
Professional Standards
What You Will Learn in This Chapter
Ethics are at the heart of responsible practice. This chapter introduces you to the professional standards and ethical principles that guide qEEG and neurofeedback providers, from protecting client welfare and maintaining competence to navigating complex situations like dual relationships, scope of practice boundaries, and copyright compliance.
You will explore the ethical framework that governs certification, learn how to mitigate infection risks, understand confidentiality obligations, and discover why certification matters for both you and your clients.
Whether you are a beginning practitioner seeking certification, a licensed clinician adding qEEG to your practice, or a seasoned provider refreshing your knowledge, this chapter equips you with the ethical foundation that protects both your clients and the credibility of our field.
IQCB Blueprint Coverage: This unit addresses Ethics and Professional Conduct (VIII. Ethics), Scope of Practice and Competence (VIII. Ethics), and Confidentiality and Protection of Client Rights (VIII. Ethics).
Professional ethical standards help educators, researchers, and practitioners anticipate and identify ethical dilemmas and make choices that maintain one's professional integrity and protect our clients and profession (Striefel, 2003).

Learning Objectives
After completing this section, you will be able to:
Explain why ethical standards protect the public, the profession, and the individual practitioner.
Distinguish scope of practice from competence, and describe why both are required for ethical practice.
Describe the difference between mentoring and supervision, and identify unacceptable supervision arrangements.
Apply confidentiality rules and their legal limitations to realistic clinical situations.
Obtain informed consent and, with minors, assent, in a way that addresses uncertainty and realistic expectations.
Select equipment responsibly, recognize off-label use, and apply infection risk mitigation procedures.
Identify conflicts of interest and multiple relationships, and describe how to manage them.
Describe certification requirements and explain how certification differs from licensure.
Evaluate emerging digital ethics issues in privacy, cybersecurity, telehealth, wearables, and artificial intelligence.
What This Unit Covers
This unit supports the requirement that applicants complete 3 hours of ethics education.

This unit covers The Purpose of Ethics, Diversity and Cultural Awareness, Responsibility, Competence, Scope of Practice, Mentoring vs. Supervision, Ethical Standards, Public Statements, Confidentiality, Protection of Client Rights and Welfare, Biofeedback Equipment Selection, Infection Risk Mitigation, Professional Relationships, Research with Humans and Animals, Adherence to Professional Standards, Ethics Complaint Procedures, and Biofeedback Certification International Alliance (BCIA). It concludes with Emerging Ethical Issues in the Digital Age, covering digital privacy, cybersecurity, telehealth, wearables, and artificial intelligence.
Please click on the button below to hear a full-length lecture.
Donald Moss, PhD, contributed extensively to chapter content from his AAPB webinar, Professional Ethics and Practice Standards in Biofeedback and Neurofeedback.

Read Shaffer and Schwartz's "Entering the Field and Assuring Competence" in Biofeedback: A Practitioner's Guide (4th ed.) for an in-depth discussion of the challenges of entering the field and maintaining competence.
The Purpose of Ethics
In this section, we'll explore why ethical standards matter for neurofeedback practice, examining how they protect the public, the profession, and individual practitioners. We'll discuss the relationship between personal integrity and professional ethics, and introduce the concept of beneficence, acting in clients' best interests, as a cornerstone of ethical practice.
Ethical Standards and the Reputation of the Profession of Neurofeedback
Biofeedback providers recognize that their effectiveness and success as professionals, and the credibility of the biofeedback field, depend on their professional conduct. Each time a biofeedback or behavioral health professional is charged with serious violations of ethical behavior, the field is also tarnished, and potential patients and their family members lose their readiness to trust in professional care (Moss, 2020).
Ethical codes express our stakeholders' core values.
Listen to a mini-lecture on Core Values

Professional Ethics Reflect Personal Integrity
Ethical practices are in the first place aspirational; they reflect the kind of professional one aspires to become. Responsible behavior in professional life should express personal, social, and religious values. Compassion and empathy for one's fellow humans, who come for help with suffering, draws individuals to professional practice. Professionals with diminished empathy due to 'burnout' and 'compassion fatigue' are at greater risk for ethical transgressions. Burnout is a widespread problem in the helping professions. Compassion fatigue is one product of using up or depleting our capacities for caring. Maintaining healthy self-care practices is critical in avoiding compassion fatigue. Difficulties in establishing rapport and mutual empathy in treatment relationships are also a challenge for professionals. When patients do not feel strong rapport and trust in their provider, they are more likely to file complaints (Moss, 2020).
Beneficence in Neurofeedback Practice
The principle of beneficence, actively working to benefit clients and avoid harm, guides every decision in biofeedback practice. Providers strive to protect their clients' welfare by appreciating their impact on clients' lives and by recognizing and avoiding potential conflicts of interest (Moss, 2020). This foundational principle shapes how we interact with clients, design treatment plans, and navigate complex clinical situations.
The ethical responsibilities of biofeedback providers and their staff are collectively defined by the licensing act under which they (or their supervisors) operate, their profession, and the BCIA's Professional Standards and Ethical Principles of Biofeedback (10th rev., adopted May 2, 2026). The BCIA's PSEP represents the minimum ethical standards expected of its applicants and certificants. Physicians who provide biofeedback must also follow medical ethical guidelines, while psychologists must adhere to the Ethical Standards of the APA (Moss, 2013). Understanding these overlapping frameworks is essential for maintaining ethical practice across diverse professional backgrounds.
Providers deliver biofeedback services within a context of legal statutes, cultural norms, professional standards, and ethical codes that may vary across nations, cultures, and communities. These expectations may conflict with each other, creating ethical dilemmas that require careful navigation. For example, the American Psychological Association's (2017a) Ethics Code addresses dual relationships, situations where a provider and client share multiple roles.
Standard 3.05(a) directs psychologists to refrain from entering a multiple relationship when it could reasonably be expected to impair their objectivity, competence, or effectiveness, or to risk exploitation or harm to the person, while stating in the same paragraph that multiple relationships which would not reasonably be expected to have those effects are not unethical. A psychologist applying that standard might therefore decline a community expectation that "healers" visit the client's family and share their religious rituals, or might accept it after documenting a reasoned judgment that the risk of harm is low (Moss, 2013). Recognizing these potential conflicts helps practitioners prepare for difficult decisions.
Since ethical guidelines can never anticipate all contingencies that providers may encounter, practitioners should consult with their licensing body, professional association, and colleagues when they reach a choice point and are uncertain about future conduct. This collaborative approach to ethical decision-making strengthens practice and protects both clients and providers. Unfortunately, the most severe ethical infractions, like sexual relationships with clients, often involve intentional violations of clear prohibitions rather than difficult judgment calls.
Ethical standards serve three critical purposes: protecting the public from harm, maintaining the credibility of biofeedback as a profession, and guiding individual practitioners toward integrity. Personal values, particularly compassion and empathy, form the foundation of professional ethics, though burnout and compassion fatigue can erode these qualities. Providers must navigate multiple, sometimes conflicting, ethical frameworks from licensing boards, professional associations, and BCIA while maintaining beneficence as their guiding principle. When facing ethical uncertainty, consultation with colleagues and governing bodies provides essential guidance for making sound decisions.
Check Your Understanding
- What three purposes do professional ethical standards serve?
- How can burnout and compassion fatigue raise a practitioner's risk of ethical transgression?
- Which overlapping ethical frameworks must a licensed provider who offers biofeedback satisfy?
- What does beneficence require of you when a client's goals conflict with your financial interests?
Enforcement of Ethical Standards
This section examines how ethical standards are enforced within neurofeedback practice. We'll explore BCIA's role in responding to ethical complaints, the limitations of its authority, and the investigative approach that skilled clinicians use when patients present with unusual or treatment-resistant symptoms.
When a licensing body or court substantiates a charge of ethical misconduct, BCIA may take disciplinary action against a certificant. However, BCIA does not have the legal authority to compel testimony or the submission of documents, which means it must often wait for a licensing body or court to investigate and reach a decision before acting. Applicants who have lost or surrendered their license may not be certified until their license is restored.
BCIA has no enforcement role when an individual charged with an ethical violation is neither a certificant nor an applicant. This limitation underscores the importance of working within regulated professional frameworks where multiple oversight mechanisms exist. The absence of BCIA jurisdiction in such cases highlights why proper licensure and supervision are essential components of ethical practice in biofeedback.
BCIA's enforcement authority is limited to its certificants and applicants, and depends on investigations conducted by licensing bodies or courts. The organization cannot independently compel evidence but responds to substantiated findings with disciplinary action. This system emphasizes the critical role of state licensing boards as the primary enforcers of professional standards, with BCIA providing an additional layer of accountability for certified practitioners.
Check Your Understanding
- Whom does BCIA have authority over, and whom can it not reach?
- Why must BCIA often wait for a licensing body or court before acting on a complaint?
- What happens to certification when an applicant has lost or surrendered a license?
- Why are state licensing boards described as the primary enforcers of professional standards?
The Investigative Clinician: Beyond Initial Presentations
This section explores an essential clinical skill that extends beyond ethics into diagnostic excellence. We'll examine when and why clinicians must shift from standard diagnostic approaches to investigative thinking, focusing on identifying underlying causes that conventional frameworks might miss. This material was inspired by Dr. Ron Swatzyna, Director and Chief Scientist of the Houston Neuroscience Brain Center.

When patients present with significant sudden-onset symptoms or prove resistant to conventional treatments, clinicians must transition from diagnostician to detective. Such symptoms may be behavioral, emotional, cognitive, or somatic, with their significance judged within the context of each particular case. The emergence of abrupt changes, particularly in children and adolescents, should trigger immediate consideration of underlying medical, environmental, or infectious causes rather than immediate psychiatric diagnosis and medication trials. This investigative mindset represents a fundamental shift from treating symptoms to identifying root causes.
Several clinical scenarios warrant deeper investigation beyond standard protocols. The sudden appearance of new symptoms, particularly in previously stable or healthy individuals, demands scrutiny. Failure to respond to two adequate medication trials suggests something beyond the assumed diagnosis may be at work. Unexpected resistance to properly administered biofeedback or neurofeedback interventions similarly signals the need for broader investigation. In these cases, the standard approach of treating based on DSM-5 diagnostic criteria may obscure crucial underlying pathology and its etiology, potentially leading to years of ineffective treatment.
The EEG serves as a particularly valuable tool in this investigative process, providing objective evidence that can reveal hidden pathology. Findings such as diffuse slowing, a generalized reduction in brain wave frequency, intermittent epileptiform discharges, or excessive beta activity are nonspecific. They can accompany neuroinflammation or toxic exposure, but they also accompany drowsiness, medication effects, metabolic disturbance, and artifact, and they appear in people in whom no pathology is ever found. An EEG does not itself reveal a trigger such as mold exposure, chemical toxicity, or an infectious process; what it can do is raise the question, so that history-taking, physical examination, and laboratory work by a physician can look for one. EEG patterns may also index changes in sleep quality, medication effects, or substance use, while variations in socially-mediated supports or stressors sometimes correlate with observable EEG changes.
Case evidence supports this investigative approach across diverse clinical presentations. For instance, clinicians have reported apparent treatment-resistant depression that improved after an indoor mold exposure was identified and remediated, a presentation sometimes described as chronic inflammatory response syndrome (CIRS). CIRS is a proposed diagnostic construct rather than an established one; it appears in neither the DSM nor the ICD, and several professional bodies have questioned the evidence for it, so the provider's role is to notice a possible exposure and refer for medical evaluation, not to assign or treat that diagnosis.
Sudden-onset obsessive-compulsive symptoms might prompt evaluation for PANDAS or PANS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections; Pediatric Acute-onset Neuropsychiatric Syndrome) or for autoimmune encephalitis. These are clinically defined syndromes whose hypothesized postinfectious autoimmune mechanism remains under investigation; where a physician makes such a diagnosis, immunological or antimicrobial treatment may be added to standard OCD care rather than necessarily replacing it. Similarly, new-onset attention deficits resistant to standard treatments might result from environmental toxin exposure or nutrient deficiencies rather than primary ADHD, necessitating environmental or nutritional interventions instead of stimulant medication.
The investigative clinician approach requires shifting from symptom-based diagnosis to root-cause investigation when patients present with sudden-onset symptoms or treatment resistance. EEG findings are nonspecific, but they can raise the question of neuroinflammation, toxic exposure, or other underlying conditions that DSM-5 criteria alone might miss. This paradigm emphasizes treating pathophysiology rather than diagnostic labels, potentially preventing years of ineffective symptom management. While this approach requires additional time and resources initially, it can lead to more effective and lasting therapeutic outcomes by addressing actual causes rather than managing surface symptoms.
Check Your Understanding
- What client presentations should prompt you to shift from symptom-based diagnosis to root-cause investigation?
- What kinds of underlying conditions can EEG findings point toward that DSM-5 criteria alone might miss, and why are those findings nonspecific?
- What is the cost of the investigative approach, and what is the argument that it is worth paying?
- Why does treating pathophysiology rather than a diagnostic label change the treatment plan?
Diversity and Cultural Awareness
In this section, we'll examine how cultural context shapes ethical practice in biofeedback. We'll explore the challenges of providing services across diverse communities and navigate conflicts between professional ethical standards and community norms.
Since professionals provide biofeedback services across diverse communities, cultures, nations, and geographic regions, they must respect the norms of the cultures they serve and recognize the diversity in legal codes, professional standards, and ethical principles. This cultural competence extends beyond simple awareness to active engagement with how different communities understand health, healing, and the therapeutic relationship. Practitioners working in diverse settings must balance maintaining professional standards with showing genuine respect for cultural traditions.
Listen to Dr. Moss discuss Diversity and Cultural Awareness © Association for Applied Psychophysiology and Biofeedback.
Providers may have to resolve conflicts between the ethical standards of their professional society and community norms. For example, while the American Psychological Association's Ethics Code directs psychologists to avoid multiple relationships, such as a friendship with a client, that could reasonably be expected to impair objectivity or risk exploitation or harm, community norms may require family visits and participation in religious rituals intended to heal the client (American Psychological Association, 2017a; Moss, 2013). Navigating these conflicts requires cultural humility, consultation with colleagues familiar with the community, and careful consideration of how to honor both professional obligations and cultural expectations.

Graphic © Rawpixel.com/Shutterstock.com.
The American Psychological Association's (2017b) Multicultural Guidelines are aspirational rather than enforceable standards, and they encourage practitioners to recognize that culture influences an individual's worldview; develop sensitivity to their own cultural identities; use culturally appropriate assessments, interventions, and consultations; understand the socio-cultural contexts that impact individuals' lives; and consider historical and societal barriers that marginalized groups have faced.
This guideline applies to neurofeedback and biofeedback. Assessment and treatment protocols should be consistent with the best available research. The first-line EEG standard chosen for comparison (such as the BrainDX database) should be appropriate for this individual's background, including national and regional influences, race, socioeconomic status, and immigration history (Moss, 2020).
Likewise, neurofeedback protocols themselves should be research-based and appropriate. Normative data for parameters such as the EEG, EMG, skin conductance, heart rate and heart rate variability, skin temperature, and respiration rate may not adequately represent minorities, and practitioners should be aware that skin color influences optical sensors for PPG and pulse oximetry (Moss, 2020).
Cultural awareness in neurofeedback practice requires more than surface-level knowledge; it demands active respect for diverse legal codes, professional standards, and community norms. Practitioners must be prepared to navigate conflicts between professional ethical standards and cultural expectations, particularly around dual relationships and healing practices. This navigation requires cultural humility, consultation, and careful balancing of professional obligations with genuine cultural respect.
Check Your Understanding
- Why is surface-level cultural knowledge insufficient for ethical practice?
- Give an example of a conflict between a professional ethical standard and a community expectation.
- What does cultural humility add that cultural knowledge alone does not?
- Whom should you consult when a cultural expectation appears to conflict with your ethics code?
Responsibility
This section explores the multifaceted nature of professional responsibility in biofeedback. We'll examine how individual practitioners' actions shape the field's credibility, discuss the importance of informed consent for experimental treatments, and explore obligations to clients, referring professionals, and the broader healthcare community.
One of the most severe challenges to biofeedback is its credibility, a reputation shaped by the competence and actions of each provider. Practitioners should acquire entry-level competence in biofeedback and then progressively expand their expertise through activities like continuing education. They must adhere to the ethical principles that govern their professional practice and accept personal responsibility for the consequences of their actions. This individual accountability extends beyond technical competence to encompass every interaction with clients, colleagues, and the public.
As practitioners, providers should deliver cost-effective services consistent with the highest professional standards. They should educate their clients, referring health professionals, and third-party payers about the rationale for assessment and training procedures, the strength of empirical support for a treatment, and its risks, costs, and benefits. They should always explain when a treatment is experimental, meaning it has limited research support, since this is crucial to informed consent, a written or verbal agreement to participate in treatment after full disclosure of relevant information, and is a frequent source of ethical complaints in biofeedback. Ideally, they should obtain written informed consent for their proposed treatment. Providers never recommend experimental treatments when an established, well-supported treatment is already available (Moss, 2013).
Providers should only suggest less-documented interventions after informing clients of the available treatment options and the empirical support for each. Then, they should obtain written informed consent for the experimental procedure. This transparency about evidence levels allows clients to make truly informed decisions about their care.
Practitioners strive to protect their clients' welfare by appreciating their impact on clients' lives and recognizing and avoiding potential conflicts of interest. They candidly communicate with clients about their progress and modify or discontinue training if clients fail to make progress. When clients require services outside their expertise, providers refer them to qualified professionals and never abandon them, meaning they ensure continuity of care even when transferring to another provider.

Referral, Consultation, and Supervision
When clients do not improve and require an intervention that a clinician is not qualified to provide, options include referral to a qualified provider or consultation with or supervision by a qualified professional.
As educators, practitioners help advance knowledge through research and encourage students to value knowledge, think critically and from an interdisciplinary perspective, be reflective thinkers, appreciate the strengths and limitations of competing perspectives, and objectively investigate the questions that concern them. Educators recognize their potential impact on students' professional development and strive to provide accurate, complete, and objective information while encouraging free inquiry. Where scientific controversies exist, educators help students understand opposing positions and encourage them to evaluate each side's scientific support rather than simply advocating for one perspective.
Responsibility: Client Assessment
BCIA certificants should apply evidence-based assessment tools for every patient that are appropriate for their conditions (Moss et al., 2019). A physician with a headache should be evaluated like every other patient with this complaint. We begin with a thorough intake interview, a review of available records, and appropriate assessment and response to the available evidence. We must avoid any pressure to skip over the basics and move immediately to biofeedback or neurofeedback (Moss, 2020).
For more on best practices, click on the mini-lecture link.
Listen to a mini-lecture on Client Assessment
Responsibility: Documentation
Providers maintain appropriate records. Basic documentation requirements are covered by federal statutes (HIPAA), by state statute, and by professional licensing boards. Do not rely on memory for professional purposes (Moss, 2020).
Professional responsibility in biofeedback encompasses individual accountability, protection of the field's credibility, and commitment to evidence-based practice. Practitioners must provide transparent information about treatment options and obtain informed consent, particularly for experimental procedures. Educators bear responsibility for fostering critical thinking and presenting balanced views of scientific controversies. When clients fail to progress, providers must ensure appropriate referrals or consultation rather than persisting with ineffective approaches, recognizing that protecting client welfare sometimes means acknowledging the limits of one's expertise.
Check Your Understanding
- What must you disclose to a client before delivering an experimental procedure?
- What responsibility do educators carry when presenting scientific controversies?
- What are your obligations when a client is not improving and needs care outside your qualifications?
- Why does never abandoning a client require more than simply ending treatment?
Competence
This section examines what competence means in biofeedback practice and how practitioners develop and maintain it throughout their careers. We'll distinguish between entry-level competence and specialized expertise, explore the difference between knowing a technique and being qualified to treat specific populations, and discuss the ongoing education required to remain current in this evolving field.
Entry-Level Competence
New biofeedback practitioners should acquire entry-level competence in biofeedback and expand their expertise through activities like continuing education. BCIA certification ensures that the provider has completed training and mastered the skills and knowledge for entry-level competence and that the certificant also receives continuing education for re-certification (Moss, 2020).
Entry-level competence represents the foundation of professional practice, the minimum knowledge and skills needed to provide safe, effective biofeedback services. This baseline includes understanding fundamental psychophysiology, proper equipment operation, basic protocol implementation, and ethical practice standards. However, achieving entry-level competence is just the beginning of professional development, not its culmination.
Competence
Knowing a biofeedback technique is not sufficient when beginning to treat a new patient group. A professional who wishes to treat dissociative disorders, seizure disorders, or major mood disorders must also gain knowledge and experience, through appropriate education and supervision, of the condition and its management. Even expert application of biofeedback therapies for delicate conditions may trigger an emotional or medical crisis, and the therapist must know how to manage such events (Moss, 2020).
This distinction between technical competence and clinical competence is crucial for patient safety. A practitioner might be highly skilled at HRV biofeedback protocols yet unprepared to work with trauma survivors, where breathing exercises can trigger flashbacks or panic. Similarly, expertise in neurofeedback for attention problems doesn't automatically translate to competence treating complex PTSD or psychotic disorders, where neurofeedback might destabilize symptoms without proper safeguards and crisis management skills. Responsible practitioners recognize these boundaries and seek additional training before expanding into new clinical populations.
Maintaining Competence
Certificants progressively expand their expertise through continuing education, including teleseminars, massive open online courses (MOOCs), workshops, conference presentations, classes, reading journal articles and texts, mentoring, and their scholarship (Striefel, 2004). Providers consult experienced practitioners and obtain clinical supervision when expanding their clinical practice into new applications, equipment and software, and protocols (Moss, 2013). This ensures that they practice within the scope of their expertise, meaning they only provide services for which they have adequate training and experience (Shaffer & Schwartz, 2016).

Graphic © Eti Ammos/Shutterstock.com.
Competent providers critically evaluate biofeedback outcome studies, guide their practice using peer-reviewed findings, and strive to use the best practices in the field. They maintain a current understanding of the efficacy of biofeedback interventions and recognize where it is indicated and contraindicated, meaning where it should and should not be used. This evidence-based approach requires staying current with emerging research, understanding study quality and limitations, and translating research findings into clinical practice. AAPB's Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.) provides an authoritative evaluation of the efficacy of biofeedback applications (Moss, 2013).
Listen to a mini-lecture on Evidence-Based Practice

Providers comply with applicable laws and the ethical standards of their profession and certifying organization. They require a government license or credential to treat a medical or psychological disorder independently, meaning without supervision from another licensed professional. Those without a license or credential must obtain appropriate supervision to treat these disorders. Supervision, as legally defined by states within their practice acts, involves a qualified professional who oversees the unlicensed individual's delivery of services and assumes legal responsibility for provided care. Supervision should not be confused with consultation, where the licensed individual provides advice but has no legal responsibility for the unlicensed provider's actions.
Competence in biofeedback involves three distinct levels: entry-level competence (basic skills for safe practice), specialized competence (knowledge of specific conditions and populations), and maintained competence (staying current through ongoing education). Technical proficiency with biofeedback techniques is necessary but not sufficient; practitioners must also understand the conditions they're treating and how to manage potential crises. Maintaining competence requires critical evaluation of research, evidence-based practice, consultation when expanding into new areas, and adherence to legal requirements regarding licensure and supervision. This ongoing commitment to professional development protects both clients and practitioners.
Check Your Understanding
- Describe the three levels of competence and what distinguishes each.
- Why is technical proficiency with the equipment necessary but not sufficient?
- What activities maintain competence once entry-level competence is established?
- When should you obtain consultation or supervision rather than proceed on your own?
Scope of Practice
This section clarifies the critical distinction between what a practitioner is allowed to do legally (scope of practice) and what they're qualified to do professionally (competence). We'll explore how state laws define practice boundaries, examine the consequences of practicing outside one's scope, and discuss why this is often called "the elephant in the room" in biofeedback practice.
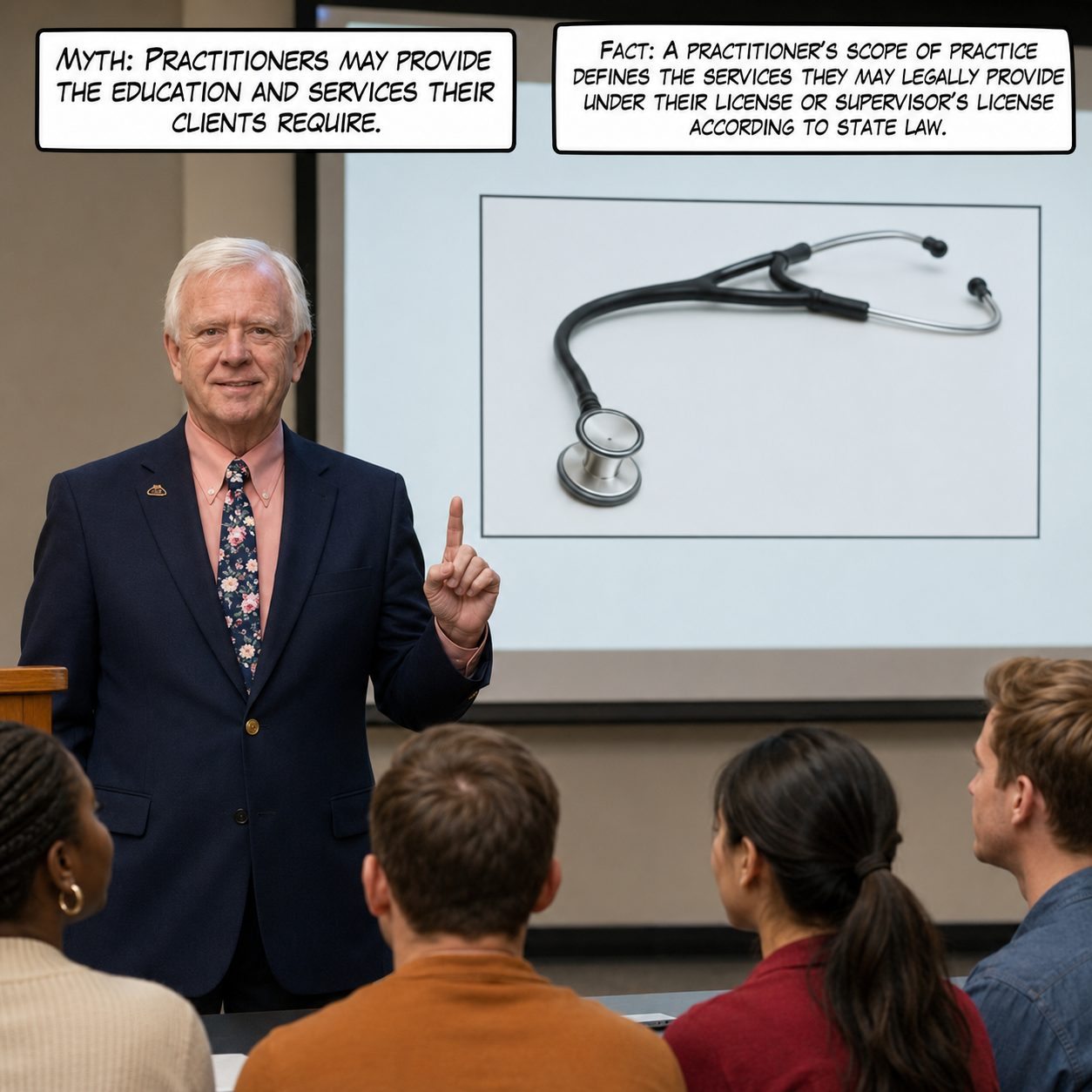
Practitioners' scope of practice, the specific services they may legally provide under their license or supervisor's license as defined by state law, establishes clear boundaries around professional activity. This legal framework varies significantly across states and professions, making it essential for practitioners to understand their specific jurisdictional requirements.

