TBI more than doubles the odds of a non-mood psychotic disorder, which makes psychiatric screening part of responsible post-injury care.
Check Your Understanding
- What are the primary causes of traumatic brain injury in the United States?
- What neurofeedback protocol did Ayers use to treat level-two coma patients, and what were the outcomes?
- How does Z-score training and LORETA improve the customization of neurofeedback treatment for TBI?
- How is mild TBI defined, and why does a normal MRI fail to rule out clinically meaningful injury?
- Why should an intake interview count cumulative head impacts rather than ask whether the client has had a concussion?
- What did Frankowski and colleagues (2022) find about inhibitory circuits in regions distant from the injury, and how should that shape your assessment montage?
- Why is a qEEG recorded four days after an injury a problematic pre-treatment baseline?
- What psychiatric risk did Trivedi and colleagues (2024) identify after TBI, and what should you do if those symptoms emerge mid-protocol?
Substance Use Disorder
Imagine trying to help someone who has lost jobs, relationships, and housing to addiction, who may feel that external forces control their life, and who has failed at recovery multiple times. Substance use disorder (SUD) presents some of the most challenging cases in clinical practice. Biofeedback can serve as a self-regulation strategy to help manage alcohol cravings and negative thinking patterns.
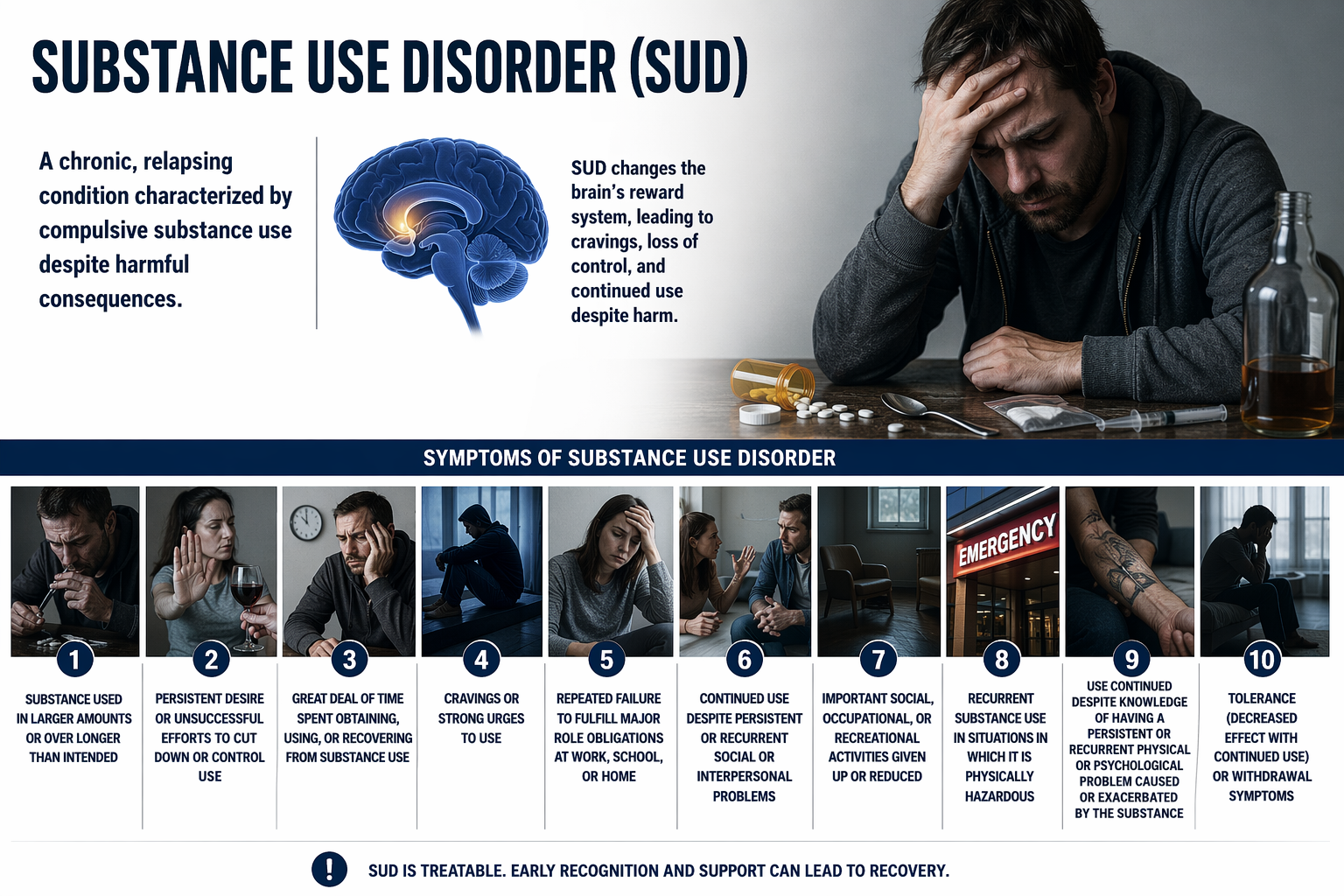
Personality Traits Without an Addictive Personality
The DSM-5-TR characterizes substance use disorders by loss of control over use, continued use despite serious negative consequences, and preoccupation with obtaining the substance, using it, and recovering from its effects (American Psychiatric Association, 2022). Jaffe (1980) anticipated that framing decades earlier, defining addiction as a behavioral pattern marked by compulsive use, securing supply, a high tendency to relapse after withdrawal, and the triad of craving, withdrawal, and tolerance. Clients and families often arrive with a different framework entirely, one built around the idea of an addictive personality, a supposed personality type that destines certain people for addiction. That concept does not survive examination, and understanding why changes how you conduct treatment.
The problem is that no set of traits applies universally. Impulsivity, sensation-seeking, and neuroticism are all repeatedly associated with addiction, yet many people who score high on them never develop a substance use disorder and many people with substance use disorders do not show them. A range of personality disorders appears among people with substance dependence, but none predicts outcome strongly (Berglund et al., 2011; Franques et al., 2000). Addiction reflects an interplay of genetic predisposition, environment, and individual history, so a highly impulsive person embedded in strong social support with little exposure may never develop a problem, while a person low in impulsivity may develop one under severe environmental stress (Koob & Volkow, 2010). The findings are not merely complex but sometimes contradictory: impulsivity is strongly tied to substance use disorders yet its relationship to behavioral addictions such as gambling is far less clear, and trait effects are moderated by age, gender, and culture, with sensation-seeking mattering most in adolescence and neuroticism mattering most in adults using substances to manage chronic distress (Kotov et al., 2010; Verdejo-García & Pérez-García, 2007; Zilberman et al., 2018).
Individual traits nevertheless carry real information, and it is information about your protocol rather than about your client's identity. Impulsivity, the tendency to act on urges with little forethought, predicts earlier experimentation, faster progression, and greater difficulty maintaining abstinence, largely through an impaired capacity to delay gratification that also undermines adherence to treatment plans and resistance to cravings and triggers (de Wit, 2009; Evenden, 1999). A highly impulsive client is therefore predictably at risk of dropping out of a 30-session alpha-theta course long before its benefits appear, which is an argument for front-loading contingency management, keeping early sessions short, and making progress visible from the first appointment. This is also the clearest rationale for the sequencing built into the Scott–Kaiser protocol described below, which begins with attention training before alpha-theta work: the attentional and impulse-control deficits that make alpha-theta training hard to complete are treated first rather than assumed away.
Neuroticism, meaning emotional instability and a propensity toward anxiety, guilt, and depressed mood, predicts substance use as self-medication and predicts the transition from use to dependence in longitudinal research (Kotov et al., 2010; Terracciano & Costa, 2004). For these clients the emotion-regulation and autonomic components of a plan, including HRV biofeedback and the reappraisal skills discussed in the depression section, are not adjuncts but a direct treatment of the maintaining mechanism. Conscientiousness, the tendency toward self-discipline, organization, and forethought, is protective and is associated with lower rates of binge drinking, drug use, and smoking even among people carrying other risk factors (Bogg & Roberts, 2004; Roberts et al., 2005). Low conscientiousness predicts missed appointments and abandoned home practice, which argues for external structure, reminders, and scheduled sessions rather than for exhortation. Sensation-seeking, a desire for novel and intense experience, raises the risk of initiation but appears largely irrelevant to continued use once dependence has developed, so it belongs in a prevention conversation more than in a relapse-prevention plan (Franques et al., 2000; Zuckerman, 2007).
Rejecting the addictive personality construct also changes what you say to clients. A label describing an entire personality as defective invites a self-fulfilling prophecy in which both clinician and client treat relapse as inevitable, and it adds shame to a population already carrying a great deal of it. Traits, by contrast, name modifiable targets: impulsivity can be trained, emotional regulation can be taught, and structure can substitute for conscientiousness that has not yet developed. Framing your formulation in those terms is more accurate, more hopeful, and more useful for planning than any personality profile would be.
Neurophysiological Basis
Individuals with substance use disorders display altered EEG patterns, particularly within the alpha, theta, and beta bands. The characteristic pattern is low alpha (the relaxed, wakeful rhythm) combined with high beta (fast activity associated with anxiety and rumination). This pattern has been interpreted as central nervous system hyperarousal, a chronically overactivated brain state associated with anxiety, higher relapse risk, and poor treatment outcomes (Sokhadze, Cannon, & Trudeau, 2008). The profile is best documented in alcohol dependence; the same review reports the opposite pattern, excess frontal alpha, in cocaine-dependent patients, so treat low alpha with high beta as one presentation among several rather than the signature of substance use disorder generally. Think of it as a brain that cannot calm down, constantly on edge and seeking relief, which substances temporarily provide.
Alpha-theta neurofeedback induces a hypnagogic state, the twilight zone between waking and sleeping where consciousness becomes fluid and dreamlike. This state may facilitate access to unconscious material and support psychological transformation. Recent research confirms that alpha-theta protocols reduce craving, anxiety, and relapse rates among individuals with alcohol and substance dependence (Sanader Vukadinovic, 2025).
Brain Differences That Precede Substance Use
A standing assumption in this field holds that the brain differences observed in people with substance use disorders, principally thinner cortex and smaller volumes in regions supporting decision-making and impulse control, are consequences of neurotoxicity, the damage substances inflict on nervous tissue. Miller and colleagues (2024) tested that assumption by reversing the temporal order. Drawing on the Adolescent Brain Cognitive Development (ABCD) Study, a National Institutes of Health project following nearly 12,000 American children from ages nine and ten into young adulthood, they scanned 9,804 children aged nine to eleven and then tracked substance use initiation through interviews every six months for three years. They measured 297 imaging-derived phenotypes, quantitative descriptors extracted from imaging such as the volume of a structure or the thickness of a cortical region, covering 68 cortical areas and 18 subcortical structures, and analyzed them with mixed-effects models that accounted for the many siblings and twins in the sample, applying stringent corrections for the number of tests performed.
By age fifteen, 3,460 children had initiated use, most commonly with alcohol. The anatomical differences that preceded initiation were not the ones the neurotoxicity account predicts. Children who later used substances had larger brains overall, with greater whole brain volume, greater cortical surface area, and larger subcortical structures, the opposite of the pattern seen in adults with established substance use disorders. Cortical thickness diverged by region: thinner cortex in frontal areas, most notably the rostral middle frontal gyrus, alongside thicker cortex in temporal, parietal, and occipital regions. Cannabis initiation was specifically associated with a smaller right caudate nucleus, a structure central to habit formation and reward. Decisively for interpretation, when the analysis was restricted to children who were entirely substance-naive at the time of their baseline scan, 14 of 21 associations remained significant, meaning the anatomy predicted behavior that had not yet occurred (Miller et al., 2024). The frontal thinning was specific to the right rostral middle frontal gyrus.
The limits deserve equal weight. The study examined initiation rather than progression to problematic use, so it cannot say whether these features predict addiction as opposed to experimentation; statistical power was inadequate for nicotine and cannabis given how few children initiated them; and the design cannot date when the anatomical differences emerged or rule out unmeasured genetic and environmental influences. What it does establish is that the neuroimaging literature on substance use disorders has probably been conflating pre-existing vulnerability with drug-induced damage (Miller et al., 2024).
Inferring Frontal Vulnerability from the qEEG
Frontal cortical thinning, particularly in the dorsolateral prefrontal cortex (dlPFC) and orbitofrontal cortex, is associated with the executive, impulse control, and decision-making deficits central to substance use disorder, and longitudinal and twin evidence indicates that this thinning can precede use rather than follow it (Cheetham et al., 2014; Ersche et al., 2012). Scalp EEG cannot measure cortical thickness, and no responsible clinician should tell a client that a qEEG shows thin cortex. What the qEEG can do is characterize the regulatory failure that such thinning would produce, and Ronald Swatzyna has identified several frequency-domain signatures worth examining in this population. Increased frontal theta from 4 to 7 Hz appears frequently in children and adolescents with attentional and executive dysfunction and may reflect maturational delay or hypofunction of frontal regulatory systems, with elevated frontal midline theta tracking poor impulse control (Clarke et al., 2001). Reduced frontal alpha from 8 to 12 Hz suggests hypofunctional prefrontal networks and diminished inhibitory control. Excess frontal beta and high beta or gamma activity have been linked to cortical hyperexcitability and disinhibition in at-risk youth and to the impulsivity, emotional dysregulation, and sensation-seeking that raise risk (Barry et al., 2003; Rangaswamy et al., 2002). Frontal hypocoherence within frontal-frontal and frontal-parietal networks indicates impaired integration across the executive control system (Thatcher et al., 2005).
Swatzyna's clinical speculation about that last group is worth taking seriously: some children, adolescents, and adults may use substances specifically to quiet excessive fast-wave activity. If so, the low-alpha, high-beta hyperarousal pattern described earlier in this section is not simply a consequence of chronic use but may in some clients be the very state the substance was recruited to manage, which reframes what the training has to accomplish. Practically, these signatures argue against applying a single protocol to everyone who carries the diagnosis. A client whose qEEG shows excess frontal fast activity and hyperarousal is a candidate for protocols that quiet that activity, and the alpha-theta work that dominates this field is well matched to them. A client whose record instead shows elevated frontal theta, reduced frontal alpha, and frontal hypocoherence presents a picture closer to the executive dysfunction described in the ADHD section, which supports beginning with attention and connectivity training exactly as the Scott–Kaiser sequencing prescribes.
The developmental evidence also gives you something useful to say. Because vulnerability is measurable years before the first drink, the abnormalities you observe in a client's qEEG cannot all be attributed to what they have done to themselves, and telling them so is both accurate and clinically productive. Vulnerability is not destiny, in the same way that a family history of a disease is not a diagnosis, and the appropriate response to identified risk is more protection rather than resignation (Miller et al., 2024).

Substance use disorders present unique challenges for treatment, often complicated by comorbid psychiatric conditions and adverse life circumstances.
The Menninger and Peniston Protocols
The Menninger ON-OFF-ON EEG protocol teaches patients to increase the amplitude (power) within a frequency band, reduce it, and then increase it again during 100- or 200-second segments. This approach may produce superior control compared to procedures that only train amplitude increases, because it demonstrates that the patient can move brain activity in both directions rather than just hoping it happens to change in the desired direction.
Importantly, temperature biofeedback and frontal SEMG (surface electromyography) biofeedback precede alpha-theta training. These preliminary sessions serve a crucial purpose: they teach patients the strategy of passive volition, sometimes called "allowing" rather than "trying." Active effort and straining actually interfere with alpha-theta training; patients must learn to let changes happen rather than force them. This counterintuitive skill must be established before the deeper alpha-theta work can succeed.
