Aseptic Techniques
What You Will Learn in This Chapter
How do you keep a noninvasive procedure from becoming a route of infection? This unit prepares you to prevent infection transmission in neurofeedback and biofeedback practice. You will learn how to trace an infection risk through the six links of the chain of transmission, screen clients and staff, perform proper hand hygiene, select personal protective equipment by risk rather than by habit, control the physical environment, put administrative expectations in place, disinfect and sterilize equipment, prevent cross-contamination, and follow best practices for skin preparation, electrode cleaning, and sensor placement.
You will also learn to think like an investigator who treats every surface as a potential transmission vector, and to use the Spaulding classification system to match each device to the right level of disinfection or sterilization. By the end of this unit, you will be able to apply these infection mitigation strategies confidently, whether you work in a hospital, VA facility, private clinic, or performance training center.
BCIA Blueprint Coverage: This unit addresses III. Instrumentation and Electronics - D. Aseptic Techniques.
A neurofeedback provider applied reusable EEG sensors to the scalp of a high school wrestler with skin lesions. When questioned, the wrestler explained that the lesions were due to mat abrasion and that all the wrestlers on his team had them. Because the clinician did not disinfect the sensors between sessions, several clients developed MRSA infections and sued for malpractice. This vignette was adapted from Moss (2013).

This opening scenario shows why aseptic technique is not merely a best practice—it is a clinical and legal imperative. Neurofeedback providers may underestimate their infection transmission risk because the procedure is noninvasive, yet everyday contact points like handshakes, reclining chairs, cables, and sensors can easily transfer infectious organisms between clients. The risk escalates when over-abrasion exposes sensors to blood, which the Spaulding classification system designates a semi-critical risk, or when equipment enters sterile tissues or the vascular system, a critical risk. This process, in which a shared object spreads pathogens to multiple individuals, is called common vehicle transmission—a concept that will reappear throughout this unit.
The word aseptic means free from disease-causing microorganisms such as harmful bacteria, viruses, and fungi. It is worth separating that idea from two neighboring ones that are often used interchangeably in conversation. Sterile is a stricter standard, meaning free of all living microorganisms rather than merely the harmful ones. Antiseptic, by contrast, describes a substance applied to living tissue to destroy microorganisms or inhibit their spread—the alcohol you wipe on a scalp site is an antiseptic, not a sterilant. As the Spaulding classification presented later in this unit makes clear, different procedures, client presentations, and circumstances call for different degrees of cleanliness along a range that runs from an aseptic state to a fully sterilized one, and each point on that range has its own matching set of steps.
In clinical practice, aseptic techniques form a systematic barrier between your clients and these invisible threats. As Hagedorn (2014) summarizes, effective infection risk mitigation rests on three pillars: handwashing and drying, disinfection of all surfaces clients will contact, and disinfection or sterilization of sensors and cables. The sections that follow examine each pillar in detail so you can apply them in your own practice setting.
BCIA Blueprint Coverage
This unit covers III. Instrumentation and Electronics - D. Aseptic Techniques.

The sections below address Assumptions and Principles, the Chain of Transmission, the Forensic Mindset, Best Practices for Routine Client Care, Risk Assessment Screening, Hand Cleaning, Personal Protective Equipment, Equipment Disinfection and Sterilization, Control of the Environment, Administrative Controls, Cross-Contamination, Electrode Cleaning, and Best Practices.
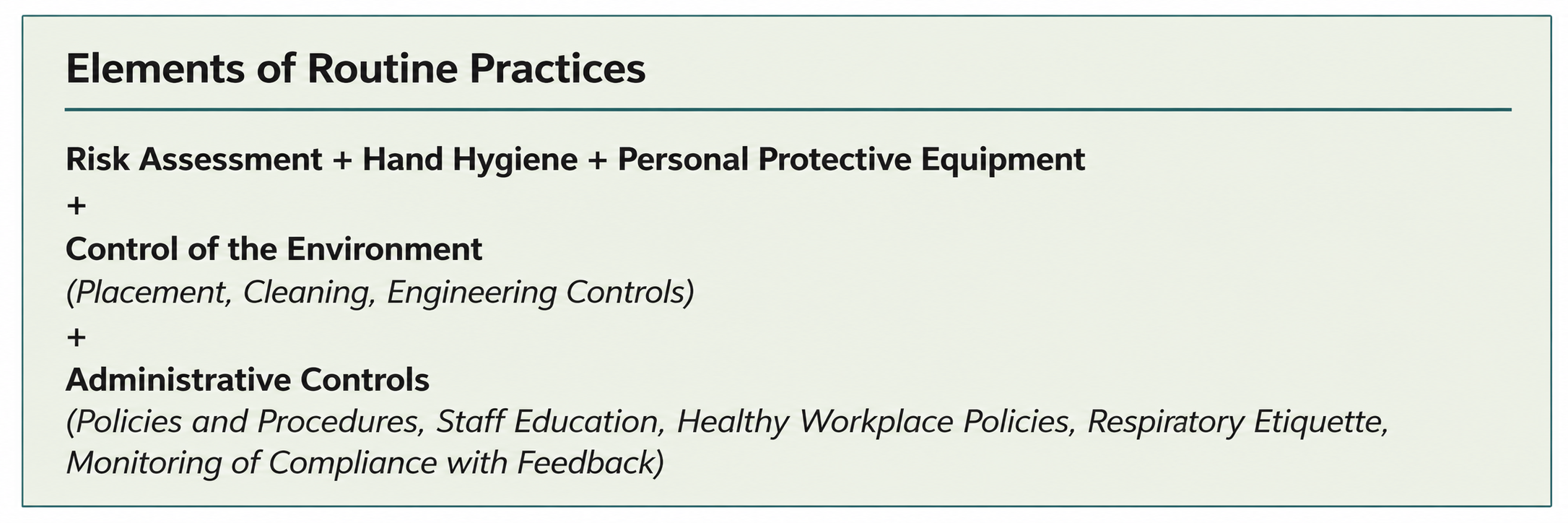
Everything that follows applies to neurofeedback (NFB, or EEG biofeedback) and quantitative EEG (qEEG) assessment wherever you conduct it—a professional office, a client's home, a rehabilitation facility, a school, or a performance training center. What changes from setting to setting is not the underlying principle but the level of precaution the situation demands. In some settings you are more likely to work with clients whose condition carries a higher risk of transmitting infection. Most NFB practice requires only routine practices, the infection prevention and control measures used with every client during every contact regardless of known diagnosis. A smaller number of situations call for additional precautions, the contact, droplet, and airborne measures layered on top of routine practices for particular pathogens or clinical presentations. The most useful reference for deciding which of the two a given situation requires, and for knowing what the additional measures involve, is the Ontario Agency for Health Protection and Promotion (Public Health Ontario) and its Provincial Infectious Diseases Advisory Committee (2025), whose routine practices and additional precautions guidance is freely available and unusually practical.
Assumptions and Principles
This section describes the conditions that have to be in place before any specific technique can work. Public Health Ontario (2025) frames its guidance around a set of assumptions about the setting itself, and those assumptions translate directly to neurofeedback practice.
The first is that resources are actually devoted to the work. Infection prevention and control (IPAC) is the coordinated set of policies, practices, and physical measures a setting uses to prevent the transmission of microorganisms, and it costs something—supplies, time, and attention to housekeeping in the spaces for which you are responsible. A provider who intends to practice aseptically but budgets nothing for it will fall back on improvisation at exactly the moments that matter. The second assumption is that education is ongoing rather than one-time. New and existing staff need regular review of IPAC methods so that practice stays consistent across people and across months, and the effectiveness of those practices deserves periodic assessment rather than assumption. Habits drift, and drift is invisible without a scheduled look.
The third assumption is that you are not doing this alone. Collaboration with other professionals—and, when circumstances warrant, with occupational health and public health staff—produces better decisions than solitary judgment, particularly in the ambiguous cases. That leads to the fourth: access to IPAC information, advice, and guidance should be arranged before you need it, so that a question arising on a Tuesday afternoon has somewhere to go. The fifth is vigilance. Health advisories are issued for a reason, and a practice that monitors and responds to them will adjust before a problem arrives rather than after. The sixth ties the others together: sustained IPAC depends on the support of senior staff and on the resources to implement what the policies describe. In a solo practice, you are the senior staff, and the commitment has to be deliberate.
Chain of Transmission
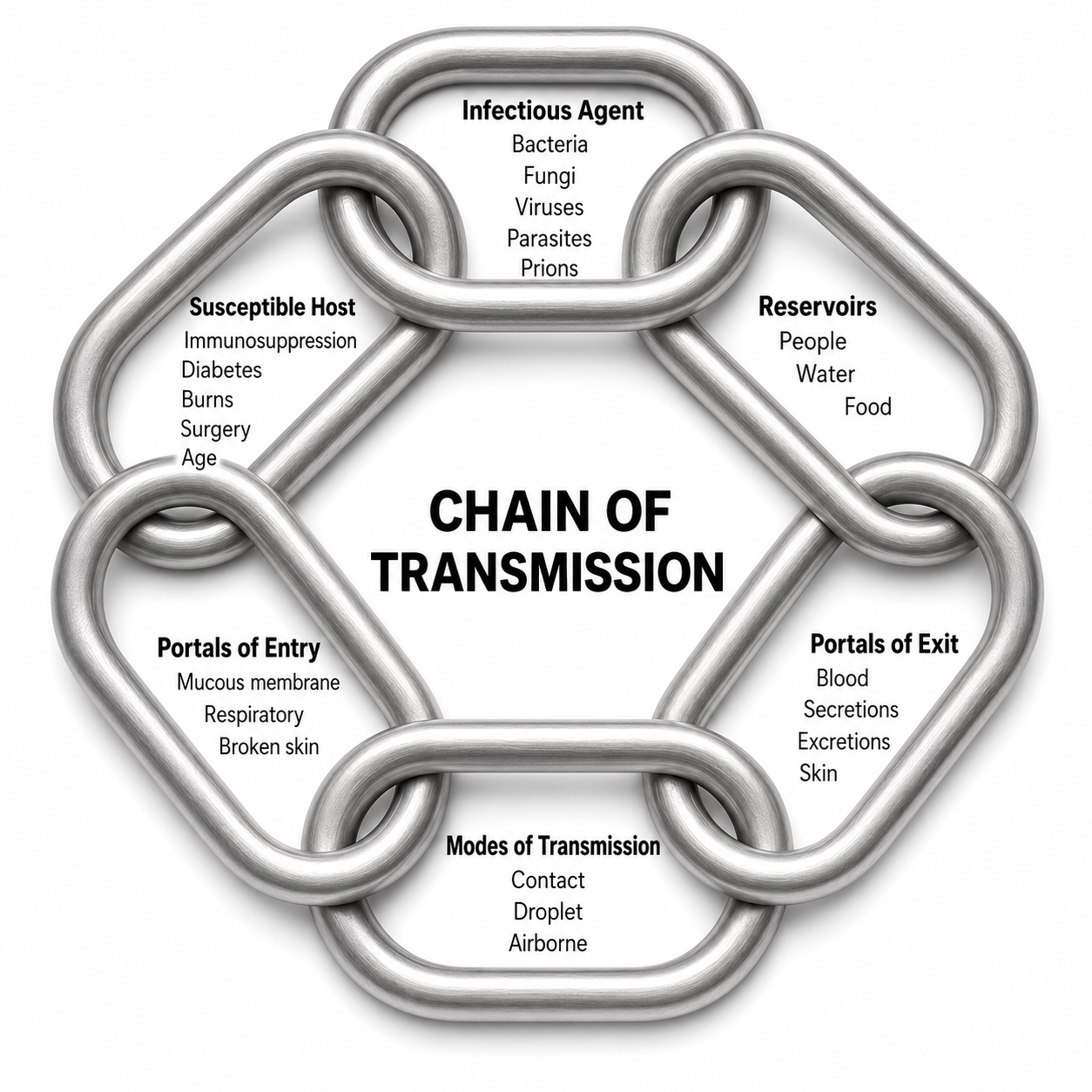
This section gives you a diagnostic framework for thinking about any infection risk you encounter. Several factors govern whether an infectious microorganism actually reaches a new person: the characteristics of the microorganism itself, the source it comes from, the environment it passes through, and the susceptibility of the person who receives it. Public Health Ontario (2025) organizes these factors into a chain, and the crucial property of that chain is that all six of its links must be present for transmission to occur.
The chain of transmission begins with an infectious agent—the bacterium, virus, or fungus capable of causing disease. That agent must live somewhere, and the place it lives and multiplies is the reservoir, which may be a person, a piece of equipment, water, food, or a surface. To reach anyone else it must leave the reservoir through a portal of exit such as the respiratory tract, broken skin, or a bodily fluid. It then travels by a mode of transmission—contact, droplet, or airborne—before arriving at a portal of entry, the route by which it gets into the next person, whether mucous membranes, non-intact skin, or the airway. Finally it needs a susceptible host, a person whose immune status, age, or underlying condition leaves them vulnerable to that particular agent.
