Alpha-Theta Training
What You Will Learn in This Chapter
Alpha-theta (A-T) training stands as one of the earliest neurofeedback protocols ever developed—and one of the most enduring. This chapter traces its evolution from pioneering alpha biofeedback experiments to the refined clinical protocols in use today. You will explore the underlying neurophysiology, the key research milestones, and the practical details that make this approach relevant across clinical and performance settings.
Along the way, you will encounter the theory of oscillatory timing and cross-frequency synchronization, the foundational contributions of researchers like Kamiya, Peniston, and the Greens, and how decades of refinement have shaped current practice. You will also see how quantitative EEG findings can guide the design of an individualized training plan, illustrated through a detailed trauma case study. A demonstration of an A-T training session and supporting graphics will help bring these concepts to life.
This unit covers Underlying Theory, Cross-Frequency Synchronization, Local Field Potential, Global and Local Synchronization, History and Development, Benefits of A-T Training, Comparison of Interventions, A-T Training Protocols, Expected Results, Applications, Trauma and A-T Training, Cautions, and Final Thoughts.
BCIA Blueprint Coverage: This unit addresses VIII. Treatment Implementation - D. Introduction to Alpha-Theta Training.
Learning Objectives
After completing this section, you will be able to:
Describe the underlying theory of oscillatory timing and cross-frequency synchronization in A-T training.
Explain the historical development of A-T training from Kamiya's alpha research through the Peniston Protocol and subsequent refinements.
Compare different A-T training protocol approaches, including dual-tone, ratio-based, and targeted 6-9 Hz methods.
Identify clinical applications, expected results, and cautions associated with A-T training.
Explain how qEEG findings can guide protocol selection and the sequencing of interventions when A-T training is used with trauma clients.
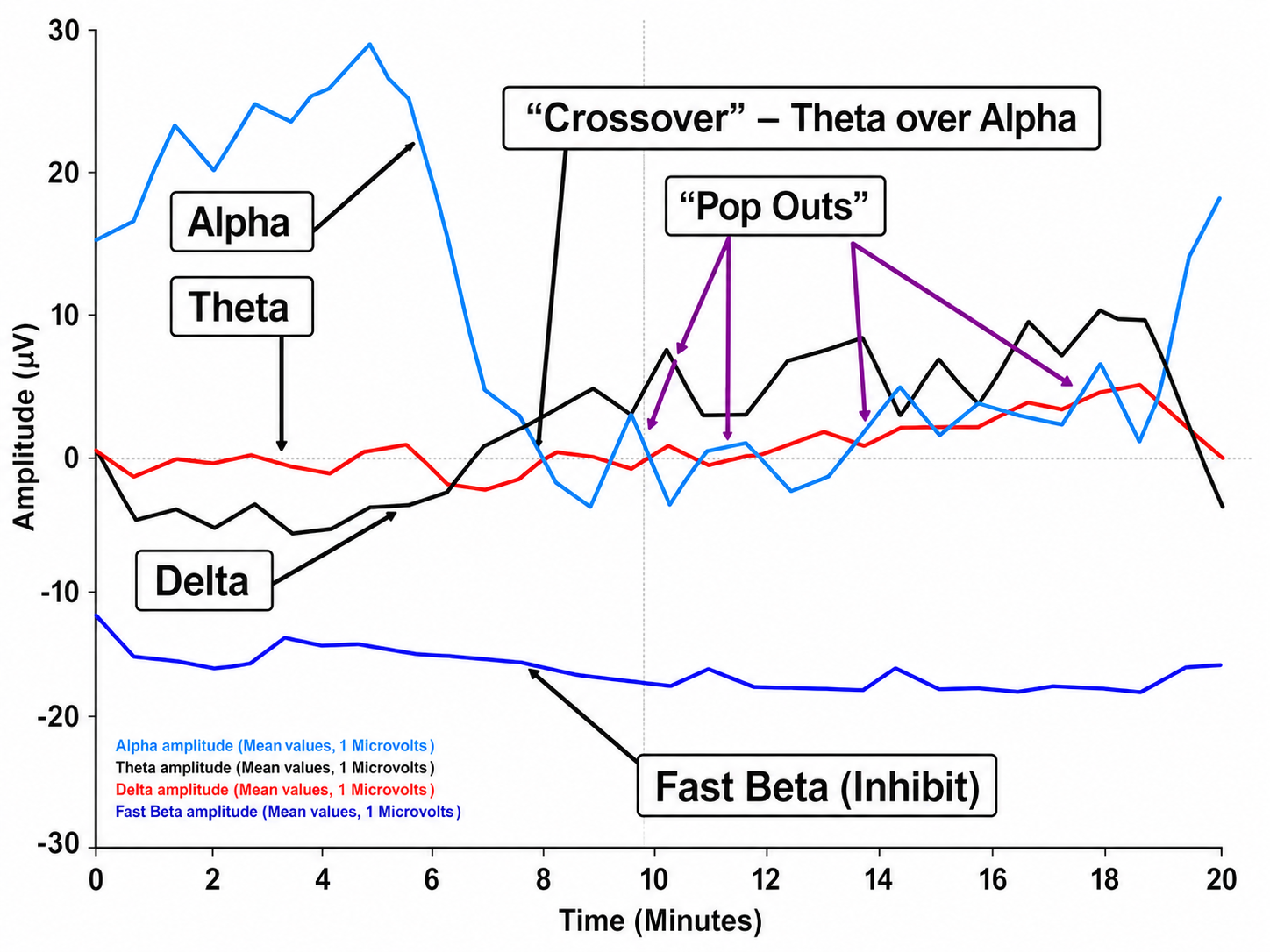
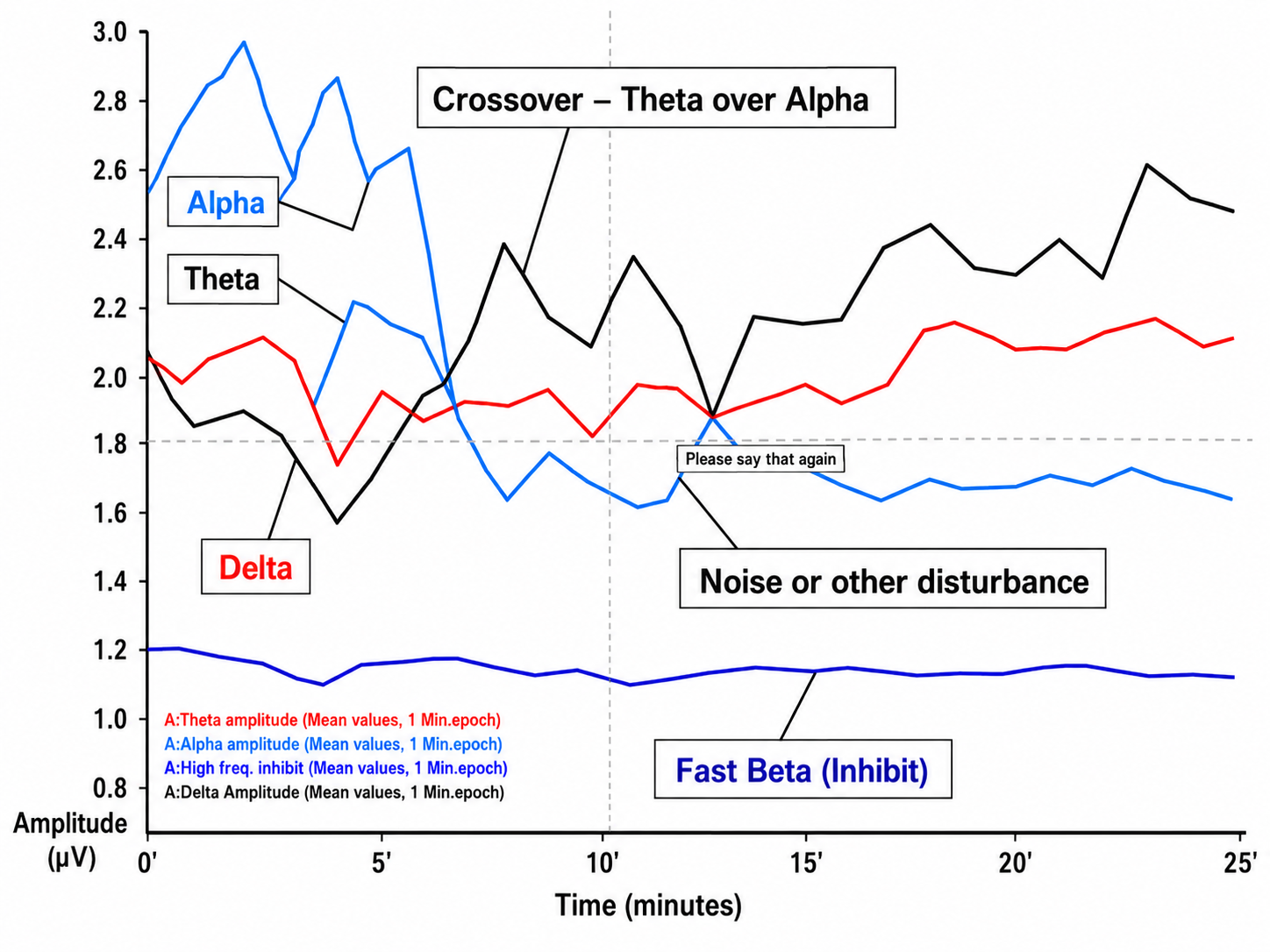
Interpret A-T training session data, including crossover events and inhibit feedback indicators.

Underlying Theory: Timing is Everything
This section introduces the neurophysiological foundation of A-T training, beginning with how the brain uses oscillatory timing to organize information and moving through cross-frequency synchronization, local field potentials, and the distinction between global and local synchronization. Understanding these mechanisms will clarify why A-T training targets specific frequency bands and how changes in brain rhythms translate into clinical outcomes.
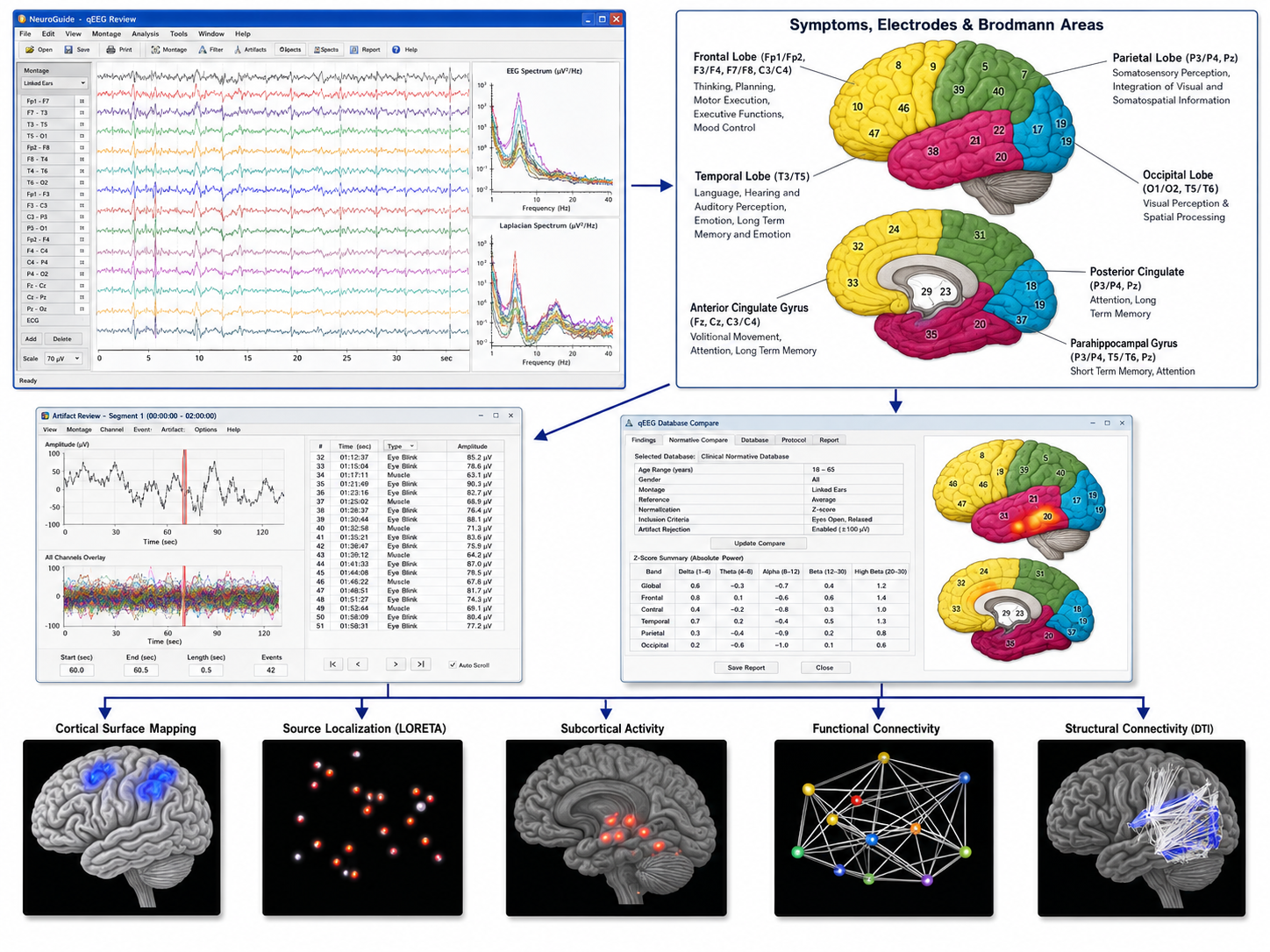
Oscillatory timing—the rhythmic, coordinated activity of neuronal populations at specific frequencies—is the brain's fundamental method for organizing information. According to Buzsáki (2006), brain activity consists of multiple nested rhythms that emerge from the coordinated activity of small-world networks, interconnected groups of neurons that communicate through hubs and nodes. Think of it like an orchestra: individual instruments (neurons) play their own parts, but the resulting music depends on how well those parts synchronize with one another. NeuroGuide™ graphic courtesy of Applied Neuroscience.
