Ongoing Assessment
What You Will Learn in This Chapter
Ongoing assessment is the backbone of effective neurofeedback practice. While intake and EEG assessments establish your starting baseline, it is the continuous process of tracking, measuring, and evaluating client progress that determines whether training is achieving its goals. Without ongoing assessment, you are essentially flying blind.
In this unit, you will explore the measures and methods used for ongoing evaluation, including EEG variables, qualitative reports, quantitative self-report tools, self-monitoring, behavioral observation, rating scales, cognitive tests, and psychophysiological measures. You will also learn how to integrate these data into evidence-based decision-making frameworks that guide protocol adjustments and treatment planning.
BCIA Blueprint Coverage: This unit addresses VI. Patient/Client Assessment - C. Ongoing Assessment.
Learning Objectives
After completing this section, you will be able to:
Describe the purpose and ethical rationale for ongoing assessment during neurofeedback training.
Identify and explain EEG-based measures used for tracking session-to-session progress.
Differentiate among qualitative anecdotal reports, quantitative self-report, and behavioral observation methods.
Apply the SMART goals framework to define measurable treatment objectives.
Explain how evidence-based practice principles guide decision-making about protocol continuation, modification, or discontinuation.
Overview
This section covers the rationale for ongoing assessment, including why it matters clinically, how it connects to core ethical principles, and how it supports the therapeutic relationship. Intake and initial EEG assessment provide a baseline against which you can gauge subsequent progress—or its absence. This baseline is essential because, despite group-level evidence supporting the efficacy and effectiveness of neurofeedback across a range of conditions—evidence whose strength varies considerably from one application to the next (Schwartz & Andrasik, 2016; Tan et al., 2016), benefits are never guaranteed for any individual client.
The primary purpose of ongoing assessment—the continuous evaluation of client progress throughout training—is to verify that expected outcomes are occurring and, when they are not, to use that data to adjust training protocols. In other words, ongoing assessment transforms neurofeedback from a fixed procedure into an adaptive, responsive treatment. Graphic courtesy of Mitsar.
The ethical foundations of ongoing assessment map directly onto the four principles of biomedical ethics set out by Beauchamp and Childress (2019) and summarized by Beauchamp (2003). Beneficence asks whether training is helping, while nonmaleficence asks whether it is causing harm—including the indirect harm of ongoing costs in time and money for an ineffective treatment. Autonomy requires that the client remain well-informed about outcomes so they can provide meaningful consent to continue, and justice asks whether training is efficient enough that it does not unreasonably deny access to other clients who need services.
Beyond ethics, ongoing assessment strengthens the therapeutic alliance by giving the client and practitioner shared data from which to make collaborative, evidence-based decisions. Seeing measurable progress motivates clients to persist with training and to apply emerging self-regulation skills outside the session. Reviewing data together can also help clients recognize connections between their internal states and real-world behavior—for example, noticing that the calm, focused state they achieve during neurofeedback can be intentionally recreated before a stressful meeting or exam.
Ultimately, because the goal of neurofeedback extends beyond changing EEG activity to improving emotion, cognition, physiological function, and real-life behavior, ongoing assessment must also include non-EEG measures that track whether brain-level changes are generalizing to the domains that matter most to the client.
Ongoing assessment verifies that neurofeedback produces expected outcomes and provides data to adjust protocols when it does not. It is grounded in the ethical principles of beneficence, nonmaleficence, autonomy, and justice. Continuous assessment supports collaborative decision-making, motivates clients, and tracks whether EEG changes generalize to real-life improvements in emotion, cognition, and behavior.
BCIA Blueprint Coverage
This unit covers VI. Patient/Client Assessment - C. Ongoing Assessment.

This unit covers Measures and Methods and Decision-Making.
Measures and Methods
EEG Variables
This section covers how EEG data serve as the most direct index of neurofeedback training effects, including session-to-session tracking, within-session monitoring, and network-level assessment. The most natural measure for ongoing assessment is the EEG variable you have targeted for training—for example, sensorimotor rhythm (SMR) amplitude, the strength of brain activity in the 12–15 Hz range recorded over the sensorimotor cortex and expressed in microvolts. Amplitude and power are not interchangeable: power is amplitude squared and is reported in microvolts squared, so thresholds and ratios do not carry over between them. The underlying logic is straightforward: if you are rewarding SMR production, you should see SMR amplitude increase over time.
Neurofeedback at a single electrode site may also produce changes that generalize to other sites and broader brain networks. A sham-controlled trial of alpha training at a single site (Pz) in posttraumatic stress disorder reported evidence of restored default mode and salience network connectivity on fMRI, in what its authors called a preliminary investigation (Nicholson et al., 2020). Practitioners who have access to 19-channel quantitative EEG (qEEG) hardware and software—systems that record from multiple scalp locations and apply digital analysis to amplitude, power, coherence, and phase—can therefore assess whether single-channel training has influenced network-level function (Thatcher, 2020). This capacity to look beyond the trained site is especially valuable when treating complex conditions that involve widespread dysregulation.
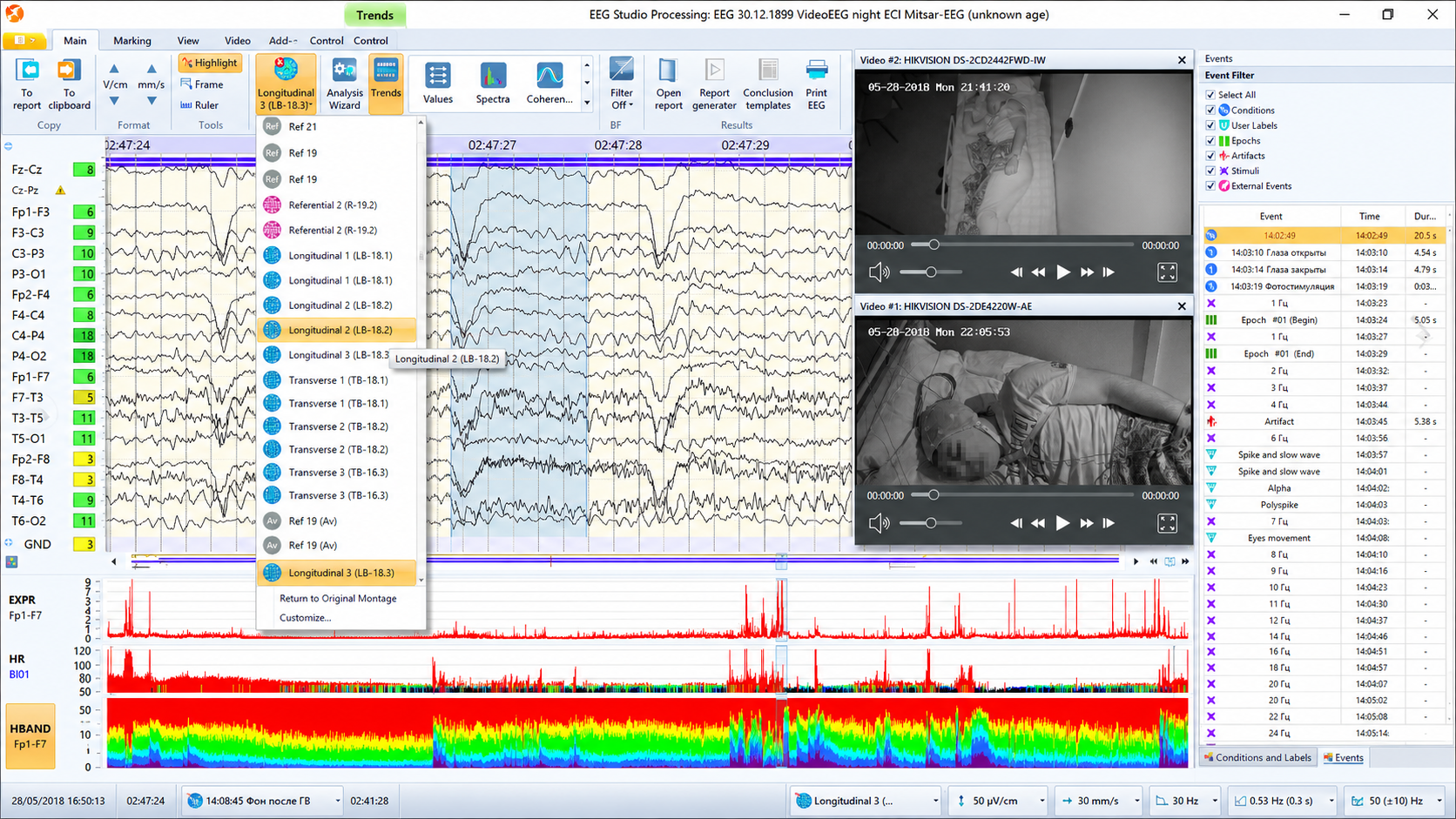
The movie below is a 19-channel BioTrace+ /NeXus-32 display of SMR activity © John S. Anderson. Brighter colors represent higher SMR amplitudes. Frequency histograms are displayed for each channel. Notice the runs of high-amplitude SMR activity.
