Steps in Protocol Development
What You Will Learn in This Chapter
Every neurofeedback session starts with a critical question: where do you place the electrodes, and what do you train? This unit gives you a systematic framework for answering that question. You will learn to evaluate functional causes that may underlie a client's symptoms, review the key factors that guide protocol selection, and apply an evidence-based decision-making process that integrates neuroscience research with clinical reasoning.
You will also work through detailed case examples that follow the full arc from assessment through protocol selection, training, and reassessment. These cases illustrate how practitioners apply the framework across diverse clinical presentations in real-world settings.
BCIA Blueprint Coverage: This unit addresses VII. Developing Treatment Protocols - B. Steps in protocol development and treatment planning using one or more of the treatment models (Blueprint Code VII-B).
Learning Objectives
After completing this section, you will be able to:
Identify red flags that should trigger a functional or integrative medicine consultation before starting neurofeedback.
Describe the key factors to consider when selecting neurofeedback training protocols, including client condition, research findings, practitioner expertise, resources, environmental context, and client values.
Explain how an arousal model can guide the classification of client presentations and protocol selection.
Apply an evidence-based decision-making flowchart to match client problems with appropriate neurofeedback protocols.
Interpret qEEG assessment findings and translate them into training protocol recommendations through case example analysis.
Overview
This section covers three essential topics: when to pause and investigate functional causes before starting neurofeedback, the factors that shape protocol selection, and a decision-making flowchart you can apply in practice. Think of this framework as a starting point for clinical reasoning rather than a rigid recipe. Practitioners should always be prepared to account for why they chose a particular protocol.
We begin with a question that may surprise you: should you start neurofeedback at all? In challenging cases, the answer may be "not yet." Some clients present with symptoms that have functional causes, such as environmental exposures, infections, or metabolic imbalances, that require extensive blood and urine testing before training can be effective.
Dr. Ron Swatzyna and colleagues (2024) urge clinicians to think beyond DSM-5 diagnoses. They advocate collaborating with neurologists and functional and integrative medicine professionals to uncover the root causes of a client's complaints before beginning biofeedback or neurofeedback. This represents a paradigm shift: rather than treating only the symptoms that appear in the EEG, you investigate what might be driving those symptoms in the first place.
What are the "red flags" that should trigger a functional or integrative medicine consult? The first red flag is that symptoms such as hyperactivity or tics are new or have worsened dramatically (R. J. Swatzyna, personal communication, August 9, 2024). The second involves abnormal EEG amplitude and peak frequency values. For example, a low-amplitude 6.5-Hz peak frequency in a 10-year-old is not age-appropriate and should be investigated; a series of EEGs can reveal whether the pattern is worsening over time (R. J. Swatzyna, personal communication, August 9, 2024).
The third red flag appears when a neurologist confirms biomarkers in the raw EEG. These include focal slowing (FS), meaning slower-than-normal brainwave activity localized to a specific brain region; spindling excessive beta (SEB), abnormal bursts of beta activity that appear as spindles and may indicate cortical irritability; encephalopathy (EN), or widespread brain dysfunction; and isolated epileptiform discharges (IEDs), brief abnormal electrical bursts that can signal cortical irritability even in non-epileptic individuals. These biomarkers may point to underlying physiological processes like neuroinflammation. Collaborating with a board-certified neurologist can sharpen your raw EEG interpretation and strengthen your credibility with the client's physician (Swatzyna et al., 2024).
The use of EEG biomarker identification represents a positive step toward personalized medicine. By directly testing the organ being treated, practitioners can gain a deeper understanding of the underlying brain activity and create treatment plans tailored to the specific needs of each patient. (Swatzyna et al., 2024, p. 9)
When red flags point to possible environmental causes such as lead or mold exposure, or to gut-brain dysfunction, you can recommend that your client consult with a functional or integrative medicine professional in your area. That specialist will determine which tests are needed based on the patient's symptoms, medical history, and EEG findings. Crucially, you should not begin biofeedback and neurofeedback until suspected causes are ruled out or treated, which might mean waiting several months for gut-wall repair in cases of dysbiosis or for a mold detox protocol to reduce mycotoxin levels.

This paradigm shift might feel overwhelming, but it doesn't have to be if you "stay in your lane." Your role is to do what you already do best: identify red flags and make referrals when needed. The functional and integrative medicine professionals will decide which tests to order, interpret the results, and recommend evidence-based treatments (R. J. Swatzyna, personal communication, August 9, 2024). Collaboration, not reinvention, is what this shift requires.
Swatzyna and colleagues (2024) encourage clinicians to look beyond DSM-5 diagnoses and partner with neurologists and functional medicine professionals. Three red flags should prompt referral: new or dramatically worsening symptoms, abnormal EEG amplitude and peak frequency values, and the presence of raw EEG biomarkers such as focal slowing, spindling excessive beta, encephalopathy, and isolated epileptiform discharges. Swatzyna advises against beginning neurofeedback until suspected functional causes have been ruled out or addressed (R. J. Swatzyna, personal communication, August 9, 2024).
Clinical Examples
The following twelve cases were contributed by a diverse group of medical professionals. They are uncontrolled clinical vignettes reported by the treating clinicians rather than published case studies, so read the outcomes as illustrations of a reasoning process rather than as evidence that the identified cause produced the symptoms. In this section, you will see how functional causes, ranging from mold exposure to nutrient deficiencies, can masquerade as psychiatric diagnoses. In each case, the treating clinician judged that addressing the DSM-5 diagnosis alone with medication and neurofeedback would have missed the underlying problem.
Case Example 1: Mold Exposure and Cognitive Decline. A 40-year-old woman presented with depression, anxiety, and cognitive decline. Antidepressants provided only partial relief. A functional medicine assessment uncovered significant mold exposure in her home, and testing confirmed the presence of mycotoxins, toxic compounds produced by mold, in her body.
Treatment involved remediating her home, detoxification protocols to eliminate mycotoxins, and support for her immune system and gut health. As the toxins cleared, her psychological symptoms improved dramatically and her cognitive function returned to normal. This case illustrates why addressing the root cause, mold toxicity, was essential for effective treatment.
Case Example 2: Glyphosate Exposure and ADHD. A 10-year-old boy diagnosed with ADHD was prescribed stimulant medication. While helpful for symptom management, the medication caused insomnia and decreased appetite. A functional medicine practitioner explored environmental factors and discovered that the family lived near agricultural fields regularly sprayed with glyphosate, a widely used herbicide with potential neurotoxic effects. Testing revealed high glyphosate levels in the boy's system.
The treatment plan included dietary changes to support detoxification, nutritional supplementation for brain health, and measures to reduce ongoing glyphosate exposure. As his glyphosate levels dropped, his ADHD symptoms improved and he was able to reduce his reliance on stimulant medication.
Case Example 3: Chronic Inflammatory Response Syndrome (CIRS). A 35-year-old man experienced severe fatigue, brain fog, and mood swings. Despite seeing multiple specialists and trying various medications, his symptoms persisted. A functional medicine assessment raised chronic inflammatory response syndrome (CIRS), a proposed condition attributed to biotoxin exposure and said to produce chronic inflammation and multi-system symptoms, though it appears in neither the DSM nor the ICD and its evidence base is disputed. Advanced testing confirmed elevated inflammatory markers and biotoxin levels, likely from water-damaged buildings.
Treatment involved detoxification protocols, binders to remove biotoxins, and immune and nervous system support. Addressing the biotoxin exposure and inflammation led to significant improvements in energy, cognitive function, and mood, underscoring the importance of identifying root causes in treatment-resistant cases.
Case Example 4: Lyme Disease and Psychiatric Symptoms. A 28-year-old woman presented with severe anxiety, depression, and panic attacks. Antidepressants and anxiolytics provided minimal relief. A functional medicine practitioner considered the possibility of underlying infections and ordered comprehensive testing, which revealed Lyme disease and co-infections, a finding that reframed her psychiatric symptoms as consequences of a treatable medical condition.
Treatment included antimicrobial therapies to address the infections, immune support, and anti-inflammatory interventions. As the infections came under control, her psychiatric symptoms began to resolve. This case powerfully demonstrates the need to investigate underlying medical conditions rather than treating symptoms in isolation.
Case Example 5: Addison's Disease and Depression. A 45-year-old man was experiencing severe fatigue, weight loss, and depression. Antidepressants and therapy had little effect. A functional medicine practitioner discovered Addison's disease, a condition in which the adrenal glands produce insufficient cortisol. Because cortisol regulates energy, mood, and stress response, this deficiency was directly driving his psychological symptoms.
Hormone replacement therapy corrected the cortisol deficiency, supplemented by measures to strengthen his overall health. Once the Addison's disease was managed, his depression and fatigue improved markedly. This case illustrates how an endocrine disorder can mimic a primary psychiatric condition.
Case Example 6: Environmental Toxins and New OCD Symptoms. A 22-year-old woman developed new-onset obsessive-compulsive disorder (OCD) symptoms, including severe anxiety and compulsive behaviors. Psychiatric medications provided minimal relief. A detailed environmental assessment revealed high-level exposure to volatile organic compounds (VOCs) in her workplace, and testing confirmed elevated toxin levels in her body.
Treatment focused on reducing VOC exposure, detoxification protocols, and nutritional support to enhance her body's toxin-elimination pathways. As her toxin burden decreased, her OCD symptoms and anxiety significantly improved, a reminder that new-onset psychiatric symptoms warrant investigation of environmental exposures.
Case Example 7: Tics and Heavy Metal Toxicity. A 15-year-old boy developed motor tics and was diagnosed with a tic disorder. Behavioral therapy and medications were only partially effective. Comprehensive functional medicine testing revealed high levels of heavy metals, particularly lead, in his system, a likely contributor to his neurological symptoms.
The treatment plan included chelation therapy to remove heavy metals, dietary modifications to support detoxification, and supplements to restore nutritional balance. As heavy metal levels decreased, the boy's tics diminished in frequency and severity. This case illustrates the importance of screening for environmental toxins when neurological symptoms resist standard treatments.
Case Example 8: PANS/PANDAS and Psychiatric Symptoms. A 12-year-old girl suddenly developed severe anxiety, obsessive-compulsive behaviors, and mood swings. Psychiatric treatments were ineffective. A functional medicine practitioner suspected Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) or Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS), conditions in which infections trigger the immune system to attack the brain. Dr. Melissa Jones expects these terms to eventually be subsumed under the broader diagnosis of autoimmune encephalitis, which refers to brain inflammation caused by the body's own immune system.
Comprehensive testing confirmed a recent streptococcal infection and elevated autoimmune markers. Treatment included antibiotics, anti-inflammatory therapies, and immune-modulating treatments. As the underlying infection and inflammation resolved, the girl's psychiatric symptoms improved significantly, highlighting the need for comprehensive workup when psychiatric symptoms appear suddenly in children.
Case Example 9: Autism and Gut Health. A 6-year-old boy diagnosed with autism spectrum disorder (ASD) exhibited severe gastrointestinal issues, including chronic diarrhea and abdominal pain. Behavioral interventions addressed his autism but did nothing for his physical discomfort. A functional medicine evaluation revealed significant dysbiosis, an imbalance in his gut microbiome, the vast community of microorganisms living in and on the human body, particularly in the digestive tract.
Treatment included a specialized diet to eliminate food sensitivities, probiotics to restore healthy gut flora, and anti-inflammatory supplements. As his gut health improved, notable enhancements appeared in his mood, behavior, and communication skills. This case demonstrates the profound impact that gut-brain axis health can have on ASD symptoms.
Case Example 10: Oppositional Defiant Disorder and Nutrient Deficiencies. An 8-year-old girl diagnosed with oppositional defiant disorder (ODD) was struggling with severe temper tantrums, defiance, and aggression. Behavioral therapy provided limited success. A functional medicine assessment revealed multiple nutrient deficiencies, including low levels of zinc, magnesium, and vitamin D, all of which play important roles in brain function and mood regulation.
Treatment included dietary changes to ensure nutrient-rich meals and targeted supplementation. As her nutrient levels normalized over time, her behavior improved significantly. This case highlights how nutritional imbalances can masquerade as psychological and behavioral disorders.
Case Example 11: Strep Infection Leading to Tonsillectomy and Adenoidectomy. A 7-year-old girl developed sudden-onset obsessive-compulsive behaviors and tics. Standard psychiatric medications were ineffective for several weeks, prompting a functional medicine consultation. A detailed medical history revealed a recent bout of strep throat, and blood tests showed elevated anti-streptolysin O (ASO) titers, confirming a recent streptococcal infection.
Despite initial antibiotic treatment, her symptoms persisted, and recurrent strep infections were suspected. To eliminate the chronic infection source, a tonsillectomy and adenoidectomy were recommended. Post-surgery, the patient showed significant improvement in her neuropsychiatric symptoms. This case illustrates the importance of addressing persistent infection sources in pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections.
Case Example 12: UTI-Related Dementia Symptoms in an Elderly Patient. An 82-year-old man experienced rapid cognitive decline and behavioral changes, initially diagnosed as dementia by his primary care physician. Symptoms included confusion, agitation, and memory loss that severely affected his quality of life. A functional medicine practitioner was consulted for a second opinion.
A thorough evaluation, including laboratory tests, identified a urinary tract infection (UTI) as the underlying cause of his symptoms. In elderly patients, UTIs can trigger delirium and dementia-like presentations due to systemic inflammation and infection. Appropriate antibiotic treatment eradicated the infection, and his cognitive function improved markedly. This case underscores the necessity of considering infections and other reversible conditions when evaluating cognitive decline in elderly patients.
These twelve cases demonstrate that functional causes, including mold exposure, glyphosate toxicity, CIRS, Lyme disease, Addison's disease, environmental toxins, heavy metals, autoimmune encephalitis (PANS/PANDAS), gut dysbiosis, nutrient deficiencies, streptococcal infections, and UTIs, can produce psychiatric and neurological symptoms. In each, the treating clinician judged that addressing the DSM-5 diagnosis alone would have been insufficient. Because these are uncontrolled vignettes, they cannot establish how often such causes are present or how reliably treating them resolves symptoms; what they do establish is that the possibility is worth ruling out. The common thread is the value of collaboration with functional and integrative medicine professionals in identifying and addressing underlying conditions before neurofeedback begins.
A Neurofeedback Decision-Making Framework
Once functional causes have been treated or ruled out, neurofeedback can begin. This section introduces the evidence-based framework that guides protocol selection. You will learn how clinical outcome research, neuroscience, and brain-behavior relationships converge to inform your decision about where to place electrodes and what to train.
John S. Anderson discusses the process of developing evidence-based treatment protocols. Video © J. S. Anderson.
The model used here is evidence-based in the fullest sense: it draws on research studies, clinical experience, neuroscience, and brain-behavior relationships to select training protocols. We are indebted to Michael and Lynda Thompson, who have long advocated that clinical outcome research and neuroscience should inform neurofeedback protocol development (e.g., Thompson & Thompson, 2015). Their influence is central to the approach presented in this unit.
