Procedures and Mechanics of Conducting a Neurofeedback Session
What You Will Learn in This Chapter
This unit guides you through the hands-on, session-by-session procedures that neurofeedback practitioners follow when delivering training. You will learn how to prepare for each session, check in with your client, obtain clean EEG recordings, select appropriate electrode montages, set and adjust thresholds, and monitor client progress throughout the training process.
You will also explore the learning processes that make neurofeedback work, from operant reinforcement and classical conditioning to metacognition and mindfulness, along with the filters, caps, and placement procedures that determine whether the signal you train is trustworthy in the first place.
Finally, you will examine the critical elements of effective training, including readiness, repetition, reinforcement, and shaping, as well as medication effects on the EEG, contraindications for training, adverse effects, and how to interpret session graphs for data-driven decision-making.
BCIA Blueprint Coverage: This unit addresses VIII. Treatment Implementation - C. Procedures and Mechanics of Conducting a Neurofeedback Session.
Learning Objectives
After completing this section, you will be able to:
Describe how to monitor client reaction to treatment using pre-session questionnaires and self-report measures.
Explain the steps required to obtain clean EEG data, including proper electrode attachment, impedance testing, and artifact elimination.
Select appropriate electrode montages and explain the consequences of each montage option.
Explain how filter type, filter order, and latency affect the quality and timing of feedback, and describe the landmarking and cap placement procedures that make qEEG data reproducible.
Distinguish frequency, amplitude, absolute power, and relative power, and explain why relative power must be interpreted alongside absolute power.
Set and adjust thresholds for amplitude training using fixed, ratio, z-score, and dynamic methods.
Describe the learning processes underlying neurofeedback, including operant reinforcement, classical conditioning, generalization, metacognition, and mindfulness.
Identify the critical elements in neurofeedback training, including readiness, repetition, reinforcement, and shaping.
Monitor client progress by identifying drowsiness, revising protocols, managing medication issues, identifying contraindications and adverse reactions, and reading session reports and graphs.
Overview
This section covers the typical procedures practitioners follow when conducting individual neurofeedback sessions, drawing extensively from the work of Demos (2019), Soutar and Longo (2020), and Thompson and Thompson (2015). Whether you work in a VA medical center, a hospital neurology department, or a private clinic, these foundational procedures apply across settings.
EEG equipment literacy is essential. Practitioners must know how to measure the scalp, identify International 10-20 System sites, and attach electrodes properly. They also need to recognize what a normal raw EEG looks like, gain hands-on experience producing and controlling artifacts so that measurements and brain maps are valid, and learn to distinguish abnormal EEG waveforms from benign activity.
Clinicians monitor EEG activity using the classical International 10-20 System for standardized electrode placement, or the modified "10-10" system known as the Modified Combinatorial Nomenclature System. They often record from several sites and measure the amplitude of EEG signals within frequency bands (such as alpha and theta) to build a complete picture of brain activity. Software-based montage reformatting then allows clinicians to reanalyze session data by referencing an electrode to other sites or combinations of sites, enabling the computation of multiple variables associated with communication and network functions within the central nervous system (CNS).
The Quantitative EEG (qEEG), the digitized statistical analysis of the EEG, measures amplitude or power within selected frequency bands and compares the result against a normative database. Topographic brain mapping typically uses 19 or more channels, but abbreviated and single-channel applications exist. A full-cap 21-channel recording (19 scalp sensors plus two reference sensors) and the resulting qEEG analysis can be particularly valuable when designing treatment protocols for complex presentations such as autism spectrum disorder, which absorbed the former Asperger's disorder diagnosis in DSM-5, or traumatic brain injury. EEG topography displays these data on a cortical surface map to reveal the spatial distribution of brain activity.
However, contamination by physiological and exogenous artifacts requires extensive precautions, careful inspection of the raw EEG record, and the removal of contaminated epochs through a process called artifacting. Impedance tests and behavioral tests help ensure the fidelity of EEG recording. Finally, clinicians must interpret EEG recordings with an understanding of how normal values are affected by eye closure, age, diurnal influences, alertness and drowsiness, medication, and relaxation.
This unit reviews: 1. Monitoring client reaction to treatment (e.g., use of pre-session questionnaires), 2. Selecting electrode montages and obtaining a clean signal, 3. Reading the EEG in terms of frequency, amplitude, and power, 4. Setting and adjusting thresholds for amplitude training, 5. The learning processes that drive neurofeedback, 6. Critical elements in neurofeedback training, and 7. Monitoring client progress (e.g., identifying drowsiness, revising protocols and moving to new sites, medication issues, identifying contraindications to treatment and adverse reactions, reading/interpreting session reports/graphs).

Monitoring Client Reaction to Treatment
This section covers the pre-session review process, client check-in procedures, and the integration of quantitative data into session planning. Effective monitoring before a session begins sets the stage for productive training and informed decision-making.
Before a session, the practitioner should review information from previous sessions, including training goals, self-report graphs, questionnaire data, and EEG results. Constructing and updating these graphs as soon as possible after each session ensures the data are ready for review. While self-report rating scales can usually be graphed in a straightforward manner, questionnaires often require converting raw responses to norm-based results, and EEG data from the previous session may need to be artifacted before calculating parameters such as mean amplitude or coherence.
In some cases, clients forward self-report scales and questionnaires electronically between sessions or complete them online. In other cases, the client brings these measures to the session or completes them upon arrival. Depending on the situation, the practitioner may want to schedule time before training to score and review these data. The practitioner should also consider how consistent the results are with the hypothesis that training will lead to problem resolution or goal achievement, a consideration that prepares them to discuss continuing with the current montage, making changes to the training regimen, or concluding training.
A session preparation form can be invaluable for guiding each appointment. Before the session, the form can document the montage(s) to use, findings to review, and questions to ask. During the session, the practitioner records responses and pertinent information.
Updated graphs, printed or electronic, serve as a vehicle for engaging the client in discussion about progress or problem-solving. In-person sessions also require good hygiene and infection control: hands washed, surfaces disinfected, and electrodes cleaned. Equipment and materials should be arranged for efficient access, including the computer, monitor, speakers, EEG amplifier, electrodes, gel, paste, alcohol, cotton balls, and facial tissue.
Client Check-In
Self-report
Though it may seem a small matter, greeting the client attentively and setting them at ease is important at the outset of each session. A natural opening, asking how they are generally, invites more specific inquiry and self-disclosure. Direct behavioral observation with follow-up inquiry can also begin at this point.
The practitioner should assess the client's current state, asking how they are that day and following up about any changes to their health and circumstances. Practitioners should also inquire about training effects following the previous session, progressing from general open-ended questions to more specific closed-ended questions about emotional, cognitive, somatic, and behavioral changes the client noticed in the hours and days after training. Asking about the particular situations in which those changes occurred adds clinical richness.
Changes can be contrasted with the client's condition before training began, and connections can be drawn between the previous week's experiences and in-session neurofeedback training. The practitioner should also follow up on homework practice and use of ancillary devices, reinforcing the link between in-clinic gains and everyday life.
Review of quantitative data
Following the client's subjective self-report, the practitioner reviews any self-monitoring scales or questionnaires completed before the session. The key question is how these quantitative data compare to pre-training assessment benchmarks and the client's verbal self-report about their current state and response to training.
The practitioner can then review EEG results with the client, focusing on metrics that are training targets and that fall outside normal expectations. This review also provides a natural opportunity for client education about brain-behavior relationships: how their brain is changing with neurofeedback training and what they can expect from those changes. Presenting self-reported ratings, questionnaires, and EEG data in graphs makes these trends tangible and promotes client engagement.
Before transitioning to neurofeedback training, it is wise to ask whether the client has any further questions or comments about their progress before asking if they are ready to proceed with that day's session.
Key Takeaways
Before each session, review previous session data and prepare graphs to track progress. During client check-in, assess the client's current state, inquire about post-training effects, and review quantitative data from self-monitoring scales and EEG results. A session preparation form helps organize montage plans, findings, and questions for each appointment.
Selecting Appropriate Electrode Montages
This section covers how montage selection shapes what the EEG recording reveals, including the key differences between referential and sequential montages. Choosing the right montage is a clinical decision that directly affects the quality of your assessment and the precision of your training.
Additional EEG channels sample more of the scalp, and multi-channel assessment yields metrics that a single channel cannot produce. The evidence on how many channels are needed is more nuanced than it is usually reported. Lau et al. (2012) decimated 256-channel recordings and concluded that "an EEG montage with as few as 35 channels may be sufficient to record the two most dominate electrocortical sources," with recovery of the less dominant sources degrading as channels were removed. That study examined signal recovery during standing and walking, not clinical or performance outcomes, so it cannot be cited for either.
Although some practitioners still conduct assessment and training with a single channel, multi-channel methods have become increasingly accessible. The cost of a full 19-channel EEG assessment has decreased substantially, and such assessments can provide not only EEG amplitude data from all 10-20 sites but also metrics like coherence and phase that reveal how well different brain regions communicate with each other. These data are especially beneficial for complex symptom profiles such as Autism Spectrum Disorders, epilepsy, and traumatic brain injury (Thompson & Thompson, 2015).
A channel is an EEG amplifier output resulting from scalp electrical activity detected by three electrode connections. These are commonly known as active, reference, and ground electrodes, though more precisely they are called positive (+), negative (-), and reference. An active or positive electrode is placed over a known EEG generator like Cz. A reference or negative electrode may be located on the scalp, earlobe, or mastoid. A ground/reference electrode may also be placed on an earlobe or mastoid (Thompson & Thompson, 2015).
Active and reference sensors are identical balanced inputs and are technically interchangeable, though some neurofeedback systems require designating a specific sensor as the "reference," as in a linked-ears configuration. One clarification is worth carrying forward: the ground is shared across all channels rather than being a component of any single one. It supplies the amplifier's input stage with a common voltage reference and thereby enables common-mode rejection, which the differential amplifier itself performs.
A derivation is the assignment of two electrodes to an amplifier's inputs 1 and 2. For example, Fp1 to O2 means Fp1 is placed in input 1 and O2 in input 2. A montage groups electrodes together (combines derivations) to record EEG activity (Thomas, 2007). All montages compare EEG activity between one or more pairs of electrode sites. Modern amplifiers record all input sensors in reference to a common sensor (often Cz), and all montage changes are performed in software; amplifiers no longer require manual switching of electrodes between inputs.
The narrated video below © John S. Anderson displays the same 21-channel recording viewed using different montages with a 60-Hz notch filter on and off.
Please review the Signal Acquisition unit in Neurofeedback Tutor: An Introduction to review montage options and their consequences.
Obtaining a Clean Signal: Filters, Caps, and Placement
Choosing a montage decides which comparison you record. This section covers what happens to that comparison next: the signal-processing and sensor-application choices that determine whether the feedback your client receives actually reflects their brain. Anderson and Davis (2025a) describe modern neurofeedback as resting on two foundations: signal fidelity, meaning the reliable measurement of microvolt-level cortical rhythms, and learning theory, meaning the reinforcement processes that help people reproduce useful brain states. The most elegant protocol cannot rescue a recording contaminated by a gel bridge or a feedback signal that arrives too late to teach anything.
What Filters Do
Filters exclude waveforms of relatively high or low frequency so that activity in the most clinically important range, roughly 1 to 30 Hz, can be recorded clearly and without distortion (Fisch, 1999). Four filter types do most of the work in neurofeedback. A high-pass filter allows frequencies above its cutoff point, such as 1 or 2 Hz, to pass through. A low-pass filter allows frequencies below its cutoff, such as 30 Hz or higher, to pass through.
A notch filter blocks a narrow band around 60 Hz, or 50 Hz outside North America, to keep power line interference out of the EEG. A band-pass filter lets you select a specific frequency range, for instance 4 to 7 Hz, in order to define and measure a particular EEG band. Remember throughout that filters only attenuate frequencies outside their boundaries. They never eliminate them.
FIR, IIR, and FFT: Three Ways to Compute a Band
When a signal requires more processing, digital filters convert it from an analog, time-based format to a digital, frequency-based one. Three approaches dominate. A finite impulse response (FIR) filter acts like a weighted moving average, is always stable, and delays all frequencies equally, which preserves waveform shape. That linear phase response makes FIR filters ideal when timing matters, as in event-related potential work, at the cost of higher computational demand and longer latency.
An infinite impulse response (IIR) filter feeds part of its output back into its input, which achieves sharp cutoffs with far fewer calculations. The trade-off is nonlinear phase distortion, because different frequencies are shifted by slightly different amounts in time. For most neurofeedback applications, where the focus is band amplitude rather than precise waveform alignment, IIR filters are preferred because they minimize delay and keep feedback as nearly instantaneous as possible (Anderson & Davis, 2025a).
The fast Fourier transform (FFT) is not a filter design at all but a mathematical algorithm that decomposes a time-domain signal into its frequency components. FFT processing is widely used to estimate spectral power in near real time, and its window length governs the trade-off between speed and frequency resolution. The catch is that a Fourier calculation needs at least 1 second of data, and most implementations use 2 seconds or more for precision. Sliding windows, which overlap successive snapshots of data, do not repeal that requirement no matter how often the window recalculates.
That delay makes FFT better suited to offline data processing and database comparisons than to real-time training. The one partial exception is training slow frequencies below approximately 10 Hz, where the slower response may be acceptable although still not ideal (Anderson & Davis, 2025a). When you use digital filters for several frequencies at once, keep them all of the same type. The practical exception is displaying an FFT-derived theta/beta ratio for information while third-order IIR filters drive the actual reward and inhibit feedback.
Filter Order and the Precision-Speed Trade-Off
The precision with which IIR and FIR filters measure a frequency is set by their filter order, which is simply the number of samples used to calculate the output. Samples come from the amplifier's sampling rate, the number of times per second the amplifier measures the incoming signal. A higher-order filter uses more samples and therefore measures more precisely, but it is also slower to produce an output.
Consider a typical third-order IIR filter running on an amplifier that samples at 256 samples per second. It delivers an output to the display in about 11 milliseconds, which is fast enough that changes on the screen closely mirror the brain-based behavior being measured (Anderson & Davis, 2025a). When you process a recording offline, where real-time feedback is not required, a higher-order filter buys you greater precision at no clinical cost. Whatever you choose, use the same filter type and parameters across sessions so that any change you observe reflects the brain rather than the mathematics. Collura (2014) provides a fuller technical treatment for readers who want the underlying mathematics.
Phase Distortion and Latency
Phase distortion occurs when a filter delays different frequencies by unequal amounts, subtly shifting parts of the EEG waveform in time and altering the true timing relationship among components of the signal. Latency refers to the total delay between when brain activity occurs and when feedback about it reaches the client. Both matter because learning depends on the brain recognizing a clear, immediate link between its own activity and the feedback it receives.
Excessive phase distortion can misrepresent which brain events are being rewarded, and prolonged latency weakens the sense of cause and effect that drives operant learning. Ideally, filters and processing pipelines keep total delay short enough, usually under 250 milliseconds, for feedback to feel instantaneous (Anderson & Davis, 2025a; Fisch, 1999). You will recognize that number from the reinforcement literature discussed later in this unit, where Sherlin et al. (2011, p. 297) recommend that feedback latency "should not exceed 250 to 350 ms" while noting that "there is no fixed rule on what is the minimum or maximum acceptable delay." Treat the range as a practical engineering ceiling rather than a measured optimum.
Key Concept
Filter choice is a clinical decision, not a technical footnote. An 11-millisecond third-order IIR filter preserves the contiguity between a brain event and its reward, while a 2-second FFT window does not. When you select a filter, you are deciding how tightly your client's brain can link what it just did to what it just heard or saw.
Placing a qEEG Cap Accurately
Correct qEEG begins long before you press record. Measure head circumference just above the ears and choose a cap size that is snug without being constrictive. Ask clients to arrive with hair that is clean, dry, and free of heavy product, remove metal clips and accessories, and seat the client comfortably with head support. Parting dense hair along the anticipated electrode sites improves scalp contact and reduces movement and muscle artifact (Anderson & Davis, 2025a; Fisch, 1999).
Stabilize the cap using whatever mechanisms it provides, such as chin straps or perimeter tensioners. Chest anchor straps are not recommended, because respiration tugs on them and creates movement artifacts. With clients whose hair is dense, curly, or springy, the hair will hold cap electrodes away from the scalp no matter how carefully you prepare the site, and injected gel must form a column that connects the electrode to the skin.
Next, establish the cranial landmarks that anchor all proportional placement. With a flexible tape, locate and lightly mark the nasion at the bridge of the nose, the inion at the external occipital protuberance, and the left and right preauricular notches just anterior to the tragus. Measure the nasion to inion arc along the midline and the ear to ear arc over the vertex. Their 50% points intersect at Cz, the keystone of the montage.
Place the cap so its midline aligns precisely with the nasion, Cz, and inion line and its lateral markers align with the preauricular notches. Verify that Cz on the cap matches the intersection you actually measured rather than trusting a printed cap logo (Acharya et al., 2016; Jasper, 1958). Then monitor symmetry: left and right distances from the midline should match, and anterior to posterior distances should maintain the intended ratios. Small errors at Cz propagate across the entire scalp, so re-measure whenever the two halves of the nasion to inion or the left to right preauricular arcs are unequal.
With Cz verified, the remaining electrodes fall at 10% or 20% intervals along those arcs, yielding the canonical 19-channel set. Note the modern nomenclature, in which T7 and T8 replace the historical T3 and T4, and P7 and P8 replace T5 and T6 (Acharya et al., 2016). The 10-10 and 5% systems, introduced in the overview as the Modified Combinatorial Nomenclature System, apply the same proportional logic at finer increments, improving topographic resolution while preserving cross-session reproducibility.
Site Preparation and Impedance Control
Prepare each site for stable contact. With gel caps, gently reduce impedance at the stratum corneum, the upper layer of the skin, using a mild abrasive through the grommet, then introduce conductive gel until the electrode makes firm contact with skin rather than hair. Once the cap is secure, avoid pressing down on it or on individual electrodes as they are filled. Pressure compresses the gel column, which can then be disrupted when the electrode springs back, and it raises the chance of forming a gel bridge to a neighboring sensor.
A gel bridge is the cap-based form of the bridging artifact described in the glossary, and it short-circuits channels and distorts topography. There is no way to repair one once it has occurred. The cap must come off, the client must wash and completely dry their hair, and a fresh, clean, dry cap must be applied. Overfilling the gel column is the most common cause, so err on the side of less gel.
A saline net presents a related hazard. Its pads or sponges must contact the scalp, which often requires significant pressure with very dense hair, yet over-wetting produces salt bridging between adjacent sensors. Fortunately, a salt bridge is recoverable: remove the net, dry the scalp and hair with a hair dryer, have the client brush the hair well to remove loose mineral salts, and place a freshly hydrated net on the dry scalp. Aim for low and balanced impedances, commonly 5 to 10 kOhms depending on your amplifier, and recheck after a few minutes to catch drift as the gel settles (Fisch, 1999). Careful site preparation serves two ends at once, since scalp abrasion technique affects both data quality and infection risk (Ferree et al., 2001), and unbalanced impedances across channels degrade the statistical sensitivity of the recording even when the raw trace looks acceptable (Kappenman & Luck, 2010).
Dry electrode caps take a different approach, using small rounded points around or across each sensor to reach the scalp through dense hair. They are effective contacts and fast to apply, but they often suffer from cardioballistic (pulse) artifact, particularly at the F3 and F4 locations. Knowing that tendency in advance keeps you from mistaking a pulse-locked deflection for a frontal EEG finding.
Reference, Ground, and Auxiliary Channels
Choose a reference and ground consistent with your amplifier and your analysis plan. Linked mastoids, the nose, and an average reference are all common choices. Whichever you adopt, keep the reference quiet by placing it away from muscle hotspots, and use the same scheme across sessions to protect longitudinal comparability, particularly if you plan qEEG database comparisons.
Add auxiliary channels whenever your system allows. Electro-oculography (EOG) sensors near the canthi or the inferior orbit track eye movements, and optional frontalis or masseter EMG channels capture muscle activity, so that you can identify and manage these artifacts during review rather than guessing about them later (Acharya et al., 2016; Fisch, 1999).
Functional Checks, Noise Control, and Documentation
Before recording in earnest, run rapid functional checks. A brief eyes-closed segment should increase occipital alpha at O1 and O2 relative to eyes-open. Marked asymmetries, unusually low alpha, or isolated band spikes confined to one site usually indicate a local placement, contact, or cable problem rather than a clinical finding. Inspect for drying gel, hair trapped under the cup, cable tension, and cap drift whenever a pattern looks implausible.
Manage the environment before you reach for filtering. Route the cable bundle down the client's back with strain relief, keep power supplies and transformers away from the head and leads, and reserve notch filtering for last, since placement, cabling, and environmental control are your first-line noise solutions (Fisch, 1999). Then document everything needed for reproducibility: cap size, sampling rate, filter settings, reference and ground scheme, per-channel impedances, and any deviation such as moving a site to avoid a scar. Replicating the same measurement protocol at every session is what stabilizes spectral features and topography over a course of training.
Clinical Application
Maria arrives for her fourth qEEG-guided session with damp hair after a rushed morning. You seat her, prepare the sites, and notice during your eyes-closed check that alpha at O1 barely rises while O2 responds normally. Rather than recording and explaining the asymmetry as a finding, you inspect the site, discover hair trapped under the cup, re-prepare it, and watch the asymmetry disappear. Five minutes of checking just prevented a spurious occipital asymmetry from entering her record and shaping her protocol.
Key Takeaways
Neurofeedback depends on clean signals and fast, faithful processing. High-pass, low-pass, notch, and band-pass filters shape what you measure, while the choice among FIR, IIR, and FFT methods, along with filter order and sampling rate, governs both accuracy and delay. IIR filters dominate real-time training because they minimize latency, and FFT calculations need at least 1 second of data, which is too slow for most feedback. Precise 10-20 and 10-10 placement anchored to cranial landmarks, careful gel or saline management, quiet referencing, and thorough documentation are what convert a cap full of sensors into reliable, comparable brain data.
Check Your Understanding
- Why are IIR filters generally preferred over FFT-based processing for real-time neurofeedback, and what is the one partial exception?
- What does filter order control, and what is the trade-off involved in raising it?
- Describe the steps you would take to verify that Cz on an EEG cap is correctly positioned on a particular client.
- Compare a gel bridge and a salt bridge. Which one can be corrected without removing and re-applying the sensor array, and how?
- Your eyes-closed functional check shows almost no alpha at a single posterior site. What should you check before interpreting this as a clinical finding?
Reading the Signal: Frequency, Amplitude, and Power
This section covers the vocabulary you will use every time you set a threshold, read an assessment report, or explain a brain map to a client. Anderson (2025) observed that many practitioners find these concepts confusing in day-to-day work, largely because the field uses so many overlapping terms for the same measurements. Getting them straight protects you from a specific and consequential clinical error described at the end of this section.
Frequency and Amplitude
Frequency means how often a wave occurs within 1 second, that is, the number of waves per second. This value was once called cycles per second and is now known as hertz or Hz. One simple way to determine frequency is the zero-crossing method: count the number of times the wave crosses the zero line within a 1-second segment and divide by 2. Counting the peaks above the zero line during that same second gives you the same answer.
Amplitude is the strength of the EEG signal, measured in microvolts (μV). Amplitude and power are different quantities and do not share a unit: power is amplitude squared and is expressed in μV², as the next section explains. When you view a filtered 8 to 12 Hz trace, the alpha activity looks reassuringly sinusoidal because everything else has been removed. Look at the raw signal from the same recording and that clean wave becomes hard to pick out among all the other frequencies occurring simultaneously. This is precisely why we separate frequencies from each other, and it is also why you should always check the scale on the vertical and horizontal axes before drawing conclusions from a display.