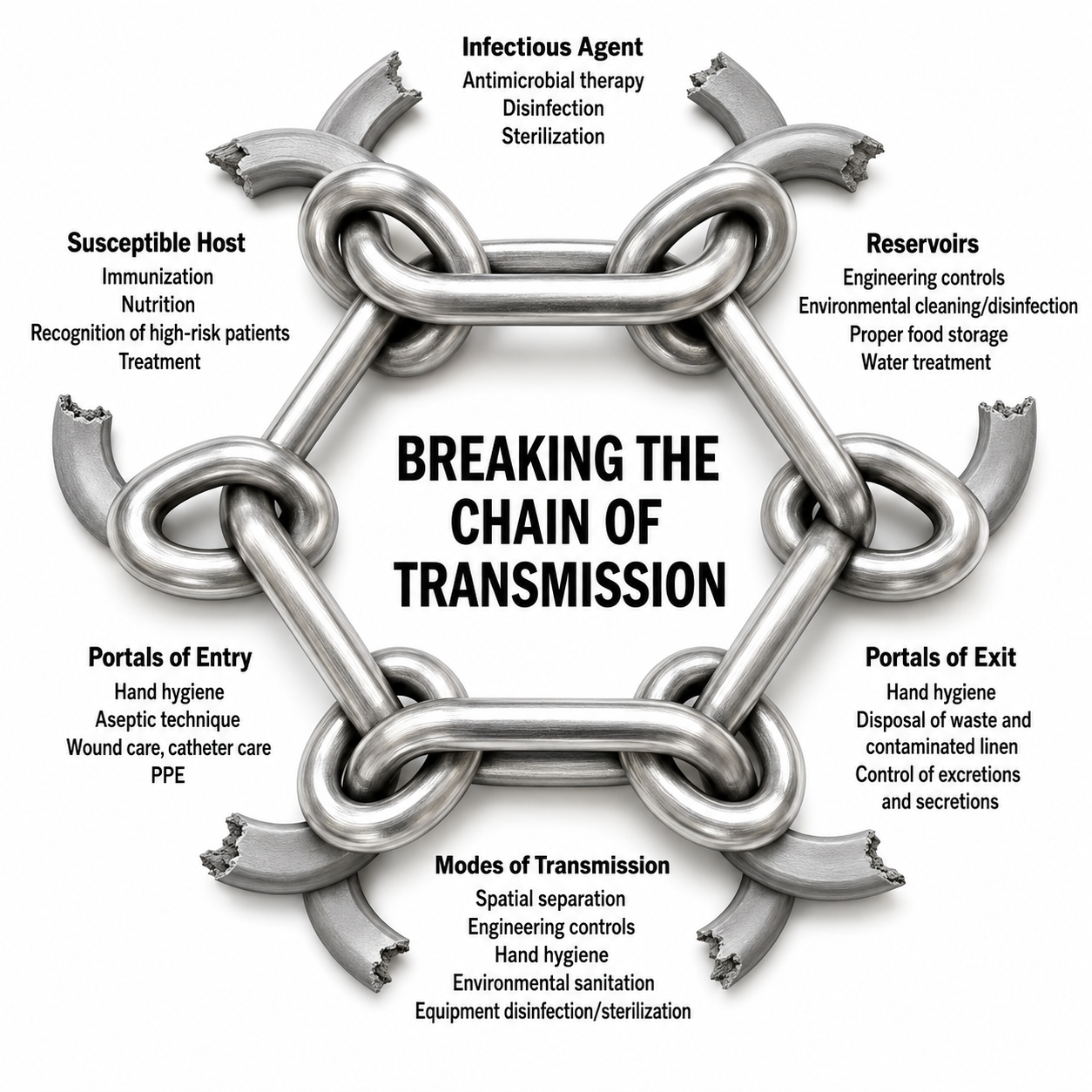
The practical value of the chain is that breaking any single link stops transmission entirely, which means you have six independent opportunities rather than one. Eliminating or inactivating the infectious agent breaks the first link, and preventing an agent from establishing itself in a person, in water, or on equipment denies it a reservoir. Containing portals of exit with good hand hygiene, prompt waste disposal, and control of bodily fluids blocks the agent’s route out. Barriers and safe practices—hand hygiene, disinfection, and environmental sanitation—interrupt the mode of transmission. Hand hygiene and aseptic technique close portals of entry. And screening that recognizes high-risk clients addresses the susceptible host. Nearly every specific recommendation in this unit is an attack on one of these six links, and it is worth pausing over any new procedure you adopt to ask which link it breaks.
Public Health Ontario (2025) grounds routine practices in a deliberately pessimistic assumption: every client may be carrying potentially infectious microorganisms, including clients who show no symptoms and report none. Routine practices are therefore used with all clients rather than reserved for those known to be infectious, because, as the guidance puts it, “the consistent and appropriate use of Routine Practices by all health care providers with all patient encounters will lessen microbial transmission in the health care setting and reduce the need for Additional Precautions” (Section 1.B). In short, doing the ordinary things well and universally is what keeps the extraordinary measures rare. When they are needed, additional precautions add barriers such as face shields and other personal protective equipment along with more stringent equipment disinfection and sterilization.
Forensic Mindset
This section introduces a practical mindset for maintaining hygiene throughout every neurofeedback session. Moss and colleagues (2019) capture it best by encouraging clinicians to adopt a forensic perspective:
Think like a crime scene investigative agent. When you're working with a client, it is easy to touch the client, equipment, and workspace surfaces without awareness. If the client has a skin condition or even a cold, any object the practitioner touches in the environment can become a health hazard for the practitioner and for other clients. Restrict touching to a minimum and keep the things you touch in the same area, so they can be cleaned between clients (pp. 338–339).
This forensic mindset is the foundation for every aseptic strategy discussed in this unit. By treating each client and each surface as a potential transmission vector, you cultivate the situational awareness needed to protect yourself, your clients, and your colleagues. Whether you work in a busy hospital EEG lab or a solo private practice, minimizing unnecessary surface contact and clustering the items you touch into cleanable zones will dramatically reduce your infection risk.
Best Practices for Routine Client Care
The sections that follow work through the routine practices Public Health Ontario (2025) recommends for every client contact, translated into the specific circumstances of neurofeedback and qEEG work. Take them as a sequence rather than a menu: screening establishes what the encounter requires, hand hygiene and protective equipment govern how you conduct it, equipment disinfection and sterilization govern what you reuse afterward, and control of the environment and administrative measures decide whether the setting supports the rest.
Risk Assessment Screening
This section covers procedures for identifying potentially infectious individuals as early as possible, before they enter your clinical space and before transmission has any opportunity to occur. It helps to picture a protective screen standing between the outside world and the area where training takes place. Providers and staff put that screen in place, and its purpose is to hold clients and colleagues outside it temporarily, away from the training site, until the risk has been reduced. Screening is your first line of defense because it catches symptoms early, before an ill staff member or client can expose others.
Screening runs in both directions. Staff should monitor their own temperature, respiratory symptoms, and other indicators of illness before leaving for work, and should put the same short symptom checklist to clients before those clients set out for the clinic. When clients arrive, you can take their forehead temperature using a contactless infrared thermometer—a quick, noninvasive check that provides immediate data without requiring physical contact. Treat a normal reading as weak reassurance rather than clearance, because temperature screening misses people who are afebrile or presymptomatic; the symptom questions carry more weight than the number.
A good opening question at the beginning of every client contact is simply, “Has there been any change to your health?” Asking it routinely breaks the ice, and once the subject is open, follow-up questions come far more easily than they would if you introduced them cold partway through a session. Treat risk assessment as a dynamic process rather than a checkpoint at the door: the picture can change as an interaction progresses, and Public Health Ontario (2025) advises reassessing before each interaction precisely because a client's status is not fixed.
Your assessment should run in two directions. Consider what the training tasks themselves involve—whether they risk contaminating your skin or clothing, whether they bring you into contact with bodily fluids or non-intact skin, whether mucous membranes are involved, and whether you will handle equipment or surfaces that may already be contaminated. Then consider the client in front of you, and be prepared to recognize signs that may indicate an infection: coughing, sneezing, fever, shivering, fatigue or weakness, rash or swelling, nausea or abdominal pain, diarrhea, confusion, or neck stiffness. Neither assessment takes long once it becomes habit, and together they tell you whether routine practices will suffice or whether the encounter calls for something more.
For a fuller account of which conditions require which level of precaution, which clinical syndromes justify personal protective equipment before a diagnosis is confirmed, and how to work through the decision algorithms, consult Public Health Ontario's Routine Practices and Additional Precautions in All Health Care Settings (2025).

Graphic © Dimitry Naumov/Shutterstock.com.
In short, systematic screening of both staff and clients creates a consistent safety net that reduces the likelihood of infectious individuals entering the treatment environment.
Hand Cleaning
This section addresses the single most effective weapon against infection transmission: proper hand hygiene. Upon arrival, staff should clean their hands with soap and water or with an alcohol-based hand sanitizer. CDC's general guidance is a product containing at least 60% alcohol, but the effective floor differs by alcohol: at least 60% for ethanol and at least 70% for isopropanol, with CDC's health care hand hygiene guideline identifying solutions of 60–95% alcohol as most effective (CDC, 2002, 2024c). The Centers for Disease Control and Prevention (CDC, 2024c) recommends a five-step handwashing protocol:
- Wet your hands with clean, running water (warm or cold), turn off the tap, and apply soap.
- Lather your hands by rubbing them together with the soap. Lather the backs of your hands, between your fingers, and under your nails.
- Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from beginning to end twice.
- Rinse your hands well under clean, running water.
- Dry your hands using a clean towel or air dry them.

Graphic © Black Duck Style/Shutterstock.com.
Gloves come next, but they are governed by the task rather than by habit. Wear them whenever you anticipate that your hands will contact mucous membranes, non-intact skin or tissue, bodily fluids, or equipment and surfaces contaminated with any of these—which in neurofeedback practice means abraded scalp sites, used sensors, and soiled prep materials. Gloves are not required for routine training in which contact is limited to intact skin. This is a meaningful distinction rather than a technicality, because indiscriminate or improper glove use has itself been linked to the transmission of pathogens (Public Health Ontario, 2025). Gloves are task-specific and single-use for that task; change them between clients and between a contaminated site and a clean one, and never wash a pair for reuse (Siegel et al., 2007). Above all, remember that gloves are not a substitute for hand hygiene but an additional barrier layered on top of it, and that hands must be cleaned both before donning and immediately after removal (CDC, 2024a; World Health Organization, 2009, 2025).
Clients should also disinfect their hands upon arrival with a sanitizing product, and both clients and staff should repeat the hand-cleaning process before leaving the clinic.

Graphic © TRADOL/Shutterstock.com.
Key Takeaways
Screening and hand hygiene form the first and most effective barriers against infection transmission. Staff and clients should check for symptoms before arriving, and everyone should clean their hands on entry using soap and water or a sanitizer containing at least 60% alcohol—60% or more for ethanol, 70% or more for isopropanol. Gloves are chosen by task rather than by habit—required when hands will meet mucous membranes, non-intact skin, bodily fluids, or contaminated equipment, and unnecessary for routine training on intact skin—and they never replace handwashing. Both staff and clients should clean their hands again before leaving. Building these habits into every visit creates a consistent safety net that catches problems before they reach the treatment room.
Personal Protective Equipment
This section addresses the barriers you place between yourself and an infectious agent. Personal protective equipment (PPE) covers gloves, masks, gowns, and eye protection—items whose shared function is to interpose a physical barrier between infectious microorganisms and a person's mucous membranes, skin, airway, and clothing. Sensor placement and skin preparation put you closer to a client than almost anything else you do, so these are the moments when the choice of barrier matters most, and disposable masks should always be available for clients who need them.
What governs the choice is the risk assessment described earlier under Risk Assessment Screening. Select PPE according to the kind of interaction the session involves and the routes by which any suspected pathogen travels, rather than donning a standard set for every client. Public Health Ontario (2025) is emphatic that PPE should never be used indiscriminately. Overuse interferes with the quality of client care and wastes resources; improper use does worse than that, since indiscriminate or improper glove use, and the re-use of gloves and gowns, have been linked to the transmission of pathogens. A gown worn from one room to the next, or a mask handled repeatedly with contaminated hands, moves organisms rather than blocking them.
Applied item by item, the principle is straightforward. Gloves, as the Hand Cleaning section described, are unnecessary for routine care when the skin is intact, and hand hygiene remains paramount regardless.
Gowns are warranted only when you anticipate splashes or sprays of bodily fluids. Masks belong on you when you are working within two meters of a coughing client or when splashes or sprays are possible, with the specific mask chosen by risk assessment—an N95 respirator, a tight-fitting mask that filters at least 95% of airborne particles and requires periodic fit-testing, is the appropriate choice when infectious particles travel by the airborne route rather than in larger droplets.
Some clients will nonetheless feel more comfortable masking at every contact and will prefer that you do the same, and accommodating that preference costs you nothing. Eye protection follows the same two-meter rule: safety glasses, goggles, or a face shield when you are close to a coughing client or when sprays and splashes are possible.
In short, PPE provides a critical barrier during the close interactions that neurofeedback and biofeedback sessions demand, but it earns its value only when the choice of equipment follows from an assessment of the specific risk in front of you.

Graphic © theskaman306/Shutterstock.com.
Equipment Disinfection and Sterilization
This section explains the critical difference between sterilization and disinfection and identifies the products that effectively protect your clients. Sterilization destroys all microbial life—including resistant bacterial spores—using chemical or physical methods. Disinfection, by contrast, uses chemical agents or wet pasteurization to eliminate many microorganisms but does not destroy bacterial spores on inanimate objects (CDC, 2020). Because most neurofeedback equipment contacts only intact skin, clinics will mainly mitigate infection through disinfection, reserving sterilization for equipment that enters sterile tissue or the vascular system.
