Remote Neurofeedback Training
What You Will Learn in This Chapter
Remote neurofeedback training is changing how practitioners deliver services, extending access to clients who may be across town or on another continent. This chapter explores what remote neurofeedback looks like in practice, examines the research that supports it, and walks through the critical considerations you must address before offering it.
You will learn how advances in communication and computer technologies have expanded access to neurofeedback, review the research evidence for both remote biofeedback and remote neurofeedback, and evaluate the client-related, financial, ethical, and legal factors that shape safe and effective remote practice.
BCIA Blueprint Coverage: This unit addresses VIII. Treatment Implementation - E. Guidelines and Cautions for Remote Training.
Learning Objectives
After completing this section, you will be able to:
Define remote neurofeedback training and describe how it differs from in-clinic training.
Summarize the research evidence supporting remote biofeedback and remote neurofeedback.
Identify client-related, financial, ethical, and legal considerations for remote training.
Describe the typical course of remote neurofeedback training from assessment through follow-up.
Explain the precautions necessary to ensure safe and effective remote neurofeedback practice.
BCIA Blueprint Coverage
This unit covers VIII. Treatment Implementation - E. Guidelines and Cautions for Remote Training.

This unit covers What is Remote Training?, Research Review, Considerations with Remote Training, Typical Course of Training, and Summary and Conclusions.
What is Remote Neurofeedback Training?
This section introduces the concept of remote neurofeedback, explains how it works, and describes the technology and preparation it requires. Advances in communications and computer technologies now allow neurofeedback training to occur when the client and practitioner are not in the same room. Remote neurofeedback training, a form of telehealth, uses electronic and communication technologies to deliver neurofeedback to clients in a different location than the neurofeedback practitioner. The geographic distance between them may be small, such as across town, or large, such as across continents. This expanded reach can significantly increase accessibility to training, but many issues must be addressed to ensure that remote delivery remains effective and safe.

The degree of practitioner involvement during remote sessions varies considerably. The practitioner may be virtually present in real-time, meaning events are monitored as they occur, using screen-sharing software to control the neurofeedback software on the client's computer while interacting verbally via video. Alternatively, the practitioner may be available only by phone while the client operates pre-configured software. In some arrangements, the practitioner is not present at all during sessions but follows up at scheduled intervals to monitor progress and adjust settings.
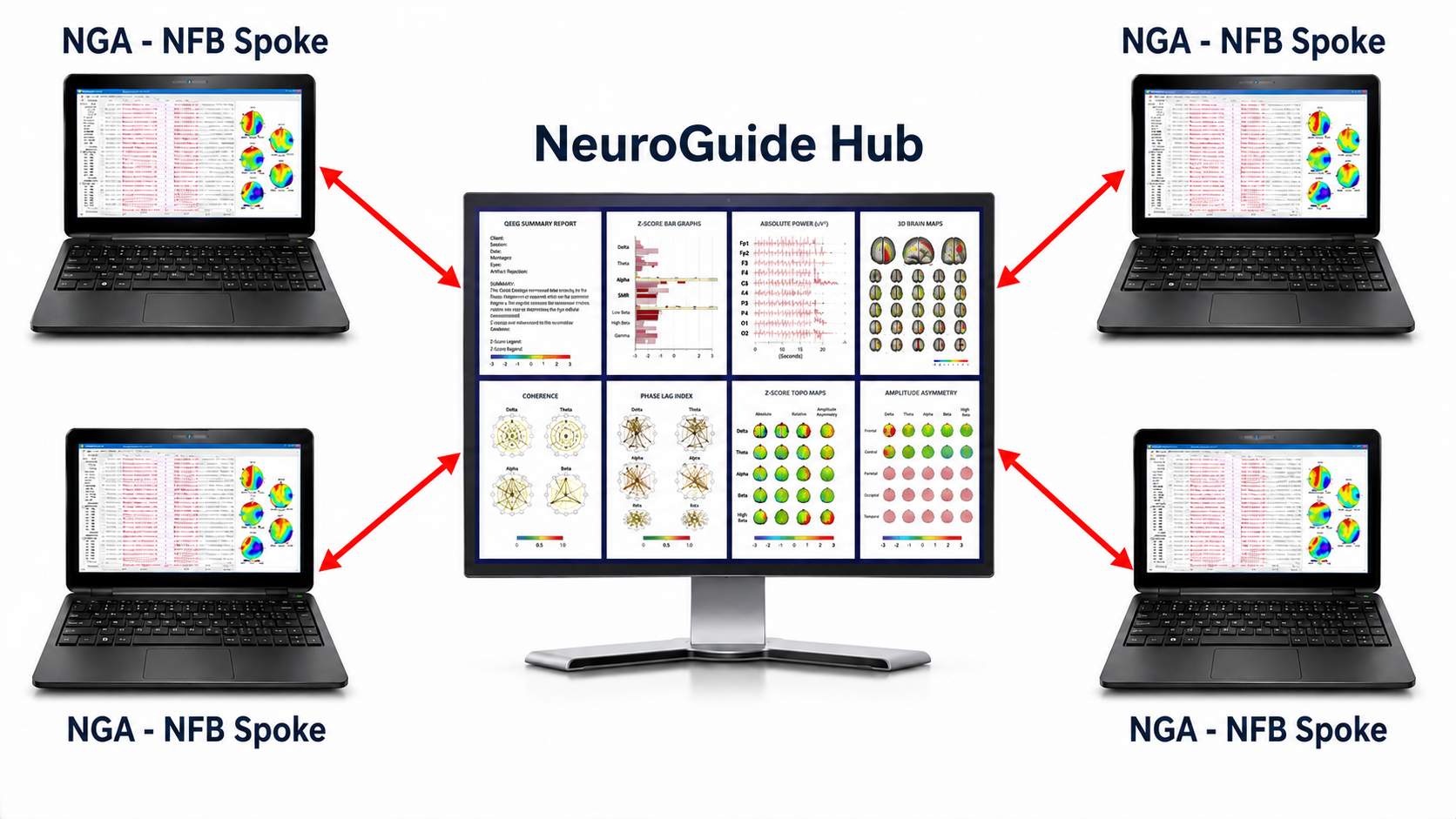