The Peniston addiction protocol is a comprehensive multimodal approach that incorporates both biofeedback and non-biofeedback components. Patients begin with systematic desensitization and visualization training, complete a temperature biofeedback phase of at least five sessions, and learn rhythmic breathing, autogenic exercises, and guided imagery. This preparation readies them for the alpha-theta training itself. Distinguish the original trial from the protocol it generated: Peniston and Kulkosky (1989) used 15 thirty-minute alpha-theta sessions with 10 alcoholic patients per group, while the generalized protocol that later circulated under Peniston's name specifies 30 sessions.
The Scott–Kaiser protocol, also written Kaiser–Scott, starts with neurofeedback ADHD training (theta/beta training) and then progresses to the Peniston protocol. The rationale is that many substance abusers have underlying ADHD or attention problems that interfere with their ability to benefit from alpha-theta training.
Scott, Kaiser, Othmer, and Sideroff (2005) randomly assigned patients with mixed substance abuse to EEG biofeedback or a control group. Of those reassessed at 12 months, 36 of 47 experimental completers (77%) were abstinent compared with 12 of 27 controls (44%). Read that alongside its denominator: 74 of the original 121 participants contributed 12-month data, so this is a per-protocol rather than an intention-to-treat result, and because the training also improved retention, differential attrition is entangled with the abstinence outcome.
This video takes the viewer through an alpha-theta training demonstration using the Nexus/Biotrace system.
Clinical Efficacy
Estate M. Sokhadze and David Trudeau rated NFB for SUD as probably efficacious based on an RCT (N = 121) using the Scott–Kaiser NFB protocol.
The five other RCTs incorporated alpha and high beta regulation, alpha/theta with TEMP and guided imagery, SMR and beta upregulation with 1–13 Hz and high beta (18–22 Hz) suppression, SMR/theta followed by alpha-theta, and the Scott–Kaiser NFB protocol.
The Scott–Kaiser protocol, which starts with NF ADHD training and then progresses to the Peniston protocol, has improved retention and abstinence in these hard-to-treat populations. Participants increased abstinence, quality of life, self-efficacy, time in the program, and TOVA (continuous attention), and reduced addiction severity and craving.
The Scott–Kaiser modification of the Peniston Protocol can be classified as probably efficacious with residential or office-based rehabilitation and opioid replacement for alcohol, opioid, mixed-substance, and stimulant abusers.
Alpha-theta NF received a level-2 rating of possibly efficacious.
Key Takeaways
The Scott-Kaiser modification of the Peniston Protocol is rated probably efficacious for substance use disorders. This comprehensive multimodal approach combines ADHD neurofeedback training with the Peniston protocol, which includes visualization, temperature biofeedback, autogenic training, and 30 alpha-theta sessions that induce a hypnagogic state facilitating psychological processing. The protocol improves treatment retention, abstinence rates, and quality of life while reducing craving.
There is no addictive personality, but individual traits predict which parts of a protocol will be difficult. Impulsivity threatens completion of a long alpha-theta course and argues for contingency management and visible progress tracking, neuroticism identifies self-medication and makes emotion regulation and HRV biofeedback central rather than supplementary, low conscientiousness calls for external structure, and sensation-seeking matters for prevention more than for relapse prevention. Anatomical vulnerability is measurable in substance-naive nine-year-olds, with thinner frontal cortex and larger overall brain volume predicting initiation years later, which means the differences seen in clients are not all self-inflicted damage. Although the qEEG cannot measure cortical thickness, elevated frontal theta, reduced frontal alpha, excess frontal fast activity, and frontal hypocoherence functionally index the same regulatory weakness and should determine whether a client begins with attention and connectivity training or moves directly toward alpha-theta work.
Check Your Understanding
- What is the purpose of temperature and SEMG biofeedback in the Menninger/Peniston protocols?
- Describe the concept of "passive volition" and explain why it is critical to alpha-theta training success.
- How does the Scott-Kaiser protocol modify the original Peniston protocol?
- What outcomes did the Scott, Kaiser, Othmer, and Sideroff (2005) study report for 12-month abstinence rates?
- Why does the evidence fail to support the concept of an addictive personality, and how do individual traits still inform treatment planning?
- How would high impulsivity and low conscientiousness each change the way you structure a course of alpha-theta training?
- What did Miller and colleagues (2024) find about brain structure in substance-naive nine-year-olds, and why does the finding challenge the neurotoxicity account?
- Which qEEG signatures functionally index the frontal regulatory weakness associated with substance use risk, and how might each steer your protocol selection?
Epilepsy
Epilepsy is a neurological condition marked by recurrent, unprovoked seizures resulting from abnormal electrical activity in the brain. The International League Against Epilepsy classifies seizures first by where they begin, as focal, generalized, or unknown onset (Fisher et al., 2017), and focal seizures are the single most common type. Two generalized-onset types recur throughout the neurofeedback literature. Absence seizures, historically called petit mal, feature brief loss of consciousness without abnormal movement; the patient appears to be daydreaming. Tonic-clonic seizures, historically called grand mal, are generalized seizures with convulsions, featuring a cry, loss of consciousness, falling, and rhythmic jerking of all extremities. The older petit mal and grand mal labels persist in clinical conversation and in diagnostic coding but are not part of the current classification.
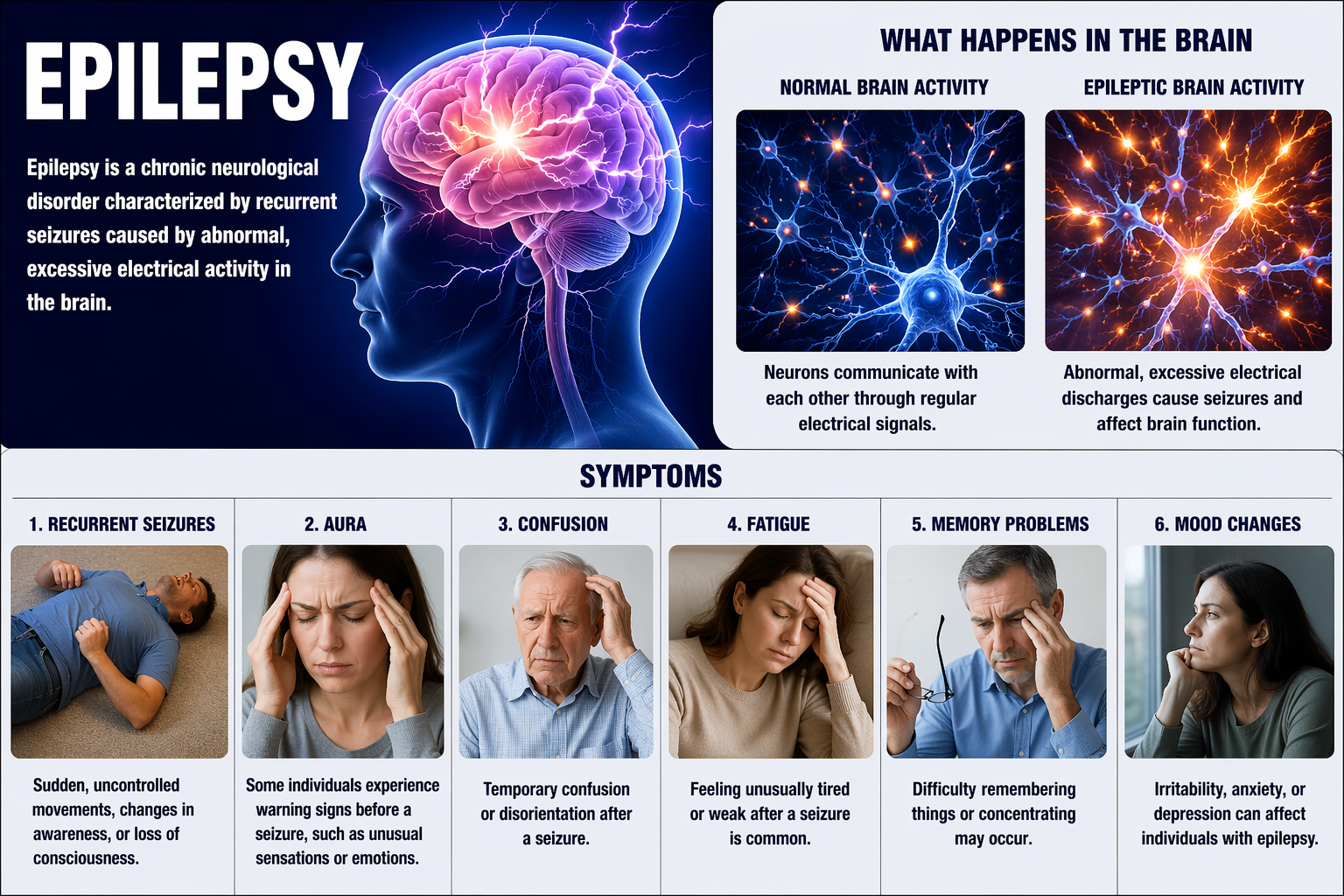
Demographics
Active epilepsy affects approximately 1.1% of U.S. adults, about 2.9 million people, and roughly 456,000 children, for a national total near 3.4 million (Centers for Disease Control and Prevention, 2024; Kobau, Luncheon, & Greenlund, 2023). The World Health Organization (2024) reports that around 50 million people worldwide have epilepsy, making it one of the most common neurological diseases globally. About 1.5 million community-dwelling U.S. adults with active epilepsy reported uncontrolled seizures in the past 12 months (Kobau, Luncheon, & Greenlund, 2024), highlighting the need for additional therapeutic approaches.
Neurophysiological Basis
The sensorimotor rhythm (SMR) is an EEG rhythm conventionally defined as 12-15 Hz, with a spectral peak around 12-14 Hz, located over the sensorimotor cortex. SMR is associated with inhibition of movement and reduced muscle tone. When Barry Sterman was researching sleep in cats in the 1960s, he discovered that cats trained to increase SMR were remarkably resistant to seizure-inducing compounds. This serendipitous finding led to the development of SMR up-training for epilepsy in humans.
Sterman's protocol trains epileptic patients to increase SMR (12-14 Hz) amplitude and duration while suppressing theta (slow-wave activity), high beta (fast activity associated with tension), epileptiform spikes, and EMG artifact during 36 sessions. The training essentially strengthens the brain's natural inhibitory mechanisms.

Dr. Maurice Barry Sterman, pioneer of SMR neurofeedback for epilepsy.
Sterman (2000) summarized the accumulated SMR literature and found that 82% of 174 patients whose seizures were otherwise uncontrolled achieved clinically significant improvement, defined as at least a 50% reduction in seizure incidence, with about 5% reporting no seizures for up to a year after training ended (Sterman & Egner, 2006). Reviewing the same body of work later, Sterman (2010) put the totals at 24 studies and 243 patients with the same 82% figure, so treat the study and patient counts as approximate. An independent meta-analysis of 10 studies selected from 63 by Tan and colleagues (2009) reached a convergent conclusion: 79% of patients trained with SMR feedback showed a statistically significant reduction in seizure frequency despite a collective history of failed medication.
Clinical Efficacy
Lauren Frey rated SMR-based and SCP-based neurofeedback as level 4, efficacious for seizures. SMR neurofeedback improves seizure control by enhancing functional connectivity across the brain (Frey, 2023).
Clinical Application
For the 1.5 million Americans whose seizures are not controlled by medication, neurofeedback offers a genuine alternative. The training teaches the brain to produce its own internal stabilization, potentially reducing both seizure frequency and the side effects that often accompany anti-seizure medications.
Key Takeaways
SMR-based and SCP-based neurofeedback are rated efficacious for seizures. SMR (12-14 Hz) reflects thalamocortical inhibitory circuits, essentially the brain's braking system. When patients learn to increase SMR through operant conditioning, they raise excitation thresholds and reduce seizure susceptibility. In Sterman's summary, 82% of patients achieved at least a 50% reduction in seizures, and an independent meta-analysis by Tan and colleagues (2009) found significant seizure reduction in 79%.
Check Your Understanding
- What distinguishes absence seizures (petit mal) from tonic-clonic seizures, and where do both sit in the current ILAE classification?
- Describe Sterman's SMR protocol for epilepsy, including what is trained and what is inhibited.
- What percentage of patients showed clinical improvement in Sterman's summary of 18 peer-reviewed SMR studies?
Anxiety and Anxiety Disorders
Generalized anxiety disorder (GAD) is defined by excessive anxiety and worry occurring more days than not for at least 6 months. Unlike normal worry that comes and goes with life circumstances, GAD involves persistent, hard-to-control worry about multiple areas of life.
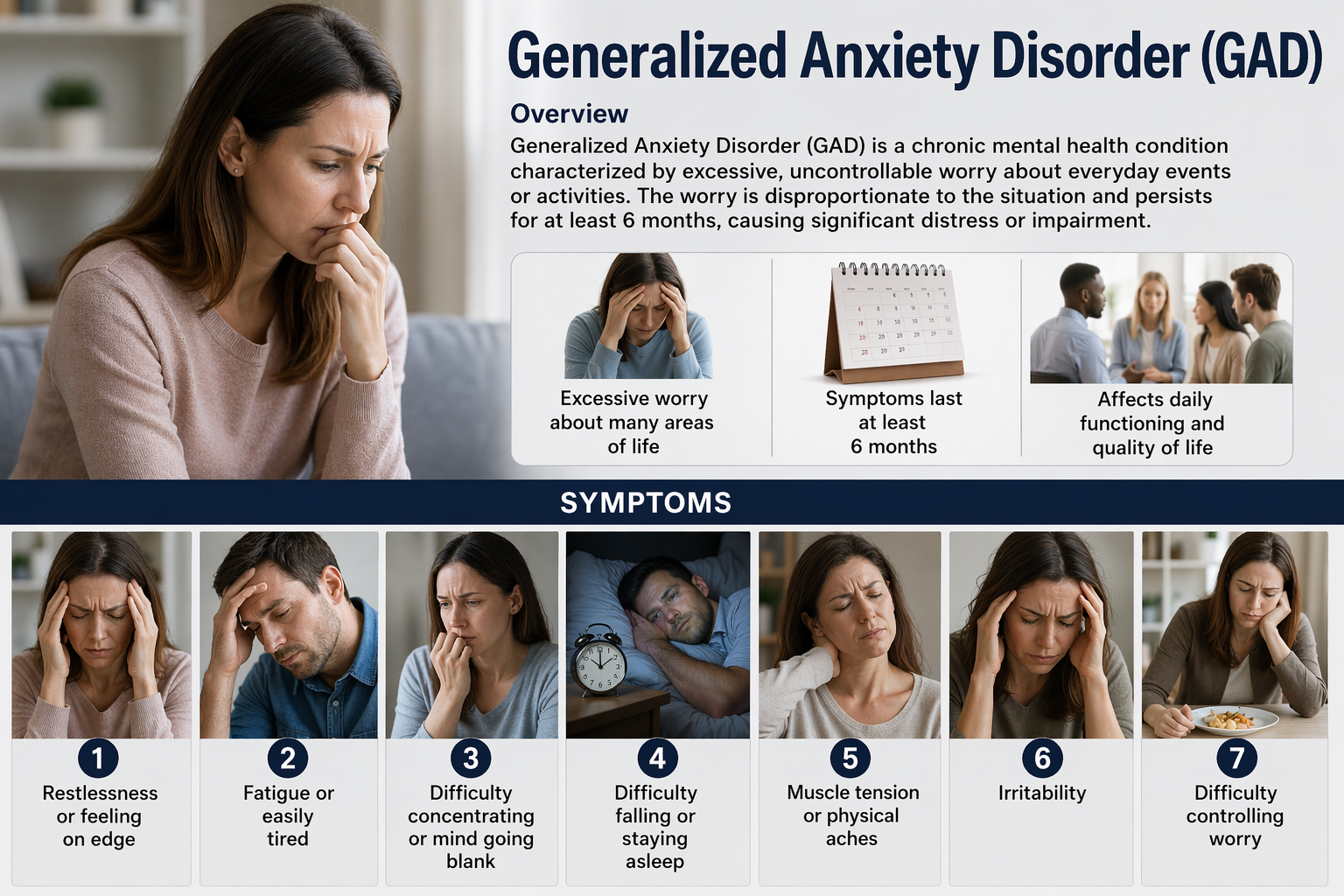
DSM-5 classifies Post-traumatic stress disorder (PTSD) as one of the Trauma and Stress-Related Disorders. PTSD develops in some people following exposure to a traumatic event like assault, military combat, rape, or witnessing death or serious injury.