This section is also consistent with John Anderson's NewQ assessment method. Abbreviated Q assessments can provide useful information about the client, help validate and explain their symptoms, and assist with protocol selection. Video © J. S. Anderson.
The basic building blocks of any neurofeedback training protocol include electrode location, EEG frequency to be trained, EEG parameters (e.g., amplitude, amplitude ratios, connectivity measures, symmetry, peak frequency), and the direction of training, whether the selected parameter is trained up or down. When using 19-channel LORETA training, additional protocol features come into play, including specific cortical structures, Brodmann areas (cytoarchitectural zones of the cerebral cortex distinguished by Nissl staining; Brodmann numbered them 1-52, and roughly 43-47 are delineated in the human map), and brain networks.

BCIA Blueprint Coverage
This unit covers VII. Developing Treatment Protocols - B. Steps in protocol development and treatment planning using one or more of the treatment models (Blueprint Code VII-B).

The remainder of this unit covers three main topics: Factors to Consider when selecting protocols, Decision-Making and Ongoing Problem-Solving during training, and a practical Flowchart that ties the process together.
Factors To Consider
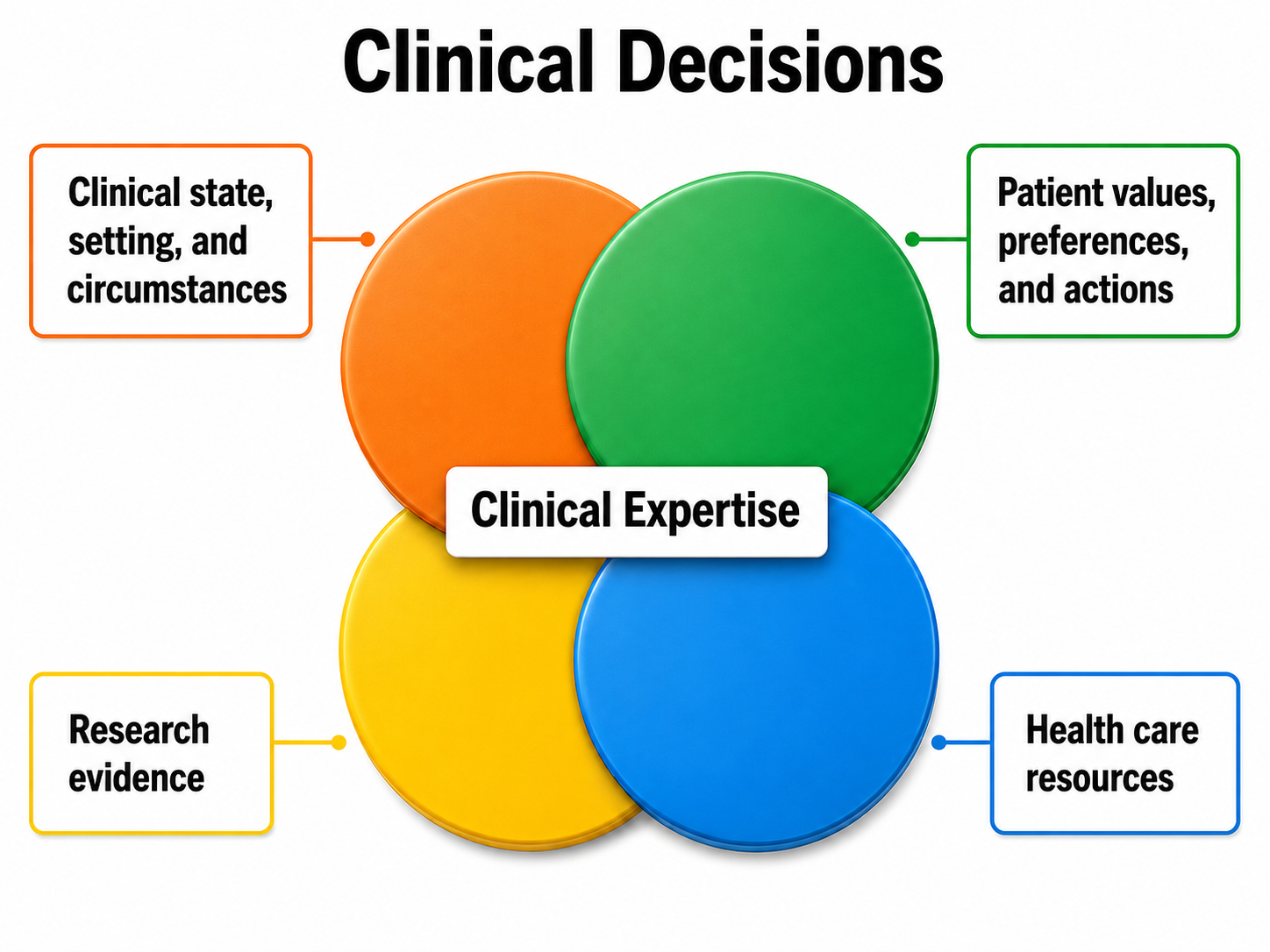
This section examines the six factors that shape protocol selection: the client's condition, research findings, practitioner expertise, available resources, environmental context, and client values and preferences. Each factor contributes a different piece of the puzzle, and weighing them together produces a protocol tailored to the individual rather than a one-size-fits-all approach. We will walk through each factor in turn.
Client Condition and Goals
The initial assessment tells you what the client wants to achieve, whether there are symptoms to decrease, abilities to enhance, or both. Contributing to your understanding of the client's condition are their personal and health histories, professional reports, and test findings. As described in the Assessment section of Neurofeedback Tutor: Assessment and Training, relevant information comes from diverse sources: self-report, direct behavioral observation, cognitive tests, questionnaires, and reports from significant others such as a parent, teacher, or spouse. EEG assessment results are central, and peripheral psychophysiological findings are often considered as well.
Training goals operate at three levels of analysis. The first level is biological and identifies where to train and which EEG variable to target. For example, finding excess posterior beta activity in a client seeking anxiety reduction may suggest electrode placement at P4.
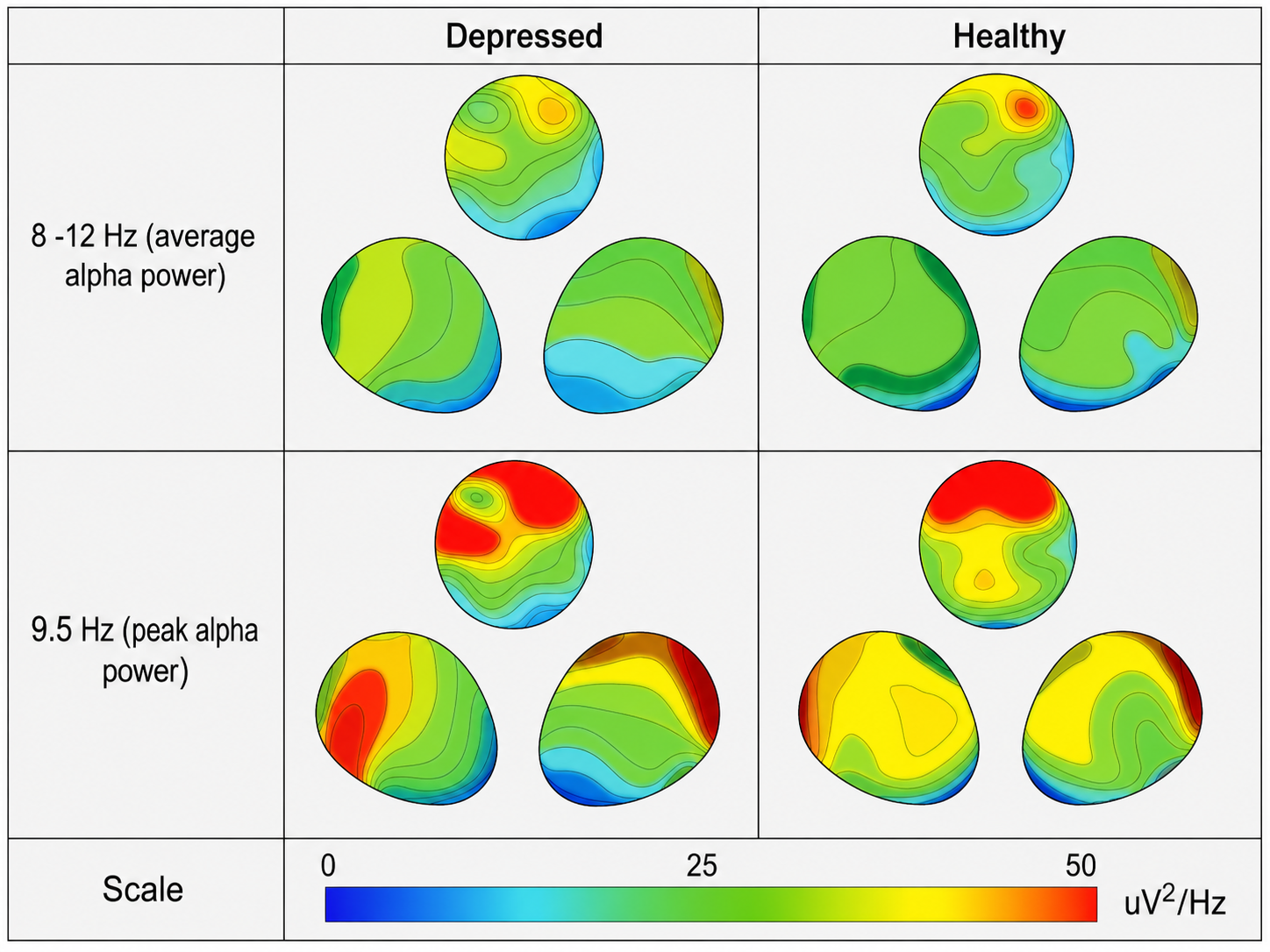
The second level is psychological, addressing the client's cognitive and emotional condition. If a client with depression shows prefrontal alpha asymmetry reversal, that is, greater alpha amplitude at F3 than at F4, this suggests placing electrodes at F3 and F4 and using an alpha asymmetry protocol. Gollan et al. (2014) found alpha asymmetry significantly higher in depressed than in healthy participants before treatment, but their study tested behavioral activation therapy rather than neurofeedback, and the asymmetry persisted after treatment whether or not clients remitted, so the pattern is better read as a marker identifying candidates for the protocol than as an index certain to normalize with recovery.
The third level concerns socially significant behavior change in a specific context. For example, a child with ADHD may show distractible behavior and poor grades in the classroom, deficient sustained attention, anxiety, and significantly excessive central theta EEG. A central bipolar electrode placement with a protocol rewarding sensorimotor rhythm (SMR), the 12-15 Hz spindle-shaped rhythm detected from the sensorimotor strip when individuals reduce attention to sensory input and motor activity, could improve both attention and academic performance.
Considering all three levels together within real-world contexts such as school, work, play, or social situations yields a holistic biopsychosocial description of the client's condition. Combined with neuroscience research, this formulation explains why the client may have the symptoms they present and points toward where to place electrodes and what EEG variables to train.
Research Findings
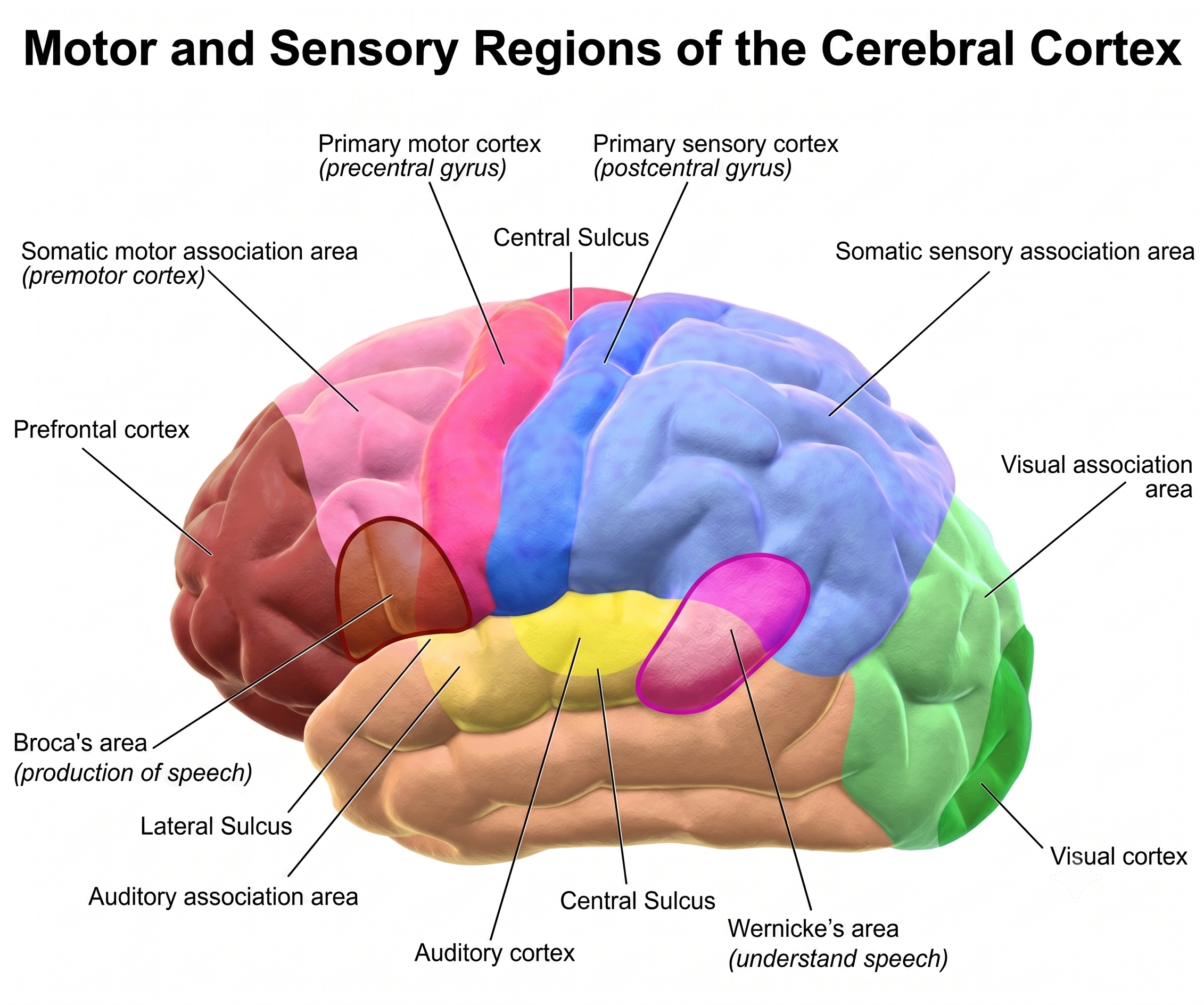
This section covers the four types of research findings that inform protocol selection: brain-behavior relationships, EEG correlates of clinical conditions, brain network anomalies, and neurofeedback efficacy studies. These layers of evidence build on one another: understanding where a function lives in the brain helps you interpret what the EEG is telling you, which in turn guides your choice of a research-supported protocol. One type of finding concerns brain-behavior relationships and functional neuroanatomy. For instance, language functions are a strength of the left hemisphere, and damage to the left temporal region may compromise language use.