On the technical side, signal acquisition and processing, feedback delivery, and data collection all take place on the client's remote computer. Session data may be stored locally first and then uploaded or transmitted for inspection by the practitioner, who can then artifact the data, analyze metrics, and graph results for review with the client. Hardware requirements beyond a standard neurofeedback setup may include high-speed internet, a webcam, a computer microphone, or a phone line. Screen-sharing software is essential when the practitioner needs to adjust feedback settings or control the duration of sessions in real time.

Watch a BrainMaster Technologies Inc. YouTube video on remote/home training.
Remote neurofeedback is typically preceded by the same preliminary steps as in-clinic training, including obtaining consent and conducting an assessment. After a client responds positively to initial in-clinic sessions, the practitioner and client discuss the advantages and disadvantages of transitioning to remote training and develop a plan that specifies responsibilities, equipment needs, and costs. The client, and with consent a family member or other support person, particularly when the client is a child, then receives training in electrode placement and, where feasible, in operating the software independently. Regardless of the level of practitioner involvement during sessions, the practitioner reviews session data regularly, discusses results with the client, and adjusts the training protocol as needed.
Remote neurofeedback training uses electronic and communication technologies to deliver neurofeedback when clients and practitioners are in different locations. The practitioner may be present in real-time via screen sharing, available by phone, or may follow up at intervals. Signal acquisition, feedback, and data collection occur on the client's computer, with data transmitted to the practitioner for review. Remote training typically follows successful in-clinic sessions and requires planning for hardware, software, electrode placement training, and role responsibilities.
Research Review
This section examines the evidence base for remote training, beginning with peripheral biofeedback studies and then turning to the more limited neurofeedback literature. A growing number of providers are offering remote neurofeedback, with several training platforms currently available (e.g., BrainMaster, Myndlift, Versus). Published studies specifically on remote neurofeedback remain scarce, but peripheral biofeedback research demonstrates the feasibility and efficacy of remote delivery and highlights issues directly relevant to neurofeedback practitioners.
Remote Biofeedback
Among the earliest published accounts of telehealth-delivered biofeedback are two reports from the Tripler Army Medical Center program (Earles et al., 2001; Folen et al., 2001), which used remarkably low-tech equipment by today's standards, including telephone landlines and commercially available screen-control software. At the client's location, an assistant attached electrodes and sensors and then left once the practitioner established contact by videophone. Even with this low-bandwidth setup, the accompanying case illustrations indicated that remote training was feasible; neither report presents controlled outcome data. The authors noted that patient-provider rapport was satisfactory, although audio quality was a concern, a limitation that modern broadband has largely resolved.