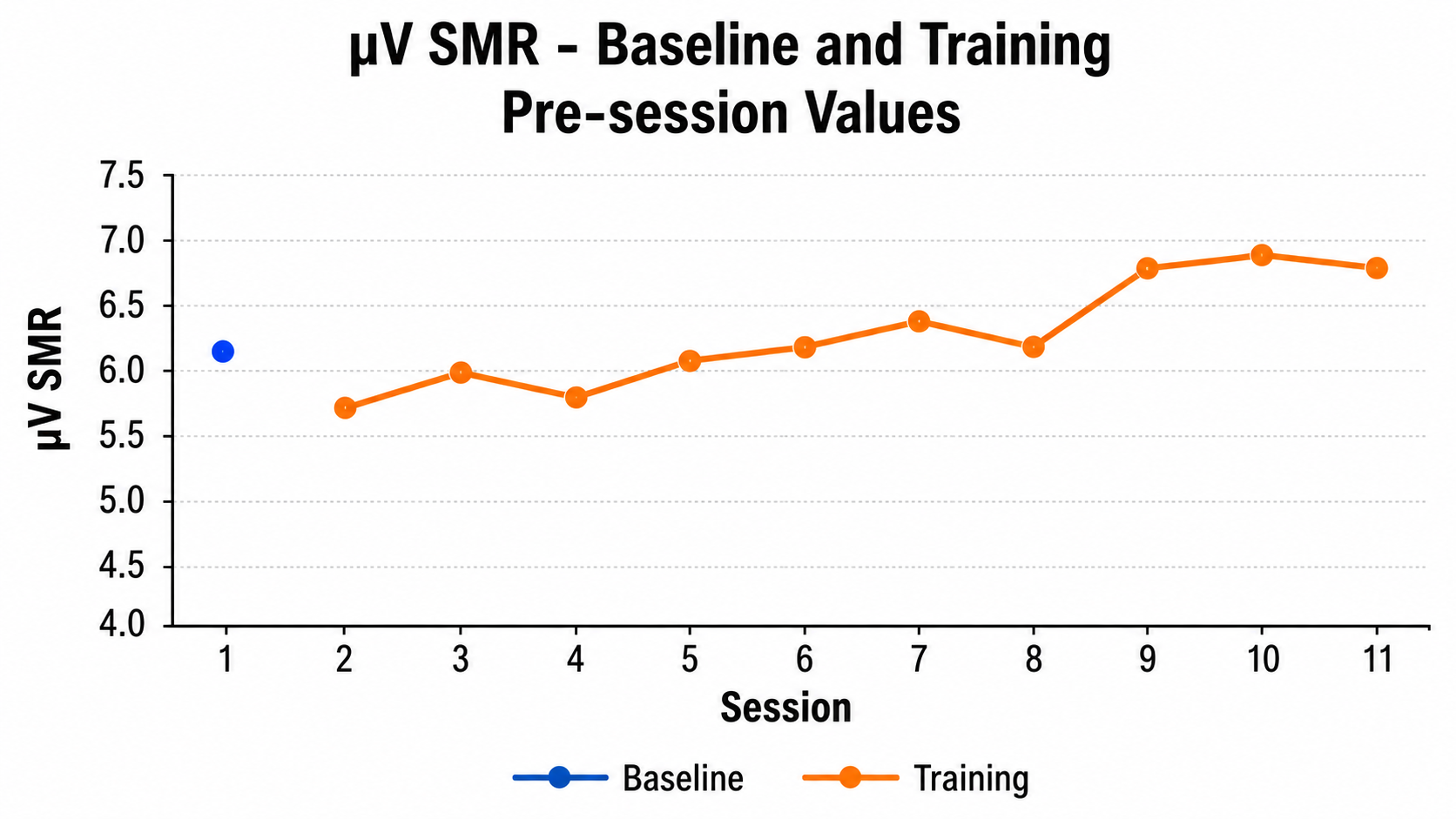
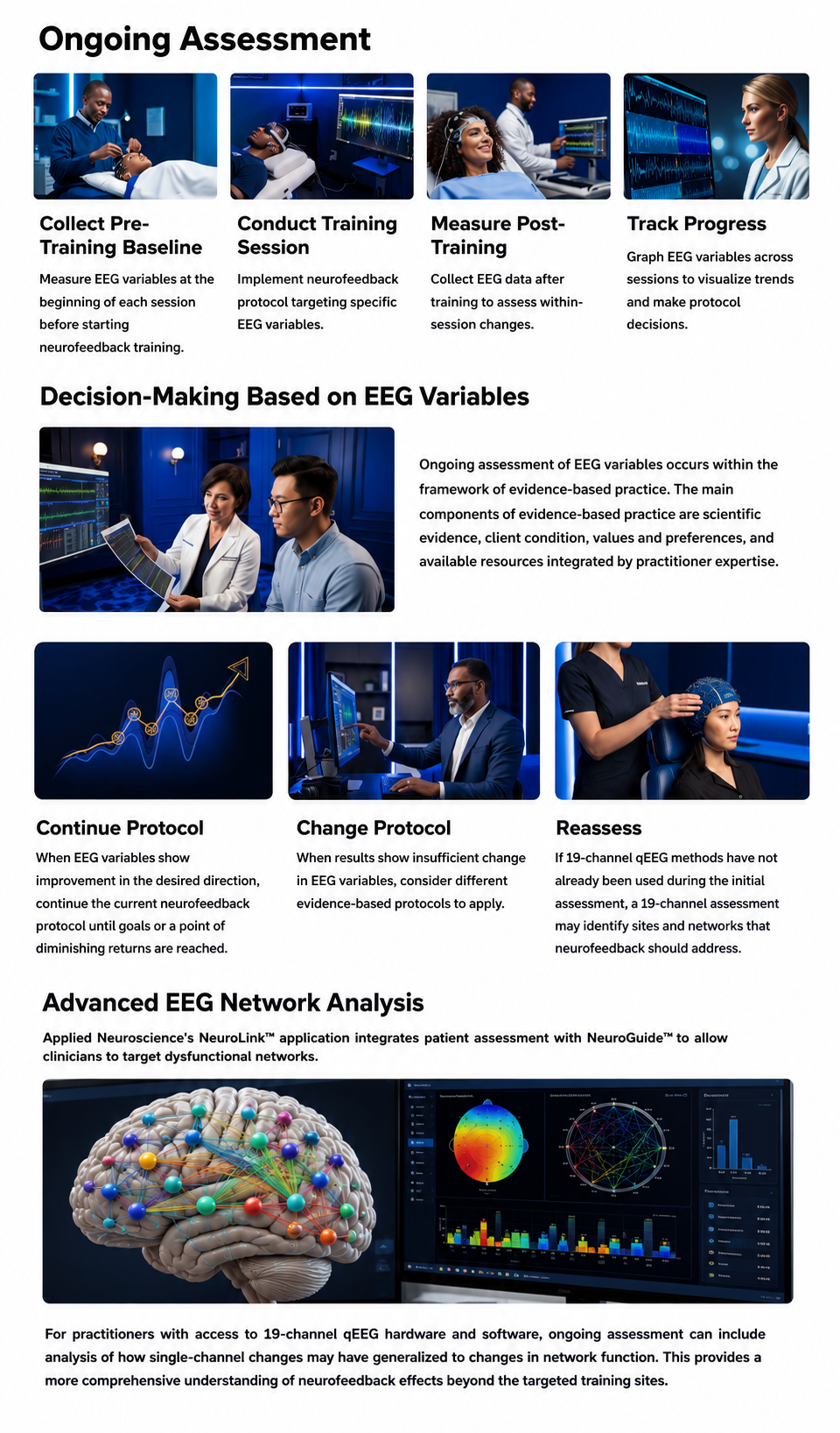
In practice, you typically measure the targeted EEG variable during a pre-training baseline—a brief resting recording at the start of each session—and then graph that value from session to session, using the intake assessment as the reference point (see Figure 1).