Staff should wipe all surfaces that they or clients could touch with a disinfectant selected for the organisms that matter in their setting; products named in the biofeedback literature include Protex Disinfectant Spray®, Virusolve®, and FreshnIT® (Hagedorn, 2019). Read the label rather than the category, because these three are not equivalent. Virusolve+® carries a sporicidal claim tested to EN 13704 and EN 14347 and is labeled as effective against bacterial spores including Clostridioides difficile (formerly Clostridium difficile). Protex Disinfectant Spray® is a low-concentration quaternary ammonium product whose registered label claims methicillin-resistant Staphylococcus aureus (MRSA) but makes no C. difficile or sporicidal claim, and FreshnIT® is a washroom cleaner-disinfectant with neither claim. Where sporicidal action is genuinely required, choose a sporicidal chemistry—sodium hypochlorite, hydrogen peroxide or peroxyacetic acid, or hypochlorous acid—of the kind listed by the Environmental Protection Agency as effective against C. difficile spores (U.S. Environmental Protection Agency, 2025). Alcohol concentration is a separate question: a product containing only 20% isopropyl alcohol falls far below the 60–90% range in which alcohols are reliably bactericidal, but no alcohol concentration is sporicidal, so raising the percentage will handle MRSA and still will not kill C. difficile spores (Rutala et al., 2008). Product selection therefore matters as much as the cleaning routine itself.

Graphic courtesy of Bio-Medical Instruments.
For sensors and leads applied to abraded skin, staff should use high-level disinfectants; for routine training in which sensors contact intact or lightly prepared skin, low-level disinfection after each use is typically adequate. Apply the product with a cloth, remove excess with a wet cloth after a few minutes, then rinse the sensors, leads, and straps with lukewarm water and air dry to minimize skin irritation. Never immerse sensors and leads in a cleaning product, as this can damage their internal components (Moss et al., 2019).
Despite the cost of disposable electrodes, they substantially reduce the risk of infection transmission and should be discarded after each use rather than reprocessed. Reusing them risks accidental application on a different client, and their surfaces degrade quickly, compromising signal quality (Moss et al., 2019); the regulatory and practical case against reuse is developed further in the Sensors discussion under Best Practices. Effective equipment management therefore requires matching the right disinfectant or sterilization method to each surface and device type, a decision guided by the Spaulding classification system taken up below under Cross-Contamination.
Key Takeaways
Sterilization destroys all microbial life, including bacterial spores, while disinfection removes many organisms but spares spores on inanimate surfaces. Because most neurofeedback equipment contacts only intact skin, clinics rely mainly on disinfection and reserve sterilization for equipment that enters sterile tissue or the vascular system. Wipe every touchable surface with a sporicidal disinfectant, reserve high-level disinfectants for sensors and leads that have contacted abraded skin or mucous membranes, and use low-level disinfection for the routine case. Never immerse sensors, and discard disposable electrodes rather than reprocessing them. Matching the right method to each surface and device is the core of sound equipment management.
Control of the Environment
This section covers the setting itself rather than the people in it. Controlling the environment reduces infection risk in three ways at once: it puts distance between potential carriers of infection, it keeps the air and surfaces of the room in good condition, and it establishes reliable cleaning practices for both the equipment and the space around it.
Distance is the first of these levers. Remote neurofeedback training is the safest approach since clients remain at home, eliminating in-person transmission entirely. Clinicians who offer remote services should select models that ensure the same quality of training provided within a clinic.

Graphic © Symphonic Mind Ltd.
For facilities that require in-person visits, thoughtful space management can substantially reduce risk. If there are two doors, designate one as an entrance and another as an exit to manage foot traffic. Space waiting-area chairs generously. CDC's health care guidance asks for spatial separation of ideally more than 3 ft (0.9 m) between people with respiratory symptoms in common waiting areas; it no longer publishes a single 6-ft rule, noting that no one distance is reliably safe, so more separation is better than less. Some neurofeedback offices train more than one client at a time in a single room; where that is the case, partitions can be placed between training stations if the risk merits it.

After skin preparation and cap or individual sensor placement, staff should interact with clients from the recommended distance or remotely from a control room. Distance obtained this way—through remote training, a redesigned layout, or control-room monitoring—shortens the window of close contact during which respiratory and surface transmission are most likely, and it costs nothing once the room is arranged for it.
Housekeeping is the least glamorous and most consistently underrated of these measures. Regular, thorough cleaning should be routine at every NFB training site rather than an occasional catch-up. Linen and cloth-covered items such as pillows and headrest covers must be laundered after each use, not merely straightened. Waste should be removed promptly rather than accumulating in the training room, and if blunted needles are used with qEEG electrode caps they belong in a proper sharps container, which a pharmacy will supply and will also accept for disposal once it is full.
Two additions to the physical setting are worth the modest cost. Gel-based hand sanitizer in pump bottles, or wall-mounted where clients and staff will pass it, makes hand hygiene the path of least resistance rather than a detour; this supplements rather than replaces bathrooms stocked with soap and water. Air handling is the second. Portable air cleaners fitted with a HEPA filter—a high-efficiency particulate air filter, which captures at least 99.97% of airborne particles 0.3 µm in diameter, the size that penetrates filter media most readily, with larger and smaller particles captured even more efficiently—measurably reduce exposure to airborne infectious aerosols. Lindsley and colleagues (2021) found that two portable HEPA air cleaners reduced aerosol exposure by up to 65% on their own and by as much as 90% when combined with universal masking, and the National Institute for Occupational Safety and Health (2024) recommends portable or built-in HEPA filtration particularly in medical offices and other spaces frequently occupied by people more likely to carry a respiratory illness. In short, a well-managed environment does quiet, continuous work between sessions that no amount of careful technique during a session can replace.
Administrative Controls
This section addresses the policies and expectations that make everything else stick. Clients need education, and they need it before they arrive rather than in the moment. Tell them plainly that you expect them to use hand sanitizer when they enter the training office, and ask them not to come at all if they have an acute respiratory infection. Post or hand out basic respiratory etiquette in whatever form suits your setting—coughing into the elbow rather than the hand, sneezing into a tissue, disposing of that tissue immediately, and washing hands afterward. None of this is unfamiliar to most people, but stating it as a practice expectation rather than assuming it changes behavior.
Staff work under the same expectations. If you employ or supervise anyone, they should receive the same guidance you give clients, and they should be asked—genuinely, with scheduling and pay arranged so that the request is realistic—to stay home when they have symptoms that might indicate an infection. Ideally, staff immunizations should be current. A policy that quietly punishes absence all but guarantees that ill staff will come in anyway.
The routine practices described throughout this unit are sufficient for nearly every situation in which neurofeedback is conducted. Unusual cases will occasionally warrant additional precautions, and when they do, the decision should rest on published guidance rather than improvisation. Public Health Ontario's Routine Practices and Additional Precautions in All Health Care Settings (2025) remains the most practical reference for that judgment. In short, administrative controls cost little and determine whether the rest of your infection-control effort is applied consistently or only when someone remembers.
Cross-Contamination
This section introduces the classification system that should guide every equipment-related infection control decision you make. Cross-contamination is the inadvertent transfer of microorganisms from one individual or site to another—precisely the chain of events described in this unit's opening scenario. To manage this risk systematically, infection mitigation should follow the Spaulding classification system, a widely used framework that categorizes reusable medical devices into three levels of ascending infection risk (Rutala et al., 2008).
The three Spaulding levels are critical, semi-critical, and noncritical. Applied to EEG equipment, the assignment turns on two questions and nothing else: how invasive the electrode is, and which tissue it actually contacts—intact skin, mucous membranes, or sterile tissue. The framework stratifies infection transmission risk according to the tissue a device will touch during use (Nanosonics, n.d.), and the category a device lands in determines the level of reprocessing it requires (Rutala et al., 2008). Neurofeedback caps and electrodes typically fall into the semi-critical and noncritical categories, although certain sharp instruments can reach critical status (Moss et al., 2019). Understanding which category your equipment belongs to determines the required level of disinfection or sterilization—a decision that directly impacts client safety.
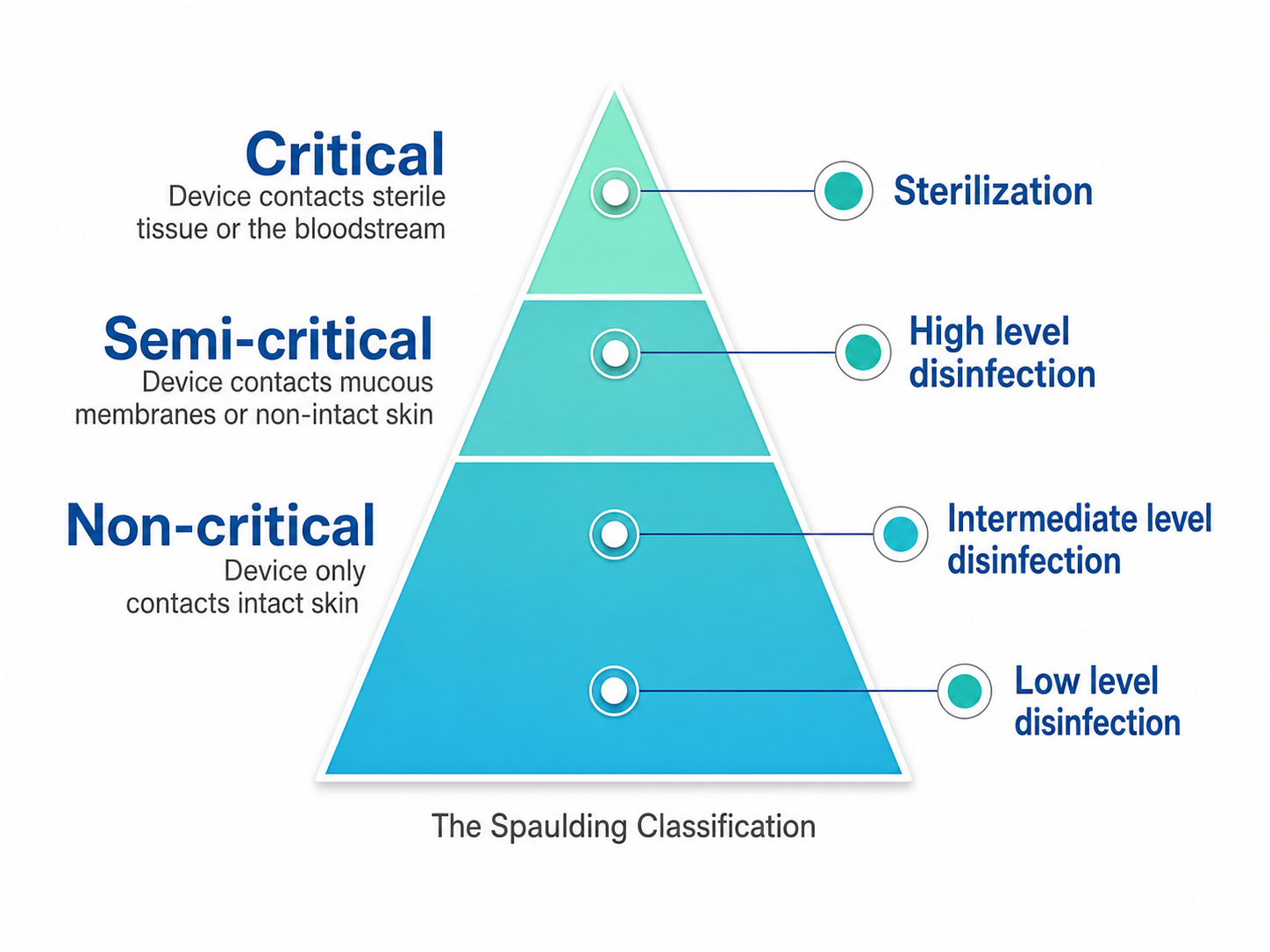
We adapted this graphic from Nanosonics. The Spaulding Classification System stratifies infection transmission risk based on the patient tissue a device will contact during use. The device classification determines the level of disinfection/sterilization required.
Key Concept
Critical means that equipment enters sterile tissues or the vascular system. Depth electrodes used in stereotactic EEG and the subdural or epidural strips and grids placed directly on the brain surface during intracranial monitoring belong in this highest-risk category, as do electrode prongs that can penetrate skin layers, and all of them require sterilization (Shah & Mittal, 2014; World Health Organization, 2018). Vaporized hydrogen peroxide is a low-temperature sterilization method, running at roughly 50 °C (about 120 °F), that will not damage heat-sensitive sensors the way steam autoclaving at 121–134 °C (250–273 °F) or dry heat at 160–190 °C (320–375 °F) can (Moss et al., 2019).
Semi-critical means that sensors can contact mucous membranes or non-intact skin. Nasopharyngeal and sphenoidal EEG leads belong here by design, as does any other EEG electrode that may have contacted over-abraded skin. These require high-level disinfection, destroying most microorganisms. Avoid abrasive cleaning products. Instead, use disinfectants like “Cidex®, Protex®, and Sekusept® PLUS” (Moss et al., 2019, p. 340).
Noncritical means that the sensors contact intact skin but not mucous membranes. All surface EEG electrodes used for routine NFB training, along with their associated cables, belong in this category and require low-level disinfection, escalating to intermediate-level when a surface is visibly contaminated with blood (Rutala et al., 2008; World Health Organization, 2018). This is where the great majority of neurofeedback work sits, which is why minimizing abrasion pays a dividend in reprocessing burden as well as in client comfort.