What an FFT Display Shows and Hides
An FFT converts the raw EEG into frequency and magnitude, which is amplitude over time, displaying how much activity occurs at each frequency along the horizontal axis. Collections of single frequencies form the familiar bands of delta at 1 to 4 Hz, theta at 4 to 7 Hz, alpha at 8 to 12 Hz, SMR at 12 to 15 Hz, low beta at 15 to 22 Hz, middle beta at 22 to 36 Hz, and high beta at 36 to 45 Hz, though these designations vary somewhat among systems. The display makes it easy to see at a glance how much activity occupies each band and where the peak frequency falls within a band.
That clarity comes at a price. Once the data are processed, you cannot tell how much of the displayed activity is artifact from eye movement or muscle. Eye movement and blinking produce electrical discharges in the delta and low theta range that are not cerebral in origin yet are plotted into the EEG graph as though they were. An FFT also represents a composite of its calculation window, typically 2 seconds, so the moment-by-moment information visible in the raw display is lost. That averaging becomes an advantage when you use windows of several minutes to build normative databases and topographic maps.
To summarize, frequency means how frequently the wave occurs within 1 second, and amplitude means the amount of electrical activity within that frequency band during that period.
Power, Relative Power, and a Costly Trap
Power means amplitude squared. Squaring serves two purposes. First, because the EEG constantly fluctuates above and below the zero line, averaging raw values over time would produce numbers near zero, whereas squared values are always positive and therefore support means, maxima, minima, and standard deviations. Second, squaring exaggerates differences between bands, so a theta/beta ratio of 4 to 2 becomes a more visually distinct 16 to 4.
Relative power, also called percent power or normalized EEG, converts absolute power values into percentages of the power in the entire recorded band. If the whole 1 to 45 Hz band has a power value of 100 and the 8 to 12 Hz band has a value of 25, then 8 to 12 Hz represents 25% of total EEG power. This transformation dates to the early days of EEG analysis, when amplifiers produced widely varying voltage values even from the same person, so percentages allowed one recording to be compared with another.
Here is the trap. When one frequency band carries very high amplitude, it claims a disproportionate share of the pie and leaves every other frequency looking smaller than it really is. Anderson (2025) presented a case in which 1 Hz and 2 Hz accounted for 22.9% and 20.7% of total power, together taking 43.6% of the pie. The relative power z-score maps for that client then showed apparent deficits of up to 3 standard deviations across the 6 to 16 Hz range, while the absolute power z-scores showed no deficient activity in any frequency bin at all.
A practitioner reading only the relative power maps might set about uptraining 6 to 16 Hz. In an absolute sense there were no deficits, only excesses at 1 and 2 Hz, and the other values might well normalize on their own once that excess were reduced. The problem becomes more dangerous when the excess sits in the higher beta frequencies such as 22 to 36 Hz, because the 1 to 6 Hz range then appears deficient and a practitioner may decide to train those slow frequencies upward. Anderson cautioned that this can cause serious negative effects and is generally not recommended. Hold that caution in mind when you reach the z-score threshold methods described later in this unit, since those methods normalize a client's values against a database.
Key Concept
Always consult absolute power before you interpret relative power. Relative power answers the question "what share of this client's total EEG lives in this band," not "does this client have too little of this activity." Those two questions have different answers whenever a single band is dominant, and acting on the wrong one can send you training in exactly the wrong direction.
Saying What You Mean
Terminology in this field is genuinely inconsistent, and that inconsistency reaches back to the earliest days of electroencephalography. Beta frequencies between 24 and 36 Hz may be called high, fast, or beta 3, while 25 to 45 Hz may be called gamma or beta 4. Alpha may be described as low, slow, high, or fast and simultaneously as high or low amplitude, which is how a report ends up saying something like "low high alpha."
Anderson (2025) recommended a simple remedy: identify the EEG by the frequency you are actually discussing. Say 8 to 10 Hz rather than alpha 1, 24 to 36 Hz rather than beta 3, and 36 to 44 Hz rather than beta 4 or gamma. Vague quantifiers deserve the same scrutiny. A paper that reports "an increase in the frontal EEG" tells you almost nothing, because you cannot tell whether it means 8 to 12 Hz, 15 to 18 Hz, or 4 to 8 Hz.
Compare that with a precise description: an increase in 4 to 8 Hz amplitude from 4 uV to 6 uV was noted in the prefrontal cortex during an active memory recall task. Combined with behavioral information such as performance on the task, a statement like that can support a specific hypothesis and a specific protocol. If elevated prefrontal 4 to 8 Hz amplitude accompanies lower memory scores, then training to decrease prefrontal 4 to 8 Hz becomes a reasonable candidate intervention.
Key Concept
The scalp EEG results from activity that has already occurred within the brain, so training scalp EEG rewards the brain for making internal changes that show up in the signal. Raising a client's alpha amplitude does not necessarily make them more relaxed. Becoming more relaxed may increase alpha, in which case the increased alpha is a physiological correlate of relaxing rather than its cause, and the feedback reinforces a multifaceted relaxation experience (Anderson, 2025). Frame your instructions to clients accordingly, a point you will see applied in the discussion of what to say to a client during their first session.
Key Takeaways
Frequency counts waves per second and amplitude measures their strength, while power is amplitude squared and relative power expresses a band as a percentage of total EEG power. FFT displays make band activity easy to read but conceal artifact and average away moment-to-moment detail. Relative power is systematically misleading when one band is dominant, so absolute power must be consulted before concluding that a band is deficient. Precise frequency language, such as 24 to 36 Hz instead of beta 3, prevents both clinical and publication errors.
Check Your Understanding
- Using the zero-crossing method, how would you determine the frequency of a filtered waveform?
- Why is EEG amplitude squared before many statistical calculations are performed?
- A client's relative power map shows apparent deficits from 6 to 16 Hz. What should you examine before designing a protocol to increase those frequencies, and why?
- Rewrite the statement "the client showed an increase in frontal EEG" so that it conveys clinically useful information.
- If a client's alpha amplitude rises during training, what can and cannot be concluded about their level of relaxation?
Setting Thresholds in Amplitude Training
This section covers the various threshold types used in neurofeedback amplitude training, from fixed manual thresholds to z-score approaches. Understanding how thresholds shape the operant conditioning process is essential for effective training, and for avoiding common pitfalls that can inadvertently undermine client progress.
Fixed Thresholds
In single-channel training, a clinician can manually set reward and inhibit thresholds, which correspond to microvolt values in amplitude training (Demos, 2019). The reward threshold is designed to increase brainwave amplitude (e.g., SMR). A practitioner typically sets it slightly beneath the average amplitude for that brainwave, so that exceeding the threshold initially results in feedback being presented somewhat over 50% of the time. Demos likens reward thresholds to hurdles in track: as training progresses, the reward threshold is gradually raised to shape increases in amplitude. A percentage instrument on the practitioner's screen that shows how often the threshold is exceeded provides a clearer picture of whether amplitude is increasing, helping the practitioner gauge when to raise the bar.

Conversely, an inhibit threshold is set to reduce brainwave amplitude (e.g., theta). If the goal is to decrease theta, the threshold is usually placed slightly above the average theta amplitude, so that feedback is presented somewhat more than 50% of the time when theta remains below threshold. Demos (2019) compares inhibit thresholds to a limbo bar: as training progresses, the provider gradually lowers the threshold, requiring theta amplitude to decrease further in order for feedback to continue. Again, a percentage instrument showing the proportion of time theta remains below threshold is invaluable for tracking progress.

Practitioners often want to simultaneously increase the amplitude of one EEG band while controlling or decreasing others. For example, training may aim to increase SMR amplitude while limiting theta and high beta. Using percentage instruments for each band, the practitioner can calculate how often all three thresholds will be simultaneously met. If the SMR threshold is exceeded 80% of the time and both the theta and high-beta amplitudes remain below threshold 90% of the time, then feedback is presented about 65% of the time (.80 × .90 × .90 = .65). As SMR percentage gradually climbs from 80% to the 85% to 90% range and stabilizes, the practitioner can very slightly increase the threshold, progressively shaping increased CNS capacity to produce that frequency band through operant conditioning.
Automatic Thresholds
Many neurofeedback systems have implemented auto-thresholding to simplify the process for both beginning and advanced clinicians. However, Sherlin et al. (2011, p. 299) cautioned that automatic threshold setting violates the learning principle of shaping, on which operant training depends. The problem is subtle but significant: once the client increases voltage in the reward signal, the threshold automatically rises to maintain the clinician's preset reward percentage. The client never experiences the increase in positive feedback that should accompany improved performance.
The same principle works in reverse for inhibit signals. If the voltage of an inhibit signal increases (moving in the wrong direction), the threshold automatically rises to maintain the set percentage, and the client continues to receive the same level of positive feedback despite worsening performance. In essence, auto-thresholding can punish desired change and reward undesired change. The video below provides a visual demonstration of how this works and why it is not recommended.
Single-Channel Ratio Thresholds
A ratio-threshold reinforces changes in the ratio of two EEG bandpasses rather than the absolute amplitude of either. For example, clinicians use a theta-to-beta ratio-threshold when training children diagnosed with ADHD, whose ratios may far exceed 3:1. Clients typically receive variable-pitch feedback when the theta-to-beta ratio falls (Demos, 2019). This arrangement is called inverse proportional feedback, in which a smaller ratio produces more feedback and a larger ratio produces less.
Sum Squash Threshold
A sum squash threshold reduces bandpass amplitude over a wide scalp area by using inhibit thresholds on two channels with referential (monopolar) or sequential (bipolar) recording. For example, clients would receive feedback when theta at Cz and Fz decreases simultaneously (Demos, 2019). This approach is useful when the clinical goal is broad regional reduction of a particular frequency band.
Alpha Synchrony Threshold
An alpha synchrony threshold increases alpha amplitude across the scalp. For example, trainers may reward simultaneous increases in alpha amplitude at O1 and O2 (Demos, 2019). This approach targets concurrent alpha production at two sites rather than the amplitude at either one alone. Note that co-occurring amplitude increases are not the same thing as phase synchrony, which requires a phase or coherence measure.
Alpha Variability Threshold
Alpha variability refers to fluctuation in alpha amplitude measured in standard deviations (SDs). When alpha amplitude or its variability is excessively high, as can occur in migraines, clinicians can use an alpha variability threshold to reduce them. For example, when monitoring alpha using a C3-C4 sequential montage, feedback would be enabled when alpha variability drops below a dynamic threshold (Demos, 2019).
Z-Score Thresholds
Z-score thresholds consist of upper and lower boundaries expressed in z-scores (standard deviation units). Clinicians use z-score thresholds like a precision tool to normalize specific EEG metrics and regions of interest (ROIs). For example, if mean alpha power has a z-score of 3 (i.e., 3 standard deviations above normal), the z-score threshold might be set to 2.5, producing feedback when alpha amplitude falls to 2.5 or fewer standard deviations from normal.
When z-score training involves multiple channels, numerous ROIs, and hundreds to thousands of z-score metrics, a percentage of success protocol offers greater flexibility than fixed boundaries. In this approach, a client receives feedback when a predetermined percentage of EEG components fall within ±1, 2, or 3 standard deviations from normal. If the training criteria are too demanding, the clinician can either expand the range (from ±1 to ±2 or 3) or reduce the required percentage of success.
Dynamic Z-Score Thresholds
Dynamic z-score thresholds incorporate thresholds that deliver feedback approximately 50% of the time. Unlike automated thresholds that use 60-second calculation windows, dynamic thresholds are calculated over shorter periods (e.g., 10 seconds). Demos (2019) warns that this protocol is particularly vulnerable to contamination by various artifacts, connecting back to the critical importance of artifact management covered earlier in this unit.
Unanswered Questions
Despite decades of clinical use, several fundamental questions about optimal feedback parameters remain unresolved. Researchers have not determined whether amplitude-integration (Hardt & Kamiya, 1976) or percent-time alpha feedback (Lansky et al., 1979) yields superior outcomes (Sherlin et al., 2011). The effectiveness of automatic versus manual threshold adjustment protocols is still debated (Strehl, 2014).
Additional open questions include whether neurofeedback training sessions should be continuous or discontinuous (Strehl, 2014). Does game or video feedback interfere with the post-reinforcement synchronization (PRS) that may be essential to neurofeedback learning by eliminating the small breaks needed for PRS? Would discontinuous training, interspersed with breaks, produce superior outcomes? And finally, does z-score training produce superior clinical outcomes compared to amplitude training? These questions represent important frontiers for neurofeedback research.
Key Takeaways
Threshold types include fixed reward and inhibit thresholds, ratio thresholds, sum squash, alpha synchrony, alpha variability, z-score, and dynamic z-score thresholds. Manual threshold setting is preferred over auto-thresholding, which can inadvertently punish desired changes and reward unwanted ones. Several fundamental questions about optimal feedback parameters and threshold methods remain unanswered by current research.
Learning Processes That Drive Neurofeedback
This section covers the learning mechanisms that make neurofeedback work: operant reinforcement, classical conditioning, generalization and discrimination, metacognition, and mindfulness. The critical elements described in the next section are practical applications of these mechanisms, so it is worth understanding the machinery before you adjust its settings (Anderson & Davis, 2025b).
Operant Reinforcement
Reinforcement through operant conditioning happens when a consequence that follows a behavior makes that behavior more likely to happen again in similar situations (Skinner, 1953). The consequence can be the delivery of something desired or the removal of something unpleasant. Whether a given consequence actually functions as a reinforcer depends entirely on whether it changes the behavior, and you cannot know that in advance.
This point deserves emphasis, because it is easy to substitute your own taste for your client's. Reinforcing and punishing properties are not inherent in a consequence itself; they are determined only by measuring the effect on the behavior that preceded them. A movie that motivates your client's best performance is reinforcing that client, regardless of what you personally think of the movie.
Four processes appear routinely in neurofeedback displays. Positive reinforcement increases the frequency of a desired behavior by making a desired outcome contingent on acting, as when a movie plays while a client increases low beta and decreases theta. Negative reinforcement increases a desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on acting, as when an athlete's anxiety decreases by shifting from high beta to low beta.
Positive punishment decreases an undesirable behavior by adding an unwanted consequence, as when rising EMG artifact introduces a burst of static into the audio feedback. Negative punishment decreases an undesirable behavior by removing something desired, as when a child's increased fidgeting dims the screen and lowers the sound, or when oppositional behavior results in the clinician turning off a popular game. The standard neurofeedback inhibit display, dimming a movie or muting its sound, is negative punishment, because what physically happens is that an appetitive stimulus is withdrawn. For each cell, ask what happens to the stimulus rather than how the change feels to the client, and remember that punishment is defined by whether the behavior decreases, not by how aversive the consequence seems. Recognizing which of these your display is actually delivering is more useful than assuming it delivers only reward.
Three design variables drive results. Contingency is the reliability with which a feedback event depends on the target neural state. Contiguity is the immediacy of that feedback, which is where the filter latency discussed earlier becomes a learning variable rather than an engineering detail. Schedule is the third, and small continuous feedback combined with intermittent bonus events helps reduce habituation over a long session. This is precisely the territory of the unanswered questions raised in the previous section about continuous versus discontinuous training.
Classical Conditioning
Classical conditioning is an unconscious learning process that establishes connections between events occurring together in time. A neutral stimulus that initially produces no response is repeatedly paired with a stimulus that naturally produces a response, until the once-neutral stimulus elicits a similar response on its own. Pavlov's bell is the familiar illustration, and the mechanism is very much alive in your training room.
In neurofeedback, the beneficial brain states shaped through operant conditioning also become linked to the thoughts, mental images, actions, and situations present during training. Later, when those thoughts or situations arise outside the clinic, they can automatically evoke the same beneficial state. You can use this deliberately by establishing a simple state-entry routine, such as one slow exhale, a softening of the gaze, and a cue tone, paired with successful state changes during training. Over time the routine itself begins to trigger the target pattern outside the training room.
Two related processes shape what happens next. Extinction occurs when the conditioned stimulus stops predicting its outcome and the conditioned response weakens or disappears. Spontaneous recovery, the reappearance of that response after a delay, tells us that extinction is not forgetting but new learning layered over the old. Expect both when clients report that a cue works beautifully for two weeks, fades, and then partially returns.
Generalization and Discrimination
Neurofeedback has three kinds of generalization to consider. Stimulus generalization refers to a trained state occurring in situations different from where it was first learned, and it is the most important type for our purposes. Response generalization refers to a slightly different response occurring to the same stimulus. Temporal generalization refers to the behavior continuing after training has ended.
Stimulus generalization is the whole point of clinical work, because a focused state that exists only in your office is of little use during a work meeting or a school test. Decades of applied behavior analysis research demonstrate that generalization does not occur by accident and must be deliberately engineered (Stokes & Baer, 1977). Successful practitioners build it in from the start by varying training contexts and task demands, interleaving brief state probes to test whether the skill transfers, and scheduling booster check-ins so gains last.
One inexpensive tool is a written If-Then plan that acts as a portable cue. A client might carry the plan "If I feel rushed or anxious, then I will take one slow exhale, broaden my visual field, and recall my last training success." Simple action plans like this bridge the gap between the training room and the situations that actually matter to your client.
Discrimination is the mirror image of generalization: responding to a genuine danger signal while staying calm for a safe one. In posttraumatic stress disorder this system breaks down, and fireworks or a slamming door can trigger the response that gunfire would (Anderson & Davis, 2025b). Viewed through this lens, protocols that promote alpha or SMR states associated with calm alertness are working to reduce overreactions to safety cues rather than simply reinforcing a behavior.
Metacognitive Strategies
Metacognition, literally thinking about thinking, is the capacity to observe, evaluate, and regulate one's own mental processes. It encompasses both metacognitive knowledge, meaning an understanding of how one thinks and learns, and metacognitive control, meaning the use of that understanding to guide attention, emotion, and behavior. In neurofeedback it forms the bridge between the patterns trained in session and their application in real-world contexts.
Early in training, learning is largely implicit: the brain responds to feedback signals without conscious analysis. Over repeated sessions, clients begin to reflect on what it feels like when the feedback improves, asking themselves what they are doing mentally when the tone becomes steady and what changes when it stops. Those reflections mark the emergence of metacognitive awareness, and they enable the transition from automatic conditioning to intentional self-regulation.
Once a client can articulate the qualities of their optimal state, saying something like "I widen my attention field" or "my thoughts quiet but stay clear," they can deliberately re-enter that state outside the training environment. This is why advanced protocols pair signal-based feedback with guided reflection, journaling, or brief self-observation periods between sessions. Metacognition also enriches motivation, because clients who see that brain changes follow their intentional choices develop a sense of agency that predicts adherence.
The benefit runs in both directions. A client's remark that "when I relax too much, the feedback drops" gives you valuable information about whether your target frequency represents calm alertness or the beginning of drowsiness. Encouraging clients to describe their mental strategies turns the session into a collaborative dialogue and lets you refine the protocol iteratively rather than guessing.
Mindfulness as a Companion Practice
Mindfulness, understood as systematic training in attentive, non-reactive awareness, originates in early Buddhist practice and entered contemporary health care through Mindfulness-Based Stress Reduction (MBSR) and related programs (Kabat-Zinn, 2003). A widely used operational account describes mindfulness through two components: self-regulation of attention toward present-moment experience, and an orientation of openness, curiosity, and non-judgment toward whatever is noticed (Bishop et al., 2004). Khazan (2019) prefers Christopher Germer's formulation of mindfulness as preverbal awareness of the present moment with acceptance, where preverbal awareness means the sensory experience that precedes verbal description.
Reviews converge on mindfulness enhancing self-regulation through attention control, emotion regulation, and embodied self-awareness (Hölzel et al., 2011; Tang et al., 2015). Experienced practitioners often show reduced engagement of the posterior cingulate cortex (PCC), a hub of the default mode network (DMN), during focused attention and open monitoring (Brewer et al., 2011). At the oscillatory level, EEG studies frequently report increased alpha and theta power during practice, although findings vary across techniques and levels of expertise (Cahn & Polich, 2006; Lomas et al., 2015).
The convergence with neurofeedback is easy to see. Mindfulness cultivates meta-awareness of attention and mind-wandering, while neurofeedback supplies an external mirror for internal states, creating a tighter loop between subjective noticing and objective signal change (Ros et al., 2014; Sitaram et al., 2017). Some EEG protocols train the same alpha and theta ranges that mindfulness practice tends to increase, which gives beginners a concrete scaffold for stabilizing a mindful state.
Integrating the two is straightforward. Before a session, invite the client to set a brief intention, such as noticing the breath and meeting each signal without judgment, and review what the feedback actually represents. During the session, the breath or another agreed anchor stabilizes attention while the display becomes simply another sensation to observe, so the client notices, names what they observe as rising, falling, wandering, or returning, and then re-centers. The aim is not to force the graph but to practice non-reactive adjustment.
Keep expectations realistic. Many clients need multiple sessions to map inner cues to feedback changes, and responses vary considerably between individuals (Sitaram et al., 2017). A systematic review of mindfulness-based neurofeedback found that although it has been implemented with high fidelity in clinical populations, "there is a lack of evidence for transfer effects," most studies lacked adequate sham controls, and "the mental health benefits of mbNF have not been established" (Treves et al., 2024). Mindfulness combined with neurofeedback is best understood as skills training within broader, ethically guided care rather than as a stand-alone treatment.
Clinical Application
Devon, a college sophomore training for test anxiety, produces beautiful SMR increases in your office and none at all during finals week. Rather than raising his reward threshold, you address transfer. You vary the training context by dimming the lights on some segments and adding mild background noise on others, insert 30-second state probes without feedback so he can practice finding the state unaided, and help him write an If-Then plan he can use at his desk. You also pair each successful segment with a fixed state-entry routine so the routine itself begins to cue the state. You are engineering generalization rather than hoping for it.
Key Takeaways
Operant reinforcement is the primary learning mechanism in neurofeedback, and its effectiveness rests on contingency, contiguity, and an appropriate schedule. Classical conditioning supplies a second route to transfer, because cues and routines paired with successful in-session states can later evoke those states outside the clinic. Generalization must be deliberately engineered through varied contexts, state probes, boosters, and portable If-Then plans. Metacognitive strategies convert implicit feedback learning into intentional self-regulation, and mindfulness practice complements neurofeedback by strengthening attention control and emotion regulation, although it is a companion to training rather than a stand-alone treatment.
Check Your Understanding
- Why can a clinician not know in advance whether a particular feedback display will function as a reinforcer for a given client?
- Give a neurofeedback example of each of the following: positive reinforcement, negative reinforcement, positive punishment, and negative punishment.
- How do contingency and contiguity differ, and how does your choice of digital filter affect one of them?
- What is stimulus generalization, and name three specific techniques for engineering it into a course of training.
- How can a client's metacognitive comments help you decide whether your target frequency band is producing calm alertness or drowsiness?
Critical Elements in Neurofeedback Training
This section covers the foundational principles that make neurofeedback training effective: readiness, repetition, reinforcement, primacy, recency, intensity, freedom, and resources. Each one is a practical application of the learning mechanisms described in the previous section, and each has direct implications for how you structure sessions, engage clients, and set thresholds.
These eight elements have a mixed pedigree worth stating plainly. Three are Thorndike's own laws of learning: exercise and effect, from Animal Intelligence (Thorndike, 1911, p. 244), and readiness, added in the second volume of Educational Psychology (Thorndike, 1913). Primacy, recency, and intensity came from later educational psychologists and were codified for instructors in handbooks such as the Federal Aviation Administration's Aviation Instructor's Handbook, which names no originators (Federal Aviation Administration, 1999, 2020). Freedom and requirement circulate widely in that literature but have not been traced to a primary source, and they appear in neither Thorndike nor the FAA handbook; treat them as practical maxims rather than findings. The parenthetical labels below (Exercise, Effect, Requirement) map neurofeedback vocabulary onto the older terms.