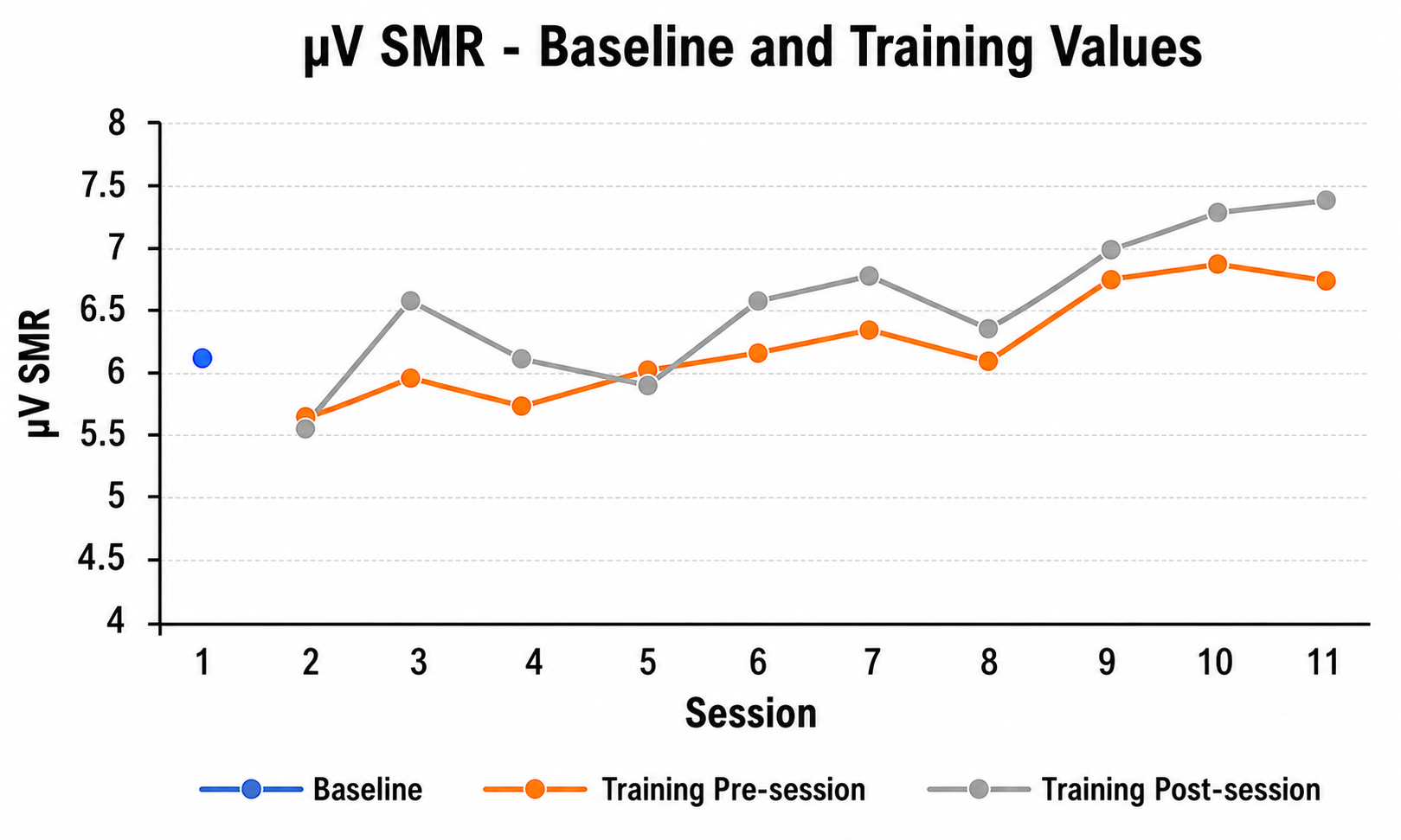
You can also record a post-training baseline at the end of each session and compare it to that session's pre-training value, which reveals whether the session itself produced a change in the intended direction. Plotting pre- and post-training data together, or graphing a series of within-session change scores, gives you a richer picture of how training effects accumulate over time (see Figure 2).
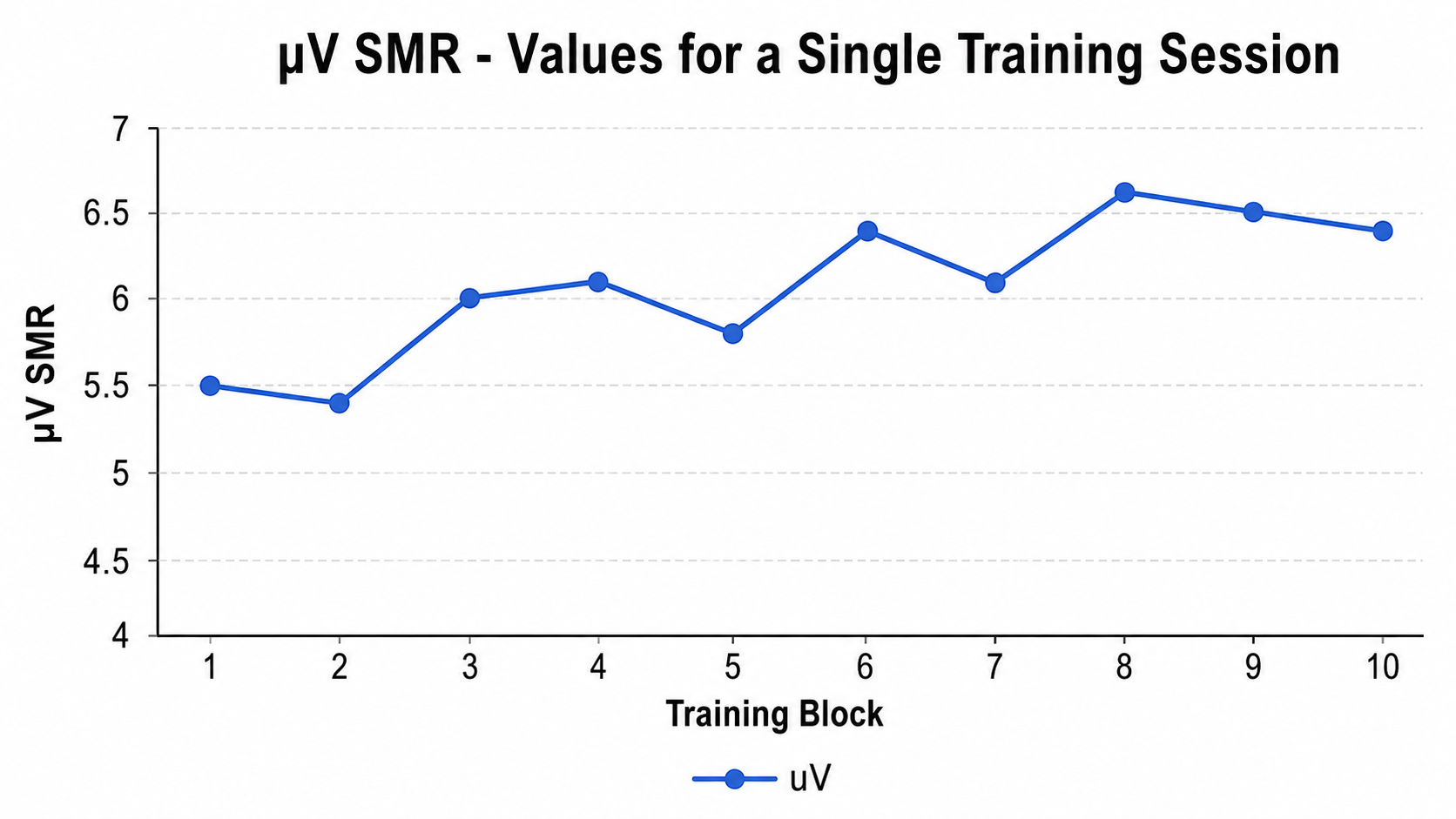
For even finer resolution, you can graph EEG data across individual training blocks within a session—for example, plotting ten consecutive 3-minute trials to see whether amplitude shifts emerge during a single sitting (see Figure 3).