Cross-Frequency Synchronization
This section examines how slower brain rhythms scaffold faster ones, how the alpha response and alpha blocking work, and why these dynamics matter for A-T training. These concepts are essential for understanding how the crossover state—the central goal of A-T training—emerges from coordinated shifts in brain rhythm activity.
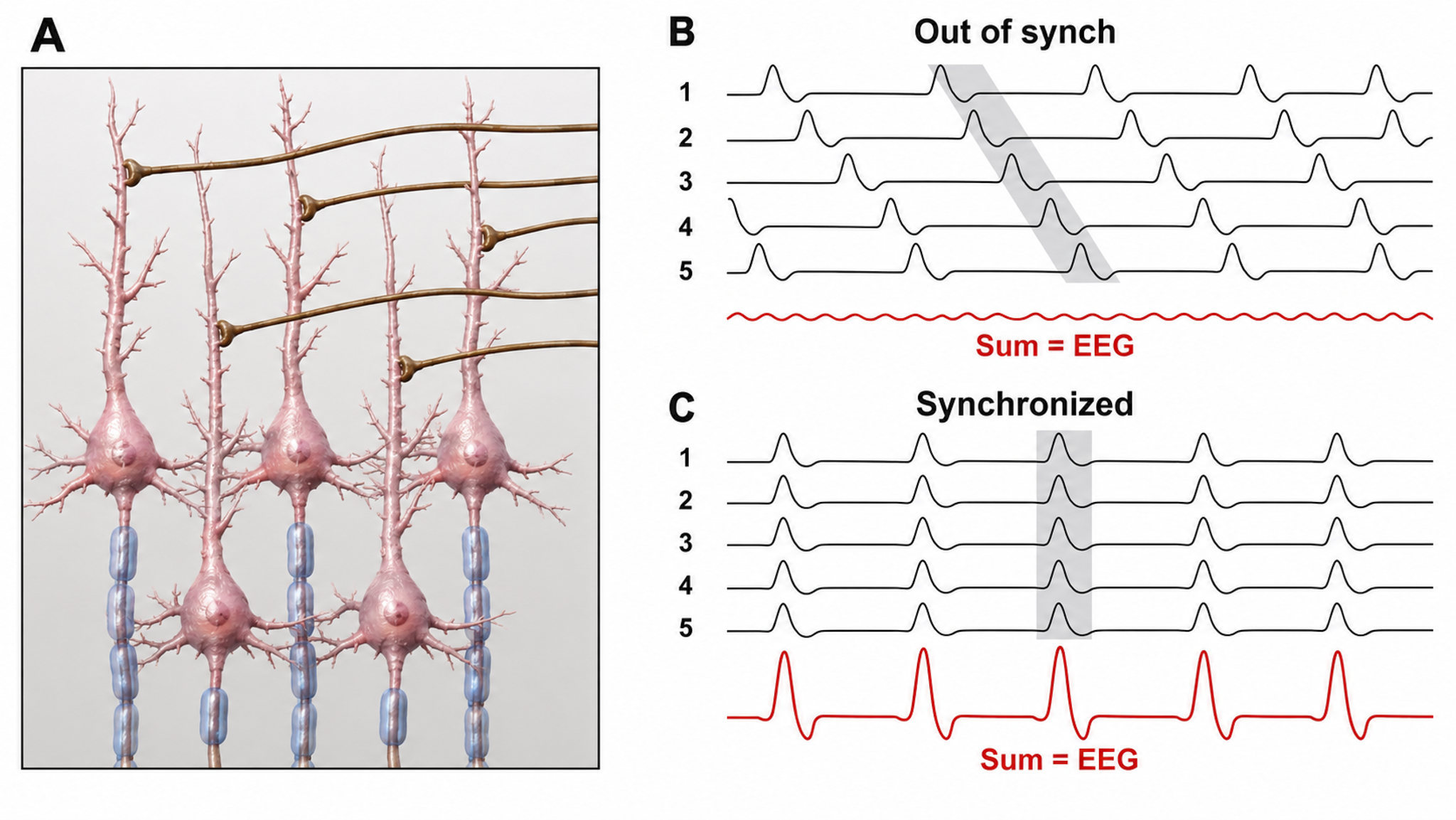
Slower brain frequencies act as an organizing framework within which faster frequencies can operate in a coordinated manner. Gunkelman (2005) described how faster frequencies emerge from bound networks—groups of neurons whose slower rhythmic activity has become synchronized. As these networks lock into step, the neuronal activity they generate gives rise to higher-frequency oscillations. At the scalp, EEG frequencies reflect the synchronized postsynaptic potentials of large populations of similarly oriented neurons: the more of those potentials that rise and fall together at a given frequency, the higher the recorded voltage (amplitude). Amplitude indexes synchrony and dendritic alignment, not firing rate.
A clear example of this process is the alpha response. When the eyes are open, millions of visual processing neurons are busy responding to sensory input relayed by the thalamocortical relay (TCR) system—the ascending pathway from the thalamus, gated by the reticular nucleus of the thalamus (nRt). When the eyes close and visual input ceases, these same neurons begin responding to a rhythmic signal generated by interactions between the thalamus and the nRt (Cox et al., 1997), modulated by ascending neurochemical input from the brainstem and reticular activating system. This rhythmic signal, first described by Berger (1929), is the alpha rhythm, also known as the posterior dominant rhythm (PDR). As the postsynaptic potentials of these visual neurons come into synchrony with this thalamic rhythm, alpha amplitude increases—the alpha response.
The reverse happens when the eyes reopen. Visual neurons resume processing incoming sensory information relayed by the TCR system, and fewer neurons respond to the rhythmic PDR input. The result is a decrease in scalp-recorded alpha amplitude, a phenomenon known as alpha blocking. The total number of active neurons may remain similar, but because they now work more independently on separate tasks, the overall voltage of the EEG decreases. Reduced synchrony of postsynaptic potentials means reduced amplitude—a principle that is central to understanding EEG measurement in biofeedback practice.
Local Field Potential (LFP)
The local field potential (LFP) and the scalp EEG it contributes to are generated by the sum of postsynaptic potentials from synchronized neuronal excitation. In practical terms, the LFP reflects input into neurons rather than their output, and greater synchrony among those postsynaptic potentials produces larger potentials detectable at the scalp surface. This is why EEG-based biofeedback can meaningfully track brain state changes: when large groups of neurons synchronize, the signal becomes robust enough to measure through the skull.
Global and Local Synchronization
Everyday waking activity relies on relatively weak, local interactions among small cortical neuronal groups, organized by slower rhythmic patterns. In contrast, global synchronization—the widespread coordination of neuronal activity across brain regions—generally occurs during resting states and various stages of sleep. It is during global synchronization that the brain integrates and consolidates experiences, memories, and skills.
A-T training may facilitate improved global synchronization within a semi-waking state, bridging the gap between full wakefulness and sleep. On this account, that positioning is what would allow clients to remain conscious while accessing integrative processes usually associated with deeper resting states—a proposed distinction from simple relaxation techniques that has not been tested directly.
Oscillatory timing organizes neuronal information through nested rhythms, with slower frequencies providing a scaffold for faster, coordinated activity. The alpha response occurs when visual neurons synchronize to thalamic input with eyes closed, while alpha blocking occurs when eyes open and neurons resume independent processing. Local field potentials reflect the sum of synchronized postsynaptic activity—the basis for all scalp EEG measurement. A-T training leverages the distinction between local and global synchronization, facilitating widespread neural coordination within a semi-waking state that supports integration and consolidation.
History and Development
This section traces the evolution of A-T training from its origins in alpha biofeedback research through the development of the Peniston Protocol and the contributions of subsequent researchers. Understanding this history is important because each generation of investigators refined the technique, addressed limitations, and expanded the evidence base—shaping the protocols you may use in clinical practice today.
The story of A-T training begins with Joe Kamiya, who demonstrated in the early 1960s that individuals could learn to control their alpha activity when given adequate feedback about its state (Ancoli & Kamiya, 1978; Kamiya, 1961, 1962, 1968, 1969). This was a landmark finding: it established that a brain rhythm previously considered involuntary could be brought under conscious influence through operant conditioning. Kamiya later collaborated with James Hardt on an anxiety study whose design is often misreported (Hardt & Kamiya, 1978). Participants high or low in trait anxiety were trained both to increase and to decrease alpha. Anxiety tracked alpha only in the high-anxiety participants, falling as alpha rose and rising as alpha was suppressed. The pair also argued that alpha changes are not merely an oculomotor artifact (Hardt & Kamiya, 1976).

Menninger Foundation
In 1967, Elmer and Alyce Green of the Menninger Foundation launched the Voluntary Controls program, building on the psychophysiology laboratory Elmer Green had established there in 1964; the work continued for several decades. These projects studied meditators, healers, and ordinary individuals to identify the physiological signatures of voluntary control over internal states. Together with Dale Walters and other staff, the Greens trained many individuals—including clinicians—to regulate peripheral skin temperature, electrodermal response, and EEG activity across the theta, alpha, and beta frequency bands.
One of the clinicians who attended this training was Eugene Peniston, a psychologist from Colorado. Peniston would go on to publish seminal work applying A-T training to substance use disorder treatment. Drawing on the Greens' approach, Peniston (Peniston & Kulkosky, 1989, 1990) developed a protocol he used with individuals in the alcohol treatment program at the Fort Lyon Veterans Administration Medical Center. During each training session, he provided feedback through two separate audio tones—one representing theta amplitude and the other representing alpha amplitude.
The goal was to initially increase alpha activity and then allow alpha to decrease as theta activity rose, guiding the participant into what is called the crossover state—a slightly disconnected reverie in which external sensory input is minimized and an internal, relaxed state is promoted. Peniston also combined his protocol with hypnotic inductions, suggestions, and post-session processing to facilitate changes in attitudes and beliefs regarding alcohol consumption. His reported results were striking: with 10 alcoholic patients per group (plus 10 nonalcoholic controls), 8 of the 10 trained patients were still in remission at 13-month follow-up, compared with 2 of the 10 traditionally treated controls. Three cautions belong with that figure. The remission criterion was not strict abstinence but no drinking for more than six consecutive days, and the assignment method is not stated in the published report. Graap and Freides (1998) also questioned whether the five Peniston papers describe independent samples, what the participants' pretreatment status was, and which treatment components they received; Peniston (1998) replied, acknowledging some errors. Sokhadze, Cannon, and Trudeau (2008) rated the protocol Level 3, probably efficacious, noting that A-T feedback has not been shown superior to sham.
Other researchers and clinicians were also instrumental in developing this training approach. Barbara Brown (Brown, 1974) and Elmer and Alyce Green (Green & Green, 1977) contributed foundational work that facilitated Peniston's development of his intervention. Subsequently, Tom Budzynski, Lester Fehmi, and Martin Wuttke pursued independent investigations into training within this state of relaxed, introspective consciousness (Budzynski, 1976).





William Scott, David Kaiser, Siegfried Othmer, and Stephen Sideroff (2005) published a study in the American Journal of Drug and Alcohol Abuse that advanced the evidence for A-T training with substance use disorders. They randomly assigned 121 individuals in an inpatient polysubstance abuse program to an active training group or a control group. The active group first received beta and sensorimotor rhythm (SMR) training to address attentional variables—continued until the client's Test of Variables of Attention scores reached the normal range, rather than for a fixed number of sessions—followed by 30 sessions of A-T training. The results were notable: individuals in the treatment group remained in treatment longer, and 36 of the 47 experimental completers (77%) were abstinent at 12 months compared with 12 of the 27 control completers (44%). Those denominators matter: attrition differed sharply (15% versus 44%), and because the training itself improved retention, the abstinence and retention effects are entangled. The study also documented improvements on MMPI subscales and in attention, focus, and day-to-day functioning.


Burkett and colleagues (Burkett et al., 2005) published an open clinical trial in the Journal of Neurotherapy on neurofeedback training for crack cocaine dependence in men in a residential faith-based program. Their findings pointed the same way, with the important qualification that this was an uncontrolled open trial: among the 87 men reassessed twelve months after the EEG portion of the program, the reported gains in retention, abstinence, and depression are within-participant pre-post changes, not a demonstration of superiority over any comparison condition. Subsequently, various clinicians and practice groups have conducted single-case studies and small-N intervention studies with similar results. Neurofeedback for PTSD continues to be actively investigated (Nicholson et al., 2018; Nicholson, Ros, Densmore, et al., 2020), although those trials use protocols other than A-T training, and A-T training itself is being applied to optimal performance (Gruzelier et al., 2014); both lines of work are discussed later in this unit.