A second type of research finding concerns the functional significance of EEG patterns and their correlation with specific conditions. For example, excess right frontal high beta (beta 4), 25-38 Hz activity mostly seen in the frontal lobes and associated with hyperarousal, has been linked to anxiety, as have beta spindling and excess posterior beta.
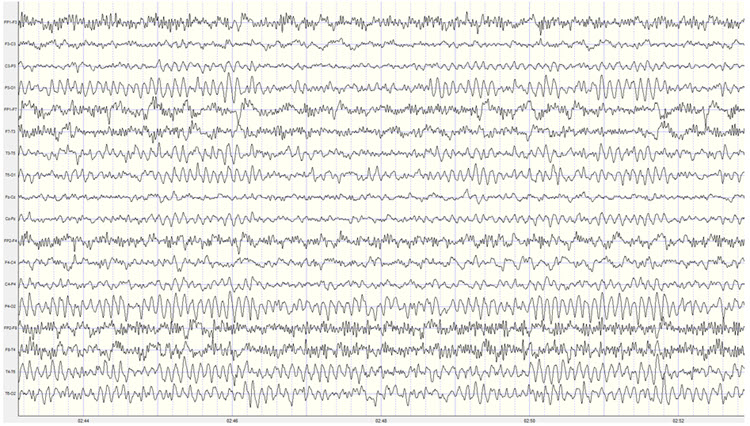
The video below is a 19-channel BioTrace+/NeXus-32 display of low beta and high beta activity. The 13-21 Hz and 22-34 Hz boundaries shown are the filter settings chosen for this display, not band definitions; this unit's glossary places beta 4 (high beta) at 25-38 Hz. Video © John S. Anderson. Brighter colors represent higher beta amplitudes, and frequency histograms are displayed for each channel.
Third, anomalies in brain networks are associated with various conditions and abilities. For example, dysfunction in the default mode network (DMN), a cortical network of frontal, temporal, and parietal regions most active during introspection and daydreaming and relatively quiet when we pursue external goals, has been linked to depression. Neurofeedback training can increase or decrease connectivity between brain sites using a normative database, which provides means and standard deviations for EEG variables calculated from healthy subjects grouped by age and condition. For example, BrainMaster's BrainAvatar software allows clinicians to train specific networks, like the DMN.
Finally, neurofeedback efficacy research is essential. For example, midline theta/beta training, a protocol that decreases theta amplitude and increases beta amplitude, has an established record of changing EEG patterns and of improving attention and classroom behavior in children with ADHD, though the largest double-blind randomized trial to date reported a null primary outcome (ICAN; Arnold et al., 2021). Knowing which protocols have research support gives you a defensible starting point for treatment.
Once you have described the client's condition and agreed on training goals, the next step is to evaluate how strongly the research supports any neurofeedback approach for similar goals. The Efficacy unit of the companion Neurofeedback Tutor: An Introduction explained the scientific evidence levels and the varying evidence available for different protocols and conditions. For some conditions, such as ADHD, a substantial body of evidence addresses the efficacy and effectiveness of neurofeedback, though the strength of that evidence remains contested and blinded trials have been less favorable than open ones. Moreover, more than one method may show benefit: for ADHD, both theta/beta training and slow cortical potential (SCP) training along the midline have research support.
A useful strategy for protocol selection, as presented in the training protocol development video, is an arousal model that classifies client presentations as overaroused or underaroused. Research supports various protocols for each category. Electrode site and EEG training parameters can also be guided by functional neuroanatomy, that is, the function of the cortical tissue beneath an electrode site or within a Brodmann area. Researchers have revised the Brodmann maps and correlated specific areas with their functions, giving practitioners a neuroanatomical rationale for electrode placement.
Protocol selection also draws on normative values of frequency bands at particular locations. Understanding whether excess EEG parameters represent overarousal or underarousal in a given area helps you determine which psychological or behavioral functions may be compromised. Robert Thatcher and his team have continued to develop the NeuroGuide database and the features of 19-channel z-score training, a strategy that attempts to normalize brain function relative to database means, most recently with the development of swLORETA, which improves on sLORETA by applying a singular-value-decomposition-based weighting of the lead field, making the solution more robust under noisy recording conditions and more sensitive to deep sources (Palmero-Soler et al., 2007). Both descend from low resolution electromagnetic tomography (LORETA), the source localization method introduced by Pascual-Marqui et al. (1994).
These advances have built a large community of clinicians using z-score neurofeedback. Applied Neuroscience maintains a bibliography of more than 50 publications on the method (https://www.appliedneuroscience.com/PDFs/Z_Score_NFB_Publications.pdf). Read that list as a measure of clinical uptake rather than of efficacy: it is vendor-maintained, mixes peer-reviewed articles with book chapters, newsletter pieces, a dissertation, and single-case reports, and contains no randomized controlled trials. For biofeedback practitioners, this growing evidence base means that z-score methods offer a well-supported option when client-specific EEG findings point to network-level dysfunction.
John S. Anderson provides an example of z-score training. Video © J. S. Anderson.
Research may also reveal EEG patterns of significance at particular locations and frequencies associated with a given disorder or symptom pattern. These findings become especially relevant when a research-based protocol proves ineffective, because the practitioner can then develop a client-specific protocol guided by the intersection of symptoms, the client's own EEG findings, and what the literature has identified about those EEG patterns.
The practitioner's guiding question is: "For my client's presenting complaints, is there a research-based protocol, or a set of research-based findings, that is relevant and corresponds to the client's EEG findings from the initial assessment?" The correspondence between symptom complaints, research findings, and EEG assessment findings directs the practitioner to electrode placement locations, the frequency or parameter to train, and the direction of training.
If clinical reasoning suggests departing from research-based findings, the practitioner should be prepared to account for that decision. For instance, a client with ADHD may have shown poor benefit from theta/beta training but demonstrates abnormalities in the attention network that could account for their symptoms. In that case, an alternative method such as swLORETA z-score training to normalize the relevant network becomes a reasonable path to pursue. When a research-based protocol fails, the practitioner can draw on neuroscience and EEG research, interpreted in the context of the client's unique condition, to select an alternative approach.
Four types of research findings inform protocol selection: brain-behavior relationships and functional neuroanatomy, EEG correlates of clinical conditions, brain network anomalies, and neurofeedback efficacy studies. The practitioner seeks the best match between the client's presenting complaints, research-based protocols, and the client's EEG assessment findings. When research-based protocols prove ineffective, practitioners can draw on neuroscience knowledge and client-specific EEG data to develop individualized alternative protocols.
Environmental Context
The client's external world, including their social relationships, living situation, and daily demands, provides a context that can facilitate or impede neurofeedback training. While environmental factors are less important for selecting which protocol to use, they may greatly influence how and when that protocol is delivered. Family stability, for example, can be a major strength, whereas family instability may suggest postponing neurofeedback until circumstances are more supportive.

Context cuts both ways. While excessive job demands may signal a poor time to begin training, the everyday demands of school or work can also be an advantage: they provide real-world situations in which clients can practice skills learned during neurofeedback and develop self-awareness about changes. The support of family and friends may assist both in the training office and at home, where remote training often depends on a family member's help. Whereas having a job is normally considered a strength, periods of excessive job demand may also be times to wait before starting neurofeedback.
Resources
Protocol selection is inevitably shaped by the tools at hand. Equipment resources range from single-channel to 19-channel systems, with software capabilities spanning amplitude and coherence training to the training of individual Brodmann areas or brain networks using z-score methods. Additional practical considerations include material resources for remote training, staff availability for scheduling multiple weekly sessions, and family resources for children who need transportation and support to attend appointments.
Client psychological resources are equally important. Internal resources such as motivation, self-awareness, communication ability, and cognitive capacity all influence readiness for neurofeedback. Training is most effective when the client is interested, can demonstrate some self-awareness, communicates at an age-appropriate level, and has stable physical and mental health.
When a client has fewer psychological or physical resources than average, preliminary steps can bridge the gap. These might include motivational interviewing to build readiness for change, peripheral biofeedback to enhance self-awareness, matching verbal information to the client's ability level, and scheduling sessions when health is most stable. In general, however, these accommodations affect how a protocol is delivered more than which protocol is selected.
Practitioner Expertise
Given the client's condition and the available evidence, the practitioner must honestly assess whether their training, skills, experience, and equipment allow them to provide effective treatment. One key factor is the neurofeedback model to which they subscribe. Because different models have different applications, a practitioner trained in multiple models has the broadest armamentarium from which to draw when addressing a client's goals.

Most practitioners will have expertise in an evidence-based model grounded in scientific investigations of neurofeedback efficacy and effectiveness, as described in Evidence-Based Practice in Biofeedback and Neurofeedback (4th ed.; Khazan et al., 2023). Beyond this foundation, models based on clinical studies and the neuroscience of brain-behavior relationships may be essential when research does not provide strong support for a specific protocol. In those situations, the practitioner must draw on clinically-based models and neuroscience knowledge to guide the training plan.
Ethical principles are central here. Practitioners should provide neurofeedback only for conditions for which they have adequate training, or they should seek supervision. Ideally, the practitioner will have sound understanding and experience with the client's clinical condition, skill with neurofeedback methods for that condition, and knowledge of how it relates to brain and psychophysiological findings.
Client Values and Preferences
After weighing all the preceding factors, the practitioner presents the client with a formulation: a description of the problem, a provisional model of its cause, and suggested training options. The options, with their likely costs and benefits, are reviewed so the client can make an informed decision about whether to pursue neurofeedback and, if so, which method to use. This process respects the ethical principle of autonomy, fulfills the requirement for informed consent, and acknowledges the client's own values and preferences.

Protocol selection requires weighing six interrelated factors: the client's condition and goals (assessed at biological, psychological, and behavioral levels), research findings, environmental context, available resources (equipment, staff, and client readiness), practitioner expertise, and client values and preferences. Ethical principles of autonomy and informed consent are central throughout. A holistic biopsychosocial description of the client, combined with neuroscience knowledge, ultimately guides electrode placement and EEG variable selection.
Decision-Making and Ongoing Problem-Solving
This section covers how the factors just reviewed translate into an evidence-based, collaborative decision-making process, from initial protocol selection through ongoing monitoring and adjustment. The approach is biopsychosocial: it combines biological, psychological, and behavioral evidence with the client's active participation to select protocols that are most likely to help and least likely to cause harm.
Together with the choice of a training protocol, the practitioner and client should agree on explicit, measurable goals at one or more levels of analysis. At a biological level, changes in EEG variables are one type of goal. At a psychological level, neurofeedback may aim to improve emotional regulation or cognitive function. At the level of observable behavior, goals may target specific actions in context, such as academic performance at school or focus in a competitive sport. Goals are typically measured and quantified using the same methods employed during the initial assessment.
Once a protocol is underway, the neurofeedback provider should conduct ongoing assessment of EEG, psychological, and behavioral variables so that progress can be reviewed with the client. If improvement toward the client's goals is not seen within a reasonable time, the provider should re-assess and generate new training options. Adjustments or alternative protocols should also be considered if unwanted side effects occur. Neurofeedback concludes when goals have been achieved or when no further progress is evident.
Flowchart
The factors discussed above can be organized into a practical decision-making flowchart. This flowchart is intentionally simplified; practitioners should be prepared to depart from it when there are valid clinical reasons, and they should always be able to account for their reasoning when they do so.
For any individual case, the relative weight of each factor will vary, making one component more prominent in choosing a training regimen. This variability is a feature, not a flaw: it reflects the reality that each client is unique. The flowchart also gives the practitioner recourse for problem-solving when an initially chosen training plan fails to provide sufficient benefit.
Below is a simplified flowchart that depicts the preceding discussion.
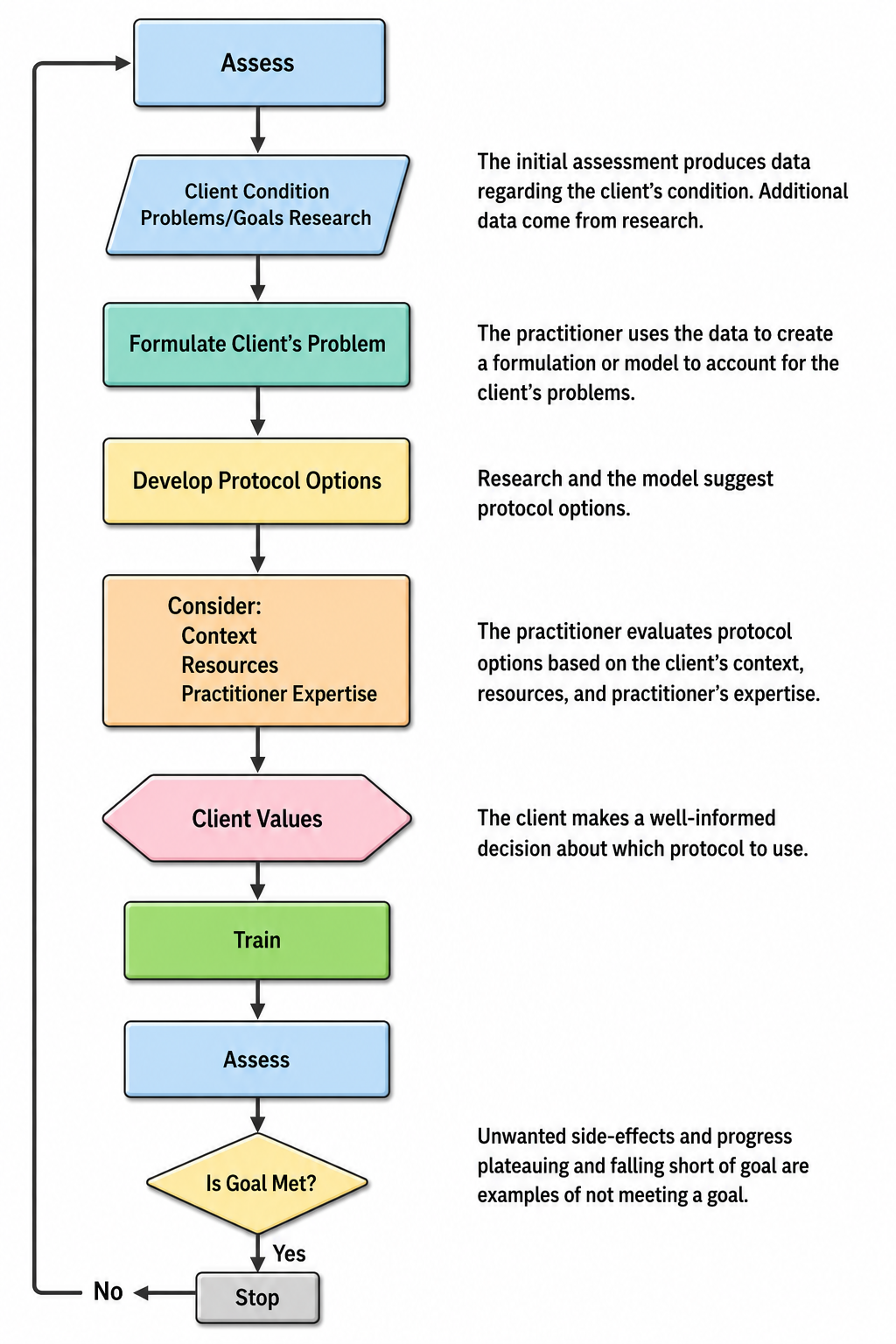
Underlying the flowchart's Formulate Client's Problem and Develop Protocol Options steps are four key questions: (1) What is the client's psychological or behavioral problem? (2) What does the EEG reveal about location and EEG parameters? (3) What do other tests show? (4) What research evidence supports the efficacy of a neurofeedback protocol for the issues identified by questions 1 through 3?