Many neurofeedback platforms make it easy to collect and graph EEG variables of interest, whether derived from single or multiple channels. Some platforms include built-in graphing capabilities, while others require you to export data into a spreadsheet for visualization.
EEG variables provide the most direct measure of neurofeedback training effects. Pre-training and post-training baselines can be graphed session to session, and within-session training blocks can reveal whether changes are occurring during individual sessions. Practitioners with 19-channel qEEG systems can additionally assess whether single-site training has generalized to broader network-level changes.
Qualitative Anecdotal Report
This section covers how narrative, open-ended reports from clients and informants complement EEG data by capturing real-world changes in experience and behavior. One product of intake assessment is the identification of a goal with practical consequences for the client—such as feeling less depressed, experiencing fewer headaches, concentrating better, or avoiding social situations less often. Goals may be framed positively or negatively (more of A, or less of B) and may reference either internal states like thoughts and emotions or observable behaviors like pages written or hours studied (Hurn et al., 2006).
A qualitative anecdotal report is a narrative description in which the client recounts a specific personal situation—together with the internal experiences and behavioral details surrounding it—to represent the current state of their presenting problem or progress toward their goal. At the beginning of each session, you can ask the client or a collateral informant—someone such as a parent, spouse, or teacher who can provide detailed background information or a different perspective on the client's functioning—to describe changes they have noticed. For example, both a child receiving neurofeedback and their parent can be asked how distractible the child has been over the past few days, and their responses can be compared for consistency.
To sharpen these reports, you might ask the client to describe the specific situation in which they were most distractible, anchoring the anecdote to a particular time and place rather than relying on vague generalizations. Practitioner notes from these conversations can then be compared from session to session to build an impressionistic but informative picture of change over time.
Qualitative assessment is also essential during the first several training sessions for monitoring unwanted side effects of training, such as fatigue, excessive arousal, or headache. Catching these early allows you to adjust protocols before minor complaints become significant obstacles to progress. Graphic courtesy of Migraine Buddy.

Qualitative anecdotal reports capture the client's narrative description of how their presenting problem is changing in everyday life. Both the client and collateral informants provide valuable, complementary perspectives. These reports are particularly important during the early stages of training for monitoring unwanted side effects such as fatigue or headache.
Quantitative Self-Report
This section covers how numerical rating tools transform subjective experiences into trackable data, and how structured goal frameworks improve the reliability of ongoing assessment. Although clients may initially describe their problems in imprecise, everyday language, it is helpful to define those concerns more formally so that progress can be quantified. Quantification makes it possible to graph changes over time and more easily detect meaningful trends. A review of patient-based measures in routine practice found little evidence that collecting them, by itself, improved outcomes (Greenhalgh & Meadows, 1999), so plan to review the data with the client and act on them.
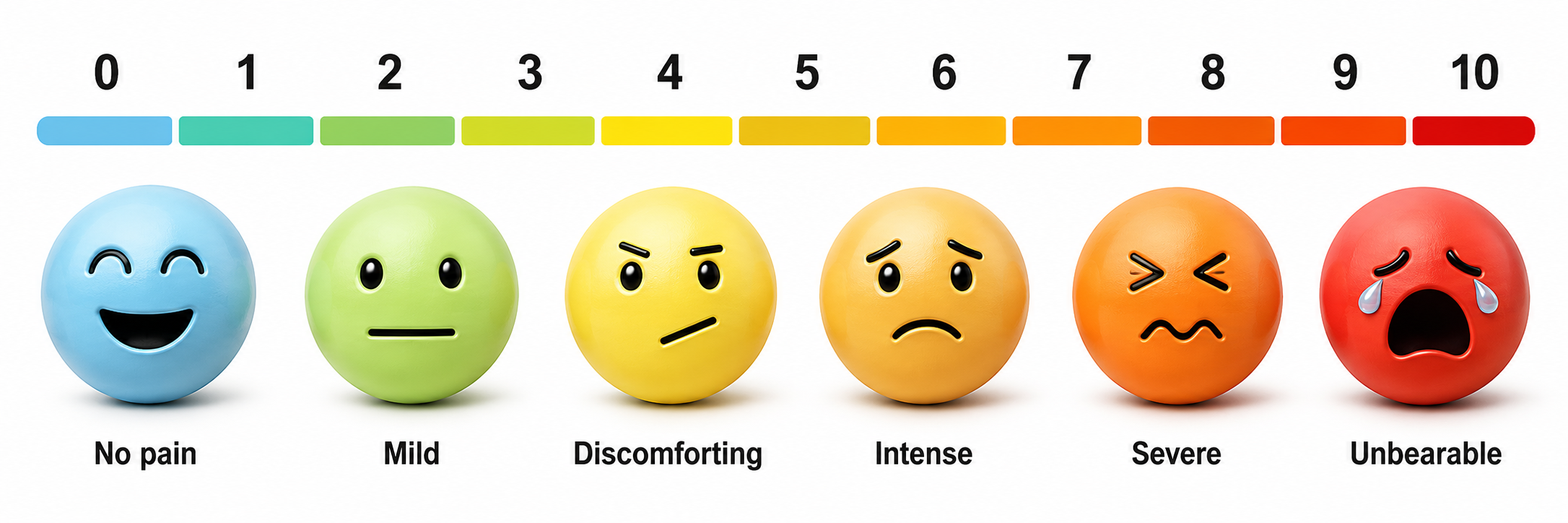
Internal subjective states can be measured using visual analog scales (VAS)—continuous lines on which the client marks a point between two extremes—or Likert scales, which offer a set of labeled response options (e.g., 1 = "not at all" to 5 = "extremely"). Strictly, one such question is a Likert item; a Likert scale is the composite formed by summing several such items. Clearly defining each scale item and labeling the anchor points helps make these tools more reliable and valid (Joshi et al., 2015; Wewers & Lowe, 1990). At the beginning of a session, the client can mark their typical state over the previous few days, or their state at that moment, and the resulting values can be graphed across sessions for collaborative review. We adapted the pain rating scale graphic below from © Overearth/Shutterstock.com. Note that a 0-to-10 scale with discrete numbers and faces is a numeric rating scale rather than a true VAS, which uses an unmarked continuous line.