Compliance with Relevant Laws
Providers comply with applicable laws and the ethical standards of their profession and certifying organization. They require a government license or credential to treat a medical or psychological disorder independently. Those without a license or credential must obtain appropriate supervision to treat these disorders. BCIA certifies licensed practitioners to treat diagnosed disorders, technicians to treat diagnosed disorders under supervision, and non-licensed practitioners to apply biofeedback for relaxation, stress management, or optimal performance (Moss, 2020).
One clarification belongs alongside this summary. BCIA certification attests that a candidate has met education, training, and examination standards; it does not itself confer authority to treat. BCIA's own Professional Standards and Ethical Principles of Biofeedback states that certification is not a license to practice independently. The authority to assess and treat a diagnosed disorder comes from a government license and the scope of practice that license defines, and certification adds a field-specific credential on top of it.
Listen to Dr. Moss explain compliance © Association for Applied Psychophysiology and Biofeedback.
For example, in most states, psychologists may not make nutritional recommendations, and health coaches may not diagnose or treat medical or psychological disorders (Moss, 2013). Although BCIA certifies technicians to practice under supervision, their scope of practice is defined by their supervisor's scope of practice, meaning they can only provide services that their supervisor is legally authorized to oversee. Understanding these boundaries prevents legal and ethical violations that could harm both clients and practitioners (Moss, 2020).
Scope of practice is the largest elephant in the room, a pervasive issue that practitioners avoid discussing until problems arise. Until they face complaints, licensed practitioners rarely read the statutes that regulate their scope of practice and professional responsibilities (Hopkins, 2013). Unlicensed certificants may not understand how scope of practice applies to their activities or their supervisor's license limitations. Without an appropriate license, they may not even legally purchase FDA-regulated devices like electroencephalographs, a restriction that many practitioners discover only when attempting to acquire equipment. The restriction comes from the prescription-device labeling rule, 21 CFR 801.109, which limits sale and distribution to or on the order of a licensed practitioner; it binds the seller, while state practice acts determine who qualifies as such a practitioner.

Graphic © Aleksandr_Kuzmin/Shutterstock.com.
Scope vs. Competence
Licensure defines whether a procedure is allowed for a professional with a given license, the professional's scope of practice. The principle of competence requires that a practitioner also know and train to use a procedure and deal with a specific patient population. Responsible practitioners will practice within the limits of their competence/expertise. When undertaking new applications of biofeedback, it is essential to obtain training on the application and relevant techniques and seek supervision by a professional with experience in biofeedback treatment of this disorder or the use of this technique (Moss, 2020).
This distinction is critical: being legally allowed to provide a service doesn't mean you're qualified to do so. A licensed psychologist might legally be within their scope of practice to treat epilepsy with neurofeedback, but without proper training in seizure management and neurofeedback for epilepsy, they lack the competence to do so safely. Conversely, extensive training in a technique doesn't grant legal authority to use it outside one's licensure scope. Both scope and competence must align for ethical practice.
Scope of practice defines what practitioners are legally allowed to do, while competence defines what they're qualified to do; both must be present for ethical practice. State laws vary significantly in defining professional boundaries, making it essential for practitioners to understand their specific jurisdictional requirements. Many practitioners remain unaware of their scope limitations until facing complaints, creating significant professional risk. BCIA certification does not expand scope of practice; it only validates competence within the boundaries already established by licensure or supervision.
Check Your Understanding
- What is the difference between scope of practice and competence?
- Why does BCIA certification not expand your scope of practice?
- How does a supervisee's scope of practice relate to the supervisor's?
- Why do many practitioners discover their scope limits only after a complaint is filed?
Competence Beyond Licensure
This section examines the legal requirements for treating medical and psychological disorders independently. We'll explore BCIA's certification requirements, the consequences when licenses are suspended or lost, and why certification is not equivalent to licensure.
BCIA professionals who treat medical or psychological conditions must demonstrate professional competence as defined by applicable local, state, and national licensing/credentialing laws. BCIA certification becomes invalid when a license is suspended, revoked, or not renewed due to an investigation of a complaint, and the individual is not allowed to provide services under supervision. A professional may only apply for recertification after the license has been reinstated. This policy ensures that BCIA certification remains meaningful and tied to continued professional good standing.
It is illegal to treat medical or psychological conditions without appropriate supervision if you are not licensed or credentialed to do so. BCIA certification becomes invalid when a certificant loses and cannot replace appropriate supervision. An individual may only apply for recertification after documenting that appropriate supervision has been reestablished (BCIA, 2016). This requirement protects clients by ensuring that all treatment occurs within legally and ethically appropriate frameworks.
Practitioners accurately disclose their regionally-accredited degrees, training, specialty areas, experience, and their license or credential and certification status. Ethical providers recognize that participation in a membership organization does not imply competence and that certification is not a license for independent practice. This transparency allows clients and referral sources to make informed decisions about care. Misrepresenting credentials, even through omission or ambiguity, undermines trust and violates ethical standards.
Treating medical or psychological disorders requires either appropriate licensure or supervision by a licensed professional; BCIA certification alone does not authorize independent practice. When licenses are suspended or lost, BCIA certification becomes invalid until the license is restored. Practitioners must accurately represent their credentials and understand that membership in professional organizations does not establish competence. These requirements create a layered system of accountability that protects clients while supporting properly credentialed practitioners in maintaining ethical practice.
Check Your Understanding
- What two routes authorize a practitioner to treat medical or psychological disorders?
- What happens to BCIA certification when a license is suspended or lost?
- Why does membership in a professional organization not establish competence?
- How does the layered system of licensure, supervision, and certification protect clients?
Mentoring vs. Supervision
This section clarifies a critical distinction that many practitioners misunderstand: the difference between mentoring (an educational relationship) and supervision (a legally defined relationship with liability). We'll explore BCIA's requirements for each, examine why physical proximity matters for supervision, and discuss what makes supervision arrangements unacceptable.
BCIA requires mentoring as an educational process for individuals seeking BCIA certification. Graphic © fizkes/Shutterstock.com.

BCIA requires legal clinical supervision for individuals certified as technicians. Peer consultation with colleagues and consultation with area experts are recommended as lifelong strategies to assure the quality of care and to protect against potential patient complaints (Moss, 2020).
Mentoring Defined
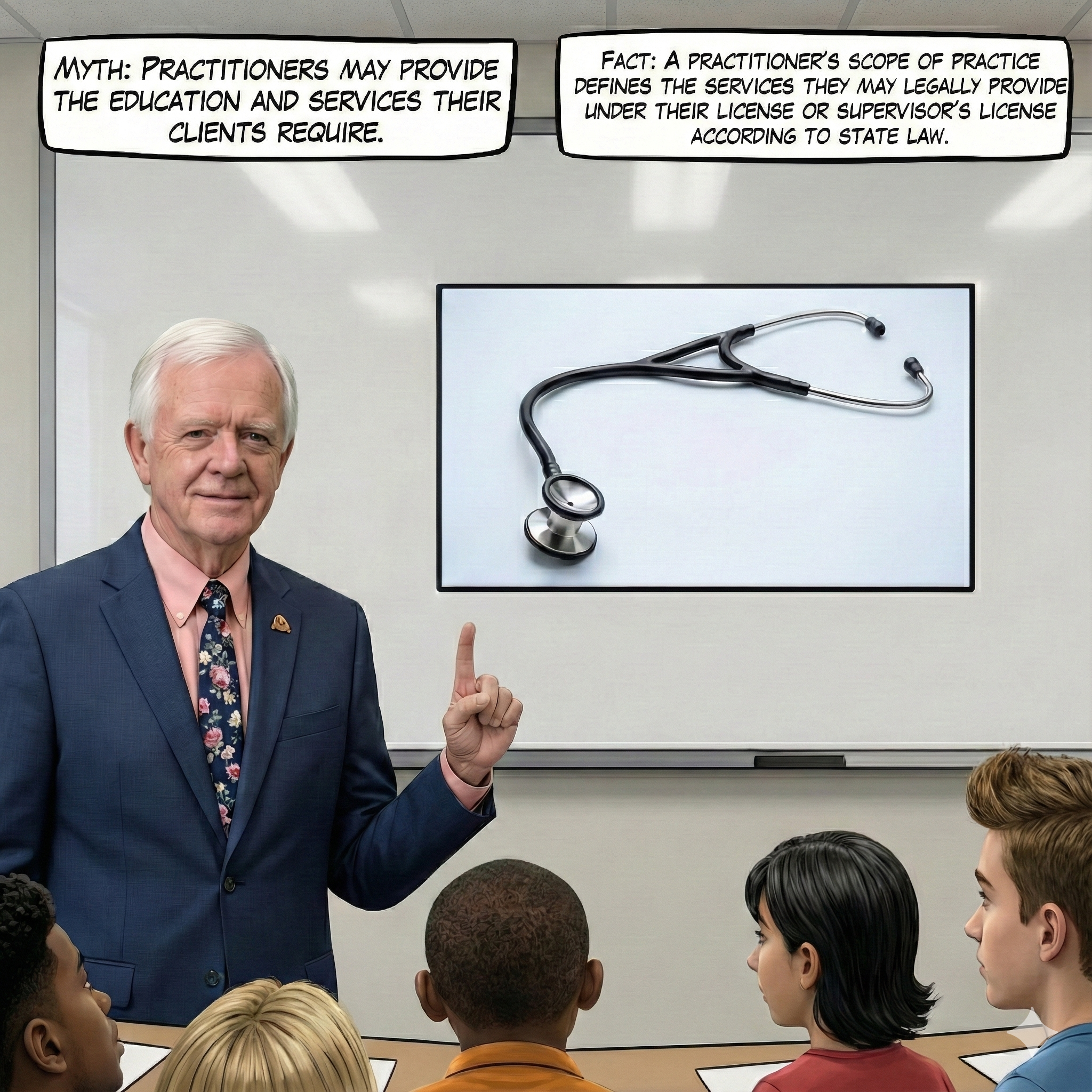
Mentoring is the 'process of transmitting knowledge and skills from the trained to the untrained or the experienced to the inexperienced practitioner. Mentoring involves a relationship between a mentor and candidate that promotes the development of skill, knowledge, responsibility, and ethical standards in the practice of biofeedback' (bcia.org). Typically, the mentor does not assume legal responsibility for the mentee's patients receiving treatment or training. The mentor's focus is on the planning and delivery of biofeedback services, not on the entirety of the client's care (Moss, 2020).
Mentoring is fundamentally an educational relationship designed to transfer knowledge and develop professional judgment. The mentor guides the mentee through learning biofeedback techniques, understanding protocols, and developing clinical reasoning skills. This relationship can be flexible; mentors and mentees might work in different locations, communicate remotely, and focus specifically on biofeedback aspects of cases. While mentors provide valuable guidance and share their expertise, they don't carry legal responsibility for the mentee's clinical decisions or patient outcomes.
Supervision Defined
Supervision is providing guidance for clinical practice for qualified health professionals by a more experienced health professional. In supervision, the supervisor assumes some legal responsibility (and liability) for the quality of care and the patient's wellbeing in the treatment process. A supervisor is responsible to remain cognizant of the entirety of the technician's caseload, client assessment, treatment planning, and treatment delivery (Moss, 2020).
Supervision is a legally defined relationship in which a licensed professional assumes responsibility for clinical care provided by someone under their oversight. This goes far beyond teaching; supervisors are legally liable for their supervisees' actions and clinical decisions. They must maintain awareness of the supervisee's entire caseload, review assessments and treatment plans, and be available for consultation on challenging cases. This legal responsibility means supervisors must be more deeply involved in day-to-day practice than mentors, understanding not just the biofeedback techniques being used but the complete clinical picture for each client.

Unacceptable Supervision
Since supervisors assume legal responsibility for client care, they must be physically present at the site where an applicant or unlicensed certificant works. BCIA rejects applications from technicians whose supervisors are not licensed, not legally allowed to supervise biofeedback services, or who can only oversee the delivery of services at a distance. Worst case scenario: supervision from another state represents a complete failure to meet legal and ethical requirements. Physical proximity enables supervisors to observe practice directly, respond immediately to crises, and fulfill their legal obligations to clients.
The requirement for on-site supervision reflects the legal reality that supervisors cannot adequately oversee care they cannot directly observe. Remote supervision might seem convenient in an era of telehealth, but it fails to meet the legal standard of assuming responsibility for client care. Supervisors must be able to step in immediately if problems arise, review sessions directly when needed, and maintain genuine oversight rather than nominal authority. Distance supervision creates liability without actual control, putting both clients and supervisors at risk.
Mentoring is an educational relationship focused on skill development without legal liability, while supervision is a legally defined relationship where the supervisor assumes responsibility for client care. Mentors can work remotely and focus specifically on biofeedback techniques, but supervisors must be physically present at the practice site and oversee the supervisee's entire caseload. BCIA rejects supervision arrangements where supervisors cannot provide direct, on-site oversight because remote supervision fails to meet legal standards for assuming clinical responsibility. Understanding this distinction protects both practitioners and clients from inadequate oversight arrangements.
Check Your Understanding
- What legal liability distinguishes supervision from mentoring?
- Which of the two relationships may be conducted remotely, and why?
- Why does BCIA reject supervision arrangements that lack direct, on-site oversight?
- What portion of a supervisee's caseload does a supervisor oversee?
Ethical Standards
This section explores the elements of professional conduct that extend beyond technical competence. We'll examine fiduciary responsibility, the duty to act in clients' financial best interests, and discuss how accountability, communication, and boundary maintenance contribute to ethical practice.
Biofeedback providers recognize that their effectiveness and the credibility of the field depend on their professional conduct. An aspect of ethical standards, whether those of BCIA or a licensing body, is professional conduct, the day-to-day behaviors that demonstrate respect, accountability, and integrity. Some elements of professional conduct not covered in other ethical standards include accountability, respect, good communication, giving comfort, timeliness, collaboration, responsiveness to constructive feedback, acknowledgement of errors, and maintenance of appropriate provider-client boundaries.
Biofeedback practitioners may be trained in any of a number of health professional disciplines such as nursing, social work, addiction counseling, sports psychology, medicine, occupational therapy, physiotherapy, and psychotherapy. Licensed health care providers follow the standards and guidelines of their respective professional bodies. This diversity of backgrounds enriches biofeedback practice but also requires practitioners to navigate multiple, sometimes overlapping, sets of professional standards.
Fiduciary Responsibility
Fiduciary responsibility means providers act as trustees of their clients' financial interests, placing client welfare above personal financial gain. They only bill for the services that they or supervised staff provide. When billing third-party payers, they conscientiously follow the payers' rules and regulations. This includes conservatively using billing codes, selecting the most accurate rather than most lucrative codes, obtaining written agreement in advance to use specific codes, differentiating the services they provide from those provided by their supervisees, and accurately describing staff credentials.
Providers have fiduciary responsibility.
Listen to a mini-lecture on Fiduciary Responsibility
Practitioners understand that the appearance of a conflict of interest can be as damaging to their reputation as an actual conflict. Whenever possible, they proactively identify potential conflicts and avoid them. For example, workshop presenters should refrain from promoting their products during educational events, as this blurs the line between education and sales. When a conflict of interest cannot be avoided, practitioners quickly and transparently resolve it. For example, providers who serve on boards often recuse themselves from decisions that involve their financial interests, demonstrating commitment to impartial decision-making.
Client education should include detailed information about assessment and treatment procedures, billing and fee collection, protection of confidentiality, and the limits of confidentiality. Providers should provide clients with a copy of these policies to read as they are carefully explained and only accept written consent when clients indicate that they understand them. This thorough orientation process establishes clear expectations and protects both clients and providers. Informed consent is especially essential for experimental treatment procedures, which may have a higher risk of failure and client dissatisfaction.
Professional conduct encompasses accountability, communication, boundary maintenance, and fiduciary responsibility, the obligation to prioritize clients' financial interests. Practitioners must bill conservatively and accurately, disclose potential conflicts of interest, and provide thorough orientation about policies and procedures. The diversity of professional backgrounds in biofeedback requires practitioners to navigate multiple ethical frameworks while maintaining consistent standards of care. Transparent communication about policies, procedures, and financial arrangements builds trust and prevents misunderstandings that could lead to complaints.
Check Your Understanding
- What does fiduciary responsibility obligate you to do?
- What does conservative and accurate billing look like in practice?
- What should a thorough client orientation to policies and procedures include?
- Why does the diversity of professional backgrounds in this field complicate ethical practice?
Public Statements
This section examines how practitioners should represent biofeedback to the public, discuss their credentials accurately, and market their services ethically. We'll explore the importance of evidence-based claims and transparent credential disclosure.
Providers understand that all public statements, ranging from educational talks to the description of services on their website, should be accurate, comprehensive, and conservative to facilitate informed consumer choices. They confine statements about biofeedback to scientifically supported information and communicate the limitations, uncertainties, and strength of these findings. "Discussion of treatment options in marketing materials and professional publications should be evidence-based and current" (Moss, 2020). This commitment to accuracy protects both the public and the field's credibility.

Professional Credentials and Transparency in Marketing and Promotion
Biofeedback providers must accurately disclose their degrees, training, specialty areas, experience, and the status of license or credential and certification. Advertisements for clinical practice should include only treatment or practice-relevant and regionally accredited academic degrees. Example: A PhD in French literature or mathematics should not be included on a business card or in an advertisement. It would mislead the potential client to assume the provider has doctoral-level clinical education. Example: Current controversy over nurses with PhD or DPN advertising their practices under the title, "Dr. Frances Schmidt." Unless the practitioner uses a further heading to clarify, this seems to mislead the patient to believe Dr. Schmidt is an MD. The appropriate title would be Dr. Frances Schmidt, Clinical Nurse Specialist. Participation in a membership organization such as AAPB or ISNR does not imply competence. Advertisement of one's professional association membership misleads the health consumer to assume that membership assures training and competence. Advertising BCIA and other forms of certification are legitimate ways to show competence (Moss, 2020).
The principle underlying these guidelines is simple: transparency. Clients deserve to know exactly what credentials their provider holds and what those credentials mean. Listing an irrelevant doctoral degree creates a false impression of clinical expertise, just as using the title "doctor" without clarification can mislead patients about medical credentials. Similarly, membership in professional organizations indicates interest and engagement with the field but doesn't certify competence the way BCIA certification does. Ethical marketing distinguishes between credentials that indicate expertise (certifications, relevant licenses) and those that simply demonstrate participation (membership).
Public statements about biofeedback must be accurate, evidence-based, and conservative, avoiding claims that exceed scientific support. Practitioners must disclose credentials transparently, including only practice-relevant degrees in professional materials and clarifying titles like "doctor" that could mislead about medical credentials. Professional organization membership indicates engagement but not competence, while certification demonstrates verified expertise. These standards protect consumers from misleading claims while allowing practitioners to accurately represent their qualifications and the evidence base for their services.
Check Your Understanding
- What standard must claims about biofeedback outcomes meet in your marketing materials?
- Which degrees belong in your professional materials, and which do not?
- Why can the title "doctor" mislead consumers, and how should you clarify it?
- How do organizational membership and certification differ in what they signal?
Copyright
This section addresses a growing area of legal and ethical concern: the proper use of copyrighted materials in professional presentations and publications. We'll examine fair use principles, distinguish between allowed and prohibited uses, and provide practical strategies for avoiding copyright infringement in an increasingly litigious environment.
BCIA professionals uphold the highest standards of ethical conduct in all facets of their practice, including the respectful use and dissemination of copyrighted materials. This commitment is rooted in the recognition that copyright laws are designed to protect the intellectual property rights of creators, thereby encouraging the continued creation and distribution of valuable resources. Understanding and following these laws protects both individual practitioners and their organizations from legal consequences while supporting the creative work that advances our field.