Subsequent studies have strengthened the case for remote biofeedback across multiple modalities. Arena (2010), writing on future directions for surface EMG biofeedback, a modality that displays muscle action potentials detected by an electromyograph to the client, named telehealth as one of three areas the field must address if it is to keep flourishing, rather than as a settled result. Golebowicz et al. (2015) demonstrated similar feasibility with remote biofeedback for computer operators, though in a single-group study of 12 workers whose hypothesis was only partially supported: posture improved and pain fell in some body regions but not others. The authors noted its value for decreasing cost and improving treatment access while also illustrating how remote delivery allows biofeedback in the client's natural environment; training was practiced at the participants' own workstations.
Stetz et al. (2013) further described the use of virtual reality and telepsychology applications (apps), specialized programs downloaded onto mobile devices, for military clients in the Pacific Regional Medical Command. Reports from the same Tripler program describe its telehealth services as including clinician-instructed biofeedback and as integrating landlines, the plain old telephone service or POTS, for clients without higher-bandwidth access (Stetz et al., 2011).
Remote delivery has also proven effective for heart rate variability (HRV) biofeedback, which monitors the organized fluctuation of time intervals between successive heartbeats (known as interbeat intervals). Economides et al. (2020) found that adding remote HRV biofeedback to an app-based treatment for depression (Meru Health, n.d.) significantly increased the likelihood of clinically meaningful symptom improvement (adjusted odds ratio 3.44, 95% CI [1.28, 9.26]), while also demonstrating that client adherence could be tracked objectively. The design was quasi-experimental: 48 patients receiving the enhanced program were compared with 48 matched patients from historical outcome data. Davila et al. (2021) extended this work to 245 military reservists, guardsmen, veterans, and first responders, using a self-administered remote HRV biofeedback app that integrated reminders, incentives, psychological scales, paced-breathing exercises, and secure data sharing. Offline laboratory analysis of heart rate (HR), the number of beats per minute, validated the online measures, with the two data sets showing excellent agreement and confirming that the app collected reliable data for HRV biofeedback.
Schaefer et al. (2021) adapted biofeedback-assisted relaxation training (BART), the integration of biofeedback with relaxation procedures like autogenic training and progressive relaxation, for telehealth delivery to children. Rather than controlling the client's software remotely, clients used free-to-download apps while the clinician coached via a screen-sharing program. Setting their usual in-clinic BART against virtual BART (remotely self-administered BART), the authors reported, in a commentary rather than a controlled comparison, that the virtual format called for increased psychoeducation and more parental engagement, though it was important not to overload clients and parents with information. They also raised a concern with direct implications for neurofeedback: poorly investigated apps risk providing inaccurate feedback that may be ineffective, frustrating, or at worst worsen the client's condition.
Research on remote biofeedback demonstrates that telehealth-delivered training is feasible and effective across multiple modalities including EMG, HRV, and relaxation training. Early studies used low-bandwidth equipment successfully, and more recent work shows good client adherence and reliable data collection through apps. Most of this evidence comes from small, uncontrolled, or quasi-experimental studies rather than head-to-head trials, and app validation remains an important concern.
Remote Neurofeedback
Cortoos et al. (2010) conducted what its authors describe as the first tele-neurofeedback study, an exploratory single-blind trial that provided a critical proof of concept for the field. The researchers randomized 17 patients with primary insomnia, predominantly sleep-maintenance sufferers, to 20 home sessions of either remote EMG biofeedback at Fpz (n = 8) or remote neurofeedback (n = 9). The neurofeedback protocol focused on increasing sensorimotor rhythm (SMR), a 12–15 Hz spindle-shaped rhythm detected from the sensorimotor strip when individuals reduce attention to sensory input and decrease motor activity, while inhibiting theta (slow-wave activity, defined in this study as 4–8 Hz) and high beta (fast-wave activity associated with arousal, 20–30 Hz here) at Cz. Sleep latency improved in both groups, but only the neurofeedback group showed a significant increase in total sleep time on polysomnography and on its home sleep logs. The groups were small and there was no waiting-list control.
The largest test of remote neurofeedback to date is the European NEWROFEED trial, whose published protocol (Bioulac et al., 2019) set out a comparison of at-home neurofeedback training with long-acting methylphenidate in children with ADHD. The protocol used pre-installed software on a tablet computer connected to a medical-grade eight-electrode EEG amplifier. Children were assigned by baseline score to one of two protocols: down-training of the theta/beta ratio, the ratio between 4–7 Hz theta and 13–21 Hz beta, validated at the vertex, Cz (Monastra et al., 2001), averaged here over F3, Fz, F4, and Cz, or up-training of SMR over C3, Cz, and C4. The software guided the child and parent through setup, calibration, and training, using an algorithm to remove eyeblink artifacts in real time and defining EEG frequency bands, the number of complete cycles a signal completes per second, measured in hertz (Hz), based on individualized alpha peak frequency. Data synchronized automatically with a cloud server that clinicians reached through a secured web portal, and the at-home phase was preceded by up to four clinician-supervised discovery sessions that began and ended at the clinic.