Behavioral goals can be operationally defined—that is, specified in terms of the concrete operations used to measure them (Martin & Pear, 2019). For instance, if "improved concentration" is the goal, you might define it as the number of minutes the client spent studying the previous day. A more structured approach is the SMART goals framework, which calls for goals that are specific, measurable, achievable, relevant, and time-bound (Bovend'Eerdt et al., 2009, who write the last two letters as "realistic/relevant" and "timed"; the expansion varies by author). Behavior analytic tactics (Cooper et al., 2007) can further sharpen these goals by specifying frequency, intensity, duration, and context—for example: "During a typical week with ordinary stressors, a headache will occur not more than twice, with an average duration of not more than 1 hour and an average severity of not more than 2 on a 0-to-5 scale." We adapted the SMART goals graphic from © Appleing/Shutterstock.com.

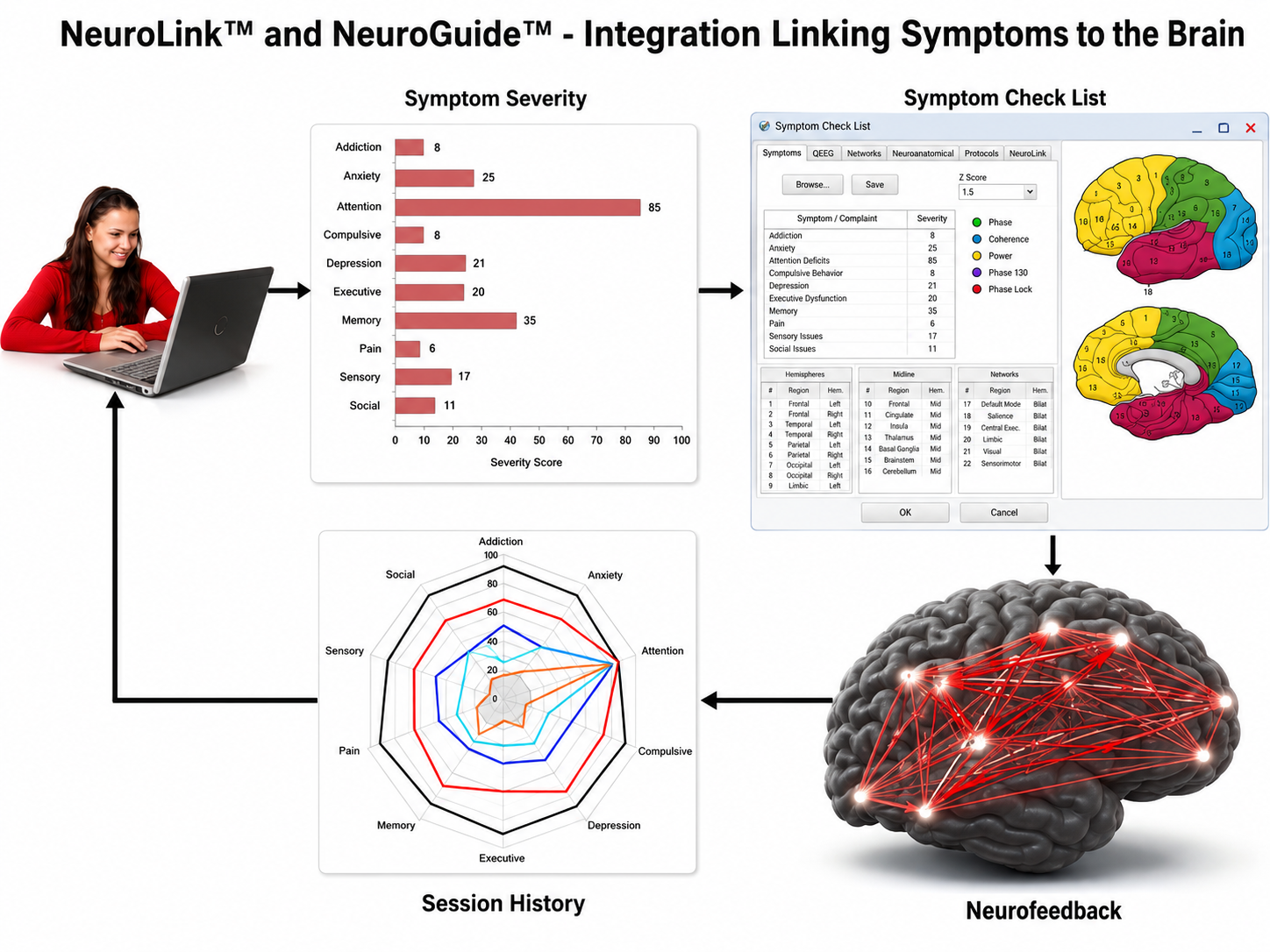
After intake assessment and SMART goal definition, the practitioner can efficiently assess progress at the start of each training session. Because SMART goals are readily quantifiable, baseline and session-by-session values can be graphed for visual inspection and joint interpretation. Applied Neuroscience's NeuroLink™ application illustrates this integration by combining patient self-assessment with NeuroGuide™ to help clinicians target dysfunctional networks.
Quantitative self-report tools, including visual analog scales and Likert scales, transform subjective experiences into trackable numerical data that can be graphed over time. The SMART goals framework provides a structured approach for defining specific, measurable, achievable, relevant, and time-bound objectives, producing outcome data that are easier to track and interpret than responses to open-ended questions alone.
Self-Monitoring
This section covers how extending assessment beyond the clinic into clients' daily routines captures real-world functioning and strengthens self-regulation skills. Like the within-session reports described in previous sections, clients can also be asked to make ratings at assigned times and in specified situations outside the neurofeedback session. This practice is called self-monitoring—the client's own systematic tracking of symptoms (e.g., stress, distractibility) or abilities (e.g., sustained attention, time on task, accuracy) relevant to their presenting concerns. Self-monitoring can begin immediately after intake assessment and continue throughout training (Bakker & Rickard, 2018; Melbye et al., 2020).
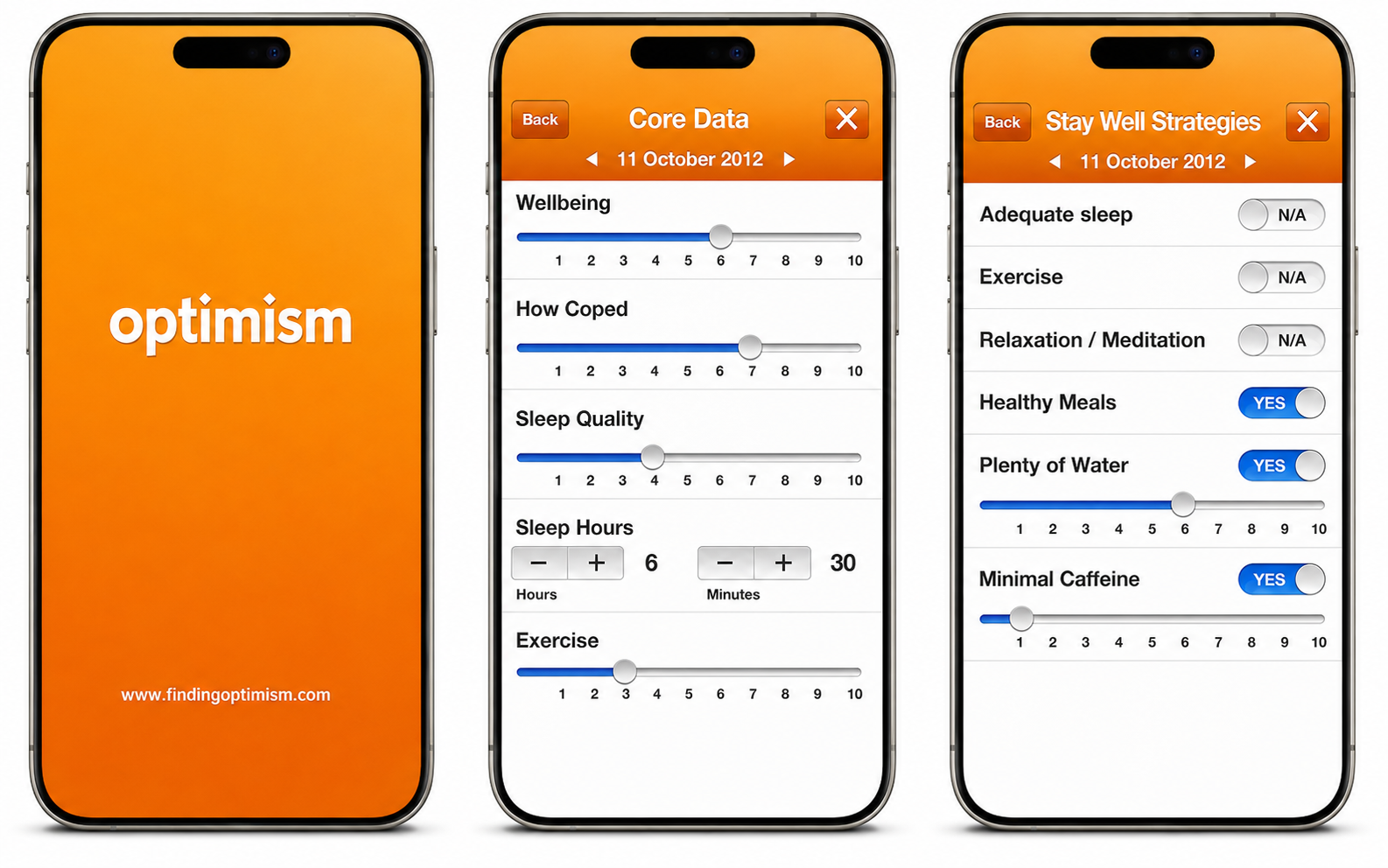
Self-monitoring benefits clients in two important ways. First, it generates data from naturalistic settings that complement in-session measures. Second, it increases the client's self-awareness in day-to-day situations, which can strengthen their ability to self-regulate internal states—emotion, cognition, and physiological arousal—in the service of more effective behavior. Graphic courtesy of the Optimism family of mental health applications.