The following guidelines aim to clarify the principles of fair use (a legal doctrine permitting limited use of copyrighted material without permission for purposes like criticism, teaching, or research) and delineate the boundaries of copyright infringement, using copyrighted material without permission in ways that violate the owner's exclusive rights.
Understanding Copyright and Fair Use: BCIA professionals acknowledge that copyrighted materials, such as graphics, videos, and texts, are the legal property of their creators. Using such materials in presentations, webinars, or handouts without proper authorization or acknowledgment can infringe on copyright holders' rights. Fair use is a legal doctrine that permits limited use of copyrighted material without requiring permission from the copyright holders, primarily for purposes such as criticism, comment, news reporting, teaching, scholarship, or research. BCIA professionals must educate themselves on the nuances of fair use to navigate the complexities of copyright law effectively.
Allowed Uses in Public Talks and Webinars: When presenting public talks or conducting webinars, BCIA professionals may incorporate copyrighted materials under the principles of fair use, provided that the use is for educational, non-commercial purposes, contributes to the creation of new knowledge or insight, and does not substitute for the original work. Short excerpts of text, small, low-resolution images, or brief video clips are more likely to be considered fair use. However, professionals should always provide proper attribution to the original source.
Proscribed Uses and Avoiding Infringement: BCIA professionals must avoid using copyrighted materials in a manner that could be construed as an infringement. This includes the use of copyrighted materials in their entirety, such as full-length videos, unaltered graphics, or entire book chapters, especially when such use could compete with the market for original works. When planning to use copyrighted materials extensively, BCIA professionals should seek permission from the copyright holder.
Use in Webinars with and without Handouts: The same principles of fair use apply to webinars, whether handouts are provided or not. When distributing handouts, either electronically or in print, that include copyrighted materials, BCIA professionals must ensure that the inclusion of such materials falls within the guidelines of fair use and that the materials are essential for educational purposes. If distributing copyrighted material is necessary, obtaining permission from the copyright holder is advised to avoid infringement.
Promoting Ethical Standards and Professional Integrity: BCIA professionals commit to promoting the highest ethical and professional behavior standards. This includes respecting the intellectual property rights of others by adhering to copyright laws and fair use doctrine. In uncertainty regarding using copyrighted materials, professionals are encouraged to consult with copyright experts, legal advisors, or professional associations to ensure compliance with copyright laws.
By adhering to these guidelines, BCIA professionals demonstrate their respect for the intellectual property rights of others, contribute to the ethical dissemination of knowledge, and maintain the integrity of their professional practice.
Strategies for Avoiding Copyright Infringement
An Increasingly Perilous Legal Environment
When you violate copyright, you jeopardize yourself and your organization. "I didn't know I couldn't use this legally" is not a defense in court. The legal landscape has become increasingly aggressive in pursuing copyright violations, making awareness and compliance more critical than ever.
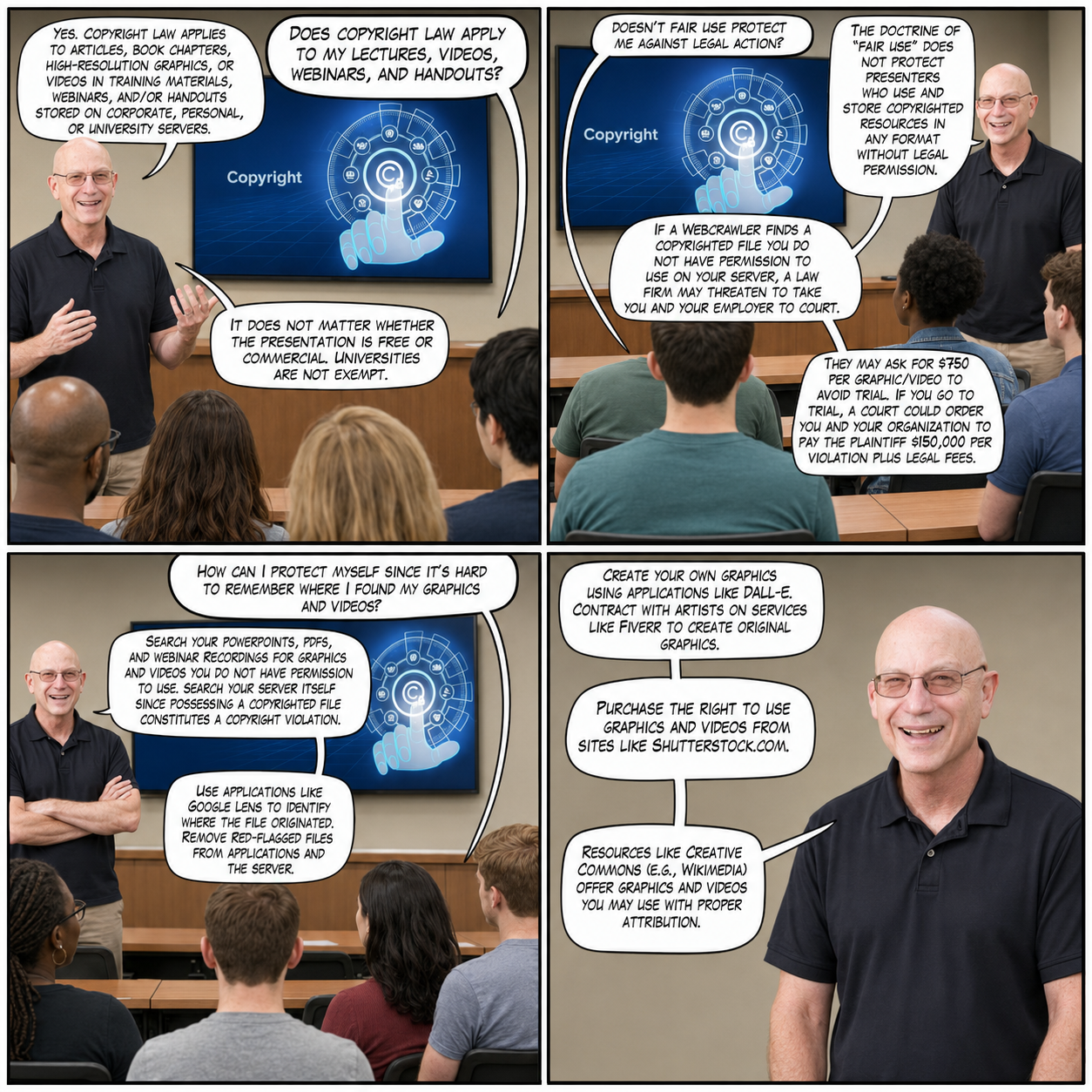
Bounties for copyright violations have become an increasingly important income stream for law firms. They contract with copyright holders to enforce their copyrights, using automated image-recognition crawlers that scan publicly reachable web pages and open file directories for matching graphics. These tools can flag graphics embedded in PowerPoint decks, PDFs, videos, and Word documents wherever a crawler can reach them, including course pages, learning-management downloads, and shared drives that were assumed to be private but are in fact indexable. Content behind a functioning password is not visible to a crawler, so the practical exposure comes from material that is less protected than its owner believes. The law firm will threaten litigation against the organization or individual on whose server the copyrighted content was found, or offer to settle for several hundred dollars or more per graphic.
What is at stake in litigation is statutory damages rather than a fine: under 17 U.S.C. § 504(c), a court may award between $750 and $30,000 for each work infringed, and as much as $150,000 per work only where the copyright owner proves the infringement was willful. Damages are counted per work infringed rather than per copy or per slide, and the court may also award costs and attorney's fees to the prevailing party.
Presenters should not assume that the doctrine of "fair use" will protect them when they include whole articles, book chapters, high-resolution commercial graphics, or videos in their training materials, webinars, and/or handouts. Fair use is neither a blanket permission nor a blanket prohibition; it is an affirmative defense decided case by case under 17 U.S.C. § 107, whose first factor expressly weighs whether the use is "of a commercial nature or is for nonprofit educational purposes." A free educational presentation therefore stands in a better position than a commercial one, though neither is automatically safe. What weighs most heavily against a presenter is reproducing a work in its entirety, or using a high-resolution image that substitutes for the licensed original. Universities are not exempt from these enforcement actions.
How to Avoid Copyright Infringement
To avoid copyright infringement in live talks and webinars that incorporate copyrighted graphics and video, webinar presenters should follow these practical steps:
Educate Yourself on Copyright and Fair Use: Gain a thorough understanding of what copyright law covers, the principles of fair use, and how they apply to educational and non-commercial presentations. This knowledge forms the foundation for making informed decisions about material use.
Use Licensed or Free-to-Use Materials: Whenever possible, use materials that are licensed for use in your context or are in the public domain. You may purchase the right to use graphics and videos from sites like Shutterstock.com. Resources like Creative Commons (e.g., Wikimedia) and various open-source platforms offer a wide range of graphics and videos that can be used legally without infringing on copyright.
Red-Flag Sources: Graphics from journal articles and textbooks, or high-resolution graphics sold by commercial sellers require your immediate attention. If you can't obtain legal permissions, remove them. These materials are particularly high-risk for enforcement actions.
Seek Permission When Necessary: If you wish to use copyrighted materials that do not fall under fair use or for which you do not have a license, seek permission from the copyright holder. This is especially important for significant uses or when distributing materials beyond a live presentation.
Use Materials for Educational Purposes: Ensure that the use of copyrighted materials clearly serves an educational purpose, adds value to your presentation, and does not compete commercially with the original works. Educational purpose alone doesn't guarantee fair use, but it's a necessary element.
Limit the Quantity of Use: Use only the amount of the copyrighted material that is necessary for the educational purpose. Short clips, small excerpts, or low-resolution images are more likely to be considered fair use than extensive reproductions.
Create Original Works: Whenever feasible, create your own graphics, videos, or slides. This not only avoids copyright issues but also tailors the materials specifically to your presentation's needs. Applications like DALL-E allow you to use AI to create original graphics. You may hire artists on services like Fiverr to create affordable graphics that you fully own.
Review and Modify Prepared Content: Before your presentation, review all materials to ensure they comply with copyright laws. You can use applications like Google Lens to identify their source. If unsure about the copyright status of any material, replace it; the safest course is always to use materials you know are properly licensed or original.
Stay Informed of Copyright Changes: Copyright laws and interpretations of fair use can evolve. Stay informed about any changes in copyright legislation or case law that might affect how you can use materials in your presentations.
By following these steps, webinar presenters can significantly reduce the risk of copyright infringement while ensuring their presentations are engaging, educational, and legally compliant. Real Genius WEBTOON by Dani S@unclebelang.
Copyright compliance protects creators' rights while shielding practitioners and organizations from legal liability. Fair use permits limited educational use of copyrighted materials, but doesn't protect extensive reproduction or distribution. Law firms actively scan for copyright violations using automated image-recognition crawlers, then threaten litigation for statutory damages that run from $750 to $30,000 per work infringed and reach $150,000 per work only when infringement is proven willful. Practitioners can avoid infringement by using licensed materials, creating original content, seeking permissions when needed, and staying informed about copyright law. When in doubt about copyright status, the safest approach is to remove questionable materials and replace them with properly licensed or original content.
Check Your Understanding
- What does the fair use doctrine permit, and where does it stop?
- What financial exposure does a copyright violation create?
- Name three strategies that reliably avoid copyright infringement.
- What should you do when you cannot determine the copyright status of an image?
Confidentiality
This section explores the complex landscape of protecting client information. We'll examine when confidentiality must be maintained, when it legally can't be, and the practical steps required to secure client data in both physical and digital formats.
© Zerbor/Shutterstock.com.
Listen to a mini-lecture on Confidentiality
While professionals strive to protect the confidentiality, a client's right to keep personal information private, of client, student, and research participant information, confidentiality is never absolute. For this reason, practitioners explain their procedures for safeguarding the confidentiality of data and the legal limits of confidentiality during orientation when they obtain informed consent. This upfront transparency about both protections and limitations allows clients to make informed decisions about what information to share.
While practitioners generally may only release information with the written consent of the individual or their representative, exceptions exist that override confidentiality protections. These include fee collection, compliance with mandated reporting laws that deal with abuse or neglect, and protecting the client or others from harm. Understanding these exceptions is crucial for ethical practice, since failing to report abuse when legally required constitutes an ethical violation, even if motivated by a desire to protect confidentiality.
Limitations to Confidentiality
Limitations to confidentiality rest on three sources. The first is the Tarasoff line of cases (Tarasoff v. Regents of the University of California, 1976); the California Supreme Court's second decision framed the obligation as a duty to protect an identifiable potential victim, with warning as one way to discharge it alongside notifying police or taking other reasonable steps. The second is state law, which varies more than the phrase "the duty to warn" suggests: some states impose a duty to warn or protect, others make disclosure permissive, and a few impose no statutory duty at all, so providers must know the rule in their own jurisdiction. The third is mandated reporting of child abuse and elder abuse. Danger to self is generally handled under state civil-commitment and emergency provisions rather than under Tarasoff.
Listen to Dr. Moss discuss confidentiality © Association for Applied Psychophysiology and Biofeedback.
Providers should consider consulting with their legal counsel if they receive a subpoena since this does not automatically shield them from their responsibility to maintain confidentiality (Moss, 2013). A subpoena represents a legal demand for information, but it doesn't necessarily override professional obligations to protect client information; navigating these competing demands often requires legal guidance.
Providers use secure procedures to store and destroy records and preserve records for the time required by applicable laws. These legal requirements vary by state and profession, making it essential for practitioners to understand their specific jurisdiction's mandates.

Graphic © Hafiez Razali/Shutterstock.com.
Practitioners must take many precautions to protect digitized client files. These include encrypting files, scrambling data so it's unreadable without a decryption key, storing them on portable media and locking them up when they are not in use, locking computers when they are unattended, using complex passwords or biometric security systems to prevent unauthorized access, and preventing unauthorized individuals from viewing displays of the client's confidential information (Striefel, 2004, p. 58). Each layer of protection addresses different vulnerability points in data security. One item on that list should be read in light of its date: Striefel's recommendation to store files on portable media and lock them up dates from 2004, and lost or stolen unencrypted laptops, thumb drives, and external disks are now among the most common causes of reportable breaches. Current practice is to keep protected health information on encrypted, access-controlled systems and to encrypt any portable media at rest, rather than relying on physical custody alone.
When electronically transmitting confidential client information, the use of encryption and assigning the client a number instead of using the client's name or national identification number protects confidentiality and reduces the risk of identity theft. The provider should include a cover page that warns the recipient that the transmitted information is confidential and must be protected and destroyed or returned and the sender notified if mistakenly received. The provider should request confirmation that the client information was received and should provide automatic acknowledgment after receipt of e-mail or fax messages (Striefel, 2004, pp. 71-72). These procedural safeguards create documentation trails and reduce the likelihood of accidental breaches.
Confidentiality protects client privacy but is never absolute, with legal exceptions for fee collection, mandated reporting, and protecting people from harm. Practitioners must explain both confidentiality protections and their limits during informed consent, allowing clients to make informed sharing decisions. Securing digitized records requires multiple layers of protection including encryption, access controls, physical security, and careful transmission procedures. Receiving a subpoena doesn't automatically override confidentiality obligations, making legal consultation essential when such demands arise. Understanding jurisdiction-specific requirements for record retention and destruction ensures compliance with applicable laws.
Check Your Understanding
- Name the principal legal exceptions to confidentiality.
- What must you explain about confidentiality during informed consent?
- Which safeguards protect digitized client records?
- Why does receiving a subpoena not automatically release client information?
Protection of Client Rights and Welfare
This section examines how practitioners protect clients' autonomy, dignity, and wellbeing. We'll explore informed consent requirements, the sensitive issues surrounding physical touch in biofeedback practice, and special considerations for working with children and vulnerable populations.
Providers protect the welfare of the individuals they serve through active listening and genuine attention to clients' priorities. Respect for clients requires that providers listen carefully to their clients to understand their goals and concerns. Successful collaboration and training are only possible when clients believe that you are focused on their priorities rather than imposing your own agenda. This client-centered approach forms the foundation of effective biofeedback practice.

Informed Consent
Respect for the patient's autonomy requires that the practitioner fully include a patient in treatment planning. The patient should be informed of the rationale for assessment and training procedures, the strength of empirical support for treatments, and the risks, costs, and potential benefits of treatment. Full understanding of all treatment options is essential to informed consent. Optimally, that informed consent will be written. A practitioner may provide less-documented biofeedback and behavioral therapies if the client is first fully informed of the available therapies for their problem, the evidence for each, and the scope of the evidence for the treatment that one is advocating. Many patients have failed to benefit from mainstream treatments and are open to innovative new treatments (Moss, 2020).
True informed consent requires more than obtaining a signature; it demands ensuring comprehension. Practitioners must explain treatment options in language clients can understand, provide realistic expectations about outcomes, and give clients genuine choice in their care. This process respects client autonomy, the right to make one's own decisions, while establishing realistic expectations that prevent disappointment and facilitate successful outcomes.
As practitioners, they carefully inform their clients about their rights during orientation and provide this information in written form. They explain the nature and purpose of all procedures and obtain permission from clients or their legal guardians before implementing them. This systematic approach to consent protects both clients and practitioners by establishing clear mutual understanding from the outset.
Sexual intimacy with current clients, trainees, supervisees, and research participants is prohibited. Following the termination of a professional relationship, providers should follow applicable statutes and the rules of their professional associations regarding when sexual intimacy is permissible. This clear boundary protects vulnerable individuals and maintains the therapeutic relationship's integrity.
Touch, Privacy, and Respect
Biofeedback practitioners should recognize that there is almost no physical contact with clients in routine psychological and mental health practice. Providers must take special precautions when attaching biofeedback sensors to a client since it invades personal space, often involves physical contact, and risks misinterpretation. "Biofeedback practice calls for careful development of procedures and routines to provide the rationale for regular touch" (Moss, 2020). Developing explicit protocols for sensor placement protects both clients and practitioners from misunderstanding.
They explain the function of the sensors and how they are attached and ask for permission to place them on the client's body. Whenever feasible, they encourage the client to attach sensors to their own body, a practice that maximizes autonomy and comfort. This is imperative in invasive protocols, such as pelvic floor biofeedback that uses vaginally- or anally-inserted sensors, where self-placement is both respectful and practical.

Providers should learn the specialized procedures that have been developed to preserve client modesty. This strategy minimizes physical contact, treats the client as a respected partner, and can strengthen the therapeutic alliance rather than undermining it. Training in modesty-preserving techniques should be part of every practitioner's skill set.
When a biofeedback protocol requires sensor placement on a sensitive region (like ECG placement on the torso), the presence of a same-sex nurse or technician and use of garments (like gowns) that preserve client modesty are recommended (Moss, 2013). Wherever possible, use alternative placements (e.g., ECG wrist placement) to afford greater client comfort. These accommodations demonstrate respect while maintaining clinical effectiveness.

Practitioners do not touch sensitive body parts like breasts or genitals during biofeedback practice, except as part of a medical examination or medical treatment performed by a licensed medical practitioner. This clear boundary maintains professional standards and protects clients from inappropriate contact.
Why is Touch a Sensitive Area?
Providers should remember that a high percentage of individuals in the general population, especially women, have been molested, raped, or otherwise violated, often by a person of trust. One multi-state and territory study showed that 18.5% of women report a history of attempted or completed nonconsensual sex (Smith & Breiding, 2011). The percentage of women violated sexually may be higher in populations with chronic illness (Santaularia et al., 2014; Smith & Breiding, 2011).
These statistics underscore why seemingly routine touch in biofeedback practice can trigger traumatic responses. Practitioners must approach all touch with awareness that many clients carry trauma histories that may not be disclosed. Offering choices, explaining procedures thoroughly, and encouraging self-placement of sensors creates safer practice for everyone. Understanding trauma prevalence transforms how we conduct every session.
Obtaining Assent from Children
They respect children's rights and seek their assent, willingness to participate without necessarily understanding all implications, before receiving biofeedback training or participating in research. This respects children's developing autonomy while acknowledging their limited capacity for full informed consent.
Consent means that the consenting person understands what they are getting into and its implications, and that they are making a choice that they control and have authority for. Assent more simply means that the person is willing to participate in something, without necessarily understanding the essential details of what they are getting into or all its consequences. If a child or person with cognitive impairments is not able to provide consent, then someone who has authority for the child or person provides consent. The child or mentally impaired person, however, is still asked for their assent. This is not mere politeness but is also practically useful because it helps to engage the child's active participation in the treatment.
Respect for Dignity and Rights
They respect the dignity and rights of all individuals and never discriminate against or refuse services to clients because of their sex, sexual orientation, sexual identity, race, religion, disability, or national origin. This commitment to equal treatment reflects both ethical obligations and legal requirements in most jurisdictions.
Protecting client rights requires informed consent that ensures genuine understanding, not just signature collection. Physical touch in biofeedback requires special protocols given trauma prevalence; practitioners should explain procedures, encourage self-placement of sensors, and use alternative placements when possible. Children receive assent procedures appropriate to their developmental level while legal guardians provide formal consent. Sexual intimacy with clients is absolutely prohibited, and practitioners must respect the dignity and rights of all individuals regardless of demographic characteristics. Understanding that many clients carry undisclosed trauma histories should shape every aspect of how practitioners conduct sessions and interact with clients.
Check Your Understanding
- Why is a signed consent form insufficient evidence of informed consent?
- What protocols should govern physical touch during sensor placement?
- How do assent and consent differ when you work with children?
- How should undisclosed trauma histories shape the way you conduct a session?
Biofeedback Equipment Selection
This section explores the regulatory landscape for biofeedback equipment. We'll examine FDA requirements, distinguish between on-label and off-label uses, and discuss the implications of equipment choices for clinical practice and insurance reimbursement.
Wherever possible, purchase equipment that is FDA approved. The major equipment manufacturers expend thousands of hours and go to considerable expense to obtain FDA approvals and to meet ISO 13485 medical device certification requirements. 'Quality first: all our products are designed and developed according to ISO 13485 and FDA requirements of quality systems' [Mind Media]. However, many small companies producing inexpensive devices do not follow these procedures. Manufacturers may have FDA waivers for some battery-operated devices.
Clinical biofeedback devices are regulated by the US Government's Food and Drug Administration (FDA). Nearly all of them reach the market as FDA-cleared devices through the 510(k) premarket notification pathway, which rests on substantial equivalence to a legally marketed predicate device, not as FDA-approved devices, a term reserved for the premarket approval (PMA) pathway used mainly for Class III devices. In an ethics unit the distinction is more than pedantry: 21 CFR 807.97 provides that representing 510(k) clearance as FDA approval of the device is misleading and constitutes misbranding. Some biofeedback devices are not "waived" but exempt: 21 CFR 882.5050 classifies the biofeedback device as Class II and, at paragraph (b), exempts it from premarket notification subject to the limitations in 21 CFR 882.9.
You should not use any biofeedback device for clinical applications unless it is cleared, approved, or exempt for a comparable use, or you are using it under an appropriate research protocol. If you are outside the US, your own government may have its own system of regulation. Each cleared or approved device carries a 'label' stating the indications for use that FDA has accepted as sufficiently well demonstrated. You must inform your clients in writing if you use the device off-label, meaning for purposes other than those listed with the FDA. For a complete discussion of FDA issues, including who can prescribe the use of biofeedback devices, please see the discussion at 'Food and Drug Administration (FDA) Biofeedback Equipment Labeling and Approval Issues' (Moss, 2020).
Strongest Position
Hypothetically, if you treat a patient with a diagnosed disorder using non-FDA equipment, the insurance company could demand re-payment. FDA-registered equipment should only be sold to licensed professionals. No practitioner who is not licensed for independent practice should advertise biofeedback treatment for diagnosed disorders (or provide a diagnosis on statements for submission to insurance companies) unless supervised by a licensed provider (Moss, 2020).
This creates a clear incentive structure favoring FDA-cleared equipment: using devices that are neither cleared, approved, nor exempt risks insurance complications and limits who can legally purchase equipment. While non-FDA devices might be less expensive, they create legal and financial vulnerabilities that can outweigh cost savings. Understanding these implications helps practitioners make informed equipment decisions.
FDA Labeling
The FDA only labels devices for specific uses that have been strongly documented. Most biofeedback and neurofeedback devices, for example, are designated for relaxation or stress management only. Licensed practitioners can utilize equipment off-label but should be careful not to advertise off-label applications (Moss, 2020).
This labeling limitation reflects the evidence base: while practitioners may use devices off-label based on emerging research, they cannot market these uses without risking regulatory action. The restriction balances clinical innovation with consumer protection, allowing licensed practitioners to apply clinical judgment while preventing misleading advertising.
Best Telehealth Practices
The Covid-19 pandemic has increased the delivery of biofeedback and neurofeedback services via telehealth both within and across state lines. Dr. Moss provides an overview of best telehealth practices © Association for Applied Psychophysiology and Biofeedback.
FDA clearance for biofeedback equipment provides quality assurance and protects against insurance reimbursement challenges, though cleared devices are typically labeled only for relaxation and stress management. Licensed practitioners can use equipment off-label but must inform clients in writing and avoid advertising these uses. Using equipment that is neither FDA-cleared nor exempt to treat diagnosed disorders creates financial risk and may violate state laws regarding equipment sales. The expansion of telehealth services requires understanding best practices for remote service delivery while maintaining regulatory compliance.
Check Your Understanding
- What does FDA approval of biofeedback equipment actually certify?
- What are your obligations when you use a device off-label?
- What risks follow from using non-FDA equipment to treat a diagnosed disorder?
- Which additional practices does telehealth delivery require?
Infection Risk Mitigation
This section examines the often-underestimated risk of transmitting infection during biofeedback and neurofeedback practice. We'll explore how everyday clinical contact can transfer infectious organisms, review the strategies practitioners use to reduce that risk, and consider the special precautions required during a pandemic.
A neurofeedback provider applied reusable EEG sensors to the scalp of a high school wrestler with skin lesions. When questioned, the wrestler explained that the lesions were due to mat abrasion and that all the wrestlers on his team had them. Since the clinician did not disinfect the sensors between sessions, several of his other clients developed MRSA infections and sued him for malpractice. This vignette was adapted from Moss (2013).

Professionals follow the most rigorous standards of infection mitigation to protect clients and staff. Practitioners should learn and implement reasonable disinfection standards for biofeedback instruments, sensors, and office environments (Moss et al., 2019).
Listen to a mini-lecture on Infection Risk Mitigation
During a pandemic or another period of elevated community transmission, distance training may be necessary. When in-person work resumes, practitioners should follow the Centers for Disease Control and Prevention (CDC) guidance then in force for screening, distancing, masking, and surface cleaning, recognizing that test positivity is only one indicator and that CDC has moved toward composite measures such as community transmission and hospital-admission levels.

Graphic © Kinga/Shutterstock.com.
Biofeedback providers may underestimate their risk of transmitting infection to their clients and may lack basic knowledge about risk mitigation strategies. Whereas clinicians may assume that infection risk is low since biofeedback is noninvasive, handshakes, reclining chairs, cables, and sensors can easily transfer infectious organisms to clients. Moreover, over-abrasion in SEMG biofeedback and neurofeedback can expose sensors to client blood, and inserted vaginal and rectal sensors contact mucous membranes. Under the Spaulding classification, both are semi-critical contacts, which call for high-level disinfection at a minimum; the critical category is reserved for devices that enter sterile tissue or the vascular system, which biofeedback sensors do not.
This ubiquitous problem is called common vehicle transmission. Risk mitigation involves three strategies: handwashing and drying, disinfection of surfaces clients will contact, and disinfection or sterilization of sensors and cables (Hagedorn, 2014).
A comprehensive prevention strategy includes handwashing by both the clinician and client. When the skin is not visibly soiled, alcohol-based products may be superior to antiseptic soap and water in terms of effectiveness, minimizing skin dehydration, and ease of use. However, soap and water are superior to alcohol-based products in removing spores of Clostridioides difficile (formerly Clostridium difficile; C. diff), because alcohols are not sporicidal at any concentration (Sullivan & Altman, 2008).
Clinicians should disinfect chair or recliner surfaces using wipes impregnated with a germicide whose label covers the organisms of concern, rather than a dilute solution such as 20% isopropyl alcohol, which falls below the 60–90% range in which alcohols are reliably bactericidal (Hagedorn, 2014). Virusolve+ is marketed with sporicidal claims; FreshnIT is a washroom cleaner and carries no sporicidal or Clostridioides difficile claim, so it should not be relied on for spore control. No alcohol-based product is sporicidal at any concentration.

When equipment like precious metal electrodes and cables can be damaged by heat, a liquid chemical germicide is used in place of heat, matched to the Spaulding category of the item and applied between clients. High-level disinfection requires a germicide cleared for that purpose and used at the concentration and contact time stated on its label; ordinary surface disinfection does not achieve it. Protex Disinfectant Spray is a surface disinfectant, not a sterilant or high-level disinfectant, and its own label states that it is not to be used as a terminal sterilant or high-level disinfectant. It is labeled to destroy a broad spectrum of bacteria, viruses, and fungi, including herpes, MRSA, and VRE, on noncritical surfaces such as chairs, cables, and instrument housings.

The risk of infection transmission can be reduced by using disposable sensors, and in the case of rectal or vaginal sensors, using dedicated sensors that belong to the client (Sullivan & Altman, 2008).