The trial results, published subsequently, temper early enthusiasm: at-home neurofeedback did not demonstrate noninferiority to methylphenidate. The clinician-rated ADHD Rating Scale fell 26.7% in the neurofeedback arm against 46.9% in the medication arm, and the confidence interval around the roughly 8-point between-group difference exceeded the trial's 4.5-point noninferiority margin (Purper-Ouakil et al., 2022). Neurofeedback did match methylphenidate on sleep, on quantitative EEG measures, and on tolerability. The study nonetheless establishes that a personalized, protocol-driven neurofeedback program can be delivered in the home at scale, and it illustrates the level of technical and supervisory infrastructure that such delivery requires.
Despite the limited published literature, manufacturers such as BrainMaster, Myndlift, and Versus have begun offering hardware and software designed for remote delivery, and several well-regarded practitioners now provide workshops on the topic. As the remote biofeedback literature makes clear, several prominent issues need to be addressed through research, including how remote neurofeedback compares to in-clinic training in terms of efficacy, whether remotely collected data are sufficiently reliable, and which factors may compromise or ensure a good outcome.
Published experimental research on remote neurofeedback remains limited. A small exploratory randomized study of 17 patients found that home-based neurofeedback targeting SMR significantly improved total sleep time in insomnia patients. The larger NEWROFEED trial showed that tablet-based neurofeedback with cloud data synchronization is feasible at scale for children with ADHD, but did not establish noninferiority to stimulant medication. Manufacturers are developing platforms for remote delivery, and more research is needed on efficacy, data reliability, and outcome factors.
Considerations with Remote Training
Client-Related
This section examines the practical factors that determine whether a particular client is a good candidate for remote training, including advantages, potential barriers, and the resources required. Remote neurofeedback can increase the accessibility of training to a large number of clients in diverse settings, from rural communities with limited specialist access to military installations where travel to a civilian clinic is impractical. Travel time and associated costs are reduced, and events that might lead to canceling an in-office appointment may be more easily accommodated remotely. Remote delivery also reduces exposure to communicable diseases and may improve outcomes by delivering training in the situations where change is most needed, for example by helping an athlete train focus in their own performance environment.

Watch a Myndlift remote training instruction video on YouTube.
However, remote training is not appropriate for every client. Physical or cognitive challenges may impede the client's ability to carry out electrode placement and other steps needed for home-based sessions. Significant psychiatric disability can make remote training risky, particularly if the client is mentally vulnerable and lacks immediate access to support. With the client's consent, enlisting a family member, friend, or local health professional can help overcome ability-related barriers, but social and material resources may pose real constraints when no support person is available or when the additional expenses of remote equipment are prohibitive.
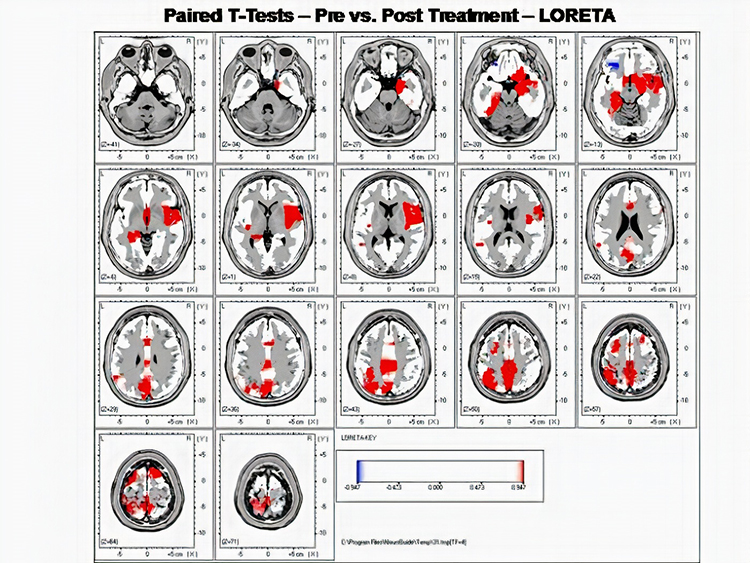
Several practical requirements must also be in place. The client needs a distraction-free, private space for training and secure storage for the equipment. A stable internet connection is essential whenever the practitioner must be present virtually. In cases requiring multiple electrode sites or LORETA neurofeedback, remote training may not be feasible, although new developments are making even LORETA-based approaches possible for clients with sufficient resources and abilities (Brainworks, n.d.). LORETA applies low resolution electromagnetic tomography, Pascual-Marqui et al.'s (1994) distributed inverse solution, which estimates a smoothly varying three-dimensional current density throughout the brain volume from multichannel scalp EEG.