Structuring self-monitoring around specific situations or times improves reliability and validity. A situation-based approach might ask the client to rate their concentration level during a particular classroom activity, such as completing algebra problems; selecting one consistent context reduces variability from situation to situation. A time-based approach might ask the client to rate their calmness at a fixed point in the day, such as after their first hour of work or at day's end.
Whichever approach you choose, planning is critical. Clients need clear situational or temporal cues to remember their ratings—a sticky note in an algebra notebook, an electronic alarm, or a smartphone app that prompts completion at the right moment (Bakker & Rickard, 2018; Melbye et al., 2020). Building self-monitoring into the client's routine, rather than relying on memory alone, is what makes the data useful over time.
Self-monitoring extends assessment beyond the training session into the client's daily life, generating naturalistic data and strengthening self-regulation skills. Structuring self-monitoring around specific situations or fixed times improves data reliability. Planning clear cues and using smartphone apps help clients maintain consistent self-monitoring practices throughout treatment.
Behavioral Observation
This section covers how direct observation of behavior provides objective, quantifiable data that complement self-report methods. Direct observation of behavior (Cooper et al., 2007; Kamphaus & Dever, 2016) is widely used in both research and clinical settings to establish how frequently, how long, or under what conditions a target behavior occurs. For example, a parent might count the number of times a child interrupts during a set period and calculate a rate per hour, or a teacher might record at defined intervals whether a student is on-task during class.
These observations are readily quantifiable and can be graphed to track change over the course of neurofeedback training. Because they capture behavior as it actually happens—rather than relying on retrospective self-report—they provide an especially valuable complement to the methods described in earlier sections. Graphic © Photographee.eu/Shutterstock.com.

Rating Scales
This section covers how standardized, psychometrically validated instruments offer a rigorous complement to informal self-report and observation. Unlike the informal scales described in the Quantitative Self-Report section, standardized rating scales have been systematically evaluated for their psychometric properties—that is, their reliability (consistency of measurement) and validity (accuracy in measuring what they claim to measure; Baer & Blais, 2010; Tate, 2010). They provide a quick, well-validated method for assessing progress during neurofeedback training, especially when the same instruments were used during intake to establish baseline scores.
Rating scales sample a wide range of domains, including emotional experience, cognitive function, physiological symptoms, and everyday functional abilities. They can be completed periodically before training sessions or at home between sessions. Common examples include the Beck Depression Inventory-II (Beck et al., 1996) for tracking depressive symptoms and the Depression Anxiety Stress Scales (DASS; Lovibond & Lovibond, 1995) for monitoring broader emotional distress. We adapted this graphic from © PsychCorp.
Many practitioners combine neurofeedback and biofeedback with mindfulness meditation training (Khazan, 2013), a practice associated with physiological, cognitive, and emotional benefits. Clients taught to apply mindfulness during neurofeedback sessions may become more aware of the mind-body state associated with successful feedback, and this heightened awareness can become the basis for voluntary self-regulation—intentionally recreating that beneficial state during relevant real-world situations. If you incorporate mindfulness into your practice, several psychometrically sound instruments can measure the client's developing skill, including the Toronto Mindfulness Scale (Lau et al., 2006) and the Mindful Attention Awareness Scale (Brown & Ryan, 2003; further validated by MacKillop & Anderson, 2007).
Cognitive Tests
This section covers how standardized tests of thinking and cognition can track neurofeedback-related gains while managing practical challenges like practice effects. Cognitive tests can be readministered periodically during neurofeedback training to assess whether changes in brain activity are translating into improvements in attention, memory, processing speed, or executive function. Two practical challenges arise, however: the practitioner's time required for administration, and the risk of spuriously inflated scores from practice effects—improvements that result from familiarity with the test rather than genuine cognitive change.
Computerized testing platforms address the time challenge by allowing clients to complete assessments independently after brief instructions—for example, CNS Vital Signs (Gualtieri & Johnson, 2006). Practice effects can be managed by using alternate forms, which are different versions of the same test designed to be equivalent in difficulty—such as the Repeatable Battery for the Assessment of Neuropsychological Status, which has four equivalent forms (RBANS; Randolph et al., 1998). Graphic © Pearson.
Psychophysiological Assessment
This section covers how peripheral physiological measures complement EEG tracking and reveal whether neurofeedback effects are generalizing across body systems. Several platforms now support concurrent neurofeedback and peripheral biofeedback, making it straightforward to record psychophysiological measures—such as skin conductance, skin temperature, respiration rate, heart rate variability, and electromyography (EMG)—alongside EEG data during each session.
These peripheral measures can be recorded during pre- or post-training baselines, just as you would with EEG variables. When peripheral biofeedback training is not part of the treatment plan, changes in these measures serve as evidence that neurofeedback effects are generalizing beyond the brain to other relevant physiological domains. Cross-system change of this kind is encouraging, but it is suggestive rather than conclusive: peripheral measures also respond to posture, breathing, medication, and the passage of time.
Behavioral observation, standardized rating scales, cognitive tests, and psychophysiological measures each provide a distinct window into client progress. Behavioral observation captures real-world functioning, rating scales offer psychometrically validated measurement, cognitive tests assess changes in thinking and processing, and psychophysiological assessment evaluates whether neurofeedback effects are generalizing across physiological domains. Used together, these methods give you a comprehensive picture of treatment outcomes.