Neurophysiological Basis
Anxiety disorders are associated with autonomic nervous system dysregulation, characterized by reduced heart rate variability (HRV) and parasympathetic withdrawal. In plain terms, the nervous system is stuck in "fight-or-flight" mode, with the calming branch (parasympathetic) unable to adequately counterbalance the arousal branch (sympathetic).
Heart rate variability biofeedback (HRVB) targets this dysregulation by training patients to breathe at their resonance frequency, typically around 6 breaths per minute, which maximizes the amplitude of respiratory sinus arrhythmia and strengthens baroreflex function (Lehrer & Gevirtz, 2014). Goessl, Curtiss, and Hofmann (2017) pooled 24 studies and found a large pre-post effect on self-reported stress and anxiety (Hedges' g = 0.81, with g = 0.83 against control conditions). A broader review of 58 randomized trials across many outcomes reported a small-to-moderate overall benefit favoring HRVB, largest for anxiety, depression, anger, and performance (Lehrer et al., 2020), so expect the large figures where anxiety is the target and more modest ones elsewhere.
Demographics
Anxiety disorders are the most common mental disorders in the United States. According to the National Institute of Mental Health, approximately 19.1% of U.S. adults, nearly one in five, experience an anxiety disorder in any given year (NIMH, 2023). Post-traumatic stress disorder affects approximately 6% of Americans at some point in their lives (Goldstein, Smith, & Chou, 2016).
Clinical Efficacy
Based on five RCTs, Donald Moss and Matthew Watkins rated BFB and NFB for GAD as level 4, efficacious. The BFB interventions included HR decrease, HRV increase, SCL decrease, SEMG decrease, and virtual reality (VRB). The NF interventions included alpha increase and alpha/theta increase.
Participants decreased HR, SCL, state and trait anxiety, and HR reactivity to stress. They increased HRV measures (HF and LF power) and theta power.
Key Takeaways
Biofeedback for anxiety is rated level 4 (efficacious). HRV biofeedback trains patients to breathe at their resonance frequency (typically around 6 breaths per minute), maximizing respiratory sinus arrhythmia and strengthening vagal tone. Multiple modalities show benefit: HRV biofeedback addresses autonomic dysregulation, temperature biofeedback promotes peripheral relaxation, SEMG biofeedback releases muscle tension, and alpha-theta neurofeedback reduces central nervous system hyperarousal.
Depression
Major Depressive Disorder (MDD) is more than just feeling sad. It is defined by persistent sadness, loss of interest or pleasure in activities that used to be enjoyable, and feelings of guilt or low self-worth, along with disturbed appetite and sleep, difficulty concentrating, and in severe cases, suicidal ideation.
Neurophysiological Basis
Richard Davidson proposed the theory of frontal alpha asymmetry (FAA) as a neurophysiological marker for depression (Davidson, 1992). The behavioral activation system (BAS), mediated primarily by the left frontal cortex, drives approach behavior and positive emotions. The behavioral inhibition system (BIS), mediated by the right frontal cortex, drives withdrawal motivation and negative affect.
Depression is associated with reduced left frontal activity relative to right frontal activity, reflecting diminished approach motivation and positive affect. The depressed brain shows the signature of withdrawal. Here is a crucial point that initially seems counterintuitive: because alpha power is inversely related to cortical activity (more alpha means less activity), the depressive signature is elevated left frontal alpha. The asymmetry is conventionally scored as the natural log of right alpha minus the natural log of left alpha, so depressed individuals score negative, and the score can be moved in the healthy direction either by reducing left alpha, which raises left activity, or by raising right alpha, which lowers right activity. Alpha asymmetry protocols have used both routes (Baehr et al., 1997).
Beyond Frontal Asymmetry: The Enlarged Salience Network
Frontal alpha asymmetry describes a functional imbalance. A recent line of work suggests that depression also involves a difference in how much cortex is allocated to a particular network in the first place. Depression is episodic, with periods of illness alternating with periods of wellness, and that fluctuation has historically frustrated efforts to identify stable brain differences, because any snapshot might capture a person mid-episode or mid-recovery. Lynch and colleagues (2024), publishing in Nature, solved that problem with precision functional mapping (PFM), an approach that collects a very large volume of functional magnetic resonance imaging data from the same individual across time so that brain organization can be estimated for that person rather than averaged across a group. More than 140 people with major depressive disorder and 37 healthy controls were scanned repeatedly over 1.5 years, some as many as 62 times.
The frontostriatal salience network, which links frontal cortex with the striatum and determines which stimuli are flagged as important enough to capture attention and which rewards are worth pursuing, was nearly twice as large in participants with depression. That expansion was stable over time, unrelated to symptom severity, and did not track mood state; the network occupied about 73% more cortical surface than in controls, which the authors describe as a nearly twofold expansion. Connectivity within the network behaved very differently. Coupling between the nucleus accumbens and anterior cingulate tracked fluctuations in anhedonia, and in one densely sampled participant it forecast anhedonia severity roughly a week ahead, a single-case finding that did not replicate in the second such participant. Extending the analysis to less frequently scanned cohorts, the team found the same enlarged network in children scanned at ages 10 and 12 who had no depression history but developed clinically significant symptoms at 13 or 14 (Lynch et al., 2024; Schimmelpfennig et al., 2023).
The clinically useful idea here is the separation of a trait marker, a stable characteristic that indicates vulnerability, from a state marker, a measure that rises and falls with the current episode. Network size behaved as a trait marker and network activity as a state marker, and confusing the two is a common source of frustration in neurofeedback practice. Frontal alpha asymmetry has substantial trait-like variance of its own, which is one reason an asymmetry score can look stubbornly unchanged while a client's mood clearly improves, or can shift without any corresponding clinical benefit. The practical response is to decide in advance which role each of your measures is playing: use symptom scales, behavioral activation logs, and state-sensitive physiological measures such as heart rate variability for weekly tracking, and reserve the qEEG or asymmetry index for pre-treatment formulation and periodic re-evaluation rather than session-to-session decision-making. The finding that reduced salience network activity forecast an episode a week ahead also points toward a use of monitoring that neurofeedback clinicians rarely exploit, which is early detection of deterioration and a scheduled booster contact before relapse becomes established.
Frontoamygdalar Connectivity and Treatment Response
Depression treatment fails often enough that predicting response has become a research priority in its own right. Only about 70% of depressed youth respond to a first-line treatment, and between 40% and 60% fail to achieve remission afterward (Kung et al., 2023). Kung and colleagues (2023) asked whether the pathway that supports emotion regulation could distinguish who is depressed and who will improve. They scanned 107 youths with moderate to severe depression and 94 healthy controls during a cognitive reappraisal task, in which participants deliberately reinterpret an emotionally distressing image in order to reduce its impact, and analyzed the data with dynamic causal modeling (DCM), a method that estimates effective connectivity, meaning the directional influence one region exerts over another, rather than the simple correlation captured by functional connectivity.
Controls used reappraisal more effectively than depressed participants. Stronger inhibitory connections running from ventrolateral prefrontal cortex to the amygdala, the structure that assigns emotional salience and drives the reactivity depressed clients struggle to dampen, were associated with a lower likelihood of carrying a depression diagnosis; depressed youths showed weaker inhibitory modulation of that pathway during reappraisal. Weaker excitatory ventromedial prefrontal-to-amygdala connectivity at baseline was associated with posttreatment remission, although that effect did not predict remission for individual participants (Kung et al., 2023). The direction of influence is the point: what separates depressed from non-depressed youth, and responders from non-responders, is how effectively the frontal cortex exerts downward control over limbic reactivity.
Three implications follow for practice. The first is that the mechanism is the same top-down regulation deficit described in the ADHD section of this unit, which argues for treating emotion regulation as a training target in its own right rather than as a symptom expected to resolve once mood lifts. The second concerns how you probe it: connectivity differences appeared during an active reappraisal task, not at rest, echoing the ICAN finding that clinically meaningful change surfaced during cognitive challenge rather than in the resting spectrum. Building a brief emotion-regulation challenge into your assessment battery, in which the client views mildly distressing material and is asked to reinterpret it while you record, gives you a functional probe that a resting baseline cannot supply. The third is that coaching matters. Because reappraisal is the behavioral expression of the frontal-to-amygdala pathway, explicitly teaching reappraisal as the client's in-session and between-session strategy trains the same circuit the imaging identifies, which is also the strongest argument for pairing neurofeedback with cognitive-behavioral work rather than delivering it in isolation.
Demographics
According to the most recent National Health and Nutrition Examination Survey (2021-2023), depression prevalence in the past two weeks was 13.1% among adolescents and adults aged 12 and older (Brody & Hughes, 2025). Depression prevalence is highest among adolescents aged 12-19, with 26.5% of adolescent females reporting symptoms. Roughly 21% of U.S. adults will experience major depressive disorder at some point in their lifetime, with a 12-month prevalence near 10% (Hasin et al., 2018).
Clinical Efficacy
Based on 10 RCTs, Zachary Meehan, Fred Shaffer, and Christopher Zerr rated biofeedback and neurofeedback for MDD as efficacious and specific in Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.).
Both alpha asymmetry neurofeedback and HRV biofeedback have demonstrated efficacy for depression. Meta-analysis found an effect size of g = 0.38 for HRV biofeedback in reducing depressive symptoms, which the authors describe as medium and as comparable to broadly applied approaches such as cognitive-behavioral therapy (Pizzoli et al., 2021). Under Cohen's conventions 0.38 sits between small and medium, and the analysis reported a prediction interval spanning zero, so a future trial could find no effect.
Positioning Neurofeedback Within a Combined Treatment Plan
Knowing that a modality works says little about where it belongs in a treatment sequence, and depression is the condition where that question is best answered. Cuijpers and colleagues (2021) conducted a network meta-analysis, a technique that compares multiple treatments simultaneously by combining direct and indirect evidence, drawing on 58 studies and 9,301 patients treated in primary care settings where most depression is actually managed. Psychotherapy and pharmacotherapy, the use of medication to treat a mental health condition, each outperformed usual care and waitlist control, confirming that active intervention beats watchful waiting. Compared directly against one another, however, they did not differ significantly, which means psychotherapy alone is a defensible first choice for many patients. Combination therapy pairing psychotherapy with medication might be better than either alone, which is the hedged conclusion the authors themselves draw rather than a demonstrated superiority. Cognitive behavioral therapy performed well both as a standalone treatment and as a component of combined care. Follow-up data in this review were too sparse to support conclusions about long-term relapse, the return of depressive symptoms after a period of improvement; the evidence that psychological treatment lowers relapse risk during antidepressant discontinuation comes from the separate relapse-prevention literature rather than from this analysis (Cuijpers et al., 2021).
Read alongside the efficacy ratings above, this evidence positions neurofeedback and HRV biofeedback much as it positions psychotherapy: as active treatments that hold their own against medication in milder presentations and that contribute most when combined rather than substituted. For a client with mild depression who prefers a non-pharmacological approach, alpha asymmetry training combined with HRV biofeedback, behavioral activation, and lifestyle change is a reasonable primary plan. For moderate to severe depression, positioning training as a replacement for combined care is not supportable, and doing so risks the outcome the meta-analysis argues hardest against. The most defensible clinical niche may be the discontinuation window. When a client tapers an antidepressant, relapse risk rises and structured psychological support demonstrably lowers it; a continuing schedule of training sessions, a maintained home HRV biofeedback practice, and rehearsed cognitive-behavioral skills all belong in that period, coordinated explicitly with the prescriber rather than arranged around them. Direct communication between the prescriber and the biofeedback clinician prevents conflicting recommendations, allows proactive adjustment when side effects or perceived non-improvement threaten adherence, and preserves the client's trust in a plan that involves more than one provider (Cuijpers et al., 2021).
Key Takeaways
Biofeedback and neurofeedback for major depressive disorder are rated efficacious and specific. Alpha asymmetry neurofeedback targets the imbalance between left frontal activity (approach/positive affect) and right frontal activity (withdrawal/negative affect). Training increases right frontal alpha (reduces right activity) to normalize the asymmetry. HRV biofeedback complements neurofeedback by addressing autonomic dysregulation.
Precision functional mapping shows that the frontostriatal salience network is roughly twice its typical size in depression, a stable trait feature detectable years before the first episode, while activity within that network falls during episodes and forecasts relapse a week in advance. Distinguishing trait markers used for formulation from state markers used for weekly tracking prevents both false discouragement and false confidence. Effective connectivity from frontal cortex to the amygdala during cognitive reappraisal separates depressed from healthy youth and predicts treatment response, which argues for probing emotion regulation under task load and for coaching reappraisal alongside training. Network meta-analytic evidence places combined psychotherapy and pharmacotherapy ahead of either alone for moderate to severe depression, positioning neurofeedback as a component of coordinated care and as a particularly valuable support during medication discontinuation.
Check Your Understanding
- Explain why higher right frontal alpha represents a healthier pattern in the alpha asymmetry model of depression.
- What did Lynch and colleagues (2024) find about the size of the frontostriatal salience network, and how did network size differ from network activity in its relationship to mood?
- Distinguish a trait marker from a state marker, and explain how that distinction should shape your choice of weekly outcome measures.
- What is effective connectivity, and what did frontoamygdalar effective connectivity predict in the Kung and colleagues (2023) study?
- Under what circumstances does the Cuijpers and colleagues (2021) evidence support neurofeedback as a primary intervention, and when does it argue against substituting training for combined care?
Tinnitus
Tinnitus involves the perception of sound, often described as ringing, buzzing, or hissing, when no external acoustic stimulus is present. Tinnitus is commonly associated with hearing loss and affected approximately 11.2% of U.S. adults, about 27 million people, in the most recent national analysis (Batts & Stankovic, 2024). Tinnitus is also the most prevalent service-connected disability among U.S. veterans, with roughly 2.9 million compensated (U.S. Department of Veterans Affairs, 2023).
Clinical Efficacy
Shaffer and Mannion (2016) rated biofeedback for tinnitus as probably efficacious and neurofeedback for tinnitus as possibly efficacious. Note that these ratings come from the third edition of Evidence-Based Practice in Biofeedback and Neurofeedback; every other rating reported in this unit is from the fourth edition.