Whether these issues apply will often depend on the characteristics of the individual client, and the practitioner should weigh them within an evidence-based framework. Key questions include: What are the details of the client's condition and goals? What does the scientific evidence say about remote training for this client's specific needs? Does the client have access to the necessary materials and internet services? And what is the client's own preference regarding remote versus in-clinic delivery?
Remote training offers significant advantages including increased accessibility, reduced travel costs, decreased infection exposure, and the ability to train in real-world environments. However, practitioners must carefully evaluate each client's physical and cognitive abilities, psychiatric stability, available support, technology access, and personal preferences before recommending remote training.
Financial
Financial planning is an essential step before beginning remote training. In cases where equipment is rented to clients, written agreements are recommended to specify rental fees and liability for damage, repair, or theft; how often session data must reach the clinician and how often in-office visits are required; that the device will be used only with the intended client; and immediate return if the clinician determines it is being used inappropriately or with people outside the original assessment (Hammond et al., 2011). For clients who wish to use insurance benefits, both the client and practitioner are well-advised to proactively investigate whether the insurance provider will reimburse for remote neurofeedback services.
Ethical and Legal
This section addresses the ethical codes, legal requirements, and privacy safeguards that govern remote neurofeedback delivery. Providers should be familiar with and follow the ethical codes and standards established for neurofeedback practice (Association for Applied Psychophysiology and Biofeedback, 2016; Biofeedback Certification International Alliance, 2026; International Society for Neuroregulation and Research, 2020). Licensed health professionals must practice according to all statutes, regulations, standards, and codes of ethics that apply both in their own location and in the location where the client is receiving remote training. This dual-jurisdiction requirement adds a layer of complexity not present in traditional in-clinic practice.

Competence is a recurring theme across ethical and practice standards. Providers should be competent not only in neurofeedback generally but also in the specific skills required for remote delivery (Hammond et al., 2011; Joint Task Force for the Development of Telepsychology Guidelines for Psychologists, 2013). Arena (2010) identifies several potential pitfalls for telehealth-delivered biofeedback, including privacy and confidentiality (a client's right to keep personal information private), use of support staff, licensing requirements in the client's jurisdiction, malpractice insurance coverage, and practitioner comfort level. Some clinicians may hold inter-jurisdictional practice certificates, and temporary waivers may be available under circumstances like the COVID-19 pandemic, but independent legal advice is recommended when there is ambiguity about providing cross-border services for formally diagnosed conditions.
Security and privacy of communications and data require careful attention before remote training begins. Confidentiality is less certain when sessions take place outside a clinical office, so the provider and client should plan how to ensure privacy and avoid interruptions during home-based training. Apps may share client data, and various regulatory bodies provide guidelines for managing privacy in telehealth that apply directly to remote neurofeedback (e.g., College of Psychologists of Ontario, 2021). Providers should understand how data is handled by any apps they recommend, discuss privacy issues in advance, and consider steps to verify the client's identity and anonymize data on the client's computer.
Informed consent deserves particular attention given the emerging nature of this field. Clients need to know that research on remote neurofeedback is limited, and as Schaefer et al. (2021) caution, some feedback software may have minimal research support and therefore pose risks that should be reviewed and consented to before training begins (cf. Cortoos et al., 2010). To prevent harm, practitioners should follow up regularly with clients to review progress and resolve problems, with a specific plan in place for managing difficulties. Risks for adverse consequences have led some authorities to state that "home training should never be done when a licensed professional is not supervising it" (Hammond et al., 2011, p. 55). Accordingly, Hammond et al. (2011) recommend using equipment that does not allow the remote trainer to change treatment protocols, which should be changed strictly by the neurofeedback professional.
Remote neurofeedback raises important financial, ethical, and legal considerations. Written rental agreements protect both parties when equipment is loaned. Practitioners must comply with ethical codes, licensing requirements in both their own and the client's jurisdiction, and privacy regulations. Informed consent must address the limited research base, and regular follow-up is essential to prevent harm.
Typical Course of Training
This section outlines the step-by-step sequence that remote neurofeedback typically follows, from initial assessment through ongoing monitoring. If the considerations discussed above suggest that remote training is appropriate, the practitioner will usually begin with an in-office assessment. Ideally, this is followed by a series of in-clinic sessions to confirm that the client responds well to training, an important safeguard that establishes a baseline for comparison once remote sessions begin. The client, and possibly a support person, then receives hands-on instruction in electrode placement, software operation, and any other procedures needed for home-based sessions, and the necessary equipment and materials are acquired.