Decision-Making
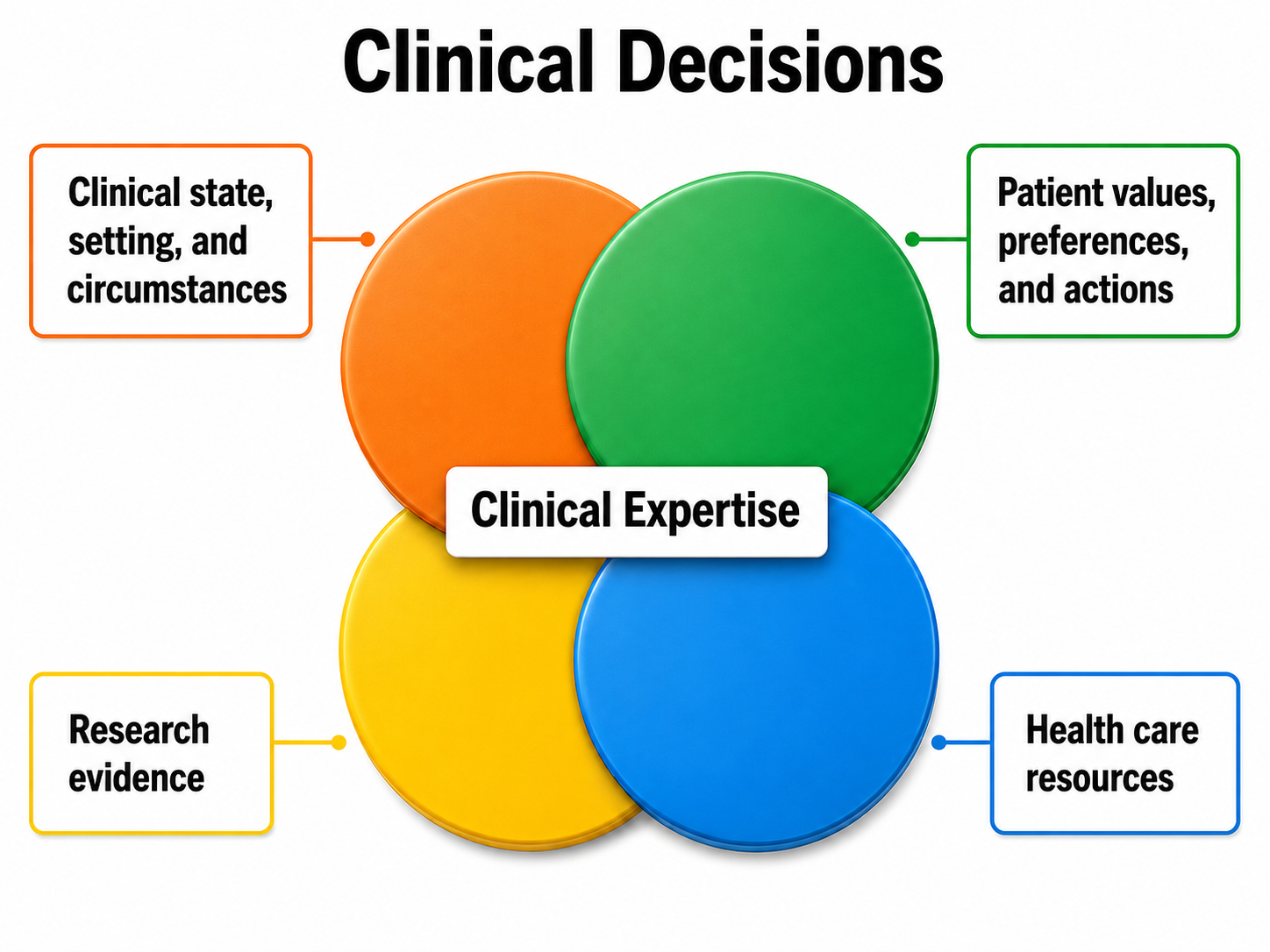
This section covers how the data collected through ongoing assessment feed into an evidence-based decision-making framework that guides protocol adjustments and treatment planning. Ongoing assessment during neurofeedback operates within the framework of evidence-based practice—an approach that integrates scientific evidence, the client's condition, values and preferences, and available resources, all synthesized through practitioner expertise (McMaster University Health Sciences Library, 2021; Melnyk et al., 2010). In practical terms, the data you collect through the measures and methods described above inform collaborative decisions about whether to continue the current protocol, change it, or discontinue training altogether.
When assessment results show improvement, the natural course is to continue neurofeedback until the client's goals are met or a point of diminishing returns is reached, at which time training may be discontinued or redirected toward new goals. When results show insufficient change, the client and practitioner can consider switching to a different evidence-based protocol (Tan et al., 2016). If 19-channel qEEG methods were not used during the initial assessment, conducting one at this point may identify sites and networks that earlier training did not address.
For many clients, neurofeedback alone—however helpful—may not be sufficient to fully resolve a presenting problem or reach a goal. Integrating neurofeedback with complementary interventions is common in practice, although the added value of any particular combination has to be judged case by case. Thompson and Thompson (2015) describe methods such as heart rate variability training and transcranial electrical stimulation that pair well with neurofeedback, while Weiner (2016) reviews how neurofeedback and psychotherapy can be conducted together for synergistic effects.
Finally, some clients experience significant developments during training—a new medical diagnosis, major family disruption, or other life crises—that make successful treatment temporarily impractical. In these cases, it may be more appropriate to pause training until the new concerns have been addressed, rather than continuing sessions that are unlikely to produce meaningful gains under the circumstances.
Decision-making in neurofeedback is guided by evidence-based practice principles that integrate scientific evidence, client preferences, and practitioner expertise. When progress stalls, options include changing protocols, conducting additional qEEG assessment, integrating complementary interventions, or postponing training when significant life events intervene. Ongoing assessment data make each of these decisions transparent and collaborative.
Summary
This unit has reviewed the full range of approaches to ongoing assessment—from EEG variable tracking and qualitative anecdotal reports to quantitative self-report, behavioral observation, standardized rating scales, cognitive tests, and psychophysiological measures—and situated them within ethical and evidence-based healthcare frameworks. Decision-making options based on observed training results have also been outlined.
Ongoing assessment is essential for ethical, effective neurofeedback practice. It encompasses EEG variable tracking, qualitative and quantitative self-report, behavioral observation, standardized rating scales, cognitive testing, and psychophysiological measures. These data feed into an evidence-based decision-making framework that guides whether to continue, modify, or discontinue training.
Digital Self-Monitoring and Ecological Momentary Assessment
Smartphone-based self-monitoring applications are transforming how clients track symptoms between neurofeedback sessions. Ecological momentary assessment (EMA) methods allow clients to report their experiences in real time, reducing recall bias and providing richer data for practitioners to evaluate training effects in naturalistic settings (Bakker & Rickard, 2018; Melbye et al., 2020). For clinicians working in VA, hospital, or community settings, EMA offers a practical way to gather high-quality between-session data without adding to an already demanding appointment schedule.
Network-Level Assessment with qEEG
Advances in 19-channel qEEG technology and network analysis are enabling practitioners to assess how single-channel neurofeedback training generalizes to broader brain network changes. Tools like NeuroGuide allow clinicians to visualize connectivity patterns and identify dysfunctional networks that may require targeted intervention (Thatcher, 2020), and single-site alpha training has been associated with network-level change on fMRI (Nicholson et al., 2020). This capability is particularly relevant for complex clinical presentations—such as PTSD in military populations or traumatic brain injury—where disrupted connectivity across multiple networks may underlie the client's symptoms.
Check Your Understanding
- What ethical principles support the need for ongoing assessment during neurofeedback training?
- How can pre-training and post-training EEG baselines be used to track session-to-session progress?
- What are the advantages of using SMART goals over general goals for measuring neurofeedback outcomes?
- How does self-monitoring between sessions complement within-session assessment methods?
- Within an evidence-based practice framework, what decision-making options are available when neurofeedback results show insufficient change?
Assignment
Now that you have completed this unit, which sounds do you prefer when you have succeeded during neurofeedback training? Which visual displays are more motivating for you?