In essence, the practitioner is looking for the best match between problems and protocols to address them. The strongest starting point is usually a protocol with supportive research evidence, introduced in a trial-and-error manner to test the hypothesis that it will be effective. If the hypothesis is not confirmed, the practitioner selects an alternative research-based protocol if one is available. Failing that, the practitioner draws on their understanding of neuroscience, brain-behavior relationships, and EEG research to make informed decisions about electrode location, training frequency, frequency parameter, and the direction of training.
Decision-making in neurofeedback follows an evidence-based biopsychosocial approach. Goals should be explicit and measurable at biological, psychological, and behavioral levels. Ongoing assessment monitors protocol effectiveness, and adjustments are made when progress stalls or side effects emerge. The decision-making flowchart guides the process through four questions: identify the client's problem, assess the EEG, consider other test findings, and match these with research-supported protocols. When initial protocols fail, practitioners draw on neuroscience knowledge and client-specific data to develop alternative approaches.
From Assessment to Training
This section walks you through the full clinical arc, from intake interview through protocol selection, training, and reassessment, using a series of client case examples. Each example illustrates how the framework described above plays out with real clinical presentations. Before diving into the cases, we review the key steps that bridge assessment and training.
The process begins with the client intake interview, often facilitated by history and symptom forms completed beforehand. Once the client's presenting concerns are identified and discussed, the history of those concerns, including prior interventions and their degree of success or failure, helps establish the level of treatment resistance the client has experienced. The client's reasons for seeking neurofeedback can also be explored, and this is often the ideal moment to explain the underlying concepts of biofeedback and neurofeedback training. Emphasizing that neurofeedback is training, not treatment, is particularly important at this stage of the developing clinical relationship.
Establishing clear roles for both the client and clinician is essential. Many clients expect neurofeedback to be a passive treatment, something done to them, like taking medication or receiving repetitive transcranial magnetic stimulation (rTMS). Because all biofeedback involves active training and education, this distinction can be difficult for some clients to accept. Comments like "it didn't work" or "that didn't do anything" reflect a disconnect between expectations and the reality of the training process, and this gap may need to be addressed throughout the intervention.
Once the client understands the nature of the biofeedback training process, the clinician proceeds with appropriate testing. Foremost among these will be objective physiological evaluations such as autonomic nervous system reactivity, EEG behavioral characteristics and task responses, and possibly a continuous performance test or other computerized neurocognitive assessment. All intake and testing information is then evaluated, and a training approach is designed to maximize effectiveness.
The training plan is described to the client, and their agreement to participate is obtained. This agreement is an ongoing component of the process; before each subsequent session, the client's responses to previous training are briefly evaluated, and the client is asked whether they wish to continue. Any protocol changes are discussed and consent is noted in the client's chart. This collaborative approach reflects one of the most important aspects of the biofeedback relationship: the clinician needs the client's active participation, and one of the clinical goals is for the client to become a genuine partner in the training process. The more informed and knowledgeable the client becomes, the more useful feedback they can provide about their experiences and how training is affecting their life.
Re-evaluation is also integral to the training process. A regular schedule of revisiting initial assessment tools helps guide protocol changes and identifies when the client has reached a plateau where no further change is likely. The case examples below illustrate each of these steps in practice.
Patient Example A
This case illustrates the full assessment-to-training arc for a client with a history of traumatic brain injury (TBI). It demonstrates how qEEG findings, clinical history, and the decision-making framework converge to guide protocol selection, and how reassessment documents training outcomes.
Client A is a 38-year-old woman referred for quantitative EEG evaluation and neurofeedback training. An EEG recording session followed an initial intake and history session, during which samples of eyes-closed EEG, eyes-open EEG, and an eyes-open task condition were obtained.
Her clinical history indicated diagnoses of persistent depressive disorder and attention deficit hyperactivity disorder (ADHD). She reported attention problems, repetitive thoughts, feelings of inferiority, memory difficulties, problems making decisions, and some difficulty with communication, including word-finding and interpersonal skills. Her prenatal and birth history were unremarkable, development was typical, and she performed well academically through college, earning a BA in education before beginning a 12-year career as an elementary school teacher.
At age 25, Client A was involved in a motor vehicle accident. Although a head CT scan and skull x-ray in the ER showed no damage, she reported brief loss of consciousness and believed she struck the left lateral frontal side of her head on the driver-side window. She experienced lingering headaches for several weeks, along with neck pain and fatigue. Physical therapy helped moderately with neck pain over approximately three months but did not resolve her headaches or fatigue.
Unable to find resolution through conventional providers, she pursued alternative approaches including massage, chiropractic care, herbal medicine, and acupuncture. Chiropractic adjustments were helpful but required regular visits (2-3 times per month), and acupuncture helped with neck pain and general malaise but similarly required ongoing sessions.
At the time of assessment, she continued to report neck pain, headaches, difficulty with focus and attention, and interpersonal difficulties, symptoms she stated were not present before the motor vehicle accident.
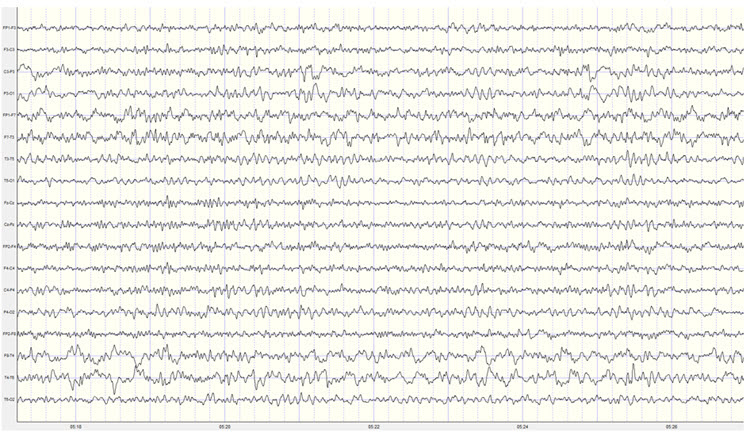
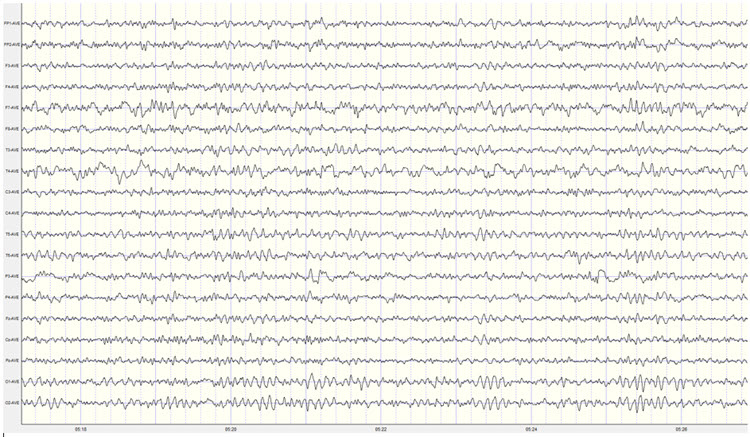
Electroencephalographic (EEG) data were collected using the international 10-20 electrode placement system with 19 active electrodes referenced to linked ear electrodes. A NeXus-32 acquisition unit with BioTrace+ software was used for neurometric EEG collection, and all electrode locations maintained a DC offset below 25 mV. Substantial eye movement was present in both eyes-closed and eyes-open recordings, along with persistent, localized EMG artifact throughout the eyes-open recording at the F7, F8, T3, and T4 electrode locations.
Following recording, the record was visually inspected and artifact-free epochs were selected from the eyes-closed recording. However, the persistent muscle artifact made it impossible to find artifact-free segments in the eyes-open recording, so the effect of this artifact is noted in the report below. Analysis was performed using the NeuroGuide database software, comparing Client A's record to age-matched normal research participants and a discriminant function database for traumatic brain injury. Further analysis used the Key Institute LORETA database version 2003 combined with Lifespan database z-scores. This appears to be a valid and interpretable administration.
The EEG was reformatted in various referential and bipolar montages for visual inspection.
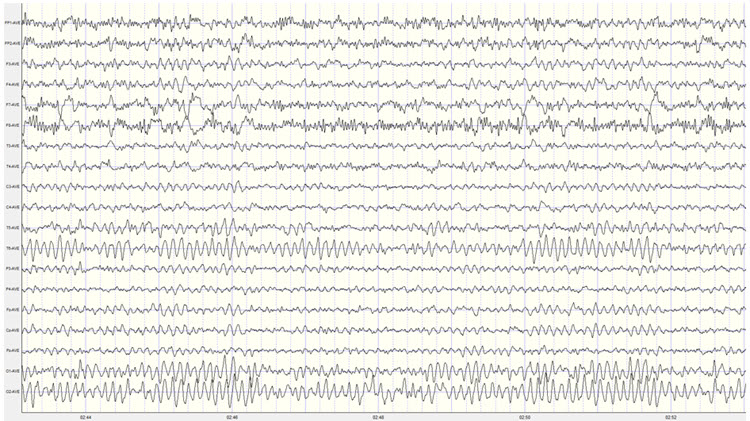
Visual Inspection of 19-Channel EEG
Eyes-Closed Condition: This fair-quality recording shows persistent EMG artifact primarily in left frontal and temporal derivations, with some presence in right frontal derivations. Typical lateral eye movement artifact appears frequently; segments containing artifacts were excluded from statistical analysis.
In the longitudinal bipolar montage, a generalized posterior dominant rhythm appears in the occipital and parietal derivations, extending somewhat to the central derivations. The frequency is approximately 9 Hz, with voltage generally in the 25-35 μV range and some bursts exceeding 50 μV at the P4-O2 derivation and 40 μV at P3-O1. Notably, the posterior rhythm is asymmetrical, with higher voltage on the right side, particularly in the T4-T6 and T6-O2 derivations.
When the record was re-montaged in various bipolar derivations, additional alpha activity appeared in the temporal leads, activity that likely also appears in the ear references. This contributes to reference contamination in the linked ears montage. Bilateral frontal, temporal, parietal, and occipital slow activity in the 3-5 Hz range was also present.
The average reference montage clearly identifies the 9 Hz activity at the T6 electrode at up to 40 μV, as well as the more right-sided, O2 distribution of the posterior rhythm.
The linked ears montage shows broadly distributed alpha activity, likely the result of reference contamination from the ear references noted earlier. Consequently, elevated z-score values for frontal alpha in the linked ears statistical topographic maps should be disregarded. In this montage, the posterior rhythm appears more symmetrical bilaterally at O1 and O2, but this is likely incorrect based on the findings from all other montage views.
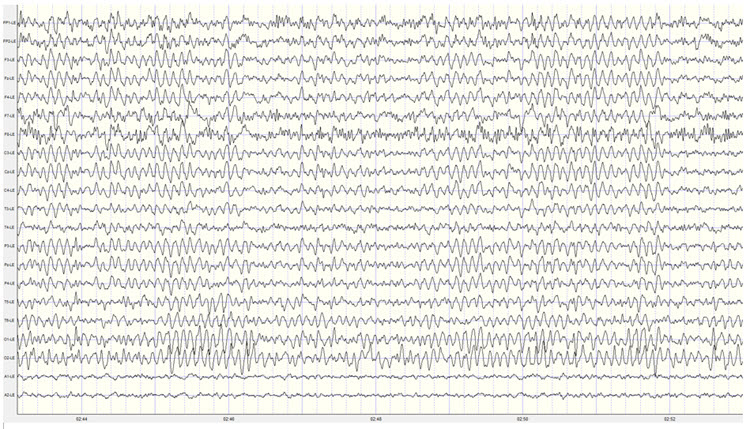
The Laplacian montage shows broadly distributed frontal and temporal EMG artifact, likely an aberration due to the reference method using adjacent electrodes for the montage calculation. Other montages localized the EMG artifact primarily to bilateral frontal and temporal derivations that did not include the F3, Fz, or F4 sensors.
Eyes-Open Condition: The linked ears montage shows appropriate attenuation of the posterior dominant rhythm to approximately 10-15 μV. Significant muscle artifact is present in frontal and temporal leads, as noted above. Removing the low pass filter confirmed this is indeed muscle artifact rather than 60 Hz or another exogenous source. Excessive, repetitive eye blink artifact was also present, rendering this eyes-open recording unsuitable for statistical analysis.