Biofeedback and neurofeedback practitioners often underestimate their potential to transmit infection because the modalities feel noninvasive, yet handshakes, shared surfaces, cables, and sensors readily spread organisms through common vehicle transmission. Risk mitigation rests on three pillars: handwashing and drying, disinfection of contacted surfaces, and disinfection or sterilization of sensors and cables. Practitioners should match the disinfection method to the exposure risk, using disposable or client-dedicated sensors for invasive placements and biocidal agents effective against resistant organisms like C. diff and MRSA. During a pandemic, distance training and current CDC standards for screening, distancing, masking, and surface cleaning further protect clients and staff.
Check Your Understanding
- Why do practitioners underestimate their potential to transmit infection?
- What are the three pillars of infection risk mitigation?
- How should the disinfection method be matched to the exposure risk?
- Which practices are indicated for invasive sensor placements?
Professional Relationships
This section examines how biofeedback practitioners build effective partnerships with colleagues and navigate potentially conflicting loyalties. We'll explore collaboration with physicians, avoiding conflicts of interest, and managing dual relationships that could compromise professional judgment.
Providers build partnerships with colleagues in diverse professions based on respect for their competencies. These networks allow allied providers to combine their expertise and resources when treating clients, conducting research, and educating the public, legislators, and third-party payers. Effective collaboration multiplies individual practitioners' impact while improving client outcomes through integrated care.
Listen to a mini-lecture on Partnerships

Practitioners should only treat medical disorders with biofeedback if their clients have been medically evaluated or are under the care of a physician. They should collaborate with the physicians who treat their clients by explaining their treatment strategy and goals, providing regular progress reports supported by physiological data, and advising physicians on how biofeedback and adjunctive procedures can interact with medication. For example, relaxation training may reduce a diabetic patient's insulin requirement, resulting in a functional overdose, when normal medication doses become excessive due to physiological changes, that could cause hypoglycemia and coma. This collaborative approach can promote sharing vital information, physician encouragement of their clients to continue biofeedback, and future referrals.
Providers respect the importance of client-physician relationships and avoid the appearance of interfering with medical treatment. If clients express the desire to adjust or eliminate medication as their symptoms improve, providers should withhold their opinion and encourage clients to discuss this issue with their physician. This maintains appropriate professional boundaries while supporting integrated care; stepping between client and physician undermines both relationships and potentially endangers the client.
They maintain good relationships with their colleagues by striving to be objective and compassionate in their judgments of others and showing respect for different perspectives. They collaborate with allied professionals to increase understanding and pursue goals that they could not achieve alone. This professional collegiality benefits the field while improving client care through cross-disciplinary learning.
Conflicts of Interest
They recognize that multiple relationships, situations where a provider and client share more than one role, can threaten their bond with those they serve and risk the exploitation of both parties. They avoid dual relationships with clients and never exploit clients, students, supervisees, employees, research participants, or third-party payers. These overlapping roles create power imbalances that can compromise professional judgment and harm vulnerable parties.
For example, practitioners should never treat their spouses, and supervisors should never treat their employees. When providers question their own objectivity, they should seek guidance from colleagues. These consultation processes provide external perspective when internal judgment may be clouded by competing loyalties or personal investment.
Effective professional relationships require building partnerships across disciplines while maintaining appropriate boundaries. Collaboration with physicians is essential when treating medical conditions, including communication about treatment plans and potential medication interactions like functional overdoses. Practitioners must avoid interfering with client-physician relationships, particularly regarding medication adjustments. Multiple relationships create conflicts of interest that can compromise professional judgment; practitioners should never treat spouses or employees, and should seek collegial consultation when questioning their objectivity. Building respectful relationships with colleagues across professions enhances client care while advancing the field.
Check Your Understanding
- When is communication with a client's physician essential?
- What is a functional overdose, and why does it require collaboration?
- Why should you never treat a spouse or an employee?
- What should you do when you begin to question your own objectivity about a client?
Research with Humans and Animals
This section explores the ethical obligations of researchers in biofeedback. We'll examine protections for human and animal subjects, requirements for informed consent in research, and the responsibilities researchers bear for accurate reporting and participant welfare.
Professionals conduct research to increase our understanding of human behavior, improve the human condition, and advance science. They believe that human and animal welfare must be their paramount concern when conducting research and strive to protect them. They adhere to applicable legal statutes and standards of their professions, consider alternative research methods that minimize participant discomfort and deception, and reduce the number of animal subjects. They cooperate completely with institutional review boards and institutional animal care and use committees that regulate human and animal research, oversight bodies that ensure ethical standards are maintained.
Their research reports completely describe their methodology and statistical analysis, accurately summarize experimental findings, and satisfy conventional scientific criteria. Descriptions of clinical procedures are factual and avoid self-promotion. They explicitly describe the limitations of their studies and exercise caution in drawing conclusions from their data. They may supplement probability testing with estimates of effect size, the magnitude of a treatment's impact, and confidence intervals to better communicate the research significance of their results. This comprehensive reporting allows other researchers to evaluate findings critically and replicate studies.
Each researcher is responsible for ensuring that research adheres to legal and professional ethical standards and that collaborators, assistants, students, and employees treat participants ethically. All members of a research team are personally responsible for their ethical conduct. This shared accountability prevents ethical violations from being attributed to "just following orders" or delegated to junior team members.
Researchers protect information obtained from participants through procedures that ensure anonymity, protecting participants' identities, and confidentiality. They protect anonymity by identifying participant records using codes rather than names. They guard confidentiality by securely storing data, by only using data as promised to the participants, and by only reporting aggregate results rather than individual data. They explain these precautions when they obtain informed consent, allowing participants to understand how their information will be protected.
They inform prospective subjects about all aspects of a study that might influence their decision to participate, including potential risks and benefits, and encourage questions when they obtain informed consent. Their responsibility to protect participants increases with the risk of harm. If participants are injured by research, they are responsible for providing effective care to make these individuals "whole," restoring them to their pre-research condition. They never employ research procedures that are likely to cause severe and lasting harm to participants, recognizing that some knowledge isn't worth the cost to human welfare.
They respect an individual's right to refuse to participate in research or to end their participation at any time and never coercively use compensation. They are especially vigilant in protecting this freedom when the investigator can affect the participant's outcomes, such as when researching with students or patients. When studying minors, investigators should seek their assent whenever possible, respecting children's developing autonomy even when legal consent comes from guardians.
When a study involves deception, withholding information or providing false information to participants, researchers are responsible for completely debriefing participants about the nature of the study, either immediately after their participation or when data collection is finished. When debriefing must be delayed, researchers redouble their precautions to ensure that participants are not harmed. The use of deception in research carries heightened ethical obligations because it undermines informed consent.
Research ethics prioritize participant welfare above scientific advancement, requiring adherence to oversight committees, minimization of harm, and complete informed consent. Researchers must accurately report methodology, acknowledge limitations, and protect participant anonymity and confidentiality through coded records and aggregate reporting. All research team members share personal responsibility for ethical conduct, and participants retain the right to withdraw at any time. When research involves deception, researchers must provide thorough debriefing and exercise heightened precautions. If participants are harmed, researchers bear responsibility for restoring them to their previous condition.
Check Your Understanding
- What oversight bodies must approve research with humans and animals?
- How do researchers protect anonymity and confidentiality?
- What obligations follow when a study involves deception?
- What is a researcher's responsibility if a participant is harmed?
Adherence to Professional Standards
This section examines how practitioners maintain current knowledge and apply evidence-based protocols in their work. We'll explore the standards documents that guide practice and the importance of documenting experimental procedures.
Providers strive to utilize the best practices in the biofeedback field. Wherever possible, they use evidence-based protocols and maintain current knowledge about treatment efficacy, the proven effectiveness of interventions. When utilizing experimental procedures, they carefully describe their protocols and objectively document treatment outcomes, contributing to the evidence base while protecting clients through transparency.
Hammond, Bodenhamer-Davis, Gluck, Stokes, Harper, Trudeau, MacDonald, Lunt, and Kirk (2011) authored Standards of practice for neurofeedback and neurotherapy: A position paper of the International Society for Neurofeedback & Research. An ISNR Task Force consisting of Randy Lyle, Cory Hammond, Jerry Gluck, Genie Bodenhamer Davis, Deb Stokes, and John Davis updated these standards in 2019. They represent ISNR's official position on the delivery of neurofeedback (EEG biofeedback) and provide detailed guidance for practitioners in this specialty.
Adherence to professional standards requires using evidence-based protocols when available and carefully documenting experimental procedures when extending beyond established practices. Practitioners must maintain current knowledge about treatment efficacy to provide informed care. Professional organizations like ISNR provide detailed practice standards that guide specialty applications like neurofeedback, offering practitioners authoritative guidance for maintaining best practices in rapidly evolving fields.
Check Your Understanding
- When may you extend practice beyond established, evidence-based protocols?
- What documentation does an experimental procedure require?
- How do you maintain current knowledge about treatment efficacy?
- What role do professional society practice standards play in specialty applications?
Ethics Complaint Procedures
This section explains how ethical complaints are handled within the biofeedback field. We'll examine BCIA's educational approach to complaints, when direct resolution is appropriate, and when complaints should be referred to licensing boards or legal authorities.
Informal Resolution of Complaints
BCIA strives to promote communication between complainants and its certificants.
For example, when a client or a professional raises ethical concerns about a certificant with BCIA's Executive Director, they will encourage the complainant to contact the certificant to resolve the matter directly. "When the violation is more grievous and not appropriate for informal resolution, or the effort at informal resolution fails, then the professional should take action appropriate to the situation (such as referral to state or national ethics committee, licensing board, or institutional authorities" (Moss, 2020). This tiered approach reserves formal proceedings for serious violations while encouraging direct communication for misunderstandings or minor issues.

Graphic © fizkes/Shutterstock.com.
Listen to Dr. Moss explain BCIA's educational approach to ethical complaints © Association for Applied Psychophysiology and Biofeedback.
When BCIA receives a written complaint about the ethical conduct of a BCIA certificant or applicant, BCIA's Executive Director will record the complaint and will write a letter to the complainant that will describe BCIA's role in ethics cases, direct the complainant to directly discuss the complaint with the provider [certificant or applicant], and if requested by the complainant, identify state and/or national regulatory agencies with jurisdiction. Since BCIA's approach to ethical issues is educational, BCIA will not recommend that complainants contact these agencies, nor will it represent complainants before these agencies. When BCIA receives a complaint, it will first encourage the complainant to carefully consider whether this is a consumer satisfaction issue or a potentially harmful violation of standard healthcare practice or professional ethics. BCIA will not intervene in complaints regarding consumer satisfaction since these issues fall outside of its mission and are better resolved by organizations that promote marketplace trust. When BCIA receives consumer satisfaction complaints, it will encourage consumers to directly discuss their concerns with the BCIA professional who provided their services or with organizations, like the Better Business Bureau, that provide voluntary dispute resolution (BCIA, 2016).
BCIA will not intervene in complaints about manufacturer or vendor products, services, or sales practices as these issues do not concern certification, and corporations are not BCIA professionals. This limitation keeps BCIA focused on its core mission: ensuring that certificants maintain ethical standards in their professional practice.
BCIA takes an educational approach to ethics complaints, first encouraging direct communication between complainants and certificants for potential resolution. The organization distinguishes between consumer satisfaction issues (outside its scope) and genuine ethical violations requiring intervention. For serious violations or failed informal resolution, complainants are directed to state licensing boards or national ethics committees with enforcement authority. BCIA does not intervene in complaints about manufacturers or vendors, maintaining focus on individual practitioner conduct. This tiered system balances accessibility with appropriate scope, ensuring serious violations receive formal attention while resolving minor issues informally.
Check Your Understanding
- What is the first step BCIA encourages when a complaint arises?
- How does BCIA distinguish consumer satisfaction issues from ethical violations?
- Where are complainants directed when informal resolution fails?
- Why does BCIA decline to intervene in complaints about manufacturers or vendors?
Biofeedback Certification International Alliance (BCIA)
This section introduces BCIA, the primary certification body for biofeedback practitioners. We'll explore what certification means, how it differs from licensure, and why BCIA certification has become the recognized standard in the field.

What is Certification?
Professional certification, recognition by a non-governmental organization that an individual has met predetermined standards, is not a license to practice. BCIA Board certification does not authorize professionals to provide services that they could not legally offer before certification. Certification is a voluntary process in which applicants demonstrate competence and commit themselves to a code of ethics and pursue continuing education to increase their proficiency. This distinction between certification and licensure is fundamental: licensure grants legal authority to practice, while certification validates competence within one's existing scope.
"Professional certification is the voluntary process by which a non-governmental entity grants a time-limited recognition to an individual after verifying that predetermined and standardized criteria have been met. Because biofeedback is an unregulated field, meaning no state requires specific credentials to practice biofeedback, certification is crucial for providing standards of care. To be viable as a professional service, standards of competence and clinical practice must be defined and measured. Since 1981, BCIA has taken on this task, establishing benchmarks that protect both clients and the profession.
Through the BCIA recertification program, each certificant is held accountable to a code of ethics, obtains specified continuing education, and maintains proper credentialing appropriate for clinical practice." (BCIA, 2011). This ongoing recertification ensures that credentials remain current rather than representing competence at a single point in time.
BCIA's Mission
BCIA, formerly the Biofeedback Institute of America, was created in 1981 with the primary mission to certify individuals who meet education and training standards in biofeedback and progressively recertify those who advance their knowledge through continuing education. This mission addresses the absence of state regulation by creating voluntary standards that establish professional credibility.
In March of 2010, the BCIA adopted a new name to reflect its global identity and became the Biofeedback Certification International Alliance. This name change recognized BCIA's international reach and commitment to serving practitioners worldwide.

BCIA is an autonomous nonprofit corporation. BCIA policies and procedures are set by an independent board of directors comprised of a rotating group of distinguished biofeedback clinicians, researchers, and educators. This governance structure ensures that certification standards reflect current best practices and are developed by practitioners actively engaged in the field.
Board certification is the mark of distinction for providers of biofeedback and neurofeedback services. Certification is valid for 4 years for providers who carry the credential in Biofeedback, HRV Biofeedback, Neurofeedback, and Pelvic Muscle Dysfunction Biofeedback. Re-certification indicates continuous peer review of ethical practice and the acquisition of advanced knowledge of recent developments in the field through required continuing education. Names of certified practitioners may be found on the BCIA website by using its Find a Practitioner search function, providing consumers with a tool to locate qualified providers.
Board certification establishes that an individual has met entry-level requirements for the clinical practice of biofeedback. However, BCIA certification is not a substitute for a state-issued license or another credential to practice one's profession. Candidates for certification who do not hold a professional license or its equivalent must stipulate that they practice under the supervision of a licensed provider when treating a medical or psychological disorder. This requirement ensures that certification complements rather than replaces legal credentialing.
Why Choose BCIA Certification?
This section explores the specific advantages of BCIA certification. We'll examine the results of certificant surveys, the recognition BCIA has achieved from major professional organizations, and the rigorous standards that make BCIA the preferred credential in biofeedback.

BCIA certificants reported in a comprehensive survey that they initially sought certification for credibility, validation of their skills and knowledge, professional satisfaction, to ensure proper training, and to promote the field. BCIA biofeedback certification is internationally recognized for six reasons: 1. BCIA is a nonprofit institute that has been an effective advocate for our field. The American Psychological Association (APA) has recognized biofeedback as a proficiency in professional psychology because of the petition that BCIA filed with them. BCIA has been dedicated to a singular mission since 1981: BCIA certifies individuals who meet education and training standards in biofeedback and progressively recertifies those who advance their knowledge through continuing education. 2. BCIA's biofeedback certification is the only program that is recognized by the three major international membership organizations: the Association for Applied Psychophysiology and Biofeedback (AAPB), the Biofeedback Federation of Europe (BFE), and the International Society for Neurofeedback and Research (ISNR). 3. BCIA's biofeedback certification is based on scientific evidence published in refereed journals. BCIA rejects narrow, unsubstantiated perspectives and the conflict of interest that exists when certification depends on a specific vendor's equipment, databases, and protocols. BCIA certification is based on a reading list, Blueprint of Knowledge, and Professional Standards and Ethical Principles that were developed following an extensive job analysis and that are regularly updated by a task force of international authorities in biofeedback. BCIA continually gathers data to validate and revise its exams through the psychometric process to ensure the relevance, integrity, and value of its certification program. 4. BCIA's biofeedback certification exam adheres to the highest psychometric standards. We painstakingly evaluate and revise its exam on a regular basis. Several independent experts, who include clinicians and the most experienced educators in our field, regularly review exam items to ensure that they represent key blueprint concepts, are sourced to its suggested reading list, and are psychometrically sound. BCIA regularly replaces outdated exam questions with new ones contributed by biofeedback authorities and then validated by our certificants. 5. BCIA requires that its certificants adhere to one of the strongest ethical codes in our field. In addition, we require that its certificants complete 3 hours of ethics continuing education when they renew their certification. BCIA's rigorous ethical standards are one of the many reasons that its international colleagues have chosen BCIA biofeedback certification. 6. BCIA's Board of Directors consists of clinicians, educators, and researchers who have guided the development of biofeedback. BCIA's Board includes leaders of the three major international membership organizations who have contributed decades of service to our field (Why Choose BCIA Biofeedback Certification?).
BCIA certification validates entry-level competence in biofeedback but does not replace licensure or expand scope of practice. The organization's mission focuses on establishing and maintaining professional standards in an otherwise unregulated field. BCIA certification is internationally recognized by all major professional organizations, based on scientific evidence rather than vendor-specific protocols, and maintained through rigorous psychometric standards. Certificants must adhere to strong ethical standards and complete ongoing continuing education for recertification every four years. The organization's governance by distinguished clinicians, researchers, and educators ensures that standards reflect current best practices.
Check Your Understanding
- What does BCIA certification validate, and what does it not confer?
- Why does certification matter especially in an unregulated field?
- What makes BCIA certification independent of any particular vendor?
- What is required to maintain certification over time?
Certification Programs
This section outlines BCIA's four certification programs and their requirements. We'll examine the distinctions between different certifications, understand the common requirements across all programs, and clarify the difference between certification and certificates of completion.
BCIA has four certification programs:
Biofeedback Certification
HRV Biofeedback
Neurofeedback Certification
Pelvic Muscle Dysfunction Biofeedback Certification
Individuals certified in Biofeedback have demonstrated entry-level competence in biofeedback modalities, including EMG (electromyography, muscle electrical activity), HRV (heart rate variability), respiration, skin conductance (electrodermal activity), and temperature. This broad certification prepares practitioners to work with multiple physiological systems.
Individuals certified in HRV Biofeedback have demonstrated entry-level competence in modalities including ECG (electrocardiography), EMG, PPG (photoplethysmography, blood volume measurement), and respiration. This specialized certification focuses on cardiovascular and respiratory training.
Individuals exclusively certified in Neurofeedback, commonly called EEG Biofeedback, are certified to utilize only that specialty modality. This certification requires specific expertise in brain electrical activity training and does not authorize practice in other biofeedback modalities.
The Pelvic Muscle Dysfunction Biofeedback Certification is only for licensed providers wishing to use biofeedback and behavioral interventions to treat elimination disorders and pelvic pain within their scope of practice. This specialized certification addresses intimate health concerns requiring additional sensitivity and expertise.
Three Distinct Certification Categories
BCIA now formally distinguishes among three categories of certificants, reflecting differences in professional roles, qualifications, and intended scope of practice. This framework overlays the modality programs above: every future applicant will follow one of these three pathways, determined by academic qualifications, credentials, and licensure.
Individuals who hold a valid clinical license carry the Licensed (L) designation, identified as BCN-L (Board Certified in Neurofeedback – Licensed) or BCB-L (Board Certified in Biofeedback – Licensed). The suffix clearly identifies their status as licensed practitioners.
Those who are not clinically licensed but work in performance enhancement contexts, such as sports, corporate, military, or academic research settings, receive the new Performance (P) credential as BCN-P or BCB-P.
The Technician (T) category applies to support personnel who operate under appropriate supervision within their supervisor's scope. Technician certification is available only to individuals residing and working in the United States or Canada who are under the legal supervision of a licensed professional holding a BCIA biofeedback or neurofeedback certification. This pathway does not require a specific educational background, making it accessible to a broad range of applicants.
Technicians must work under the direct oversight of a BCIA-certified and licensed supervisor who is legally authorized to oversee non-licensed personnel. They must operate strictly within the scope of their supervisor's practice and are not permitted to supervise or mentor other certification candidates. If a technician's employment status changes, the certification becomes inactive and remains invalid until the individual can again demonstrate active employment under appropriate supervision in full compliance with the certification standards.
BCIA's new performance designation will not affect didactic and anatomy course requirements or the services you can legally provide. Full stop.
BCIA will automatically reassign current certificants under this revised framework. Those with clinical licenses will transition to the Licensed designation, while those without licenses will be redesignated under the Performance category. This shift brings greater clarity to credentialing, helping to align professional titles with training, regulatory standing, and intended application. International certificants will continue to be designated as BCN-L or BCB-L, since licensure remains a requirement for international certifications.
All certification programs require strict adherence to the Professional Standards and Ethical Principles of Biofeedback.
All certification programs are based on:
prerequisite educational degrees, except for the Technician certification
proof of human anatomy/physiology and human biology coursework
didactic coursework that is based on the Blueprint of Knowledge statements that cover the fundamental science, history, and theory of biofeedback specific to that certification program
clinical training or mentoring to learn the application of skills
certification exam
Certification is no substitute for a state-sanctioned license. BCIA's certificants must carry an appropriate license/credential valid in the state of practice in a BCIA-approved health care field when treating a medical or psychological disorder. If unlicensed, the certificant must work under appropriate supervision (Shaffer et al., 2012). Your biofeedback or neurofeedback provider's licensing body or their supervisor has legal jurisdiction over his or her clinical practice (Crawford, 2013). This layered accountability ensures both professional competence and legal authorization.
Certifications are valid for a set period: 4 years for Biofeedback, HRV Biofeedback, Neurofeedback, and Pelvic Muscle Dysfunction Biofeedback. Re-certification is granted upon application, payment of fees, documentation of accredited continuing education specific to the Blueprint, and adherence to the Professional Standards and Ethical Principles of Biofeedback. This time-limited credential ensures practitioners maintain current knowledge rather than relying on outdated training.
In 2012, BCIA created a Certificate of Completion in Heart Rate Variability (HRV) Biofeedback that requires 15 hours of didactic HRV biofeedback instruction, 3 hours over professional conduct, and a passing score on a nationally standardized exam (Crawford, 2013). A certificate of completion, recognition of completing an approved workshop and passing an exam, is not a certification. This credential attests to completing an approved didactic workshop based on BCIA's Blueprint and passing an exam over its content, but it doesn't include the clinical training and mentoring required for full certification.