Glossary
alternate forms: equivalent versions of the same test, used to limit practice effects on retesting.
autonomy: the ethical principle that the client stay informed about outcomes so that consent to continue remains meaningful.
beneficence: the ethical principle that an intervention should benefit the client.
classical conditioning: unconscious associative learning process that builds connections between paired stimuli that follow each other in time.
collateral informant: a parent, spouse, teacher, or other individual who can provide detailed background information or a different perspective on the client's functioning.
ecological momentary assessment (EMA): real-time reports of experience in the client's natural environment, which reduce recall bias.
evidence-based practice: integration of scientific evidence, the client's condition, values and preferences, and available resources through practitioner expertise.
justice: the ethical principle that treatment be efficient enough not to deny services unreasonably to other clients.
Likert scale: a composite score summed from several labeled-response questions; one such question is a Likert item.
nonmaleficence: the ethical principle that an intervention should not harm the client, including by continuing an ineffective treatment.
ongoing assessment: the continuous evaluation of client progress.
operational definition: a goal or variable stated in terms of the operations used to measure it.
post-training baseline: a brief resting recording at the end of a session.
practice effects: score gains from familiarity with a test rather than from genuine change.
pre-training baseline: a brief resting recording at the start of a session.
qualitative anecdotal report: a narrative description of changes in the problem or goal by the client or collateral informant.
quantitative EEG (qEEG): digital analysis of EEG amplitude, power, coherence, and phase, usually from 19 or more scalp locations.
quantitative self-report: a client's numerical ratings of symptoms, subjective states, and behaviors.
rating scale: a standardized instrument whose reliability and validity have been systematically evaluated.
self-monitoring: a client's systematic tracking of symptoms or abilities at assigned times in specified situations outside the neurofeedback session, which generates naturalistic data and increases self-awareness.
sensorimotor rhythm (SMR): EEG activity from 12 to 15 Hz recorded over the sensorimotor cortex.
SMART: a framework that prescribes goals that are specific, measurable, achievable, relevant, and time-bound.
visual analog scale (VAS): a continuous unmarked line on which the client marks a point between two labeled extremes.
References
Baer, L., & Blais, M. A. (Eds.). (2010). Handbook of clinical rating scales and assessment in psychiatry and mental health. Humana Press.
Bakker, D., & Rickard, N. (2018). Engagement in mobile phone app for self-monitoring of emotional wellbeing predicts changes in mental health: MoodPrism. Journal of Affective Disorders, 227, 432-442. https://doi.org/10.1016/j.jad.2017.11.016
Beauchamp, T. L. (2003). Methods and principles in biomedical ethics. Journal of Medical Ethics, 29(5), 269-274. https://doi.org/10.1136/jme.29.5.269
Beauchamp, T. L., & Childress, J. F. (2019). Principles of biomedical ethics (8th ed.). Oxford University Press.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. Psychological Corporation.
Bovend'Eerdt, T. J. H., Botell, R. E., & Wade, D. T. (2009). Writing SMART rehabilitation goals and achieving goal attainment scaling: A practical guide. Clinical Rehabilitation, 23(4), 352-361. https://doi.org/10.1177/0269215508101741
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822-848. https://doi.org/10.1037/0022-3514.84.4.822
Cooper, J. O., Heron, T. E., & Heward, W. L. (2007). Applied behavior analysis (2nd ed.). Pearson Merrill Prentice Hall.
Greenhalgh, J., & Meadows, K. (1999). The effectiveness of the use of patient-based measures of health in routine practice in improving the process and outcomes of patient care: A literature review. Journal of Evaluation in Clinical Practice, 5(4), 401-416. https://doi.org/10.1046/j.1365-2753.1999.00209.x
Gualtieri, C. T., & Johnson, L. G. (2006). Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology, 21(7), 623-643. https://doi.org/10.1016/j.acn.2006.05.007
Hurn, J., Kneebone, I., & Cropley, M. (2006). Goal setting as an outcome measure: A systematic review. Clinical Rehabilitation, 20(9), 756-772. https://doi.org/10.1177/0269215506070793
Joshi, A., Kale, S., Chandel, S., & Pal, D. K. (2015). Likert scale: Explored and explained. British Journal of Applied Science & Technology, 7(4), 396-403. https://doi.org/10.9734/BJAST/2015/14975
Kamphaus, R. W., & Dever, B. V. (2016). Behavioral observations and assessment. In J. C. Norcross, G. R. VandenBos, D. K. Freedheim, & R. Krishnamurthy (Eds.), APA handbook of clinical psychology: Applications and methods (Vol. 3, pp. 17-29). American Psychological Association.
Khazan, I. Z. (2013). Clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. Wiley-Blackwell.
Lau, M. A., Bishop, S. R., Segal, Z. V., Buis, T., Anderson, N. D., Carlson, L., Shapiro, S., Carmody, J., Abbey, S., & Devins, G. (2006). The Toronto Mindfulness Scale: Development and validation. Journal of Clinical Psychology, 62(12), 1445-1467. https://doi.org/10.1002/jclp.20326
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety Stress Scales (2nd ed.). Psychology Foundation.
MacKillop, J., & Anderson, E. J. (2007). Further psychometric validation of the Mindful Attention Awareness Scale (MAAS). Journal of Psychopathology and Behavioral Assessment, 29(4), 289-293. https://doi.org/10.1007/s10862-007-9045-1
Martin, G., & Pear, J. J. (2019). Behavior modification: What it is and how to do it (11th ed.). Routledge.
McMaster University Health Sciences Library. (2021, May 5). Introduction to evidence-based practice. https://hslmcmaster.libguides.com/c.php?g=306765&p=2044668
Melbye, S., Kessing, L. V., Bardram, J. E., & Faurholt-Jepsen, M. (2020). Smartphone-based self-monitoring, treatment, and automatically generated data in children, adolescents, and young adults with psychiatric disorders: Systematic review. JMIR Mental Health, 7(10), e17453. https://doi.org/10.2196/17453
Melnyk, B. M., Fineout-Overholt, E., Stillwell, S. B., & Williamson, K. M. (2010). Evidence-based practice: Step by step: The seven steps of evidence-based practice. American Journal of Nursing, 110(1), 51-53. https://doi.org/10.1097/01.NAJ.0000366056.06605.d2
Nicholson, A. A., Ros, T., Densmore, M., Frewen, P. A., Neufeld, R. W. J., Théberge, J., Jetly, R., & Lanius, R. A. (2020). A randomized, controlled trial of alpha-rhythm EEG neurofeedback in posttraumatic stress disorder: A preliminary investigation showing evidence of decreased PTSD symptoms and restored default mode and salience network connectivity using fMRI. NeuroImage: Clinical, 28, 102490. https://doi.org/10.1016/j.nicl.2020.102490
Randolph, C., Tierney, M. C., Mohr, E., & Chase, T. N. (1998). The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. Journal of Clinical and Experimental Neuropsychology, 20(3), 310-319. https://doi.org/10.1076/jcen.20.3.310.823
Schwartz, M. S., & Andrasik, F. (Eds.). (2016). Biofeedback: A practitioner's guide (4th ed.). Guilford Press.
Tan, G., Shaffer, F., Lyle, R., & Teo, I. (2016). Evidence-based practice in biofeedback & neurofeedback (3rd ed.). Association for Applied Psychophysiology and Biofeedback.
Tate, R. (2010). Compendium of tests, scales and questionnaires: Practitioner's guide to measuring outcomes after acquired brain impairment. Psychology Press.
Thatcher, R. W. (2020). Handbook of quantitative electroencephalography and EEG biofeedback (2nd ed.). ANI Publishing.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Weiner, G. (2016). Evolving as a neurotherapist: Integrating psychotherapy and neurofeedback. In T. F. Collura & J. A. Frederick (Eds.), Handbook of clinical QEEG and neurotherapy (pp. 45-54). Routledge.
Wewers, M. E., & Lowe, N. K. (1990). A critical review of visual analogue scales in the measurement of clinical phenomena. Research in Nursing & Health, 13(4), 227-236. https://doi.org/10.1002/nur.4770130405
Return to Top