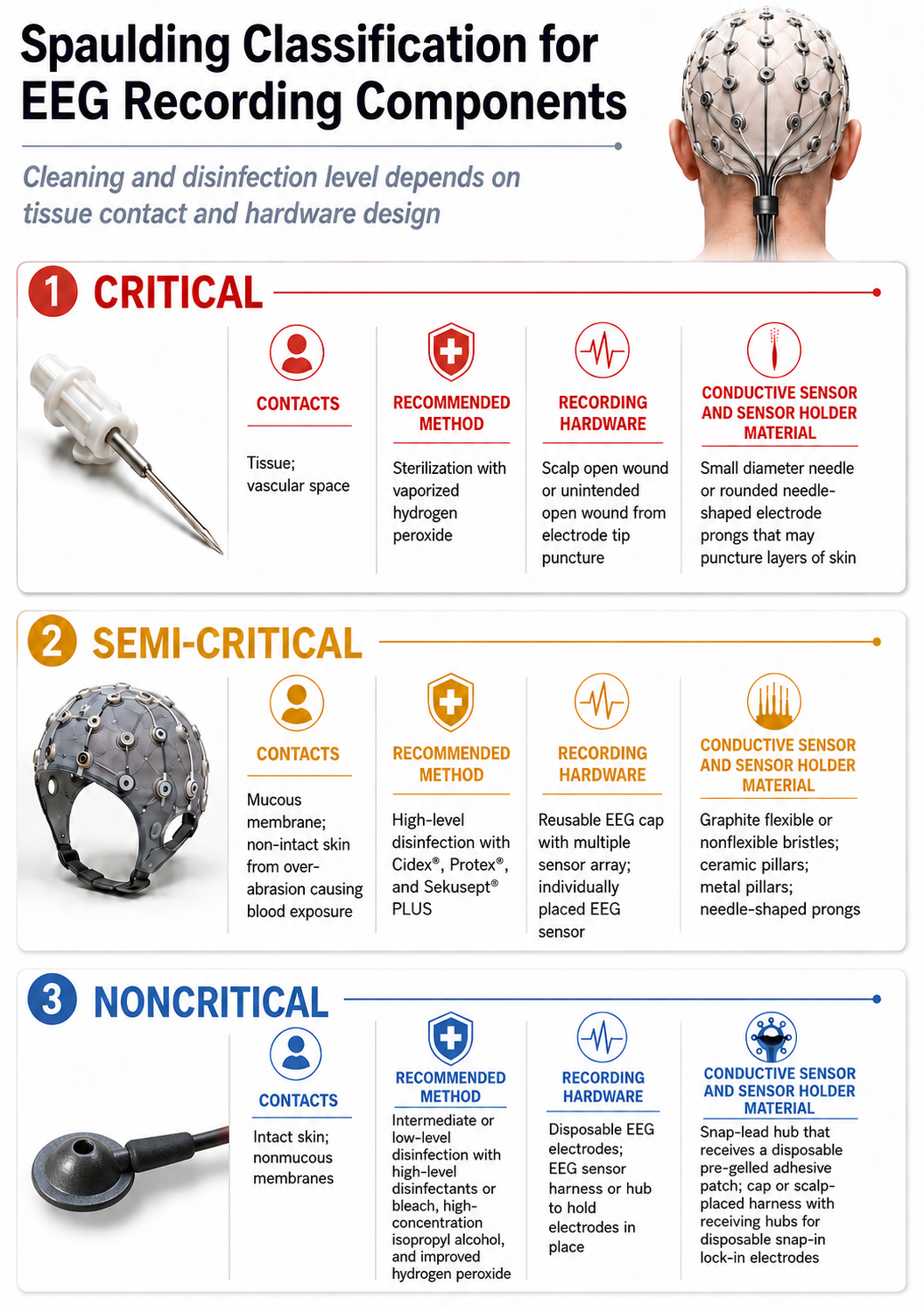
Dr. Donald Moss greatly contributed to this infographic.
Knowing a device’s category tells you what to do with it, and the three answers form a ladder whose rungs all rest on the same foundation. That foundation is cleaning, and no level of processing may skip it. As the CDC guideline puts it, “[t]horough cleaning is essential before high-level disinfection and sterilization because inorganic and organic materials that remain on the surfaces of instruments interfere with the effectiveness of these processes” (Rutala et al., 2008). Residual gel, paste, skin cells, and blood do not merely conceal microorganisms; they neutralize the germicide you apply on top of them, which is why a sensor that was disinfected but never properly cleaned has been processed in appearance only. Every reprocessing sequence therefore begins the same way, whatever the destination (CS Medical, 2024).
From that shared foundation the three levels diverge. Noncritical EEG devices—the standard surface scalp electrodes, whether Ag/AgCl cups or bridge electrodes, together with the external cables that touch only intact skin—require thorough cleaning followed by low- to intermediate-level disinfection (Health PEI, Quality and Patient Safety Division, 2025). Semi-critical devices require cleaning followed by high-level disinfection as a minimum, and “as a minimum” is the operative phrase, since it names a floor rather than a target (Rutala et al., 2008; World Health Organization, 2018). Nasopharyngeal and sphenoidal leads live in this category permanently because they are built to contact mucous membranes, and an ordinary surface electrode joins them whenever the skin beneath it was aggressively abraded or prepared until it broke (“Reducing the Risk,” 2019). Critical devices—the depth electrodes used in stereotactic EEG (McGinty & Balatskaya, 2023) and the subdural or epidural strips and grids placed directly on the brain surface during intracranial monitoring (Shah & Mittal, 2014)—require thorough cleaning followed by true sterilization. The CDC directs that such items be purchased sterile or steam sterilized where the device tolerates heat, with ethylene oxide or hydrogen peroxide gas plasma available for heat-sensitive equipment (Rutala et al., 2008); FitzGerald (2025) offers a compact walkthrough of how a facility should structure reusable device reprocessing around these tiers.
Two rules keep the ladder from being misread. The first is that movement is always upward. A device may be processed at a higher level than its category demands, never a lower one, and a crowded schedule is not an argument for the exception. Vancouver Coastal Health (n.d.) states the second in its infection prevention and control guidance: a semi-critical item that will contact open lesions or irritated mucous membranes should be handled as though it were critical. Translated into neurofeedback terms, a client whose scalp shows broken or inflamed lesions escalates the sensors you place on it, regardless of how routine the training protocol is. Both rules point back to the same practical conclusion reached in the skin preparation discussion: because the decontamination process a device needs is set by the tissue it touches (Ecolab, 2022), how gently you prepare the scalp and how heavily you must reprocess afterward are one decision seen from two ends.
In short, the Spaulding classification system provides a clear decision framework: identify the risk level of each device, then match it to the appropriate disinfection or sterilization method. This systematic approach removes guesswork from your infection control protocol and connects directly to the electrode cleaning and best practices sections that follow.
Clinical Application
Consider a clinician preparing for two very different sessions on the same afternoon. The first client will receive a standard EEG cap, and because the scalp is only lightly prepared and the sensors contact intact skin, the cap and its cables are noncritical and call for low-level disinfection between clients. The second client arrived with a fragile, flaking scalp, and preparation at two sites left the skin visibly broken despite a light touch; that moves those sensors into the semi-critical category and calls for high-level disinfection instead. Had either client required a depth electrode or a subdural grid—equipment that enters sterile tissue—that device would be critical and would require true sterilization rather than disinfection of any kind. By pausing to classify each device before the session, the clinician matches the method to the risk rather than treating all equipment the same way, and notices along the way that reducing abrasion in the second protocol would lower the reprocessing burden as well.
Key Takeaways
The Spaulding classification system removes guesswork by sorting devices into critical, semi-critical, and noncritical categories of ascending infection risk. Critical devices that enter sterile tissue or the vascular system require sterilization, semi-critical devices that contact mucous membranes or over-abraded skin require high-level disinfection, and noncritical devices that touch only intact skin require low-level disinfection, or intermediate-level when blood is visibly present. Surface electrodes and cables used for routine neurofeedback training are noncritical, which is where most practice sits; aggressive abrasion is what pushes them up a category. Classify each device first, then match it to the appropriate method to prevent cross-contamination systematically.
Check Your Understanding
- Why does the noninvasive nature of neurofeedback lead some providers to underestimate their infection transmission risk?
- What are the three pillars of infection risk mitigation described by Hagedorn, and why does each one matter?
- How does sterilization differ from disinfection, and when is each appropriate in a neurofeedback clinic?
- Into which Spaulding category do surface electrodes used for routine NFB training fall, and what would move them into a higher category?
- How would you decide whether a particular sensor requires sterilization rather than high-level disinfection?
Electrode Cleaning
This section translates the disinfection principles developed across this unit into a concrete routine for the sensors you handle every day. Before you adopt any cleaning protocol, however, you need to absorb one idea that overrides everything else in this unit: there is no universal electrode-cleaning procedure. The correct steps depend entirely on what your sensors are made of. A vigorous soak-scrub-disinfect routine that restores a tin or gold-plated sensor to nearly new condition can permanently degrade a coated silver–silver chloride sensor, often on its very first pass. Published cleaning guidance circulates widely on the internet without this qualification, and clinicians who follow it faithfully often destroy expensive sensors while believing they are practicing good infection control. Albert and colleagues (2019) documented exactly this problem in epilepsy monitoring units, where site variation in cleaning and reprocessing practice was high and no standardized method emerged. Your first task, therefore, is not to memorize a protocol but to identify your hardware.
Know What Your Sensors Are Made Of
Silver–silver chloride (Ag/AgCl) sensors reach you in two constructions that look nearly identical and behave nothing alike. A coated Ag/AgCl electrode—also called an electroplated or electrodeposited electrode—is a silver disk carrying an extremely thin surface film of silver chloride, often only a few micrometers thick, deposited either electrically or by immersion in a chloride solution. A sintered Ag/AgCl electrode is manufactured by pressing a homogeneous powder mixture of silver and silver chloride into a pellet and baking it at roughly 400 °C, so that the chloride is distributed throughout the full thickness of the sensor rather than resting on its surface (Neuman, 2010). Sintered pellets are typically one to two millimeters thick and never require rechloriding, because grinding, sanding, or wearing away the outer layer simply exposes more of the same material underneath.
That structural difference determines how much cleaning a sensor can survive. The recording property at stake is the half-cell potential, the small steady voltage that develops wherever a metal meets an electrolyte such as conductive paste. Bare silver and chlorided silver sit roughly 0.58 V apart in the table of standard electrode potentials—0.799 V and 0.223 V, respectively—so when patches of the chloride film flake away and expose the silver beneath, the sensor presents two mismatched half-cells at once. Those tabulated values are defined at unit activity and are not the offset you would measure in conductive gel, where chloride pushes bare silver toward the Ag/AgCl value; what matters clinically is that the mixed surface is unstable, not that it is offset by any particular amount. Neuman (2010) observed that electrodeposited silver chloride “has a tendency to flake off under mechanical stress, leaving portions of metallic Ag in contact with the electrolyte, which can cause the electrode's half-cell potential to be unstable and noisy” (p. 200), and concluded that sintered electrodes “tend to have a greater endurance… and they are best applied when repeated usage is necessary” (p. 200). A stripped sensor also loses its resistance to electrode polarization, the buildup of an opposing voltage at the metal-electrolyte junction as current passes through it. Intact Ag/AgCl is essentially nonpolarizable, which is why Tallgren and colleagues (2005) found that sintered Ag/AgCl outperformed silver, tin, gold, platinum, and stainless steel for slow-potential work, while the other reusable types showed “diverse degrees of polarization, baseline drift, low-frequency noise, high resistance, and changes in properties due to wear and tear” (p. 799); the six disposable Ag/AgCl models they tested also proved electrically appropriate. If you record slow cortical potentials, DC-coupled EEG, or infra-low frequencies, an aggressively cleaned sensor is not merely cosmetically worn—it is no longer capable of the measurement you are attempting (Vanhatalo et al., 2005).
Key Concept
Ask your manufacturer a single question before you clean anything: are these sensors coated or sintered? Coated Ag/AgCl sensors carry their conductive surface as a microscopically thin film that tissue-wiping preserves and almost any other cleaning method removes. Sintered Ag/AgCl sensors, whether individual disks or the disks mounted in a cap, carry silver chloride throughout the pellet and tolerate the full soak-brush-rinse-disinfect routine. Gold-plated and solid tin sensors have no chloride layer to lose and tolerate mechanical cleaning, though gold plating is itself soft and thin. When you cannot determine the construction, treat the sensor as coated until the manufacturer tells you otherwise.
Caring for Coated Silver-Silver Chloride Sensors
Coated Ag/AgCl sensors call for the most counterintuitive protocol in this unit, because for these sensors the recommended cleaning method is almost no cleaning at all. Soaking, detergent, brushing, alcohol, and abrasive pads each remove some portion of the conductive surface, and the surface does not grow back. The approach we recommend in most settings is to assign each client a dedicated set of sensors, store that set in its own labeled zipper-top plastic bag, and simply wipe the sensors with a tissue after each session. Nothing else touches them. This single practice preserves the electrode surface, eliminates client-to-client transfer at the sensor entirely, and reduces the waste generated by discarding serviceable hardware.