A-T training evolved from Kamiya's pioneering alpha biofeedback research through the Menninger Foundation's Voluntary Controls projects to Peniston's seminal protocol for treating alcoholism at the VA. Researchers including Brown, the Greens, Budzynski, Fehmi, Wuttke, Scott, Kaiser, and Burkett each contributed to developing and validating this approach. Across studies, A-T training has been associated with improved abstinence rates and better psychological outcomes for substance use disorders—a record that motivated its expansion into PTSD and performance applications, though reviewers have rated the evidence probably efficacious rather than efficacious, largely because the protocols were reported too sparsely to replicate and have not been tested against sham (Sokhadze et al., 2008).
Benefits of A-T Training
This section covers the reported benefits of A-T training and then examines a landmark comparison study that helps clarify which elements of treatment drive change. For practitioners, these findings highlight the importance of treatment context—particularly the therapeutic relationship—while identifying A-T training's specific contribution to client outcomes.
Research participants have described their A-T training experiences as "transformative." Commonly reported benefits include spiritual and religious imagery, recall of significant memories, insight into personal behavior patterns, and shifts in interpersonal relationships. Participants also report a renewed sense of purpose, resolution of longstanding anxiety and depression, release of trauma-related reactivity, improved self-esteem, and sustained abstinence from substance and behavioral addictions. These are participant self-reports from open trials and case series rather than from blinded comparisons, and none of the studies cited here separates the crossover state from the hypnotic suggestion, therapeutic relationship, and post-session processing delivered alongside it. They suggest that the state facilitates access to psychological material that may be difficult to reach through conventional talk therapy alone.
Comparison of Interventions
Patricia Norris, Steven Fahrion, and others left the Menninger Foundation in the early 1990s to form the Life Sciences Institute of Mind-Body Health in Topeka, Kansas. They conducted a 5-year study of A-T training in a prison population (described in Norris, 2017) that offers valuable insight into how A-T training fits within a broader treatment framework.
Both groups in the study received a comprehensive program of self-regulation, educational, and supportive components: temperature training, breath training, didactic presentations on philosophy, psychodynamic aspects of self, and psychosynthesis exercises. Importantly, all participants were treated with "deference, respect, and compassion." One group additionally received 45 daily sessions of A-T neurofeedback training. The 2-year follow-up results (N = 35) were encouraging compared to standard substance use disorder (SUD) treatment in prison settings, where "survival" rates—defined as abstinence with no violations or criminal activity—are reported to be far lower.
At one year, 78% of the A-T group survived compared with 75% of controls; at two years, 69% versus 64%. When analyzed by subgroup, however, meaningful differences emerged. Younger participants showed a more pronounced benefit from A-T training: 74% versus 54% at one year, and 60% versus 45% at two years. African-American and Hispanic participants showed a similar pattern: 70% versus 48% at one year, and 48% versus 40% at two years. These subgroup differences suggest that age and ethnicity functioned as moderator variables, and that A-T training was a more critical component for certain populations. Read them as exploratory: they come from a small follow-up sample divided several ways. The same directional pattern does appear in Fahrion's larger completed prison study, which found little overall difference at two years but greater benefit for younger and non-white participants (Sokhadze et al., 2008).
What Was the Mechanism of Change?
This study reveals an important insight for practitioners: the overall treatment program was remarkably effective compared to standard interventions, and the difference between A-T and control groups was not statistically significant when the groups were viewed as a whole. The program's design—combining self-regulation skills, education, and a genuinely respectful therapeutic environment—was likely the most crucial factor. A-T training appears to have functioned as one effective component within that broader effort, with particular value for younger and minority participants.
As discussed in the Therapeutic Relationships section of Neurofeedback Tutor, the relationship between clinician and client is one of the most important factors in any intervention. This is especially true for A-T training, because the crossover state requires complete trust on the client's part. Clients must be willing to lower emotional, psychological, and physical defenses so they can disconnect from external sensory input and allow the reverie state to emerge. Clinicians must cultivate this trusting relationship before implementing A-T training.
This is one reason many practitioners use a variety of preparatory and concurrent interventions alongside A-T training. These may include breathing and heart rate variability (HRV) training, guided relaxation, peripheral temperature training, EMG biofeedback, electrodermal biofeedback, SMR and beta neurofeedback protocols, z-score-based neurofeedback, hypnotic inductions, behavior change scripts, and post-session psychotherapy and processing.
What Role Does A-T Training Play in the Changes Experienced by Clients?
A client's ability to enter the desired reverie state depends on many factors, including set and setting, expectations, clinician self-training, and interpersonal skills. Multiple interventions—mindfulness meditation, HRV training, A-T training, other forms of neurofeedback, hypnosis, and psychotherapy—can all facilitate access to states that promote change. What these approaches share is a common challenge: without real-time feedback, it is difficult for the client to know whether they are in the desired state, approaching it, or far from it.
This is where A-T neurofeedback offers a distinct advantage. When implemented correctly, it provides continuous information about the client's position on the continuum between alert wakefulness and the crossover state. Practitioners hold that this real-time guidance allows the client to move toward and sustain the desired state more quickly, accelerating skill acquisition in a way that interventions without moment-to-moment feedback cannot easily match; that comparison has not been made in a published controlled trial.
Participants consistently report transformative experiences during A-T training, including insight, emotional resolution, and sustained behavior change. The Life Sciences Institute prison study demonstrated that comprehensive treatment programs—incorporating self-regulation, education, and genuine respect—are highly effective, with A-T training contributing particularly for younger and minority participants. The therapeutic relationship is essential for A-T success because the crossover state requires the client to lower their defenses. A-T training's unique clinical advantage lies in providing continuous, real-time feedback about the client's proximity to the desired state.
A-T Training Protocols
This section covers the three main approaches to A-T training protocols: Peniston's original dual-tone method, the simplified ratio-based approach, and the targeted 6-9 Hz protocol. You will also learn about reward and inhibit feedback mechanisms and see how a sample training session unfolds. Understanding the strengths and limitations of each approach will help you select and implement the protocol best suited to your clients and clinical setting.
The original protocol developed by Eugene Peniston (Peniston & Kulkosky, 1989, 1990) used two separate audio tones—one representing alpha amplitude and the other representing theta amplitude. As alpha amplitude increased, its tone sounded more frequently; as theta amplitude increased, the theta tone became more prominent. This dual-tone design allowed the trainee to perceive the relative voltage of each frequency band and to practice strategies for increasing theta while decreasing alpha. The feedback guided the trainee toward the crossover state, where theta amplitude exceeds alpha amplitude.
Contemporary practitioners of the dual-tone method describe threshold settings intended to elicit this shift, beginning with settings that reward alpha 50-70% of the time and theta approximately 20-40% of the time. The published Peniston reports do not specify these percentages; they state only that alpha was rewarded more heavily than theta at the outset. As training progressed, the percentage of alpha reward was allowed to decrease as alpha amplitude dropped, while the theta reward tone was allowed to increase with rising theta amplitude. Even if theta voltage decreased, the instruction was to maintain the theta reward at approximately 40% to ensure a minimum level of positive reinforcement. Some practitioners, however, found this protocol difficult to administer correctly, and some clients became confused about which signal to follow.
In response to these difficulties, a simplified approach emerged that uses the theta-alpha ratio to provide a single feedback tone representing the crossover state. When theta amplitude exceeds alpha amplitude and surpasses a set threshold, the client hears a tone indicating they have reached the crossover state. This ratio-based protocol has been incorporated into several commercial neurofeedback platforms, including the Thought Technology BioGraph system and the Nexus/BioTrace+ system from Mind Media. However, this simplification comes with trade-offs: the broad frequency bands reduce specificity, an increase in slower theta components can trigger the reward without representing a true crossover state, and the client receives no information about how close they are to the goal. A single tone for the crossover leaves the client without the continuous, graded feedback that supports efficient learning.
Targeted Training: 6-9 Hz
Following extensive experimentation and clinical experience, John Anderson and others developed a protocol that targets the 6-9 Hz frequency band—in their clinical experience, the range in which the crossover state actually appears. This band straddles the theta (4-7 Hz) and alpha (8-12 Hz) ranges used throughout this curriculum, directly training the activity that defines the desired state. Band edges vary by author, so 6-9 Hz should be read as a filter setting, not as a claim about where theta ends and alpha begins. The protocol also incorporates an inhibit channel for 2-6 Hz activity, which is intended to keep the client from drifting into a deeper, more sleep-like state. Without this safeguard, excessive slow-wave activity during A-T training can trigger what clinicians call an abreaction—a negative reaction that may involve traumatic recall or depersonalization experiences.
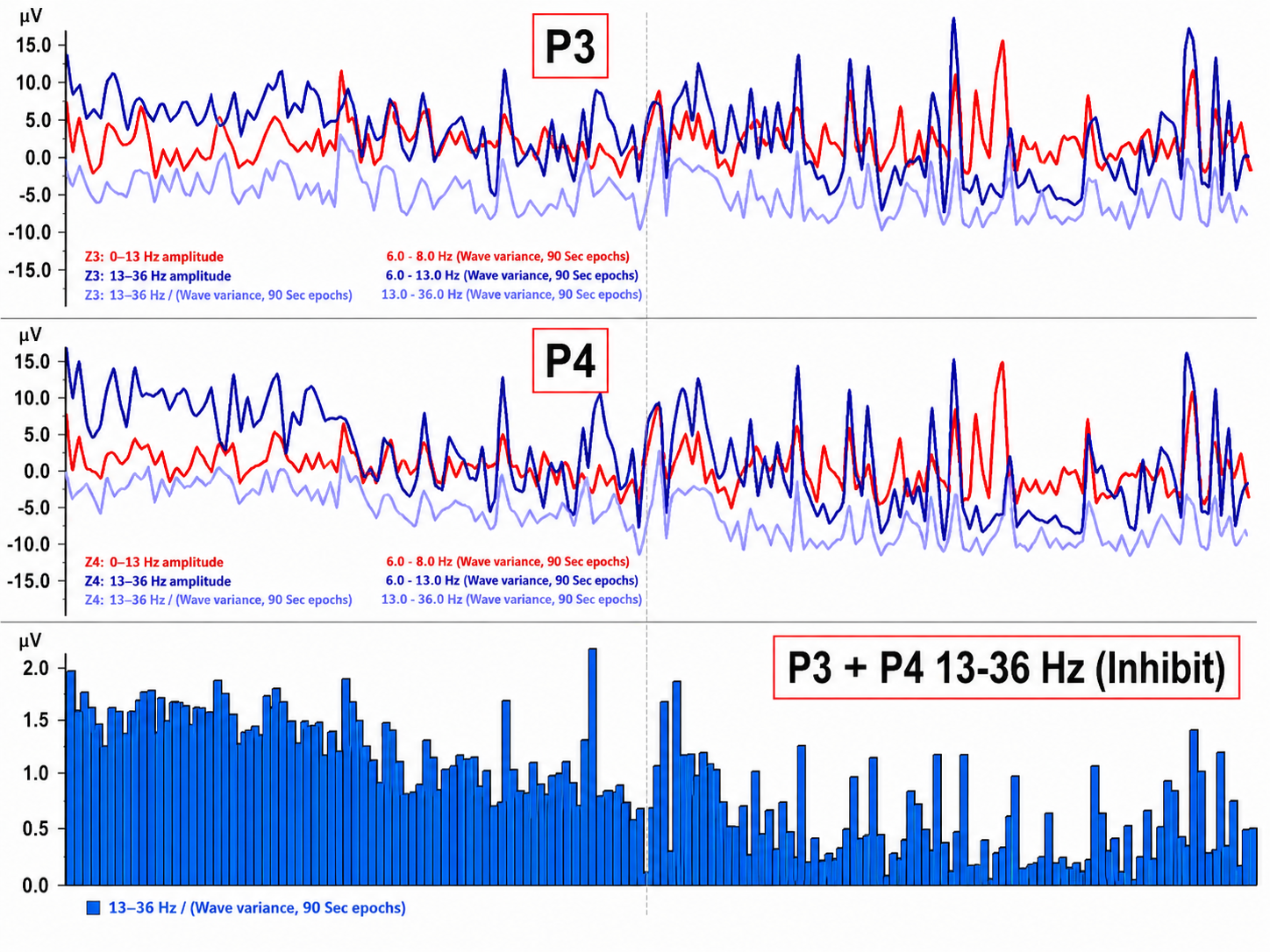
Practitioners using this protocol report that the 2-6 Hz inhibit prevents these negative reactions; that judgment rests on clinical experience rather than on controlled comparison. Additionally, a second inhibit band from approximately 13-36 Hz is used to limit increases in faster EEG frequencies associated with cognitive activity, keeping the client in the relaxed reverie state rather than shifting into active thinking and problem-solving. While this targeted approach is more complex to administer than the simple ratio method, its proponents hold that it is more likely to produce desirable outcomes while minimizing the risk of negative reactions or unproductive cognitive engagement. That case rests on clinical experience; the targeted protocol has not been compared with the dual-tone or ratio-based protocols in a published controlled trial.