Once remote training begins, the practitioner regularly reviews session data with the client to track progress and make decisions about next steps. The client may be asked to return to the office periodically for re-assessment and adjustment of training parameters. This ongoing feedback loop, connecting remote sessions to periodic in-person evaluation, helps ensure that training remains on target and that any emerging problems are caught early.
The typical course of remote training begins with in-office assessment and initial sessions, followed by training the client (and possibly a support person) in the procedures needed for home-based sessions. Equipment is acquired, and once remote training begins, the practitioner regularly reviews session data, tracks progress, and adjusts protocols as needed.
Summary and Conclusions
This unit has reviewed the expanding practice of remote neurofeedback training. Remote delivery presents several clear advantages, including broader access, reduced travel burden, and training in real-world environments, but it may not be feasible in every situation due to client characteristics, available resources, or regulatory constraints. Before offering remote training, practitioners must carefully evaluate ethical, legal, and financial issues, and the limited research base calls for caution when presenting it as an option to clients. Nevertheless, when the relevant issues can be addressed thoughtfully, remote neurofeedback can be a valuable addition to a practitioner's service options, extending the reach of evidence-based care to clients who might otherwise go unserved.

Remote neurofeedback training offers meaningful benefits for accessibility and convenience but requires careful attention to client suitability, ethical and legal compliance, financial arrangements, and the current limitations of the research base. With appropriate planning and precautions, remote training can be a valuable addition to a practitioner's service options.
Expanding Access Through Technology
The rapid development of consumer-grade EEG devices and cloud-based data platforms is making remote neurofeedback increasingly practical. Tablet-based systems with automated artifact rejection algorithms, individualized frequency band definitions, and secure cloud synchronization are enabling practitioners to monitor and guide training from a distance with greater confidence in data quality. As these technologies mature and receive more rigorous validation, remote neurofeedback may become a standard component of clinical practice rather than an alternative to it.
Lessons from the COVID-19 Pandemic
The COVID-19 pandemic accelerated telehealth adoption across all health disciplines, including neurofeedback. Temporary regulatory waivers and expanded insurance coverage for telehealth services provided a large-scale natural experiment in remote delivery. The lessons learned during this period, including effective protocols for remote electrode guidance, strategies for maintaining therapeutic rapport through video, and methods for ensuring data security, are now shaping best practices for remote neurofeedback going forward.
Check Your Understanding
- What are the key components of remote neurofeedback training, and how does it differ from in-clinic training?
- What does the research evidence from remote biofeedback studies suggest about the feasibility of remote neurofeedback?
- What client-related factors should a practitioner evaluate before recommending remote neurofeedback training?
- What ethical and legal considerations must practitioners address when offering remote neurofeedback across jurisdictions?
- Why is regular follow-up with clients particularly important during remote neurofeedback training?
Assignment
Now that you have completed this unit, summarize the most critical precautions required by remote neurofeedback training.
Glossary
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with relaxed wakefulness. Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
alpha-theta training: a protocol to slow the EEG to the 6-9 Hz crossover region while maintaining alertness.
amplitude: the strength of a signal, expressed for the EEG in microvolts (µV). Amplitude and power are not interchangeable: power is the square of amplitude and is expressed in µV² for the EEG and in ms² for heart rate variability.
application (app): a specialized program downloaded onto a mobile device.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in both the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
biofeedback-assisted relaxation training (BART): the integration of biofeedback with relaxation procedures like autogenic training and progressive relaxation.
confidentiality: a client's right to keep personal information private.
delta rhythm: 1-4-Hz oscillations generated by thalamocortical neurons during stage N3 sleep (formerly stages 3 and 4). Some sources start the band at 0.5 Hz; activity below about 1 Hz is treated in this curriculum as the slow cortical potential or infra-low range.
EEG activity: a single wave or series of waves.
EMG biofeedback: the display of muscle action potentials detected by an electromyograph to a client.
frequency: the number of complete cycles a waveform completes in one second, expressed in hertz (Hz).
gamma rhythm: EEG activity above about 30 Hz. Frequencies from 30-70 Hz are called low gamma, while those above 70 Hz represent high gamma. Because this curriculum extends beta to 38 Hz, the beta and gamma bands overlap, and scalp activity above about 30 Hz is vulnerable to EMG contamination.
heart rate (HR): the number of beats per minute.
heart rate variability (HRV): the organized fluctuation of time intervals between successive heartbeats defined as interbeat intervals.
hertz (Hz): the unit of frequency measured in cycles per second.
in-clinic BART: BART administered in a provider's office.
informed consent: a client's voluntary agreement to proceed with training, documented in writing after disclosure of the procedures, the expected benefits, the risks, the costs, the limits of confidentiality, and the alternatives. In remote training the disclosure also covers the limited research base, the equipment arrangements, and the plan for handling problems between sessions.