Dedicating equipment to one person is not an improvisation; it is an established infection-control strategy. Siegel and colleagues (2007) recommend that facilities “use disposable noncritical patient-care equipment… or implement patient-dedicated use of such equipment,” reserving shared use for situations in which dedication is impossible. This practice is known as patient-dedicated equipment, meaning reusable items assigned to a single individual for the duration of care rather than rotated among clients. Because a dedicated sensor never contacts a second person, the cross-contamination pathway that ordinarily requires high-level disinfection is closed at its source. Two cautions keep the strategy sound. First, the burden of hygiene shifts onto your hands: wash them thoroughly, and because used sensors count as contaminated equipment, glove for that handling and change gloves between clients and between one client's bagged materials and the next, since gloves become contaminated exactly as hands do and are never a substitute for hand hygiene (CDC, 2024a; World Health Organization, 2009, 2025). Second, let the sensors dry before you seal the bag. Rutala and colleagues (2008) emphasize that items “should be dried and stored… in a manner that protects them from recontamination,” and a sealed bag holding damp hardware becomes a small incubator rather than a container.
Clinics and hospitals governed by stricter reprocessing policies will not be permitted to stop at a tissue wipe. In those settings, the honest answer is that coated Ag/AgCl sensors become effectively disposable, and you should budget for them accordingly. One intermediate option preserves a few additional uses. Wipe the sensor with a tissue to remove paste, then soak it in a 10% household bleach solution—one part 5.25% to 6.15% sodium hypochlorite to nine parts water—for 10 to 30 minutes. The soak disinfects the sensor and, as a useful side effect, deposits a small amount of chloride back onto the silver surface. This is the chemical form of chloriding, the process of laying a silver chloride layer onto a silver base; Warner Instruments (2009) describes immersing silver in bleach “until a light gray color is observed (typically 10-15 minutes is sufficient)” (p. 1) as the standard low-technology alternative to electrical plating. A bleach-soaked sensor can usually be returned to service at least a few more times before its performance degrades beyond use.
Three practical constraints govern the bleach option. The solution must be mixed fresh and discarded daily, because free available chlorine dissipates and a stale container gives you a false sense of protection; Bonner and Davidson (2020) instruct neurodiagnostic laboratories to date each bottle and discard prepared solutions within 24 hours. The term available chlorine refers to the concentration of active hypochlorite in a solution, expressed in parts per million, and it is what actually does the killing. Concentration deserves a closer look than it usually gets, because the 10% preparation above delivers roughly 5,000 to 6,000 parts per million of available chlorine, and Rutala and colleagues (2008) note that hypochlorite is corrosive to metals above about 500 ppm. That corrosiveness is precisely what makes the soak useful here—it attacks the silver surface and leaves chloride behind—but it is also why a sensor treated this way has a short remaining life. Published EEG protocols accordingly use far weaker solutions when disinfection alone is the goal: Bonner and Davidson (2020) specify 0.1% sodium hypochlorite, or 1,000 ppm, for a 30-minute immersion, which reliably kills vegetative organisms while doing less damage. Choose deliberately between the two. If your aim is disinfection and continued service, use the 1,000 ppm preparation; if the sensor is near the end of its life and you want to refresh the chloride layer as well, the stronger soak buys a few more sessions at the cost of the sensor. Finally, many clinics simply prohibit bleach on their premises. Where that is the case, or where a client presents with a bloodborne-pathogen risk, single-use disposable sensors are the defensible choice, and the cost-effectiveness modeling by Sohrt and colleagues (2019) supports treating that expense as an investment rather than a loss.
Cleaning Sintered Silver-Silver Chloride Sensors and Caps
Sintered Ag/AgCl sensors, whether supplied as individual disks or mounted in an electrode cap, tolerate the same thorough routine used for tin electrode caps, with two points of extra care: rinse with distilled water and hang the assembly to dry. Begin the moment the session ends. Conductive paste that dries inside an electrode cup hardens into a residue that resists removal, and gel that spreads beyond the cup can create an electrode bridge, an unintended electrolyte connection between adjacent sites that makes two channels record nearly identical signals. Alschuler and colleagues (2014) surveyed publicly available EEG datasets and found bridging in 54% of recording sessions, with more than 40% of channels bridged in 9 of 203 sessions—an artifact that flattens topography and invalidates source localization. Immediate cleaning is therefore a data-quality practice as much as a hygiene practice, and every major cap manufacturer specifies it (Brain Products, n.d.; OpenBCI, n.d.; Wuhan Greentek, n.d.).
Start by unsnapping and setting aside every removable accessory—chin straps, ear clips, and gauze—so they can be washed separately. Then submerge the cap or the loose sensors in lukewarm water containing a small amount of mild, residue-free liquid detergent. Water temperature matters: Wuhan Greentek (n.d.) sets a ceiling of 50 °C for its sintered caps, and Electro-Cap International (n.d.) specifies lukewarm tap water for the same reason, since heat degrades elastic fabric. Ten to fifteen minutes of soaking dissolves most paste. Detergent choice matters as much as temperature, because ordinary hospital soaps leave an invisible film on the metal that raises impedance and generates artifact (Electro-Cap International, n.d.). Critically, submerge only the fabric and the sensors. The connector, splitter box, and any cable termination must stay dry; Brain Products (n.d.) warns that the splitter box “contains highly sensitive electronic components… Never let them come into contact with water,” and eemagine Medical Imaging Solutions (2017) instructs users to keep all cables and connectors away from the water entirely.
Once the paste has softened, work each electrode mount gently with a cotton-tipped applicator or a soft-bristled toothbrush, cleaning the inside of the cup and the surrounding fabric. Electro-Cap International (n.d.) recommends the wooden end of a cotton swab or an orange stick precisely because wood will not scratch metal. Never reach for a metal scraper, an abrasive pad, or a scouring cleanser, and never point a high-pressure water jet such as a Waterpik at a cap; BIOPAC Systems (n.d.) states plainly that such a jet “will drastically shorten the life of these electrodes and is not recommended,” and eemagine Medical Imaging Solutions (2017) prohibits hard brushes and hard materials of any kind. Handle the sensors by the disk rather than the wire, and never tug a lead to reposition it. Cap wiring is the most fragile part of the assembly: eemagine Medical Imaging Solutions (2017) warns bluntly that “dragged-out cables are not covered by the cap warranty,” and Brain Products (n.d.) notes that wet pins are more vulnerable to mechanical stress than dry ones. A sensor that detaches from its lead during cleaning costs far more to repair than the minute you saved by scrubbing quickly.
Rinse the cap thoroughly under running lukewarm tap water until no soap or gel remains, then finish with a rinse of distilled or deionized water. Several manufacturers specify this final purified rinse for the metal specifically, on the reasoning that it leaves behind no mineral residue to accumulate on the sensor surface (eemagine Medical Imaging Solutions, 2017; OpenBCI, n.d.). If your caps are used across multiple clients or in a clinical setting, disinfect at this stage using an agent your hardware manufacturer has approved—commonly Envirocide, Perfektan TB, CaviWipes, or a glutaraldehyde solution such as Metricide or Cidex—and observe the stated exposure limits, which typically run 5 to 15 minutes. Longer is not better. Prolonged contact with strong chemicals degrades cap fabric and corrodes metal, and alcohol solutions in particular should be used for wiping only, never for soaking, because they leave plastic components brittle (Brain Products, n.d.). Follow every chemical disinfection with another distilled-water rinse so that no residue remains against the client's scalp.
Cleaning Gold-Plated and Tin Sensors
Gold-plated sensors and the solid tin electrodes used in Electro-Caps have no chloride layer to lose, which is why the widely circulated soak-and-scrub protocols suit them well. Electro-Cap International (n.d.) directs users to fill a sink with lukewarm water and a small amount of Ivory or Palmolive liquid detergent, submerge only the cap, clear the electrode mounts with an orange stick or cotton swab, rinse thoroughly, and hang the cap to dry with the cap positioned lower than the connector so that water cannot run down into the terminals and corrode them. Air drying takes about an hour; a hair dryer may be used on a warm setting but never on high, and the caps must never be steam autoclaved, because the process weakens the elastic material and shortens cap life. Tin electrodes accumulate an oxide film with use, and Electro-Cap International (n.d.) recommends scraping the disks thoroughly with an orange stick or the wooden end of a cotton swab once a month.
Gold plating deserves one qualification. Although gold is chemically noble and its recording properties do not depend on a surface reaction product, the plating itself is soft and only two to three micrometers thick, so abrasive cleansers and hard tools wear through it to the silver substrate beneath. Górecka and Makiewicz (2019) measured impedance across repeated use and found that gold cup electrodes deteriorated faster than other types, concluding that a set of gold electrodes should be retired after roughly ten examinations while other materials tolerated about twenty. Clean gold gently with a damp soft cloth or foam swab and mild detergent, and inspect the plating periodically for the dull silver-gray patches that signal wear-through.
Drying, Inspection, and Storage
How you finish matters more than most clinicians assume. Albert and colleagues (2018) took 124 swabs from reusable EEG cup electrodes and lead wires that had been cleaned and staged as ready to use at four hospitals, and recovered bacterial growth on 25% of them. In the companion analysis of cleaning practice, Albert and colleagues (2019) found that a drying time of five minutes or less cut the odds of a positive culture by 71%, and concluded that air drying should give way to drying with a clean towel. Blot first, then let the equipment finish drying completely on a clean towel or an electrode rack. Hang caps with the connector above the cap so gravity pulls residual water away from the electronics rather than into them (Electro-Cap International, n.d.). Skip the hair dryer unless your manufacturer permits one—Electro-Cap International (n.d.) allows a warm setting but never high—since heat warps plastic and degrades elastic fabric.
Inspect before you store. Run your eye and fingers along each lead wire and connector, looking for cracks, kinks, exposed conductor, greenish corrosion at the terminals, and any looseness where the wire enters the sensor. Damaged leads generate intermittent artifact that is easily mistaken for physiological signal, and a lead that is beginning to separate is far cheaper to repair than to replace. Store the completely dry equipment in a cool, dark, dry place away from direct sunlight, and avoid airtight containers for anything that might still hold moisture (OpenBCI, n.d.; Wuhan Greentek, n.d.). For coated Ag/AgCl sensors on the dedicated-set protocol, this is the point at which each client's dry sensors return to their labeled bag.
In short, match the cleaning method to the sensor construction, not to the protocol you found first. Coated Ag/AgCl sensors get a tissue wipe, a labeled per-client bag, and scrupulous hand hygiene, with a fresh dilute bleach soak as the compromise for facilities that require chemical disinfection and disposal as the fallback when they do not permit bleach. Sintered Ag/AgCl sensors and caps get the full routine—immediate lukewarm soak, gentle brushing, dry connectors, distilled-water final rinse, manufacturer-approved disinfectant within its stated exposure limit, and hanging to dry. Gold and tin tolerate mechanical cleaning, with gold plating watched for wear. Every construction ends the same way: fully dry, inspected, and stored cool and dark.
Clinical Application
Consider a practice that runs individual coated Ag/AgCl sensors for two-channel training in the morning and a sintered Ag/AgCl cap for qEEG assessments in the afternoon. The morning routine is deliberately minimal. The clinician washes her hands and dons gloves—not for the intact scalp, which would not require them, but because she will be handling used sensors afterward—then retrieves the labeled bag holding this client's dedicated sensors, and after the session wipes each sensor with a tissue and nothing more. She removes her gloves, washes her hands again, lets the sensors sit briefly until dry, returns them to their bag, and repeats the sequence with fresh gloves for the next client's bag. The afternoon routine looks entirely different. The moment the cap comes off, she unsnaps the chin strap, drapes a towel over the splitter box, and lowers only the cap into a sink of lukewarm water with a few drops of mild detergent. After ten minutes she works each electrode mount with a soft toothbrush, rinses under running water, finishes with distilled water, immerses the cap in the manufacturer-approved disinfectant for its stated twelve minutes, rinses with distilled water once more, blots the sensors with a clean towel, and hangs the cap connector-up to finish drying overnight. Same clinic, same afternoon, two protocols—because the hardware, not the schedule, dictates the method.
Key Takeaways
Sensor construction determines the cleaning protocol. Coated Ag/AgCl electrodes carry silver chloride as a film only micrometers thick, and virtually any cleaning method other than a tissue wipe strips it, leaving an unstable half-cell potential and a polarizing surface unsuitable for slow-potential work. The preferred management is a dedicated sensor set per client, stored dry in a labeled zipper bag, with rigorous handwashing and glove changes between clients; a 0.1% (1,000 ppm) bleach soak for 30 minutes disinfects with minimal corrosion, while a stronger 10% soak for 10 to 30 minutes also refreshes the chloride layer at the cost of the sensor’s remaining life, and disposal is the fallback where bleach is prohibited. Sintered Ag/AgCl sensors and caps tolerate the full routine of immediate lukewarm soaking with mild residue-free detergent, gentle brushing with a soft toothbrush or cotton swab, dry connectors, a distilled-water final rinse, and manufacturer-approved disinfection within stated exposure limits. Gold and tin sensors tolerate mechanical cleaning, though gold plating is only microns thick and wears through. Cap wiring is fragile at the sensor junction, so handle disks rather than leads, and finish every protocol by blotting dry, inspecting the leads, and storing cool, dark, and dry.
Check Your Understanding
- What is the structural difference between a coated and a sintered Ag/AgCl electrode, and why does that difference change the cleaning protocol?
- How does stripping the silver chloride layer affect the half-cell potential and electrode polarization, and which recording applications suffer most?
- Why does assigning a dedicated sensor set to each client reduce infection risk, and what two practices must accompany it for the strategy to work?