Readiness
Readiness means preparation for training and involves both concentration and enthusiasm. The instructor-training literature puts it crisply: "Individuals learn best when they are ready to learn, and they do not learn well if they see no reason for learning" (Federal Aviation Administration, 1999, p. 1-5). Readiness in this sense is physical, mental, and emotional at once, and it requires adequate rest and nutrition along with a positive, supportive environment. Client education that clearly explains the training process, defines goals and outcomes, and links training to personally relevant benefits directly enhances readiness.

In contrast, poor client motivation, lack of understanding of potential benefits, and biopsychosocial impediments can impair readiness. Significant constraints include a chaotic, disruptive, or traumatic environment, inadequate rest and nutrition, developmental delays, lack of resources, and traumatic brain injury or other medical problems. For practitioners working in VA settings or with military populations, combat-related factors such as irregular sleep schedules and hypervigilance may specifically compromise readiness.
Nutrition and Readiness: What the Brain Map Shows
Nutrition deserves a closer look here, because it is one of the most concrete levers a client can pull on their own readiness. It is tempting to treat "eat something before your session" as generic wellness advice, yet the brain's electrical activity tells a more specific story. A revealing illustration comes from MacInerney and colleagues (2017), who used quantitative EEG (qEEG), the digitized brain-mapping method introduced earlier in this unit, to record how three different breakfasts changed one child's brainwaves.
Their subject was a healthy, neurotypical (developmentally ordinary, with no diagnosed neurological or psychiatric condition) 12-year-old girl who habitually skipped breakfast and reported feeling anxious and unfocused by late morning. On three separate school days, the researchers recorded her resting, eyes-closed EEG at noon after one of three conditions: no breakfast, a high-sugar and high-carbohydrate breakfast (a toaster pastry and orange juice), and a nutritionally balanced breakfast (eggs, whole-grain toast, fruit, tomatoes, and milk). They held sleep, timing, and recording conditions constant so that the meal was the only thing that changed.
The analysis focused on absolute power (the power, in microvolts squared, within a frequency band at a single electrode site, compared against an age-matched normative database) in the high beta range. High beta is fast EEG activity commonly associated with hyperarousal, anxiety, worry, and mental "over-revving." The investigators assessed 1 to 30 Hz and found effects only in the fastest bins, at 26 to 28 Hz with no breakfast and 27 to 30 Hz after the sugary one.
On the no-breakfast day, her high beta ran "2.0 to 4.0 standard deviations (SD) above the mean," with a mean of 2.9 SD, across frontal, central, and left posterior temporal sites (F7, F3, Fz, F4, C3, C4, T5, P3). The affected sites included electrode positions over Wernicke's area (a posterior temporal region essential for understanding spoken and written language), hinting that a skipped breakfast may reach the very systems a student relies on for schoolwork. In other words, an ordinary child, simply by skipping breakfast, produced a resting brain map that looked anxious and overaroused.
Eating the high-sugar breakfast helped, but only partway. Her high beta was still elevated, though less so than with no breakfast, which suggests that any food is better than none. The nutritionally balanced breakfast produced the most striking result: her qEEG normalized completely, with no significant deviation from the mean at any of the 19 sites. The authors had expected some residual abnormality and were surprised to see it disappear. The girl's own reports tracked the data, with her anxiety worst after skipping breakfast, milder after the sugary meal, and nearly absent after the balanced one, when her focus was also at its best.
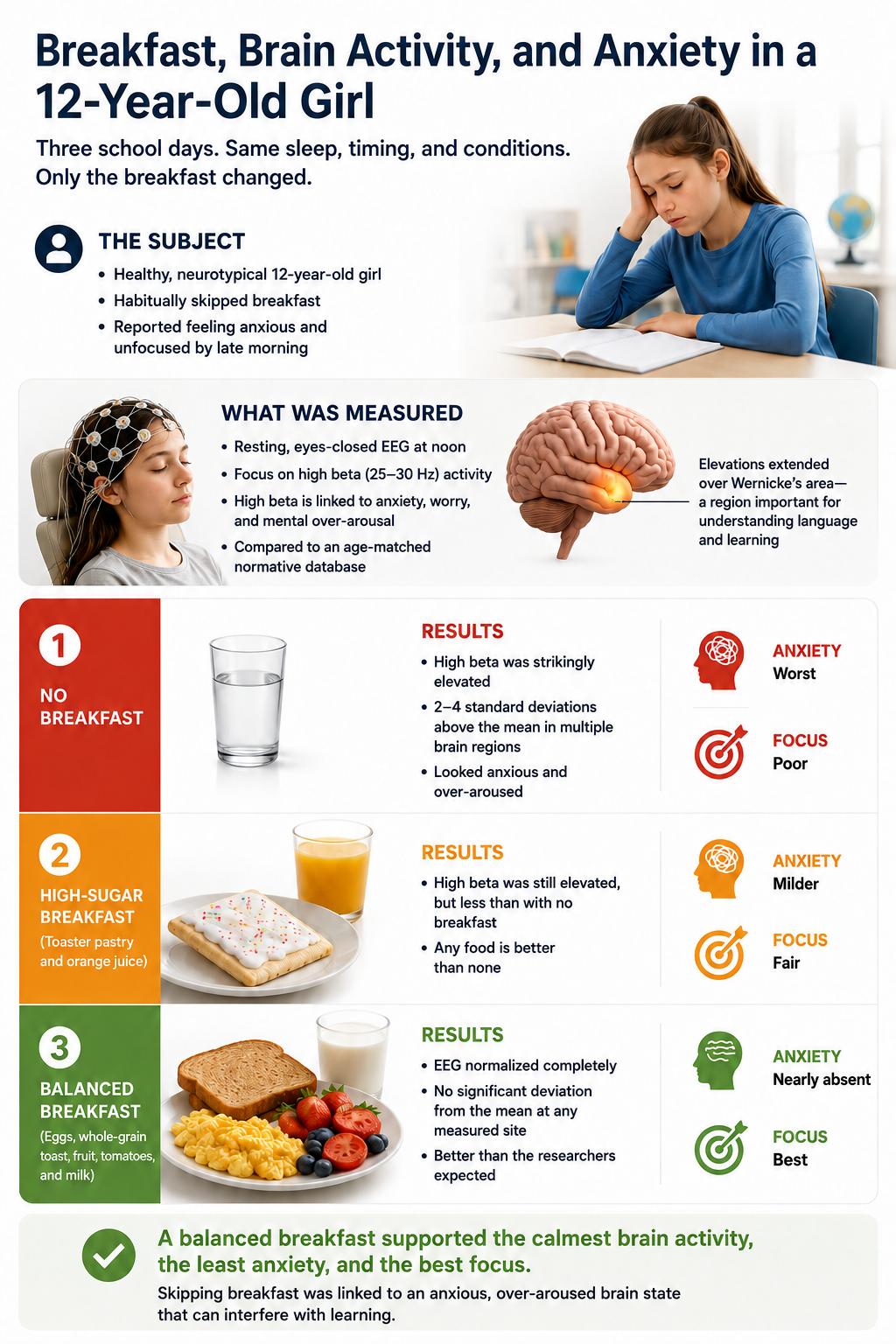
Why should you care about a single child's brainwaves? Because excessive high beta is not a harmless curiosity. Clarke and colleagues (2001) identified a small subset of children with attention-deficit/hyperactivity disorder (ADHD) whose EEGs show excess beta rather than the usual excess slow-wave activity, and who were "more prone to temper tantrums and to be moody" than other children with ADHD.
They concluded that these children "are probably not hypoaroused as previously suggested," and that the excess, found "primarily in the frontal regions," "may be associated with frontal lobe self-regulation and inhibition control," the very capacities neurofeedback aims to strengthen. Note that they analyzed beta from 12.5 to 25 Hz, a lower and wider range than the fast bins in the breakfast study. When a hungry client arrives with a brain that is already over-revving, you may be asking them to learn self-regulation from a starting line that a balanced breakfast could have moved for them.
Clinical Application
Imagine a 10-year-old boy referred for attention training who arrives for his after-school sessions cranky, restless, and quick to frustrate. Before adjusting a single threshold, ask what and when he last ate. If he takes a stimulant medication, remember that appetite suppression is one of its most common effects, and that skipped meals may quietly push his EEG toward the overaroused, high beta pattern you are trying to reduce.
Currie and colleagues (2014), studying a Quebec insurance expansion that sharply increased stimulant use, found "little evidence of improvement" in academic or emotional outcomes in either the medium or the long run. They do not identify appetite suppression as a mechanism; the nutritional concern raised here is a clinical inference rather than their finding. A simple protein-containing snack before the session may do as much for his readiness as any change you make to the protocol.
Keep the study's limits in view. This was a single case with one healthy child, so its numbers cannot be generalized, and controlled research is still needed. Even so, the message aligns with a large body of work linking breakfast to better attention, learning, and behavior in children, and it gives you a concrete, low-cost readiness intervention to raise with clients and families before you ever adjust a threshold.
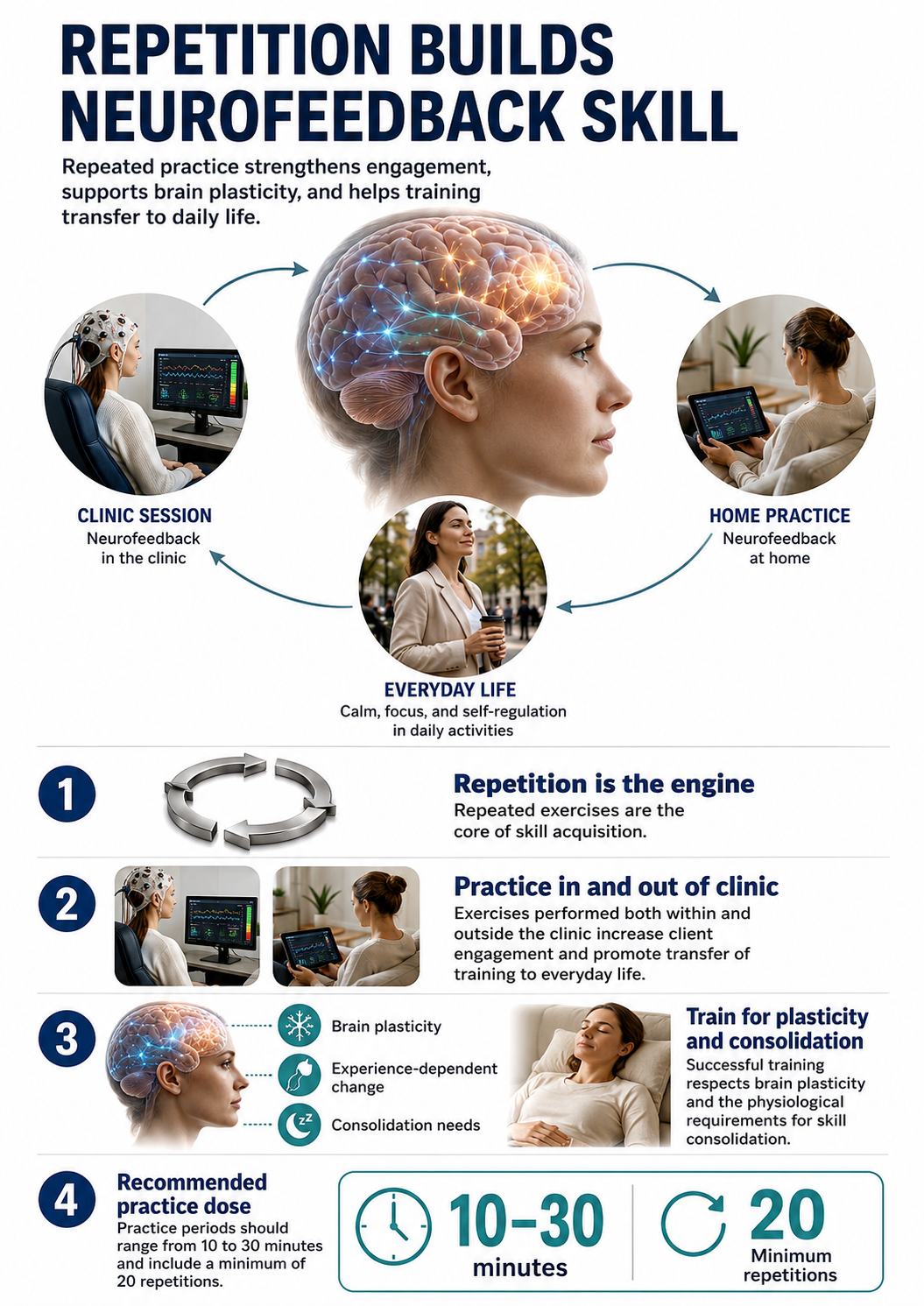
Repetition (Exercise)
Repetition is the engine of skill acquisition. Exercises performed both within and outside the clinic promote client engagement and transfer of training to everyday life. Successful training recognizes brain plasticity, the nervous system's capacity to reorganize in response to experience, and the physiological requirements for skill consolidation. The commonly repeated guideline that practice periods should run 10 to 30 minutes and include at least 20 repetitions could not be traced to a primary source; treat it as a practical rule of thumb rather than a documented finding.
Reinforcement (Effect)
Building on the operant principles described earlier, remember that rewards must be personally desirable to the client. Clinicians confirm reinforcer effectiveness the only way it can be confirmed, by observing its impact on engagement, motivation, and performance. Intrinsically reinforcing outcomes accelerate mastery development and improve retention, while clear evidence of success builds confidence and reduces frustration. Encouragement by staff and family is essential to sustain progress when clients encounter difficulty.
Sherlin et al. (2011) speculated that secondary reinforcement for neurofeedback achievement (monetary rewards or points redeemed for a prize) might accelerate learning of self-regulation skills, but they cautioned that such reinforcement should be delivered for EEG changes rather than simple attendance.
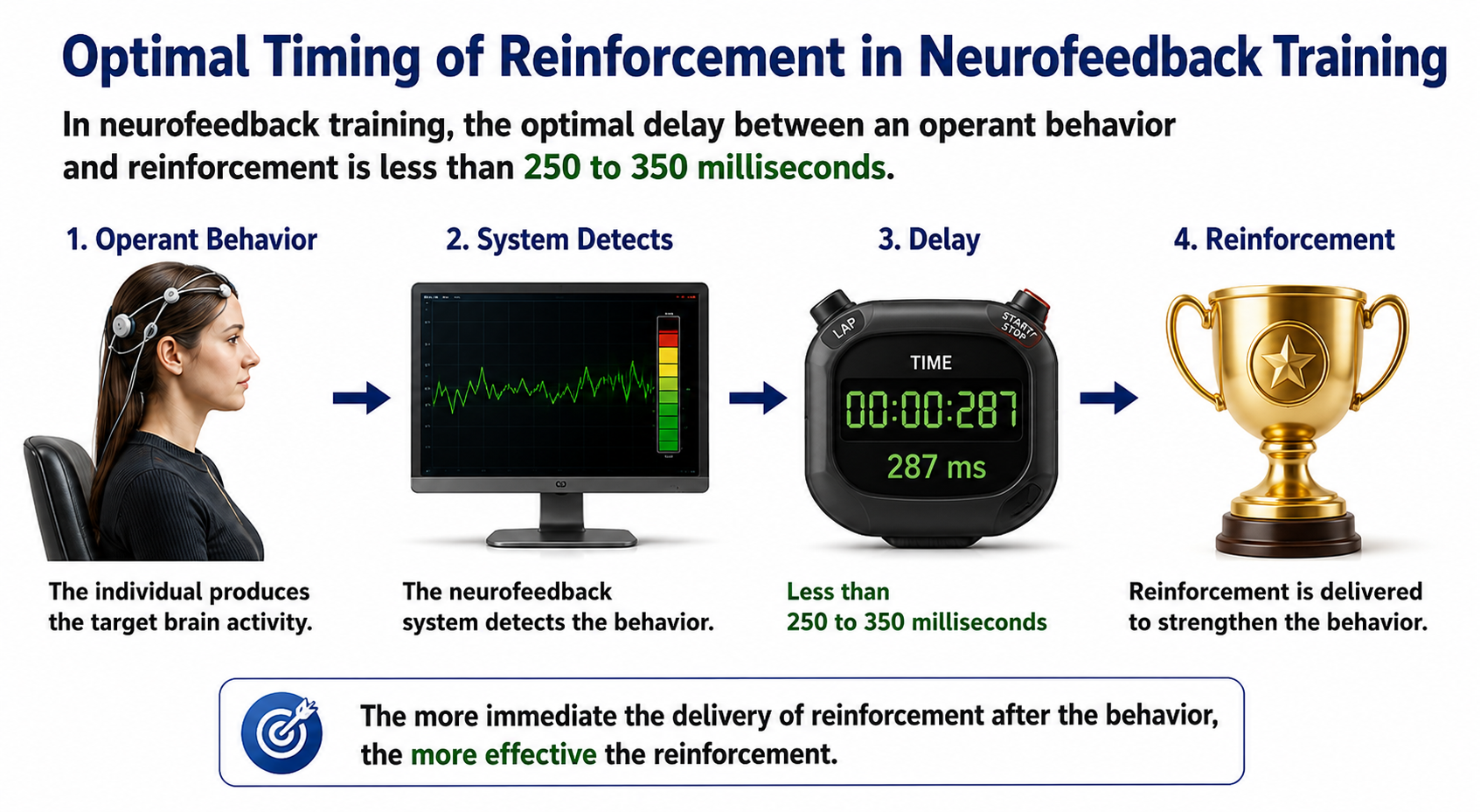
The timing of reinforcement is critical. Classic operant research showed how steeply learning degrades as reward is delayed: Grice (1948) found that rats needed a median of 20 trials to master a visual discrimination under immediate reward, 580 trials at a 5 s delay, and 155 trials when an immediate signal marked the correct response, demonstrating that a conditioned reinforcer can bridge a delay. Working from that literature, Sherlin et al. (2011) recommended that feedback latency "should not exceed 250 to 350 ms," while noting that "there is no fixed rule on what is the minimum or maximum acceptable delay" (p. 297).
Treat that range as a practical engineering ceiling, not a measured optimum for learning, and note that the figure is often attributed directly to Felsinger et al. (1947), whose paper measures reaction latency as a function of the number of reinforcements and says nothing about delay of reinforcement. As Miller (2006) stated, "The more immediate the delivery of the reinforcer after the behavior, the more effective the reinforcer." For neurofeedback, this means shorter EEG filter response times are better because they reduce the delay between the desired brain state and the feedback signal (Sherlin et al., 2011). This is the clinical reason behind the filter comparisons presented earlier in this unit, where a third-order IIR filter delivers an output in roughly 11 milliseconds while an FFT calculation requires at least a full second of data.
Sterman and Egner (2006) warned that neurofeedback "software programs and training strategies should stress exercise rather than entertainment, at least most of the time." The rationale, that complex games prevent clients from linking brain responses to the reinforcement signal because a more salient stimulus-reinforcer association overshadows the response-reinforcer one, belongs to Sherlin et al. (2011, p. 298); see also Egner and Sterman (2006), the companion review. This tension between engagement and learning is a practical challenge for every practitioner.
Primacy
Clinicians should approach neurofeedback training like a contractor building a house: start with a strong foundation. Client education should present the core principles that set the stage for future learning. Like home construction, skill acquisition should proceed in a stepwise fashion that builds upon previous experience. The successful acquisition of initial skills builds confidence and aids the mastery of more complex skills later.

Recency
Clients more readily recall material learned most recently. The combination of recency and repetition improves the retention of self-regulation skills. The frequency of training sessions directly impacts learning, since more frequent sessions mean that skill practice and reinforcement occur closer together in time.

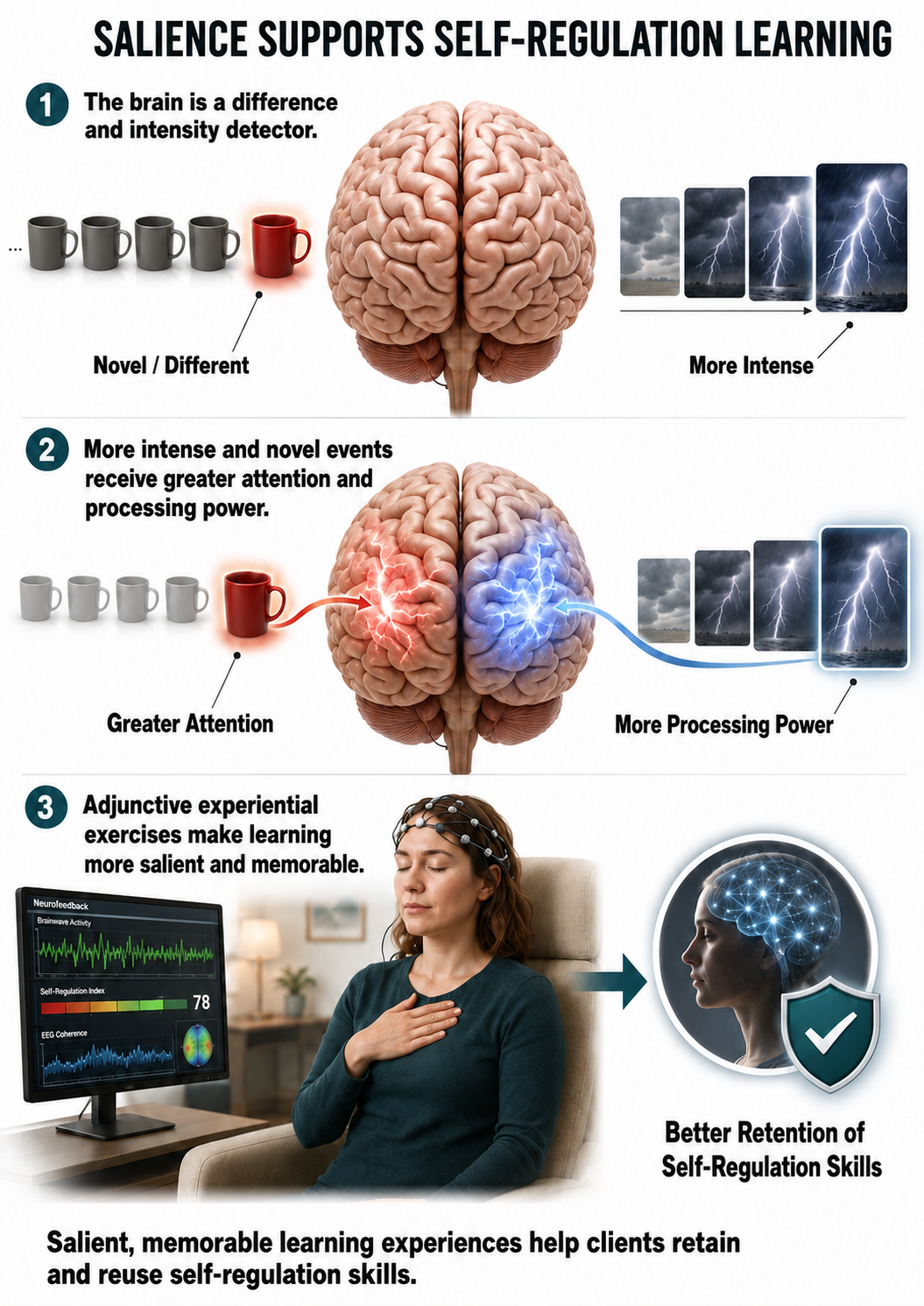
Intensity
The brain is a difference and intensity detector, and it allocates greater attention and processing power to more intense and novel events. This suggests that adjunctive experiential exercises can facilitate the retention of self-regulation skills by making the learning experience more salient and memorable.
Mindfulness meditation practice is one example of a powerful home practice assignment, and the earlier discussion of mindfulness as a companion practice explains why it pairs so naturally with neurofeedback.