When Clients Do Not Respond: Modifiable Biological Contributors
The ADHD section of this unit introduced a habit worth generalizing: when a client fails to respond to a treatment that ordinarily works, look for something the diagnosis did not tell you. There, the overlooked variable was a feature of the raw EEG. Across conditions, two other candidates have accumulated enough evidence to belong in a neurofeedback clinician's intake interview, even though neither falls within a non-physician's scope to test or treat. Both matter for the same practical reason: a client whose progress stalls because of an unaddressed metabolic or physiological contributor is easily misread as a training failure, and the usual response of adding more sessions will not fix a problem the training was never addressing.
Methylation, Folate, and the MTHFR Gene
The methylenetetrahydrofolate reductase (MTHFR) gene encodes an enzyme with two jobs that matter for the brain. It converts homocysteine, an amino acid that becomes harmful at elevated concentrations, into methionine, which the body needs for protein synthesis; and it converts dietary folate, a B vitamin, into active folate, the usable form required for DNA synthesis and repair and for manufacturing neurotransmitters (Bailey & Gregory, 1999; Finkelstein, 2000; Lucock, 2000). Two common polymorphisms, meaning naturally occurring variants of a gene present in a substantial fraction of the population, reduce that enzyme's efficiency: C677T and A1298C. They are not rare. Roughly 10% to 15% of people of European ancestry carry two copies of C677T, and up to half carry at least one, with A1298C showing comparable frequencies that vary by population (Wilcken et al., 2003).
Reduced enzyme efficiency produces two downstream problems. Homocysteine accumulates, and elevated homocysteine is associated with cardiovascular disease and with cognitive decline and neurodegenerative risk (Clarke et al., 1998). Meanwhile the body struggles to activate folate even when dietary intake is adequate, and because active folate is required for neurotransmitter synthesis, the resulting functional deficiency can contribute to the imbalances implicated in mood and psychotic disorders (Reynolds, 2002). Meta-analytic work links the C677T polymorphism to depression and, more broadly, to psychiatric disorders including schizophrenia (Gilbody et al., 2007; Roffman et al., 2008; Wu et al., 2013).
Clinicians who work with refractory cases have developed a practical screening heuristic. Ron Swatzyna reviews family history for miscarriages and for heart problems or strokes occurring before the seventies, because both are statistically associated with these polymorphisms, and recommends testing when that history is positive (R. Swatzyna, personal communication, 2024; Kim & Becker, 2003; Ray et al., 1999; Xuan et al., 2014). What to test is genuinely contested. Writing for the Cleveland Clinic, the geneticist Charis Eng (2020) argues that homocysteine levels rather than MTHFR genotype should determine action, since the genotype is common and its consequences are what actually need correcting. The counterargument is that homocysteine assays carry their own problems, including substantial intra-individual variability across repeated draws and genotype-dependent responses to supplementation (Crider et al., 2011; Santhosh-Kumar et al., 1997). Either way, ordering and interpreting these tests belongs to the client's physician.
When a deficiency is identified, the correction is dietary folate from leafy greens, legumes, and fortified grains, plus supplementation with methylfolate, the already-active form that bypasses the impaired enzyme entirely (Bailey & Gregory, 1999). The evidence for benefit is real but should be described to clients as modest augmentation rather than treatment. Methylfolate improves antidepressant response in patients with major depressive disorder who show partial or no response to standard medication (Hoepner et al., 2021; Jain et al., 2019; Maruf et al., 2021), preliminary randomized controlled trials suggest benefit for manic symptoms in bipolar disorder though not yet for bipolar depression (Sylvia et al., 2012), and it is associated with improvement in the negative symptoms of schizophrenia while its effects on positive and general symptoms remain unclear (Roffman et al., 2017; Sakuma et al., 2018).
The actionable step for a neurofeedback clinician is narrow and entirely within scope: ask about family history of miscarriage, early cardiac events, and stroke during the intake, and when a client with depression, anxiety, or a psychotic disorder plateaus despite an adequate training dose, raise the possibility of a metabolic contributor with the prescribing physician rather than escalating the protocol. Framing that referral as a question about homocysteine and folate status, supported by the family history you documented, is more likely to be acted on than a general suggestion that something else might be wrong.
The Gut–Brain Axis and the Microbiome
The gut microbiome, the community of bacteria, fungi, and viruses inhabiting the gastrointestinal tract, communicates with the central nervous system through neural, hormonal, and immune pathways collectively called the gut–brain axis. Gut bacteria synthesize neurotransmitters including gamma-aminobutyric acid, serotonin, and dopamine, and they produce short-chain fatty acids (SCFAs), metabolites generated by fermenting dietary fiber that maintain the integrity of the gut barrier and restrain systemic inflammation. Reviewing this literature for serious mental illnesses (SMIs), meaning schizophrenia, bipolar disorder, and major depressive disorder, Nguyen and colleagues (2021) found consistent evidence of dysbiosis, an imbalance in microbial composition. Reduced microbial diversity appeared across conditions, with increased pro-inflammatory Prevotella and Bacteroides in schizophrenia, reduced anti-inflammatory Faecalibacterium in the limited bipolar literature, and reduced SCFA-producing Lactobacillus and Bifidobacterium in major depressive disorder. The proposed common pathway is neuroinflammation, the inflammatory activation of nervous tissue that a depleted SCFA supply fails to restrain. These directional findings should be held loosely. Later syntheses covering the same three disorders report that most analyses find no difference in microbial diversity between cases and controls, and they reverse or fail to confirm several genus-level directions, including those for Bacteroides in schizophrenia and Lactobacillus in major depressive disorder, so the pattern is better described as unsettled than as established.
The honest appraisal is that this field is early. Most studies are observational and small, sequencing methods and diagnostic criteria vary enough to make cross-study comparison difficult, and diet, lifestyle, and medication confound nearly every finding. The relationship also runs in both directions: antipsychotics and mood stabilizers themselves alter microbial composition, so differences observed in medicated patients cannot be interpreted as causes of their illness (Nguyen et al., 2021). Among interventions, probiotics using Lactobacillus and Bifidobacterium strains have shown potential for improving depressive symptoms and cognition, but results vary with strain, dose, and design. Dietary change emphasizing high-fiber foods and fermented products is linked to greater microbial diversity and SCFA production, with adherence the main obstacle. Fecal microbiota transplantation (FMT), the transfer of gut microbiota from a healthy donor to a patient, shows early promise but faces unresolved questions of safety and standardization.
For neurofeedback practice, the appropriate posture is interest without overreach. General wellness education about fiber, fermented foods, and dietary quality sits comfortably within the lifestyle counseling that already accompanies biofeedback training, and it is the intervention with the best risk-benefit profile in this literature. Recommending specific probiotic regimens, and certainly anything involving FMT, does not. There is also a mechanistic connection worth noting without overstating: the vagus nerve is one channel of the gut–brain axis, and HRV biofeedback strengthens the vagally mediated regulation this unit describes in the anxiety and depression sections, which makes the pairing of dietary counseling with HRV training conceptually coherent even though no trial has yet tested that combination directly. The most concrete clinical use is a referral trigger. A client with treatment-resistant mood symptoms, prominent gastrointestinal complaints, and a history of repeated antibiotic courses is a client whose medical workup is incomplete, and saying so is more useful than adding sessions.
Staying Within Scope While Broadening the Formulation
Both of these literatures invite a failure mode that the ethics unit of this course addresses directly. Understanding that a genetic polymorphism or a microbial imbalance may be contributing to a client's presentation does not authorize a non-physician to order tests, interpret laboratory values, or recommend supplements, and clients under pressure from a stalled treatment are unusually receptive to advice that exceeds a provider's competence. The defensible practice is to broaden the formulation while narrowing the action. Take a history detailed enough to notice these possibilities, document what you observe, name the question for the physician who can pursue it, and continue delivering the intervention you are trained to deliver. Doing so also protects the training itself from an unfair verdict, because a client who plateaus for a metabolic reason has not demonstrated that neurofeedback failed; they have demonstrated that the formulation was incomplete.
Key Takeaways
When a client stalls despite an adequate training dose, the formulation rather than the protocol may be incomplete. Common MTHFR polymorphisms reduce the enzyme that activates folate and clears homocysteine, and methylfolate supplementation modestly augments treatment in depression, mania, and the negative symptoms of schizophrenia. A family history of miscarriage or early cardiac events and strokes is a practical prompt for a physician referral. Dysbiosis and reduced microbial diversity appear consistently across serious mental illnesses, plausibly acting through neuroinflammation, though the evidence remains observational and confounded by diet and psychotropic medication. Dietary counseling sits within a biofeedback clinician's scope; ordering tests, interpreting laboratory values, and recommending supplements or fecal microbiota transplantation does not.
Check Your Understanding
- What two biochemical functions does the MTHFR enzyme perform, and what happens to each when the C677T or A1298C polymorphism reduces its efficiency?
- Why does methylfolate supplementation bypass the problem created by these polymorphisms?
- What family history findings should prompt you to raise the question of MTHFR testing with a client's physician?
- Describe the gut–brain axis and explain why psychotropic medication complicates causal interpretation of microbiome findings in serious mental illness.
- Which microbiome-related recommendations fall within a biofeedback clinician's scope of practice, and which do not?
Cutting-Edge Topics in Neurofeedback Research
Neurofeedback and Brain-Computer Interfaces
Advances in brain-computer interface (BCI) technology are transforming what is possible with neurofeedback. Modern BCI systems can detect and respond to brain signals with unprecedented precision, opening new avenues for treating conditions from ADHD to severe depression.
Real-Time fMRI Neurofeedback for Psychiatric Disorders
Real-time functional MRI (rtfMRI) neurofeedback allows patients to observe and regulate activity in specific brain regions with high spatial precision. While EEG-based neurofeedback can localize activity only roughly, fMRI can target structures deep in the brain with millimeter accuracy. The amygdala is the obvious candidate in mood disorders, since the frontoamygdalar pathway that separates depressed from healthy youth and predicts treatment response lies well below the reach of scalp electrodes (Kung et al., 2023), and the same logic extends to the frontostriatal salience network whose expansion marks vulnerability to depression years before the first episode (Lynch et al., 2024). The open questions are practical rather than conceptual: rtfMRI remains expensive and scarce, and whether the regulation skills learned in a scanner transfer to daily life as durably as the EEG-based gains documented earlier in this unit is not yet established.
Personalized Neurofeedback Protocols
The field is moving toward individualized treatment approaches based on each patient's unique brain patterns. Machine learning algorithms can now analyze qEEG data to identify subtypes within diagnostic categories like ADHD, allowing clinicians to select protocols most likely to benefit specific patients. Monte Carlo modeling of network coherence has already isolated connectivity signatures that a conventional spectral report would miss (Kerson et al., 2023), deep learning applied to event-related spectral EEG has separated adults with ADHD from controls with accuracy approaching 88% (Dubreuil-Vall et al., 2020), and decoded neurofeedback, which trains feedback on machine-learned patterns of activity rather than on raw band power, points toward protocols targeted at specific neural representations rather than at broad frequency ranges. The unresolved question is not whether these methods can detect subgroups but whether subgroup-matched protocols outperform standard ones in prospective trials.
Glossary
A1 score: frontal alpha asymmetry score calculated by subtracting log left-alpha power from log right-alpha power to assess hemispheric activation balance.
A1298C: a common polymorphism of the MTHFR gene that reduces enzyme efficiency, impairing folate activation and homocysteine clearance.
absence seizures: generalized-onset seizures, historically called petit mal, featuring brief loss of consciousness without abnormal movement; the patient appears to be daydreaming.
active epilepsy: self-reported doctor-diagnosed epilepsy with current treatment using antiseizure medicines or at least one seizure in the past 12 months.
active folate: the bioavailable form of folate required for DNA synthesis and repair and for neurotransmitter production.
addictive personality: the disproven notion that a single personality type destines an individual for addiction; specific traits raise or lower vulnerability, but no unified profile predicts who develops a substance use disorder.
alpha asymmetry neurofeedback for mood disorders: a protocol that trains depressed clients to increase right frontal alpha relative to left frontal alpha, thereby reducing right frontal activity or increasing left frontal activity.
amyloid beta: a peptide implicated in Alzheimer’s disease that accumulates following the mechanical stresses of mild head injury.
attention dorsal network (AttDN): a large-scale network that directs and sustains goal-driven attention; shows reduced coherence in children with ADHD.
behavioral activation system (BAS): brain system associated with approach motivation and positive emotions, mediated primarily by left frontal cortex.
behavioral inhibition system (BIS): brain system associated with withdrawal motivation and negative affect, mediated primarily by right frontal cortex.
Brodmann area (BA): a numbered cortical region defined by differences in cell architecture, each associated with characteristic sensory, motor, or cognitive functions.
C677T: the most studied MTHFR polymorphism, substantially decreasing enzyme activity and raising homocysteine levels.
caudate nucleus: a basal ganglia structure central to habit formation, reward processing, and motor control.
central nervous system hyperarousal: a chronically overactivated brain state characterized by low alpha and high beta activity, associated with anxiety and poor treatment outcomes in substance use disorders.
clinical remitter: a participant who shows a meaningful reduction in ADHD symptoms following treatment as determined by standardized behavioral assessment; a non-remitter shows no clinically significant improvement.
cognitive behavioral therapy (CBT): a structured psychotherapy that identifies and changes the negative thought patterns and behaviors associated with a mental health condition.
cognitive flexibility: an executive function involving the ability to shift between mental sets, tasks, or strategies.
cognitive reappraisal: an emotion regulation strategy in which a distressing situation is deliberately reinterpreted to reduce its emotional impact.
coherence: a measure of how consistently the signals recorded from two brain regions maintain their phase relationship, used as an index of functional communication between them.
collateral information: diagnostic data gathered from informants other than the client, such as parents, partners, teachers, or roommates; especially important when self-report is subject to elevated bias.
combination therapy: a treatment approach that delivers psychotherapy and pharmacotherapy together rather than choosing between them.
concussion: the common term for a mild traumatic brain injury produced by a blow or jolt that moves the brain rapidly within the skull.
connectivity training: neurofeedback designed to correct deficient or excessive communication between two brain sites as measured by indices like coherence and comodulation.
conscientiousness: a personality trait comprising self-discipline, organization, dependability, and forethought; protective against substance use disorders.
contingent negative variation (CNV): a slow negative event-related potential that builds between a warning signal and an expected stimulus, indexing anticipation and motor preparation; reduced in ADHD.
contrecoup injury: damage occurring on the side of the brain opposite the point of impact, produced when the brain rebounds against the inner skull.
cortical hypoarousal: an underactivated cortical state associated with reduced alertness and impaired attention, often seen in ADHD.
cortical surface area: the total area of the cortical sheet measured across all of its folds and grooves.
cortical thickness: the depth of the gray matter layer at a given point on the cortical surface.
decoded neurofeedback: a technique that uses machine learning to identify specific patterns of brain activity and delivers feedback based on these decoded neural representations rather than on raw band power.
default mode network (DMN): a network associated with self-referential thought and mind-wandering that normally deactivates during goal-directed tasks; frequently dysregulated in ADHD.
derivation sample: the population from which diagnostic criteria, normative data, or validity statistics were originally generated; its characteristics set the boundaries of appropriate generalization.
diffusion tensor imaging (DTI): an MRI technique that maps white matter tracts by measuring the direction in which water diffuses through tissue.
dopaminergic signaling: neural communication using dopamine; its dysregulation is a long-standing account of psychotic symptoms.
dorsolateral prefrontal cortex (dlPFC): a frontal region supporting working memory, cognitive flexibility, and impulse control.
dynamic causal modeling (DCM): an analytic method that estimates the directional influence one brain region exerts over another from neuroimaging data.