- What does a 10% bleach soak accomplish beyond disinfection, what does it cost the sensor, and why must the solution be discarded daily?
- Why must the connector and splitter box stay out of the water, and how should a cap be hung to dry?
- What did Albert and colleagues (2019) find about drying time, and how should that change your end-of-session routine?
Best Practices
Skin Preparation
This section covers practical steps that reduce infection risk during skin preparation and sensor placement—procedures you will perform in virtually every session. Begin by asking how much preparation you actually need, because the answer has changed. Electrode impedance is the opposition that the sensor, the conductive medium, and the underlying tissue jointly present to the small test currents your equipment uses to check the connection, and clinicians have traditionally driven it below 5,000 ohms by abrading the scalp. Ferree and colleagues (2001) tested whether that target is necessary by varying scalp-electrode impedance systematically within each participant—lowering it by abrading the site, raising it by letting the electrolyte dry—and found no significant amplitude change in any EEG frequency band as impedance rose from below 5,000 ohms on abraded skin to 40,000 ohms on intact skin. What did rise was 60-Hz line noise, which increased with both absolute impedance and the mismatch between the measurement and reference electrodes, and rose only modestly with mismatch—about 8%—a problem better solved with balanced impedances and digital filtering than with sandpaper. The American Clinical Neurophysiology Society has since raised its own ceiling, and Sinha and colleagues (2016) now describe impedances up to 10,000 ohms as acceptable with modern digital equipment, while noting that readings below 100 ohms usually indicate a shunt or short circuit—possibly a salt bridge on the scalp—rather than an excellent connection.
Abrasion does buy something real, and honesty requires naming it. Kappenman and Luck (2010) recorded at high- and low-impedance sites simultaneously and found that high-impedance sites carried more low-frequency noise, particularly in warm and humid rooms, because removing the outer layer of dead skin cells suppresses skin potential artifact—the slow, large voltage shifts that arise as sweat gland activity and skin hydration change the standing potential across the epidermis. Their practical conclusion is a trade-off rather than a prohibition: keep the room cool and dry, apply appropriate high-pass filtering and artifact rejection, and the case for aggressive abrasion largely disappears. The infection argument then settles the matter. Bonner and Davidson (2020) point out that the CDC defines non-intact skin to include abrasions, and argue that preparing a site with an abrasive to lower impedance therefore creates non-intact skin, moving the sensor into the semi-critical Spaulding category and exposing it to blood products even when no blood is visible. Where that line falls in practice is a matter of degree: light preparation that leaves the stratum corneum essentially intact keeps a surface electrode in the noncritical category, while abrasion vigorous enough to break the skin does not. Because you cannot always tell by looking, prepare as gently as the recording allows, and reprocess at the higher level whenever you have reason to think a site was over-abraded.
Every item you touch to a prepared site should be single-use. Alcohol swabs, cotton swabs, cotton balls, gauze, and tissues are used once, on one client, and then discarded—never set aside for a second pass, never carried to another site on another person. This matters more than it may appear, because alcohol is a weak agent working on a surface you have just compromised. The CDC classifies isopropyl and ethyl alcohol as effective against vegetative bacteria, fungi, and many viruses but not against bacterial spores, and notes that alcohols are not recommended for sterilizing because they lack sporicidal action and cannot penetrate protein-rich material (Rutala et al., 2008). Because it is tuberculocidal, fungicidal, and virucidal but not sporicidal, CDC classifies alcohol as an intermediate-level disinfectant—an agent that kills vegetative bacteria including tubercle bacilli, along with fungi and most viruses, but leaves spores intact—and excludes it from high-level disinfection altogether. That places it a rung above a low-level disinfectant, which spares tubercle bacilli as well as spores. It sanitizes the skin; it does not sterilize your supplies, and it will not rescue a contaminated cotton ball.
That last point drives the rule that most often gets broken. When you moisten cotton balls from an alcohol dispenser or a bulk container, never return a used cotton ball to the dispenser for a second helping. Reaching back into a shared reservoir with an applicator that has touched skin is the textbook mechanism of extrinsic contamination, the introduction of microorganisms into a product during handling and use within the facility, as distinguished from intrinsic contamination, which occurs during manufacture or shipping (Weber et al., 2007). The consequences are documented rather than theoretical. Nakashima and colleagues (1987) traced ten cases of septic arthritis to a canister of cotton balls soaking in benzalkonium chloride, and the outbreak stopped when the antiseptic was withdrawn. Nasser and colleagues (2004) traced 411 episodes of Burkholderia cepacia bacteremia in 361 patients to an alcohol skin antiseptic that had been diluted with contaminated tap water, and the epidemic ended once the hospital switched to single-use alcohol swabs, leaving only sporadic cases attributable to breaches of protocol. Even factory-packaged products are not immune: Dolan and colleagues (2012) cultured Bacillus species from the internal contents of 63.3% of alcohol prep pads that were not labeled sterile, and prep-pad recalls for bacterial contamination have recurred since. Read the package, know whether your pads are labeled sterile, and reserve the sterile ones for compromised skin.
The only defensible exception to the one-cotton-ball-one-trip rule is a case in which you are genuinely certain the client carries nothing transmissible—and that certainty is rarely available. Bloodborne pathogens can remain asymptomatic for years (Ferree et al., 2001), which is precisely why routine practices treat every client as potentially infectious. Where the client is known or suspected to carry a highly infectious or dangerous organism, the exception inverts entirely and the practice becomes stricter, not looser.
Handle the used supplies with the same discipline. Treat all used cotton-tipped applicators, tissues, gauze, and alcohol-impregnated wipes as contaminated and discard them immediately after use. Never place them on a desk or tabletop, where they can serve as vehicles for disease transmission to the next client (Moss et al., 2019). Items saturated enough to release blood or other potentially infectious material if compressed meet the regulatory definition of regulated waste and belong in a biohazard container; used sharps always do (Occupational Safety and Health Administration, n.d.). One substitution reduces the risk at its source: when a blunt needle is used to inject conductive gel through an electrode, as with a qEEG cap, a small-diameter wooden cuticle stick is often a better tool for migrating the gel down to the scalp than the harder-edged needle, since wood spreads the load and cannot cut. Measuring tapes used to calculate head circumference present a noncritical risk under the Spaulding system and require low-level disinfection between clients. Some of the best preparation happens before the client arrives: ask clients to wash their face and hair thoroughly before an NFB session and to skip cosmetics that day. Clean, product-free skin and hair make it far easier to reach acceptable impedances and offsets with minimal effort, which in turn means less abrasion and less infection risk. In summary, minimize abrasion because modern amplifiers no longer require it, use every prep supply exactly once, never re-enter a shared alcohol container with a used applicator, and dispose of everything immediately rather than staging it on a shared surface.
Conductive Gels and Pastes
This section addresses the container problem: conductive gels and pastes arrive in jars, tubes, and bottles that get opened dozens of times a week, and every opening is an opportunity to seed the product with organisms that will be pressed against the next client's scalp. The governing principle is simple. Nothing enters a gel or paste container except a clean electrode or a clean applicator that has touched nothing else. Bonner and Davidson (2020) state the neurodiagnostic profession's version of this rule plainly—prep materials should be removed from the container immediately before use, avoiding what they call “double-dipping” (p. 30), with excess discarded after each client—and add that electrodes should never be dipped into the paste jar during application.
The evidence behind that rule comes largely from the ultrasound literature, where coupling gel has caused repeated outbreaks and the mechanisms are well characterized. Conductive gel is not self-sterilizing; Hutchinson and colleagues (2004) investigated Burkholderia cepacia infections traced to contaminated gel and found that the implicated organisms could degrade the parabens meant to preserve the product, effectively consuming the preservative as food. Oleszkowicz and colleagues (2012) note that gel has been shown to lack intrinsic antimicrobial properties and can function as a growth medium. Contamination rates in ordinary outpatient practice are not trivial: Spratt and colleagues (2014) sampled nine outpatient clinics and found bacteria on 52.7% of gel bottle tips and inside 14.5% of the gel supplies themselves. Outbreaks continue to occur: a 2021 multistate outbreak of Burkholderia stabilis was traced to nonsterile multiuse gel that proved contaminated in unopened containers, and the investigators’ guidance is not to refill a container but to discard and replace it when empty (Hudson et al., 2022). The professional guidance that follows from this is consistent: discard and replace multidose containers when they are empty rather than refilling them, keep the container sealed when not in use, and keep the dispensing tip from touching the client, the sensors, or any equipment (American Institute of Ultrasound in Medicine, 2025).
The practical workflow follows directly. If a single cotton swab will be used repeatedly during one client's setup, do not shuttle it back and forth to the jar. Instead, use a clean utensil or squeeze a sufficient quantity for that entire session onto a clean intermediate surface such as a small plate, a medicine cup, or a square of gauze, and retrieve successive amounts from that surface. The portion on the plate now belongs to that client alone; whatever remains at the end of the session is discarded rather than returned to the container. Note the distinction from a practice that infection-control agencies do prohibit: decanting a working portion for one client is not the same as decanting gel into a second storage bottle for reuse across clients, which is what caused several of the documented outbreaks. Thoroughly clean and disinfect the intermediate surface after the session, since a reusable plate or tray is a noncritical item requiring low-level disinfection after each client (Rutala et al., 2008). In short, treat the gel container the way you would treat a shared medication vial—enter it only with something clean, dispense what you need for one person, and never send a used applicator back in.
Blunt-Tip Needles and Syringes
This section covers the tools used to deliver gel through the electrode openings of a 19-channel cap, where a single careless habit can injure the scalp, corrupt the recording, and transmit infection at the same time. Both the blunt-tip needle and the syringe are single-use items. A single-use device is one the manufacturer intends for one use on one client during one procedure, and Bonner and Davidson (2020) are explicit that items labeled single use may not be reused on another client regardless of whether disinfection has been attempted, that a syringe used to insert electrolyte paste or gel must be discarded after that client, and that changing only the tip while reusing the syringe is unacceptable. The CDC states the same principle for injection equipment in four words that transfer cleanly to gel delivery: one needle, one syringe, only one time (CDC, 2024b).
Draw enough gel into the syringe in one pass to serve every electrode on the cap. If you run short and need more, mount a new needle rather than reintroducing the used one into the gel container—the needle has by now contacted the client's scalp and hair, and returning it converts your gel supply into a shared reservoir of exactly the kind described in the previous section. When the session ends, discard the needle and syringe together. Never recap a used needle, even a blunt-tipped one, and place it directly into a puncture-resistant sharps container positioned as close as practical to where you are working (Bonner & Davidson, 2020). Regulatory language supports treating these as sharps: contaminated sharps are defined by the capacity to penetrate skin rather than by the sharpness of the tip, and the definition explicitly extends beyond hypodermic needles (Occupational Safety and Health Administration, n.d.).
The second risk is mechanical. A blunt needle used vigorously can still break the skin. The ASET position statement on skin safety warns that a blunt needle tip can easily over-abrade the skin and injure the surface, and lists the use of blunt-tipped needles to reduce electrode impedance among the practices technologists should avoid (ASET–The Neurodiagnostic Society, 2016). The damage is not only dermatological. Breaking the skin at a site changes what you are recording: it alters impedance, and it can shift the DC offset—the standing direct-current voltage difference between a sensor and its reference—in ways that produce baseline drift and unstable readings. It also converts a noncritical contact into a semi-critical one, since the sensor now touches blood.
Check skin integrity at every electrode site as a matter of routine, not only when a client complains. Ouchida and colleagues (2019) assessed the scalps of 251 adults undergoing ambulatory EEG—92 monitored for two to three days and 159 for four to five—and documented a significant acceleration of inflammation between day two and days four and five, with older age, fair skin, dry skin, and fine hair emerging as risk factors; they note that previously reported skin injury rates range from 7.8% to 27.3%. Inspect before you apply, inspect during long sessions, and inspect again at removal. If the scalp has been excessively abraded, say so to the client directly, document it, move the sensor away from the injured site, and reconsider how much preparation your protocol genuinely requires (ASET–The Neurodiagnostic Society, 2016). In short, treat the needle and syringe as a single-use pair, load enough gel for the whole cap in one draw, change the needle rather than re-entering the container, dispose of both as sharps, and let the condition of the client's scalp—not a habitual impedance target—set the limit on how hard you prepare.
Sensors
This section addresses sensor-specific precautions that connect directly to the Spaulding classification system discussed earlier. When clinicians place EEG sensors on highly abraded skin, this presents a semi-critical risk and requires high-level disinfectants such as Cidex®, Protex®, and Sekusept® PLUS. Routine training is a different matter. Because surface electrodes applied to intact or lightly prepared skin are noncritical devices, low-level disinfection of electrodes and caps after each use is typically adequate, and dedicating a sensor set to a single client remains a sound additional safeguard. Whatever the level, use soft materials for cleaning—a cotton-tipped applicator, a soft-bristled brush, or a wooden orange stick—so that the sensor surface is not scratched. In short, matching your sensor disinfection protocol to the appropriate Spaulding risk level, and keeping your cleaning tools softer than the metal they touch, closes one of the most common gaps in neurofeedback infection control.