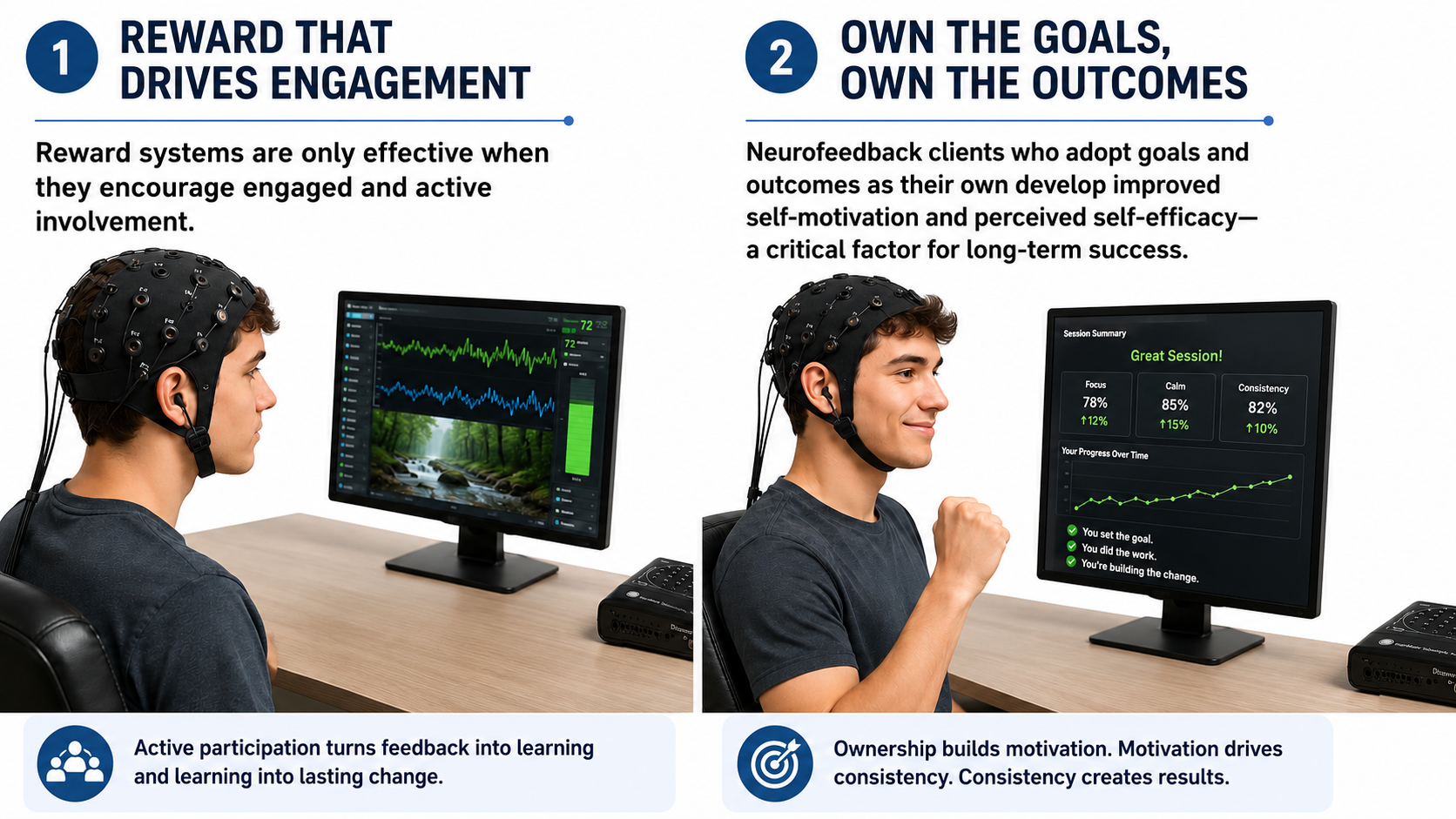
Freedom
Active, willing participation facilitates learning, while coercion, compulsion, and forced participation inhibit it. Reward systems are only effective when they encourage engaged and active involvement. Clients who adopt goals and outcomes as their own develop improved self-motivation and perceived self-efficacy, a critical factor for long-term success. This principle has particular relevance for practitioners working with mandated clients or reluctant adolescents.
Resources (Requirement)
Neurofeedback professionals start with skills already in a client's repertoire and then build from there. For example, heart rate variability (HRV) biofeedback builds on a client's existing breathing skills and then shapes the mechanics and rate. Shaping, the gradual reinforcement of successive approximations of a target behavior, is the mechanism by which new skills are added to the client's repertoire.
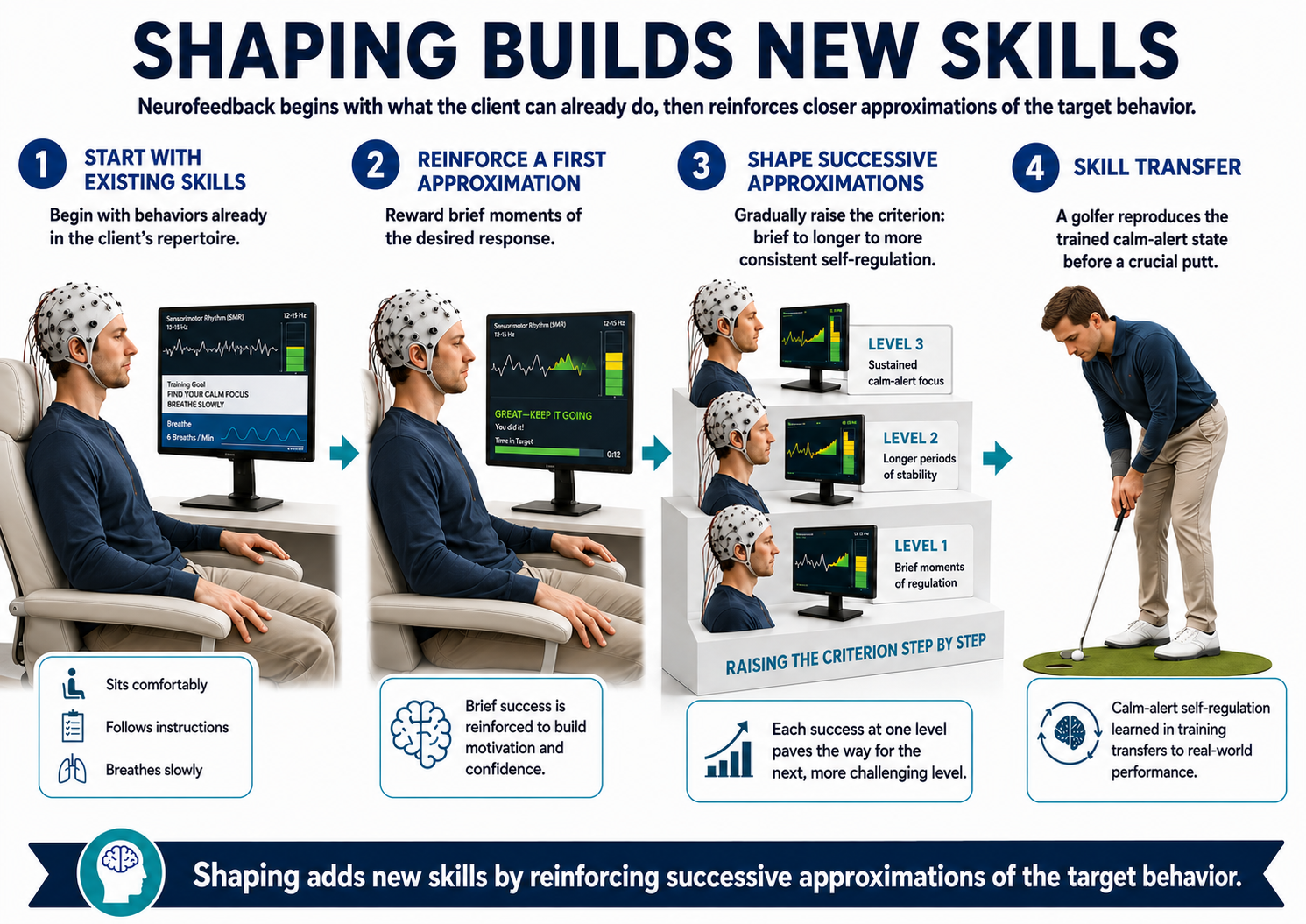
Olton and Noonberg (1980) are the source usually given for a practical guideline: raise performance goals when a client succeeds more than 70% of the time, and lower them when success drops below 30%. That passage could not be located in their text, so treat the numbers as clinical lore rather than a documented recommendation. The range is close to reported practice: Lansbergen et al. (2011) rewarded children about 80% of the time, and Strehl (2014) reports that automatic threshold regulation commonly rewards 60% to 70% of trials, while cautioning that rewarding at a fixed rate regardless of improvement is at odds with the logic of shaping. Many neurofeedback systems incorporate algorithms that automatically revise goals based on the client's performance (e.g., time above threshold) to maintain motivation and ensure sufficient challenge.
Selecting and Modifying Thresholds
Thresholds should be set manually rather than by auto-thresholding to accomplish the operant conditioning of EEG that is fundamental to neurofeedback. Before starting feedback during the first session, the practitioner may collect one to two minutes of pre-training baseline EEG data by turning off the speakers and secondary monitor. If using a single monitor, it can be turned away from the client and muted. During this baseline, the practitioner adjusts thresholds by observing the display instruments and the percentage of time they are on or off, aiming for feedback to be on between 50 and 75 percent of the time.
Some practitioners select a threshold closer to 50%, others closer to 75%. Setting the threshold for more frequent feedback may reduce frustration in some clients, while less frequent feedback can offer a teaching opportunity if the client can learn to attentively observe when feedback occurs and identify what correlates with it. One caution: the client may become more alert simply by viewing the feedback screen when it is enabled, resulting in a non-optimal feedback rate. If this pattern appears, thresholds for the first few sessions can be set during the first minute of active feedback instead.
Pre-training baseline data can be saved for later artifacting and analysis, or used for quick calculation of relevant EEG variable values to show the client immediately. These values can then be compared with data from training epochs and post-training values at the session's end.
Instructions to the client
After the pre-training baseline, the practitioner provides instructions that vary depending on the stage of training. For the first neurofeedback session, fairly non-directive instructions work well, such as: "Let yourself be comfortably relaxed and notice when the feedback is on. If possible, notice what it feels like when the feedback is on." More specific directions may guide the client to notice how active their thinking is, the content of their thoughts, their emotions, and physical sensations, and how these evolve during training.
In later stages of training, the client may have learned to identify distinct subjective qualities associated with feedback being on or off and developed strategies to voluntarily produce those states. At that point, the practitioner can more successfully instruct the client to "make the feedback occur as much as possible."
Training segments
Depending on the type of neurofeedback used, training may occur in one continuous period or a series of briefer segments. For deep states training, feedback is typically provided during one continuous period of 45 minutes or longer. For many other applications, feedback may be presented as ten 3-minute segments with brief rest periods in between, or in a series of segments of other durations.
Key Takeaways
The critical elements for successful neurofeedback training include readiness (client preparation), repetition (practice within and outside sessions), reinforcement (immediate, personally meaningful rewards), primacy (building a strong foundation), recency (frequent sessions), intensity (engaging exercises), freedom (willing participation), and resources (building on existing skills through shaping). Thresholds should be set manually using pre-training baseline data, targeting feedback on 50-75% of the time.
Adjusting Thresholds Across Sessions
Where the earlier section catalogued the types of threshold available to you, this section covers the practical art of adjusting them across sessions: when to raise or lower them, when to hold steady, and how to apply the operant conditioning principle of shaping by successive approximations. Threshold management is where clinical science meets clinical judgment.
The practitioner may cautiously modify threshold settings either within a single session or from session to session, adjusting them to require greater or lesser change relative to preceding sessions or pre-training baseline data, depending on the client's needs. If a session begins with the threshold from the end of the previous session, it may sometimes need adjustment if feedback occurs at too high or too low a rate. In those cases, patience is key. Allow a minute or two, or even a full training segment, before making changes. The client may naturally increase feedback if it had been low, or cortical state changes may bring an overly high rate down to a more productive level.
As the session proceeds, the rate of feedback may show a changing trend from segment to segment. If feedback gradually increases, it suggests the brain is learning to function in a manner more consistent with the protocol's intention (e.g., producing more SMR and less theta). This raises the question of whether to change threshold settings to maintain the earlier feedback rate, in other words, making training more difficult. However, it may be more consistent with the operant conditioning principle of overlearning to keep the current thresholds so that improvement can be consolidated and made more durable. If session-to-session trends demonstrate that a high rate of feedback is achieved earlier within sessions or that pre-training baseline data are improving, the case for changing thresholds becomes stronger.
When considering stricter thresholds, the practitioner should follow the operant conditioning method of shaping by successive approximations (Cooper et al., 2019; Martin & Pear, 2019): proceed slowly based on stable trends in the data. Moving too quickly risks making the reinforcement schedule too lean, leading to performance deterioration. If performance does deteriorate and stabilizes at a less desirable level, thresholds need to be eased so that more feedback is forthcoming.
Conversely, a gradual decrease in feedback percentage from segment to segment may signal client fatigue rather than a threshold problem. Rather than adjusting thresholds, consider shortening the duration of training segments or reducing the number of segments for that session. Over time, you may see session-to-session improvement in the client's ability to sustain productive brain states for the entire session.
The threshold types themselves are covered in the Setting Thresholds in Amplitude Training section earlier in this unit, and additional worked examples appear toward the end of the Therapeutic Relationship, Coaching, and Reinforcement Strategies unit.
Key Takeaways
Threshold adjustment requires patience and careful observation of data trends. Follow the operant conditioning principle of shaping by successive approximations, proceeding slowly based on stable trends. If the reinforcement schedule becomes too lean, ease the thresholds. If the client is fatiguing, shorten segments rather than adjusting thresholds. Session-to-session consistency in threshold settings may be appropriate when trends are stable.
Monitoring Client Progress
This section covers how to monitor client progress within individual sessions and across a course of training. Effective monitoring integrates quantitative EEG data, qualitative observation, peripheral biofeedback measures, and direct client communication into a coherent clinical picture.
During a session, the practitioner intermittently asks the general question: "How is the client doing today?" The answer draws on quantitative data (e.g., values of EEG variables) and qualitative inspection of the EEG for changes in alpha, theta, or high beta production that may signal increasing drowsiness, emotional distress, or physical discomfort. Direct observation of the client's motor and verbal behavior throughout the session can also be revealing. For example, noting whether the client appears more relaxed, alert, drowsy, or tense as the session progresses. Pauses between training segments provide natural moments to ask about the client's state and offer coaching.
Peripheral biofeedback monitoring, such as hand temperature, skin conductance, or respiration, provides additional response information, helping both practitioner and client identify changes in physiological arousal during training. The practitioner should also inquire about the client's experience when feedback has been sustained for a particularly long time or when it has been absent for an extended period. This inquiry helps the client discriminate between the internal subjective states and volitional efforts associated with more versus less feedback. With practice, the client may begin making successful intentional efforts to produce more feedback for longer periods, strengthening their ability to apply self-regulation skills in relevant situations (e.g., paying attention in a classroom or managing stress in a clinical environment).
A recording form prepared before the session can document changes the client experiences in their own words, so that these possibly idiosyncratic labels can be used in future sessions to prompt a return to the desired state.
Identifying drowsiness
Drowsiness artifact is the appearance of stage N1 or N2 sleep patterns (formerly stages 1 and 2) in the EEG, most likely during eyes-closed recording. Alpha amplitude (especially occipital) may decrease, while theta (especially frontal) may increase. EMG and beta amplitude reductions often accompany slow eye-rolling movements, and sleepiness may be signaled by spike-like transients known as vertex waves or V-waves (Thompson & Thompson, 2015). Recognizing these patterns promptly allows the practitioner to intervene before the training segment is compromised.
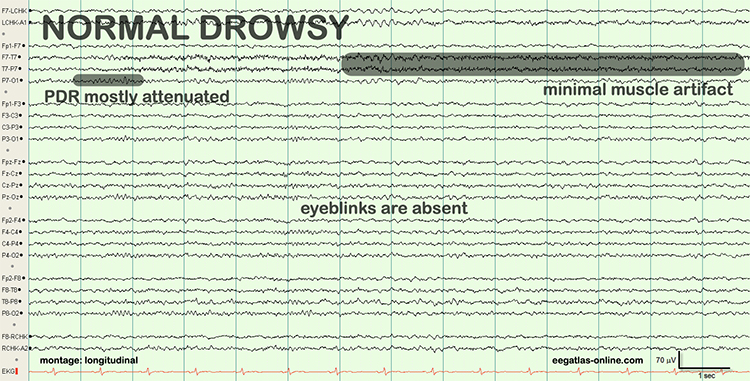
Revising protocols and moving to new sites
Neurofeedback is most effective when guided by ongoing assessment and reassessment. The initial assessment should inform the clinician's first protocol and site selection, while ongoing data should guide adjustments to both clinical and performance interventions. This movie provides an overview of how clinicians integrate continuous assessment with treatment © John S. Anderson.
Medication issues
Understanding psychopharmacology is important to neurofeedback because drugs can affect a client's clinical presentation, EEG patterns, assessment accuracy, and training success.
To interpret initial and ongoing assessment data accurately, the clinician should obtain a complete list of prescription drugs, over-the-counter supplements, and social drugs (including caffeine and nicotine). Encourage clients to report medication changes promptly so you can differentiate drug effects from training effects on the EEG, performance, and symptoms.
Take drug effects into account when interpreting your initial assessment battery and subsequent reassessment testing: develop training goals based on initial testing with medication, and retest with the same medication unless it has been withdrawn to ensure a valid comparison. Most importantly, develop a personalized training strategy that does not attempt to train against a drug's principal effects on the EEG.
Gunkelman (n.d.) offered valuable context for understanding how drugs affect the EEG.
There is a generally reciprocal effect between alpha and beta, as brain stem stimulation desynchronizes the alpha generators, beta is seen. During states of under-arousal, this relationship is not seen, as when the subject is alerted, when both alpha and beta increase. The point is that the arousal level changes the EEG responses expected, as when a stimulant is given to an under-aroused subject, increasing alpha. In a normally aroused subject, stimulants decrease alpha, and in an anxious (low voltage fast EEG variant) subject alpha will not be seen as changed by a stimulant. Though there is a response stereotype for each medication, there are also individual responses, which vary. Mixtures of medications become too complex to evaluate each individual medication's contribution, not to speak of synergistic effects not seen with any single medication, which may be seen in polytherapy.
Medication Effects on the EEG video © J. S. Anderson. Click on the thumbnail below to view this video in YouTube.
Medication and recreational drug considerations for monitoring client progress during neurofeedback sessions
A broad generalization, but an important one, is that large individual differences exist in how psychoactive medications affect a unique individual's EEG. Arriving at an absolute description of how different doses of different medications reliably affect the EEG is therefore extremely difficult. For example, while the effects of barbiturates or alcohol on the EEG are fairly well understood, the dose that produces those effects may differ greatly between individuals.
What matters for practitioners is knowing what consequences are possible so that EEG patterns are not misattributed to brain pathology when they actually reflect drug effects. When monitoring client progress across a course of training, good practice includes asking at the beginning of each session whether there has been any significant change to medications or use of drugs and alcohol. If the EEG during that session is inconsistent with previous sessions, and the inconsistencies align with reported medication changes, the practitioner can reasonably hypothesize a connection.
As Blume (2006) described, medication factors to consider include dose, method of administration, rate of metabolism, systemic effects, and genetic or epigenetic patient characteristics. These observations may sometimes appear paradoxical (e.g., increased beta activity following a sedative such as a barbiturate), and it must be remembered that not all clients will show such effects.
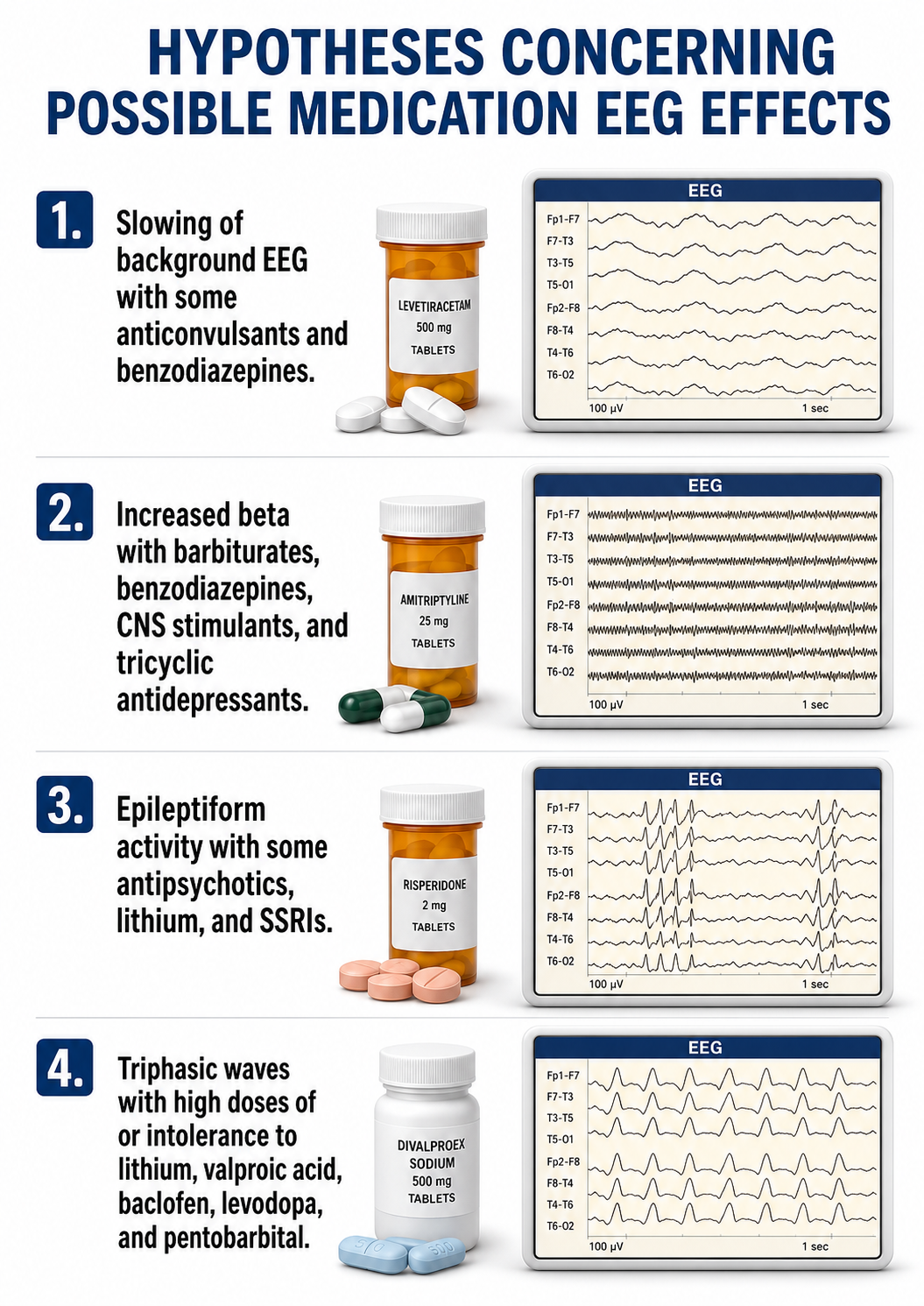
For sessions when medication effects seem likely, neurofeedback training may be altered or even compromised. If the medication change is ongoing (e.g., the client's physician has introduced an SSRI), reassessment after dosing has stabilized may be warranted. The guiding principle is to make only one treatment change at a time and wait for any subsequent response to stabilize before introducing a second change. Equally important is supporting client autonomy by acting only with informed consent. The practitioner must be clear about their scope of practice and limitations regarding medication management.