Reward Feedback
Reward feedback in the targeted protocol is a proportional audio signal—typically music—that increases and decreases in volume in direct proportion to changes in 6-9 Hz amplitude. Clients select from calming, relaxing musical options. The continuous volume changes allow the client to know, moment by moment, where they are on the continuum from an alert eyes-closed state to the deep reverie of the crossover state. In effect, it works like the "hot and cold" game children play—a constant, intuitive stream of guidance.
Inhibit Feedback
The low-frequency inhibit (2-6 Hz) uses a recording of birds chirping that sounds only when the signal exceeds a set threshold, growing louder as slow-wave amplitude increases. This gently alerts the client when they are drifting toward sleep without startling them out of the reverie state. Most clients intuitively associate birds chirping with waking up in the morning, making it an easy-to-remember signal that feels natural rather than intrusive.
The high-frequency inhibit (13-36 Hz) uses a recording of ocean waves with an inverse proportional relationship to signal amplitude: it becomes louder as "busy brain" activity decreases, thereby rewarding reduced cognitive engagement. Together, the ocean waves and rewarding music blend to create a calming auditory environment that encourages the correct state while providing constant, meaningful feedback. This layered audio design—reward music for the target band, birds for excessive slow activity, and ocean waves for cognitive quieting—gives the client a rich, continuous stream of information without requiring conscious analysis.
A-T training protocols have evolved from Peniston's original dual-tone approach through a simplified ratio-based method to the targeted 6-9 Hz protocol developed by Anderson and colleagues. The targeted approach trains the actual crossover frequency band while using low-frequency (2-6 Hz) and high-frequency (13-36 Hz) inhibits intended to limit negative reactions and cognitive activation. Proportional audio reward feedback provides the client with continuous, intuitive information about their proximity to the desired state—a significant advantage over single-tone feedback designs.
Sample Training Session
Before beginning A-T training, practitioners typically employ preparatory interventions tailored to the client's needs. Peniston and Kulkosky (1989) began with a temperature biofeedback pretraining phase; the published abstract does not give its length, and secondary accounts describe roughly five to eight sessions to a criterion near 94-95°F. Scott et al. (2005) used beta and SMR training to stabilize the nervous system before continuing with A-T training. Other practitioners incorporate heart rate variability training, combinations of biofeedback modalities, or—in some optimal performance settings—proceed directly to A-T training as the primary or sole neurofeedback intervention.
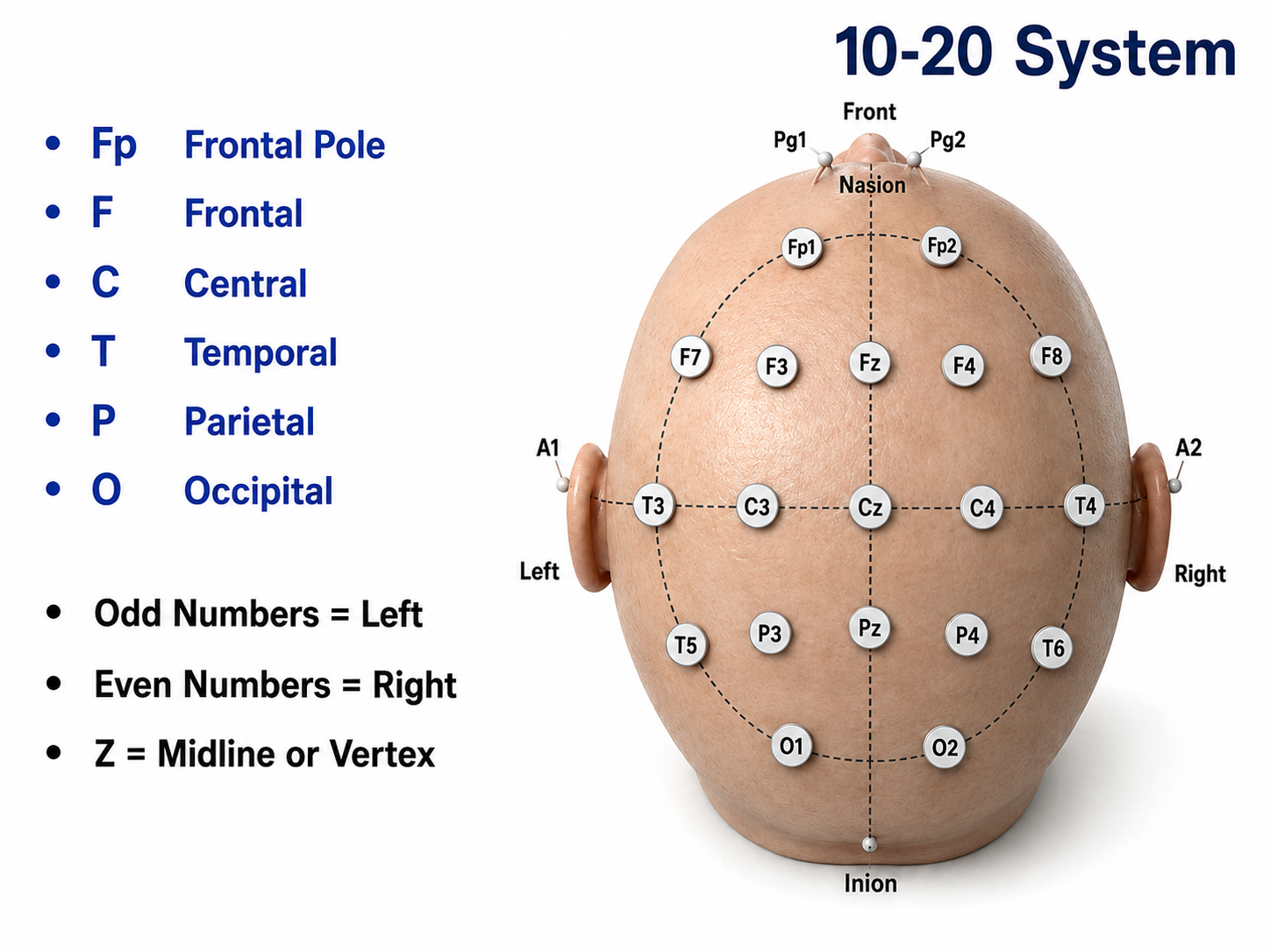
Training schedules also vary by setting and clientele. Peniston and Kulkosky's (1989) published trial used 15 thirty-minute A-T sessions; the widely quoted figure of 30 sessions belongs to Peniston's later PTSD work and to Scott et al. (2005), who used 30 A-T sessions in their Phase II. Other practitioners have used once- or twice-weekly sessions, and some intensive programs provide twice-daily training. Regarding electrode placement, Peniston and Kulkosky's (1989) initial approach used the O1 location of the International 10-20 electrode placement system. Subsequent practitioners have also used Pz, or the P3 and P4 locations for two-channel A-T training. Where a qEEG has been obtained, site selection may instead be individualized: Davis (2022) delivered A-T training at P4 with eyes closed after first down-training excess high beta at frontal sites, a sequence described in detail in the Trauma and A-T Training section. John Balven adapted the diagram below from Fisch (1999).
Peniston's approach included behavior change scripts read to the participant before each session, along with post-session debriefing conversations (personal communication, 1995). Other practitioners have adopted variations such as affirmations, ideal-behavior scenario instructions, tape-recorded relaxation practices, and post-session psychotherapy or processing. These adjunctive elements underscore the point made earlier: A-T training is most effective as part of a comprehensive approach that addresses the client's psychological readiness and therapeutic relationship.
The following images are generated by the Nexus neurofeedback system, showing initial and subsequent A-T training sessions that illustrate crossover events in both single-channel and two-channel configurations.
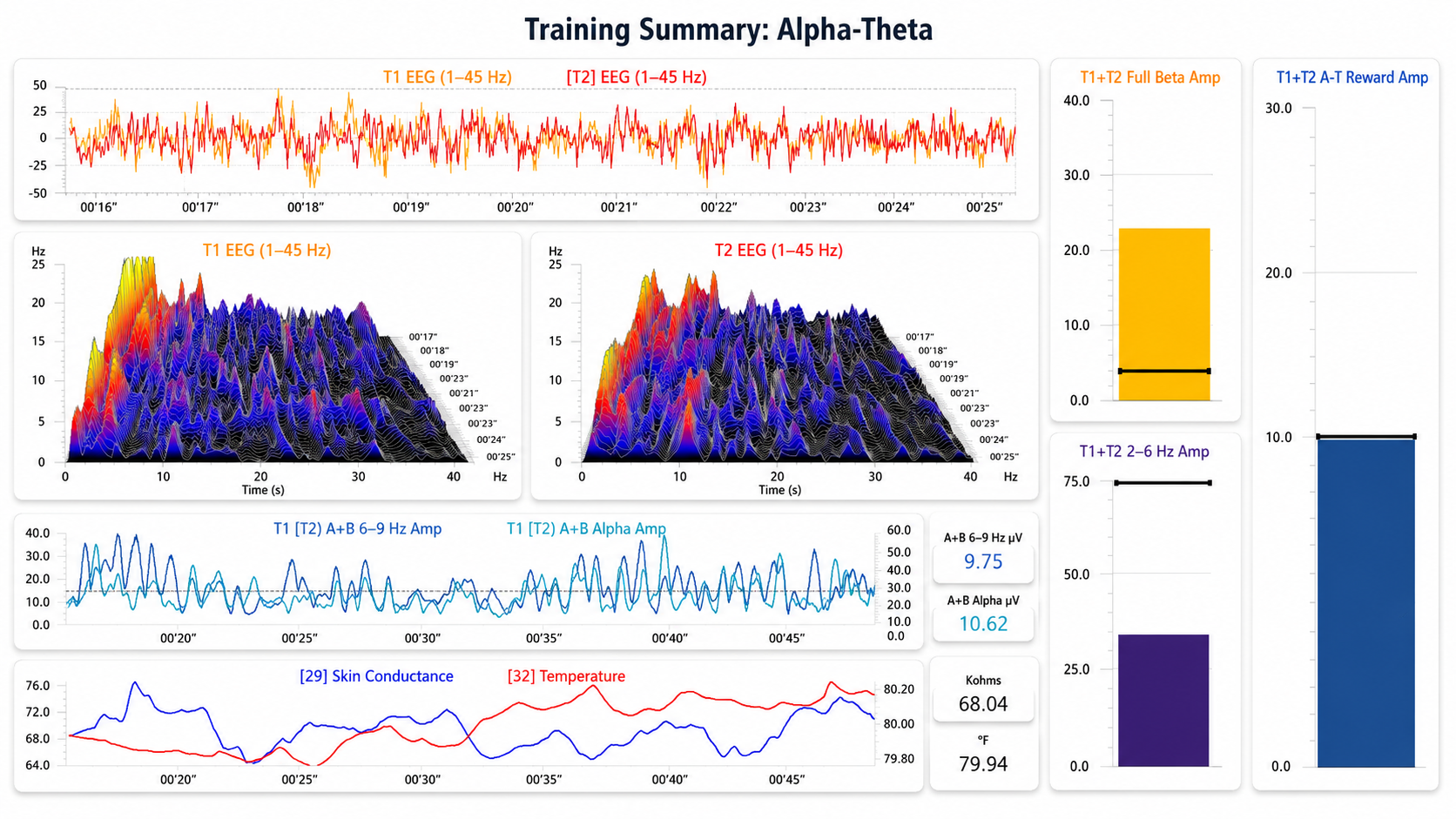
The image below shows the beginning of a 2-channel A-T training session. Note that the eyes-closed EEG shows no clear posterior rhythm (alpha) and that peripheral skin temperature is 79.94°F measured from the small finger of the non-dominant hand, indicating increased sympathetic nervous system (SNS) activity. The electrodermal channel is shown as resistance in Kohms, measured from the palm of the non-dominant hand, where higher values indicate decreased sweat gland activity. The current reading is 68.04 Kohms. Because resting electrodermal levels vary widely between individuals, it is the change across the session, not the absolute value, that indexes this client's shift in arousal. The sum of the P3 + P4 6-9 Hz activity is 9.75 µV, while 8-12 Hz alpha is 10.62 µV. Graphic © John S. Anderson.