LORETA neurofeedback: neurofeedback that trains activity estimated by low resolution electromagnetic tomography (LORETA), Pascual-Marqui et al.'s (1994) distributed inverse solution, which estimates a smoothly varying three-dimensional current density throughout the brain volume from multichannel scalp EEG. Clinical neurofeedback commonly applies it to 19-channel 10-20 recordings, but the method is not restricted to any electrode count, and localization accuracy improves substantially with higher-density arrays.
noninferiority trial: a trial designed to test whether a new treatment is not worse than an established one by more than a pre-specified margin. Failing to demonstrate noninferiority means the margin was not excluded; it is not the same as demonstrating that the treatments are equivalent.
power: amplitude squared, expressed in microvolts squared (µV²) for the EEG and in milliseconds squared (ms²) for heart rate variability. Values in picowatts appear in some software only under the convention of a 1-ohm reference resistance, which must be stated whenever picowatts are used.
real time: as events occur.
remote HRV biofeedback: the delivery of heart rate variability biofeedback to a client who is in another physical location than the provider.
remote neurofeedback training: the use of electronic and communication technologies to deliver neurofeedback to clients in a different location than the neurofeedback practitioner.
sensorimotor rhythm (SMR): 12-15-Hz spindle-shaped rhythm, with a spectral peak usually around 12-14 Hz, detected over the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
telehealth: the delivery of health services using electronic and communication technologies when the provider and the client are in different locations.
theta/beta ratio: the ratio between 4-7 Hz theta and 13-21 Hz beta, measured at the vertex (Cz) in the studies that validated it (Monastra et al., 2001).
theta rhythm: 4-7-Hz rhythms generated by a cholinergic septohippocampal system that receives input from the ascending reticular formation and a noncholinergic system that originates in the entorhinal cortex, which corresponds to Brodmann areas 28 and 34 at the caudal region of the temporal lobe.
virtual BART: remotely self-administered BART.
References
Arena, J. G. (2010). Future directions in surface electromyography. Biofeedback, 38(2), 78–82. https://doi.org/10.5298/1081-5937-38.2.78
Association for Applied Psychophysiology and Biofeedback. (2016). Code of ethics. https://aapb.org/Code_of_Ethics
Biofeedback Certification International Alliance. (2026). Professional standards and ethical principles of biofeedback (10th rev.). https://bcia.memberclicks.net/assets/docs/ProfessionalStandardsAndEthicalPrinciplesofBiofeedback.pdf
Bioulac, S., Purper-Ouakil, D., Ros, T., Blasco-Fontecilla, H., Prats, M., Mayaud, L., & Brandeis, D. (2019). Personalized at-home neurofeedback compared with long-acting methylphenidate in an European non-inferiority randomized trial in children with ADHD. BMC Psychiatry, 19(1), Article 237. https://doi.org/10.1186/s12888-019-2218-0
BrainMaster Technologies. (2020, September 3). BrainMaster Technologies, Inc. – Telehealth (remote/home training) [Video]. YouTube. https://www.youtube.com/watch?v=GFct171tAb0
BrainMaster Technologies. (n.d.). Training your brain at home: BrainMaster telehealth. Retrieved July 25, 2026, from https://brainmaster.com/tele-health/
Brainworks. (n.d.). For therapists. Home Neurofeedback. Retrieved July 25, 2026, from https://homeneurofeedback.com/fortherapists/
College of Psychologists of Ontario. (2021, April 30). Virtual health care – Enhanced privacy practices for services provided electronically. https://cpbao.ca/virtual-health-care-enhanced-privacy-practices-for-services-provided-electronically-april-2021
Cortoos, A., De Valck, E., Arns, M., Breteler, M. H. M., & Cluydts, R. (2010). An exploratory study on the effects of tele-neurofeedback and tele-biofeedback on objective and subjective sleep in patients with primary insomnia. Applied Psychophysiology and Biofeedback, 35(2), 125–134. https://doi.org/10.1007/s10484-009-9116-z