However, it is appropriate to discuss with clients the possibility that medications they are taking may have different effects after neurofeedback training begins. If this develops, encourage the client to report changes to their prescribing physician so that medication adjustments can be considered. Proactive communication with the client's healthcare providers before initiating neurofeedback ensures those providers are better prepared for medication adjustment discussions. Sharing pre-training assessment information may also suggest improvements to the medication regimen and alert the prescribing physician that a good response to neurofeedback may set the stage for safe medication reduction.
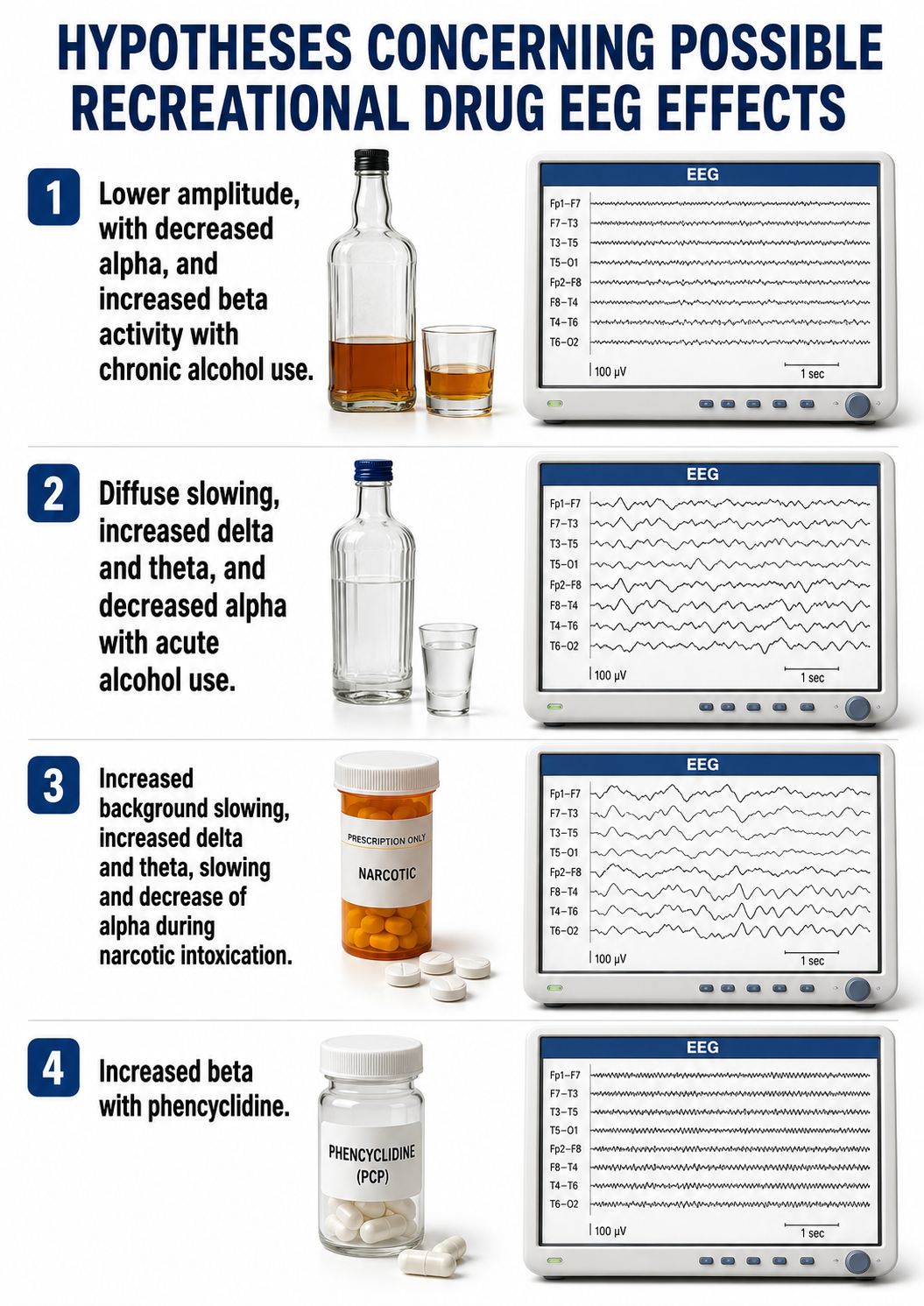
Concerning occasional alcohol or drug use that appears to be producing EEG changes during a training session, the practitioner is wise to defer the session until the likely EEG effects have subsided. Recreational substances leave signatures of their own. Herning and colleagues, for instance, documented cocaine-related increases in EEG beta activity and later in both alpha and beta, which they interpreted as evidence of reduced cortical processing (Herning et al., 1985, 1994).
Drugs can rapidly affect the EEG
A single dose of a prescription psychotropic drug can markedly change the EEG within 1 to 3 hours of administration. Families of psychotropic drugs that share therapeutic equivalence (e.g., chlorpromazine-like neuroleptics and haloperidol-like neuroleptics) produce similar systematic EEG changes (Knott, 2000). A drug's plasma level, which depends on dose, distribution volume, and metabolism, influences the magnitude of EEG alterations, which should be symmetrical and often widespread. Common EEG changes include slowing of background activity, increased beta activity, epileptiform activity, triphasic waves, and widespread delta and increased theta activity (Blume, 2006).
Where to find an overview of the drugs
Neurofeedback Tutor: An Introduction's Psychopharmacology unit summarizes the effects of antidepressants, antipsychotics, benzodiazepines, CNS stimulants, mood stabilizers, opioid analgesics, and recreational drugs on the EEG. For each drug class, understanding the typical EEG signature helps practitioners avoid misinterpreting drug effects as pathological findings or training outcomes.
When you need more detail than a summary can provide, several sources repay the effort. Banoczi (2005) and Van Cott and Brenner (2003) survey drug effects and toxic encephalopathies from an electrodiagnostic perspective, Bauer and Bauer (2005) cover drug effects and central nervous system poisoning, and Saletu and colleagues (2010) illustrate how EEG topography and tomography inform pharmacotherapy in depression. For pharmacology itself, Advokat and colleagues (2019) and Stahl (2017) are standard references.
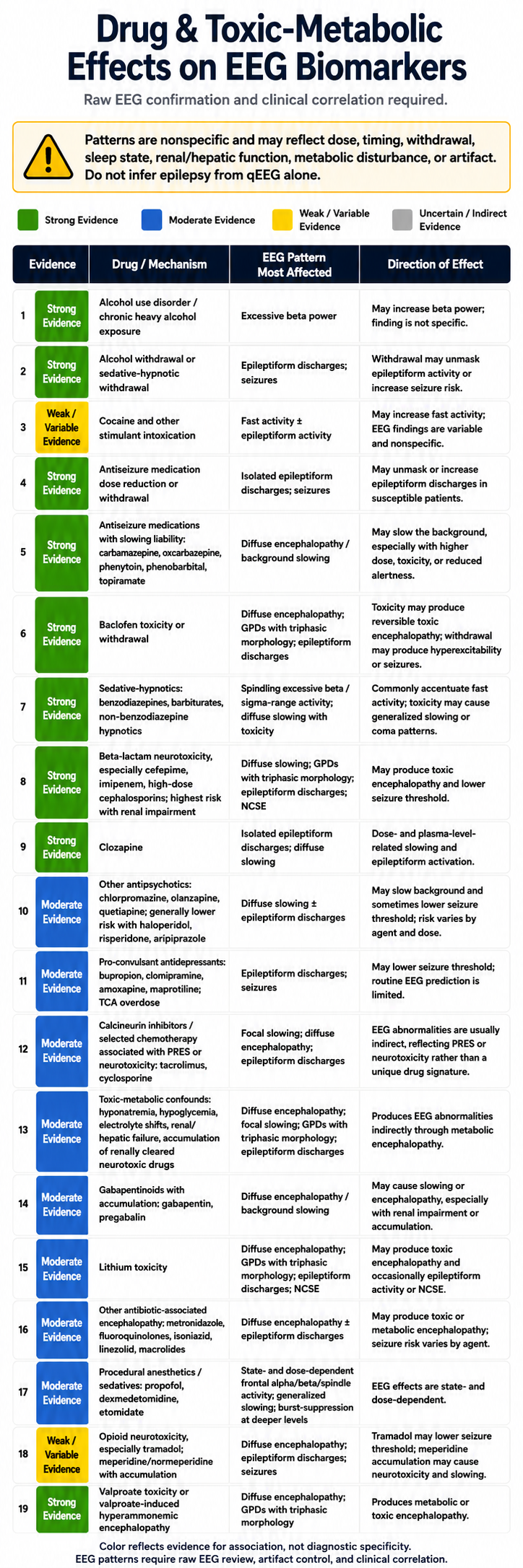
Recommended medication management approaches
Begin by discussing the scope and limitations of your professional license and your ability to address medication issues. Review your client's plans regarding their medications. Are they continuing current prescriptions? If not, have they consulted with their prescribing physician?
If the client wishes to decrease or eliminate medications, their best option is to discuss this with the prescribing physician. If they wish to proceed without physician consultation, explain your limitations and ethical concerns about proceeding with neurofeedback under these circumstances. Medications often need adjustment due to the effects of training, and the clinician or client must coordinate with the prescribing physician regarding these changes. As neurofeedback changes brain function and structure, medications may need to be titrated or withdrawn. Standardized instruments, such as the Beck Depression Inventory for psychological measures or the Computerized Continuous Performance Test for performance measures, can help inform the physician's decision.
Wherever possible, involve your client in this process. Physicians may not always welcome the neurofeedback provider's direct involvement in medication decisions, and clients may find it easier to interact with the prescribing physician when armed with accurate information from their training.
Key Takeaways
Psychoactive medications can rapidly alter the EEG within 1-3 hours. Each drug class (antidepressants, antipsychotics, benzodiazepines, stimulants, mood stabilizers, opioids, and recreational drugs) has characteristic EEG effects. The practitioner should ask about medication changes at each session, develop training strategies that do not train against a drug's principal EEG effects, and coordinate with prescribing physicians regarding medication adjustments as training progresses.
Neurofeedback contraindications
This subsection covers conditions and circumstances that may contraindicate neurofeedback training, as well as adverse effects that practitioners must monitor for and manage. Understanding both helps practitioners make ethically sound decisions about when to proceed with training and when to defer.
Paul Swingle (2015) astutely warned:
Not every individual or family is ready for EEG neurofeedback training. It may be contraindicated due to the nature of the disorder or the limits of the treatment facility. During the initial interview (before qEEG analysis), it is essential to continue to assess clients' readiness to undergo the training process. They must have the time and the finances to complete the training process. Also, it is essential to determine if the clients have Axis II disorders. If the initial interview has revealed a pattern of interpersonal problems, biofeedback training may be contraindicated. Dialectical behavior therapy may be the first place to start treatment (Linehan, 1993). Neurofeedback training will not magically undo the covert nature of transference, countertransference, splitting, or distrust (Demos, 1995). Neither will the risk of suicidality, self-harm, or explosive anger melt away with biofeedback training. (p. 273) Neurofeedback training may be contraindicated for those with severe learning disorders, psychotic behaviors, or mental deficits. The appropriate candidate must be able to learn a new skill in a relatively healthy and supportive environment. If you are a new provider, some problems will be over your head. Consult with your supervisor (mentor) and jointly determine if you are ready to take on a new challenge. (p. 275)

The following are conditions and issues that may be viewed as contraindications for neurofeedback training.
Recent stroke, TBI, or other brain trauma
This caution is speculative and is not supported by specific research findings. However, work with hemoencephalography (HEG), a technique that monitors cerebral blood oxygenation, gives some reason for caution. In an uncontrolled study, Toomim et al. (2004) reported that participants with brain disorders could intentionally raise regional cerebral blood oxygenation at trained sites, with SPECT in a small subsample showing increased vascularity after 30 half-hour sessions. HEG is the training signal in that work rather than an independent measure of it, so the finding does not establish that brain training generally increases blood flow to the areas trained.
If a potential client has recently experienced a hemorrhagic stroke or an impact or acceleration/deceleration trauma, it may be prudent to delay neurofeedback training to avoid potentially exacerbating damage. Consulting the client's physician about appropriate timing is recommended. Conversely, beginning training as soon as is prudent may enhance the recovery process and encourage further healing.
Childhood attention disorders, behavioral disorders, and trauma
Children diagnosed with ADHD, oppositional defiant disorder (ODD), and related conditions have been shown to respond readily to neurofeedback training. In fact, neurofeedback for ADHD is the most extensively studied application of this modality (Arns et al., 2009; Van Doren et al., 2019). The evidence is not settled, however.
The double-blind, placebo-controlled ICAN trial found no significant difference on its primary outcome, a composite parent and teacher inattention rating (d = 0.01, p = .965), even though both groups improved substantially within-group (Arnold et al., 2021). Any statement about theta/beta efficacy should travel with that result. Separately, Joel Lubar, one of the leading researchers in this area, has suggested that family therapy interventions are essential for successfully resolving the child's ADHD condition (Lubar, 1995; Swingle, 2008).
Therefore, if a family is not willing or able to participate in family therapy, it may be counterproductive to train the child alone, an insight that extends to other childhood behavioral conditions. Similarly, childhood disorders of attentional and behavioral regulation often respond well to complementary interventions such as occupational therapy and vision therapy (New Visions School Annual Reports, 1992-1998), suggesting that a comprehensive intervention strategy may be more effective than neurofeedback alone.
Emotional and physical trauma
Individuals who have experienced emotional or physical trauma, are in abusive relationships, are experiencing racism, gender identity, or other types of discrimination, or are enduring a toxic work environment may need additional types of support and protection. Before initiating neurofeedback training, these issues should be addressed to ensure that training is effective and not simply masking ongoing harm.
Dementia
Dementia is a progressive decline in cognitive ability accompanied to varying degrees by changes in emotional and behavioral functioning. Various dementias can be characterized as having prodromal, early, middle, and late stages. The delivery of neurofeedback may be most beneficial during the prodromal and early stages, when the client can more consistently cooperate with the practitioner and sustain attention to the feedback stimuli.
Severe mental illness
Some mental illnesses are so severe that they may preclude the client from paying sufficient attention to feedback stimuli. Examples include schizophrenia and bipolar disorder whose symptoms have not yet responded to treatment. In such cases, the neurofeedback provider can collaborate with other treatment providers to deliver training during intervals when the illness has abated. As discussed below, some mental illnesses show exacerbation and remission patterns: although training might best be deferred during exacerbation, neurofeedback may be effectively delivered during remission.
Significant instabilities
Neurofeedback is best conducted when the client is in a relatively steady state, when they and their world are not already changing in a significantly problematic direction. If a client is rapidly declining due to a physical or mental condition, or if their life is undergoing major upheaval in social or material resources, it may be wise to postpone training. Similarly, significant variability, major "ups and downs" in mental or emotional condition, or unpredictable disruptions in social, work, or living circumstances, suggests that a better response to training is likely once stability improves.
Sometimes, however, a client may already be showing improvement before neurofeedback begins. In that case, training may proceed because it may accelerate or add benefit to whatever is already driving improvement. Nevertheless, ethical practice dictates that the practitioner review the improving trend with the client before beginning, allowing them to choose whether to wait and see if the current trajectory achieves their goals or whether remaining issues warrant neurofeedback.
Cautions
Paul Swingle (2015) outlined interpersonal cautions (e.g., trauma survivors) and interventional cautions (e.g., relaxation-induced anxiety) that could rise to the level of contraindications. Below are two clinical pearls from his excellent Adding neurofeedback to your practice: Clinician's guide to ClinicalQ, neurofeedback, and braindriving:
If the prescribing physician frequently changes medication type and dosage, it will likely sabotage training. Once a new medication has been started, it takes 3-6 weeks to become fully active. If EEG neurofeedback is started immediately, the results are questionable. What is causing changes for the better or worse? Is it the medication? Is it the training? Or is it a combination of the two? Never train an artifact: An entire training session can be in vain if muscle tension or eye movements are skewing the EEG. Z-score training targets can shift from normalizing real EEG component Z-scores to artifact reduction. Excessive artifacts often have the highest power Z-scores, and sEMG often lowers Z-score coherence; be watchful of electrodes near the temporomandibular region (T3, T4, F7, and F8). The raw EEG must be reviewed before training begins. Note that some artifact is normal; perfection is not possible. (p. 277)
Adverse effects
Intermittent assessment of client progress during the session provides an opportunity to detect unwanted side effects of training such as sedation, overarousal, headache, or excessive muscle tension. Once identified, these side effects can be addressed and minimized to prevent them from interfering with training success or persisting beyond the session. Please see the Cautions section in the Alpha-Theta unit for a detailed discussion of negative reactions to A-T training.
The ethical principle at stake is nonmaleficence, the obligation to do no harm. Reported adverse effects include excessive arousal, excessive sedation, anxiety or irritability, headache, and emotional abreaction (Hammond, 2011). Although consensus suggests that unwanted side effects are probably mild, infrequent, and brief (cf. Luctkar-Flude & Groll, 2015), neurofeedback providers disagree about the level of risk. This disagreement may partly reflect differing training protocols, varying client populations, and different thresholds for reporting (e.g., Rogel et al., 2015). However, adverse effects may be prolonged unless you adjust the training protocol that was in use when they appeared.
How do adverse effects become apparent? During initial assessment, the practitioner can inquire about whether the client has ever experienced adverse effects from any treatment and about their general level of sensitivity. After training has begun, the practitioner should remain alert to EEG or psychophysiological signs, behavioral indicators, and client statements that may suggest an adverse reaction. EEG signs include patterns of excessive high-beta (suggesting overarousal) or excessive low-frequency activity (suggesting sedation). Peripheral psychophysiological changes, in EMG, skin temperature, skin conductance, breathing pattern, heart rate, or HRV, may also signal adverse reactions.
Behavioral indicators include changes in motor behavior (moving more slowly or quickly), changes in speech production (rate, volume, or content suggesting strong emotions), untoward cognitive changes (grogginess, racing thoughts), physical experiences (unsteadiness), or behavioral associations (ideas about going to bed, pursuing conflict, or engaging in harmful activities). Regardless of the modality in which an adverse sign appears, the practitioner should immediately follow up by asking the client about their current condition.
If the client has experienced a change for the worse, determining whether to attribute it to neurofeedback can be challenging. This may require observing a pattern across several sessions. The practitioner should inquire about the client's own attribution and what might help alleviate the effect. Some clients may be more prone to adverse effects.
In a clinical commentary, Matthews (2007) named a different set of risk markers, namely blood glucose abnormality, serious brain injury, and high IQ, and reported that such patients may fatigue early, tolerate only a few minutes of training at a time, and show "transient, site-specific functional decline" if overtrained. Clinical experience also points to caution with severe anxiety, PTSD, dissociative disorders, personality disorders, and severe mental illness such as bipolar disorder and schizophrenia, although we could not locate a source for that list.
Rogel et al. (2015), in a double-blind, sham-controlled study of 30 healthy undergraduate volunteers trained across ten sessions, found that side effects occurred even in normal undergraduates and that the "Sensory Motor Rhythm protocol seems to be the most sensitive to side effects." More side effects appeared among those who received SMR feedback than those who received upper alpha feedback, with the latter group showing about the same level of side effects as the sham-control group. Rogel et al. recommended that practitioners use signed informed consent, ask clients about side effects, and document reports of side effects. Protocol characteristics may also be associated with adverse effects: training that increases theta may worsen ADHD symptoms (Lubar & Shouse, 1976), protocols training theta increases and SMR decreases may increase epileptiform activity (Lubar et al., 1981), protocols that increase power may be more likely to produce undesirable results (Hammond & Kirk, 2008), and training continued past the point of task fatigue may be associated with side effects, particularly in vulnerable patients (Matthews, 2007).
Deep state training in which feedback rewards lower frequencies at occipital or parietal sites may also be related to emotional states requiring urgent attention (Martins-Mourao & Kerson, 2016). These authors recommend that practitioners providing alpha/theta training be competent in treating abreactions and formulate an emergency plan ahead of time.
Prevention of adverse effects is an important goal. Given the above discussion, downtraining EEG bands may be a useful initial protocol. Following downtraining, you can introduce protocols that reinforce frequency bands.
Consider preliminary peripheral biofeedback training before introducing EEG biofeedback, and begin neurofeedback when the client's condition and circumstances are reasonably stable. Gradually increase training duration to avoid premature overtraining. Common protocols that initially focus on SMR along the sensorimotor strip or occipital alpha training before providing feedback for upper theta rhythms may reduce risk. Z-score training, which trains EEG values toward the normal range, may also minimize the likelihood of side effects.
If adverse effects appear, several strategies can be considered. First, interview the client in detail about the side effects: what they are, when they began, and whether they resemble experiences occurring outside training. Based on this information, protocol modifications may include adjusting segment duration, total session length, rate of feedback, or type of feedback (e.g., eyes closed versus eyes open, or the specific quality of visual or auditory feedback). The protocol itself may also be changed, for example, from amplitude reinforcement to downtraining, from conventional amplitude protocols to z-score protocols, or from standard frequency band feedback to slow cortical potential approaches. A core principle is to avoid treating conditions for which the practitioner lacks training or supervision, as this risks missing adverse effects, misattributing them to neurofeedback, or managing them suboptimally.
Key Takeaways
Neurofeedback contraindications include recent brain trauma, childhood behavioral disorders without family therapy involvement, unaddressed emotional or physical trauma, advanced dementia, severe mental illness during exacerbation, and significant life instabilities. Adverse effects such as excessive arousal, sedation, anxiety, headache, and emotional abreaction require vigilant monitoring through EEG signs, behavioral indicators, and client self-report. Prevention strategies include starting with downtraining protocols, gradual session length increases, and beginning training only when the client's condition is reasonably stable.
Reading/interpreting session reports/graphs
For some clients, generating statistics for EEG variables at the end of each training segment can be extremely informative. Most software platforms make this easy, since data can be copied and pasted to an Excel file before continuing to the next segment. The data can also be saved for later artifacting and graphing if more precise values are needed. Building an Excel template in advance allows the practitioner to paste data from session trials and automatically add new data points to a running graph. Even using unartifacted data, these graphs can show the client how their performance is changing from segment to segment in a tangible, motivating way.
Concluding a Session
A neurofeedback session typically concludes with several steps, some occurring while the client is present and others after they leave.
With the Client Present
Session post-training baseline EEG
Some practitioners collect session post-training baseline data to compare with pre-training data from the start of the session. The rationale is to investigate whether EEG values have shifted in a desirable direction. If collected, these data allow the practitioner to graph session-to-session trends in both pre-training and post-training baselines, as well as change scores (the difference between pre- and post-training values).
Removing electrodes
The practitioner removes the electrodes and can use a facial tissue or cotton ball with a small quantity of isopropyl alcohol to remove residual electrode paste. The client may then wish to arrange their hair or replace jewelry, either in the training room or an adjacent bathroom.
Debriefing
It can be helpful for the practitioner to ask open-ended questions about the client's experience of the session, following up with more specific questions as needed to clarify clinically useful information.
Home practice instructions
The client may be given tasks to complete before the next session. These may include self-monitoring of emotional states, cognition, somatic experience, and specific behaviors in specific situations. Homework may also include practice with supplementary biofeedback devices (e.g., HRV, temperature, skin conductance, respiration), mindfulness meditation, voluntary practice of states achieved during neurofeedback in particular situations, or supplementary electronic devices (e.g., audio-visual entrainment stimulation, micro-electrical stimulation).
Because generalization must be engineered rather than assumed, home practice is also where you build the bridge to daily life. Ask the client to carry a written If-Then plan that names a trigger and the state-entry routine that answers it, and encourage brief self-observation notes about which strategies felt steadying. Reviewing those notes at the next session gives you metacognitive information no graph can supply (Anderson & Davis, 2025b; Stokes & Baer, 1977).