How does certification differ from licensure?
Certification means that a non-governmental organization like BCIA has recognized that an individual has satisfied its requirements and demonstrated entry-level competence in a field like biofeedback. Certification is not a license to practice and does not authorize professionals to provide services they could not legally offer before certification (Shaffer, Crawford, & Moss, 2012). Licensure means that a state agency has authorized an individual to use a professional designation, like Psychologist, and provide services specified by the state's practice act for a fee. This distinction is crucial: certification validates competence within existing scope, while licensure grants legal authority to practice.
Individuals who engage in diagnosing or treating disorders outside their legal scope of practice may face state prosecution. This risk underscores why understanding both certification and licensure requirements is essential for ethical practice.
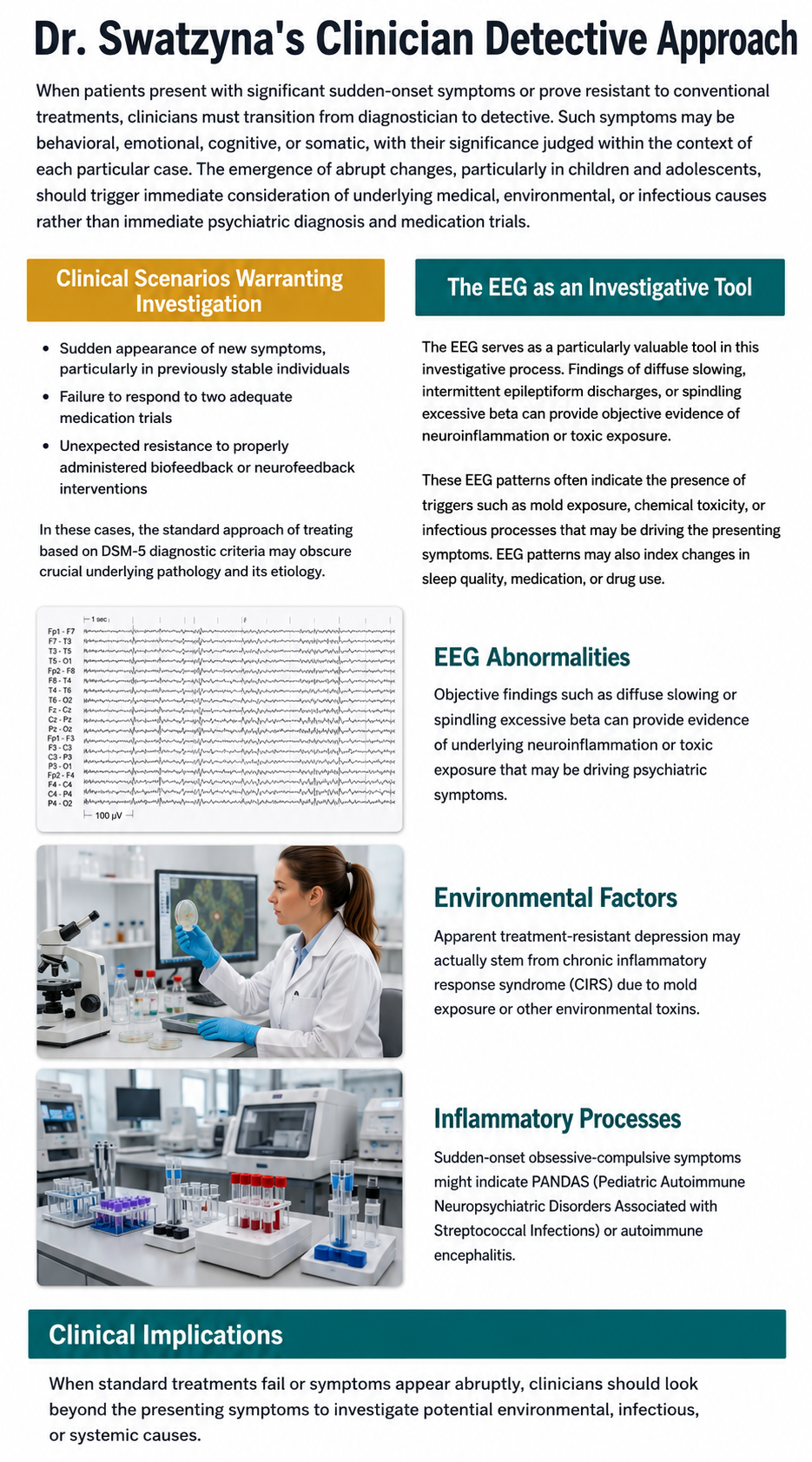
BCIA offers four certification programs covering different biofeedback modalities, each requiring education, coursework, clinical training, and examination. All programs mandate adherence to Professional Standards and Ethical Principles and are valid for four years before requiring recertification. Certification validates competence but doesn't replace licensure; certificants must either hold appropriate licenses or work under supervision when treating medical or psychological disorders. Certificates of completion differ from certification by requiring only didactic training and examination, not clinical mentoring. Understanding the distinction between certification (non-governmental competence recognition) and licensure (state-granted practice authority) is essential for maintaining ethical practice boundaries.
Check Your Understanding
- Name the four certification programs and the modalities each covers.
- What requirements are common to all of the certification programs?
- How does a certificate of completion differ from a certification?
- Why must certificants still hold a license or work under supervision?
Ethical Practice in EEG Neurofeedback
Most neurofeedback providers already bring careful practice to their work: thorough assessment, real-time signal review, artifact control, informed consent, consultation, and outcome monitoring. This article is written to support that practice, not to portray the field as careless or uniform. It is a practical reference for work already underway.
Neurofeedback also carries a distinctive set of ethical questions. The path from scalp voltage to a clinical or performance claim passes through electrode placement, reference choice, filtering, artifact handling, feature extraction, normative comparison, thresholding, feedback logic, and human interpretation.
Each layer can be executed well. Each can also add uncertainty, hide an error, or make a weak inference look more persuasive than it is (Association for Applied Psychophysiology and Biofeedback [AAPB], 2013; Collura et al., 2025; Ros et al., 2020). Identifying these layers is not a criticism of the field; it is a requirement for using a powerful tool responsibly.
This article focuses on the EEG and the qEEG. It does not claim that every ethical issue discussed here is unique to neurofeedback, nor does it cover every form of neurofeedback or neuromodulation. Where law, regulation, licensure, an employer's policy, or a professional code sets a higher or more specific requirement, that requirement governs.
I am grateful to Donald Moss, Ronald J. Swatzyna, and Frans J. Cronje for conversations that informed my thinking about this rapidly changing area, especially artificial intelligence.
I extensively used Dr. Swatzyna and Dr. Barbara Peavey's 2026 Biofeedback Society of Texas ethics presentation. None of my colleagues reviewed or endorsed this article. Any mistakes are exclusively the author's.
Central principle. Keep the client or trainee, the raw physiology, the full context, and accountable human judgment ahead of the tools that summarize them. Everything else in this article elaborates that one idea.
1. Start by naming the practice context
Neurofeedback is delivered in several materially different contexts, and ethical language becomes clearer when the provider names the context before making a claim. Doing so protects both the client and the provider.
Contexts, purposes, and responsibilities
| Context or assessment layer | Primary purpose and permissible claims | Core responsibilities |
|---|---|---|
| Clinical assessment or treatment | Address symptoms, impairment, or a diagnosed health condition. Clinical claims stay within the responsible professional's legal scope and competence. | Multimethod assessment, clinical formulation, informed consent, adverse-event monitoring, referral procedures, records, and coordination with other care. |
| Performance or educational training | Improve a defined skill or performance outcome in a generally healthy person. Diagnosis or treatment is not implied unless the provider is authorized and the service is actually clinical. | Accurate representation of evidence, safety screening, clear nonclinical boundaries, functional outcome measures, and referral when a health concern emerges. |
| Research | Produce generalizable knowledge under an approved protocol. Research participation is not presented as individualized clinical care. | Ethics review where required, protocol fidelity, consent, privacy, adverse-event procedures, appropriate controls, and transparent reporting. CRED-nf is a research design and reporting checklist, not a clinical practice guideline (Ros et al., 2020). |
| Use of formal qEEG assessment | Add quantitative summaries or normative comparisons to raw EEG review. | Reviewable raw data, transparent acquisition and artifact procedures, database and method fit, qualified interpretation, and clear limits on diagnostic and treatment-selection claims. |
Some safeguards apply in every context: accurate representation of competence, valid recording, attention to artifact and state, understandable consent, data protection, and a plan for unexpected symptoms. Other duties depend on whether the service is clinical, performance-oriented, or research.
Some neurofeedback approaches do not use formal qEEG, z-scores, or normative databases; the sections on maps, database fit, and quantitative reports apply only when those tools are used, while the raw-signal, artifact, state, consent, supervision, data, and outcome safeguards apply more broadly.
2. Use evidence labels, not a single rhetorical volume
The recommendations below are deliberately labeled. The goal is accuracy: an author's preference should never be presented as settled consensus. Labeling distinguishes established standards from the author's own recommendations and leaves the judgment to the reader.
How to read these recommendations
| Label | Meaning |
|---|---|
| Professional or ethical standard | Explicitly stated in law, regulation, a professional code, or a relevant practice standard. The exact force varies by jurisdiction and profession. |
| Evidence-informed risk-management recommendation | Supported by technical, clinical, or ethical evidence, but not necessarily mandated in one universal form. |
| Author-proposed conservative clinic policy | A deliberately cautious operational suggestion offered where standards do not prescribe a single method. Clinics may use another model if they can demonstrate equivalent safety, observation, accountability, and legal compliance. |
3. Seven core safeguards
Seven safeguards form the backbone of this framework, and they function together rather than in isolation. Except where a stronger standard or a specific line of evidence is noted, each is an evidence-informed risk-management recommendation grounded in professional judgment. The first is to build raw-signal competence and to know where to find qualified review: anyone who acquires or trains from EEG can learn to verify recording quality, recognize common artifacts and vigilance changes, and identify when a record requires a more qualified look.
The second is to let EEG and qEEG inform rather than stand alone whenever a mental or neurodevelopmental question is on the table, since they contribute to a clinical picture rather than function as a solo diagnostic test, a point grounded in biomarker evidence.
The third is to treat candidate biomarkers as questions rather than verdicts, because a correlation is a reason to look closer rather than jump to a diagnosis, cause, prognosis, or automatic training target.
The fourth safeguard is to consider competing explanations before interpreting a pattern, because artifact, drowsiness, sleep loss, medication, substances, pain, illness, a past head injury, an environmental exposure, time of day, and recording conditions can all shift the signal; this practice protects the client.
The fifth is to keep qEEG in a supporting relationship with the raw EEG and the full formulation, so that no map, z-score, classifier, or normative report carries decisive weight by itself.
The sixth is to keep accountable clinical authority with qualified people: software may assist within transparent bounds, but it should not silently determine candidacy, diagnosis, treatment target, protocol, or stopping decisions, a stance consistent with broad health-AI guidance.
And the seventh is to design supervision and staffing around continuous observation and prompt help. I recommend that a technician provide neurofeedback training to one client at a time.
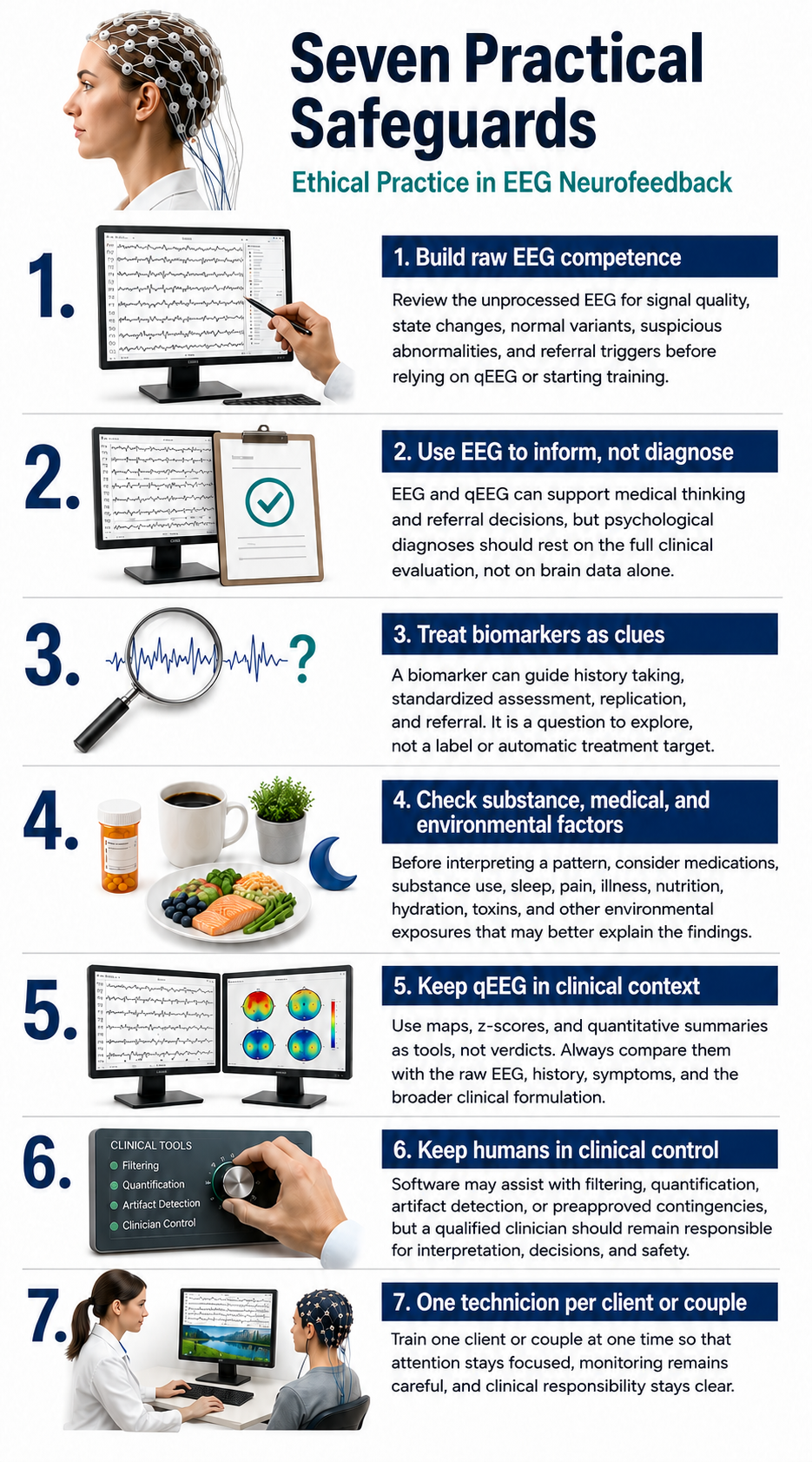
4. Raw EEG competence comes first and can be shared across a team
Competence with the raw EEG is not the same as being a clinical electroencephalographer, and no one has to carry every level of expertise alone. A workable standard distinguishes three levels of responsibility and allows collaboration across them.
Three levels of competence
| Level | Minimum competence |
|---|---|
| Everyone who acquires or trains from EEG | Verify electrode placement, reference, channel integrity, sampling and filter settings; recognize common eye, muscle, movement, sweat, line, pulse, cable, and electrode artifact; distinguish alert wakefulness from drowsiness well enough to avoid obvious state-trait errors; pause when the signal is invalid or the client is not safely participating. |
| Responsible clinician or qualified qEEG reviewer | Judge whether the recording is adequate for the intended use; review in alternate montages and time scales; evaluate normal variants and suspicious focal, generalized, rhythmic, or paroxysmal activity without exceeding the scope of one's health profession; integrate findings with history, symptoms, medication, sleep, and other assessment data; determine when consultation or referral is warranted. |
| Medical EEG specialist | Diagnose or formally characterize epileptiform activity, encephalopathy, focal dysfunction, and other medical EEG findings within appropriate credentials and clinical context. |
A provider does not have to perform every level personally. A documented team arrangement with timely access to qualified review meets the safety requirement. One caution: a map or automated report should not be relied upon when no one involved can evaluate whether the underlying recording is physiologically plausible.
Current technical guidance for clinical QEEG emphasizes standardized acquisition, visual inspection, artifact management, data selection, and transparent processing (Collura et al., 2025).
Routine diagnostic EEG standards offer useful technical context, though they were written for clinical neurophysiology rather than outpatient neurofeedback (Peltola et al., 2023). AAPB and ISNR likewise value competence with the device, physiology, scope, and relevant supervision (AAPB, 2013; International Society for Neuroregulation & Research [ISNR], 2024).
Beyond what the table itemizes, a practical baseline adds a few habits: inspecting unprocessed or minimally processed data in alternate montages when the system permits, reproducing common artifacts when it is safe to do so, and, just as importantly, documenting uncertainty, inviting consultation, and deferring interpretation or training when validity or significance is still an open question.
Practice rule. If the raw record is unavailable, inadequate, or not competently reviewed, the quantitative output is best not given decisive clinical weight. This protects the client and takes pressure off the provider.
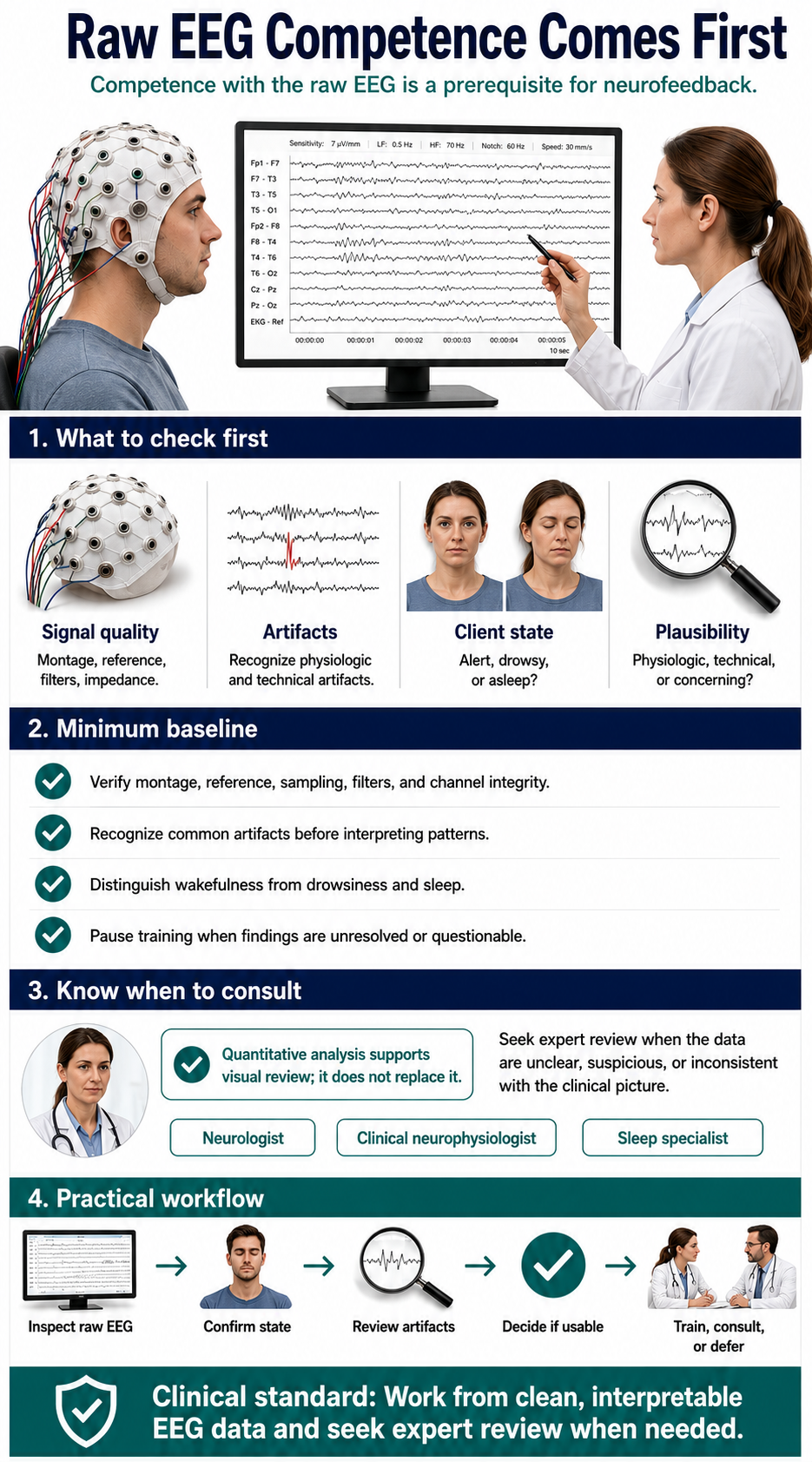
5. Knowing when to consult or refer
Referral is not a sign that neurofeedback "failed." It protects clients from scope errors and delayed care and often identifies the real, treatable driver of their symptoms.
The right action depends on urgency, the provider's own license and competence, and local procedures. A psychiatrist, psychologist, physician, counselor, or other licensed provider may be able to assess and manage a concern directly; another provider may consult or refer.
An important habit for a neurofeedback provider is to consider the underlying cause of a presentation. Symptoms that look like anxiety, depression, ADHD, or even psychosis can arise from substance use, medication effects, a medical condition, a past head injury, or an environmental exposure.
Swatzyna and Peavey (2026) have made this point for the whole mental-health field: presenting signs and symptoms do not always reveal what is happening underneath. For a neurofeedback provider, this means a well-considered referral can sometimes produce relief that no training protocol would have reached on its own.
Immediate emergency or crisis response
| Concern | Immediate action | Important limits |
|---|---|---|
| Any current suicidal ideation or recent suicidal behavior | Pause routine neurofeedback and complete or arrange a same-day structured suicide-risk assessment. Active intent, a plan with intent, preparatory behavior, or an inability to maintain safety calls for the clinic's emergency or crisis procedure and the level of care indicated by risk and local law, not an ordinary future referral. In the United States, the 988 Suicide & Crisis Lifeline may be one component of the response, while imminent danger may require emergency services (National Institute of Mental Health [NIMH], n.d.). | A questionnaire score alone does not determine risk. SAFE-T calls for risk and protective factors, suicide inquiry, risk-level determination, intervention, and documentation (Substance Abuse and Mental Health Services Administration [SAMHSA], 2024). |
| First or prolonged seizure-like event, sustained altered consciousness, acute focal neurological deficit, or a severe sudden headache with neurological signs | Stop the session and obtain urgent or emergency medical evaluation. | Describe observations rather than diagnosing epilepsy or another disorder unless qualified. Preserve relevant raw data. |
| Chest pain, exertional loss of consciousness, severe unexplained shortness of breath, or sustained palpitations with instability | Stop the session and obtain urgent or emergency medical evaluation. | A pulse channel, HRV display, consumer sensor, or EEG artifact is not a diagnostic ECG. |
Prompt consultation or referral
| Observation or history | Usual destination | What to document and communicate |
|---|---|---|
| Recurrent unexplained lapses of awareness; new focal neurological symptoms; unexplained cognitive decline or abnormal movements; persistent focal or generalized slowing after artifact, vigilance, medication, and known-history effects have been considered; repeated suspicious sharp, rhythmic, or paroxysmal activity that persists across montages | Neurology or clinical neurophysiology | Objective observations, relevant history, state and medication information, montage and settings, artifact checks, and preserved raw data. Avoid diagnostic labels outside scope. |
| Recurrent syncope or presyncope; exertional loss of consciousness; sustained palpitations; chest pain; unexplained dyspnea; family history suggestive of sudden cardiac death; persistent apparent rhythm irregularity after artifact checks; unexpected bradycardia accompanied by symptoms or clinical concern | Primary care, urgent care, or cardiology depending on severity | Syncope evaluation centers on history, examination, and a 12-lead ECG, not qEEG pattern matching (Shen et al., 2017). Asymptomatic sinus bradycardia can be physiologic; context and symptoms matter (Kusumoto et al., 2019). |
| Psychosis, mania or hypomania, severe depression, panic, trauma-related symptoms, substance-related instability, or other symptoms that substantially impair safety or function | Assess and manage within the responsible clinician's competence and scope; otherwise consult or refer to an appropriately licensed mental-health professional | Symptoms, onset, duration, impairment, medication and substance factors, risk assessment, and actions taken. qEEG is not the diagnostic basis. |
| Loud habitual snoring, witnessed apneas, excessive daytime sleepiness, sleep attacks, marked sleep fragmentation, or persistent insomnia with functional impairment | Primary care or sleep medicine | Sleep history, current sleepiness, medication and substance factors, and whether the recording included drowsiness or sleep. |
| Suspected medication interaction, recent medication change with adverse symptoms, intoxication or withdrawal, uncontrolled medical illness, recurrent hypoglycemic symptoms, or another medical concern affecting safe participation | Prescriber, pharmacist, primary care, urgent care, or the relevant specialty | What was taken, dose and timing, recent changes, observed symptoms, vital or device information if valid, and what the provider did. Never direct cessation of prescribed medication outside appropriate authority. |
| Nutrition, endocrine, gastrointestinal, chronic pain, or lifestyle concerns without emergency features | Primary care or the relevant licensed professional; an integrative clinician may participate when care is coordinated | Use specific concerns rather than vague labels such as "hormonal imbalance" or "chronic inflammation." Integrative care should complement, not replace or delay, indicated conventional evaluation (National Center for Complementary and Integrative Health [NCCIH], 2021). |
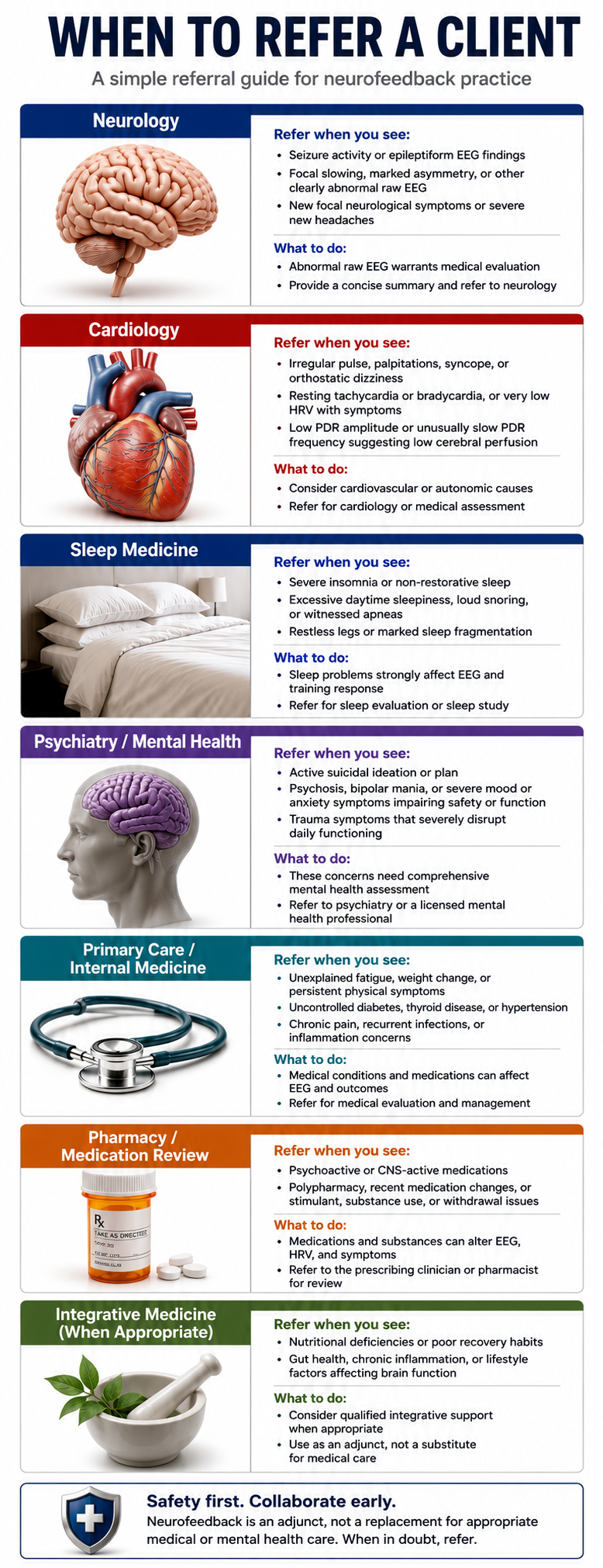
Several signals indicate that a physiological or environmental contributor may warrant investigation alongside the neurofeedback work. None is conclusive on its own; each is a prompt to investigate further and, where appropriate, to consult a medical or specialist colleague (Swatzyna & Peavey, 2026).
An atypical presentation, symptoms that do not fit familiar patterns or carry unusual features, is one such signal, as is a limited response that shows little change despite appropriate, well-delivered evidence-based care.
Concurrent physical symptoms, such as unexplained physical complaints or abnormal examination findings alongside the psychological picture, warrant the same scrutiny, and so does an abrupt onset in which severe symptoms emerge suddenly without a clear psychological precipitant.
The most telling prompt is an environmental correlation, where symptoms rise and fall with a change of setting or exposure, for example, easing when the person is away from home.
A few findings are best not treated as stand-alone referral triggers. Some observations are simply too nonspecific to send someone along on their own. A supposed "normal-pressure hydrocephalus pattern" inferred from generalized slowing does not qualify, nor does low posterior dominant rhythm amplitude or frequency offered as a test of cerebral perfusion. A PHQ-9 or other questionnaire cutoff is not a referral trigger without clinical assessment and risk inquiry, and neither is a software-generated diagnosis or arrhythmia label drawn from a non-diagnostic signal. Generalized slowing and posterior rhythm changes are nonspecific.
6. EEG and qEEG are contributors, not stand-alone diagnostic tests
A raw EEG can reveal findings that meaningfully change a medical differential, which is valuable. That is a different matter from diagnosing ADHD, depression, anxiety, PTSD, autism, bipolar disorder, schizophrenia, or a personality disorder.
A qEEG can summarize spectral power, asymmetry, connectivity, phase, source estimates, or database deviations. These metrics are useful for research, measurement, hypothesis generation, and clinical correlation. What they cannot do, on their own, is establish or exclude a mental or neurodevelopmental diagnosis.
The heart of the matter is the gap between group-level association and individual-level decision-making. A feature may differ on average between research samples yet lack the sensitivity, specificity, predictive value, stability, transportability, or incremental validity needed for diagnosis in a particular person. Similar features can appear across diagnoses, in healthy participants, and under fatigue, drowsiness, medication, pain, or artifact (Abi-Dargham et al., 2023; Hammond, 2010).
The same presentation can also be shaped by contributors that lie outside the EEG entirely: substance use and the medications used to treat it, prescribed psychiatric medications, a mild traumatic brain injury, a structural finding such as an arachnoid cyst or Chiari malformation, an endocrine or metabolic condition, a nutritional factor, sleep loss, or an environmental exposure (Swatzyna & Peavey, 2026).
Widely used diagnostic frameworks already require clinicians to consider substance, medical, and environmental factors before assigning a mental-health diagnosis, so a neurofeedback provider who keeps these possibilities in view is following established practice.
AAPB states that biofeedback is an adjunct and cannot be used alone to make a diagnosis (AAPB, 2013). A responsible diagnostic formulation therefore rests on symptoms, duration, impairment, developmental and medical history, sleep and substance factors, validated measures, differential diagnosis, and the qualified clinician's scope, and would still stand even if the EEG were removed from the chart.
Clinically defensible language
| Instead of | Consider |
|---|---|
| "The qEEG confirms ADHD." | "This quantitative finding is nonspecific and does not establish or exclude ADHD. It may help guide additional clinical evaluation." |
| "This is a depression pattern." | "Similar features have been reported in some research samples, but this individual's finding is not diagnostic and calls for clinical correlation." |
| "Your trauma is stored in this brain region." | "This recording cannot localize a psychological experience or determine its cause." |
| "The map tells us exactly what to train." | "The map is one helpful data source. A protocol also draws on the raw EEG, the full assessment, the evidence, the person's goals, and a safety plan." |
| "The algorithm detected your disorder." | "The software classified a signal feature under a particular model. A qualified professional weighs its validity, limitations, and relevance." |
7. Treat biomarkers as questions, not verdicts
The word biomarker can sound more authoritative than the evidence warrants. A measurable feature can correlate with a disorder yet remain unfit for diagnosis, prognosis, treatment selection, or monitoring. This means the finding is a lead to follow, not a conclusion to announce.
A clinically useful diagnostic biomarker performs at the individual level in the intended population under realistic conditions, with validated thresholds and known error rates. A treatment-selection biomarker shows that using it improves outcomes compared with not using it.
Psychiatry still lacks robust, broadly validated biomarkers for most individual diagnoses and treatment decisions (Abi-Dargham et al., 2023). This is a limitation of the current evidence base, not of any individual practitioner.
When a putative EEG biomarker appears, the next step is to interrogate it.
Faced with excess theta, the reviewer should consider whether the person is drowsy, sleep-deprived, developmentally younger than the database, taking a sedating medication, or producing eye or movement artifact.
High beta invites a look for facial, temporalis, neck, or scalp EMG, along with a thought about the timing of anxiety, stimulant use, pain, or reference instability. An asymmetry raises its own set of questions: does it replicate, does it persist in alternate montages, and could electrode contact, skull factors, state, or database mismatch explain it?
A connectivity or phase deviation is worth interrogating for stability across clean epochs, preprocessing choices, reference methods, and software implementations. In every one of these cases, no single finding needs to become a protocol target on its own.
A z-score is not the probability of a disease. It is a standardized distance from a reference mean under assumptions about the sample, age range, recording conditions, hardware, preprocessing, artifact handling, and distribution. A value outside a statistical interval can be real yet clinically irrelevant; a value inside the interval can coexist with genuine impairment.
Practice rule. Let a candidate biomarker sharpen the next step (replication, history, testing, consultation, or referral) rather than convert correlation into identity.