dysbiosis: an imbalance in the composition of the gut microbiota, commonly marked by reduced diversity and an excess of pro-inflammatory species.
dysregulated EEG patterns: abnormal brainwave signatures that deviate from healthy functioning and correlate with neurocognitive impairments.
effective connectivity: the directional influence that one brain region exerts over another, distinguished from functional connectivity, which describes correlation without direction.
emotion dysregulation: persistent difficulty managing emotional responses, producing heightened reactivity, prolonged distress, and reliance on maladaptive strategies such as suppression or rumination.
encephalopathy: diffuse slowing and attenuation of EEG amplitude reflecting toxic, metabolic, or hypoxic compromise of global brain function.
error positivity (Pe): a positive event-related potential deflection following the error-related negativity, associated with conscious awareness of a mistake.
error-related negativity (ERN): a sharp negative event-related potential deflection appearing within roughly 100 ms of an incorrect response, reflecting performance monitoring.
event-related potentials (ERPs): voltage changes in the ongoing EEG that are time-locked to a specific sensory, cognitive, or motor event and index discrete stages of information processing.
executive function: the family of higher-order cognitive processes supporting planning, inhibition, working memory, and goal-directed behavior.
fecal microbiota transplantation (FMT): transfer of gut microbiota from a healthy donor to a recipient in order to restore microbial balance.
focal slowing: localized low-frequency EEG activity indicating regional cerebral dysfunction, often associated with underlying lesion or injury.
folate: a B vitamin required for DNA synthesis and repair and for the production of neurotransmitters, obtained from leafy greens, legumes, and fortified grains.
frontal alpha asymmetry (FAA): the difference in alpha power between left and right frontal regions, proposed as a neurophysiological marker for depression.
frontal-midline theta: theta activity arising from medial prefrontal regions during tasks requiring cognitive control such as error monitoring and conflict resolution.
frontal–subcortical circuits: pathways connecting the frontal lobes with subcortical structures, supporting executive function, emotion regulation, and behavioral control.
frontostriatal salience network: a network linking frontal cortex and striatum that detects behaviorally significant stimuli and processes reward; approximately twice its typical size in individuals with depression.
functional magnetic resonance imaging (fMRI): a non-invasive imaging method that maps brain activity by detecting blood-oxygenation changes associated with neural activity.
generalized anxiety disorder (GAD): excessive anxiety and worry occurring more days than not for at least 6 months.
global theta: an averaged measure of theta power across multiple electrode sites, reflecting general cortical slowing or underactivation.
gut–brain axis: the bidirectional communication system linking the gastrointestinal tract and the central nervous system through neural, hormonal, and immune pathways.
gut microbiome: the community of bacteria, fungi, and viruses inhabiting the gastrointestinal tract.
halo effect: a cognitive bias in which the presence of one salient trait or symptom cluster influences the perception or diagnosis of another.
heart rate variability biofeedback (HRVB): a technique that trains people to breathe at specific rates to optimize heart rhythm patterns and improve autonomic function.
homocysteine: an amino acid that, at elevated concentrations, is associated with cardiovascular disease, cognitive decline, and neurodegenerative risk.
hypnagogic state: the twilight zone between waking and sleeping where consciousness becomes fluid and dreamlike, induced by alpha-theta neurofeedback.
hypocoherence: reduced connectivity between brain regions, indicating functional network inefficiency.
imaging-derived phenotypes (IDPs): quantitative measurements extracted from brain imaging, such as the volume, thickness, or surface area of a defined region.
impulsivity: a trait marked by acting on urges with little consideration of consequences; associated with earlier substance use initiation, faster progression, and greater relapse risk.
inhibitory control: an executive function involving suppression of impulsive or inappropriate responses.
inverse problem: the challenge in EEG analysis that surface recordings cannot uniquely identify the cortical generators that produced them, because many source configurations yield identical scalp potentials.
isolated epileptiform discharges (IEDs): brief abnormal EEG waveforms indicating cortical hyperexcitability, often subclinical, present in a substantial minority of ADHD cohorts and rare in healthy controls.
Kaiser-Scott protocol: also written Scott–Kaiser protocol; a modification of the Peniston protocol that starts with ADHD neurofeedback training before progressing to alpha-theta training; developed for stimulant and cannabis dependence.
late-identified ADHD: ADHD in which symptoms were present since childhood but not recognized until later in development, distinct from late-onset ADHD in which symptoms first emerge in adulthood.
late positive potential (LPP): a sustained positive event-related potential reflecting continued attention to emotionally salient material; enlarged in adults with ADHD.
long-range input: synaptic input arriving from distant brain regions, as opposed to local input from neighboring neurons.
LORETA (low-resolution electromagnetic tomography): a computational method that estimates three-dimensional cortical sources of scalp-recorded EEG, permitting source-level assessment and training.
Lubar ADHD protocol: trains clients to inhibit theta (4-8 Hz) and increase beta (13-21 Hz) over approximately 40 sessions using 30-minute training periods.
major depressive disorder (MDD): a mood disorder defined by persistent sadness, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed appetite and sleep, difficulty concentrating, and suicidal ideation.
Menninger ON-OFF-ON EEG protocol: teaches patients to increase, decrease, and then increase amplitude within a frequency band during 100- or 200-second segments.
mesolimbic pathway: a dopamine circuit linking midbrain to limbic structures, associated with reward, motivation, and psychotic symptoms.
methionine: an essential amino acid produced from homocysteine, required for protein synthesis and methylation reactions.
methylenetetrahydrofolate reductase (MTHFR) gene: the gene encoding the enzyme that converts homocysteine to methionine and dietary folate to its active form.
methylfolate: the already-active form of folate, which bypasses the impaired MTHFR enzyme and is used as a supplement to correct functional folate deficiency.
microbial diversity: the variety and relative abundance of microbial species in the gut, reduced across serious mental illnesses.
mild traumatic brain injury (mTBI): injury producing loss of consciousness of up to 30 minutes, altered mental status for up to 24 hours, or post-traumatic amnesia for up to 24 hours, without intracranial pathology on structural imaging.
Monte Carlo model: a machine learning method that repeatedly generates random samples and aggregates the results to establish confidence in patterns within complex datasets.
network meta-analysis: a statistical technique that compares several treatments at once by combining direct comparisons with indirect evidence linking them through common comparators.
networks: distributed sets of brain structures whose coordinated activity supports a common function, such as the default mode, salience, and dorsal attention networks.
neurofeedback (NF): a specialized form of biofeedback that trains people to modify their brainwave patterns through operant conditioning.
neuroinflammation: inflammatory activation within nervous tissue, implicated as a common pathway linking systemic inflammation to psychiatric symptoms.
neuroplasticity: the brain's capacity to reorganize neural pathways and form new connections in response to experience or injury.
neuroticism: a personality trait marked by emotional instability and a propensity toward anxiety, guilt, and depressed mood; associated with substance use as self-medication.
neurotoxicity: damage to nervous system tissue caused by exposure to a substance.
non-mood psychotic disorders: conditions such as schizophrenia and delusional disorder in which psychosis is not driven primarily by mood disturbance.
normative database: a reference set of EEG recordings used to compare an individual’s brain activity against age-matched norms.
oddball task: a cognitive task in which participants respond to infrequent target stimuli embedded among frequent standard stimuli, used to elicit event-related brain responses.
oppositional defiant disorder (ODD): a behavioral disorder characterized by a recurring pattern of angry or irritable mood, argumentative or defiant behavior, and vindictiveness toward authority figures.
oxidative stress: an excess of reactive oxygen species that overwhelms antioxidant defenses, producing cellular damage and inflammation.
P300: a positive event-related potential peaking roughly 300 to 600 ms after a task-relevant stimulus, reflecting attentional resource allocation; reduced in amplitude and delayed in ADHD.
passive volition: a strategy of allowing changes to happen rather than actively forcing them, critical to alpha-theta training success.
Peniston addiction protocol: a multimodal treatment including visualization training, temperature biofeedback, rhythmic breathing, autogenic training, and 30 alpha-theta sessions.
performance-based protocols: neurofeedback that uses tasks and training to correct symptoms and improve performance, comparing clients to themselves rather than normative databases.
petit mal seizures: the historical term for absence seizures; not part of the current International League Against Epilepsy classification. See absence seizures.
pharmacotherapy: the use of medication, such as an antidepressant, to treat a mental health disorder.
phase: the timing relationship between EEG signals recorded at two sites, used with coherence to index how efficiently information travels between regions.
polymorphism: a naturally occurring variant of a gene present in a substantial proportion of a population.
post-traumatic stress disorder (PTSD): a trauma and stress-related disorder following exposure to traumatic events like assault, combat, or rape.
PracticeWise: the private company that produces the Blue Menu of Evidence-Based Psychosocial Interventions distributed with American Academy of Pediatrics materials; its Level 1, Best Support rating for biofeedback in attention and hyperactivity behaviors is often misattributed to the Academy itself.
precision functional mapping (PFM): an imaging approach that collects a large volume of fMRI data from the same individual over time to characterize that person’s brain organization rather than a group average.
probiotics: live microorganisms, commonly Lactobacillus and Bifidobacterium strains, administered to improve the balance of gut microbiota.
psychosis: a mental state involving loss of contact with reality, including hallucinations, delusions, and disorganized thinking.
quantitative EEG (qEEG): computerized analysis of brain electrical activity recorded from multiple scalp locations, providing real-time information about power distribution and connectivity.
relapse: the return of symptoms after a period of improvement or remission.
resonance frequency: the breathing rate, typically around 6 breaths per minute, that maximizes respiratory sinus arrhythmia and strengthens baroreflex function.
resting-state EEG: brain activity recorded while an individual is awake but not engaged in a task, used to assess baseline neural function.
rostral middle frontal gyrus: a prefrontal region supporting executive control and decision-making; thinner in children who later initiate substance use.
salience network (SalN): a network that detects behaviorally relevant stimuli and switches processing resources toward them.
sample drift: the loss of diagnostic accuracy that occurs when a test is applied to a population differing from the sample on which its validity statistics were established.
second hit hypothesis: the model that a genetic or developmental vulnerability constitutes a first hit and a later environmental insult such as head injury constitutes a second, together precipitating psychiatric illness.
sensation-seeking: a trait marked by pursuit of novel, complex, and intense experience; raises the risk of substance use initiation but appears largely irrelevant once dependence is established.
sensitivity: the probability that a test result will be positive when the condition is actually present; a highly sensitive test misses few true cases.
sensorimotor rhythm (SMR): an EEG rhythm from 12-14 Hz located over the sensorimotor cortex, associated with inhibition of movement and reduced muscle tone.
serious mental illnesses (SMIs): disorders producing substantial functional impairment, including schizophrenia, bipolar disorder, and major depressive disorder.
sham neurofeedback: a control condition in which participants receive feedback generated from prerecorded or non-contingent EEG rather than their own real-time brain activity.
short-chain fatty acids (SCFAs): metabolites produced when gut bacteria ferment dietary fiber, supporting gut barrier integrity and restraining inflammation.
slow cortical potentials (SCP): slow shifts in cortical electrical activity linked to the regulation of cortical excitability and attentional preparation, trained in a distinct neurofeedback protocol.
SMR up-training: neurofeedback protocol that trains patients to increase sensorimotor rhythm (12-14 Hz) amplitude while inhibiting slow-wave activity; used primarily for epilepsy treatment.
somatostatin (SST) interneurons: a class of inhibitory neuron that regulates the input and output of local networks and reorganizes brain-wide after traumatic brain injury.
specificity: the probability that a test result will be negative when the condition is actually absent; a highly specific test produces few false positives.
spindling excessive beta (SEB): frontocentral beta activity in the 15 to 35 Hz range with a spindle-like morphology, associated with impulse control problems and cortical hyperarousal.
standardized mean difference (SMD): a meta-analytic effect size that expresses results measured on different scales in common units so they can be pooled.
state marker: a measure that rises and falls with the current episode of a disorder and is therefore suited to tracking change over treatment.
Sterman's protocol: trains epileptic patients to increase SMR (12-14 Hz) amplitude and duration while suppressing theta, high beta, epileptiform spikes, and EMG artifact during 36 sessions.
substance use disorder: a pattern of symptoms from substance use despite experiencing significant problems in multiple life areas.
substance use initiation: the first use of alcohol, nicotine, cannabis, or another psychoactive substance.
susceptibility-weighted imaging (SWI): an MRI sequence exploiting magnetic differences between tissues to reveal microhemorrhages, small veins, and iron deposits.
task-related theta: theta activity observed during engagement with a cognitive task, associated with attention and executive control.
theta/beta ratio (TBR): the ratio of theta to beta power in the brain's electrical activity, proposed as a biomarker for ADHD reflecting cortical hypoarousal.
theta/beta training: a neurofeedback procedure that down-trains theta and up-trains beta to address the elevated theta/beta ratio seen in ADHD.
tinnitus: the perception of sound, often described as ringing or buzzing, when no external acoustic stimulus is present.
tonic-clonic seizures: generalized-onset seizures with convulsions, historically called grand mal, featuring a cry, loss of consciousness, falling, and rhythmic jerking of all extremities.
trait marker: a stable characteristic that indicates vulnerability to a disorder and does not fluctuate with symptom severity.
transdiagnostic factor: a symptom or process that appears across multiple mental health disorders rather than being specific to one diagnosis.
traumatic brain injury (TBI): intracranial injury due to acceleration or direct impact that disrupts normal brain function through both structural damage and altered neural connectivity.
volume conduction: the spread of electrical current through brain, skull, and scalp tissue so that a single cortical source appears at multiple electrodes, complicating source localization and connectivity estimates.
white matter damage: disruption of myelinated axonal pathways, impairing communication between brain regions.
working memory: an executive function responsible for briefly holding and manipulating information during cognitive tasks.
Z-score training: a neurofeedback strategy that attempts to normalize brain function with respect to database mean values, targeting activity that is 2 or more standard deviations from the norm.
Test Yourself
Click on the ClassMarker logo to take 10-question tests over this unit without an exam password.

Review Flashcards on Quizlet
Click on the Quizlet logo to review our chapter flashcards.

Visit the BioSource Software Website
BioSource Software offers Physiological Psychology, which satisfies BCIA's Neuroanatomy requirement, and the Neurofeedback100 Testing Service, which provides extensive multiple-choice testing over the Neurofeedback Blueprint.

Assignment
Now that you have completed this module, consider the elements that neurofeedback training shares with modalities like EMG and temperature biofeedback. How is neurofeedback training different? What unique challenges does training brain activity present compared to training peripheral physiological signals?
References
American Academy of Pediatrics. (2012). Evidence-based child and adolescent psychosocial interventions.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author.
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). Author.
American Psychological Association. (2016, February 22). Persistent ADHD associated with overly critical parents. https://www.apa.org/news/press/releases/2016/02/adhd-critical-parents
Anderson, B. A. (2021). An adaptive view of attentional control. American Psychologist, 76(9), 1410-1422.