HRV biofeedback practice
Portable HRV biofeedback devices like the Institute of HeartMath's Inner Balance allow clients to train whenever they choose, making between-session practice more accessible and reinforcing the self-regulation skills developed in the clinic.

Apps like Optimal HRV allow you to assess your resonance frequency and perform biofeedback and mindfulness training.
 |
 |
Temperature biofeedback practice
Encourage your clients to monitor their hand temperature using inexpensive alcohol thermometers to see whether their practice resulted in warming or cooling.
Rating scales and questionnaires
Before the client leaves, the practitioner may ask them to quantify various aspects of their post-training state using rating scales developed for the individual client, standardized rating scales, or brief standardized questionnaires.
After the Client Leaves
Clean-up
Electrodes and desk surfaces should be cleaned as soon as possible following a session for infection control. Depending on the office, it may be wise to store equipment where it is safe from damage.
Documenting the session
Documentation as soon as possible after a session is recommended. If the practitioner has already written notes on the pre-session form, the amount of additional documentation may be modest. On the other hand, the practitioner may want to elaborate entries or type notes into a word processing file. In addition to detailed session notes, a running table showing the dates of training sessions along with the montage(s) used is a valuable clinical record.
Post-session artifacting
Depending on the level of detail desired, there will be pre-training baseline data, data from multiple training segments, and post-training baseline data to artifact. After removing artifacts and saving the cleaned data file, the practitioner can generate accurate statistics for copy-and-paste into an Excel file. The resulting graphs efficiently show how the client is responding to training and are ready to review at the next session or to include in any written report for the client, their healthcare provider, or insurer.
Reading and Interpreting Session Graphs
Introduction
This section covers the graphic representation, visual inspection, and interpretation of session graphs, skills that are central to data-driven decision-making in neurofeedback. An essential principle is that neurofeedback should always be guided by quantitative data, drawn from initial assessment, training sessions, end-of-training recordings, and follow-up data. The discussion that follows is based largely on Cooper et al.'s (2019) applied behavior analysis text.
Baseline logic
In addition to informing protocol selection, the initial EEG assessment provides a pre-training baseline against which training and post-training EEG values can be evaluated. However, these initial assessment data typically represent only a single data point rather than a series of baseline values. Although rarely discussed in the neurofeedback literature, this limitation is significant: a single data point cannot reveal whether baseline data are stable, trending upward or downward, or highly variable.
Figure 1 shows three hypothetical initial assessment baseline points with a possibly increasing trend and significant variability. One interpretation is that the pre-training data are unstable and suggest that improvement might continue even without neurofeedback training. Variability alone complicates interpretation of subsequent data because some uncontrolled factor may be influencing both the baseline and training-phase data. The practical lesson is to exercise caution when interpreting training effects against a single baseline data point.
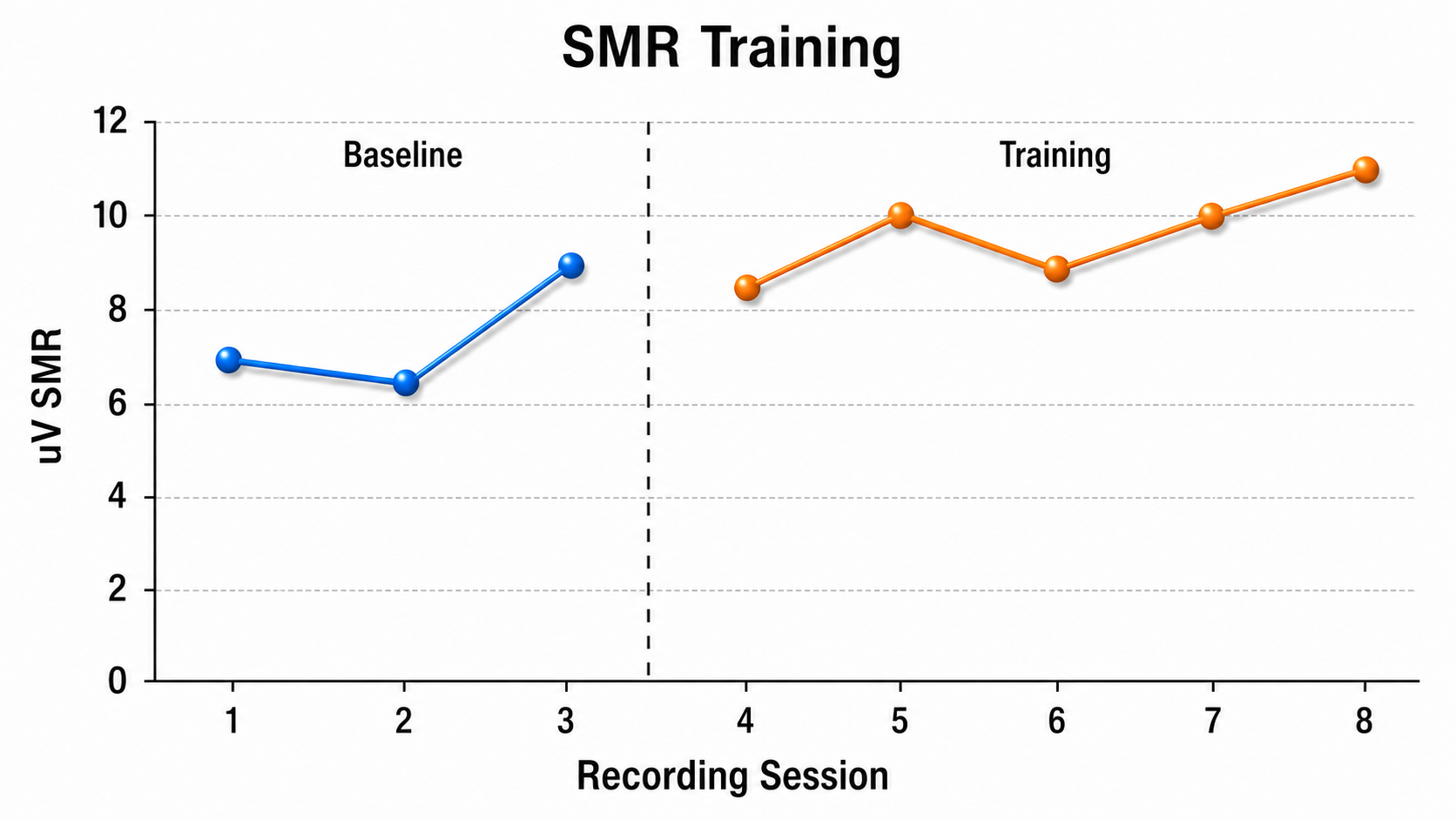
Because clinical neurofeedback practice rarely allows for more than a single initial assessment, the practitioner typically assumes that these data are stable and can serve as a valid benchmark. However, the caution raised here, that interpretation of training-phase changes should account for the inherent limitations of a single baseline data point, is worth keeping in mind throughout a course of treatment.
Session data
Session data should be based on the same EEG variables that were important during the initial baseline assessment. Apples should be compared to apples: average SMR amplitude from baseline should be compared to average SMR amplitude from training sessions, for example.
When to collect session data
An important consideration is when to save EEG data during training sessions. Data can be collected, saved, and graphed from a pre-training baseline period, training periods or segments, and a post-training baseline period. Data collected during sessions may come from before feedback begins, during periods of feedback, and after feedback concludes.
Pre-training baseline session data
If practitioners graph and save data from training sessions, they most commonly do so from a pre-training baseline. This approach allows both practitioner and client to answer two questions. First, is neurofeedback producing a stable change in EEG values, the core objective of training? Data from training periods and post-training baselines answer this question less well because training is actively perturbing the EEG in the first case, and insufficient time has elapsed to assess stability in the second. The second question involves setting appropriate thresholds for a given session.
Figure 2 represents hypothetical data in which session pre-training baseline data show a trend of increasing SMR amplitude, with values higher than those from the initial assessment. Visual inspection of this graph is consistent with neurofeedback increasing SMR production relative to pre-training levels. Note the limit that the previous subsection established: with a single initial assessment point, the graph cannot rule out a trend that was already under way, so "consistent with" is as far as these data reach.
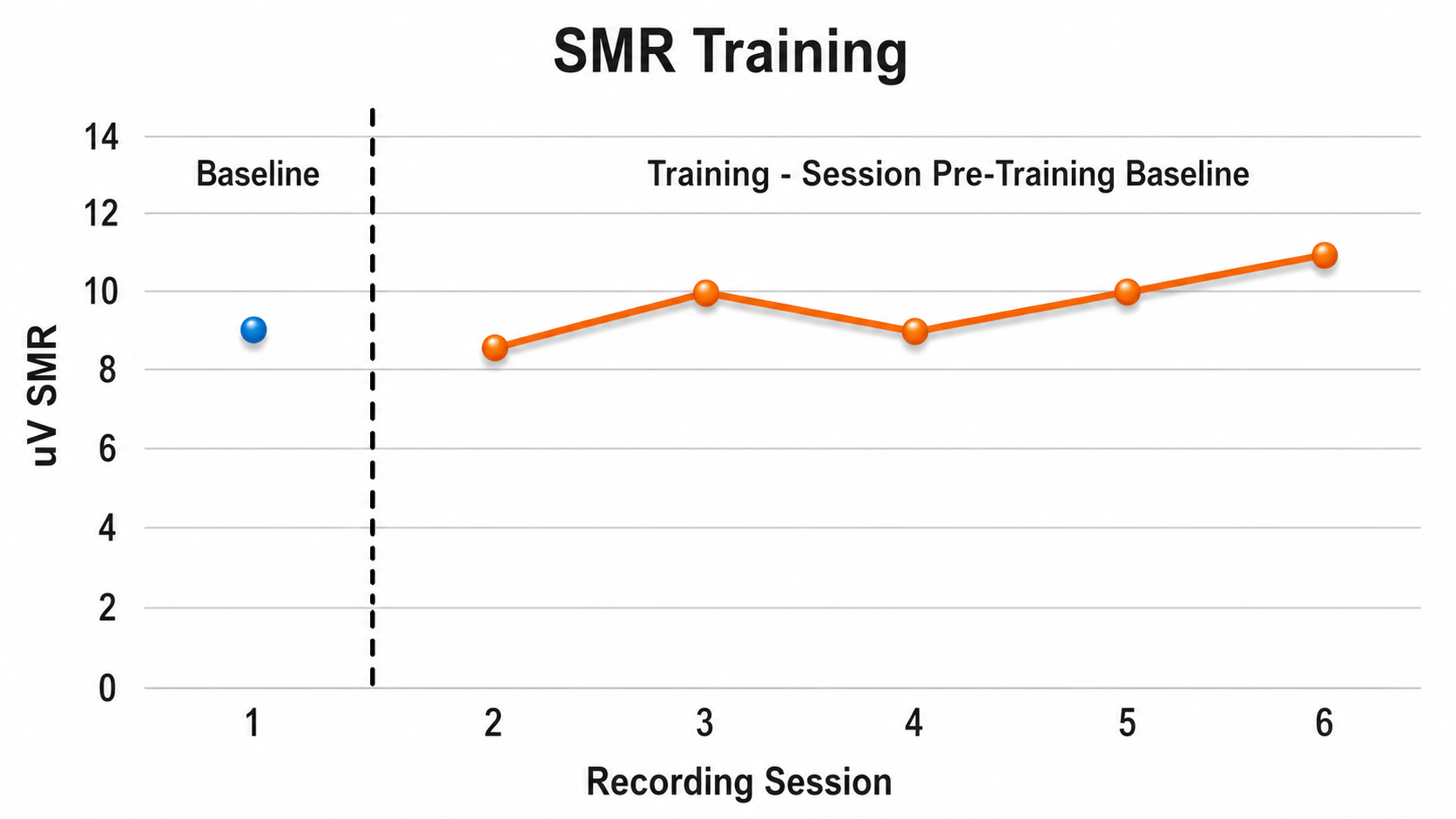
Should pre-training data be collected at every session? Collecting data each time identifies variability and trends in greater detail. For example, factors causing variability (such as inconsistent sleep) might be identified and minimized. The cost is approximately 2 minutes of data collection plus subsequent artifacting and graphing time, though these steps become very efficient with practice. If collecting data for only a sample of sessions, it is best to do so at equal intervals (e.g., every other session or every fifth session).
Data from training periods within a session
Most software platforms make it easy to generate EEG data before, during, or after training. During a session, unartifacted data can be immediately copied into a prepared Excel template to produce a graph. While these data can be saved for post-session artifacting and more precise graphing, it can be useful to immediately see whether training is producing EEG changes during the session, particularly when recording from 10-20 sites with minimal artifact during an eyes-closed condition.
There are several benefits to graphing and displaying within-session data. They can encourage client engagement and assist the practitioner in coaching. Trends in these data can also inform the practitioner when to discontinue training for that day. For instance, if changes plateau or decline toward the end of a series of training periods (see Figure 3). The fundamental question these data answer is whether, during this particular session, training is producing an EEG change.
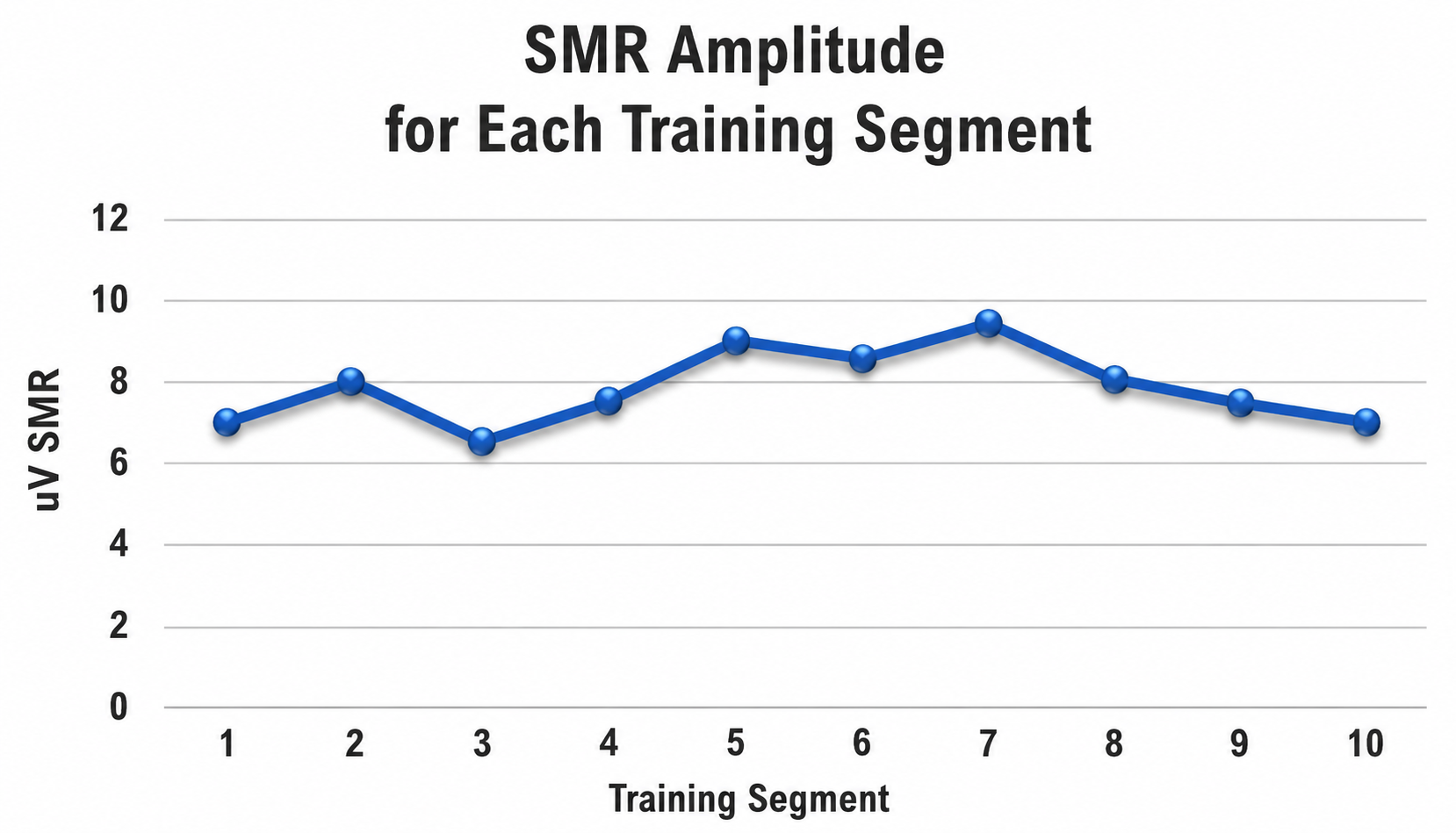
Post-training baseline session data
After the training portion of a session concludes, a brief post-training baseline can be collected and contrasted with pre-training baseline data to assess whether a short-term change occurred from the beginning to the end of the session. Either absolute values or z-scores can be compared, or change scores can be calculated (see Figure 4). However, clinicians should exercise caution: post-training data may be unstable immediately after training ceases and may also reflect fatigue rather than meaningful change.
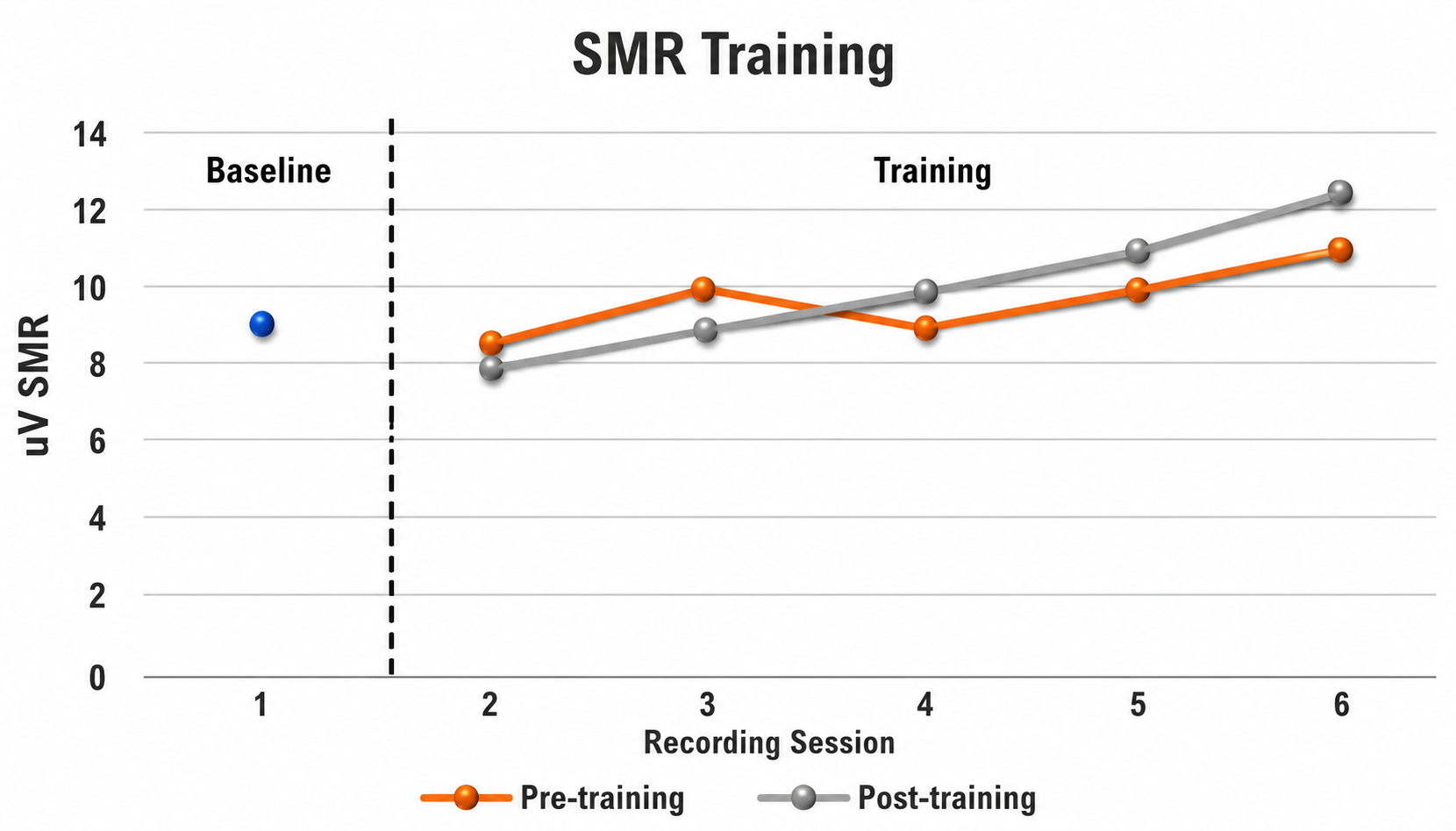
Decision-making
Session data graphs inform decision-making both before introducing feedback and during the feedback segments of a session. Before beginning training, the practitioner should examine whether the graph of session pre-training baseline values shows a value that may influence thresholds or the protocol montage for that session. Figure 5 shows a trend that increases after baseline, then stabilizes. The leveling off may suggest that SMR training can conclude and a new montage can be introduced.
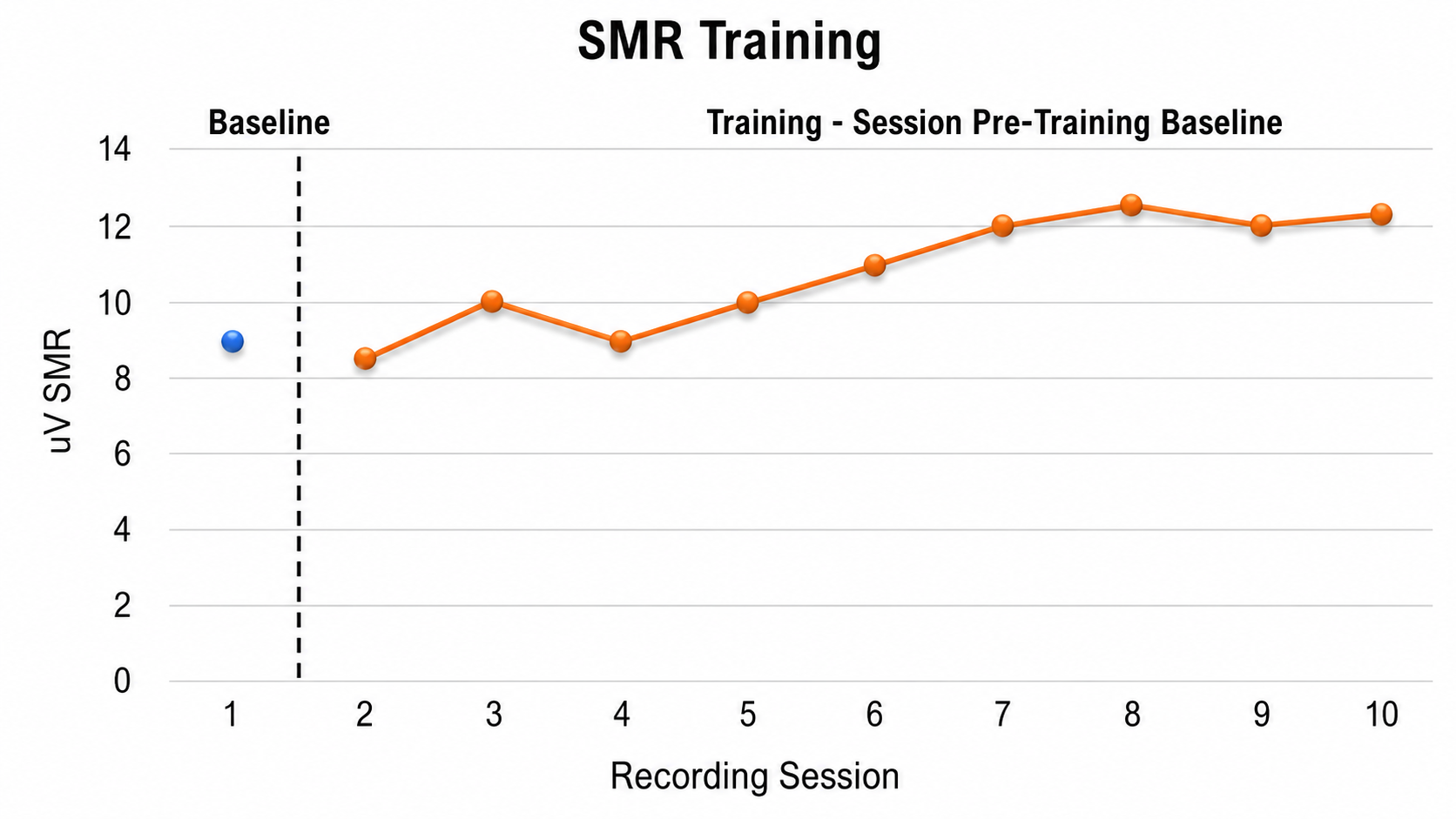
Examining graphs of within-session EEG data can also help decide when to change thresholds or discontinue training for that day.