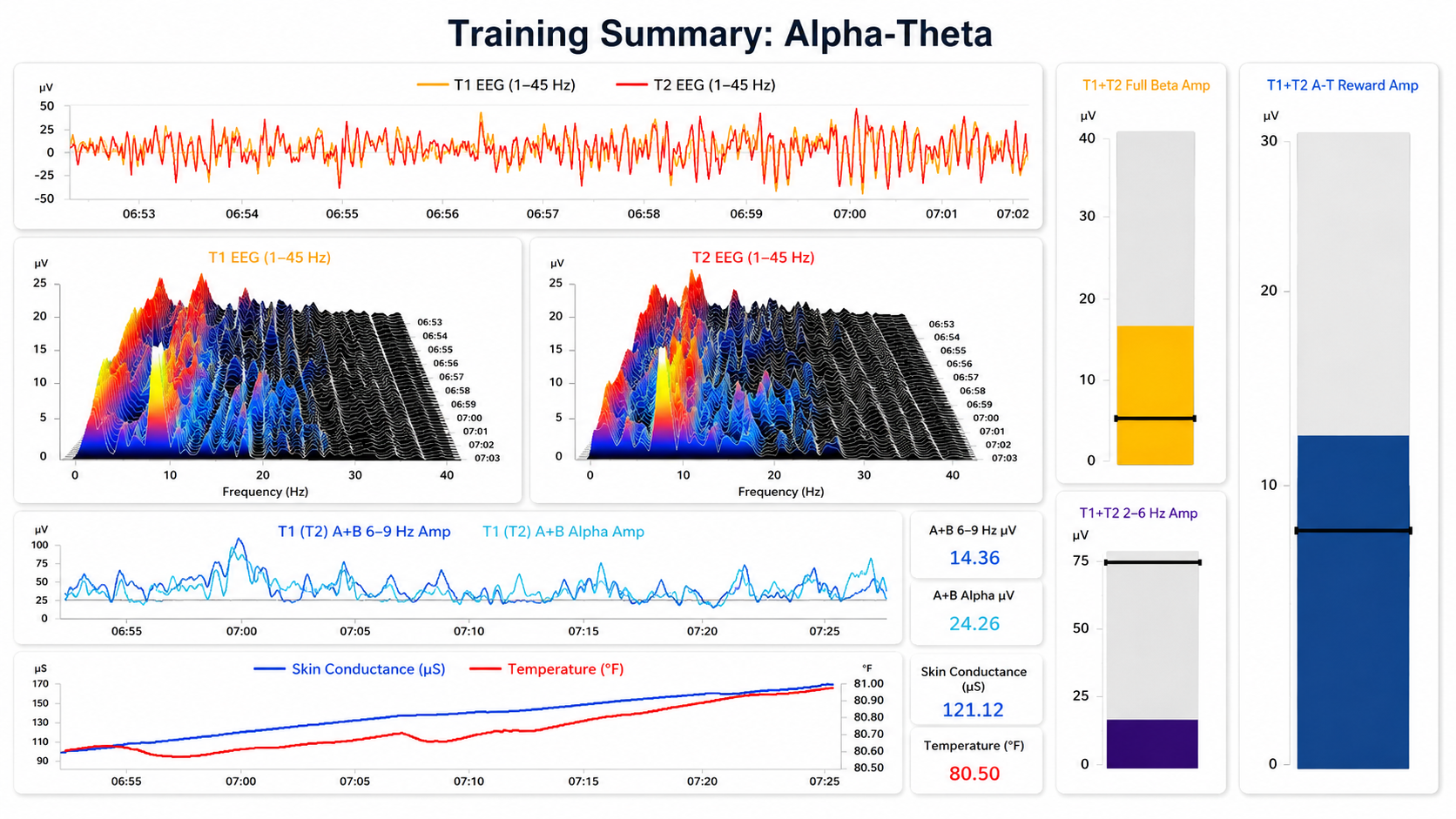
The image below shows the same session when the initial increase in alpha amplitude occurs. Peripheral skin temperature has increased to 80.50°F, and skin resistance has increased to 121.12 Kohms—both indicating decreased arousal. P3 + P4 6-9 Hz activity has increased to 14.36 µV, while 8-12 Hz alpha has increased to 24.26 µV. Note that alpha has risen more than the 6-9 Hz band at this point, so no crossover has yet occurred. Graphic © John S. Anderson.
The image below shows the same session near the end. Peripheral skin temperature has increased to 90.57°F, and skin resistance has increased to 289.54 Kohms—both reflecting continued decreased arousal. P3 + P4 6-9 Hz activity has increased to 48.12 µV, while 8-12 Hz alpha is at 27.50 µV. The 6-9 Hz activity now substantially exceeds alpha, confirming a sustained crossover state. Graphic © John S. Anderson.
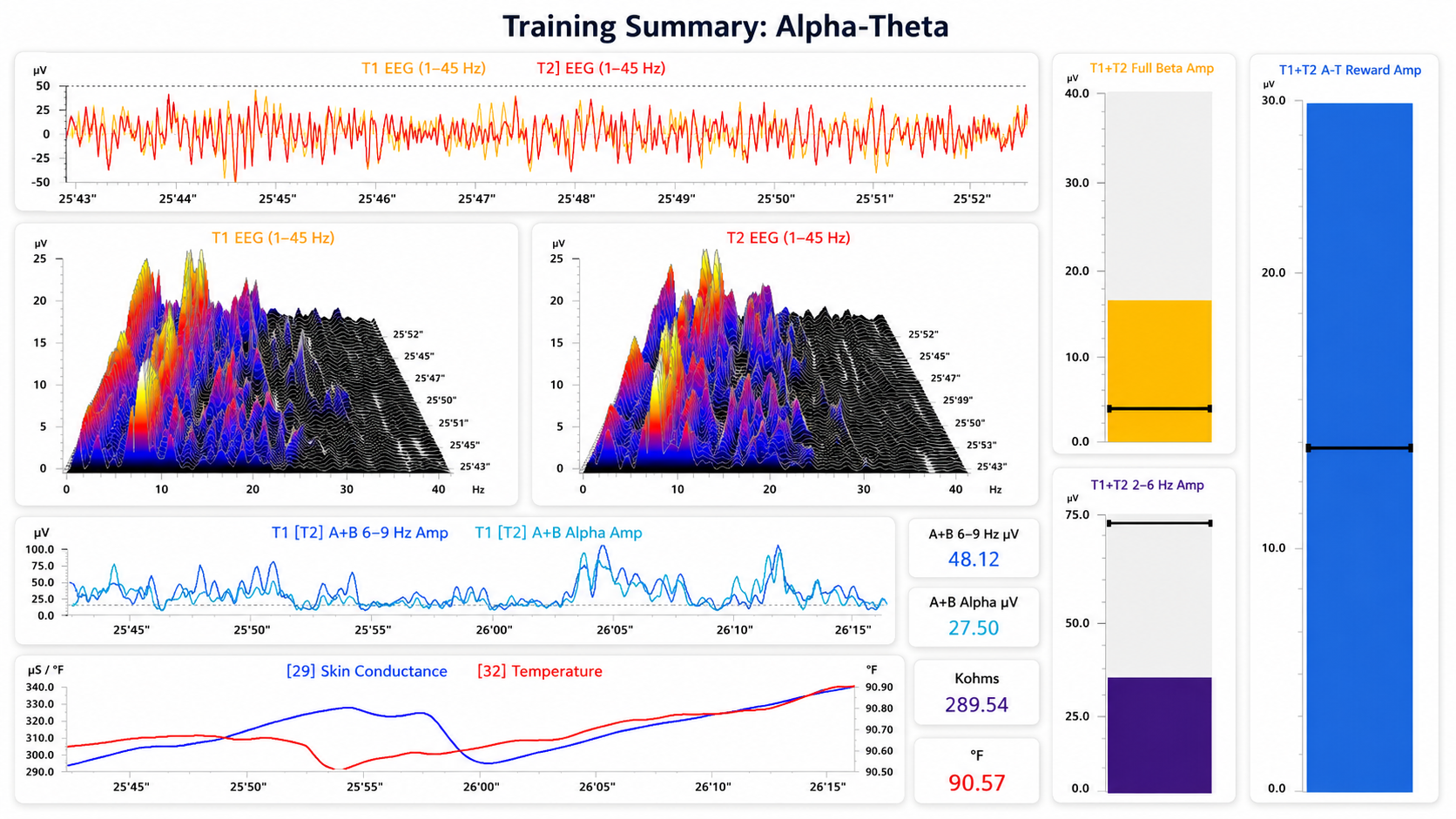
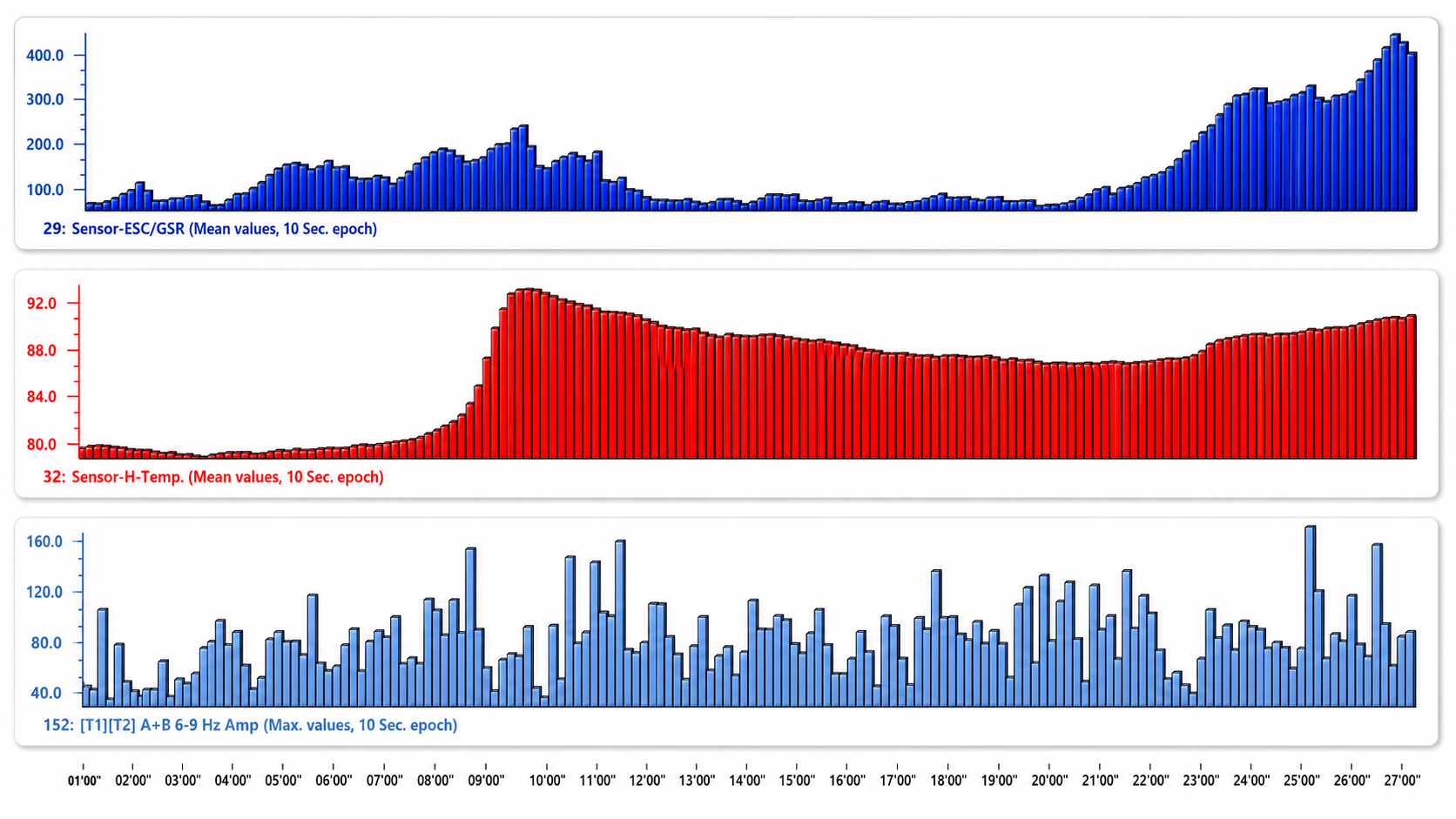
The final image is a summary screen plotting skin resistance (top), temperature (middle), and P3 + P4 6-9 Hz activity (bottom) across the session. Skin resistance and temperature both end higher than they began, consistent with a shift toward deeper relaxation, but neither rises steadily: both peak about ten minutes in, fall back through the middle of the session, and rise again near the end. The 6-9 Hz panel fluctuates without a clear trend. Graphic © John S. Anderson.
This video takes the viewer through an A-T training demonstration using the Nexus/Biotrace system (Mind Media, Roermond, The Netherlands) using the training approach developed by John Anderson. The demonstration uses saved session data to illustrate the functions and discuss the threshold settings and training concepts. The video begins with a black screen, and the visual portion does not begin until the 1-minute mark.
Expected Results
This section describes what clients and practitioners can expect from A-T training, including the subjective experiences reported by participants and the neurological states the training appears to engage. Understanding these expected outcomes will help you set appropriate expectations with clients and recognize signs of productive training.
The state encouraged by A-T training appears similar to what occurs during mindfulness meditation—what is sometimes called a witness state, in which the individual observes the flow of consciousness, memory, and internal thoughts without actively pursuing or analyzing them. The training operationalizes this experience through audio feedback that rewards remaining in the desired state and discourages shifts in either direction—toward deeper sleep or toward activated cognitive engagement. Individuals report increased receptiveness to suggestion, free association and streaming consciousness, symbolic or spiritual imagery, and experiences of emotional resolution and insight.
The theories underlying this approach suggest that the A-T crossover state produces brain activity similar to that seen in hypnotic induction and in the lightly sleeping states associated with memory consolidation. There is also evidence that this state may overlap with the default mode network (DMN), the best known of several resting-state networks. The DMN is a network of brain regions associated with what researchers term the self-referential state—a condition of self-awareness involving memory recall and non-directed cognition that appears strikingly similar to the experiences described by A-T training participants (Davey & Harrison, 2018). For clinicians, this connection is significant: it suggests that A-T training may engage the same neural circuits that support self-reflection, emotional processing, and memory integration.