Disposable sensors resolve several of these problems at once, but only if they are genuinely disposed of. A single-use sensor that is cleaned and applied to a second client forfeits every advantage that justified its cost, and the regulatory picture is less forgiving than most clinicians realize. The FDA treats any facility that reprocesses a single-use device as a manufacturer of that device, subject to the same premarket submission and quality-system requirements as the original maker, including validated data on cleaning, disinfection, sterilization, and functional performance (U.S. Food and Drug Administration, 2024). A clinic that wipes down disposable electrodes and reuses them is not merely cutting a corner; it is distributing an uncleared device. The CDC's disinfection guideline defers to the FDA on this question rather than establishing a separate standard (Rutala et al., 2008), and the neurodiagnostic profession's own guidance reaches the same conclusion by a different route, noting that no disinfection method has ever been validated for these products (Bonner & Davidson, 2020).
Where a clinic nonetheless elects to reuse disposable sensors—restricted, at minimum, to the same client—the sensors must be carefully cleaned with an appropriate disinfectant before every reapplication, and you should expect their performance to fall off. We are aware of no published study measuring impedance or artifact in reused disposable electrodes, so the honest position is that reuse is unvalidated rather than proven harmful. What the adjacent evidence shows is not encouraging: impedance climbs measurably with each successive use even in electrodes designed to be reused, and standard clinical impedance checks do not detect the underlying electrochemical degradation (Górecka & Makiewicz, 2019), while the hydrogel dries and the adhesive weakens once a package is opened. Weigh that against the economics before assuming reuse saves money. Sohrt and colleagues (2019) modeled single-use against reusable EEG cup electrodes across 73,834 patients and found single-use electrodes both less costly and more effective in the base case—$18.50 against $19.95 per procedure—once an incidence of 33 sepsis cases per 100,000 EEG procedures and the cost of treating sepsis were included. Their own probabilistic sensitivity analysis was not robust, however: in 38% of simulations single-use electrodes averted more sepsis but cost more.

Clinical Application
Picture a provider setting up a new client for a 19-channel recording from start to finish. She washes and dries her hands, dons fresh gloves, and clusters her prep supplies on a single cleanable tray so that nothing touches the shared desk. She takes one cotton ball to the alcohol dispenser, uses it, and discards it rather than reaching back for a second helping. She squeezes enough conductive gel onto a small plate to serve the whole cap, applies abrasive gel with a cotton-tipped applicator rather than a gloved finger, and draws a full syringe of gel through a fresh blunt needle in one pass so that nothing used ever re-enters the jar. Working gently, she checks each site for redness or broken skin as she goes and mentions to the client that one frontal site looks slightly irritated, moving the sensor a short distance rather than pressing on. At the end of the session, the needle and syringe go into the sharps container, the leftover gel on the plate is discarded, the plate is cleaned and disinfected, and the reusable sensors are processed at the level their Spaulding category requires and returned to this client's dedicated bag. This deliberate, forensic routine turns the abstract principles of this unit into a repeatable sequence that protects every client who follows.
Key Takeaways
Careful skin preparation, container discipline, and sensor handling close the most common gaps in neurofeedback infection control. Because modern amplifiers record well at impedances far above the traditional 5,000-ohm target, minimize abrasion; any abrasive that lowers impedance creates non-intact skin and moves the sensor into the semi-critical category. Use alcohol swabs, cotton swabs, cotton balls, and tissues exactly once, and never return a used cotton ball to a shared alcohol dispenser, since alcohol is an intermediate-level agent that cannot kill spores and in-use antiseptic containers have caused documented outbreaks. Enter gel and paste containers only with a clean electrode or applicator; when repeated access is needed, decant a single-client portion onto a clean plate, discard the remainder, and disinfect the plate afterward. Blunt-tip needles and syringes are single-use, must be loaded in one pass, require a new needle rather than a re-entry if more gel is needed, and go into a sharps container without recapping. Because a blunt needle can still break skin and alter impedance and DC offset, inspect every site for skin integrity and tell the client when the scalp has been over-abraded. Disposable sensors deliver their benefit only when discarded; reprocessing them makes the clinic a manufacturer in the FDA's eyes, and if reuse occurs at all it should be limited to one client, preceded by disinfection, and expected to degrade signal quality.
Check Your Understanding
- What did Ferree and colleagues (2001) find about EEG amplitude across the range from 5 kΩ to 40 kΩ, and how should that change your preparation routine?
- What does abrasion buy you in exchange for creating non-intact skin, and what two adjustments reduce the need for that trade?
- Why is alcohol insufficient to protect a cotton ball returned to a shared dispenser, and what outbreak evidence supports the single-trip rule?
- What is the difference between intrinsic and extrinsic contamination, and which one does double-dipping cause?
- How does decanting a single-client portion of gel onto a clean plate differ from decanting gel into a second storage bottle?
- Why must a new blunt needle be used if additional gel is needed mid-setup, rather than reinserting the original?
- How can a blunt-tip needle affect impedance and DC offset, and what should you do when you find an over-abraded site?
- What regulatory status does a clinic assume when it reprocesses a device labeled single use?
Cutting Edge
A growing body of research is pushing the field toward single-use, disposable sensors as a frontline infection-control strategy. In a multicenter study of four epilepsy monitoring units, Albert et al. (2018) swabbed cleaned, ready-to-use reusable EEG electrodes and found bacterial growth on 25% of them, with about 22.6% carrying organisms that posed a potential or actual infection risk. Routine cleaning, in other words, does not reliably eliminate the risk of healthcare-associated infection—a concern that sharpens further when skin abrasion pushes those same sensors into the semi-critical Spaulding category. Sohrt et al. (2019) extended this work with a cost-effectiveness model in which single-use electrodes were both less expensive and more effective than reusable ones in the base case once the cost of sepsis was considered, although the model’s sensitivity analysis left that conclusion uncertain. For neurofeedback providers, the practical takeaway is that disposable sensors are increasingly viewed not as a luxury but as a defensible standard of care whenever you abrade the skin.
Glossary
additional precautions: contact, droplet, and airborne measures used in addition to routine practices for particular pathogens or clinical presentations.
antiseptic: a substance applied to living tissue to destroy microorganisms or inhibit their spread.
aseptic: free from disease-causing microorganisms such as harmful bacteria, viruses, and fungi; a less strict standard than sterile.
available chlorine: the concentration of active hypochlorite in a bleach solution, expressed in parts per million, which determines its disinfecting power and declines as the solution ages.
chain of transmission: the six linked conditions—infectious agent, reservoir, portal of exit, mode of transmission, portal of entry, and susceptible host—all of which must be present for an infection to spread.
chloriding: the process of depositing a silver chloride layer onto a silver surface, accomplished either electrically or by immersing the metal in a dilute bleach solution.
coated Ag/AgCl electrode: a silver sensor carrying an electroplated or chemically deposited silver chloride film only micrometers thick, which cleaning methods more aggressive than a tissue wipe will remove.
common vehicle transmission: a mode of transmission of infectious pathogens from a source that is common to all the cases of a specific disease.
contaminated sharps: used objects capable of penetrating the skin, including blunt-tip needles, which must be discarded without recapping into a puncture-resistant container.
critical: a Spaulding infection risk category for devices that enter sterile tissue or the vascular system, including sensors that puncture the skin; these require sterilization.
cross-contamination: the inadvertent transfer of microorganisms from one individual or site to another.
DC offset: the standing direct-current voltage difference between a sensor and its reference, which shifts when skin is broken or a sensor surface degrades, producing baseline drift.
disinfection: a process involving chemical agents or wet pasteurization that removes many microorganisms except for bacterial spores on inanimate objects.
electrode bridge: an unintended electrolyte connection between adjacent sensor sites, usually caused by spreading conductive gel, that makes two channels record nearly identical signals.
electrode impedance: the opposition that the sensor, conductive medium, and underlying tissue jointly present to the small test currents used to check a connection.
electrode polarization: the buildup of an opposing voltage at the metal-electrolyte junction as current passes through it, which distorts low-frequency and DC recordings.
extrinsic contamination: the introduction of microorganisms into a product during handling and use within the facility, as when a used applicator is returned to a shared container.
half-cell potential: the small steady voltage that develops wherever a metal contacts an electrolyte such as conductive paste; mismatched or unstable half-cell potentials produce baseline drift and noise.
healthcare-associated infection (HAI): an infection that a patient acquires during the course of receiving treatment for another condition within a healthcare setting.
HEPA filter: a high-efficiency particulate air filter that captures at least 99.97% of airborne particles 0.3 µm in diameter, the size that penetrates filter media most readily.
infection prevention and control (IPAC): the coordinated set of policies, practices, and physical measures a setting uses to prevent the transmission of microorganisms.
infectious agent: the bacterium, virus, or fungus capable of causing disease; the first link in the chain of transmission.
intermediate-level disinfectant: an agent that destroys vegetative bacteria including tubercle bacilli, along with fungi and most viruses, but not bacterial spores.
intrinsic contamination: contamination of a product during manufacture or shipping, before it reaches the facility.
low-level disinfectant: an agent that destroys most vegetative bacteria, lipid viruses, and some fungi, but neither tubercle bacilli nor bacterial spores.
mode of transmission: the route by which an infectious agent travels from its reservoir to a new host, whether by contact, droplet, or airborne spread.
N95 respirator: a tight-fitting mask that filters at least 95% of airborne particles and requires periodic fit-testing; used when infectious particles travel by the airborne route.
noncritical: a Spaulding infection risk category for sensors that contact intact skin but not mucous membranes.
non-intact skin: skin opened by dermatitis, cuts, abrasions, or chapping; preparing a site with any abrasive to lower impedance creates non-intact skin.
patient-dedicated equipment: reusable items assigned to a single individual for the duration of care rather than rotated among clients, which closes the cross-contamination pathway at its source.
personal protective equipment (PPE): gloves, masks, gowns, and eye protection, whose shared function is to interpose a barrier between infectious microorganisms and a person’s mucous membranes, skin, airway, and clothing.
portal of entry: the route by which an infectious agent gets into a new person, such as mucous membranes, non-intact skin, or the airway.
portal of exit: the route by which an infectious agent leaves its reservoir, such as the respiratory tract, broken skin, or a bodily fluid.
reservoir: the place where an infectious agent lives and multiplies, which may be a person, a piece of equipment, water, food, or a surface.
routine practices: the infection prevention and control measures used with every client during every contact, regardless of known diagnosis.
semi-critical: a Spaulding infection risk category for sensors that can contact mucous membranes or non-intact skin, including skin broken by abrasion; these require high-level disinfection.
single-use device (SUD): a device the manufacturer intends for one use on one client during one procedure, which may not be reprocessed and applied to another client.
sintered Ag/AgCl electrode: a sensor pressed from a homogeneous powder mixture of silver and silver chloride and baked into a pellet, so that chloride runs through its full thickness and it tolerates repeated cleaning.
skin potential artifact: slow, large voltage shifts arising as sweat gland activity and skin hydration change the standing potential across the epidermis.
Spaulding classification system: a scheme that places reusable medical instruments or devices into three categories of ascending infection risk.
sterile: free of all living microorganisms; a stricter standard than aseptic, which refers only to the absence of disease-causing microorganisms.
sterilization: a process that destroys all microbial life using chemical or physical methods.
susceptible host: a person whose immune status, age, or underlying condition leaves them vulnerable to a particular infectious agent.
Test Yourself on ClassMarker
Click on the ClassMarker logo below to take a 10-question exam over this entire unit.

Review Flashcards on Quizlet
Click on the Quizlet logo to review our chapter flashcards.

Visit the BioSource Software Website
BioSource Software offers Physiological Psychology, which satisfies BCIA's Physiological Psychology requirement, and Neurofeedback100, which provides extensive multiple-choice testing over the Biofeedback Blueprint.

Assignment
Now that you have completed this module, identify ways to improve infection mitigation in your clinical practice. Consider the screening procedures, hand hygiene protocols, equipment disinfection methods, and Spaulding classification principles covered in this unit, and evaluate how each applies to your specific setting.