Arnold, L. E., Arns, M., Barterian, J., Bergman, R., Black, S., Conners, C. K., Connor, S., Dasgupta, S., deBeus, R., Higgins, T., Hirshberg, L., Hollway, J. A., Kerson, C., Lightstone, H., Lofthouse, N., Lubar, J., McBurnett, K., Monastra, V., Buchan-Page, K., . . . Williams, C. E. (2021). Double-blind placebo-controlled randomized clinical trial of neurofeedback for attention-deficit/hyperactivity disorder with 13-month follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 60(7), 841–855. https://doi.org/10.1016/j.jaac.2020.07.906
Arns, M., Conners, C. K., & Kraemer, H. C. (2013). A decade of EEG theta/beta ratio research in ADHD: A meta-analysis. Journal of Attention Disorders, 17(5), 374-383. https://doi.org/10.1177/1087054712460087
Arns, M., Swatzyna, R. J., Gunkelman, J., & Olbrich, S. (2015). Sleep maintenance, spindling excessive beta and impulse control: An RDoC arousal and regulatory systems approach? Neuropsychiatric Electrophysiology, 1, Article 5. https://doi.org/10.1186/s40810-015-0005-9
Arns, M., Feddema, I., & Kenemans, J. L. (2014). Differential effects of theta/beta and SMR neurofeedback in ADHD on sleep onset latency. Frontiers in Human Neuroscience, 8, 1019. https://doi.org/10.3389/fnhum.2014.01019
Arns, M., & Kenemans, J. L. (2014). Neurofeedback in ADHD and insomnia: Vigilance stabilization through sleep spindles and circadian networks. Neuroscience and Biobehavioral Reviews, 44, 183-194. https://doi.org/10.1016/j.neubiorev.2012.10.006
Arrondo, G., Mulraney, M., Iturmendi-Sabater, I., Musullulu, H., Gambra, L., Niculcea, T., Banaschewski, T., Simonoff, E., Döpfner, M., Hinshaw, S. P., Coghill, D., & Cortese, S. (2024). Systematic review and meta-analysis: Clinical utility of continuous performance tests for the identification of attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 63(2), 154-171. https://doi.org/10.1016/j.jaac.2023.03.011
Ayers, M. E. (1995). EEG neurofeedback to bring individuals out of level 2 coma. Biofeedback and Self-Regulation, 20(3), 304-305.
Baehr, E., Rosenfeld, J. P., & Baehr, R. (1997). The clinical use of an alpha asymmetry protocol in the neurofeedback treatment of depression: Two case studies. Journal of Neurotherapy, 2(3), 10-23.
Bailey, L. B., & Gregory, J. F. (1999). Folate metabolism and requirements. The Journal of Nutrition, 129(4), 779-782. https://doi.org/10.1093/jn/129.4.779
Banaschewski, T., & Brandeis, D. (2007). Annotation: What electrical brain activity tells us about brain function that other techniques cannot tell us—A child psychiatric perspective. Journal of Child Psychology and Psychiatry, 48(5), 415-435. https://doi.org/10.1111/j.1469-7610.2006.01681.x
Barkley, R. A. (2015). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (4th ed.). Guilford Press.
Barry, R. J., Johnstone, S. J., & Clarke, A. R. (2003). A review of electrophysiology in attention-deficit/hyperactivity disorder: II. Event-related potentials. Clinical Neurophysiology, 114(2), 184-198. https://doi.org/10.1016/S1388-2457(02)00363-2
Batts, S., & Stankovic, K. M. (2024). Tinnitus prevalence, associated characteristics, and related healthcare use in the United States: A population-level analysis. The Lancet Regional Health - Americas, 29, 100659.
Beauchamp, M. H., Beare, R., Ditchfield, M., Coleman, L., Babl, F. E., Kean, M., Crossley, L., Catroppa, C., Yeates, K. O., & Anderson, V. (2013). Susceptibility weighted imaging and its relationship to outcome after pediatric traumatic brain injury. Cortex, 49(2), 591-598. https://doi.org/10.1016/j.cortex.2012.08.015
Belanger, H. G., Tate, D. F., & Vanderploeg, R. D. (2018). Concussion and mild traumatic brain injury. In J. E. Morgan & J. H. Ricker (Eds.), Textbook of clinical neuropsychology (2nd ed., pp. 411-448). Routledge.
Belanger, H. G., Spiegel, E., & Vanderploeg, R. D. (2010). Neuropsychological performance following a history of multiple self-reported concussions: A meta-analysis. Journal of the International Neuropsychological Society, 16(2), 262–267. https://doi.org/10.1017/S1355617709991287
Biederman, J., Mick, E., & Faraone, S. V. (2000). Age-dependent decline of symptoms of attention deficit hyperactivity disorder: Impact of remission definition and symptom type. American Journal of Psychiatry, 157(5), 816–818. https://doi.org/10.1176/appi.ajp.157.5.816
Berglund, K., Roman, E., Balldin, J., Berggren, U., Eriksson, M., Gustavsson, P., & Fahlke, C. (2011). Do men with excessive alcohol consumption and social stability have an addictive personality? Scandinavian Journal of Psychology, 52(3), 257-260. https://doi.org/10.1111/j.1467-9450.2010.00872.x
Bishop, S. J. (2008). Neural mechanisms underlying selective attention to threat. Annals of the New York Academy of Sciences, 1129(1), 141-152. https://doi.org/10.1196/annals.1417.016
Bluschke, A., Broschwitz, F., Kohl, S., Roessner, V., & Beste, C. (2016). The neuronal mechanisms underlying improvement of impulsivity in ADHD by theta/beta neurofeedback. Scientific Reports, 6, 31178.
Bogg, T., & Roberts, B. W. (2004). Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin, 130(6), 887-919. https://doi.org/10.1037/0033-2909.130.6.887
Bong, S. H., & Kim, J. W. (2021). The role of quantitative electroencephalogram in the diagnosis and subgrouping of attention-deficit/hyperactivity disorder. Journal of the Korean Academy of Child and Adolescent Psychiatry, 32(3), 85-92. https://doi.org/10.5765/jkacap.210010
Brody, D. J., & Hughes, J. P. (2025). Depression prevalence in adolescents and adults: United States, August 2021-August 2023. NCHS Data Brief, 527, 1-11.
Broglio, S. P., Eckner, J. T., Martini, D., Sosnoff, J. J., Kutcher, J. S., & Randolph, C. (2011). Cumulative head impact burden in high school football. Journal of Neurotrauma, 28(10), 2069-2078. https://doi.org/10.1089/neu.2011.1825
Bussalb, A., Collin, S., Barthélemy, Q., Ojeda, D., Bioulac, S., Blasco-Fontecilla, H., Brandeis, D., Purper Ouakil, D., Ros, T., & Mayaud, L. (2019). Is there a cluster of high theta-beta ratio patients in attention deficit hyperactivity disorder? Clinical Neurophysiology, 130(8), 1387-1396. https://doi.org/10.1016/j.clinph.2019.02.021
Byeon, J., Choi, T.-Y., Won, G.-H., Lee, J., & Kim, J. W. (2020). A novel quantitative electroencephalography subtype with high alpha power in ADHD: ADHD or misdiagnosed ADHD? PLOS ONE, 15(11), e0242566. https://doi.org/10.1371/journal.pone.0242566
Centers for Disease Control and Prevention. (2013). Key findings: Trends in the parent-report of health care provider diagnosed and medicated ADHD, United States, 2003-2011. National Center on Birth Defects and Developmental Disabilities.
Centers for Disease Control and Prevention. (2024). Epilepsy: Facts and stats. https://www.cdc.gov/epilepsy/data-research/facts-stats/index.html
Centers for Disease Control and Prevention. (2023). TBI data. Retrieved from https://www.cdc.gov/traumatic-brain-injury/data-research/index.html
Chaves, R. S., Tran, M., Holder, A. R., Balcer, A. M., Dickey, A. M., Roberts, E. A., Bober, B. G., Gutiérrez, E., Head, B. P., Groisman, A., Goldstein, L. S. B., Almenar-Queralt, A., & Shah, S. B. (2021). Amyloidogenic processing of amyloid precursor protein drives stretch-induced disruption of axonal transport in hiPSC-derived neurons. The Journal of Neuroscience, 41(49), 10034-10053. https://doi.org/10.1523/JNEUROSCI.2553-20.2021
Cheetham, A., Allen, N. B., Whittle, S., Simmons, J., Yücel, M., & Lubman, D. I. (2014). Volumetric differences in the anterior cingulate cortex prospectively predict alcohol-related problems in adolescence. Psychopharmacology, 231(8), 1731-1742. https://doi.org/10.1007/s00213-014-3483-8
Chen, P.-Y., Su, I.-C., Shih, C.-Y., Liu, Y.-C., Su, Y.-K., Wei, L., Luh, H.-T., Huang, H.-C., Tsai, P.-S., Fan, Y.-C., & Chiu, H.-Y. (2023). Effects of neurofeedback on cognitive function, productive activity, and quality of life in patients with traumatic brain injury: A randomized controlled trial. Neurorehabilitation and Neural Repair, 37(5), 277-287.
Chronis, A. M., Chacko, A., Fabiano, G. A., Wymbs, B. T., & Pelham, W. E. (2004). Enhancements to the behavioral parent training paradigm for families of children with ADHD: Review and future directions. Clinical Child and Family Psychology Review, 7(1), 1-27. https://doi.org/10.1023/B:CCFP.0000020190.60808.a4
Clarke, A. R., Barry, R. J., McCarthy, R., & Selikowitz, M. (2001). Excess beta activity in children with attention-deficit/hyperactivity disorder: An atypical electrophysiological group. Psychiatry Research, 103(2-3), 205-218. https://doi.org/10.1016/S0165-1781(01)00277-3
Clarke, R., Smith, A. D., Jobst, K. A., Refsum, H., Sutton, L., & Ueland, P. M. (1998). Folate, vitamin B12, and serum total homocysteine levels in confirmed Alzheimer's disease. Archives of Neurology, 55(11), 1449-1455. https://doi.org/10.1001/archneur.55.11.1449
Crider, K. S., Zhu, J.-H., Hao, L., Yang, Q.-H., Yang, T. P., Gindler, J., Maneval, D. R., Quinlivan, E. P., Li, Z., Bailey, L. B., & Berry, R. J. (2011). MTHFR 677C→T genotype is associated with folate and homocysteine concentrations in a large, population-based, double-blind trial of folic acid supplementation. The American Journal of Clinical Nutrition, 93(6), 1365-1372. https://doi.org/10.3945/ajcn.110.004671
Crisco, J. J., Fiore, R., Beckwith, J. G., Chu, J. J., Brolinson, P. G., Duma, S., McAllister, T. W., Duhaime, A.-C., & Greenwald, R. M. (2010). Frequency and location of head impact exposures in individual collegiate football players. Journal of Athletic Training, 45(6), 549-559. https://doi.org/10.4085/1062-6050-45.6.549
Cuijpers, P., Oud, M., Karyotaki, E., Noma, H., Quero, S., Cipriani, A., Arroll, B., & Furukawa, T. A. (2021). Psychologic treatment of depression compared with pharmacotherapy and combined treatment in primary care: A network meta-analysis. Annals of Family Medicine, 19(3), 262-270. https://doi.org/10.1370/afm.2676
D'Aiello, B., Menghini, D., Di Vara, S., De Rossi, P., & Vicari, S. (2024). Predictors of methylphenidate response in children and adolescents with ADHD: The role of sleep disturbances. European Archives of Psychiatry and Clinical Neuroscience. Advance online publication. https://doi.org/10.1007/s00406-024-01932-7
Davidson, R. J. (1992). Anterior cerebral asymmetry and the nature of emotion. Brain and Cognition, 20(1), 125-151.
de Wit, H. (2009). Impulsivity as a determinant and consequence of drug use: A review of underlying processes. Addiction Biology, 14(1), 22-31. https://doi.org/10.1111/j.1369-1600.2008.00129.x
Deiber, M.-P., Hasler, R., Colin, J., Dayer, A., Aubry, J.-M., Baggio, S., Perroud, N., & Ros, T. (2019). Linking alpha oscillations, attention and inhibitory control in adult ADHD with EEG neurofeedback. NeuroImage: Clinical, 25, 102145. https://doi.org/10.1016/j.nicl.2019.102145
Denworth, L. (2024). Kids with ADHD may still have symptoms as adults. Scientific American.
Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64, 135-168. https://doi.org/10.1146/annurev-psych-113011-143750
Dubreuil-Vall, L., Ruffini, G., & Camprodon, J. A. (2020). Deep learning convolutional neural networks discriminate adult ADHD from healthy individuals on the basis of event-related spectral EEG. Frontiers in Neuroscience, 14, 251. https://doi.org/10.3389/fnins.2020.00251
DuPaul, G. J., & Stoner, G. (2014). ADHD in the schools: Assessment and intervention strategies (3rd ed.). Guilford Press.
Eng, C. (2020). A genetic test you don't need. Cleveland Clinic Health Essentials. https://health.clevelandclinic.org/a-genetic-test-you-dont-need
Enriquez-Geppert, S., Brown, T., Heinrich, H., Arns, M., & Garcia Pimenta, M. (2023). Treatment efficacy and clinical effectiveness of EEG neurofeedback as a personalized and multimodal treatment in ADHD: A critical review. In I. Khazan, F. Shaffer, D. Moss, R. Lyle, & S. Rosenthal (Eds.), Evidence-based practice in biofeedback and neurofeedback (4th ed.). AAPB.
Enriquez-Geppert, S., Krc, J., van Dijk, H., deBeus, R. J., Arnold, L. E., & Arns, M. (2024). Theta/beta ratio neurofeedback effects on resting and task-related theta activity in children with ADHD. Applied Psychophysiology and Biofeedback, 50(4), 667-685. https://doi.org/10.1007/s10484-024-09675-w
Enriquez-Geppert, S., Smit, D., Pimenta, M. G., & Arns, M. (2019). Neurofeedback as a treatment intervention in ADHD: Current evidence and practice. Current Psychiatry Reports, 21(6), 46.
Epstein, J. N., Willoughby, M., Valencia, E. Y., Tonev, S. T., Abikoff, H. B., Arnold, L. E., & Hinshaw, S. P. (2005). The role of children's ethnicity in the relationship between teacher ratings of attention-deficit/hyperactivity disorder and observed classroom behavior. Journal of Consulting and Clinical Psychology, 73(3), 424-434. https://doi.org/10.1037/0022-006X.73.3.424
Ersche, K. D., Jones, P. S., Williams, G. B., Turton, A. J., Robbins, T. W., & Bullmore, E. T. (2012). Abnormal brain structure implicated in stimulant drug addiction. Science, 335(6068), 601-604. https://doi.org/10.1126/science.1214463
Evans, S. W., Owens, J. S., & Bunford, N. (2014). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 43(4), 527-551. https://doi.org/10.1080/15374416.2013.850700
Evenden, J. L. (1999). Varieties of impulsivity. Psychopharmacology, 146(4), 348-361. https://doi.org/10.1007/PL00005481
Finkelstein, J. D. (2000). Pathways and regulation of homocysteine metabolism in mammals. Seminars in Thrombosis and Hemostasis, 26(3), 219-226. https://doi.org/10.1055/s-2000-8466
Fisher, R. S., Cross, J. H., French, J. A., Higurashi, N., Hirsch, E., Jansen, F. E., Lagae, L., Moshé, S. L., Peltola, J., Roulet Perez, E., Scheffer, I. E., & Zuberi, S. M. (2017). Operational classification of seizure types by the International League Against Epilepsy: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia, 58(4), 522–530. https://doi.org/10.1111/epi.13670
Forssman, L., Eninger, L., Tillman, C. M., Rodriguez, A., & Bohlin, G. (2012). Cognitive functioning and family risk factors in relation to symptom behaviors of ADHD and ODD in adolescents. Journal of Attention Disorders, 16(4), 284-294. https://doi.org/10.1177/1087054710385065
Foster, S. R., Foster, D. S., & Gross, M. N. (2023). Traumatic brain injury. In I. Khazan, F. Shaffer, D. Moss, R. Lyle, & S. Rosenthal (Eds.), Evidence-based practice in biofeedback and neurofeedback (4th ed.). AAPB.