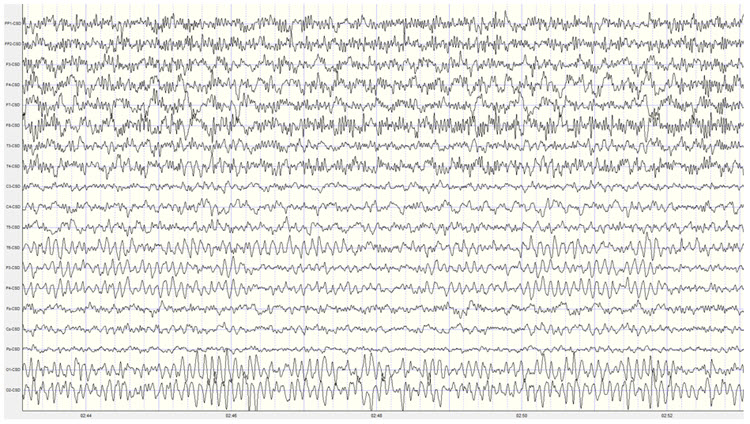
The quantitative analysis of Client A's eyes-closed EEG record reveals the following findings:
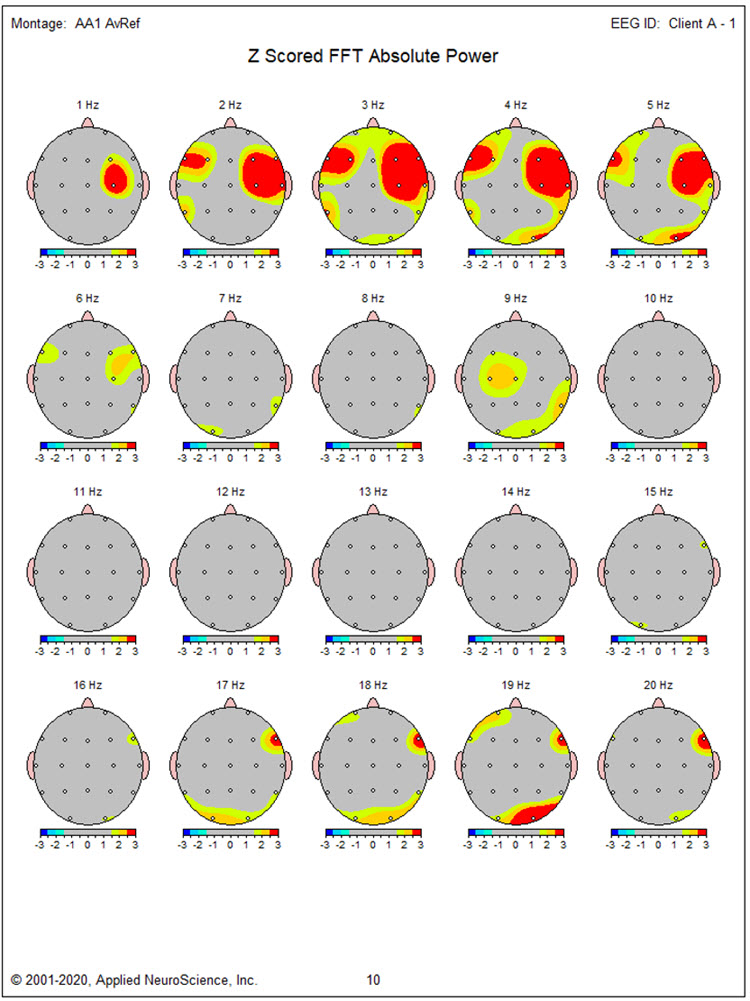
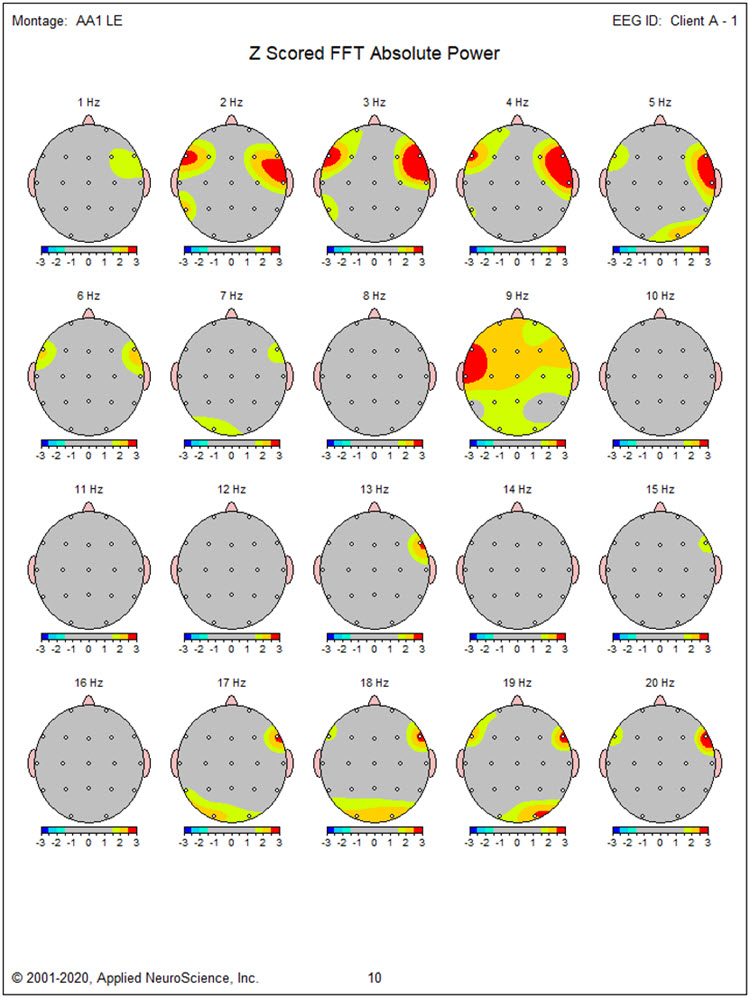
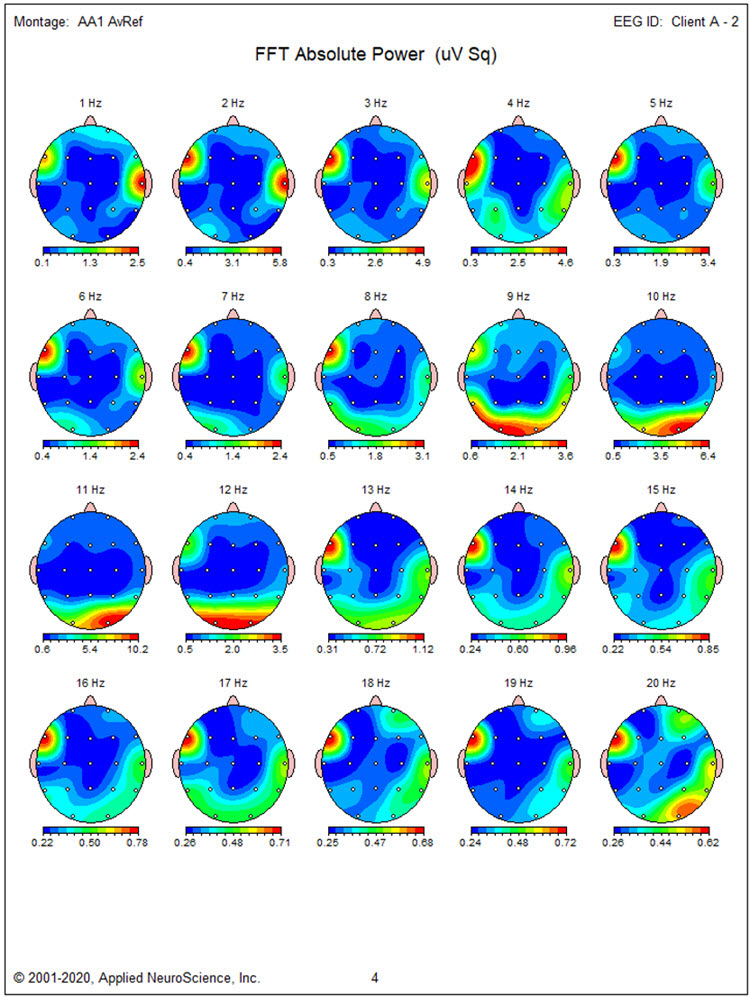
Absolute power topographic maps of the eyes-closed average reference montage show maximum voltage in the 8-12 Hz frequency range, peaking at 9 Hz at the O2 and T6 electrode locations.
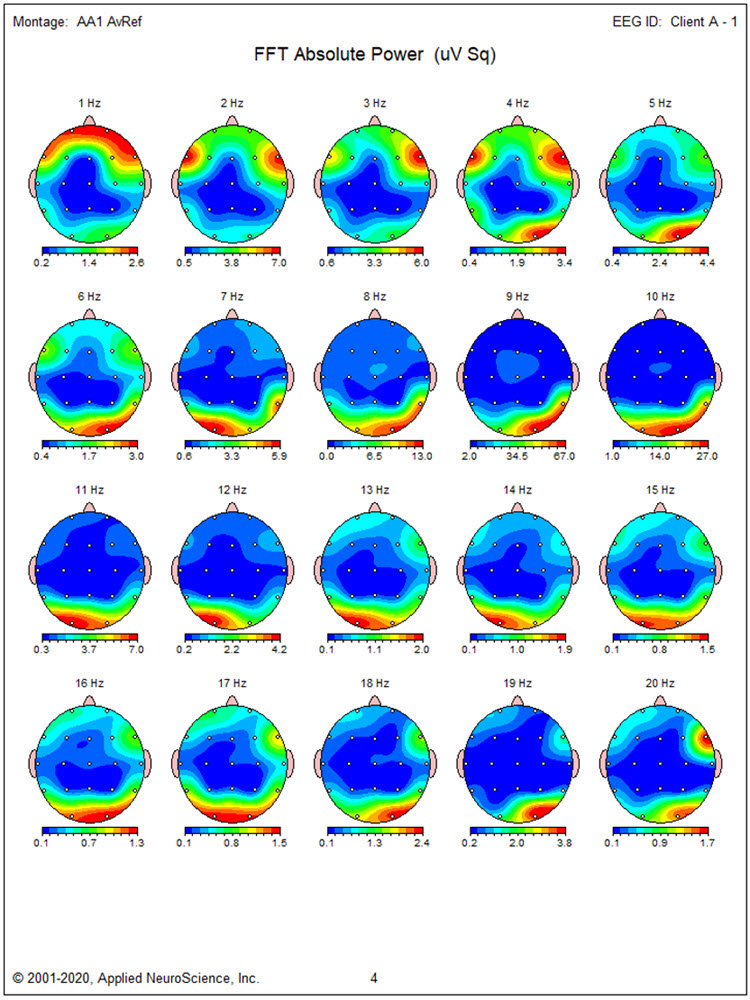
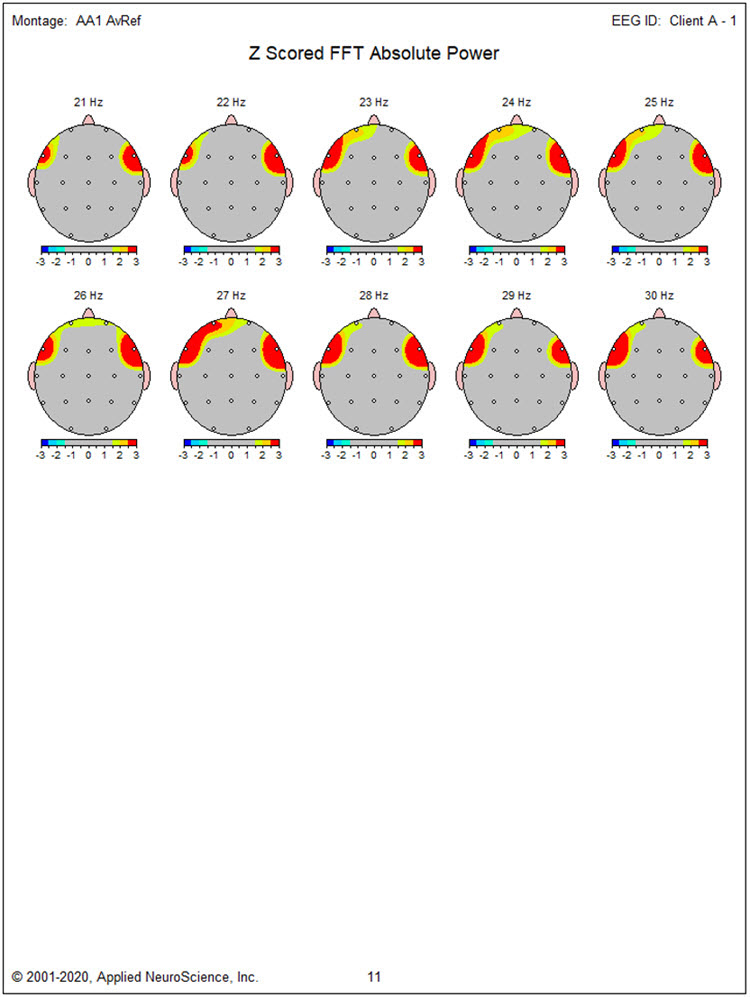
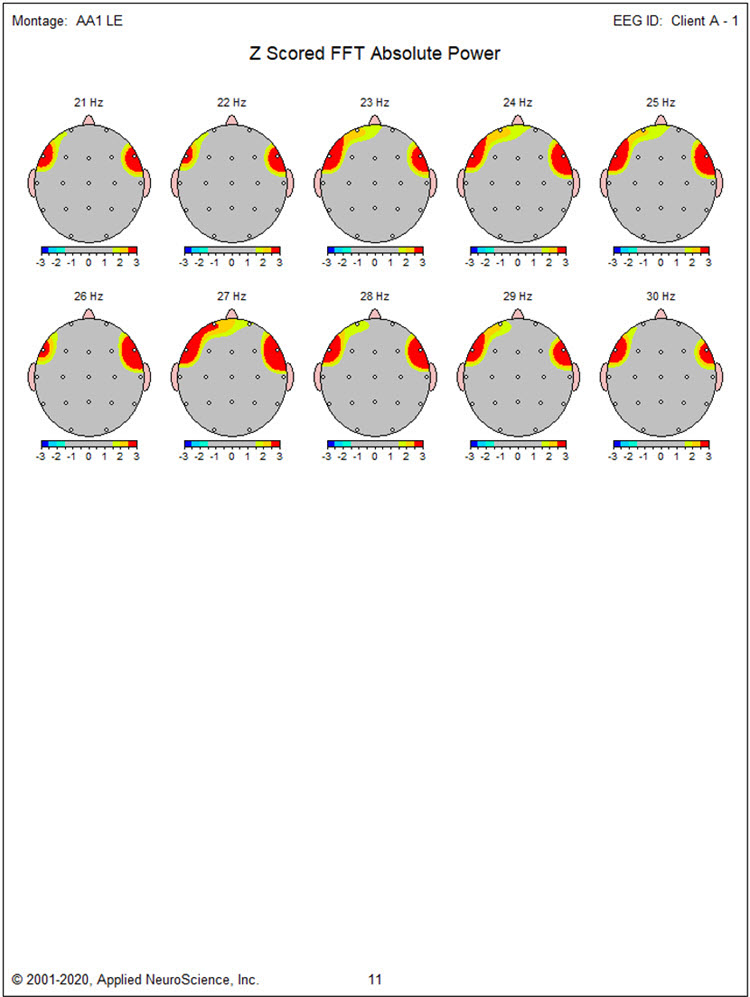
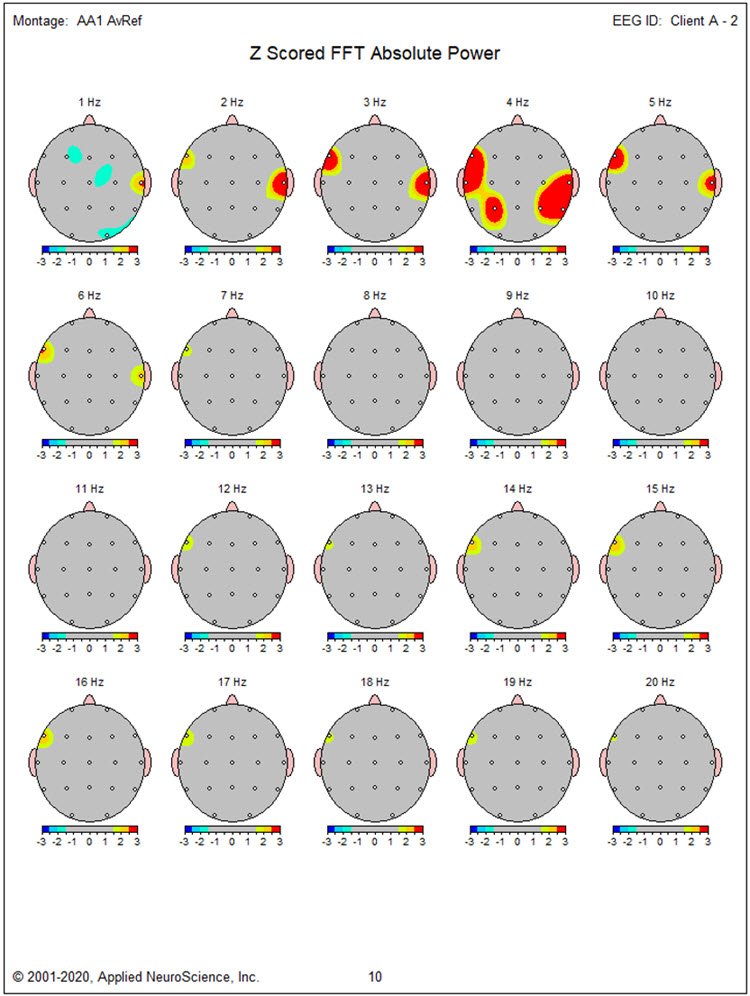
The statistical topographic maps of the eyes-closed average reference montage show the bilateral distribution of excess activity from 2-6 Hz with the greatest deviation from 2-5 Hz in bilateral frontal, temporal, right lateral parietal, and occipital electrodes. Excess activity at 9 Hz is localized to the F3, Fz, C3, and Cz electrodes and O2, T6, T4, and O1, with the greatest deviations in left central and right T6/P8 locations. Excess posterior 17-19 Hz activity and excess 17-30 Hz activity in bilateral frontal sensors are almost certainly associated with the EMG artifact noted earlier.