References
Albert, N. M., Bena, J. F., Ciudad, C., Keleekai-Brapoh, N., Morrison, S. L., Rice, K., Slifcak, E., & Runner, J. C. (2018). Contamination of reusable electroencephalography electrodes: A multicenter study. American Journal of Infection Control, 46(12), 1360–1364. https://doi.org/10.1016/j.ajic.2018.05.021
Albert, N. M., Bena, J. F., Keleekai-Brapoh, N., Rice, K., Runner, J. C., Ciudad, C., Morrison, S. L., & Slifcak, E. (2019). Reusable electroencephalography electrodes: Variability in cleaning and reprocessing practices. The Neurodiagnostic Journal, 59(1), 45–57. https://doi.org/10.1080/21646821.2019.1571357
Alschuler, D. M., Tenke, C. E., Bruder, G. E., & Kayser, J. (2014). Identifying electrode bridging from electrical distance distributions: A survey of publicly-available EEG data using a new method. Clinical Neurophysiology, 125(3), 484–490. https://doi.org/10.1016/j.clinph.2013.08.024
American Institute of Ultrasound in Medicine. (2025). Guidelines for cleaning and preparing external- and internal-use ultrasound transducers and equipment between patients as well as safe handling and use of ultrasound coupling gel, 2025 revision. https://www.aium.org/resources/official-statements/view/guidelines-for-cleaning-and-preparing-external--and-internal-use-ultrasound-transducers-and-equipment-between-patients-as-well-as-safe-handling-and-use-of-ultrasound-coupling-gel
ASET–The Neurodiagnostic Society. (2016). ASET position statement on skin safety during EEG procedures – A guideline to improving outcome. The Neurodiagnostic Journal, 56(4), 296–300. https://doi.org/10.1080/21646821.2016.1246336
BIOPAC Systems. (n.d.). Are there cleaning guidelines for reusable transducers and electrodes? https://www.biopac.com/knowledge-base/cleaning-guidelines/
Bonner, A. M., & Davidson, P. (2020). Infection prevention: 2020 review and update for neurodiagnostic technologists. The Neurodiagnostic Journal, 60(1), 11–35. https://doi.org/10.1080/21646821.2020.1701341
Brain Products. (n.d.). How to clean the actiCAP slim. https://www.brainproducts.com/support-resources/how-to-clean-the-acticap/
Centers for Disease Control and Prevention. (2002). Guideline for hand hygiene in health-care settings. MMWR Recommendations and Reports, 51(RR-16), 1–45. https://www.cdc.gov/mmwr/pdf/rr/rr5116.pdf
Centers for Disease Control and Prevention. (2020). Introduction, methods, definition of terms: Guideline for disinfection and sterilization in healthcare facilities (2008). https://www.cdc.gov/infectioncontrol/guidelines/disinfection/introduction.html
Centers for Disease Control and Prevention. (2024a). Clinical safety: Hand hygiene for healthcare workers. U.S. Department of Health and Human Services. https://www.cdc.gov/clean-hands/hcp/clinical-safety/index.html
Centers for Disease Control and Prevention. (2024b). Preventing unsafe injection practices. https://www.cdc.gov/injection-safety/hcp/clinical-safety/index.html
Centers for Disease Control and Prevention. (2024c). About handwashing. https://www.cdc.gov/clean-hands/about/index.html
CS Medical. (2024, November 6). What should reprocessing really look like? Part 1. https://csmedicalllc.com/news/what-should-reprocessing-really-look-like
Dolan, S. A., Littlehorn, C., Glodé, M. P., Dowell, E., Xavier, K., Nyquist, A. C., & Todd, J. K. (2012). Association of Bacillus cereus infection with contaminated alcohol prep pads. Infection Control & Hospital Epidemiology, 33(7), 666–671. https://doi.org/10.1086/666334
Ecolab. (2022, June 9). Classifying the decontamination process. https://healthcare-au.ecolab.com/classifying-the-decontamination-process/
eemagine Medical Imaging Solutions. (2017). waveguard connect EEG cap & accessories user guide (Rev. 5). https://bio-medical.com/media/support/waveguard-connect-user-guide-en-us-rev5-2017-03-20-01.pdf
Electro-Cap International. (n.d.). Electro-Cap instruction manual. http://images.shoutwiki.com/tagsync/8/82/ELECTRO_CAP_CLEANING_INSTR_MANUAL.pdf
Ferree, T. C., Luu, P., Russell, G. S., & Tucker, D. M. (2001). Scalp electrode impedance, infection risk, and EEG data quality. Clinical Neurophysiology, 112(3), 536–544. https://doi.org/10.1016/s1388-2457(00)00533-2
FitzGerald, S. (2025). Good practice: Reusable medical device reprocessing. College of Physiotherapists of Alberta. https://www.cpta.ab.ca/news-and-updates/news/good-practice-reusable-medical-device-reprocessing/
Górecka, J., & Makiewicz, P. (2019). The dependence of electrode impedance on the number of performed EEG examinations. Sensors, 19(11), Article 2608. https://doi.org/10.3390/s19112608
Hagedorn, D. (2014). Infection risk mitigation for biofeedback providers. Biofeedback, 42(3), 93–95. https://doi.org/10.5298/1081-5937-42.3.06
Hagedorn, D. (2019). Infection risk mitigation for biofeedback providers. In D. Moss & F. Shaffer (Eds.), Physiological recording technology and applications in biofeedback and neurofeedback (pp. 334–336). Association for Applied Psychophysiology and Biofeedback.
Health PEI, Quality and Patient Safety Division. (2025). Spaulding’s classification [Fact sheet]. Government of Prince Edward Island. https://src.healthpei.ca/sites/src.healthpei.ca/files/DidYouKnowSpauldingsClassification.pdf
Hudson, M. J., Park, S. C., Mathers, A., Parikh, H., Glowicz, J., Dar, D., Nabili, M., LiPuma, J. J., Bumford, A., Pettengill, M. A., Sterner, M. R., Jr., Paoline, J., Tressler, S., Peritz, T., Gould, J., Hutter, S. R., Moulton-Meissner, H., & Perkins, K. M. (2022). Outbreak of Burkholderia stabilis infections associated with contaminated nonsterile, multiuse ultrasound gel—10 states, May–September 2021. MMWR Morbidity and Mortality Weekly Report, 71(48), 1517–1521. https://doi.org/10.15585/mmwr.mm7148a3
Hutchinson, J., Runge, W., Mulvey, M., Norris, G., Yetman, M., Valkova, N., Villemur, R., & Lépine, F. (2004). Burkholderia cepacia infections associated with intrinsically contaminated ultrasound gel: The role of microbial degradation of parabens. Infection Control & Hospital Epidemiology, 25(4), 291–296. https://doi.org/10.1086/502394
Kappenman, E. S., & Luck, S. J. (2010). The effects of electrode impedance on data quality and statistical significance in ERP recordings. Psychophysiology, 47(5), 888–904. https://doi.org/10.1111/j.1469-8986.2010.01009.x
Lindsley, W. G., Derk, R. C., Coyle, J. P., Martin, S. B., Jr., Mead, K. R., Blachere, F. M., Beezhold, D. H., Brooks, J. T., Boots, T., & Noti, J. D. (2021). Efficacy of portable air cleaners and masking for reducing indoor exposure to simulated exhaled SARS-CoV-2 aerosols—United States, 2021. MMWR Morbidity and Mortality Weekly Report, 70(27), 972–976. https://doi.org/10.15585/mmwr.mm7027e1
McGinty, R., & Balatskaya, A. (2023, June 20). Stereotactic EEG, intraoperative electrocorticography and brief potentially ictal rhythmic discharges (BIRDs). European Academy of Neurology. https://www.ean.org/research/resources/neurology-updates/detail/stereotactic-eeg-intraoperative-electrocorticography-and-brief-potentially-ictal-rhythmic-discharges-birds
Moss, D., Hagedorn, D., Combatalade, D., & Neblett, R. (2019). Care for biofeedback and neurofeedback instrumentation. In D. Moss & F. Shaffer (Eds.), Physiological recording technology and applications in biofeedback and neurofeedback (pp. 337–347). Association for Applied Psychophysiology and Biofeedback.
Nakashima, A. K., McCarthy, M. A., Martone, W. J., & Anderson, R. L. (1987). Epidemic septic arthritis caused by Serratia marcescens and associated with a benzalkonium chloride antiseptic. Journal of Clinical Microbiology, 25(6), 1014–1018. https://doi.org/10.1128/jcm.25.6.1014-1018.1987
Nanosonics. (n.d.). Spaulding classification. Retrieved July 26, 2026, from https://www.nanosonics.us/infection-prevention-education/spaulding-classification
Nasser, R. M., Rahi, A. C., Haddad, M. F., Daoud, Z., Irani-Hakime, N., & Almawi, W. Y. (2004). Outbreak of Burkholderia cepacia bacteremia traced to contaminated hospital water used for dilution of an alcohol skin antiseptic. Infection Control & Hospital Epidemiology, 25(3), 231–239. https://doi.org/10.1086/502384
National Institute for Occupational Safety and Health. (2024). Improving air cleanliness. Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/ventilation/prevention/air-cleanliness.html
Neuman, M. R. (2010). Biopotential electrodes. In J. G. Webster (Ed.), Medical instrumentation: Application and design (4th ed., pp. 189–240). John Wiley & Sons.
Occupational Safety and Health Administration. (n.d.). Bloodborne pathogens (29 C.F.R. § 1910.1030). U.S. Department of Labor. https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1030
Oleszkowicz, S. C., Chittick, P., Russo, V., Keller, P., Sims, M., & Band, J. (2012). Infections associated with use of ultrasound transmission gel: Proposed guidelines to minimize risk. Infection Control & Hospital Epidemiology, 33(12), 1235–1237. https://doi.org/10.1086/668430
Ontario Agency for Health Protection and Promotion (Public Health Ontario), Provincial Infectious Diseases Advisory Committee. (2025). Routine practices and additional precautions in all health care settings (3rd ed., 4th rev.). King’s Printer for Ontario. https://www.publichealthontario.ca/-/media/Documents/B/2012/bp-rpap-healthcare-settings.pdf Contains information licensed under the Open Government Licence – Ontario.
OpenBCI. (n.d.). Gel electrode cap guide. https://docs.openbci.com/AddOns/Headwear/ElectrodeCap/
Ouchida, S., Nikpour, A., Fairbrother, G., & Senturias, M. (2019). EEG electrode-induced skin injury among adult patients undergoing ambulatory EEG monitoring. The Neurodiagnostic Journal, 59(4), 219–231. https://doi.org/10.1080/21646821.2019.1660548
Reducing the risk of infection with disposable EEG electrodes. (2019, January 22). Infection Control Today. https://www.infectioncontroltoday.com/view/reducing-risk-infection-disposable-eeg-electrodes
Rutala, W. A., Weber, D. J., & Healthcare Infection Control Practices Advisory Committee. (2008). Guideline for disinfection and sterilization in healthcare facilities, 2008. https://www.cdc.gov/infectioncontrol/pdf/guidelines/disinfection-guidelines.pdf
Shah, A. K., & Mittal, S. (2014). Invasive electroencephalography monitoring: Indications and presurgical planning. Annals of Indian Academy of Neurology, 17(Suppl. 1), S89–S94. https://doi.org/10.4103/0972-2327.128668
Siegel, J. D., Rhinehart, E., Jackson, M., Chiarello, L., & Healthcare Infection Control Practices Advisory Committee. (2007). 2007 guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. Centers for Disease Control and Prevention. https://www.cdc.gov/infection-control/hcp/isolation-precautions/
Sinha, S. R., Sullivan, L., Sabau, D., San-Juan, D., Dombrowski, K. E., Halford, J. J., Hani, A. J., Drislane, F. W., & Stecker, M. M. (2016). American Clinical Neurophysiology Society Guideline 1: Minimum technical requirements for performing clinical electroencephalography. Journal of Clinical Neurophysiology, 33(4), 303–307. https://doi.org/10.1097/WNP.0000000000000308
Sohrt, A., Mærkedahl, A., & Padula, W. V. (2019). Cost-effectiveness analysis of single-use EEG cup electrodes compared with reusable EEG cup electrodes. PharmacoEconomics Open, 3(2), 265–272. https://doi.org/10.1007/s41669-018-0090-3
Spratt, H. G., Jr., Levine, D., & Tillman, L. (2014). Physical therapy clinic therapeutic ultrasound equipment as a source for bacterial contamination. Physiotherapy Theory and Practice, 30(7), 507–511. https://doi.org/10.3109/09593985.2014.900836
Tallgren, P., Vanhatalo, S., Kaila, K., & Voipio, J. (2005). Evaluation of commercially available electrodes and gels for recording of slow EEG potentials. Clinical Neurophysiology, 116(4), 799–806. https://doi.org/10.1016/j.clinph.2004.10.001
U.S. Environmental Protection Agency. (2025). EPA's registered antimicrobial products effective against Clostridioides difficile spores (List K). https://www.epa.gov/pesticide-registration/epas-registered-antimicrobial-products-effective-against-clostridioides
U.S. Food and Drug Administration. (2024). Reprocessing single-use medical devices: Information for health care facilities. https://www.fda.gov/medical-devices/products-and-medical-procedures/reprocessing-single-use-medical-devices-information-health-care-facilities
Vancouver Coastal Health. (n.d.). Spaulding classification of equipment & medical devices. Infection Prevention and Control. Retrieved July 26, 2026, from https://ipac.vch.ca/
Vanhatalo, S., Voipio, J., & Kaila, K. (2005). Full-band EEG (FbEEG): A new standard for clinical electroencephalography. Clinical EEG and Neuroscience, 36(4), 311–317. https://doi.org/10.1177/155005940503600411
Warner Instruments. (2009). Chloriding Ag/AgCl electrodes: Disk, pellet, or wire (Rev. 090727). https://www.warneronline.com/sites/default/files/2018-09/Chloriding%20Ag-AgCl%20electrodes%20(090728).pdf
Weber, D. J., Rutala, W. A., & Sickbert-Bennett, E. E. (2007). Outbreaks associated with contaminated antiseptics and disinfectants. Antimicrobial Agents and Chemotherapy, 51(12), 4217–4224. https://doi.org/10.1128/AAC.00138-07
World Health Organization. (2009). Glove use information leaflet. https://cdn.who.int/media/docs/default-source/integrated-health-services-(ihs)/infection-prevention-and-control/hand-hygiene/tools/glove-use-information-leaflet.pdf
World Health Organization. (2018). Table 3.3.3, Spaulding classification of equipment decontamination. In Global guidelines for the prevention of surgical site infection (2nd ed.). https://www.ncbi.nlm.nih.gov/books/NBK536426/table/ch3.tab7/
World Health Organization. (2025, May 5). Gloves do not replace hand hygiene – reminder from WHO. https://www.who.int/news/item/05-05-2025-gloves-do-not-replace-hand-hygiene---reminder-from-who
Wuhan Greentek. (n.d.). Cleaning and disinfecting of Greentek sintered Ag-AgCl electrode cap. https://pdf.medicalexpo.com/pdf/wuhan-greentek/cleaning-disinfecting-greentek-sintered-ag-agcl-electrode-cap/118176-242584.html
Return to Top