Frankowski, J. C., Tierno, A., Pavani, S., Cao, Q., Lyon, D. C., & Hunt, R. F. (2022). Brain-wide reconstruction of inhibitory circuits after traumatic brain injury. Nature Communications, 13(1), 3417. https://doi.org/10.1038/s41467-022-31072-2
Franques, P., Auriacombe, M., & Tignol, J. (2000). Addiction and personality. L’Encéphale, 26(1), 68-78.
Frey, L. C. (2023). Epilepsy. In I. Khazan, F. Shaffer, D. Moss, R. Lyle, & S. Rosenthal (Eds.), Evidence-based practice in biofeedback and neurofeedback (4th ed.). Association for Applied Psychophysiology and Biofeedback.
Geddes-Klein, D. M., Schiffman, K. B., & Meaney, D. F. (2006). Mechanisms and consequences of neuronal stretch injury in vitro differ with the model of trauma. Journal of Neurotrauma, 23(2), 193-204. https://doi.org/10.1089/neu.2006.23.193
Gevensleben, H., Holl, B., Albrecht, B., Schlamp, D., Kratz, O., Studer, P., Rothenberger, A., Moll, G. H., & Heinrich, H. (2010). Neurofeedback training in children with ADHD: 6-month follow-up of a randomised controlled trial. European Child & Adolescent Psychiatry, 19(9), 715-724. https://doi.org/10.1007/s00787-010-0109-5
Gevensleben, H., Holl, B., Albrecht, B., Vogel, C., Schlamp, D., Kratz, O., Studer, P., Rothenberger, A., Moll, G. H., & Heinrich, H. (2009). Is neurofeedback an efficacious treatment for ADHD? A randomised controlled clinical trial. Journal of Child Psychology and Psychiatry, 50(7), 780-789. https://doi.org/10.1111/j.1469-7610.2008.02033.x
Gilbody, S., Lewis, S., & Lightfoot, T. (2007). Methylenetetrahydrofolate reductase (MTHFR) genetic polymorphisms and psychiatric disorders: A HuGE review. American Journal of Epidemiology, 165(1), 1-13. https://doi.org/10.1093/aje/kwj347
Gloss, D., Varma, J. K., Pringsheim, T., & Nuwer, M. R. (2016). Practice advisory: The utility of EEG theta/beta power ratio in ADHD diagnosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology, 87(22), 2375-2379. https://doi.org/10.1212/WNL.0000000000003265
Goessl, V. C., Curtiss, J. E., & Hofmann, S. G. (2017). The effect of heart rate variability biofeedback training on stress and anxiety: A meta-analysis. Psychological Medicine, 47(15), 2578-2586.
Goldstein, R. B., Smith, S. M., Chou, S. P., Saha, T. D., Jung, J., Zhang, H., Pickering, R. P., Ruan, W. J., Huang, B., & Grant, B. F. (2016). The epidemiology of DSM-5 posttraumatic stress disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Social Psychiatry and Psychiatric Epidemiology, 51(8), 1137-1148. https://doi.org/10.1007/s00127-016-1208-5
Groom, M. J., Cahill, J. D., Bates, A. T., Jackson, G. M., Calton, T. G., Liddle, P. F., & Hollis, C. (2010). Electrophysiological indices of abnormal error-processing in adolescents with attention deficit hyperactivity disorder. Journal of Child Psychology and Psychiatry, 51(1), 66-76. https://doi.org/10.1111/j.1469-7610.2009.02128.x
Häger, L., Åsberg Johnels, J., Kropotov, J., Weidle, B., Hollup, S., Zehentbauer, P., Gillberg, C., Billstedt, E., & Ogrim, G. (2021). Biomarker support for ADHD diagnosis based on event related potentials and scores from an attention test. Psychiatry Research, 300, 113879. https://doi.org/10.1016/j.psychres.2021.113879
Hamburg, M. A., & Collins, F. S. (2010). The path to personalized medicine. New England Journal of Medicine, 363(4), 301-304. https://doi.org/10.1056/NEJMp1006304
Hasin, D. S., Sarvet, A. L., Meyers, J. L., Saha, T. D., Ruan, W. J., Stohl, M., & Grant, B. F. (2018). Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry, 75(4), 336–346. https://doi.org/10.1001/jamapsychiatry.2017.4602
Hoepner, C. T., McIntyre, R. S., & Papakostas, G. I. (2021). Impact of supplementation and nutritional interventions on pathogenic processes of mood disorders: A review of the evidence. Nutrients, 13(3), 767. https://doi.org/10.3390/nu13030767
Jaffe, J. H. (1980). Drug addiction and drug abuse. In A. G. Gilman, L. S. Goodman, & A. Gilman (Eds.), Goodman and Gilman’s the pharmacological basis of therapeutics. Macmillan.
Jain, R., Manning, S., & Cutler, A. J. (2019). Good, better, best: Clinical scenarios for the use of L-methylfolate in patients with MDD. CNS Spectrums, 25(6), 750-764. https://doi.org/10.1017/S1092852919001469
Kaiser, A., Aggensteiner, P.-M., Baumeister, S., Holz, N., Banaschewski, T., & Brandeis, D. (2020). Earlier versus later cognitive event-related potentials (ERPs) in attention-deficit/hyperactivity disorder (ADHD): A meta-analysis. Neuroscience & Biobehavioral Reviews, 112, 117-134. https://doi.org/10.1016/j.neubiorev.2020.01.019
Kaźmierczak-Mytkowska, A., Butwicka, A., Lucci, K., Wolańczyk, T., & Bryńska, A. (2022). The functioning of families of teens with attention deficit hyperactivity disorder and oppositional defiant disorder. Psychiatria Polska, 56(4), 889-902. https://doi.org/10.12740/PP/OnlineFirst/128372
Keller, I. (2001). Neurofeedback therapy of attention deficits in patients with traumatic brain injury. Journal of Neurotherapy, 5(1-2), 19-32. https://doi.org/10.1300/J184v05n01_03
Keller, I., Hülsdunk, A., & Müller, F. (2015). The influence of neurofeedback training on physiological arousal and attention in three patients in the state of unresponsive wakefulness. Applied Psychophysiology and Biofeedback, 40(4), 349–356. https://doi.org/10.1007/s10484-015-9296-7
Kerson, C., Lubar, J., deBeus, R., Pan, X., Rice, R., Allen, T., Yazbeck, M., Sah, S., Dhawan, Y., Zong, W., Roley-Roberts, M. E., & Arnold, L. E. (2023). EEG connectivity in ADHD compared to a normative database: A cohort analysis of 120 subjects from the ICAN study. Applied Psychophysiology and Biofeedback, 48(2), 191-206. https://doi.org/10.1007/s10484-022-09569-9
Kim, R. J., & Becker, R. C. (2003). Association between factor V Leiden, prothrombin G20210A, and methylenetetrahydrofolate reductase C677T mutations and events of the arterial circulatory system: A meta-analysis of published studies. American Heart Journal, 146(6), 948-957. https://doi.org/10.1016/S0002-8703(03)00519-2
Kobau, R., Luncheon, C., & Greenlund, K. (2023). Active epilepsy prevalence among U.S. adults. Epilepsy & Behavior, 142, 109180.
Kobau, R., Luncheon, C., & Greenlund, K. J. (2024). About 1.5 million community-dwelling US adults with active epilepsy reported uncontrolled seizures. Epilepsy & Behavior, 157, 109852.
Koberda, J. L. (2015). LORETA z-score neurofeedback effectiveness in rehabilitation of patients suffering from traumatic brain injury. Journal of Neurology and Neurobiology, 1(4). https://doi.org/10.16966/2379-7150.113
Koob, G. F., & Volkow, N. D. (2010). Neurocircuitry of addiction. Neuropsychopharmacology, 35(1), 217-238. https://doi.org/10.1038/npp.2009.110
Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010). Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136(5), 768-821. https://doi.org/10.1037/a0020327
Krepel, N., van Dijk, H., Sack, A. T., Swatzyna, R. J., & Arns, M. (2021). To spindle or not to spindle: A replication study into spindling excessive beta as a transdiagnostic EEG feature associated with impulse control. Biological Psychology, 165, 108188. https://doi.org/10.1016/j.biopsycho.2021.108188
Kung, P.-H., Davey, C. G., Harrison, B. J., Jamieson, A. J., Felmingham, K. L., & Steward, T. (2023). Frontoamygdalar effective connectivity in youth depression and treatment response. Biological Psychiatry, 94(12), 959-968. https://doi.org/10.1016/j.biopsych.2023.06.009
Lefler, E. K., Flory, K., Canu, W. H., Willcutt, E. G., & Hartung, C. M. (2021). Unique considerations in the assessment of ADHD in college students. Journal of Clinical and Experimental Neuropsychology, 43(4), 352-369. https://doi.org/10.1080/13803395.2021.1936462
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., Sgobba, P., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Applied Psychophysiology and Biofeedback, 45(3), 109-129.
Lehrer, P. M., & Gevirtz, R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 5, Article 756. https://doi.org/10.3389/fpsyg.2014.00756
Lenartowicz, A., Mazaheri, A., Jensen, O., & Loo, S. K. (2018). Aberrant modulation of brain oscillatory activity and attentional impairment in attention-deficit/hyperactivity disorder. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 3(1), 19-29. https://doi.org/10.1016/j.bpsc.2017.09.009
Levine, B., Kovacevic, N., Nica, E. I., Cheung, G., Gao, F., Schwartz, M. L., & Black, S. E. (2008). The Toronto traumatic brain injury study: Injury severity and quantified MRI. Neurology, 70(10), 771-778. https://doi.org/10.1212/01.wnl.0000304108.32283.aa
Lin, H.-Y., Tseng, W.-Y. I., Lai, M.-C., Matsuo, K., & Gau, S. S.-F. (2015). Altered resting-state frontoparietal control network in children with attention-deficit/hyperactivity disorder. Journal of the International Neuropsychological Society, 21(4), 271-284. https://doi.org/10.1017/S135561771500020X
Louthrenoo, O., Boonchooduang, N., Likhitweerawong, N., Charoenkwan, K., & Srisurapanont, M. (2022). The effects of neurofeedback on executive functioning in children with ADHD: A meta-analysis. Journal of Attention Disorders, 26(7), 976-984. https://doi.org/10.1177/10870547211045738
Lubar, J. F., & Shouse, M. N. (1976). EEG and behavioral changes in a hyperkinetic child concurrent with training of the sensorimotor rhythm (SMR): A preliminary report. Biofeedback and Self-Regulation, 1(3), 293-306. https://doi.org/10.1007/BF01001170
Lubar, J. F. (1995). Neurofeedback for the management of ADHD. In M. S. Schwartz (Ed.), Biofeedback: A practitioner's guide (2nd ed.). Guilford Press.
Lubar, J. F., Swartwood, M. O., Swartwood, J. N., & O'Donnell, P. H. (1995). Evaluation of the effectiveness of EEG neurofeedback training for ADHD in a clinical setting as measured by changes in T.O.V.A. scores, behavioral ratings, and WISC-R performance. Biofeedback and Self-Regulation, 20(1), 83–99. https://doi.org/10.1007/BF01712768
Lubar, J. O., & Lubar, J. F. (1984). Electroencephalographic biofeedback of SMR and beta for treatment of attention deficit disorders in a clinical setting. Biofeedback and Self-Regulation, 9(1), 1-23. https://doi.org/10.1007/BF00998842
Lucock, M. (2000). Folic acid: Nutritional biochemistry, molecular biology, and role in disease processes. Molecular Genetics and Metabolism, 71(1-2), 121-138. https://doi.org/10.1006/mgme.2000.3027
Lynch, C. J., Elbau, I. G., Ng, T., Ayaz, A., Zhu, S., Wolk, D., Manfredi, N., Johnson, M., Chang, M., Chou, J., Summerville, I., Ho, C., Lueckel, M., Bukhari, H., Buchanan, D., Victoria, L. W., Solomonov, N., Goldwaser, E., Moia, S., Caballero-Gaudes, C., … Liston, C. (2024). Frontostriatal salience network expansion in individuals in depression. Nature, 633(8030), 624-633. https://doi.org/10.1038/s41586-024-07805-2
Maruf, A. A., Poweleit, E. A., Brown, L. C., Strawn, J. R., & Bousman, C. A. (2021). Systematic review and meta-analysis of L-methylfolate augmentation in depressive disorders. Pharmacopsychiatry. https://doi.org/10.1055/a-1681-2047
Miller, A. P., Baranger, D. A. A., Paul, S. E., Garavan, H., Mackey, S., Tapert, S. F., LeBlanc, K. H., Agrawal, A., & Bogdan, R. (2024). Neuroanatomical variability and substance use initiation in late childhood and early adolescence. JAMA Network Open, 7(12), e2452027. https://doi.org/10.1001/jamanetworkopen.2024.52027
Monastra, V. J., Monastra, D. M., & George, S. (2002). The effects of stimulant therapy, EEG biofeedback, and parenting style on the primary symptoms of attention-deficit/hyperactivity disorder. Applied Psychophysiology and Biofeedback, 27(4), 231-249.
Murray, A. L., Ribeaud, D., Eisner, M., Murray, G., & McKenzie, K. (2019). Should we subtype ADHD according to the context in which symptoms occur? Criterion validity of recognising context-based ADHD presentations. Child Psychiatry & Human Development, 50, 308-320. https://doi.org/10.1007/s10578-018-0842-4
National Institute of Mental Health. (2023). Any anxiety disorder. Retrieved from https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder
National Research Council. (2011). Toward precision medicine: Building a knowledge network for biomedical research and a new taxonomy of disease. National Academies Press.
Nguyen, T. T., Hathaway, H., Kosciolek, T., Knight, R., & Jeste, D. V. (2021). Gut microbiome in serious mental illnesses: A systematic review and critical evaluation. Schizophrenia Research, 234, 24-40. https://doi.org/10.1016/j.schres.2019.08.026
Pelham, W. E., & Fabiano, G. A. (2008). Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 37(1), 184-214. https://doi.org/10.1080/15374410701818681
Peniston, E. G., & Kulkosky, P. J. (1989). Alpha-theta brainwave training and beta-endorphin levels in alcoholics. Alcoholism: Clinical and Experimental Research, 13(2), 271-279.
Peris, T. S., & Miklowitz, D. J. (2015). Parental expressed emotion and youth psychopathology: New directions for an old construct. Child Psychiatry & Human Development, 46, 863-873. https://doi.org/10.1007/s10578-014-0526-7
Peskind, E. R., Brody, D., Cernak, I., McKee, A., & Ruff, R. L. (2013). Military- and sports-related mild traumatic brain injury: Clinical presentation, management, and long-term consequences. Journal of Clinical Psychiatry, 74(2), 180-188. https://doi.org/10.4088/JCP.12011co1c
Pizzoli, S. F. M., Marzorati, C., Gatti, D., Monzani, D., Mazzocco, K., & Pravettoni, G. (2021). A meta-analysis on heart rate variability biofeedback and depressive symptoms. Scientific Reports, 11, 6650.