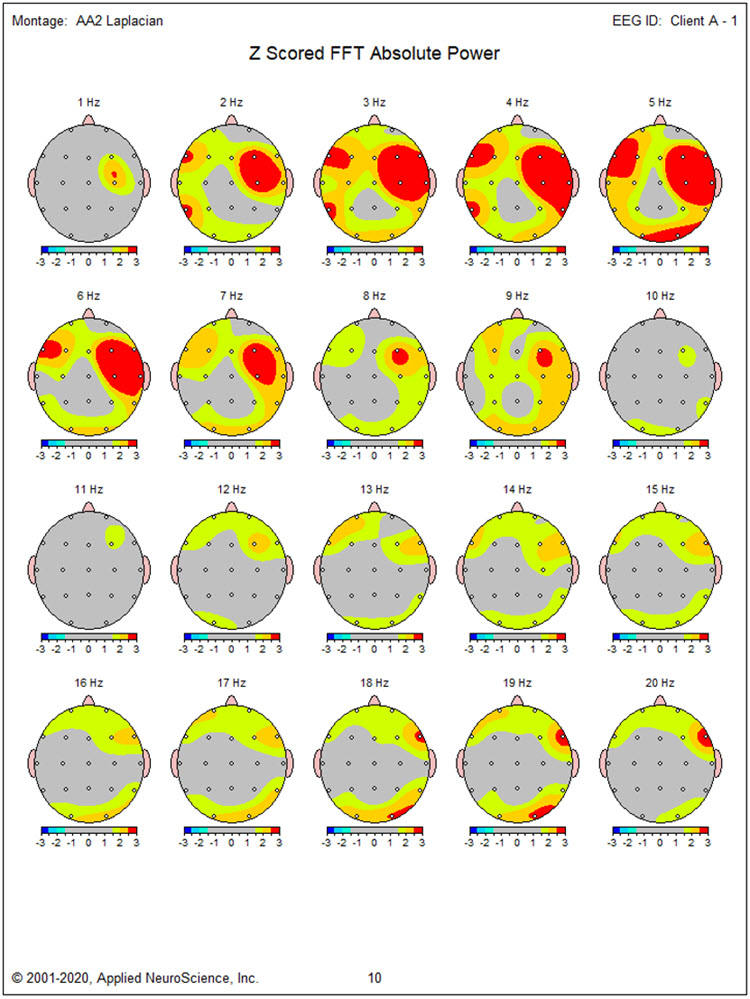
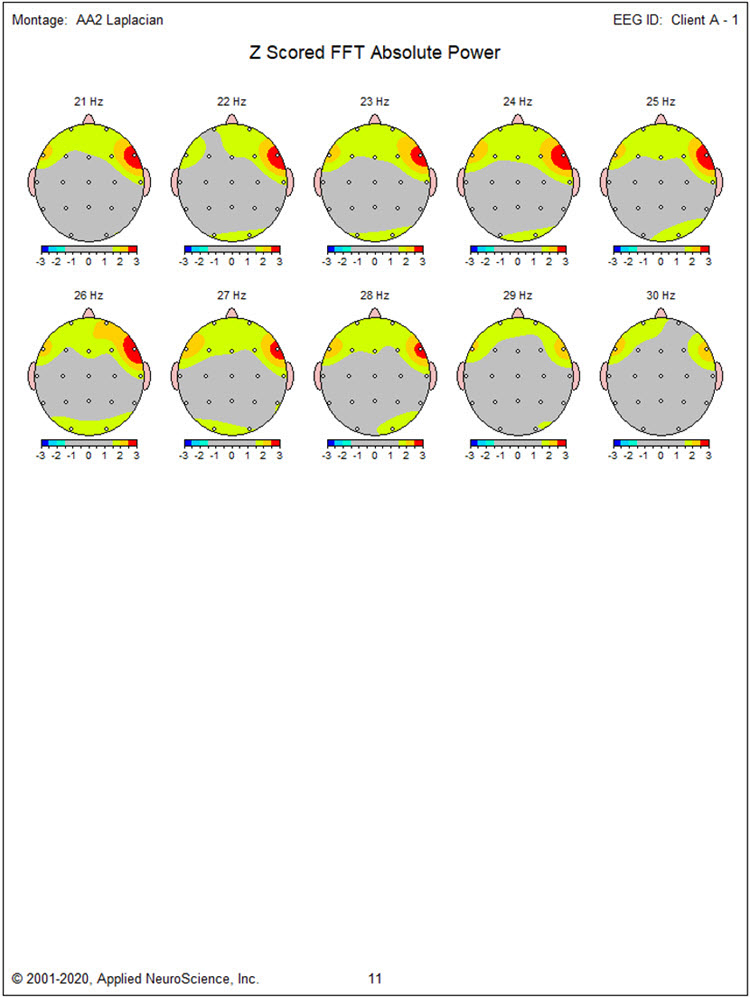
The Laplacian montage shows findings that are quite similar to those seen in the average reference montage with excess activity present from 2-9 Hz in this case. As discussed earlier, the excess fast activity is more pronounced and more broadly distributed, reflecting the EMG artifact, and should be disregarded.
The linked ears montage shows the bilateral slow activity from 2-6 Hz that extends to the right temporal and parietal/occipital areas. The excess 9 Hz activity is more localized to the left lateral frontal and temporal areas, although this may be related to the effect of reference contamination noted earlier. The excess activity from 17-19 Hz is seen in occipital sensors, and the excess lateral frontal 17-30 Hz EMG-related activity is seen here.
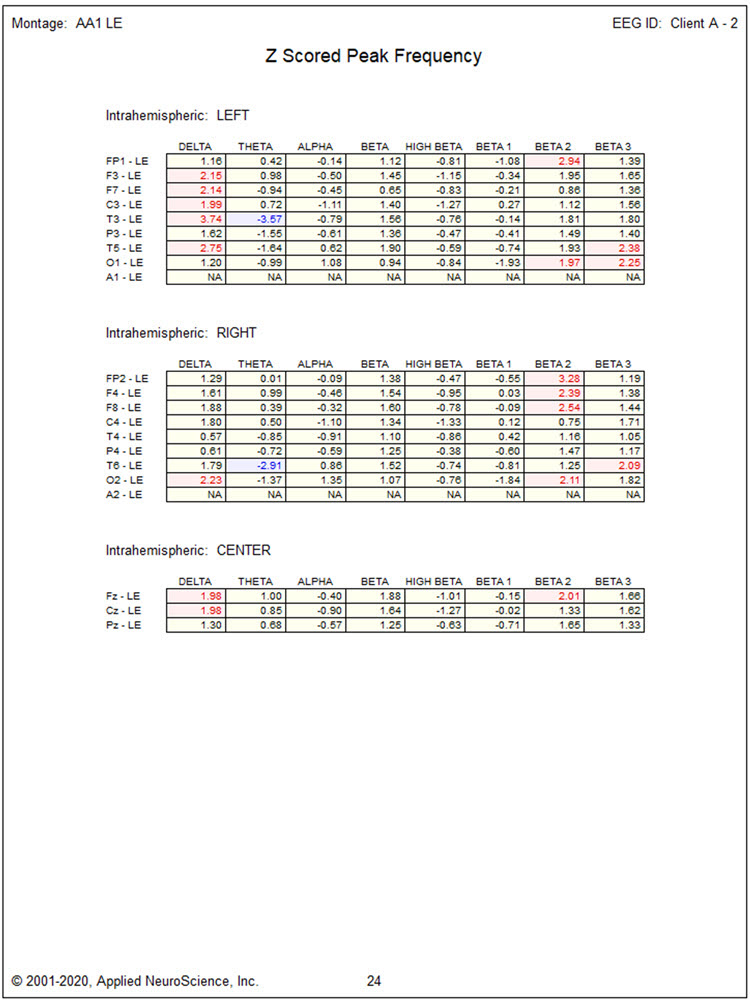
The z-scored peak frequency analysis in the linked ears montage shows some slowing of the peak alpha frequency, exceeding -1 standard deviation at C3, T3, P3, C4, T4, P4, T6, O2, and Pz, with the greatest slowing at the P4 electrode site at -1.31 SD.
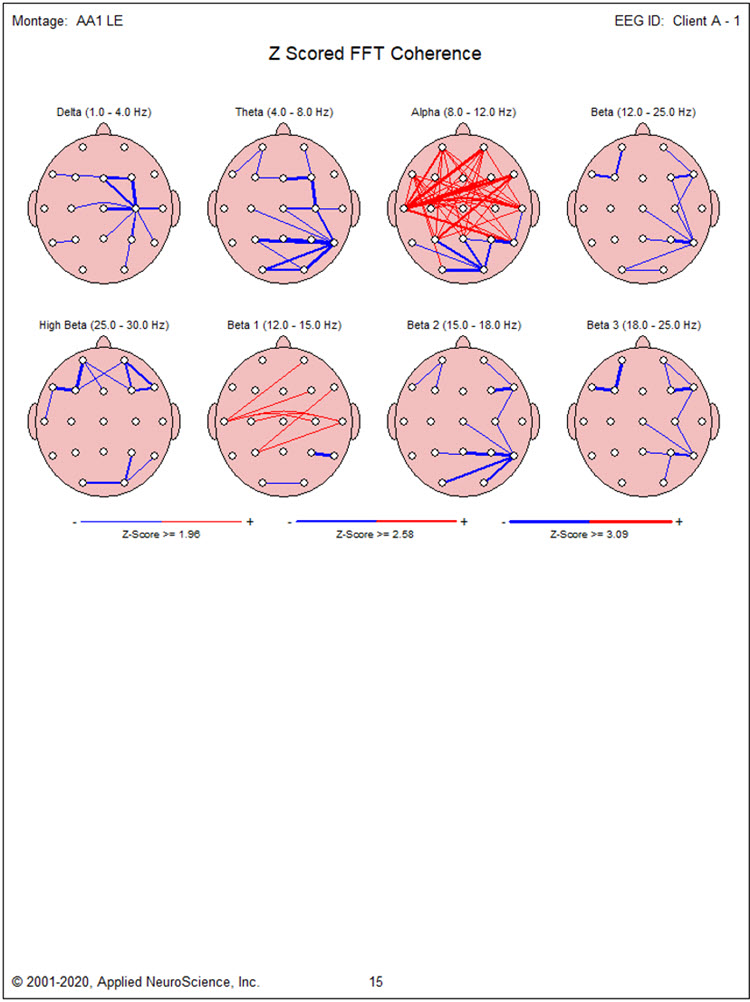
Coherence abnormalities show excess frontal, central, temporal and parietal hypercoherence in the alpha frequency band with some right lateral posterior and occipital hypocoherence in the theta and alpha frequency bands. There appear to be 2 somewhat focal areas of hypocoherence in multiple frequencies at the F7 and T6 locations.
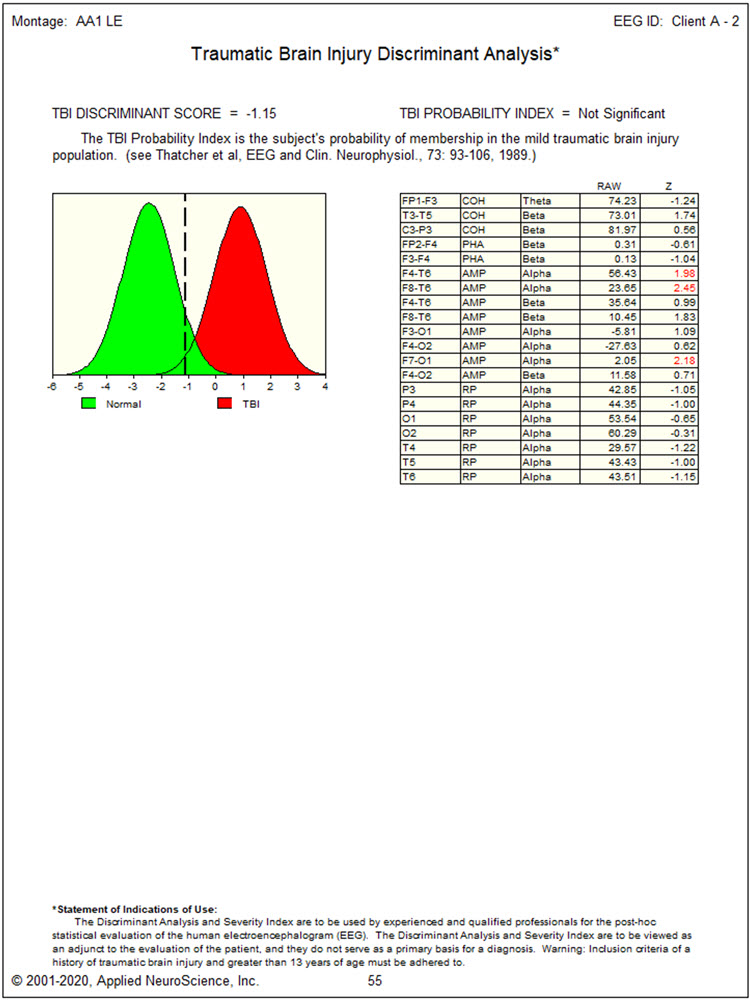
Due to the history of an automobile accident, the traumatic brain injury discriminant analysis was performed. It yielded a TBI discriminant score of 0.66, a TBI probability index of 99.5%, and a TBI severity index of 4.86, which is in the middle of the moderate range on a 0-10 scale where zero represents mild effects and 10 represents severe effects.