8. Interpret qEEG alongside the raw EEG and the full context
A qEEG is derived from the raw EEG; it is a companion to it, not an independent test. Quantification can compress data, support reproducible measurement, and surface patterns worth reviewing. It can also hide morphology, timing, state transitions, artifacts, and normal variants that determine whether the numbers mean anything. The two must be interpreted together.
A defensible and satisfying sequence unfolds in order. It begins by establishing recording quality and verifying settings, then moves to inspecting the raw EEG in appropriate montages and time scales. From there it identifies the person's vigilance and behavioral state, marks, removes, or models artifact using transparent rules, and confirms that enough representative clean data remain.
Only then does it make sense to examine quantitative summaries and database comparisons, and finally to integrate the findings with the full clinical or performance formulation.
Reversing this order invites confirmation bias: a dramatic map appears first, and the reviewer then searches the record for support while overlooking alternatives. Working in order guards against this error.
Keeping the raw data, not only screenshots or a vendor report, is essential for later review. It lets someone determine which epochs entered the analysis, what artifact decisions were made, what reference and preprocessing were used, which database and software version were applied, and whether the result reproduces after correction.
Current IQCB technical guidance places strong emphasis on these acquisition, inspection, selection, and processing steps (Collura et al., 2025).
Vendor opacity is simply a reason to assign a little less weight to an output. A proprietary system is not automatically invalid, but a report is best not allowed to drive consequential decisions when clinically material details (raw traces, epoch selection, artifact handling, database characteristics, processing parameters, or model limitations) cannot be examined.
CRED-nf supports transparent reporting of signal processing, regulation success, artifact procedures, adverse effects, and clinically meaningful outcomes in neurofeedback experiments (Ros et al., 2020). It is a useful transparency model, though it is not a clinical practice standard and should not be cited as if it settled every operational rule in a clinic.
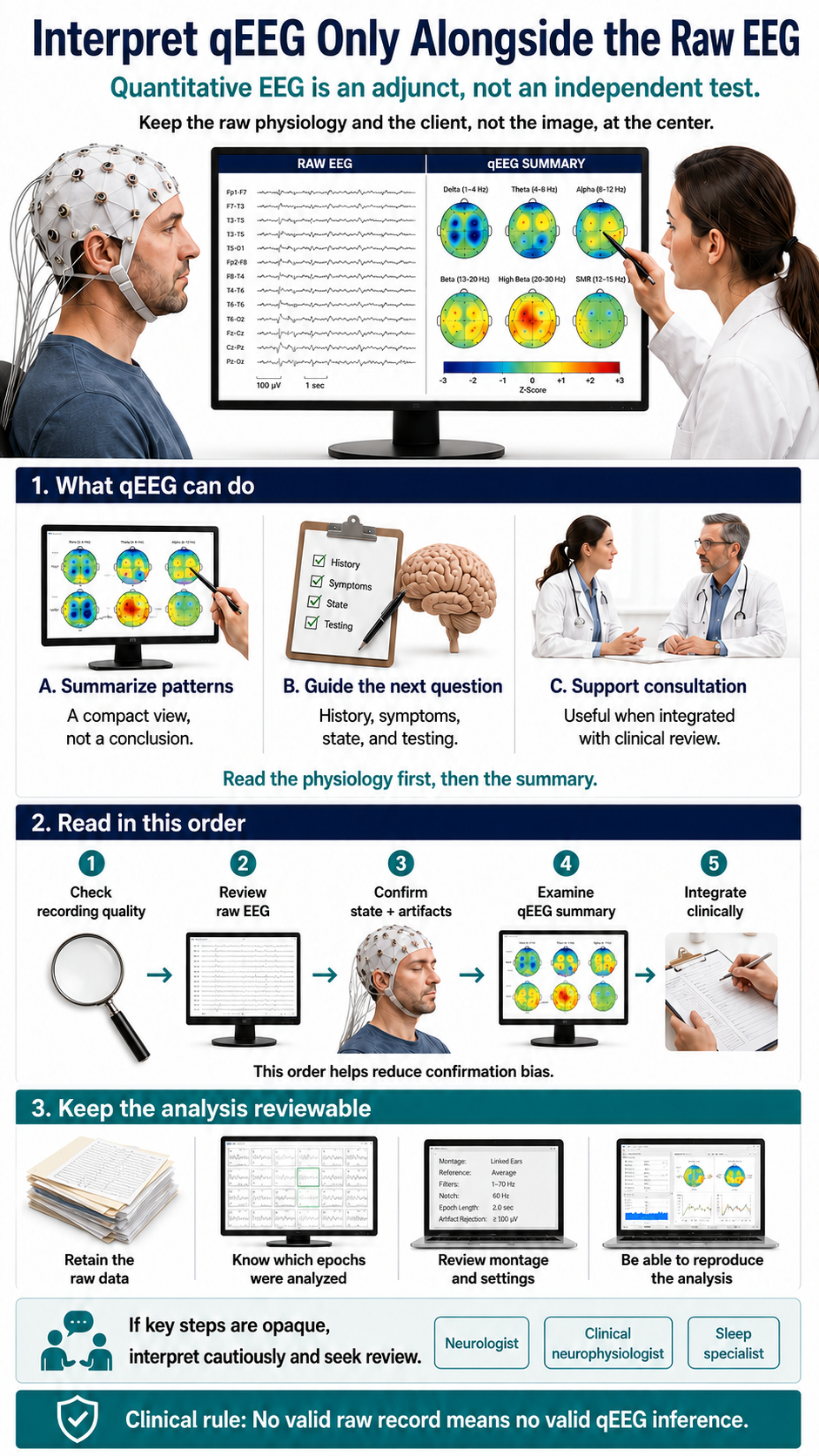
9. Expect artifacts, and continuously monitor your client's state
Artifacting is not a one-time housekeeping step finished during preprocessing. It is a competing explanation, worth reconsidering whenever the signal or reward rate changes. Treating it that way is a mark of expertise.
Blinks and slow eye movements can inflate low frequencies, especially frontally. Jaw, temporalis, neck, and scalp muscle can elevate faster frequencies. Movement, cable sway, poor contact, bridging, electrode pops, sweat, mains interference, pulse, and reference instability can create spatially convincing noncerebral patterns. Drowsiness can shift alpha and theta in ways that resemble a training effect.
Watch the client or trainee and the raw signal together. When a reward rate jumps, wonder aloud whether the person closed the eyes, tensed the jaw, shifted posture, spoke, swallowed, touched a lead, held the breath, or became drowsy. Check whether contact quality changed, the reference became noisy, or automated correction began removing a different share of the data.
Automated artifact detection is a helpful partner, and it works best when the operator knows what it detects, what it misses, whether it merely withholds feedback or transforms the signal, and how false detections affect learning. Over-aggressive cleaning can remove genuine activity; permissive cleaning can reward artifact. A little familiarity goes a long way.
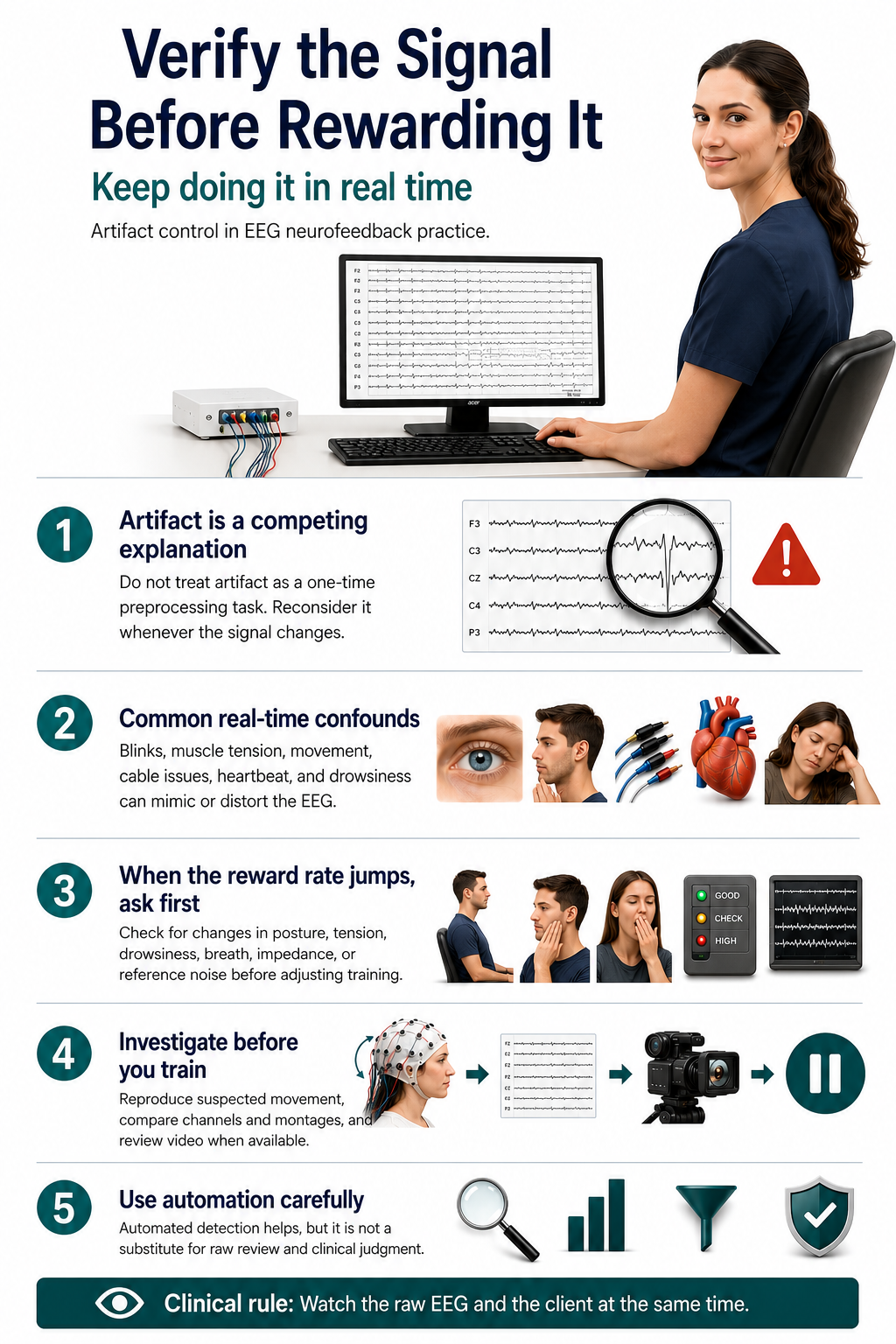
This is also the natural place to assess the wider physiological picture. Many everyday and environmental factors can shift either the symptoms or the signal, and asking about them as routine care often reveals a contributor worth addressing or referring (Swatzyna & Peavey, 2026).
A pre-session check
| Domain | Ask and document | Typical action |
|---|---|---|
| Sleep and vigilance | Sleep duration and quality, naps, shift work, insomnia, snoring or apnea, current sleepiness | Standardize conditions; pause when drowsy; reschedule or refer when the state is unsafe or unrepresentative. Because sleep and mental health influence each other so strongly, addressing sleep is often a high-value first step. |
| Medications and other substances | Prescription and over-the-counter medication, supplements, dose and timing, recent changes, alcohol, cannabis, nicotine, caffeine, and other substances | Consult the prescriber or pharmacist when helpful. Do not independently direct medication cessation. Remember that both substances and the medications used to treat substance use can carry mood and cognitive effects of their own. |
| Food, hydration, and nutrition | Time of last meal, a missed usual meal, fluid intake, diabetes, hypoglycemic symptoms, and general dietary patterns | Address immediate safety; document; reschedule or obtain medical care when appropriate. Nutritional factors and blood-sugar swings can influence mood and attention, so a primary-care or nutrition referral is sometimes the appropriate next step. |
| Illness, pain, and physiology | Fever, infection, migraine, pain flare, endocrine or metabolic symptoms, recent strenuous exercise, and any history of head injury | Defer, modify, or refer according to clinical significance. A history of even mild head injury should be documented, since its effects can emerge over time. |
| Environment and setting | Time of day, posture, eyes-open or eyes-closed condition, task, room conditions, and whether symptoms track with a particular living or working environment | Replicate under matched conditions before treating a difference as meaningful. When symptoms clearly ease away from a specific setting, an environmental evaluation may be worth suggesting. |

An EEG samples activity under particular conditions; it is a snapshot, not a fixed portrait of the person. Pharmaco-EEG guidance exists precisely because medications can change vigilance, spectral power, and reactivity (Jobert et al., 2012). Sleep, pain, illness, stress, exercise, caffeine, nicotine, alcohol, cannabis, time of day, hydration, and food intake can also shift state or artifact burden.
A missed meal does not produce one universal EEG pattern. A small 2025 crossover study found no broad behavioral or absolute-power impairment after an 18-hour fast, while reporting a possible frontal-theta change that calls for cautious interpretation (Ávila-Garibay et al., 2025). The practical, non-dramatic point is to document last food intake and symptoms, not to conclude that fasting "caused theta."
10. Keep assessment and planning matched to the context
Clinical treatment. A clinical neurofeedback assessment is richer and more rewarding than qEEG acquisition plus a software report. The responsible clinician gets to know the client's goals, symptoms, functional impairment, developmental and medical history, sleep, medication and substance use, pain, relevant trauma history, current treatment, preferences, and risk factors. Standardized measures fit the actual treatment target.
This is also where a brief screen for underlying and contributing causes fits into good care. Without overreaching scope, a clinician can keep open questions about substance use, medication side effects, possible medical or neurological contributors (including past head injuries and structural findings), genetic and metabolic factors, and environmental exposures, and can order or refer for appropriate testing when the picture warrants it.
Frameworks that move from simple observation toward more detailed testing, and that rely on interdisciplinary collaboration, help ensure nothing important is missed (Swatzyna & Peavey, 2026). The aim is not to turn a neurofeedback clinic into a medical workup center; it is to remain alert to the person's whole presentation and to coordinate with medical and environmental colleagues.
The evaluation is performed or supervised by someone whose license and competence cover the presenting problem. Neurofeedback or qEEG certification does not, by itself, create authority to diagnose or treat outside a professional scope (AAPB, 2013; ISNR, 2024).
A written plan works well when it states the functional target together with the evidence for the proposed approach in this indication and population, and when it names the reasonable alternatives.
It is stronger still when it sets out the expected session range and cost, the outcome measures and a predetermined review point, and the adverse-event monitoring and stop rules, along with the referral and coordination contingencies and, where qEEG was used, how it contributed.
The protocol makes sense from the client's goals, formulation, evidence, and safety profile, even if the qEEG image were removed from the chart.
Performance or educational training. Performance providers do well to define a measurable nonclinical goal, such as sustained attention during a task, recovery after stress, sleep regularity, or a sport-specific outcome. There is no need to convert ordinary variation into a disorder label or to imply that training treats a condition, unless the service is legitimately clinical and within scope.
Safety screening, artifact control, understandable consent, privacy, and referral remain part of the care. When symptoms suggest a medical or diagnosable mental-health condition, the provider explains the limits of the service and directs the client to consult an appropriately licensed professional, as ISNR guidance recognizes (ISNR, 2024).
Research. Research invites a protocol, appropriate ethics review, and consent that distinguish research from care, data governance, adverse-event procedures, and transparent reporting. CRED-nf is especially relevant here because it addresses experimental design, control conditions, regulation success, artifact handling, behavioral outcomes, adverse effects, and reporting (Ros et al., 2020).
A research protocol is best kept from quietly turning into individualized treatment, and clinical services are best not marketed as research to sidestep ordinary professional responsibilities.
When the qEEG and the rest of the assessment disagree. Do not give the map automatic priority. A mismatch may reflect artifact, state, database mismatch, unreliable measurement, an incomplete assessment, or a genuine but nonspecific finding. Recheck the raw signal, replicate under matched conditions, broaden the assessment, consult, or set the quantitative finding aside. Disagreement is information, not an obstacle.
11. Let algorithms assist, and keep accountable authority with people
Modern neurofeedback runs on algorithms. Filters, transforms, artifact gates, thresholds, reward schedules, adaptive difficulty, source estimates, classifiers, and displays are all computational. The ethical question is not whether an algorithm is present; it is whether software might silently control a decision for which a human professional remains accountable.
Where software helps, and where people lead.
| Appropriate assistance under human control | Decisions that call for qualified human authority |
|---|---|
| Filtering and transforms whose effects are understood | Determining whether a person is an appropriate clinical candidate |
| Displaying raw data, trends, and performance | Diagnosing a medical, mental, or neurodevelopmental disorder |
| Flagging possible artifact or state changes | Selecting the clinical target and rationale |
| Running a clinician-approved contingency | Choosing a new protocol or changing sites or frequency targets for clinical reasons |
| Adjusting difficulty or thresholds within explicit, visible, reversible bounds | Deciding that an adverse change is acceptable or that referral is unnecessary |
| Logging parameters and changes | Extending treatment or overriding a stop rule without review |
A responsible professional understands the rule, watches its effects, can override it, and documents material changes. Keeping the raw EEG and artifact information visible, rather than watching only the reward display, keeps the human in the loop. Recording software, model, and database versions rounds it out.
Broad WHO and medical-device guidance supports human autonomy, transparency, intended-use clarity, disclosure of limitations, and evaluation of the human-software team (World Health Organization [WHO], 2021; U.S. Food and Drug Administration et al., 2024).
These documents are not neurofeedback practice standards, and FDA device guidance applies only when a product and use fall within the relevant regulatory framework. They are offered here as general design and governance principles, not as direct authority for a particular protocol or staffing model.
Unexpected software behavior is best treated as a quality or safety event: pause, determine what changed, preserve logs, check whether the delivered intervention still matches the approved plan, and report or escalate as appropriate. There is no need to explain an unexplained system change as the client's brain "resisting."

12. Keep technician roles clear and well-supervised
AAPB endorses technicians providing clinical biofeedback under the direct supervision of an appropriately trained and licensed clinician. It states that treatment changes are directed by the supervisor and that the supervisor is present at the location where training occurs (AAPB, 2013).
ISNR asks providers to disclose the technician's qualifications, role, and degree of supervision (ISNR, 2024).
A skilled technician contributes substantially: electrode application, recording, coaching, documentation, and implementation of an established plan. To protect both the client and the technician, several decisions must remain outside the technician's independent authority: diagnosing or formulating a clinical condition, dismissing suspicious activity as benign, or selecting a clinical target or accepting a software-recommended protocol without review.
In the same spirit, a technician is best not asked to independently change sites, frequency targets, or other clinically material parameters outside delegated bounds, to decide that an adverse change is acceptable, or to decide that referral or escalation is unnecessary.
The supervising professional reviews the assessment and relevant raw EEG, approves the plan and permitted adjustments, defines escalation criteria, remains available as required by the applicable standard and law, and reviews outcomes and adverse events.
A written delegation protocol that names actions permitted independently, actions requiring real-time approval, and actions that are off-limits gives everyone confidence and clarity.
13. Design staffing around observation and response, not a universal slogan
Professional sources support direct supervision, observation, coaching, and accountable changes in treatment.
For clinical neurofeedback, we recommend assigning one technician to one client or to a couple trained together to improve interpersonal synchrony.
A responsible supervisor should be present and accountable as required, clients should understand the staffing model and who is responsible for them, and incidents, near misses, and outcomes are reviewed.
The concern with high-throughput arrangements is divided attention and delayed intervention, not the mere presence of multiple monitors or rooms. Neutral, observable language keeps the discussion focused on safety rather than motives.
14. Let consent explain uncertainty, supervision, and incidental findings
The step of requesting consent is an opportunity to build trust, not merely a form to complete. Alongside electrode placement and session length, it helps to explain what scalp EEG measures and what qEEG mathematically summarizes, and to be clear that EEG and qEEG are not stand-alone diagnostic tests for mental or neurodevelopmental disorders.
A thorough consent conversation covers the evidence and uncertainty for the specific indication, protocol, and population; the reasonable alternatives, expected cost and duration, outcome measures, and review points; and the possible adverse experiences the client should report.
It also specifies who will be present, whether a technician is involved, and who may make protocol changes, describes what adaptive or algorithmic features are active and what their limits are, and explains how incidental or suspicious findings will be reviewed and communicated as well as how data will be stored, shared, processed by vendors, retained, and deleted.
Teach-back is an effective way to surface misunderstandings: ask the client to explain what the qEEG can and cannot tell them, who makes decisions, what symptoms to report, and when continuation will be revisited.
A neutral incidental-finding statement is safer than either reassurance or speculation: "This observation is not diagnostic, but it warrants review by a professional qualified in medical EEG."
15. Keep an auditable record
A good record enables the next qualified professional to reconstruct what was measured, inferred, delivered, and changed.
At assessment, document the person's state, sleep, medications and other substances, dose timing, food and fluid intake, caffeine and nicotine, time of day, recording conditions, montage, reference, sampling rate, filters, contact quality or impedances, hardware and software versions, artifact procedures, rejected epochs, and the normative database or model used. Preserve the raw EEG and, when applicable, the relationship between raw epochs and quantitative results.
For planning, record the functional target, evidence base, formulation, alternatives considered, reason for the protocol, who approved it, permitted automatic adjustments, stop rules, referral contingencies, and review date.
For each session, record signal quality, observed artifacts, client state, parameters actually delivered, algorithmic changes, coaching, adverse experiences, deviations from plan, and consultation. When a technician conducts the session, identify the technician and supervisor.
"The system adjusted itself" is not quite enough on its own. Version and parameter records make it possible to confirm that a later session still delivered the intervention approved at the outset.