Poil, S.-S., Bollmann, S., Ghisleni, C., O'Gorman, R., Klaver, P., Ball, J., Eich-Höchli, D., Brandeis, D., & Michels, L. (2014). Age dependent electroencephalographic changes in attention-deficit/hyperactivity disorder (ADHD). Clinical Neurophysiology, 125(8), 1626-1638. https://doi.org/10.1016/j.clinph.2013.12.118
Polich, G., Gray, S., Tran, D., Morales-Quezada, L., & Glenn, M. (2020). Comparing focused attention meditation to meditation with mobile neurofeedback for persistent symptoms after mild-moderate traumatic brain injury: A pilot study. Brain Injury, 34(10), 1408-1415. https://doi.org/10.1080/02699052.2020.1802781
PracticeWise. (2026). PracticeWise blue menu of evidence-based psychosocial interventions. PracticeWise, LLC. https://www.practicewise.com
Quinn, P. O., & Madhoo, M. (2014). A review of attention-deficit/hyperactivity disorder in women and girls: Uncovering this hidden diagnosis. Primary Care Companion for CNS Disorders, 16(3). https://doi.org/10.4088/PCC.13r01596
Rangaswamy, M., Porjesz, B., Chorlian, D. B., Wang, K., Jones, K. A., Bauer, L. O., Rohrbaugh, J., O’Connor, S. J., Kuperman, S., Reich, T., & Begleiter, H. (2002). Beta power in the EEG of alcoholics. Biological Psychiatry, 52(8), 831-842. https://doi.org/10.1016/S0006-3223(02)01362-8
Ray, J. G., & Laskin, C. A. (1999). Folic acid and homocyst(e)ine metabolic defects and the risk of placental abruption, pre-eclampsia and spontaneous pregnancy loss: A systematic review. Placenta, 20(7), 519-529. https://doi.org/10.1053/plac.1999.0417
Reynolds, E. H. (2002). Folic acid, ageing, depression, and dementia. BMJ, 324(7352), 1512-1515. https://doi.org/10.1136/bmj.324.7352.1512
Roberts, B. W., Walton, K. E., & Bogg, T. (2005). Conscientiousness and health across the life course. Review of General Psychology, 9(2), 156-168. https://doi.org/10.1037/1089-2680.9.2.156
Roffman, J. L., Petruzzi, L. J., Tanner, A. S., Brown, H. E., Eryilmaz, H., Ho, N. F., Giegold, M., Silverstein, N. J., Bottiglieri, T., Manoach, D. S., Smoller, J. W., Henderson, D. C., & Goff, D. C. (2017). Biochemical, physiological and clinical effects of L-methylfolate in schizophrenia: A randomized controlled trial. Molecular Psychiatry, 23(2), 316-322. https://doi.org/10.1038/mp.2017.41
Roffman, J. L., Weiss, A. P., Purcell, S., Caffalette, C. A., Freudenreich, O., Henderson, D. C., Bottiglieri, T., Wong, D. H., Halsted, C. H., & Goff, D. C. (2008). Contribution of methylenetetrahydrofolate reductase (MTHFR) polymorphisms to negative symptoms in schizophrenia. Biological Psychiatry, 63(1), 42-48. https://doi.org/10.1016/j.biopsych.2006.12.017
Rosenfeld, J. V., McFarlane, A. C., Bragge, P., Armonda, R. A., Grimes, J. B., & Ling, G. S. (2013). Blast-related traumatic brain injury. The Lancet Neurology, 12(9), 882-893. https://doi.org/10.1016/S1474-4422(13)70161-3
Rossiter, T. R., & La Vaque, T. J. (1995). A comparison of EEG biofeedback and psychostimulants in treating attention deficit/hyperactivity disorders. Journal of Neurotherapy, 1(1), 48-59. https://doi.org/10.1300/J184v01n01_07
Sakuma, K., Matsunaga, S., Nomura, I., Okuya, M., Kishi, T., & Iwata, N. (2018). Folic acid/methylfolate for the treatment of psychopathology in schizophrenia: A systematic review and meta-analysis. Psychopharmacology, 235(8), 2303-2314. https://doi.org/10.1007/s00213-018-4926-4
SAMHSA. (2023). Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health.
Sanader Vukadinovic, B. (2025). Neurofeedback in substance and non substance-related addictions: A mini review of current evidence and future directions. Frontiers in Psychiatry, 16, Article 1716390. https://doi.org/10.3389/fpsyt.2025.1716390
Santhosh-Kumar, C. R., Deutsch, J. C., Ryder, J. W., & Kolhouse, J. F. (1997). Unpredictable intra-individual variations in serum homocysteine levels on folic acid supplementation. European Journal of Clinical Nutrition, 51(3), 188-192. https://doi.org/10.1038/sj.ejcn.1600385
Schimmelpfennig, J., Topczewski, J., Zajkowski, W., & Jankowiak-Siuda, K. (2023). The role of the salience network in cognitive and affective deficits. Frontiers in Human Neuroscience, 17, 1133367. https://doi.org/10.3389/fnhum.2023.1133367
Scott, W. C., Kaiser, D., Othmer, S., & Sideroff, S. I. (2005). Effects of an EEG biofeedback protocol on a mixed substance abusing population. American Journal of Drug and Alcohol Abuse, 31(3), 455-469.
Seppä, S., Huikari, S., Korhonen, M., Nordström, T., Hurtig, T., & Halt, A.-H. (2024). Associations of symptoms of ADHD and oppositional defiant disorder (ODD) in adolescence with occupational outcomes and incomes in adulthood. Journal of Attention Disorders, 28(10), 1392-1405. https://doi.org/10.1177/10870547241259329
Shaffer, F., & Mannion, M. (2016). Tinnitus. In G. Tan, F. Shaffer, R. Lyle, & I. Teo (Eds.), Evidence-based practice in biofeedback and neurofeedback (3rd ed.). Association for Applied Psychophysiology and Biofeedback.
Shouse, M. N., & Lubar, J. F. (1979). Operant conditioning of EEG rhythms and Ritalin in the treatment of hyperkinesis. Biofeedback and Self-Regulation, 4(4), 299–312. https://doi.org/10.1007/BF00998960
Silk, T. J., Malpas, C. B., Beare, R., Efron, D., Anderson, V., Hazell, P., Jongeling, B., Nicholson, J. M., & Sciberras, E. (2019). A network analysis approach to ADHD symptoms: More than the sum of its parts. PLOS ONE, 14(1), e0211053. https://doi.org/10.1371/journal.pone.0211053
Sokhadze, T. M., Cannon, R. L., & Trudeau, D. L. (2008). EEG biofeedback as a treatment for substance use disorders: Review, rating of efficacy, and recommendations for further research. Applied Psychophysiology and Biofeedback, 33(1), 1-28.
Solanto, M. V. (2002). Dopamine dysfunction in AD/HD: Integrating clinical and basic neuroscience research. Behavioural Brain Research, 130(1-2), 65-71. https://doi.org/10.1016/S0166-4328(01)00431-4
Soler-Gutiérrez, A.-M., Pérez-González, J.-C., & Mayas, J. (2023). Evidence of emotion dysregulation as a core symptom of adult ADHD: A systematic review. PLOS ONE, 18(1), e0280131. https://doi.org/10.1371/journal.pone.0280131
Spencer, T. J., Biederman, J., & Mick, E. (2007). ADHD: Diagnosis, lifespan, comorbidities, and neurobiology. Ambulatory Pediatrics, 7, 73-81.
Sterman, M. B., & Egner, T. (2006). Foundation and practice of neurofeedback for the treatment of epilepsy. Applied Psychophysiology and Biofeedback, 31(1), 21-35.
Sterman, M. B. (2000). Basic concepts and clinical findings in the treatment of seizure disorders with EEG operant conditioning. Clinical Electroencephalography, 31(1), 45-55.
Sterman, M. B. (2010). Biofeedback in the treatment of epilepsy. Cleveland Clinic Journal of Medicine, 77(Suppl. 3), S60–S67. https://doi.org/10.3949/ccjm.77.s3.11
Swanson, J. M., Arnold, L. E., Molina, B. S. G., Sibley, M. H., Hechtman, L. T., Hinshaw, S. P., & Wigal, T. (2017). Young adult outcomes in the follow-up of the multimodal treatment study of attention-deficit/hyperactivity disorder: Symptom persistence, source discrepancy, and height suppression. Journal of Child Psychology and Psychiatry, 58(6), 663-678. https://doi.org/10.1111/jcpp.12684
Swatzyna, R. J., Arns, M., Tarnow, J. D., Turner, R. P., Barr, E., MacInerney, E. K., Hoffman, A. M., & Boutros, N. N. (2020). Isolated epileptiform activity in children and adolescents: Prevalence, relevance, and implications for treatment. European Child & Adolescent Psychiatry. https://doi.org/10.1007/s00787-020-01597-2
Swatzyna, R. J., Kozlowski, G. P., & Tarnow, J. D. (2015). Pharmaco-EEG: A study of individualized medicine in clinical practice. Clinical EEG and Neuroscience, 46(3), 192-196. https://doi.org/10.1177/1550059414556120
Swatzyna, R. J., Morrow, L. M., Collins, D. M., Barr, E. A., Roark, A. J., & Turner, R. P. (2024). Evidentiary significance of routine EEG in refractory cases: A paradigm shift in psychiatry. Clinical EEG and Neuroscience. https://doi.org/10.1177/15500594231221313
Sylvia, L. G., Peters, A. T., Deckersbach, T., & Nierenberg, A. A. (2012). Nutrient-based therapies for bipolar disorder: A systematic review. Psychotherapy and Psychosomatics, 82(1), 10-19. https://doi.org/10.1159/000341309
Tan, G., Thornby, J., Hammond, D. C., Strehl, U., Canady, B., Arnemann, K., & Kaiser, D. A. (2009). Meta-analysis of EEG biofeedback in treating epilepsy. Clinical EEG and Neuroscience, 40(3), 173–179. https://doi.org/10.1177/155005940904000310
Terracciano, A., & Costa, P. T., Jr. (2004). Smoking and the Five-Factor Model of personality. Addiction, 99(4), 472-481. https://doi.org/10.1111/j.1360-0443.2004.00687.x
Thatcher, R. W., North, D. M., & Biver, C. J. (2005). EEG and intelligence: Relations between EEG coherence, EEG phase delay and power. Clinical Neurophysiology, 116(9), 2129-2141. https://doi.org/10.1016/j.clinph.2005.04.026
Thatcher, R. W., Walker, R. A., Gerson, I., & Geisler, F. H. (1989). EEG discriminant analyses of mild head trauma. Electroencephalography and Clinical Neurophysiology, 73(2), 94-106. https://doi.org/10.1016/0013-4694(89)90188-0
Thompson, L., & Thompson, M. (1998). Neurofeedback combined with training in metacognitive strategies: Effectiveness in students with ADD. Applied Psychophysiology and Biofeedback, 23(4), 243-263.
Tough, P. (2025). Have we been thinking about ADHD all wrong? The New York Times Magazine.
Tripp, G., & Wickens, J. R. (2024). The dopamine hypothesis for ADHD: An evaluation of evidence. Frontiers in Psychiatry, 15, 1492126. https://doi.org/10.3389/fpsyt.2024.1492126
Trivedi, C., Reddy, P., Rizvi, A., Husain, K., Brown, K., Mansuri, Z., Nabi, M., & Jain, S. (2024). Traumatic brain injury and risk of schizophrenia and other non-mood psychotic disorders: Findings from a large inpatient database in the United States. Schizophrenia Bulletin, 50(4), 924-930. https://doi.org/10.1093/schbul/sbae047
Van Doren, J., Arns, M., Heinrich, H., Vollebregt, M. A., Strehl, U., & Loo, S. K. (2019). Sustained effects of neurofeedback in ADHD: A systematic review and meta-analysis. European Child & Adolescent Psychiatry, 28(3), 293-305. https://doi.org/10.1007/s00787-018-1121-4
U.S. Department of Veterans Affairs. (2023). Veterans Benefits Administration annual benefits report, fiscal year 2023. https://www.benefits.va.gov/REPORTS/abr/
Verdejo-García, A., & Pérez-García, M. (2007). Profile of executive deficits in cocaine and heroin polysubstance users: Common and differential effects on separate executive components. Psychopharmacology, 190(4), 517-530. https://doi.org/10.1007/s00213-006-0632-8
Walker, J. E., Norman, C. A., & Weber, R. K. (2002). Impact of qEEG-guided coherence training for patients with a mild closed head injury. Journal of Neurotherapy, 6(2), 31-43. https://doi.org/10.1300/J184v06n02_05
Waltzman, D., Black, L. I., Daugherty, J., Peterson, A. B., & Zablotsky, B. (2025). Prevalence of traumatic brain injury among adults and children. Annals of Epidemiology, 103, 40-47.
Wang, T.-S., Wang, S.-S., Wang, C.-L., & Wong, S.-B. (2024). Theta/beta ratio in EEG correlated with attentional capacity assessed by Conners Continuous Performance Test in children with ADHD. Frontiers in Psychiatry, 14, 1305397.
Wilcken, B., Bamforth, F., Li, Z., Zhu, H., Ritvanen, A., & Czeizel, A. E. (2003). Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): Findings from over 7,000 newborns from 16 areas worldwide. Journal of Medical Genetics, 40(8), 619-625. https://doi.org/10.1136/jmg.40.8.619
Wolraich, M. L., Hagan, J. F., Jr., Allan, C., Chan, E., Davison, D., Earls, M., Evans, S. W., Flinn, S. K., Froehlich, T., Frost, J., Holbrook, J. R., Lehmann, C. U., Lessin, H. R., Okechukwu, K., Pierce, K. L., Winner, J. D., & Zurhellen, W. (2019). Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 144(4), e20192528. https://doi.org/10.1542/peds.2019-2528
World Health Organization. (2024). Epilepsy fact sheet. Retrieved from https://www.who.int/news-room/fact-sheets/detail/epilepsy
Wu, Y.-L., Ding, X.-X., Sun, Y.-H., Yang, H.-Y., Chen, J., Zhao, X., Jiang, Y.-H., Lv, X.-L., & Wu, Z.-Q. (2013). Association between MTHFR C677T polymorphism and depression: An updated meta-analysis of 26 studies. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 46, 78-85. https://doi.org/10.1016/j.pnpbp.2013.06.015
Xuan, C., Li, H., Zhao, J.-X., Wang, H.-W., Wang, Y., Ning, C.-P., Liu, Z., Zhang, B.-B., He, G.-W., & Lun, L.-M. (2014). Association between MTHFR polymorphisms and congenital heart disease: A meta-analysis based on 9,329 cases and 15,076 controls. Scientific Reports, 4, 7311. https://doi.org/10.1038/srep07311
Yap, Y. C., King, A. E., Guijt, R. M., Jiang, T., Blizzard, C. A., Breadmore, M. C., & Dickson, T. C. (2017). Mild and repetitive very mild axonal stretch injury triggers cytoskeletal mislocalization and growth cone collapse. PLOS ONE, 12(5), e0176997. https://doi.org/10.1371/journal.pone.0176997
Zhong, X., Yuan, X., Dai, Y., Zhang, X., & Jiang, C. (2025). Neurofeedback training for executive function in ADHD children: A systematic review and meta-analysis. Scientific Reports, 15, 28148. https://doi.org/10.1038/s41598-025-94242-4
Zilberman, N., Yadid, G., Efrati, Y., Neumark, Y., & Rassovsky, Y. (2018). Personality profiles of substance and behavioral addictions. Addictive Behaviors, 82, 174-181. https://doi.org/10.1016/j.addbeh.2018.03.007
Zuckerman, M. (2007). Sensation seeking and risky behavior. American Psychological Association. https://doi.org/10.1037/11555-000
Return to Top