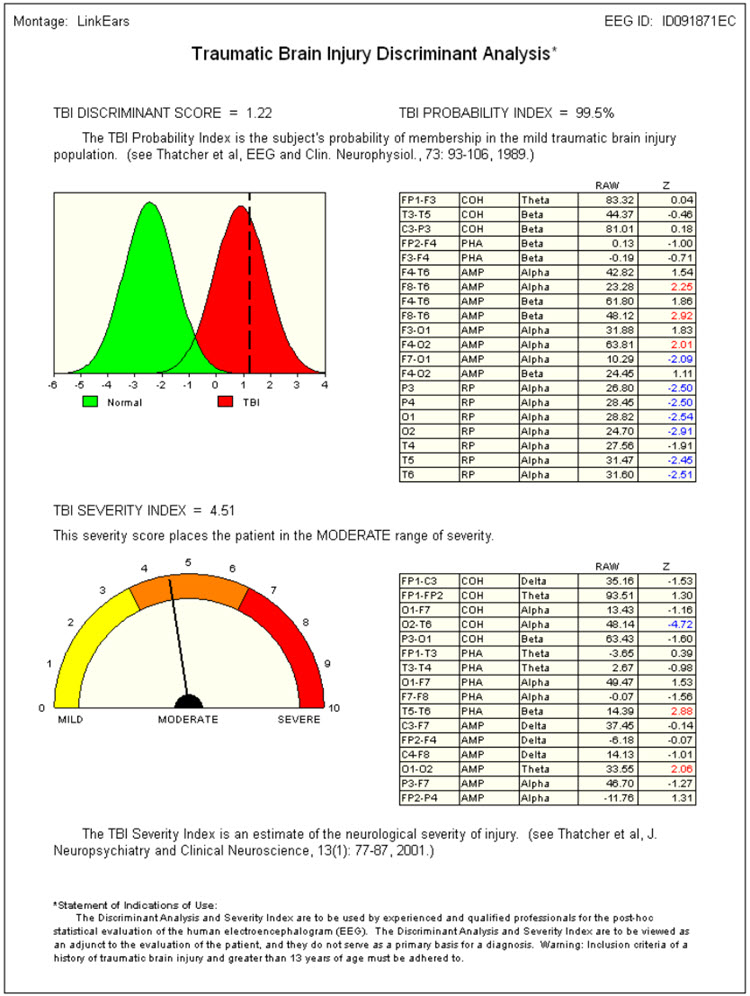
Conclusions: This client's findings suggest a possible lingering effect of the motor vehicle accident, with a pattern consistent with coup-contrecoup injury extending from the left lateral frontal area at approximately F7 to the right posterior temporal/parietal/occipital area at T4, T6, and O2. The left lateral frontal slowing may be associated with her experience of depression, the bilateral frontal slowing with her perception of attentional difficulties, and the right temporal and parietal involvement with her difficulties in social interactions.
A course of neurofeedback training is recommended, beginning with 4-channel z-score training to address these difficulties by correcting excess slow-frequency activity, normalizing coherence, and possibly resolving the slow peak alpha frequency. Initial sensor placement will be on F7, F8, T6, and O2 to normalize delta and theta frequencies, followed by O1, O2, Fz, and Pz to normalize the frequency and distribution of the posterior rhythm.
Finally, alpha-theta training, rewarding an increase in 6-9 Hz while stabilizing 2-6 Hz and 13-36 Hz, will be used to integrate changes and help resolve social anxiety. Additional home training is recommended, including heart rate variability training and peripheral temperature training with home devices. Sufficient in-clinic practice with these modalities should be provided to build familiarity with the techniques.
Disclaimer: This evaluation is not intended to diagnose any medical or psychological condition. It is also not intended to substitute for appropriate medical or psychological diagnosis and intervention. Diagnosis and treatment should rely on a physician or mental health provider. Areas that show differences from expected values and the description of common symptoms associated with dysregulation in these areas are speculative, based on current neuropsychological understandings. Descriptions may not apply to this client, and any suggested findings may need to be confirmed through other testing.
Neurofeedback Training: Client A participated in 32 sessions of neurofeedback training, scheduled 1 to 3 times weekly, and practiced daily at home with a RESPeRATE respiration training device. Initial 4-channel z-score training at F7, F8, T6, and O2 encouraged all 168 z-score variables to decrease toward zero. This approach proved quite successful; her referring psychologist reported that her depression was significantly improved, along with her ability to function in day-to-day situations, particularly in terms of focus and attention.
At session 15, her symptoms and training protocols were reviewed, and the electrode locations were changed to O1, O2, Fz, and Pz because the peak alpha frequency remained somewhat depressed. This configuration was used for 5 sessions before alpha-theta training was implemented using a 2-channel sum training approach with sensors at P3 and P4 and ear references. The reward was set to encourage an increase in 6-9 Hz while inhibiting 2-6 Hz and 13-36 Hz. This eyes-closed procedure used auditory feedback and was well tolerated; she reported finding it particularly calming and helpful.
After 12 sessions of alpha-theta training, Client A decided she had achieved her goals and requested a repeat 19-channel recording to see whether her EEG reflected the changes she was experiencing in her life.
This reassessment evaluates changes in Client A's EEG to guide decisions about further training. Data were collected using the same equipment and software as before and processed in the same manner.
Client A reports significant reductions in depression, improved focus and attention, and more energy to engage with others and participate in activities. She does report feeling slightly over-activated at times, which she says reminded her of how she was before the motor vehicle accident when she was a "go getter." She can manage this occasional overactivation using the breathing and heart rate training she has practiced at home.
This is a good-quality eyes-closed recording with minimal EMG artifacts at T3 and T4. Eye movement artifact is minimal, and overall voltage is somewhat reduced from the previous recording.
When viewed in the longitudinal bipolar montage, a posterior rhythm is seen primarily in the O1 and O2 derivations with a frequency of approximately 10 Hz and amplitudes in the 15-25 μV range, with some bursts exceeding 30 μV. The voltage is more symmetrical than was seen in the previous recording, and the voltage at the P3-O1 and P4-O2 electrode derivations is quite similar. As the recording progresses, the frequency does speed up a bit to the 10-11 Hz range.
A pattern of slow activity with a frequency of approximately 3-5 Hz is seen in derivations associated with the F7, T3, P3, T4, and T6 electrodes. However, the voltage is significantly lower than in the previous recording.
The average reference montage shows the more symmetrical posterior rhythm with a 10-11 Hz frequency and amplitudes of 20-25 μV range. There is beta activity in the 15-20 Hz range in frontal and central sensors, and the slow pattern appears to be most pronounced in the F7 electrode location.
The linked ears montage continues to show reference contamination. Still, it is in the 20-25 Hz range in this case. This frequency pattern is seen in nearly every sensor at similar frequency and amplitude and with the type of phase synchrony often seen in cases of reference contamination. This contamination may be related to the EMG artifact seen in the T3 and T4 electrodes.
The Laplacian montage shows more EMG artifacts in the T3 and T4 electrodes than in the other montages. This montage also seems to isolate the slow activity to the F7 electrode.
The absolute power topographic maps of the average reference montage show the more bilateral distribution of the posterior rhythm. The maximum voltage in the 8-12 Hz frequency band is at 11 Hz, closely followed by 10 Hz, though it remains somewhat lateralized to the right occipital at those frequencies.
The statistical topographic maps show excess 2-6 Hz activity at F7, T3, T4, P3, P4, and T6. The distribution of excess activity is less than seen in the previous recording but remains a potential for further training to resolve the slow activity in these areas.
The z-scored peak alpha frequency in the linked ears montage is now more typical and shows a negative standard deviation only at C3 and C4.
The TBI discriminant analysis surprisingly shows a non-significant value, which may be due to the reference contamination in the beta frequencies since that measure is calculated from linked ears data. It is unusual for this measure to change so drastically in so short a time, particularly when there is still significant slow activity in lateral frontal and bilateral temporal locations. It is also possible that the initial TBI finding was higher than typical given the reference contamination from slow alpha activity in the previous recording.
Conclusions: Client A appears to have benefited substantially from neurofeedback training combined with home respiration biofeedback practice. However, areas of slow activity remain that may be important to resolve. The increase in peak alpha frequency and her self-report of occasional overarousal may indicate a degree of overtraining that requires additional sessions to address. Because the client wishes to conclude training, she will be encouraged to return for a follow-up session in 3 months to determine whether she has achieved a more balanced state. She will also be encouraged to return for further training if she experiences negative effects, and to continue home training with the RESPeRATE breathing pacing device.
Disclaimer: This evaluation is not intended to diagnose any medical or psychological condition. It is also not intended to substitute for appropriate medical or psychological diagnosis and intervention. Please see your physician or mental health provider for appropriate diagnosis and treatment. Areas that show differences from expected values and the description of common symptoms associated with dysregulation in these areas are speculative based on current neuropsychological understandings. Descriptions may not apply to this client, and any suggested findings may need to be confirmed through other testing.
Patient Example B
This case involves a former college football player with a history of multiple head injuries. It illustrates how neurofeedback protocol selection adapts when TBI is longstanding and the client presents with a complex mix of cognitive, emotional, and interpersonal symptoms.
Patient Information
| Name: Client B | Date: 02/20/2014 |
| Exam#: Client B 10001 | Ref. By: Self |
| Age: 57.51 | Test Site: MNI |
| Gender: Male | Handedness: Left |
Recording
| Analysis Length: 01:42 | Ave. LE Split-Half Reliability: 0.98 |
| Ave. LE Test-Retest Reliability: 0.94 | Eyes: Closed |
Medication: None noted
History: Client B presents with a diagnosis of traumatic brain injury (TBI) from multiple head injury events during high school and college football. During his college career, he sustained one particularly significant injury from helmet-on-helmet impact to the left lateral frontal area, resulting in approximately 10 minutes of loss of consciousness followed by confusion and dizziness. He returned to the game in the second half after sitting out the rest of the first half, a decision that would not meet current concussion protocols. Lingering symptoms persisted through the following summer after graduation, and although they faded over time, he reports never feeling that he returned to his "normal self." He nonetheless became a successful businessperson.
He reports persistent depression with a lack of motivation and a significant struggle to function in daily activities. He also describes a "temper" that has cost him several relationships; he is currently divorced from his third wife and believes his mood regulation problems are primarily responsible. Symptoms endorsed include depression, headaches, feelings of loneliness, memory problems, occasional dizziness, mild to moderate general anxiety, some fear or panic experiences, difficulties with sequential processing, emotional sensitivity, social discomfort, problems falling asleep and restless sleep, slow processing and response, poor reading comprehension, difficulty understanding concepts, and a lack of well-being.
Visual Inspection of 19-Channel EEG
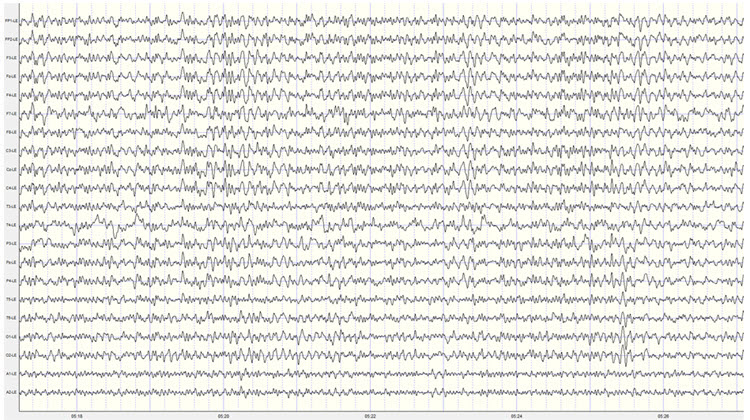
Eyes-Closed Condition: Longitudinal Bipolar Montage: this is a good quality recording with moderate eye movement artifact and only intermittent movement and EMG artifact. There are no discernable mains or equipment artifacts.
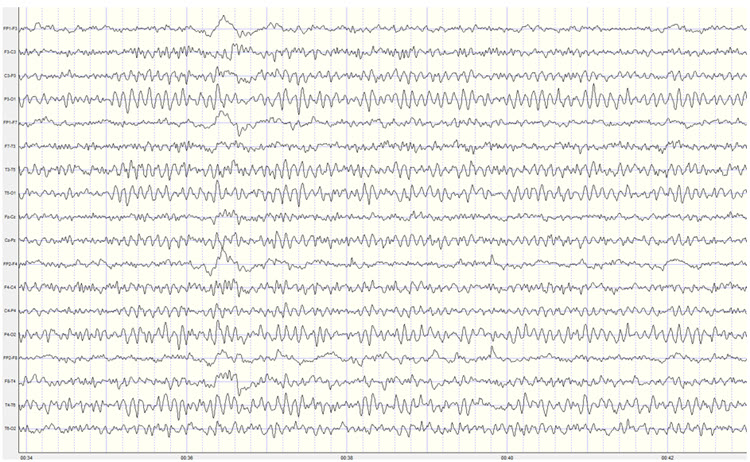
The longitudinal bipolar montage shows a clearly defined posterior rhythm in derivations including temporal, parietal, and occipital electrodes. The frequency of the posterior rhythm appears to be somewhat inconsistent and ranges from 8-10 Hz. Amplitudes are generally in the 10-15 μV range with bursts up to 40 μV, occasionally exceeding 55 μV.
There is a clear pattern of slow activity in left lateral frontal derivations that include the Fp1-F3, Fp1-F7, F7-T3, and T3-T5 electrodes. There is also what appears to be a corresponding area of slow activity in the right temporal and temporal-parietal derivations. There is beta activity frontally in the 15-20 Hz range.
There is a period of apparent light or stage one sleep in the middle of the recording, interspersed with brief awakenings. The sleep EEG shows occasional vertex sharp waves but no other sleep characteristics. This pattern resolves, and Client B returns to an awake eyes-closed state for the rest of the recording.