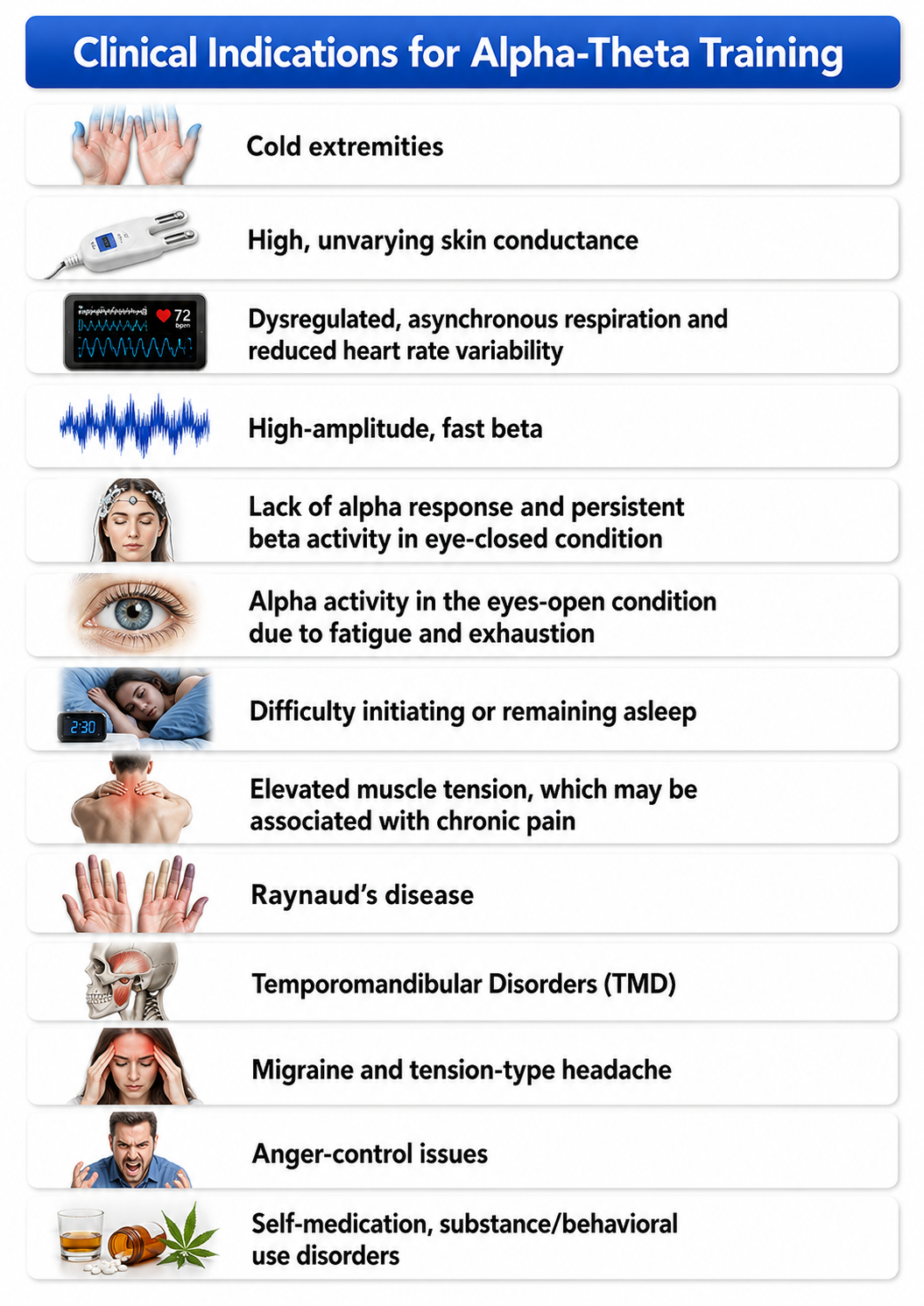
The technical aspects of this training are specific to each training platform, and practitioners will need to familiarize themselves with their system's particular software and hardware characteristics. Typical clinical indications for A-T training include the presenting symptoms shown in the figure below.
A-T training produces a state similar to mindfulness meditation and the witness state, in which clients observe their internal experience without active engagement. Participants report therapeutic reverie, symbolic imagery, emotional resolution, and insight. The crossover state may engage the default mode network—the same neural circuits involved in self-referential processing and memory consolidation—which helps explain why A-T training facilitates transformative psychological experiences.
Applications
This section examines the three primary domains in which A-T training has been applied: PTSD treatment, addictive behavior intervention, and optimal performance enhancement. Each application builds on the neurophysiological principles and clinical history covered earlier, illustrating how a single training approach can serve diverse populations—from veterans and individuals with substance use disorders to elite musicians and military personnel.
A-T training has been utilized for a variety of interventions that fall into three broad categories: PTSD (Peniston & Kulkosky, 1991), addictive behavior (Burkett et al., 2005; Scott et al., 2005; Peniston & Kulkosky, 1989, 1990), and optimal performance (Gruzelier et al., 2014). The breadth of these applications reflects the fundamental nature of the crossover state—it facilitates integration, consolidation, and self-regulation in ways that are relevant regardless of whether the client is recovering from trauma, overcoming addiction, or striving for peak performance. The trauma application receives closer attention in the next section, which examines what trauma leaves behind in the body and brain and how qEEG findings can shape an individualized training plan.
An example of optimal performance training can be seen in the work of Gruzelier and colleagues (2014), who studied university instrumentalists—experienced on their instruments but novice singers—in research published in Biological Psychology. Expert assessors rated performance in three music domains: creativity and musicality, technique, and communication and presentation. Only A-T training enhanced advanced instrumental playing, and it did so across all three domains, replicating an earlier finding in elite conservatoire musicians (Egner & Gruzelier, 2003); the A-T gains extended to the participants' novice vocal and improvised performance and were recognized by a lay audience. SMR training was not without effect: SMR learning correlated positively with technical competence and communication in the novice performances, consistent with its known influence on attention, working memory, and psychomotor skill. The pattern is one of frequency-specific effects, not of one protocol beating another on every measure.
Following Peniston's initial studies with addiction and PTSD, others have extended neurofeedback to diverse clinical environments, though not always with the A-T protocol. Nicholson and colleagues have published a series of PTSD studies that document neural change with functional magnetic resonance imaging (fMRI)—an imaging technique that infers regional neural activity from changes in blood oxygenation, at rest as well as during tasks. Their 2018 study delivered real-time fMRI neurofeedback for amygdala downregulation (this line of work is reviewed in Nicholson, Ros, Jetly, & Lanius, 2020), and their 2020 randomized, sham-controlled trial (Nicholson, Ros, Densmore, et al., 2020) randomized 36 adults with PTSD to 20 weekly sessions of training to reduce alpha amplitude at Pz (18 participants) or to sham feedback (18), reporting remission in 61% of the experimental group versus 33% of the sham group along with a shift toward normalized default mode and salience network connectivity. A third paper (Nicholson et al., 2019) is a machine-learning classification study rather than a treatment trial. This is important evidence that EEG neurofeedback can change PTSD-relevant networks, but it is not evidence about A-T training: the alpha training runs in the opposite direction and no theta reward is involved.
A-T training has been applied across three main domains: PTSD treatment, addictive behavior intervention, and optimal performance enhancement. Gruzelier's work with musicians demonstrated that A-T training produces frequency-specific improvements in creativity, technique, and communication that differ from those achieved with other neurofeedback protocols. Nicholson and colleagues have advanced PTSD applications by using fMRI to document the neural changes associated with neurofeedback, providing objective neuroimaging evidence for subjectively reported experiences.
Trauma and A-T Training
This section takes a closer look at the trauma application introduced above. You will examine what trauma leaves behind in the body and brain, why practitioners frequently begin with peripheral biofeedback before moving to neurofeedback, and how qEEG findings can be used to build an individualized training plan. A detailed case study then illustrates how amplitude down-training and A-T training can be sequenced within a single course of treatment.
What Trauma Leaves Behind
Trauma may be emotional, physical, or neurological. It arrives unexpectedly, when a sudden and overwhelming challenge exceeds what we are prepared for and able to handle—especially an event that makes us believe we could have died or that leaves us paralyzed and unable to act. Such events can occur at any age, once or repeatedly, and their effects often endure long after the event itself, limiting productivity and constraining loving relationships through the changes they produce in mind, body, and brain (Davis, 2022).
Those changes leave a measurable physical residue. Trauma alters hormones, neuromodulators—signaling molecules such as serotonin, dopamine, and norepinephrine that adjust the excitability and responsiveness of large populations of neurons rather than carrying a point-to-point message across a single synapse—and brain function itself (Sherin & Nemeroff, 2011; van der Kolk & Saporta, 1991). Practitioners also observe changes in heart rate variability (HRV), respiration, skin conductance, peripheral skin temperature, and muscle tension measured by electromyography (EMG). Changes in thinking and behavior almost invariably accompany these physiological shifts. Because each of these systems can be measured and fed back to the client, each also represents a potential point of intervention.
When adversity is chronic and begins early in life, clinicians describe it as developmental trauma—repeated, often relational harm during the years in which self-regulation, attachment, and the capacity to tolerate strong emotion are still being built. Fisher (2014) argues that this pattern produces a fear-driven brain whose regulatory difficulties differ from those following a single adult traumatic event, and that treatment must therefore be paced accordingly. The distinction matters for A-T training in particular, because clients with developmental trauma typically need more extensive preparation before they can safely lower their defenses.
Why Biofeedback Often Comes First
Biofeedback (BFB) and neurofeedback (NFB) directly address several of the key bodily and brain changes that trauma produces. Reviewing multiple randomized controlled trials, Moss, Shaffer, and Watkins (2023) assigned BFB and NFB for PTSD a Level 4 rating of efficacious—the second-highest level on the five-point efficacy scale used jointly by the Association for Applied Psychophysiology and Biofeedback (AAPB) and the International Society for Neuroregulation and Research (ISNR). Level 4 requires randomized comparison against a no-treatment, alternative-treatment, or sham condition, with defined inclusion criteria, valid outcome measures, replicable procedural reporting, and demonstration in at least two independent research settings (La Vaque et al., 2002). Superiority to a credible sham or bona fide alternative is what distinguishes Level 5, efficacious and specific.
BFB and NFB use precise sensors and computer analysis to teach self-awareness and self-control. In doing so, they demonstrate in a concrete, immediately observable way that there is a truth beyond the emotional pain, inability to act, and hopelessness that trauma seems to insist are permanent. With repetition, the client learns that they can influence physical effects of trauma that had appeared fixed, and the growing confidence that follows makes it possible to act more freely in ways that return meaning to life.
For many clients following trauma, BFB is the better place to begin, simply because functions such as breathing and muscle tension are relatively easy to bring under voluntary control. Success with HRV biofeedback, for example, is achieved through easily learned breathing skills, and remotely delivered, wearable-based HRV training paired with coaching was associated with reduced anxiety symptoms in a small, single-arm pilot study with no control group (N = 14; Chung et al., 2021). Early wins of this kind provide a firm foundation for progressing to NFB and the more demanding work of restoring brain function.
As successes with BFB and NFB accumulate, the physiological changes produced by trauma diminish—and the client also begins to think differently, believing that life stresses can be faced with confidence. That belief disconfirms what trauma had sought to teach: that one is helpless. As these successes accumulate and beliefs shift, it becomes far more possible to act differently in real life and to cope with situations and people that were previously feared and avoided. The practical implication is that integrating BFB and NFB with psychotherapy is especially helpful and can lead to enduring benefits.
A qEEG-Guided Trauma Intervention
In qEEG-guided neurofeedback, the training plan—which frequency band is rewarded, which bands are inhibited, and which electrode sites are used—is derived from the individual client's quantitative EEG findings rather than from a standard protocol assigned on the basis of diagnosis. The case described by Davis (2022) shows how this approach can combine amplitude down-training with A-T training in a single course of treatment.
TR was a 41-year-old man with a history of childhood developmental trauma who was injured in a car collision and sustained a mild concussion. He was referred for help managing anger that had worsened since the concussion. qEEG data collected during his assessment were summarized in a NeuroGuide z-score Fast Fourier Transform (FFT) summary report, which displays deviations from a normative database across five families of measures: absolute power, the raw amount of power in a frequency band at each site; relative power, the percentage of a site's total power contributed by that band; amplitude asymmetry, the difference in amplitude between paired electrode sites; coherence, the stability of the phase relationship between two sites, interpreted as an index of coupling or shared activity; and phase lag, the time delay between the appearance of a waveform at one site and its appearance at another. In TR's report, the color scale was set to display z-scores between ±1.5 and ±4.5 so that the locations of the largest elevations could be identified more precisely; several exceeded 4 standard deviations.
The most notable findings were excess high beta—activity in the upper portion of the beta band, commonly associated with hyperarousal, anxiety, rumination, and worry—at F3 and F4, present with eyes closed and with eyes open alike. These findings, rather than TR's diagnosis or presenting complaint alone, guided the selection of neurofeedback training.
Training proceeded in two stages. The first stage down-trained high beta amplitude at F3 and F4 with eyes open, targeting the frontal overarousal that the qEEG had localized. Only once that activity had come under control did the second stage introduce an A-T protocol at P4 with eyes closed, rewarding increases in the higher theta and lower alpha frequencies—the same crossover region described earlier in this unit. Integrated with the neurofeedback was cognitive-behavior therapy consistent with an Acceptance and Commitment Therapy (ACT) model, together with skills training in progressive muscle relaxation (PMR) and slow diaphragmatic breathing.