End of training and follow-up data
Graphs of session data help the client and practitioner decide when to discontinue neurofeedback training. Documenting the outcome by collecting and graphing EEG data during a session devoted entirely to post-training assessment (with no scheduled neurofeedback) provides valuable outcome data that can be contrasted with initial assessment results. Follow-up data collected at later time points can address whether gains made during training are preserved over longer periods and can inform decisions about whether additional training might help reinstate earlier gains.
Non-EEG session graphs
HRV training is a frequent adjunct to neurofeedback training and may generate data for each session. Questionnaires related to subjective emotional state or functional behavior (e.g., study time) may be completed by the client or by significant others such as a parent, teacher, or spouse. Client-specific rating scales may also be used. Graphing these data alongside EEG data answers a crucial generalization question: "Is the improvement seen in the EEG reflected in how the client feels, in their cognitive performance, or in behaviors that matter in specific situations?"
Summary
In summary, this section has focused on EEG data collected during individual sessions: where in the session those data come from, what questions they can answer, and how they inform decision-making during and after neurofeedback training. The central message is that systematic collection, graphing, and interpretation of session data transforms neurofeedback from an intuitive practice into a data-driven clinical science.
Key Takeaways
Session graphs are central to data-driven decision-making in neurofeedback. Pre-training baseline data best answer whether training is producing stable EEG changes. Within-session data help decide when to adjust thresholds or discontinue training. Post-training data should be interpreted cautiously due to instability. Graph types include pre-training baselines, within-session training segments, post-training baselines, and non-EEG measures such as HRV, questionnaires, and cognitive performance tests.
Conclusion
This unit has described the steps practitioners typically follow during a neurofeedback session, from preparation and check-in through training and post-session documentation. Throughout, the emphasis has been on a client-centered approach that values both quantitative and qualitative data. We have covered how to secure a trustworthy signal before training begins, how the learning processes of reinforcement, conditioning, and metacognition turn that signal into a durable skill, how to monitor each client's idiosyncratic response to training, how to make data-driven decisions about threshold adjustment within and between sessions, and how to recognize and manage artifacts, medication effects, contraindications, and adverse effects.
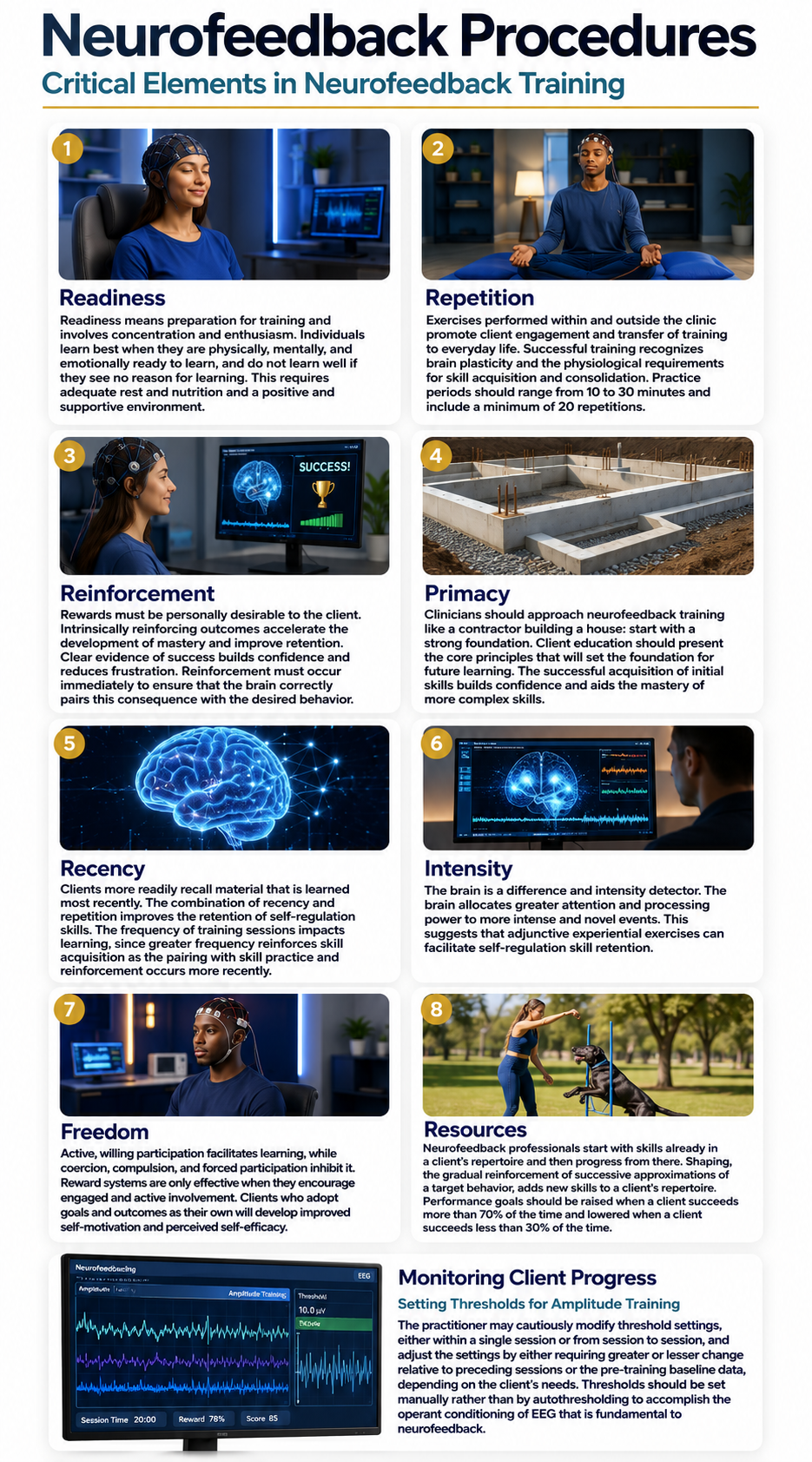
Cutting-Edge Topics in Neurofeedback Procedures
Advances in Real-Time Artifact Rejection
Machine learning algorithms are increasingly being integrated into neurofeedback platforms to detect and reject artifacts in real time, reducing the burden on practitioners to manually identify contamination during training sessions. These systems can distinguish between genuine EEG patterns and artifacts from EMG, eye movement, and cardiac sources with growing accuracy, potentially improving the quality of feedback delivered to clients.
Closed-Loop Neurofeedback and Adaptive Thresholding
Emerging research is exploring closed-loop systems that go beyond simple auto-thresholding by incorporating reinforcement learning principles. Unlike traditional auto-thresholding (which Sherlin et al., 2011, cautioned against), these newer approaches attempt to optimize threshold adjustments based on the client's learning trajectory rather than simply maintaining a fixed percentage of reward. While still experimental, these systems represent an attempt to reconcile the convenience of automation with the operant conditioning principles that underpin effective neurofeedback.
Mindfulness-Based Neurofeedback
A growing literature pairs mindfulness instruction with EEG or fMRI neurofeedback on the reasoning that the two approaches target the same capacities from opposite directions, one through introspective training and the other through an external signal. A systematic review of this work found the most robust EEG evidence for modulation of theta-band activity, but reported a lack of evidence for transfer effects, inadequate sham control in most studies, and that "the mental health benefits of mbNF have not been established" (Treves et al., 2024). Practitioners interested in this direction should treat it as promising rather than established.
Integration of Peripheral Biofeedback Monitoring
Contemporary systems increasingly combine EEG neurofeedback with simultaneous monitoring of peripheral physiological signals such as heart rate variability, skin conductance, and respiration. This multimodal approach provides practitioners with a richer picture of the client's arousal state during training and may help detect adverse effects earlier. Research is examining whether this integrated monitoring can improve clinical outcomes compared to EEG-only training.
Check Your Understanding
- Why do Sherlin et al. (2011) argue that automatic thresholding violates the principles of operant conditioning, and what specific problems can it create for reward and inhibit signals?
- Describe the steps a practitioner should take before beginning a neurofeedback session to ensure they are adequately prepared to monitor client progress.
- Compare and contrast referential (monopolar) and sequential (bipolar) montages, including the strengths and limitations of each approach.
- What are the key considerations when deciding whether neurofeedback training is contraindicated for a particular client, and what conditions warrant special caution?
- Explain how session graph data (pre-training baseline, within-session training, and post-training baseline) can inform decision-making about threshold adjustments and protocol changes across a series of neurofeedback sessions.
Assignment
Now that you have completed this unit, explain the role of shaping in neurofeedback training. How do you manually adjust reward thresholds?
Glossary
A (auricular): International 10-20 system earlobe reference placement.
absolute power: the power (amplitude squared, in μV²) within a frequency band at a single electrode site, expressed in physical units rather than as a share of the total. In qEEG reports it is typically compared against an age-matched normative database rather than against activity at other sites.
active electrode: the electrode placed over a site of interest, such as Cz, whose potential is compared with that of the reference electrode. In a balanced differential amplifier the active and reference inputs are electrically identical, so the labels describe the recording plan rather than a property of the sensor.
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with relaxed wakefulness. Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
alpha synchrony threshold: a criterion for receiving feedback that increases alpha amplitude over the scalp by rewarding simultaneous increases in alpha amplitude at two or more sites.
alpha variability: fluctuation in alpha amplitude over time, expressed in standard deviations.
alpha variability threshold: a criterion for receiving feedback that reduces alpha amplitude fluctuation measured in standard deviations (SDs).
amplitude: the strength of the EEG signal, measured in microvolts (μV). Amplitude is not power: power is amplitude squared and is expressed in μV², so amplitude-based and power-based thresholds and ratios are not interchangeable.
arousal: a process that combines alertness and wakefulness, produced by at least five neurotransmitters, including acetylcholine, histamine, hypocretin, norepinephrine, and serotonin.
artifacting: the review of a raw EEG record and removal of epochs contaminated by physiological or exogenous artifact before statistics are calculated.
artifacts: false signals like 50/60Hz noise produced by line current.
asynchronous waves: oscillating electrical potentials created when neurons depolarize and hyperpolarize independently.
band-pass filter: a filter that passes only a specified frequency range, such as 4-7 Hz, and attenuates frequencies outside it.
benzodiazepine receptor agonist (BZRA) hypnotics: nonbenzodiazepine BZRAs like zolpidem (Ambien) that are prescribed to treat insomnia.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in both the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
bilateral synchronous slow waves: bursts of high-amplitude bisynchronous slow waves are a normal drowsiness pattern in children, called hypnagogic hypersynchrony. When intermittent bursts of high-amplitude slow waves appear in alert adults they are abnormal, but they are nonspecific and nonlocalizing and most often reflect a mild-to-moderate diffuse encephalopathy rather than a lesion confined to deep midline structures.
bipolar (sequential) montage: a recording method in which each channel compares two active electrodes with no shared reference; successive channels are chained so that each shares one electrode with the next. See also sequential (bipolar) montage. Note that "bipolar" carries a second, distinct meaning in peripheral biofeedback, where it denotes two active sensors plus a ground.
bridging artifact: a short circuit between adjacent electrodes due to excessive application of electrode paste or a client who is sweating excessively or arrives with a wet scalp.
C (central): sites in the International 10-20 system that detect frontal, parietal-occipital, and temporal EEG activity.
cable sway: artifact caused by the movement of electrode cables.
canthi: the inner and outer corners where the upper and lower eyelids meet; the outer canthi are common electrode sites for tracking horizontal eye movements.
cardioballistic (pulse) artifact: small, pulse-synchronous voltages and baseline shifts caused by cardiac-related blood volume and lead movement; frequently seen with dry electrode caps, particularly at F3 and F4.
channel: one differential comparison between an active and a reference electrode, delivered as one amplifier output. A ground electrode is required for the recording, but it is shared across all channels rather than being a component of any single one.
classical conditioning: an unconscious learning process in which a neutral stimulus repeatedly paired with a stimulus that naturally produces a response comes to elicit a similar response on its own.
contiguity: the immediacy of feedback relative to the neural event that produced it; shorter delays strengthen learning.
contingency: the reliability with which a feedback event depends on the occurrence of a target neural state.
default mode network (DMN): a set of interacting brain regions, including the posterior cingulate cortex, that is prominent at rest and shows reduced activity during focused attention and mindfulness practice.
delta rhythm: 1-4-Hz oscillations generated by thalamocortical neurons during stage N3 sleep (formerly stages 3 and 4). Some sources start the band at 0.5 Hz; activity below about 1 Hz is treated in this curriculum as the slow cortical potential or infra-low range.
derivation: the assignment of two electrodes to an amplifier's inputs 1 and 2.
discrimination: the learned ability to respond to a danger cue while withholding that response to a safety cue.
drowsiness artifact: the appearance of stage N1 or N2 sleep features in a recording intended to capture waking EEG. Occipital alpha attenuates, frontal theta increases, EMG and beta decline, slow roving eye movements produce slow waveforms of opposite polarity at F7 and F8, and the posterior dominant rhythm may slow by 1 to 2 Hz before vertex waves appear.
dry electrode cap: an electrode array whose sensors contact the scalp without gel or saline, using small rounded points or spring-loaded contacts; faster to apply but more susceptible to movement and pulse artifacts.
dual-action antidepressants: medications like duloxetine (Cymbalta) that activate 5-HT1 receptors to produce antidepressant and anxiolytic effects, while they blockade 5-HT2 (agitation, restlessness, and sexual dysfunction) and 5-HT3 (nausea, headache, and vomiting) receptors to minimize their side effects.
dynamic z-score thresholds: thresholds that deliver feedback almost 50% of the time, calculated on shorter periods (e.g., 10 seconds) than automated thresholds (60 seconds).
EEG artifacts: noncerebral electrical activity in an EEG recording can be divided into physiological and exogenous artifacts.
EEG topography: display of EEG values on a map of the cortical surface to show the spatial distribution of activity across recording sites.
electrode pop artifact: sudden large deflections in at least one channel when an electrode abruptly detaches from the scalp.
electro-ocular artifact: contamination of EEG recordings by potentials generated by eye blinks, eye flutter, and eye movements.
electro-oculography (EOG): surface recording of eye activity using electrodes placed around the eyes to capture the potential changes produced by blinks and eye movements, used to detect and correct ocular artifact in the EEG.
EMG artifact: interference in EEG recording by volume-conducted signals from skeletal muscles.
exogenous artifacts: noncerebral electrical activity generated by movement, 50/60 Hz and field effect, bridging, and electrode (electrode "pop" and impedance) artifacts.
extinction: the weakening or disappearance of a conditioned response when the conditioned stimulus no longer predicts its outcome; Pavlov argued that extinction is new learning rather than forgetting.
F (frontal): sites in the International 10-20 system that detect frontal lobe EEG activity.
fast cortical potentials: EEG rhythms that range from 0.5 Hz-100 Hz. The main frequency ranges include delta, theta, alpha, sensorimotor rhythm, and beta.
fast Fourier transform (FFT): a mathematical algorithm that decomposes a time-domain signal into its frequency components, requiring a minimum of 1 second of data and commonly 2 seconds or more.
filter order: the number of samples used to calculate a digital filter's output; higher orders sharpen the filter's transitions and increase precision but also increase computation time and delay.
finite impulse response (FIR) filter: a nonrecursive digital filter that delays all frequencies equally, preserving waveform shape at the cost of greater computational demand and longer latency.
first-generation antipsychotics (FGAs): FGAs like chlorpromazine (Thorazine) are prescribed to treat the positive symptoms of schizophrenia and exert their effects through D2 receptor blockade.
focal waves: EEG waves detected within a limited area of the scalp, cerebral cortex, or brain.
Fp (frontopolar or prefrontal): sites in the International 10-20 system that detect prefrontal cortical EEG activity.
frequency: how often a wave occurs within 1 second, measured in hertz (Hz) and once called cycles per second.
gel bridge: an unwanted conductive path formed when excess conductive gel connects adjacent electrodes, short-circuiting channels and distorting amplitude and topography; it cannot be repaired without removing the cap and washing the hair.
gel cap: a fabric or silicone electrode cap with integrated electrode wells filled with conductive gel to create low-impedance scalp contacts.
ground electrode: an electrode, commonly on an earlobe or mastoid, that supplies the amplifier's input stage with a common voltage reference and thereby enables common-mode rejection. It is shared across all channels and is not a component of any single channel.
hemoencephalography (HEG): a training modality that monitors regional cerebral blood oxygenation, typically by near-infrared spectroscopy, and feeds it back to the client.
hertz (Hz): unit of frequency measured in cycles per second.
high beta: fast beta activity commonly associated with hyperarousal, anxiety, worry, and rumination. Its boundaries vary by system and by author; the qEEG findings reported in this unit concern roughly 25 to 30 Hz, while Clarke et al. (2001) analyzed beta from 12.5 to 25 Hz. Excess frontal beta has been reported to be "associated with frontal lobe self-regulation and inhibition control."
high-frequency filter (HFF): a low-pass filter that attenuates frequencies above a cutoff frequency.
high-pass filter: a filter that passes frequencies above its cutoff point, such as 1 or 2 Hz, while attenuating slower components.
impedance (Z): complex opposition to an AC signal measured in Kohms.
impedance meter: a device that uses an AC signal to measure impedance in an electric circuit, such as between active and reference electrodes.
impedance test: automated or manual measurement of skin-electrode impedance.
infinite impulse response (IIR) filter: a recursive digital filter that feeds part of its output back into its input, achieving sharp cutoffs efficiently but introducing frequency-dependent phase distortion.
inhibit threshold: criterion for suspending feedback, analogous to a limbo bar, designed to decrease bandpass amplitude.
inion: the bony prominence on the back of the skull.
intermediate-acting benzodiazepines: benzodiazepines with mean half-lives from 15-80 hours prescribed for the management of anxiety.
International 10-20 system: a standardized procedure for 21 recording and one ground electrode on adults.
irregular waves: successive waves that constantly alter their shape and duration.
irreversible MAO inhibitors (MAOIs): MAOIs like selegeline (Emsam) that form permanent bonds with the MAO enzyme and are prescribed for major depressive disorder (MDD).
latency: the total time delay between when brain activity occurs and when feedback about it is presented to the client.
long-acting benzodiazepines: benzodiazepines like diazepam (Valium) with mean half-lives ranging from 10-80 hours prescribed to manage anxiety.
low-pass filter: a filter that passes frequencies below its cutoff point, such as 30 Hz, while attenuating faster components.
low resolution electromagnetic tomography (LORETA): Pascual-Marqui et al.'s (1994) distributed inverse solution, which estimates a smoothly varying three-dimensional current density throughout the brain volume from multichannel scalp EEG. Clinical neurofeedback commonly applies it to 19-channel 10-20 recordings, but the method is not restricted to any electrode count, and localization accuracy improves substantially with higher-density arrays.
magnitude: in an FFT display, the amplitude of a frequency component expressed over time.
mastoid bone: the bony prominence behind the ear.
metacognition: the capacity to observe, evaluate, and regulate one's own mental processes; it includes metacognitive knowledge (understanding how one thinks and learns) and metacognitive control (using that understanding to guide attention, emotion, and behavior).
microvolt (μV): a unit of amplitude (signal strength) that is one-millionth of a volt.
mindfulness: systematic training in attentive, non-reactive awareness, operationally described as the self-regulation of attention toward present-moment experience combined with an orientation of openness, curiosity, and non-judgment.
Mindfulness-Based Stress Reduction (MBSR): a standardized 8-week program that translates mindfulness practice into health care contexts through formal practices and psychoeducation.
mixed opioid agonist-antagonists: drugs like pentazocine (Talwin) that are kappa agonists and weak mu antagonists that are prescribed for the management of pain.
monoamine oxidase (MAO): an enzyme that degrades and inactivates the monoamine neurotransmitters dopamine, norepinephrine, and serotonin.
monoamine oxidase inhibitors (MAOIs): antidepressant drugs that interfere with MAO's breakdown of monoamines and increase monoamine availability and are prescribed to manage major depressive disorder (MDD).
montage: a grouping of electrodes (combining derivations) to record EEG activity.
movement artifacts: voltages caused by client movement or the movement of electrode wires by other individuals.
nasion: the depression at the bridge of the nose.
negative punishment: a process that decreases an undesirable behavior by removing something desired, such as dimming a movie and lowering its sound when a child fidgets, or turning off a popular game following oppositional behavior.
negative reinforcement: a process that increases the frequency of a desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on acting.
nonmaleficence: the ethical obligation to avoid causing harm, one of the four principles of biomedical ethics.
notch filter: a filter that suppresses a narrow band of frequencies, such as those produced by line current at 50/60Hz.
O (occipital): sites in the International 10-20 system that detect occipital lobe EEG activity.
ohm (Ω): a unit of impedance or resistance.
operant conditioning: learning in which the consequences that follow a behavior alter the probability that the behavior recurs.
overlearning: continued practice after a criterion has been reached, which consolidates a skill and makes it more durable and more resistant to extinction.
P (parietal): sites in the International 10-20 system that detect parietal lobe EEG activity.
partial opioid agonists: drugs like buprenorphine (Subutex) that produce less-than-maximal analgesia and are prescribed to manage pain.
peak alpha frequency: the highest-amplitude alpha frequency (8-12, 8-13 Hz) within an epoch.
peak frequency: the frequency within a band at which the highest amplitude or power occurs.
percentage of success: a z-score training protocol in which a client receives feedback when a predetermined percentage of EEG components fall within a chosen range of standard deviations from normal.
phase distortion: the unequal delay of different frequencies by a filter, which shifts parts of the waveform in time and alters true timing relationships within the signal.
physiological artifacts: noncerebral electrical activity that includes electromyographic, electro-ocular (eye blink and eye movement), cardiac (pulse), sweat (skin impedance), drowsiness, and evoked potential.
polyphasic (multiphasic) wave: a wave that contains two or more deflections of opposite polarity from baseline.
polyspikes: a series of three or more consecutive spikes (≥ 10 Hz) that last a minimum of 300 milliseconds.
positive punishment: a process that decreases an undesirable behavior by adding an unwanted consequence, such as introducing a burst of static into the audio feedback when EMG artifact rises. Dimming a screen or lowering its volume removes an appetitive stimulus and is therefore negative punishment.
positive reinforcement: a process that increases the frequency of a desired behavior by making a desired outcome contingent on acting, such as playing a movie while the client increases low beta and decreases theta.
posterior cingulate cortex (PCC): a hub of the default mode network whose reduced engagement accompanies shifts toward focused, less self-referential awareness.
posterior dominant rhythm (PDR): the highest-amplitude frequency detected at the posterior scalp when eyes are closed.
power: amplitude squared, expressed in microvolts squared (μV²). Values in picowatts appear in some software only under the convention of a 1-ohm reference resistance, which must be stated whenever picowatts are used.
preauricular notch: the palpable depression just in front of the ear that serves as a landmark for proportional electrode placement.
preauricular point: the slight depression located in front of the ear and above the earlobe.
preverbal awareness: the sensory experience of the present moment that precedes its verbal description.
protocol: a rigorously organized plan for training.
pulse artifacts: noncerebral voltages due to mechanical movement of an electrode in relation to the skin surface due to the pressure wave of each heartbeat.
pure opioid agonists: drugs like morphine that produce maximal analgesia and are prescribed to manage pain.