16. Protect neural data and choose vendors thoughtfully
The EEG is not a transcript of thought, but it is sensitive physiological data and deserves respect. Under research conditions, EEG features can even support person identification (Yang et al., 2022). Raw EEG, qEEG features, questionnaires, medication histories, video, and session metadata can together form a detailed longitudinal profile.
It helps to map the actual data flows, minimize collection, separate identifiers where feasible, encrypt storage and transfer, restrict access, set retention and deletion rules, and disclose cloud or vendor processing. The 2026 systematic review of EEG-neurofeedback ethics highlights informed consent, psychological risk, data privacy, vulnerable populations, enhancement, and scientific validity as recurring themes (Ölçüoğlu & Yıldırım, 2026).
Vendor contracts and policies are worth reading for ownership, secondary use, breach response, data location, subcontractors, model training, sale or disclosure, deletion, and export in a usable format.
Obtaining separate authorization for research, teaching, or product-development use, and never making ordinary care contingent on agreeing to unrelated secondary use, keeps trust intact.
Planning for vendor failure or discontinuation ensures clients retain access to their records. A system that blocks access to clinically material raw data, or reserves broad secondary-use rights, is best not allowed to determine care by default.
17. Use stop rules and outcome checkpoints
Setting reassessment and stopping rules before a course begins is a sound practice.
It helps to pause a session whenever the raw signal is invalid, whenever the client becomes drowsy, distressed, medically symptomatic, or unable to participate, or whenever a concerning neurological, cardiac, psychiatric, or physical change appears. The same holds true when software behaves unexpectedly, or when the trainer cannot yet explain what is being reinforced or inhibited.
Stop or substantially revise a course when harms persist, consent is compromised, a needed referral remains incomplete, costs outweigh likely benefit, the protocol has drifted from its rationale, or meaningful progress is absent at the predetermined checkpoint.
Judge outcomes by agreed clinical, functional, educational, or performance measures, not by reward scores or qEEG "normalization" alone. Ask whether attention, sleep, pain, mood, functioning, or performance improved by a meaningful amount, and whether the change can reasonably be linked to training rather than expectancy, concurrent treatment, maturation, practice effects, or regression to the mean.
This is also a natural moment to revisit lifestyle contributors (sleep, nutrition, physical activity, and environment) since gains in those areas can support and sustain the training.
CRED-nf encourages attention to regulation success, behavioral significance, adverse effects, and the relationship between brain regulation and clinical outcomes in research, and clinics may adopt those transparency habits (Ros et al., 2020).
A periodic practice audit can review raw-signal competence, artifact rates, referrals, protocol changes, staffing and response capacity, adverse events, software versions, consent comprehension, data governance, and outcomes.
EEG neurofeedback often adds modality-specific signal-processing and interpretive layers. That is reason enough to tailor a few safeguards, without ever claiming that it is inherently more ethical, more dangerous, or more important than any form of EMG, HRV, respiratory, thermal, or other biofeedback.
18. Seven takeaways
Seven ideas capture the spirit of the whole framework. The first is to match claims and duties to the context, remembering that clinical treatment, performance training, research, and formal qEEG assessment each have their own purpose and are not interchangeable.
The second is to build raw-signal competence at the right level, since every operator can grow acquisition, artifact, vigilance, and stop-rule skills while qualified clinical or medical review can be shared across a team.
The third is to let the map inform the work while investigating the underlying cause, because EEG and qEEG enrich an evaluation even as a mental or neurodevelopmental diagnosis rests on a full, multimethod picture, one that keeps substance, medical, and environmental contributors in view.
The fourth idea is to treat biomarkers and z-scores as prompts for inquiry, replicating, checking state and artifact, consulting, and correlating before using a finding in a plan.
The fifth is to keep software and quantitative summaries in supportive relationship with reviewable physiology and accountable people, welcoming automation as an assistant within visible, reversible bounds.
The sixth is to choose supervision and staffing models that can show observation, response, and accountability, treating one trainer per independent treatment unit as a conservative author recommendation rather than a universal mandate.
And the seventh is to make the practice auditable, so that clear consent, role boundaries, referral procedures, data governance, stop rules, functional outcomes, and versioned records turn good intentions into observable, sustainable practice.
EEG neurofeedback requires consistent ethical attention because a long, layered, and persuasive processing chain makes overinterpretation easy. The safeguards above answer that risk with a single discipline: keep the client, the raw physiology, the full context, and accountable human judgment ahead of any map, z-score, classifier, or report that summarizes them. Named practice contexts, labeled recommendations, shared raw-signal competence, bounded and supervised roles, clear consent, auditable records, and prospective stop rules are the means; keeping people and physiology in charge is the end.
Check Your Understanding
- Why does a long, layered processing chain make overinterpretation easy?
- What does it mean to keep the raw physiology ahead of the summary map or report?
- Why should a candidate biomarker sharpen the next step rather than settle the diagnosis?
- What belongs in an auditable record of an EEG neurofeedback course of care?
- What is the purpose of a prospective stop rule?
Emerging Ethical Issues in the Digital Age
The biofeedback field is changing faster than at any point in its history. Smartphones, wearables, telehealth platforms, and artificial intelligence are transforming how we deliver services and how clients interact with their own physiological data. These technologies bring tremendous opportunities, but they also create ethical challenges that previous generations of practitioners never had to consider. This section explores the emerging issues you will face as you build your career in this rapidly evolving landscape.
Your Client's Digital Health Footprint: Privacy Beyond the Clinic
Here is something that might surprise you: the health information your clients generate outside your office may be far less protected than what you record during sessions. When a client uses a heart rate variability app on their phone, tracks their breathing with a smartwatch, or logs stress levels in a wellness application, they are creating what researchers call a digital health footprint. This collection of digital traces can reveal remarkably detailed health information when pieced together, yet much of it falls completely outside traditional privacy protections (Grande et al., 2020).
You are probably familiar with HIPAA, the federal framework that governs how healthcare providers handle protected health information. What you may not realize is that HIPAA only applies to "covered entities" like hospitals, insurance companies, and healthcare providers, along with their business associates. Many of the consumer apps and wearable devices your clients use operate entirely outside this framework, even when the data they collect is clearly health-relevant (Grande et al., 2020).
That calming app your anxious client uses every night? The HRV tracker they wear to monitor stress? The biofeedback game they play at home between sessions? None of that data necessarily has HIPAA protection.
The Data Broker Problem
The situation gets more complicated when you consider data brokers, businesses that collect, aggregate, and sell personal information. Your client's wellness app data might be sold to advertisers, insurance companies, or employers without your client ever realizing it. The "consent" they gave was probably buried in a lengthy terms-of-service agreement that nobody actually reads. When a client clicks "I agree" to use an app you recommended, they may be agreeing to data sharing arrangements that could affect their insurance premiums, employment prospects, or targeted advertising for years to come (Grande et al., 2020).
What does this mean for your practice? When you recommend apps, devices, or platforms to clients, you have an ethical obligation to explain, in plain language, what data will be collected, who might receive that data, how long it will be stored, and what options exist for opting out. Never imply that "health app data" receives the same protection as your clinical records. Your clients deserve to make truly informed decisions about their digital health footprint.
When Breaches Happen: Your Responsibility to Clients
Imagine this scenario: You have been recommending a popular HRV training app to your clients for stress management. One morning, you learn the company experienced a data breach, and hackers accessed user accounts including names, email addresses, and detailed physiological data. What are your obligations?
Because consumer health tools often fall outside traditional medical privacy rules, regulators increasingly rely on specialized frameworks to address breaches. The Federal Trade Commission's Health Breach Notification Rule applies to certain vendors and personal health record contexts, and it has become a central compliance issue for biofeedback educators and practitioners who integrate third-party apps into their work (Federal Trade Commission, 2024).
The ethical lesson here extends beyond legal compliance. Breach readiness is not just an IT concern; it is a client protection obligation. If a tool you recommended experiences a breach, your clients will look to you for guidance. Being prepared means knowing what information was involved, being able to explain what happened in terms clients can understand, and helping them take appropriate protective steps. This transparency supports the fidelity and trust that form the foundation of professional ethics codes in biofeedback practice (AAPB, n.d.).
Cybersecurity: No Longer Someone Else's Problem
Let us be honest: many biofeedback practitioners entered this field because they wanted to help people regulate their physiology, not because they dreamed of becoming IT security experts. But modern biofeedback practice increasingly involves electronic protected health information (ePHI) and networked systems. If you create, store, or transmit sensitive physiological data, you assume responsibility for reasonable safeguards (U.S. Department of Health and Human Services, n.d.).
Think about all the ways client data flows through your practice. Session recordings stored on your computer. Assessment results emailed to referring physicians. Training data synced to cloud platforms.
Remote sessions conducted over video conferencing. Each of these creates potential vulnerabilities that did not exist when biofeedback meant a client sitting in your office connected to a standalone device with no internet connection.
A risk analysis is a structured process for identifying threats, vulnerabilities, and the safeguards needed to protect client information. It is not a one-time exercise but an ongoing responsibility that should be revisited whenever you add new technology to your practice (U.S. Department of Health and Human Services, n.d.).
The key concept is that "reasonable security" is dynamic. Remote sessions, cloud storage, and device syncing all expand what security professionals call your "attack surface," meaning the number of potential entry points for unauthorized access. This makes data minimization, access controls, and incident planning more ethically important than ever (Tully et al., 2020).
Telehealth Biofeedback: New Setting, Amplified Duties
The expansion of telehealth, accelerated dramatically by the COVID-19 pandemic, has fundamentally changed how many practitioners deliver biofeedback services. Remote training expands access for clients who cannot travel to your office, but it also raises questions about professional boundaries and jurisdiction.
Think of telepsychology competence as traditional clinical competence plus a new layer of technology-specific skills. You still need everything you learned about biofeedback assessment, protocol selection, and client rapport. But now you also need competence in platform selection, privacy settings, emergency planning for remote sessions, and maintaining communication clarity when technology mediates your interactions (American Psychological Association, 2013).
Recent guidance from professional organizations emphasizes practical resources for documentation, risk management, and service delivery decisions in telehealth contexts (Perle et al., 2025). Rather than thinking of telehealth as creating entirely new ethical rules, consider it a setting that amplifies your classic duties. Confidentiality still matters, but now you must consider whether your client's family members can overhear sessions, whether the platform encrypts transmissions, and whether session recordings are stored securely. Competence still matters, but now it includes knowing how to troubleshoot connection problems, adapt protocols for home equipment, and recognize when remote delivery is not appropriate for a particular client.
Wearables and the Question of Measurement Honesty
Consumer wearables have made biofeedback more accessible than ever. Your clients can track heart rate variability on their smartwatches, monitor breathing patterns with chest straps, and practice stress management using smartphone apps. But this accessibility comes with an ethical responsibility that we might call "measurement honesty."
Here is the problem: because the numbers are digital, clients often assume they are precise. A heart rate of 72 beats per minute displayed on a screen feels authoritative in a way that a rough estimate never would. But consumer-grade optical sensing, often using photoplethysmography (PPG), can perform quite differently across contexts.
Movement affects accuracy. Rapid physiological changes can confuse algorithms. Different devices use different processing methods that may not be comparable (Icenhower et al., 2025).
This becomes an ethics issue when you overstate what a metric means, treat noisy data as if it were diagnostic-quality information, or fail to explain the limitations of consumer devices. The validity of a measurement, meaning whether it actually reflects what it claims to measure, and its reliability, meaning whether it produces consistent results across time and conditions, matter enormously for the conclusions your clients draw from their data.
A Simple Principle for Wearable Data
Feedback is only therapeutic when clients can trust that the signal is fit for its intended purpose. This means being honest about what consumer devices can and cannot tell us. A smartwatch HRV reading can be useful for noticing general trends and patterns over time. It should not be treated as equivalent to a clinical-grade ECG assessment. When uncertainty exists, explain it clearly so clients do not confuse "tracking" with "diagnosis."
Equity and Bias in Sensing Technologies
A related issue that is gaining attention involves potential bias in how sensing technologies perform across different populations. Some research has raised concerns that optical sensors may not work equally well for all skin tones, which could produce inequitable outcomes if biofeedback recommendations rely heavily on consumer sensors.
Even when individual studies find limited effects for a given device and protocol, the broader principle remains important: performance can vary by hardware, firmware, activity context, and population characteristics. Ethical practice requires cautious interpretation and ongoing attention to whether your tools work well for all your clients, rather than assuming that a "neutral" device produces equally valid results for everyone (Icenhower et al., 2025).
This connects to broader concerns about health equity, the principle that everyone should have fair opportunities for optimal health outcomes. An apparently neutral device can still create unequal burdens if some clients must purchase expensive upgrades to get stable readings, or if certain clients systematically receive noisier feedback that undermines their learning and self-efficacy.
Artificial Intelligence: The Black Box Problem
Biofeedback platforms increasingly incorporate artificial intelligence (AI) for tasks like artifact detection, trend prediction, coaching prompts, and personalized protocol recommendations. AI can make sophisticated analysis available to practitioners who lack specialized training, potentially improving care. But it also introduces a significant ethical challenge: opacity.
When an AI system operates as a black box, neither you nor your client can easily explain why it produced a particular recommendation. The algorithm learned patterns from training data, but the specific reasoning behind any individual output may be impossible to articulate. This creates problems for accountability and informed consent. How can clients make informed decisions about their care if neither they nor their provider can explain why the system is recommending a particular approach? (National Institute of Standards and Technology, 2023).
Before adopting any AI-powered biofeedback tool, work through these questions: What exactly does the algorithm do? What data does it use to make recommendations? What outcomes is it optimizing for? What human oversight exists to catch errors? Based on your answers, decide what information clients need to make an informed choice about using the tool (World Health Organization, 2021; National Institute of Standards and Technology, 2023).
AI as Adjunct, Not Authority
The ethical risk with AI in biofeedback practice is not the technology itself but the gradual transfer of decision authority away from the practitioner. Large language models now help clinicians draft session notes, synthesize literature, and brainstorm protocol options, while AI-driven analytics surface patterns in qEEG and HRV data that a busy practitioner might miss (Topol, 2019). These tools have genuine value: they reduce documentation burden, surface relevant literature, and highlight patterns that support evidence-based practice (Lehrer et al., 2020).
The danger is what one recent framework describes as AI-induced false confidence (Integrated Neuroregulation and Embodied Wellbeing, 2025). AI outputs are often fluent and persuasive, which can lull clinicians into accepting summaries without verifying sources, adopting protocol suggestions without checking their rationale, or signing generated notes that contain errors. Each such moment seems trivial in isolation, but together they erode professional accountability.
AI assists; the practitioner decides. AI may structure information, summarize literature, and surface patterns. AI may not initiate clinical direction, determine protocol changes, or override professional judgment. Documented decision authority remains with the certificant.
Just as clients are informed about other consultative inputs, they should know when AI tools contribute substantively to their assessment, protocol selection, or documentation. This is consistent with informed consent obligations. Documentation should reflect human review of any AI-generated content, and licensing boards will hold the licensee accountable for the final decision regardless of which tool produced the draft (Schwartz & Andrasik, 2017).
Restraint, Referral, and Human Primacy
Ethical practice in this technology-saturated era often means doing less, not more. Devices generate continuous data that invites continuous adjustment. Clients sometimes expect novelty rather than consolidation. AI tools can suggest endless refinements.
Yet the BCIA Professional Standards and Ethical Principles of Biofeedback directs practitioners to continue services only as long as clients benefit, and to help clients obtain other care when needed (Biofeedback Certification International Alliance, 2016). Holding a protocol steady when stability is what the client needs requires real discipline (Gruzelier, 2014; Sherlin et al., 2011; Thompson & Thompson, 2015).
Defined escalation thresholds support this discipline. When you articulate in advance the signals that will trigger a pause or referral, including autonomic instability, ambiguous or paradoxical response, somatic safety signs, and pressure on scope of practice, those moments become structural decisions rather than judgment calls under pressure. Acting on these thresholds protects both the client and the practitioner. Failing to act when a threshold is reached is a process lapse regardless of outcome.
Human primacy is the closing principle. Wearables, apps, and AI analytics now produce more physiological data than the field has ever had to interpret (Shaffer & Ginsberg, 2017). When those outputs conflict with what you observe in the room or what your client reports, your clinical judgment and your client's welfare govern the decision. Data informs care; data does not replace the clinician. This is the ethical anchor that keeps biofeedback practice human, accountable, and aligned with the field's founding commitment to dignity and competent service.
Software as a Medical Product: Recognizing Scope Creep
Some biofeedback-related software exists in an ambiguous zone between wellness tool and regulated medical device. This ambiguity creates opportunities for scope creep, where a tool's marketing and functionality gradually imply medical authority even when the evidence base or regulatory oversight is limited.
Consider how this might unfold. A developer creates an app for "stress awareness" using basic HRV metrics. Over time, the app adds features: it starts labeling readings as "normal" or "concerning," suggests that certain patterns indicate specific conditions, and offers clinical decision support recommendations that edge into diagnostic territory. At what point does a wellness tool become something that should be regulated by the FDA? (Food and Drug Administration, 2022a).
This matters ethically because clients often interpret authoritative language as medical validation. When an app tells them their "stress level is dangerously high" or their "nervous system is dysregulated," they may not realize they are receiving outputs from an unvalidated algorithm rather than a clinical assessment. Your responsibility includes recognizing when tools exceed their appropriate scope, maintaining discipline about claims, making appropriate referrals, and documenting accurately what any tool can and cannot do.
Conflicts of Interest in the App Economy
As biofeedback moves into apps, subscriptions, and device ecosystems, conflicts of interest become easier to create and harder for clients to detect. A conflict exists whenever your financial incentives could reasonably be perceived as influencing your clinical recommendations (Refolo et al., 2022).
Think about the ways this might arise. Perhaps a wearable company offers you affiliate commissions for recommending their device. Maybe you receive free access to premium software features in exchange for steering clients toward a particular platform. You might have invested in a biofeedback startup or developed your own app that competes with alternatives you could recommend.
Disclosure is essential but not sufficient. Even when you tell clients about financial relationships, they may not fully appreciate how incentives could shape recommendations. Ethical practice requires separating your clinical judgment from product marketing and being able to document why a recommendation is clinically appropriate independent of any financial relationship.
Navigating a Patchwork of Privacy Laws
Privacy regulation in the United States is becoming increasingly complex, with different rules applying depending on the state, the type of data, and the nature of the entity collecting it. Some states have enacted specific protections for consumer health data that go well beyond federal requirements and may define health-related information very broadly.
Washington State's My Health My Data Act, for example, creates obligations around collection, sharing, and consent for health data that apply even to entities that are not traditional healthcare providers (Washington State Legislature, 2023). If you practice in Washington, or if you have clients in Washington using apps and platforms you recommended, these rules may apply to you in ways that HIPAA does not.
The practical takeaway is that "privacy compliance" is becoming jurisdiction-dependent and platform-dependent. Rather than relying on a single federal framework to cover all your biofeedback-related tools, adopt conservative best practices: minimize the data you collect, use clear consent processes, conduct due diligence on vendors before recommending them, and stay informed about evolving regulations in the jurisdictions where you practice.
Digital tools are reshaping biofeedback faster than professional standards can be rewritten, so practitioners must extend classic ethical duties into new territory. Much of the health data clients generate through apps and wearables falls outside HIPAA, obligating providers to explain data collection, sharing, and breach risks in plain language. Telehealth, cloud storage, and networked devices expand the attack surface, making cybersecurity, risk analysis, and telepsychology competence part of ethical practice. Consumer sensors invite measurement dishonesty and equity concerns, while AI introduces opacity that can quietly shift decision authority away from the clinician. The unifying principle is human primacy: data and algorithms inform care, but the certificant remains accountable for every clinical decision.
Check Your Understanding
- Why does much of the health data clients generate fall outside HIPAA protection?
- What does it mean that telehealth and networked devices expand your attack surface?
- What should you tell clients about the accuracy limits of consumer wearables?
- How does the black box problem shift decision authority, and how do you keep it?
- What does the principle of human primacy require of you?
Test Yourself
Ready to check what you have learned? The ClassMarker test over this unit runs 10 questions and needs no exam password. You may retake it as often as you like, and your score reports immediately so you can see which sections deserve another read.
Review Your Flashcards
The Quizlet flashcard set for this chapter rehearses the glossary terms below. Work through the deck in Learn mode before you attempt the ClassMarker test, then return to it a few days later so the terminology moves into long-term memory.
Assignment
Based on your own clinical experience, what are the hardest ethical decisions you've made in biofeedback practice?
Glossary
adaptive threshold: A feedback criterion that changes according to a programmed rule. Ethical use requires bounded settings, visibility, reversibility, and clinician oversight.
algorithmic clinical authority: The power to make or effectively control a clinical decision. In neurofeedback, this authority should remain with the responsible human provider rather than with software.
anonymity: the protection of a client's identity.
arachnoid cyst: a fluid-filled sac between the brain or spinal cord and the arachnoid membrane. Usually congenital and often asymptomatic, it is a structural finding that can occasionally contribute to neurological or psychiatric symptoms.
artifact: Physiological, environmental, movement-related, or equipment-generated activity that contaminates the EEG or is mistaken for the intended cerebral signal.
artificial intelligence (AI): a set of computational methods that learn patterns from data to generate predictions, classifications, or automated decisions.
assent: willingness to participate in treatment or research without necessarily understanding all implications; typically obtained from children or individuals with cognitive impairments who cannot provide full informed consent.
atypical presentation: A symptom picture that does not fit the expected onset, course, severity, or treatment response for the working diagnosis, and that therefore warrants a search for a contributing medical, medication, or environmental factor.
automation bias: The tendency to trust a computerized recommendation more than is justified, especially when it appears precise or objective.
autonomy: the right to make one's own decisions about care and treatment.
BCIA: the Biofeedback Certification International Alliance.
beneficence: the ethical principle of actively working to benefit clients and avoid harm.
biomarker: A measurable characteristic evaluated as an indicator of a biological or clinical process. Correlation with a disorder does not by itself make a marker diagnostically or therapeutically actionable.
black box (opacity): a situation where a computational model's internal reasoning is not readily interpretable to users, limiting transparency and accountability.
bounded assistance: algorithmic or software support that operates within explicit, visible, and reversible limits under human oversight, so that it informs rather than silently controls a clinical decision.
bradycardia: a slow heart rate, generally below 60 beats per minute in adults. It can be a normal finding in physically fit individuals or, when accompanied by symptoms, a sign of a conduction problem.
candidate biomarker: a measurable characteristic associated with a biological or clinical process but not yet validated for a specific diagnostic, prognostic, treatment-selection, or monitoring use.