Two features of the outcome are worth noting. First, qEEG data collected at the conclusion of training showed reductions in excess high beta at both F3 and F4 in the eyes-open condition that had been trained and in the eyes-closed condition that had not—evidence that the learning generalized beyond the state in which it was acquired. Second, TR and his wife both reported significant reductions in anger expression, the behavioral goal that had brought him to treatment. Electrophysiological change and reported behavioral change moved together, which is the pattern practitioners hope to see when an intervention is working as intended rather than producing measurement artifacts or expectancy effects.
The sequencing in this case reflects a broader clinical principle. A-T training is rarely the first intervention. Excess fast-frequency activity, disturbed sleep, attentional difficulties, and autonomic overarousal are typically addressed first, because a client whose nervous system remains highly activated will struggle to reach and hold the crossover state. Stabilizing arousal makes the reverie state accessible; attempting A-T training before that point tends to produce frustration rather than insight.
Trauma leaves a measurable physical residue in hormones, neuromodulators, and brain function, as well as in HRV, respiration, skin conductance, skin temperature, and muscle tension—each of which is also a potential point of intervention. Moss, Shaffer, and Watkins (2023) rated BFB and NFB as efficacious (Level 4) for PTSD. Practitioners often begin with peripheral biofeedback because breathing and muscle tension are comparatively easy to control, building the confidence and skill needed before progressing to neurofeedback. In qEEG-guided neurofeedback, the client's own EEG findings determine protocol selection: in the case reported by Davis (2022), down-training excess high beta at F3 and F4 preceded A-T training at P4, gains appeared in both the trained and untrained conditions, and TR and his wife reported meaningful reductions in anger expression.
Cautions
This section addresses the safety considerations and risk mitigation strategies that practitioners should understand before implementing A-T training. Given that the crossover state involves a lowering of psychological defenses, careful preparation and appropriate protocol design are essential—particularly when working with trauma populations commonly seen in VA, hospital, and clinical settings.
Some practitioners in the neurofeedback field (Thompson & Thompson, 2003) have raised concerns about a significant probability of negative reactions to A-T training. They recommend that practitioners who use this intervention have advanced training in psychotherapeutic skills and education beyond introductory-level neurofeedback coursework. As discussed earlier in this unit, much of this concern stems from protocols that lack appropriate inhibit channels to alert the client when undesirable frequency activity is occurring. Practitioners who use the targeted 6-9 Hz protocol with low-frequency and high-frequency inhibits report that the risk of abreactions is substantially reduced; as noted earlier, that judgment rests on clinical experience rather than on controlled comparison.

That said, A-T training does encourage a decrease in emotional and psychological defenses, and it should be used with caution in individuals with a history of trauma. Client preparation is essential: clients should be instructed to immediately inform the practitioner of any negative reactions so that corrective training or a calming intervention—such as breath training via heart rate variability feedback—can be implemented promptly. Practitioners describe the hallmark outcome of well-conducted A-T training as a lasting decrease in limbic arousal of the kind often characteristic of persistent anxiety and PTSD, reported as reduced anxiety, easier transitions to sleep, deeper and more restful sleep, greater insulation from daily life stressors, and improved state management and stability. Limbic arousal here is inferred from those reports rather than measured: A-T training records scalp EEG, which does not resolve limbic activity.
Careful assessment is itself a risk-reduction strategy. When a client's qEEG shows marked overarousal—substantial excess high beta at frontal sites, for example—resolving that finding before introducing A-T training gives the client a more stable platform from which to lower their defenses, as the two-stage sequence reported by Davis (2022) illustrates. Fisher (2014) makes a parallel argument for developmental trauma, where the capacity to tolerate strong affect may itself be one of the treatment targets rather than a prerequisite the client already possesses.
As noted in the Expected Results section, there is evidence that the A-T crossover state may engage the default mode network (DMN), the brain network associated with self-referential processing, memory recall, and non-directed cognition (Davey & Harrison, 2018). This connection reinforces both the therapeutic potential and the need for caution: accessing deep self-referential processing can be profoundly beneficial, but it can also surface difficult material. Practitioners who are prepared for this possibility—and who have established a strong therapeutic alliance—are best positioned to help clients navigate these experiences safely and productively.
A-T training lowers emotional and psychological defenses, making client preparation and a strong therapeutic alliance essential—especially with trauma populations. Practitioners report that proper use of inhibit channels (2-6 Hz and 13-36 Hz) substantially reduces the risk of abreactions and negative reactions, though this has not been tested against a comparison condition. Practitioners should have advanced psychotherapeutic training, prepare clients thoroughly, and ensure immediate corrective interventions are available. When properly implemented, A-T training is reported to produce decreases in limbic arousal, improved sleep, and better overall state management.
Final Thoughts
Clients often present with conditions—such as ADHD, cognitive processing difficulties, memory deficits, or sensory processing issues—that require other training approaches before A-T training can be introduced. In practice, A-T training is frequently implemented after successful resolution of these primary concerns. When introduced at the right time, it can help clients integrate and consolidate the changes they have already achieved, providing perspective on how those improvements will shape their lives going forward.
All biofeedback ultimately aims to help clients learn skills they can apply for the rest of their lives. As clinicians, our goal is to foster independent, self-regulating individuals with new choices and opportunities. We want our clients to function optimally regardless of where they started, reducing the limitations and restrictions that once constrained them so they are free to pursue whatever goals they choose. A-T training, when used thoughtfully within a comprehensive treatment framework, is a powerful tool for achieving that vision.
Neurofeedback-Guided fMRI for PTSD
Nicholson and colleagues have advanced the integration of neurofeedback with neuroimaging technologies. Their double-blind, sham-controlled trial of alpha-rhythm EEG neurofeedback in posttraumatic stress disorder (Nicholson, Ros, Densmore, et al., 2020) reported decreased PTSD symptoms, a shift toward normalized default mode and salience network connectivity on fMRI, and remission in 61% of the experimental group versus 33% of the sham group, although the primary outcome showed a main effect of time without a group-by-time interaction. Because the training reduced alpha at Pz rather than rewarding a theta crossover, this is a neighboring protocol rather than A-T training. The convergence of real-time EEG feedback with functional imaging may nonetheless refine how clinicians target and monitor trauma interventions.
Memory Consolidation and the Crossover State
Emerging research on the role of theta rhythms in memory consolidation (Boyce et al., 2016) provides a neurobiological framework for understanding why the A-T crossover state may facilitate transformative experiences. The 6-9 Hz band targeted by A-T training falls within the frequency range of REM sleep theta, which Boyce and colleagues linked causally to contextual memory consolidation by optogenetically silencing medial septal GABAergic neurons in mice. The parallel is suggestive rather than established: that study removed hippocampal theta in a sleeping rodent, whereas A-T training rewards scalp theta in a waking human. It is a reason to take the consolidation hypothesis seriously, not evidence for it.
Slow Oscillation Stimulation and EEG Training
Work by Weise and colleagues (2013) on transcranial slow oscillation current stimulation (tSOS) has explored how externally applied slow oscillations influence EEG patterns, sleepiness, and alertness. This report is a conference poster abstract rather than a full peer-reviewed article, so it should be read as a pointer to an active research direction rather than as a finding to build on. tSOS is also a modulation technique rather than biofeedback; the interest for A-T practitioners lies in what it may eventually reveal about the slow-frequency states this training targets.
Check Your Understanding
- How does cross-frequency synchronization explain the relationship between slower and faster EEG rhythms in A-T training?
- What were the key outcomes of Peniston and Kulkosky's original alpha-theta training study with alcoholism, what limitations did later reviewers identify in it, and how did Scott et al.'s randomized trial extend and qualify these findings?
- Compare the three main A-T training approaches (dual-tone, ratio-based, and targeted 6-9 Hz) in terms of their advantages and limitations.
- Why is the therapeutic relationship particularly critical when implementing A-T training, and what preparatory interventions might a clinician use before introducing this protocol?
- What cautions should practitioners observe when using A-T training with trauma clients, and how do inhibit channels help mitigate risks?
- In the qEEG-guided case reported by Davis (2022), why was high beta down-training conducted before A-T training was introduced, and what evidence indicated that the training had generalized?
Assignment
Now that you have completed this unit, describe how clinicians have refined A-T training.
Glossary
abreaction: a strong, sometimes distressing emotional discharge during or after training, which may involve traumatic recall or depersonalization; in A-T training it is associated with drifting into slower, more sleep-like activity.
absolute power: the raw amount of EEG power within a frequency band at a given electrode site, expressed in microvolts squared, independent of activity in other bands. Power, not energy: energy would require multiplying power by time.
Acceptance and Commitment Therapy (ACT): a form of cognitive-behavior therapy that emphasizes accepting difficult internal experiences rather than attempting to eliminate them, clarifying personal values, and committing to actions consistent with those values.
alpha blocking: arousal and specific forms of cognitive activity may reduce alpha amplitude or eliminate it entirely while increasing EEG power in the beta range.
alpha response: an increased alpha amplitude.
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with relaxed wakefulness. Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
alpha spindles: trains of alpha waves that are visible in the raw EEG and are observed during drowsiness, fatigue, and meditative practice.
Alpha-Theta Training: a family of protocols that guide the EEG toward the crossover state while the client remains awake—classically by rewarding theta amplitude above alpha, and in the targeted variant by rewarding the 6-9 Hz band directly.
amplitude: the strength of a biological signal, measured for the EEG in microvolts. Amplitude is not power; power is amplitude squared and is reported in different units.
amplitude asymmetry: the difference in EEG amplitude between a pair of electrode sites, typically homologous sites in the left and right hemispheres, expressed in a qEEG report as a deviation from normative values.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
beta spindles: trains of spindle-like waveforms with frequencies that can be lower than 20 Hz but more often fall between 22 and 25 Hz. They may signal ADHD, especially with tantrums, anxiety, autistic spectrum disorders (ASD), epilepsy, and insomnia.
bipolar (sequential) montage: a recording arrangement in which each channel is the difference between two active electrodes, with no electrode serving as a common reference for all channels; successive channels share an electrode to form a chain.
bound network: a group of neurons whose slower rhythmic activity has become synchronized, providing the temporal framework within which faster oscillations are generated.
coherence: the stability of the phase relationship between the signals recorded at two electrode sites within a frequency band, interpreted as an index of the degree to which the two regions are coupled or share activity.
common-mode rejection (CMR): a differential amplifier's ability to amplify the difference between its two inputs while suppressing the voltage common to both. The common-mode rejection ratio (CMRR) expresses this as differential gain divided by common-mode gain, usually in decibels.
crossover state: the target state of A-T training, reached when theta (or, in the targeted protocol, 6-9 Hz) amplitude rises above alpha amplitude; subjectively, a reverie in which external sensory input recedes while the client remains awake.
default mode network (DMN): frontal, temporal, and parietal lobe circuits that are active during introspection and daydreaming and relatively inactive when pursuing external goals.
delta rhythm: 1-4 Hz oscillations generated by thalamocortical and cortical networks, dominant during N3 (stage 3) sleep.
developmental trauma: chronic, often relational adversity occurring during childhood, while capacities for self-regulation, attachment, and affect tolerance are still developing; its regulatory consequences differ from those following a single traumatic event in adulthood.
diaphragmatic breathing: slow, effortless breathing driven primarily by contraction of the diaphragm rather than accessory chest and shoulder muscles, producing abdominal expansion on inhalation.
EEG activity: a single wave or series of waves.
efficacious (Level 4): the second-highest rating on the five-level efficacy scale used jointly by the Association for Applied Psychophysiology and Biofeedback (AAPB) and the International Society for Neuroregulation and Research (ISNR), requiring randomized comparison against a no-treatment, alternative-treatment, or sham condition, operationally defined inclusion criteria, valid outcome measures, replicable procedural reporting, and demonstration in at least two independent research settings. Level 5, efficacious and specific, additionally requires superiority to a credible sham or bona fide alternative treatment.
epileptiform activity: spikes and sharp waves associated with seizure disorders.
Fast Fourier Transform (FFT): mathematical transformation that converts a complex signal into component sine waves whose amplitude can be calculated.
frequency: the number of complete cycles that an AC signal completes in a second, usually expressed in hertz.
functional magnetic resonance imaging (fMRI): an imaging technique that infers regional neural activity indirectly from blood-oxygenation-level-dependent (BOLD) signal changes, during tasks or at rest.
global synchronization: widespread coordination of neuronal activity across brain regions, characteristic of resting states and stages of sleep and associated with integration and consolidation.
hertz (Hz): the unit of frequency measured in cycles per second.
high beta: the upper portion of the beta band, most often defined as roughly 20-30 Hz, with some normative databases using a narrower 25-30 Hz band. Elevations are associated with hyperarousal, anxiety, rumination, and worry, and may also reflect EMG artifact.
inhibit channel: a feedback channel that signals the client when activity in an undesired frequency band rises above threshold, so that the reward band can be trained without drifting toward sleep or cognitive activation.