Davila, M. I., Kizakevich, P. N., Eckhoff, R., Morgan, J., Meleth, S., Ramirez, D., Morgan, T., Strange, L. B., Lane, M., Weimer, B., Lewis, A., Lewis, G. F., & Hourani, L. I. (2021). Use of mobile technology paired with heart rate monitor to remotely quantify behavioral health markers among military reservists and first responders. Military Medicine, 186(Suppl. 1), 17–24. https://doi.org/10.1093/milmed/usaa395
Earles, J. E., Folen, R. A., & James, L. C. (2001). Biofeedback using telemedicine: Clinical applications and case illustrations. Behavioral Medicine, 27(2), 77–82. https://doi.org/10.1080/08964280109595774
Economides, M., Lehrer, P., Ranta, K., Nazander, A., Hilgert, O., Raevuori, A., Gevirtz, R., Khazan, I., & Forman-Hoffman, V. L. (2020). Feasibility and efficacy of the addition of heart rate variability biofeedback to a remote digital health intervention for depression. Applied Psychophysiology and Biofeedback, 45(2), 75–86. https://doi.org/10.1007/s10484-020-09458-z
Folen, R. A., James, L. C., Earles, J. E., & Andrasik, F. (2001). Biofeedback via telehealth: A new frontier for applied psychophysiology. Applied Psychophysiology and Biofeedback, 26(3), 195–204. https://doi.org/10.1023/A:1011346103638
Golebowicz, M., Levanon, Y., Palti, R., & Ratzon, N. Z. (2015). Efficacy of a telerehabilitation intervention programme using biofeedback among computer operators. Ergonomics, 58(5), 791–802. https://doi.org/10.1080/00140139.2014.982210
Hammond, D. C., Bodenhamer-Davis, G., Gluck, G., Stokes, D., Harper, S. H., Trudeau, D., MacDonald, M., Lunt, J., & Kirk, L. (2011). Standards of practice for neurofeedback and neurotherapy: A position paper of the International Society for Neurofeedback and Research. Journal of Neurotherapy, 15(1), 54–64. https://doi.org/10.1080/10874208.2010.545760
International Society for Neuroregulation and Research. (2020). ISNR code of ethics. https://isnr.org/interested-professionals/isnr-code-of-ethics
Joint Task Force for the Development of Telepsychology Guidelines for Psychologists. (2013). Guidelines for the practice of telepsychology. American Psychologist, 68(9), 791–800. https://doi.org/10.1037/a0035001
Meru Health. (n.d.). Provider referrals. Retrieved July 25, 2026, from https://www.meruhealth.com/provider
Monastra, V. J., Lubar, J. F., & Linden, M. (2001). The development of a quantitative electroencephalographic scanning process for attention deficit-hyperactivity disorder: Reliability and validity studies. Neuropsychology, 15(1), 136–144. https://doi.org/10.1037/0894-4105.15.1.136
Myndlift. (n.d.). Myndlift: Better brain with therapist-guided home neurofeedback. Retrieved July 25, 2026, from https://www.myndlift.com/
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49–65. https://doi.org/10.1016/0167-8760(84)90014-X
Purper-Ouakil, D., Blasco-Fontecilla, H., Ros, T., Acquaviva, E., Banaschewski, T., Baumeister, S., Bousquet, E., Bussalb, A., Delhaye, M., Delorme, R., Drechsler, R., Goujon, A., Häge, A., Kaiser, A., Mayaud, L., Mechler, K., Menache, C., Revol, O., Tagwerker, F., . . . Brandeis, D. (2022). Personalized at-home neurofeedback compared to long-acting methylphenidate in children with ADHD: NEWROFEED, a European randomized noninferiority trial. Journal of Child Psychology and Psychiatry, 63(2), 187–198. https://doi.org/10.1111/jcpp.13462
Schaefer, M., Iskander, J., Tams, S., & Butz, C. (2021). Offering biofeedback assisted relaxation training in a virtual world: Considerations and future directions. Clinical Practice in Pediatric Psychology, 9(4), 405–411. https://doi.org/10.1037/cpp0000391
Stetz, M. C., Folen, R. A., & Yamanuha, B. K. (2011). Technology complementing military behavioral health efforts at Tripler Army Medical Center. Journal of Clinical Psychology in Medical Settings, 18(2), 188–195. https://doi.org/10.1007/s10880-011-9246-3
Stetz, M. C., Folen, R. A., Van Horn, S., Ruseborn, D., & Samuel, K. M. (2013). Technology complementing military psychology programs and services in the Pacific Regional Medical Command. Psychological Services, 10(3), 283–288. https://doi.org/10.1037/a0027896
Versus. (n.d.). Mobile brain sensing. Neuro Management. Retrieved July 25, 2026, from https://getversus.com/
Return to Top