Quantitative EEG (qEEG): digitized statistical analysis of the EEG, measuring amplitude or power within specific frequency bins and comparing the result against a normative database. Topographic brain mapping typically uses 19 or more channels, but abbreviated and single-channel applications exist, the theta/beta ratio at Cz being the validated example.
ratio-threshold: a criterion for receiving feedback that reinforces changes in the ratio of two EEG bandpasses.
readiness: a client's preparation for training, encompassing concentration and enthusiasm and resting on adequate rest, nutrition, and a supportive environment.
reference electrode: an electrode placed on the scalp, earlobe, or mastoid.
referential (monopolar) montage: a recording method that places one active electrode on the scalp and a neutral reference and ground on the ear or mastoid.
regular or monomorphic waves: successive waves with identical shapes. Regular waves may resemble sine waves (sinusoidal) or may be arched (resembling wickets), or saw-toothed (asymmetrical and triangular).
reinforcement: a consequence following a behavior that makes that behavior more likely to occur again in similar situations; whether a consequence reinforces can only be determined by measuring its effect on behavior.
relative power: the power in a frequency band expressed as a percentage of the power in the entire recorded band; also called percent power or normalized EEG.
repetition: repeated practice within and outside the clinic, which promotes engagement, consolidation, and transfer of self-regulation skills.
response generalization: the occurrence of a slightly different response to the same stimulus after learning.
reward threshold: a criterion for presenting feedback designed to increase brainwave amplitude, analogous to a hurdle.
rhythmic midtemporal theta of drowsiness (RMTD): a benign drowsiness variant, not an epileptiform pattern. It consists of notched or sharply contoured rhythmic theta waveforms over the midtemporal regions, often bitemporal and asymmetric, with the side of predominance shifting within and between recordings.
saline net: an electrode array of sponge or felt sensors hydrated with saline solution; rapid to apply but vulnerable to salt bridging if over-wetted.
salt bridging: an unintended electrical connection between neighboring electrodes caused by excess saline spreading across the scalp; unlike a gel bridge, it can be corrected by drying the scalp and hair, brushing out loose mineral salts, and re-applying a freshly hydrated net.
sampling rate: the number of measurements per second acquired by the amplifier, which sets the temporal resolution of the recording and the speed of filter output.
second-generation antipsychotics: SGAs like clozapine (Clozaril) are prescribed to treat the positive symptoms of schizophrenia and antagonize D2 receptors less effectively than D1 receptors and significantly less than 5-HT2 receptors.
selective norepinephrine reuptake inhibitors (SNRIs): drugs like atomoxetine (Strattera) that specifically interfere with norepinephrine reuptake for the management of major depressive disorder (MDD).
selective serotonin reuptake inhibitors (SSRIs): drugs like fluoxetine (Prozac) that specifically interfere with serotonin reuptake for the management of major depressive disorder (MDD).
sensorimotor rhythm (SMR): 12-15-Hz spindle-shaped rhythm, with a spectral peak usually around 12-14 Hz, detected over the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
sequential (bipolar) montage: a recording method that presents a sequence of comparisons between pairs of active electrodes attached to sites on the scalp, with no shared reference. See also bipolar (sequential) montage.
shaping: the gradual reinforcement of successive approximations of a target behavior; in neurofeedback, the stepwise tightening of a threshold as the client's performance improves.
short-acting benzodiazepines: benzodiazepines like alprazolam (Xanax) with mean half-lives that range from 2.5-12 hours prescribed to manage anxiety.
spike: a negative transient with a pointed peak at conventional paper speeds, 20-70-ms duration, and 40-100 μV amplitude.
spike-and-slow-wave complex: a spike followed by a higher amplitude slow wave at 3 Hz. In an absence seizure, the amplitudes are very high (e.g., 160 μV).
spindle waves: 11-16-Hz waves, most commonly 12-14 Hz, that originate in the thalamus and are the defining feature of stage N2 sleep.
spontaneous recovery: the reappearance of a conditioned response after extinction and a delay, taken as evidence that extinction is new learning rather than forgetting.
standardized LORETA (sLORETA): a refinement of LORETA that produces images of standardized current density, partitioning the intracerebral volume into 6,239 voxels at 5-mm spatial resolution, with exact localization for test point sources and no localization bias under noise.
stimulus generalization: the occurrence of a trained response in situations different from the one in which it was learned; the most important form of generalization for neurofeedback.
stratum corneum: the upper layer of the skin, whose gentle abrasion at an electrode site reduces impedance.
sum squash threshold: a criterion for receiving feedback that reduces bandpass amplitude over a wide scalp area by using inhibit thresholds on two channels using referential (monopolar) or sequential (bipolar) recording.
surface Laplacian (SL) analysis: a family of mathematical algorithms that provide two-dimensional images of radial current flow from cortical dipoles to the scalp.
sweat artifact: artifact resulting from sweat on the skin changing the conductive properties under and near the electrode sites.
swLORETA: a variant of LORETA that applies a lead-field weighting to improve noise robustness and sensitivity to deep sources (Palmero-Soler et al., 2007), rather than raising resolution generally.
temporal generalization: the persistence of a learned response after training has ended.
theta/beta ratio (T/B ratio): the ratio between 4-7 Hz theta and 13-21 Hz beta, measured at the vertex (Cz) in the studies that validated it (Monastra, Lubar, & Linden, 2001).
theta rhythm: 4-7-Hz rhythms generated by a cholinergic septohippocampal system that receives input from the ascending reticular formation and a noncholinergic system that originates in the entorhinal cortex, which corresponds to Brodmann areas 28 and 34 at the caudal region of the temporal lobe.
third-generation antipsychotics (TGAs): drugs like aripiprazole (Abilify) that is a partial agonist at D2 and 5-HT1A receptors and an antagonist at 5-HT2 receptors prescribed for the management of the positive and negative symptoms of schizophrenia.
tragus: the flap at the opening of the ear.
transient: a single wave or sequence of regular waves, called a complex, distinguishable from background EEG activity.
triphasic waves (TWs): medium-to-high-amplitude sharp transients that often involve a negative-positive-negative sequence. TWs are distributed diffusely and symmetrically with frontal predominance.
vertex (Cz): the intersection of imaginary lines drawn from the nasion to inion and between the two preauricular points in the International 10-10 and 10-20 systems.
Wernicke's area: a region of the posterior superior temporal lobe essential for the comprehension of spoken and written language.
zero-crossing method: a technique for estimating frequency by counting how many times a waveform crosses the zero line in 1 second and dividing by two.
z-score thresholds: upper and lower boundaries expressed in z-scores (e.g., z-score) used to normalize specific EEG metrics and regions of interest (ROIs).
z-score training: a neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Acharya, J. N., Hani, A. J., Cheek, J., Thirumala, P. D., & Tsuchida, T. N. (2016). American Clinical Neurophysiology Society Guideline 2: Guidelines for standard electrode position nomenclature. Journal of Clinical Neurophysiology, 33(4), 308-311. https://doi.org/10.1097/WNP.0000000000000316
Advokat, C. D., Comaty, J. E., & Julien, R. M. (2019). Julien's primer of drug action: A comprehensive guide to the actions, uses, and side effects of psychoactive drugs (14th ed.). Worth Publishers.
Anderson, J. S. (2025, April 10). John S. Anderson on frequency vs. amplitude. BioSource Software. https://www.biosourcesoftware.com/post/john-anderson-on-frequency-vs-amplitude
Anderson, J. S., & Davis, J. R. (2025a, November 5). John Anderson and John Davis answer your neurofeedback questions. BioSource Software. https://www.biosourcesoftware.com/post/john-anderson-and-john-davis-answer-your-neurofeedback-questions
Anderson, J. S., & Davis, J. R. (2025b, November 9). John Anderson and John Davis answer your questions about learning processes and mindfulness in neurofeedback. BioSource Software. https://www.biosourcesoftware.com/post/john-anderson-and-john-davis-answer-your-questions-about-learning-processes-and-mindfulness
Arnold, L. E., Arns, M., Barterian, J., Bergman, R., Black, S., Conners, C. K., Connor, S., Dasgupta, S., deBeus, R., Higgins, T., Hirshberg, L., Hollway, J. A., Kerson, C., Lightstone, H., Lofthouse, N., Lubar, J., McBurnett, K., Monastra, V., Buchan-Page, K., . . . Williams, C. E. (2021). Double-blind placebo-controlled randomized clinical trial of neurofeedback for attention-deficit/hyperactivity disorder with 13-month follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 60(7), 841-855. https://doi.org/10.1016/j.jaac.2020.07.906
Arns, M., de Ridder, S., Strehl, U., Breteler, M., & Coenen, A. (2009). Efficacy of neurofeedback treatment in ADHD: The effects on inattention, impulsivity and hyperactivity: A meta-analysis. Clinical EEG and Neuroscience, 40(3), 180-189. https://doi.org/10.1177/155005940904000311
Banoczi, W. R. (2005). How some drugs affect the electroencephalogram (EEG). American Journal of Electroneurodiagnostic Technology, 45, 118-129. PMID: 15989074
Bauer, G., & Bauer, R. (2005). EEG drug effects and central nervous system poisoning. In E. Niedermeyer & F. Lopes da Silva (Eds.), Electroencephalography: Basic principles, clinical applications, and related fields (5th ed.). Lippincott Williams & Wilkins.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., Segal, Z. V., Abbey, S., Speca, M., Velting, D., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230-241. https://doi.org/10.1093/clipsy.bph077
Blume, W. T. (2006). Drug effects on EEG. Journal of Clinical Neurophysiology, 23(4), 306-311. https://doi.org/10.1097/01.wnp.0000229137.94384.fa
Brewer, J. A., Worhunsky, P. D., Gray, J. R., Tang, Y.-Y., Weber, J., & Kober, H. (2011). Meditation experience is associated with differences in default mode network activity and connectivity. Proceedings of the National Academy of Sciences, 108(50), 20254-20259. https://doi.org/10.1073/pnas.1112029108
Cahn, B. R., & Polich, J. (2006). Meditation states and traits: EEG, ERP, and neuroimaging studies. Psychological Bulletin, 132(2), 180-211. https://doi.org/10.1037/0033-2909.132.2.180
Clarke, A. R., Barry, R. J., McCarthy, R., & Selikowitz, M. (2001). Excess beta activity in children with attention-deficit/hyperactivity disorder: An atypical electrophysiological group. Psychiatry Research, 103(2-3), 205-218. https://doi.org/10.1016/s0165-1781(01)00277-3
Collura, T. F. (2014). Technical foundations of neurofeedback. Taylor & Francis.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2019). Applied behavior analysis (3rd ed.). Pearson.
Currie, J., Stabile, M., & Jones, L. (2014). Do stimulant medications improve educational and behavioral outcomes for children with ADHD? Journal of Health Economics, 37, 58-69. https://doi.org/10.1016/j.jhealeco.2014.05.002
Demos, J. N. (2019). Getting started with EEG neurofeedback (2nd ed.). W. W. Norton.
Egner, T., & Sterman, M. B. (2006). Neurofeedback treatment of epilepsy: From basic rationale to practical application. Expert Review of Neurotherapeutics, 6(2), 247-257. https://doi.org/10.1586/14737175.6.2.247
Federal Aviation Administration. (1999). Aviation instructor's handbook (FAA-H-8083-9). U.S. Department of Transportation.
Federal Aviation Administration. (2020). Aviation instructor's handbook (FAA-H-8083-9B). U.S. Department of Transportation. https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/aviation_instructors_handbook
Felsinger, J. M., Gladstone, A. I., Yamaguchi, H. G., & Hull, C. L. (1947). Reaction latency (stR) as a function of the number of reinforcements (N). Journal of Experimental Psychology, 37(3), 214-228. https://doi.org/10.1037/h0055587
Ferree, T. C., Luu, P., Russell, G. S., & Tucker, D. M. (2001). Scalp electrode impedance, infection risk, and EEG data quality. Clinical Neurophysiology, 112(3), 536-544. https://doi.org/10.1016/s1388-2457(00)00533-2
Fisch, B. J. (1999). Fisch and Spehlmann's EEG primer: Basic principles of digital and analog EEG (3rd rev. and enlarged ed.). Elsevier.
Grice, G. R. (1948). The relation of secondary reinforcement to delayed reward in visual discrimination learning. Journal of Experimental Psychology, 38(1), 1-16. PMID: 18910254
Gunkelman, J. (n.d.). Drug exposure and EEG/qEEG findings. qEEGsupport.com. https://qeegsupport.com/drug-exposure-and-eegqeeg-findings/
Hammond, D. C. (2011). What is neurofeedback: An update. Journal of Neurotherapy, 15, 305-336. https://doi.org/10.1080/10874208.2011.623090
Hammond, D. C., & Kirk, L. (2008). First do no harm: Adverse effects and the need for practice standards in neurofeedback. Journal of Neurotherapy, 12(1), 79-88. https://doi.org/10.1080/10874200802219947
Hardt, J. V., & Kamiya, J. (1976). Conflicting results in EEG alpha feedback studies: Why amplitude integration should replace percent time. Biofeedback and Self-Regulation, 1(1), 63-75. https://doi.org/10.1007/BF00998691
Herning, R. I., Glover, B. J., Koeppl, B., Phillips, R. L., & London, E. D. (1994). Cocaine-induced increases in EEG alpha and beta activity: Evidence for reduced cortical processing. Neuropsychopharmacology, 11(1), 1-9. https://doi.org/10.1038/npp.1994.30
Herning, R. I., Jones, R. T., Hooker, W. D., Mendelson, J., & Blackwell, L. (1985). Cocaine increases EEG beta: A replication and extension of Hans Berger's historic experiments. Electroencephalography and Clinical Neurophysiology, 60(6), 470-477. https://doi.org/10.1016/0013-4694(85)91106-x
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537-559. https://doi.org/10.1177/1745691611419671
Jasper, H. H. (1958). The ten-twenty electrode system of the International Federation. Electroencephalography and Clinical Neurophysiology, 10, 371-375.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144-156. https://doi.org/10.1093/clipsy.bpg016
Kappenman, E. S., & Luck, S. J. (2010). The effects of electrode impedance on data quality and statistical significance in ERP recordings. Psychophysiology, 47(5), 888-904. https://doi.org/10.1111/j.1469-8986.2010.01009.x
Khazan, I. Z. (2019). Biofeedback and mindfulness in everyday life: Practical solutions for improving your health and performance. W. W. Norton.
Knott, V. J. (2000). Quantitative EEG methods and measures in human psychopharmacological research. Human Psychopharmacology, 15, 479-498. https://doi.org/10.1002/1099-1077(200010)15:7<479::AID-HUP206>3.0.CO;2-5
Lansbergen, M. M., van Dongen-Boomsma, M., Buitelaar, J. K., & Slaats-Willemse, D. (2011). ADHD and EEG-neurofeedback: A double-blind randomized placebo-controlled feasibility study. Journal of Neural Transmission, 118(2), 275-284. https://doi.org/10.1007/s00702-010-0524-2
Lansky, P., Bohdanecký, Z., Indra, M., & Radil-Weiss, T. (1979). Alpha detection: Some comments on Hardt and Kamiya, "Conflicting results in EEG alpha feedback studies." Biofeedback and Self-Regulation, 4(2), 127-131. https://doi.org/10.1007/BF01007107
Lau, T. M., Gwin, J. T., & Ferris, D. P. (2012). How many electrodes are really needed for EEG-based mobile brain imaging? Journal of Behavioral and Brain Science, 2(3), 387-393. https://doi.org/10.4236/jbbs.2012.23044
Lomas, T., Ivtzan, I., & Fu, C. H. Y. (2015). A systematic review of the neurophysiology of mindfulness on EEG oscillations. Neuroscience & Biobehavioral Reviews, 57, 401-410. https://doi.org/10.1016/j.neubiorev.2015.09.018
Lubar, J. F. (1995). Neurofeedback for the management of attention-deficit/hyperactivity disorders. In M. S. Schwartz (Ed.), Biofeedback: A practitioner's guide (pp. 493-522). The Guilford Press.
Lubar, J. F., & Shouse, M. N. (1976). EEG and behavioral changes in a hyperactive child concurrent with training of the sensorimotor rhythm (SMR): A preliminary report. Biofeedback and Self-Regulation, 1, 293-306. https://doi.org/10.1007/bf01001170
Lubar, J. F., Shabsin, H. S., Natelson, S. E., Holder, G. S., Whitsett, S. F., Pamplin, W. E., & Krulikowski, D. I. (1981). EEG operant conditioning in intractable epileptics. Archives of Neurology, 38, 700-704. https://doi.org/10.1001/archneur.1981.00510110060009
Luctkar-Flude, M., & Groll, D. (2015). A systematic review of the safety and effect of neurofeedback on fatigue and cognition. Integrative Cancer Therapies, 14, 318-340. https://doi.org/10.1177/1534735415572886
MacInerney, E. K., Swatzyna, R. J., Roark, A. J., Gonzalez, B. C., & Kozlowski, G. P. (2017). Breakfast choices influence brainwave activity: Single case study of a 12-year-old female. NeuroRegulation, 4(1), 56-62. https://doi.org/10.15540/nr.4.1.56
Martin, G., & Pear, J. (2019). Behavior modification: What it is and how to do it (11th ed.). Routledge.
Martins-Mourao, A. M., & Kerson, C. (2016). Equipment, training and ethical issues. In C. Kerson & A. Martins-Mourao (Eds.), Alpha-theta training in the 21st century: A handbook for clinicians and researchers (pp. 249-258). Foundation for Neurofeedback and Neuromodulation Research.
Matthews, T. V. (2007). Neurofeedback overtraining and the vulnerable patient. Journal of Neurotherapy, 11(3), 63-66. https://doi.org/10.1080/10874200802126290
Miller, L. K. (2006). Principles of everyday behavior analysis (4th ed.). Thomson/Wadsworth.
Monastra, V. J., Lubar, J. F., & Linden, M. (2001). The development of a quantitative electroencephalographic scanning process for attention deficit-hyperactivity disorder: Reliability and validity studies. Neuropsychology, 15(1), 136-144. https://doi.org/10.1037/0894-4105.15.1.136
Olton, D. S., & Noonberg, A. R. (1980). Biofeedback: Clinical applications in behavioral medicine. Prentice-Hall.
Palmero-Soler, E., Dolan, K., Hadamschek, V., & Tass, P. A. (2007). swLORETA: A novel approach to robust source localization and synchronization tomography. Physics in Medicine and Biology, 52(7), 1783-1800. https://doi.org/10.1088/0031-9155/52/7/002
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49-65.
Rogel, A., Guez, J., Getter, N., Keha, E., Cohen, T., Amor, T., & Todder, D. (2015). Transient adverse side effects during neurofeedback training: A randomized, sham-controlled, double-blind study. Applied Psychophysiology and Biofeedback, 40, 209-218. https://doi.org/10.1007/s10484-015-9289-6
Ros, T., Baars, B. J., Lanius, R. A., & Vuilleumier, P. (2014). Tuning pathological brain oscillations with neurofeedback: A systems neuroscience framework. Frontiers in Human Neuroscience, 8, Article 1008. https://doi.org/10.3389/fnhum.2014.01008
Saletu, B., Anderer, P., & Saletu-Zyhlarz, G. M. (2010). EEG topography and tomography (LORETA) in diagnosis and pharmacotherapy of depression. Clinical EEG and Neuroscience, 41(4), 203-210. https://doi.org/10.1177/155005941004100407
Sherlin, L. H., Arns, M., Lubar, J., Heinrich, H., Kerson, C., Strehl, U., & Sterman, M. B. (2011). Neurofeedback and basic learning theory: Implications for research and practice. Journal of Neurotherapy, 15(4), 292-304. https://doi.org/10.1080/10874208.2011.623089
Sitaram, R., Ros, T., Stoeckel, L., Haller, S., Scharnowski, F., Lewis-Peacock, J., Weiskopf, N., Blefari, M. L., Rana, M., Oblak, E., Birbaumer, N., & Sulzer, J. (2017). Closed-loop brain training: The science of neurofeedback. Nature Reviews Neuroscience, 18(2), 86-100. https://doi.org/10.1038/nrn.2016.164
Skinner, B. F. (1953). Science and human behavior. Macmillan.
Soutar, R., & Longo, R. (2020). Doing neurofeedback: An introduction (2nd ed.). ISNR Research Foundation.
Stahl, S. M. (2017). Stahl's essential psychopharmacology prescriber's guide (6th ed.). Cambridge University Press.
Sterman, M. B., & Egner, T. (2006). Foundation and practice of neurofeedback for the treatment of epilepsy. Applied Psychophysiology and Biofeedback, 31(1), 21-35. https://doi.org/10.1007/s10484-006-9002-x
Stokes, T. F., & Baer, D. M. (1977). An implicit technology of generalization. Journal of Applied Behavior Analysis, 10(2), 349-367. https://doi.org/10.1901/jaba.1977.10-349
Strehl, U. (2014). What learning theories can teach us in designing neurofeedback treatments. Frontiers in Human Neuroscience, 8, Article 894. https://doi.org/10.3389/fnhum.2014.00894
Swingle, P. G. (2008). Biofeedback for the brain: How neurotherapy effectively treats depression, ADHD, autism, and more. Rutgers University Press.
Swingle, P. G. (2015). Adding neurofeedback to your practice: Clinician's guide to ClinicalQ, neurofeedback, and braindriving. Springer.
Tang, Y.-Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience, 16(4), 213-225. https://doi.org/10.1038/nrn3916
Thomas, C. (2007). What is a montage? EEG instrumentation. American Society of Electroneurodiagnostic Technologists, Inc.
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Thorndike, E. L. (1911). Animal intelligence: Experimental studies. Macmillan.
Thorndike, E. L. (1913). Educational psychology: Vol. 2. The psychology of learning. Teachers College, Columbia University.
Toomim, H., Mize, W., Kwong, P. C., Toomim, M., Marsh, R., Kozlowski, G. P., Kimball, M., & Rémond, A. (2004). Intentional increase of cerebral blood oxygenation using hemoencephalography (HEG): An efficient brain exercise therapy. Journal of Neurotherapy, 8, 5-21. https://doi.org/10.1300/J184v08n03_02
Treves, I. N., Greene, K. D., Bajwa, Z., Wool, E., Kim, N., Bauer, C. C. C., Bloom, P. A., Pagliaccio, D., Zhang, J., Whitfield-Gabrieli, S., & Auerbach, R. P. (2024). Mindfulness-based neurofeedback: A systematic review of EEG and fMRI studies. Imaging Neuroscience, 2, 1-25. https://doi.org/10.1162/imag_a_00396
Van Cott, A., & Brenner, R. P. (2003). Drug effects and toxic encephalopathies. In J. S. Ebersole & T. A. Pedley (Eds.), Current practice of clinical electroencephalography (3rd ed.). Lippincott Williams & Wilkins.
Van Doren, J., Arns, M., Heinrich, H., Vollebregt, M. A., Strehl, U., & Loo, S. K. (2019). Sustained effects of neurofeedback in ADHD: A systematic review and meta-analysis. European Child & Adolescent Psychiatry, 28(3), 293-305. https://doi.org/10.1007/s00787-018-1121-4
Return to Top