International 10-20 electrode placement system: the standard scheme for locating scalp electrodes at 10% and 20% intervals along measured distances between the nasion, inion, and preauricular points; odd numbers mark the left hemisphere, even numbers the right, and z the midline.
local field potential (LFP): the summed extracellular voltage produced mainly by synchronized postsynaptic potentials in a local population of neurons; it reflects input to those neurons rather than their spike output, and the scalp EEG is its volume-conducted expression.
neuromodulator: a signaling molecule, such as serotonin, dopamine, norepinephrine, or acetylcholine, that adjusts the excitability and responsiveness of large populations of neurons rather than carrying a point-to-point message across a single synapse.
oscillatory timing: the rhythmic organization of neuronal activity at specific frequencies, which the brain uses to coordinate the exchange of information among populations of neurons.
phase lag: the time delay, expressed in degrees or milliseconds, between the appearance of a waveform at one electrode site and its appearance at another.
posterior dominant rhythm (PDR): the highest-amplitude frequency detected at the posterior scalp when eyes are closed.
power: amplitude squared, expressed in microvolts squared. Microvolts squared equal picowatts only under the convention of a 1-ohm reference resistance, which must be stated whenever picowatts are used. Because of the squaring, amplitude-based and power-based ratios and thresholds are not interchangeable.
progressive muscle relaxation (PMR): a skills-training procedure in which the client systematically tenses and then releases successive muscle groups to learn to discriminate tension from relaxation and to reduce resting muscle tone.
proportional audio signal: feedback whose loudness varies continuously in proportion to the amplitude of the trained band, so the client always knows how close they are to the target state rather than only whether a threshold was crossed.
qEEG-guided neurofeedback: neurofeedback in which the rewarded band, inhibited bands, and electrode sites are selected from the individual client's quantitative EEG findings rather than from a standard protocol assigned by diagnosis.
Quantitative EEG (qEEG): digitized statistical brain mapping using at least a 19-channel montage to measure EEG amplitude within specific frequency bins.
relative power: the percentage of the total EEG power at an electrode site that is contributed by a particular frequency band; unlike absolute power, it depends on activity in all other bands.
reticular nucleus of the thalamus (nRt): a thin sheet of inhibitory neurons surrounding the thalamus that gates thalamocortical transmission and participates in generating the alpha rhythm and sleep spindles.
self-referential state: a mode of processing in which attention is directed inward—toward one's own thoughts, memories, and sense of self—rather than toward external goals; associated with activity in the default mode network.
sensorimotor rhythm (SMR): 12-15-Hz spindle-shaped rhythm detected from the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
small-world network: a network in which most neurons connect locally while a small number of hub connections link distant clusters, allowing efficient communication with relatively few long-range links.
thalamocortical relay (TCR) system: the ascending pathway carrying sensory information from the thalamus to the cortex, gated by the reticular nucleus of the thalamus.
theta-alpha ratio: the ratio of theta to alpha amplitude, used in simplified A-T protocols to trigger a single feedback tone when theta exceeds alpha and passes a set threshold.
theta/beta ratio (T/B ratio): the ratio between 4-7 Hz theta and 13-21 Hz beta, measured most typically along the midline and generally in the anterior midline near the 10-20 system location Fz.
theta rhythm: 4-7-Hz rhythms generated by a cholinergic septohippocampal system that receives input from the ascending reticular formation and a noncholinergic system that originates in the entorhinal cortex, which corresponds to Brodmann areas 28 and 34 at the caudal region of the temporal lobe.
witness state: a mode of awareness, also described in mindfulness practice, in which the individual observes the flow of thoughts, memories, and images without pursuing or analyzing them.
z-score training: a neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Ancoli, S., & Kamiya, J. (1978). Methodological issues in alpha biofeedback training. Biofeedback and Self-Regulation, 3(2), 159–183. https://doi.org/10.1007/bf00998900
Berger, H. (1929). Über das Elektrenkephalogramm des Menschen. Archiv für Psychiatrie und Nervenkrankheiten, 87(1), 527–570. https://doi.org/10.1007/BF01797193
Boyce, R., Glasgow, S. D., Williams, S., & Adamantidis, A. (2016). Causal evidence for the role of REM sleep theta rhythm in contextual memory consolidation. Science, 352(6287), 812–816. https://doi.org/10.1126/science.aad5252
Brown, B. B. (1974). New mind, new body: Bio-feedback: New directions for the mind. Harper & Row.
Budzynski, T. H. (1976). Biofeedback and the twilight states of consciousness. In G. E. Schwartz & D. Shapiro (Eds.), Consciousness and self-regulation: Advances in research (Vol. 1, pp. 361–385). Plenum Press.
Burkett, V. S., Cummins, J. M., Dickson, R. M., & Skolnick, M. (2005). An open clinical trial utilizing real-time EEG operant conditioning as an adjunctive therapy in the treatment of crack cocaine dependence. Journal of Neurotherapy, 9(2), 27–47. https://doi.org/10.1300/J184v09n02_03
Buzsáki, G. (2006). Rhythms of the brain. Oxford University Press.
Chung, A. H., Gevirtz, R. N., Gharbo, R. S., Thiam, M. A., & Ginsberg, J. P. (2021). Pilot study on reducing symptoms of anxiety with a heart rate variability biofeedback wearable and remote stress management coach. Applied Psychophysiology and Biofeedback, 46(4), 347–358. https://doi.org/10.1007/s10484-021-09519-x
Cox, C. L., Huguenard, J. R., & Prince, D. A. (1997). Nucleus reticularis neurons mediate diverse inhibitory effects in thalamus. Proceedings of the National Academy of Sciences, 94(16), 8854–8859. https://doi.org/10.1073/pnas.94.16.8854
Davey, C. G., & Harrison, B. J. (2018). The brain's center of gravity: How the default mode network helps us to understand the self. World Psychiatry: Official Journal of the World Psychiatric Association (WPA), 17(3), 278–279. https://doi.org/10.1002/wps.20553
Davis, J. (2022, September 25). A successful qEEG-guided trauma intervention. BioSource Software. https://www.biosourcesoftware.com/post/a-successful-qeeg-guided-trauma-intervention
Egner, T., & Gruzelier, J. H. (2003). Ecological validity of neurofeedback: Modulation of slow wave EEG enhances musical performance. NeuroReport, 14(9), 1221–1224. https://doi.org/10.1097/00001756-200307010-00006
Fisch, B. J. (1999). Fisch and Spehlmann's EEG primer: Basic principles of digital and analog EEG (3rd ed.). Elsevier.
Fisher, S. F. (2014). Neurofeedback in the treatment of developmental trauma: Calming the fear-driven brain. W. W. Norton.
Graap, K., & Freides, D. (1998). Regarding the database for the Peniston alpha-theta EEG biofeedback protocol. Applied Psychophysiology and Biofeedback, 23(4), 265–272. https://doi.org/10.1023/A:1022265716026
Green, E., & Green, A. (1977). Beyond biofeedback. Delacorte Press.
Gruzelier, J. H., Holmes, P., Hirst, L., Bulpin, K., Rahman, S., van Run, C., & Leach, J. (2014). Replication of elite music performance enhancement following alpha/theta neurofeedback and application to novice performance and improvisation with SMR benefits. Biological Psychology, 95, 96–107. https://doi.org/10.1016/j.biopsycho.2013.11.001
Hardt, J., & Kamiya, J. (1976). Some comments on Plotkin's self-regulation of electroencephalographic alpha. Journal of Experimental Psychology: General, 105(1), 100–108. https://doi.org/10.1037/0096-3445.105.1.100
Hardt, J. V., & Kamiya, J. (1978). Anxiety change through electroencephalographic alpha feedback seen only in high anxiety subjects. Science, 201(4350), 79–81. https://doi.org/10.1126/science.663641
Kamiya, J. (1961). Behavioral, subjective, and physiological aspects of drowsiness and sleep. In D. W. Fiske & S. R. Maddi (Eds.), Functions of varied experience (pp. 145–174). Dorsey Press.
Kamiya, J. (1962, April). Conditioned discrimination of the EEG alpha rhythm in humans [Paper presentation]. Western Psychological Association meeting, San Francisco, CA, United States.
Kamiya, J. (1968, April). Conscious control of brain waves. Psychology Today, 1, 56–60.
Kamiya, J. (1969). Operant control of the EEG alpha rhythm and some of its reported effects on consciousness. In C. T. Tart (Ed.), Altered states of consciousness. Wiley.
La Vaque, T. J., Hammond, D. C., Trudeau, D., Monastra, V., Perry, J., Lehrer, P., Matheson, D., & Sherman, R. (2002). Template for developing guidelines for the evaluation of the clinical efficacy of psychophysiological interventions. Applied Psychophysiology and Biofeedback, 27(4), 273–281. https://doi.org/10.1023/A:1021061318355
Moss, D., Shaffer, F., & Watkins, M. (2023). Posttraumatic stress disorder. In I. Khazan, F. Shaffer, D. Moss, R. Lyle, & S. Rosenthal (Eds.), Evidence-based practice in biofeedback and neurofeedback (4th ed.). Association for Applied Psychophysiology and Biofeedback.
Nicholson, A. A., Rabellino, D., Densmore, M., Frewen, P. A., Paret, C., Kluetsch, R., Schmahl, C., Théberge, J., Ros, T., Neufeld, R. W. J., McKinnon, M. C., Reiss, J. P., Jetly, R., & Lanius, R. A. (2018). Intrinsic connectivity network dynamics in PTSD during amygdala downregulation using real-time fMRI neurofeedback: A preliminary analysis. Human Brain Mapping, 39(11), 4258–4275. https://doi.org/10.1002/hbm.24244
Nicholson, A. A., Densmore, M., McKinnon, M. C., Neufeld, R. W. J., Frewen, P. A., Théberge, J., Jetly, R., Richardson, J. D., & Lanius, R. A. (2019). Machine learning multivariate pattern analysis predicts classification of posttraumatic stress disorder and its dissociative subtype: A multimodal neuroimaging approach. Psychological Medicine, 49(12), 2049–2059. https://doi.org/10.1017/S0033291718002866
Nicholson, A. A., Ros, T., Densmore, M., Frewen, P. A., Neufeld, R. W. J., Théberge, J., Jetly, R., & Lanius, R. A. (2020). A randomized, controlled trial of alpha-rhythm EEG neurofeedback in posttraumatic stress disorder: A preliminary investigation showing evidence of decreased PTSD symptoms and restored default mode and salience network connectivity using fMRI. NeuroImage: Clinical, 28, 102490. https://doi.org/10.1016/j.nicl.2020.102490
Nicholson, A. A., Ros, T., Jetly, R., & Lanius, R. (2020). Regulating posttraumatic stress disorder symptoms with neurofeedback: Regaining control of the mind. Journal of Military, Veteran and Family Health, 6(S1), 3–15. https://doi.org/10.3138/jmvfh.2019-0032
Norris, P. (2017). How it all began [Chapter 2]. In A. Martins-Mourao & C. Kerson (Eds.), Alpha-theta neurofeedback in the 21st century: A handbook for clinicians and researchers (2nd ed.). Foundation for Neurofeedback and Neuromodulation Research.
Peniston, E. G. (1998). Comments by Peniston. Applied Psychophysiology and Biofeedback, 23(4), 273–275. https://doi.org/10.1023/A:1022217900096
Peniston, E. G., & Kulkosky, P. J. (1989). Alpha-theta brainwave training and beta-endorphin levels in alcoholics. Alcoholism: Clinical and Experimental Research, 13(2), 271–279. https://doi.org/10.1111/j.1530-0277.1989.tb00325.x
Peniston, E. G., & Kulkosky, P. J. (1990). Alcoholic personality and alpha-theta brainwave training. Medical Psychotherapy, 3, 37–55.
Peniston, E. G., & Kulkosky, P. J. (1991). Alpha-theta brainwave neurofeedback for Vietnam veterans with combat-related post-traumatic stress disorder. Medical Psychotherapy, 4, 47–60.
Scott, W. C., Kaiser, D., Othmer, S., & Sideroff, S. I. (2005). Effects of an EEG biofeedback protocol on a mixed substance abusing population. The American Journal of Drug and Alcohol Abuse, 31(3), 455–469. https://doi.org/10.1081/ada-200056807
Sherin, J. E., & Nemeroff, C. B. (2011). Post-traumatic stress disorder: The neurobiological impact of psychological trauma. Dialogues in Clinical Neuroscience, 13(3), 263–278. https://doi.org/10.31887/DCNS.2011.13.2/jsherin
Sokhadze, T. M., Cannon, R. L., & Trudeau, D. L. (2008). EEG biofeedback as a treatment for substance use disorders: Review, rating of efficacy, and recommendations for further research. Applied Psychophysiology and Biofeedback, 33(1), 1–28. https://doi.org/10.1007/s10484-007-9047-5
Thompson, M., & Thompson, L. (2003). The neurofeedback book: An introduction to basic concepts in applied psychophysiology. Association for Applied Psychophysiology and Biofeedback.
van der Kolk, B. A., & Saporta, J. (1991). The biological response to psychic trauma: Mechanisms and treatment of intrusion and numbing. Anxiety Research, 4(3), 199–212. https://doi.org/10.1080/08917779108248774
Weise, R., von Mengden, I., Glos, M., Garcia, C., & Penzel, T. (2013). P 153. Influence of transcranial slow oscillation current stimulation (tSOS) on EEG, sleepiness and alertness. Clinical Neurophysiology, 124(10), e137. https://doi.org/10.1016/j.clinph.2013.04.230
Return to Top