cardiac artifact: ECG or pulse-related activity that appears in an EEG channel through electrical or mechanical coupling. It should not be interpreted as cerebral activity or as a cardiac diagnosis.
cerebral perfusion: the flow of blood through the brain that delivers oxygen and nutrients to neural tissue. It cannot be validly inferred from the amplitude or frequency of the posterior dominant rhythm.
certificant: an individual who has been certified by BCIA.
certificate of completion: recognition by BCIA that an applicant has completed an approved didactic workshop based on BCIA's blueprint and passed an exam over its content.
certification: recognition by the BCIA that an applicant has met its requirements for entry-level competence in the provision of biofeedback services.
Chiari malformation: a structural condition in which brain tissue at the base of the skull extends into the spinal canal. It can be asymptomatic or produce headache, balance disturbance, and other neurological symptoms.
chronic inflammatory response syndrome (CIRS): a proposed multi-system illness attributed to biotoxin exposure, most often indoor mold. It appears in neither the DSM nor the ICD and its evidence base is disputed by several professional bodies, so a neurofeedback provider treats a suspected exposure as a reason to refer for medical evaluation rather than as an established diagnosis.
client: recipient of biofeedback services.
clinical correlation: Interpretation of a physiological finding in relation to history, symptoms, examination, state, other tests, and the clinical question rather than in isolation.
clinical decision support: software functions that provide patient-specific assessments or recommendations intended to support clinical decision-making.
clinical EEG: An EEG obtained and interpreted for medical diagnostic purposes under applicable clinical neurophysiology standards. A neurofeedback assessment is not automatically a diagnostic clinical EEG.
common vehicle transmission: transfer of infectious organisms by equipment, including cables and sensors.
competence: level of proficiency.
confidentiality: a client's right to keep personal information private.
conflict of interest: a circumstance in which secondary interests, often financial, could reasonably be perceived to influence professional judgment.
consent: agreement to participate in treatment or research after understanding what is involved and its implications, made by someone with authority to make that decision.
consumer health data: health-related information collected in consumer contexts, often defined broadly in emerging state laws and not limited to clinical records.
continuing education: organized learning experiences undertaken after a credential has been earned to ensure up-to-date knowledge.
copyright infringement: when copyrighted material is used without permission from the copyright holder, violating one or more of the copyright owner's exclusive rights, such as the right to reproduce, distribute, perform, or display the work publicly.
CRED-nf: the Consensus on the Reporting and Experimental Design of Clinical and Cognitive-Behavioural Neurofeedback studies, a 2020 best-practices checklist that sets standardized guidelines for designing and reporting neurofeedback experiments, covering things like control groups, blinding, pre-registration, and how to document regulation success, in order to improve rigor and reproducibility in the field.
cybersecurity: the protection of systems and data from unauthorized access, disruption, or misuse.
data broker: a business that collects, aggregates, and sells personal data, sometimes enabling health-relevant inferences.
deception: withholding information or providing false information to research participants.
diffuse encephalopathy: a condition characterized by widespread brain dysfunction, often resulting from various causes such as infections, toxins, metabolic imbalances, or systemic diseases. It typically manifests as altered mental status, confusion, lethargy, and other cognitive impairments. Diagnosis usually involves clinical assessment and imaging studies like EEG or MRI, and treatment focuses on addressing the underlying cause to alleviate the symptoms.
digital health footprint: the collection of digital traces that can reveal health-relevant information when aggregated across sources.
direct supervision: Active, accountable oversight in which the responsible professional is present or immediately available as required, reviews the plan and data, and directs all clinical changes.
dual relationship (also called multiple relationship): a situation where a healthcare provider and patient share multiple roles. For example, when a client is also an employee.
dyad: Two people treated as one intentional clinical unit, such as a couple engaged in a specified co-regulation intervention. It is not a label for two unrelated clients scheduled together for convenience.
EEG: Electroencephalography, the recording of voltage differences at the scalp that reflect a mixture of neural, physiological, environmental, and technical sources.
effect size: the magnitude of a treatment's impact, providing information about practical significance beyond statistical significance.
efficacy: effectiveness.
electronic protected health information (ePHI): health information stored or transmitted electronically within HIPAA-regulated contexts.
EMG biofeedback: Feedback derived from electrical activity associated with muscle contraction, usually recorded with surface electrodes.
encryption: scrambling data so it's unreadable without a decryption key.
epileptiform discharge: A waveform or pattern that may be associated with increased seizure propensity when identified and interpreted by a qualified clinical EEG professional. Suspicion in a neurofeedback record warrants referral, not independent diagnosis.
ethics: the branch of philosophy that deals with moral issues.
fair use: a legal doctrine that permits limited use of copyrighted material without acquiring permission from the copyright holder, for purposes such as criticism, commentary, news reporting, teaching, scholarship, or research, considering factors like the purpose of use, the nature of the copyrighted work, the amount used in relation to the whole work, and the effect of the use on the market for the original work.
fiduciary responsibility: the duty to act in clients' financial best interests, placing client welfare above personal financial gain.
focal neurological symptoms: signs or symptoms localized to a specific region of the nervous system, such as one-sided weakness, numbness, visual loss, or speech disturbance, that warrant prompt medical evaluation.
functional overdose: when normal medication doses become excessive due to physiological changes (such as those produced by biofeedback training), potentially causing adverse effects.
Health Breach Notification Rule: a U.S. FTC rule requiring notifications for certain breaches involving identifiable health information in covered consumer contexts.
health equity: fairness in health opportunities and outcomes, including avoiding systematic disadvantages created by technology design or access barriers.
HIPAA: the U.S. Health Insurance Portability and Accountability Act framework governing privacy and security for covered entities and business associates.
HRV biofeedback: Feedback based on variation in beat-to-beat cardiac intervals, commonly coordinated with paced or resonance-frequency breathing.
human-in-the-loop: A design in which a qualified human reviews, controls, and can override algorithmic outputs at clinically meaningful decision points.
hypomania: a distinct period of elevated, expansive, or irritable mood and increased activity that is less severe than mania and does not cause marked functional impairment or psychosis.
incidental finding: An unexpected observation that may have health significance but falls outside the original purpose of the assessment and requires a defined communication and referral process.
informed consent: a written statement in which participants voluntarily confirm their willingness to participate in a research study following disclosure of all aspects of the study relevant to their decision to participate.
integrative medicine: Coordinated care that combines conventional and complementary approaches within a whole-person framework. It should not replace indicated conventional evaluation or exceed the practitioner's credentials.
intentional dyad: an author-proposed term for two people participating as one defined intervention because their joint interaction is the target. It is not a convenience label for unrelated clients scheduled together.
Licensed (L) designation: BCIA's designation for certificants who hold a valid clinical license, shown as BCN-L or BCB-L. The suffix identifies licensure status; it does not itself expand scope of practice.
licensure: legal permission granted to a professional to practice a profession.
mental health diagnosis: A clinical determination based on recognized diagnostic criteria and a multimethod assessment by a qualified professional, not on EEG, qEEG, or a software classifier alone.
mentoring: a relationship between a mentor and candidate that promotes the development of skill, knowledge, responsibility, and ethical standards in the practice of biofeedback.
montage: The arrangement of EEG channel derivations used to display voltage differences. Different montages can reveal or obscure patterns and artifacts.
neurodiagnostic red flag: A symptom, behavior, history, or raw EEG feature that raises concern for a neurological or other medical condition and triggers pause, consultation, or referral.
normal-pressure hydrocephalus pattern: a purported EEG signature of normal-pressure hydrocephalus, typically inferred from generalized slowing. Because generalized slowing is nonspecific, it is not a valid stand-alone basis for diagnosis or referral.
normative database: A reference dataset used to compare an individual's quantitative EEG values with a selected population. Its relevance depends on sample characteristics, recording conditions, hardware, processing, and statistical assumptions.
off-label: using a medical device or medication for purposes outside the labeling that a regulator such as the FDA has cleared or approved. Most biofeedback devices are FDA-cleared through the 510(k) pathway rather than FDA-approved.
palpitations: the subjective awareness of one's own heartbeat, often described as pounding, fluttering, or skipped beats. Sustained palpitations accompanied by instability warrant medical evaluation.
PANS/PANDAS: clinically defined pediatric syndromes involving abrupt onset of obsessive-compulsive symptoms, restricted eating, or tics. PANDAS requires a temporal association with streptococcal infection; PANS is the broader category and requires no identified trigger. A postinfectious autoimmune mechanism is hypothesized but not established, and neither syndrome is classified as autoimmune encephalitis.
paroxysmal: describing activity or symptoms that begin and end abruptly, such as a sudden burst of EEG activity or an episodic clinical event.
Pelvic Muscle Dysfunction Biofeedback Certification: BCIA certification available only to licensed providers who use biofeedback and behavioral interventions for elimination disorders and pelvic pain within their scope of practice.
Performance (P) designation: BCIA's designation for certificants who are not clinically licensed and who work in performance-enhancement contexts such as sport, corporate, military, or academic research settings, shown as BCN-P or BCB-P.
photoplethysmography (PPG): an optical sensing method that estimates cardiovascular signals from light absorption changes in tissue.
physiological state confound: A temporary condition, such as drowsiness, medication exposure, fasting, pain, illness, or stimulant use, that changes the recording and may be mistaken for a stable trait.
polypharmacy: the concurrent use of multiple medications by one person, which increases the risk of drug interactions and side effects and can alter both the EEG and the clinical presentation.
protocol drift: Unplanned or poorly documented change in training targets, thresholds, sites, contingencies, or dose over time, including changes introduced by adaptive software.
provider: the professional who supervises biofeedback training.
qEEG: Quantitative electroencephalography, the numerical analysis of selected EEG features, sometimes compared with normative data. It is an adjunctive analysis, not a stand-alone psychological diagnostic test.
raw EEG: The time-series voltage record before or alongside quantitative summarization. It is the essential reference for evaluating artifact, state, morphology, timing, and the validity of qEEG findings.
reference: The electrode or mathematical reference against which EEG voltage differences are calculated. Reference choice can materially alter apparent amplitude, topography, and connectivity.
reliability: the consistency of a measurement across time or conditions.
risk analysis: a structured process for identifying threats and vulnerabilities and documenting safeguards to reduce risk.
scope creep: gradual expansion of a tool's implied purpose, such as shifting from wellness tracking toward diagnostic or treatment claims.
scope of practice: the specific services a practitioner may legally provide under their license or supervisor's license as defined by state law.
signal validity: The degree to which the recorded and processed feature actually represents the intended physiological phenomenon under the stated conditions.
stop rule: a predetermined criterion, set before treatment begins, that specifies when a session or course of training should be paused, revised, or discontinued.
supervision: the provision of guidance for clinical practice for qualified health professionals by a more experienced health professional who assumes some legal responsibility and liability for the quality of the services provided.
syncope: a transient loss of consciousness caused by a temporary reduction in blood flow to the brain, commonly called fainting. Its evaluation centers on history, examination, and a 12-lead ECG rather than qEEG.
tachycardia: a fast heart rate, generally above 100 beats per minute in adults, which may be physiologic or a sign of a cardiac or systemic condition.
technician: A person who implements defined technical or coaching tasks under appropriate supervision but does not independently diagnose, formulate treatment, or make clinical protocol changes.
Technician (T) designation: BCIA's designation for support personnel who practice under the legal supervision of a licensed, BCIA-certified professional and strictly within that supervisor's scope. Technicians may not supervise or mentor other certification candidates.
telepsychology: psychological services delivered using telecommunication technologies, requiring adapted competence, privacy, and risk management practices.
threshold: The criterion a physiological feature must meet for feedback or reward to occur. Threshold design influences learning and must be clinically justified and monitored.
trait–state distinction: The difference between a relatively enduring characteristic and a temporary condition. Neurofeedback interpretation must not mistake a single state-dependent recording for a stable trait.
underlying cause: a substance-related, medical, neurological, genetic, or environmental factor that can contribute to, or mimic, a psychiatric presentation, and that may respond to targeted, often interdisciplinary, care.
validity: the degree to which a measure reflects what it claims to measure.
z-score: A standardized value expressing distance from a reference mean in standard-deviation units. It is not the probability of a diagnosis or proof that a feature requires treatment.
References
Abi-Dargham, A., Moeller, S. J., Ali, F., DeLorenzo, C., Domschke, K., Horga, G., Jutla, A., Kotov, R., Paulus, M. P., Rubio, J. M., Sanacora, G., Veenstra-VanderWeele, J., & Krystal, J. H. (2023). Candidate biomarkers in psychiatric disorders: State of the field. World Psychiatry, 22(2), 236–262. https://doi.org/10.1002/wps.21078
American Academy of Neurology. (n.d.). Retired guideline notice: Assessment of digital EEG, quantitative EEG, and EEG brain mapping. https://neurologytoday.aan.com/doi/full/10.1212/WNL.49.1.277
American Psychological Association. (2013). Guidelines for the practice of telepsychology. American Psychologist, 68(9), 791–800. https://doi.org/10.1037/a0035001
American Psychological Association. (2017a). Ethical principles of psychologists and code of conduct (2002, amended effective June 1, 2010, and January 1, 2017). https://www.apa.org/ethics/code
American Psychological Association. (2017b). Multicultural guidelines: An ecological approach to context, identity, and intersectionality. https://www.apa.org/about/policy/multicultural-guidelines.pdf
Association for Applied Psychophysiology and Biofeedback. (n.d.). Code of ethics.
Association for Applied Psychophysiology and Biofeedback. (1994). Clinical efficacy and cost effectiveness of biofeedback therapy: Guidelines for third party reimbursement (2nd ed.). Author.
Association for Applied Psychophysiology and Biofeedback. (1995). Clinical applications of biofeedback and applied psychophysiology: A series of white papers prepared in the public interest by AAPB. Author.
Association for Applied Psychophysiology and Biofeedback. (2003). Ethical principles of applied psychophysiology and biofeedback (4th revision). Author.
Association for Applied Psychophysiology and Biofeedback. (2013). Standards for performing biofeedback.
Ávila-Garibay, A., González-Garrido, A. A., Gómez-Velázquez, F. R., Brofman-Epelbaum, J. J., Vélez-Pérez, H., Romo-Vázquez, R., & Gallardo-Moreno, G. B. (2025). Fasting and cognitive load-related changes in quantitative EEG measures during an N-back task. International Journal of Psychological Research, 18(1), 59–68. https://doi.org/10.21500/20112084.6690
Biofeedback Certification International Alliance. (n.d.). Professional standards and ethical principles.
Biofeedback Certification International Alliance. (2011). What is certification?
Biofeedback Certification International Alliance. (2015). Why choose BCIA biofeedback certification?
Biofeedback Certification International Alliance. (2016). Professional standards and ethical principles of biofeedback (9th rev.).
Biofeedback Certification International Alliance. (2026). Professional standards and ethical principles of biofeedback (10th rev., adopted May 2, 2026).
Collura, T., Cantor, D., Chartier, D., Crago, R., Hartzoge, A., Hurd, M., Kerson, C., Lubar, J., Nash, J., Prichep, L. S., Surmeli, T., Thompson, T., Tracy, M., & Turner, R. (2025). International QEEG Certification Board guideline: Minimum technical requirements for performing clinical quantitative electroencephalography. Clinical EEG and Neuroscience, 56(5), 391–399. https://doi.org/10.1177/15500594241308654
Crawford, J. (2013). What's new with BCIA? Biofeedback, 41(3), 85–87. https://doi.org/10.5298/1081-5937-41.3.07
Crawford, J., & Shaffer, F. (2014). What BCIA learned from Bob Dylan. Biofeedback, 42(1), 9–11. https://doi.org/10.5298/1081-5937-42.1.05
Federal Trade Commission. (2024). Statement of policy regarding the Health Breach Notification Rule.
Food and Drug Administration. (2022a). Clinical decision support software: Guidance for industry and Food and Drug Administration staff.
Food and Drug Administration. (2022b). Mobile medical applications: Guidance for industry and Food and Drug Administration staff.
Grande, D., Luna Marti, X., Feuerstein-Simon, R., Merchant, R. M., Asch, D. A., Lewson, A., & Cannuscio, C. C. (2020). Health policy and privacy challenges associated with digital technology. JAMA Network Open, 3(7), e208285. https://doi.org/10.1001/jamanetworkopen.2020.8285
Gruzelier, J. H. (2014). EEG-neurofeedback for optimising performance. I: A review of cognitive and affective outcome in healthy participants. Neuroscience and Biobehavioral Reviews, 44, 124–141. https://doi.org/10.1016/j.neubiorev.2013.09.015
Hagedorn, D. (2014). Infection risk mitigation for biofeedback providers. Biofeedback, 42(3), 93–95. https://doi.org/10.5298/1081-5937-42.3.06
Hammond, D. C. (2010). The need for individualization in neurofeedback: Heterogeneity in QEEG patterns associated with diagnoses and symptoms. Applied Psychophysiology and Biofeedback, 35(1), 31–36. https://doi.org/10.1007/s10484-009-9106-1
Hammond, D. C., Bodenhamer-Davis, G., Gluck, G., Stokes, D., Harper, S. H., Trudeau, D., MacDonald, M., Lunt, J., & Kirk, L. (2011). Standards of practice for neurofeedback and neurotherapy: A position paper of the International Society for Neurofeedback & Research. Journal of Neurotherapy, 15(1), 54–64. https://doi.org/10.1080/10874208.2010.545760
Hammond, D. C., Walker, J., Hoffman, D., Lubar, J. F., Trudeau, D. L., Gurnee, R., & Horvat, J. (2004). Standards for the use of quantitative electroencephalography (QEEG) in neurofeedback: A position paper of the International Society for Neuronal Regulation. Journal of Neurotherapy, 8(1), 5–27. https://doi.org/10.1300/J184v08n01_02
Herman, S. T., Abend, N. S., Bleck, T. P., Chapman, K. E., Drislane, F. W., Emerson, R. G., Gerard, E. E., Hahn, C. D., Husain, A. M., Kaplan, P. W., LaRoche, S. M., Nuwer, M. R., Quigg, M., Riviello, J. J., Schmitt, S. E., Simmons, L. E., Tsuchida, T. N., & Hirsch, L. J. (2015). Consensus statement on continuous EEG in critically ill adults and children, part II: Personnel, technical specifications, and clinical practice. Journal of Clinical Neurophysiology, 32(2), 96–108. https://doi.org/10.1097/WNP.0000000000000165
Hopkins, B. (2013). Legal aspects of counseling: What you don't know might hurt you. Workshop presented at the Biofeedback Society of Texas conference, Austin, Texas.
Humane care and use of animals (A 343401) (Federal Regulations).
Icenhower, A. L., Murphy, C. M., Brooks, A. K., & Fanning, J. (2025). Investigating the accuracy of Garmin PPG sensors on differing skin types based on the Fitzpatrick scale: Cross-sectional comparison study. Frontiers in Digital Health. https://doi.org/10.3389/fdgth.2025.1553565
Integrated Neuroregulation and Embodied Wellbeing. (2025). INEW authority and boundary guidelines: IPU-aligned guidance framework. INEW.
International Society for Neuroregulation & Research. (2024). Guidelines for practice (ratified July 28, 2024).
Jobert, M., Wilson, F. J., Ruigt, G. S. F., Brunovsky, M., Prichep, L. S., Drinkenburg, W. H. I. M., & the IPEG Pharmaco-EEG Guidelines Committee. (2012). Guidelines for the recording and evaluation of pharmaco-EEG data in man: The International Pharmaco-EEG Society (IPEG). Neuropsychobiology, 66(4), 201–220. https://doi.org/10.1159/000343478
Kusumoto, F. M., Schoenfeld, M. H., Barrett, C., Edgerton, J. R., Ellenbogen, K. A., Gold, M. R., Goldschlager, N. F., Hamilton, R. M., Joglar, J. A., Kim, R. J., Lee, R., Marine, J. E., McLeod, C. J., Oken, K. R., Patton, K. K., Pellegrini, C. N., Selzman, K. A., Thompson, A., & Varosy, P. D. (2019). 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay. Circulation, 140(8), e382–e482. https://doi.org/10.1161/CIR.0000000000000628
Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research: Recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, Article 213. https://doi.org/10.3389/fpsyg.2017.00213
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., Sgobba, P., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta-analysis. Applied Psychophysiology and Biofeedback, 45(3), 109–129. https://doi.org/10.1007/s10484-020-09466-z
Lehrer, P. M., & Gevirtz, R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 5, Article 756. https://doi.org/10.3389/fpsyg.2014.00756
Moss, D. (2013). Professional conduct in biofeedback and neurofeedback. Workshop presented at the International Society for Neurofeedback and Research conference, Dallas, Texas.
Moss, D. (2020). Professional conduct in biofeedback and neurofeedback. BCIA Webinar presented to BCIA.
Moss, D., Hagedorn, D., Combatalade, D., & Neblett, R. (2019). A guide to normal values for biofeedback. In D. Moss & F. Shaffer (Eds.), Physiological recording technology and applications in biofeedback and neurofeedback. Association for Applied Psychophysiology and Biofeedback.
National Center for Complementary and Integrative Health. (2021). Complementary, alternative, or integrative health: What’s in a name?
National Institute of Mental Health. (n.d.). Help for mental illnesses. Retrieved July 12, 2026, from https://www.nimh.nih.gov/health/find-help
National Institute of Standards and Technology. (2023). AI Risk Management Framework (AI RMF 1.0) (NIST AI 100-1).
Nuwer, M. R. (1997). Assessment of digital EEG, quantitative EEG, and EEG brain mapping: Report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology, 49(1), 277–292. https://doi.org/10.1212/WNL.49.1.277 (Retired guideline; cited for historical context only.)
Ölçüoğlu, R., & Yıldırım, R. V. (2026). Ethical challenges in EEG neurofeedback: A systematic review of gaps, risks, and responsibilities. BMC Medical Ethics, 27, Article 43. https://doi.org/10.1186/s12910-026-01408-4
Peltola, M. E., Leitinger, M., Halford, J. J., Vinayan, K. P., Kobayashi, K., Pressler, R. M., Mindruta, I., Mayor, L. C., Lauronen, L., & Beniczky, S. (2023). Routine and sleep EEG: Minimum recording standards of the International Federation of Clinical Neurophysiology and the International League Against Epilepsy. Epilepsia, 64(3), 602–618. https://doi.org/10.1111/epi.17448
Perle, J. G., Smith, K. L., & Pennington, M. L. (2025). A compendium for the 2024 APA Guidelines for the Practice of Telepsychology: Guideline applications and resources. American Psychologist. https://doi.org/10.1037/amp0001579
Refolo, P., Sacchini, D., De Nardo, F., & Sanches, M. (2022). Ethics of digital therapeutics (DTx). European Journal of Public Health, 32(Supplement_3), ckac130.217. https://doi.org/10.1093/eurpub/ckac130.217
Regulations for the protection of human research subjects (45 CFR46 and 56 FR 28003) (Federal Regulations).
Ros, T., Enriquez-Geppert, S., Zotev, V., Young, K. D., Wood, G., Whitfield-Gabrieli, S., Wan, F., Vuilleumier, P., Vialatte, F., Van De Ville, D., Todder, D., Surmeli, T., Sulzer, J. S., Strehl, U., Sterman, M. B., Steiner, N. J., Sorger, B., Soekadar, S. R., Sitaram, R., … Thibault, R. T. (2020). Consensus on the reporting and experimental design of clinical and cognitive-behavioural neurofeedback studies (CRED-nf checklist). Brain, 143(6), 1674–1685. https://doi.org/10.1093/brain/awaa009
Schwartz, M. S., & Andrasik, F. (Eds.). (2017). Biofeedback: A practitioner's guide (4th ed.). The Guilford Press.
Shaffer, F., Crawford, J., & Moss, D. (2012). What is BCIA really? Biofeedback, 40(4), 133–136.
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 258. https://doi.org/10.3389/fpubh.2017.00258
Shaffer, F., & Schwartz, M. S. (2016). Entering the field and assuring competence. In M. S. Schwartz & F. Andrasik, Biofeedback: A practitioner's guide (4th ed.). The Guildford Press.
Shen, W.-K., Sheldon, R. S., Benditt, D. G., Cohen, M. I., Forman, D. E., Goldberger, Z. D., Grubb, B. P., Hamdan, M. H., Krahn, A. D., Link, M. S., Olshansky, B., Raj, S. R., Sandhu, R. K., Sorajja, D., Sun, B. C., & Yancy, C. W. (2017). 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation, 136(5), e60–e122. https://doi.org/10.1161/CIR.0000000000000499
Sherlin, L. H., Arns, M., Lubar, J., Heinrich, H., Kerson, C., Strehl, U., & Sterman, M. B. (2011). Neurofeedback and basic learning theory: Implications for research and practice. Journal of Neurotherapy, 15(4), 292–304. https://doi.org/10.1080/10874208.2011.623089
Striefel, S. (1999). Practice guidelines and standards in psychophysiological self-regulation. Wheat Ridge, Colorado: Association for Applied Psychophysiology and Biofeedback.
Striefel, S. (2003). Professional ethics and practice standards in mind-body medicine. In D. Moss, A. McGrady, T. Davies, & I. Wickramasekera (Eds.), Handbook of mind-body medicine for primary care. Sage Publications, Inc.
Striefel, S. (2004). Practice guidelines and standards for providers of biofeedback and applied psychophysiological services. Association for Applied Psychophysiology and Biofeedback.
Substance Abuse and Mental Health Services Administration. (2024). SAFE-T suicide assessment five-step evaluation and triage (Publication No. PEP24-01-036). https://library.samhsa.gov/product/safe-t-suicide-assessment-five-step-evaluation-and-triage/pep24-01-036
Sullivan, L. R., & Altman, C. L. (2008). Infection control: 2008 review and update for electroneurodiagnostic technologists. American Journal of Electroneurodiagnostic Technology, 48, 140–165. PMID: 18998475
Swatzyna, R. J., & Peavey, B. (2026, April 24). Unmasking the underlying cause: An ethical framework for mental health diagnosis [Conference presentation]. Biofeedback Society of Texas.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Topol, E. J. (2019). High-performance medicine: The convergence of human and artificial intelligence. Nature Medicine, 25(1), 44–56. https://doi.org/10.1038/s41591-018-0300-7
Tully, L., Boverman, J., & others. (2020). Cybersecurity considerations for telehealth and connected care. Journal of Medical Internet Research. https://doi.org/10.2196/18230
U.S. Department of Health and Human Services. (n.d.). HIPAA Security Rule guidance material.
U.S. Food and Drug Administration, Health Canada, & Medicines and Healthcare products Regulatory Agency. (2024). Transparency for machine learning-enabled medical devices: Guiding principles.
Washington State Legislature. (2023). My Health My Data Act (Chapter 19.373 RCW).
World Health Organization. (2021). Ethics and governance of artificial intelligence for health.
Yang, Y.-Y., Hwang, A. H.-C., Wu, C.-T., & Huang, T.-R. (2022). Person-identifying brainprints are stably embedded in EEG mindprints. Scientific Reports, 12, Article 17031. https://doi.org/10.1038/s41598-022-21384-0
Return to Top