The average reference montage also shows a well-developed posterior rhythm with the maximum voltage in the O1 and O2 electrodes, with additional posterior rhythm activity at T5, T6, P3, and P4. The voltage at T6 is nearly as high as in occipital sensors. The frequency continues to fluctuate between 8-10 Hz, and voltage is in the 10-20 μV range with bursts regularly exceeding 40 μV and occasionally 50 μV.
A pattern of slow activity is seen in this montage as well, with the clearest and most consistent activity in the left and central frontal, left central, right frontal, and right parietal and occipital areas, with frequencies varying between 2 and 4 Hz. There is also some alpha activity in frontal sensors, particularly at F3 and Fz.
The Laplacian montage also shows the posterior rhythm in occipital and parietal areas and shows a mixed pattern of activity at the T4 and T6 electrodes, with slower activity in the delta and theta frequencies mixed with alpha and beta frequencies. Left-sided slow activity is also seen.
The linked ears montage shows broadly distributed alpha activity suggesting reference contamination. The highest voltage of the posterior rhythm is in the occipital electrodes. There is alpha activity in the reference electrodes and a pronounced ECG artifact that will likely produce excess 1 Hz statistical values in the z-score analysis. This should be disregarded.
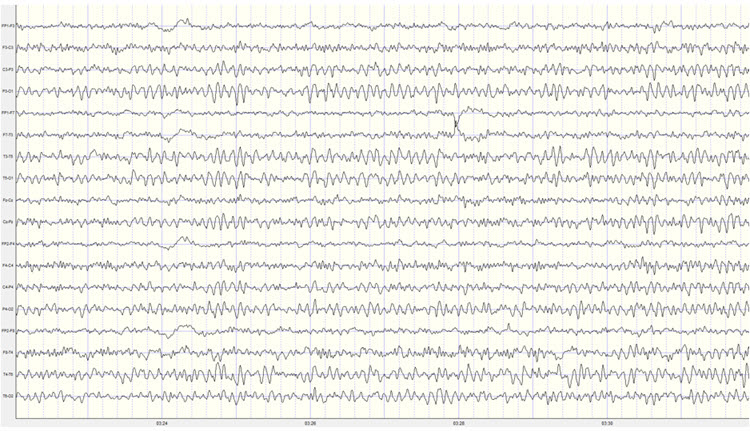
The sequential eyes-open, eyes-closed recording shows a typical alpha response upon eyes closing and appropriate alpha blocking upon eyes opening in this repetitive series of 15-30 second eyes-open and eyes-closed segments (see image below).
Eyes-Open Condition: Visual inspection of the eyes-open longitudinal bipolar montage recording shows appropriate attenuation of the posterior rhythm upon eyes opening.
Background activity shows mixed frequencies, including delta, theta, and beta frequencies. Beta frequencies are in the 20-30 Hz range. Alpha intrusions are also seen quite often in central-parietal, temporal-parietal, and parietal-occipital derivations. The slow patterns noted earlier are seen in frontal-central, central-parietal, and right-sided temporal-parietal and parietal-occipital derivations.
The average reference montage shows more widely distributed alpha activity throughout the recording, possibly due to the generalizing effect of averaging all electrodes for the reference. Otherwise, the findings are consistent with the long bipolar montage.
The Laplacian montage shows the alpha activity mostly in occipital areas and the mixed slow and fast activity in the T6 electrode noted in the eyes-closed recording.
The linked ears montage shows a generalized pattern of 9-10 Hz activity mixed with beta and theta frequencies.
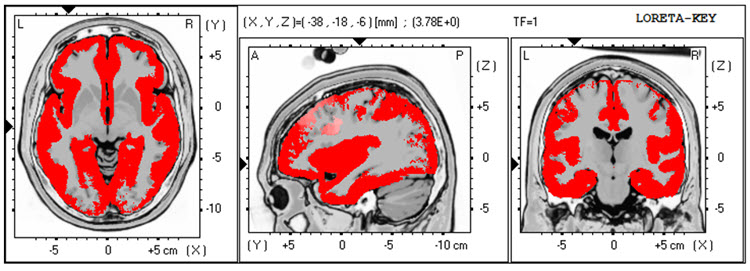
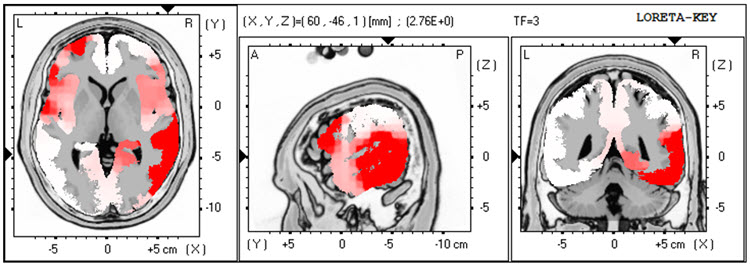
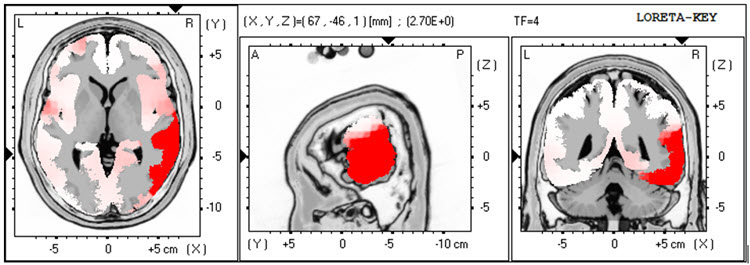
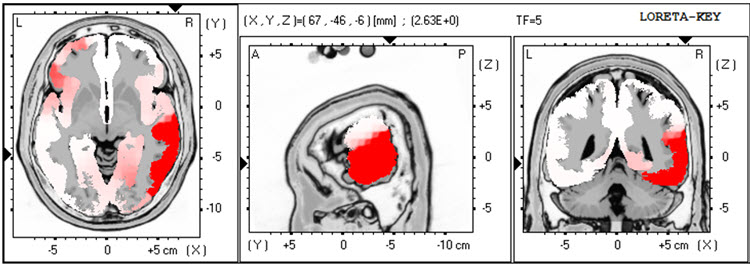
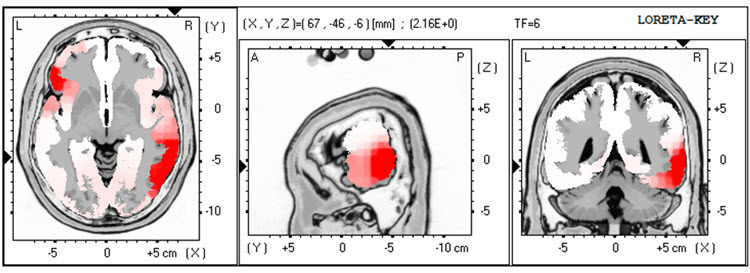
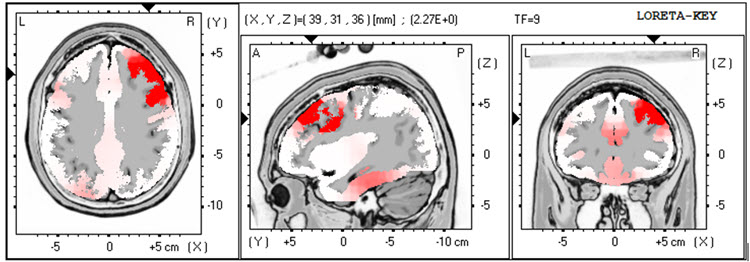
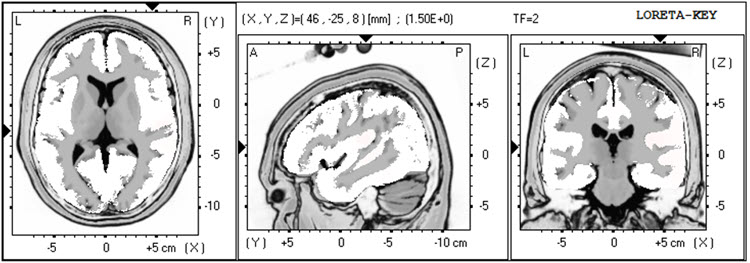
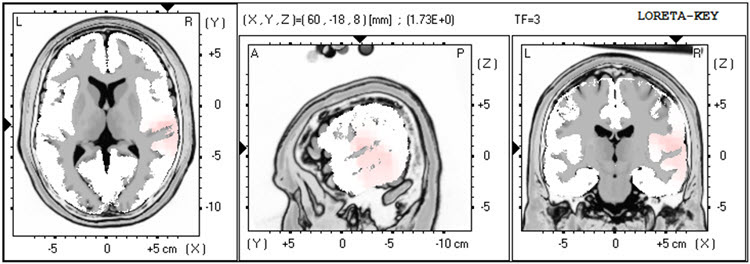
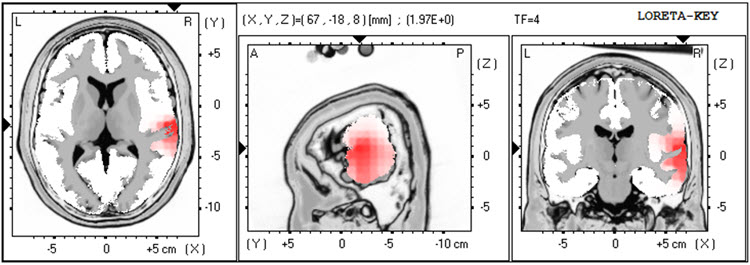
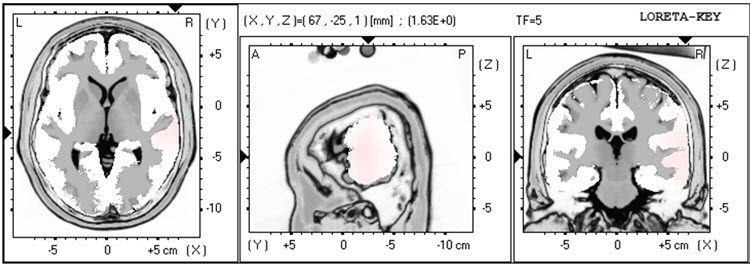
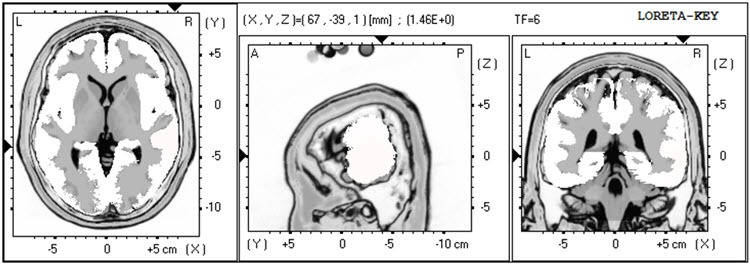
The LORETA analysis shows broadly distributed 1-Hz activity which is expected due to the ECG artifact, and also shows the lateralized left frontal and right posterior temporal/parietal areas as exceeding 2 standard deviations at 2-6 Hz, as well as right lateral frontal 9 Hz activity exceeding 2 standard deviations (see LORETA images below).
Quantitative Analysis: The analysis of the absolute power topographic maps of the average reference montage of the eyes closed recording shows the maximum of the 8-12 Hz frequency band to be at 9 Hz in bilateral occipital electrodes, followed by 10 Hz at approximately half the power. (These maps display power in μV2; power is amplitude squared, so power and amplitude differences are not interchangeable.) There is a clear right posterior temporal/parietal activity distribution from 2-15 Hz, reflecting the visual inspection findings.
The statistical topographic maps of the eyes closed average reference montage show broad distribution of 2.5-3 SD activity at 1 Hz, associated with the ECG artifact noted earlier, and this should be disregarded. There is excess activity in Fp1, F7, C3, Fz, F4, T4, T6, Pz, O1, and O2 electrodes from 2-3 Hz, with lesser, mostly right temporal and posterior excess from 4-5 Hz. The greatest deviation is at the F4, T6, and O2 electrodes exceeding 2.5-3 SD.
There is also excess bilateral frontal and left frontal/central and right parietal/occipital 9 Hz activity with the greatest deviation between F3, Fz, C3, and Cz. There are moderate excess occipital and right parietal 12-14 Hz activity and some 19-22 Hz excesses.
The peak alpha frequency is slightly slow but does not exceed -1 SD at any location.
The Laplacian montage shows the 1 Hz activity related to the ECG artifact. This montage shows the maximum deviation from 2-5 Hz at T6 with lesser deviations in the left lateral frontal, frontal, central, parietal and occipital areas. The excess 9 Hz is seen here, with some minimal 13-14 Hz activity in the right occipital and parietal areas.
The linked ears montage shows more distribution and greater deviation in most frequencies noted previously. Interestingly, the excess slow activity shows a much more lateralized presentation than was seen in the other montages. This may be due to reference contamination, and it could be coming from the area of the T4 and T6 electrodes, which are near the right-sided reference.
Coherence abnormalities are pronounced, but this is likely not reliable due to reference contamination in the linked ears montage.
Due to the reports of multiple impact injuries to the head, the Traumatic Brain Injury Discriminant Analysis was performed. It yielded a TBI discriminant score of -0.43, a TBI probability index of 80.0%, and a TBI severity index of 5.44, which is in the moderate range on a 0-10 scale, where 0 represents mild severity and 10 is severe.
Conclusions: This client presents with multiple issues that may relate to the observed EEG findings. The slow activity in left frontal areas and the combination of slow activity plus higher-than-typical alpha amplitude in right posterior temporal/parietal areas are particularly noteworthy. Although the peak alpha frequency slowing is not statistically significant, normalizing this frequency may improve his cognitive function.
Recommendations: A course of neurofeedback training is recommended, beginning with 4-channel z-score training that rotates between electrode combinations: Fz, Pz, T3, and T4 first; then F3, F4, T5, and T6; followed by C3, C4, P3, and P4. Other protocols may be explored as training progresses.
Summary of Client Responses to Training: Client B completed 25 sessions of neurofeedback training over 15 months, scheduled weekly at first and less frequently during the second half of that period. He also used a home heart rate variability training device and an audiovisual entrainment (AVE) device. Session training included 6 sessions at Fz/Pz/T3/T4, 2 sessions at Fz/Pz/P3/P4, 11 sessions at T5/T6/O1/O2, and 1 session at F3/F4/P3/P4, all using 4-channel z-score training. He also received 2 sessions of 4-channel slow cortical gradient training and 3 sessions of C3/C4 2-channel difference and sum training with variable reward frequency. Alpha-theta training was attempted on a few occasions, but he did not find it agreeable, so training was changed within those sessions to one of the other protocols.
He reports significant improvement in his ability to focus and in mood regulation. He is in a new relationship and states that his temper is much more manageable, having learned improved communication skills through couples counseling with his current significant other. He notes increased energy, improved sleep, and better cognitive function. Headaches still occur occasionally but with markedly decreased intensity and duration. Feeling that he has resolved his presenting concerns, he requested a follow-up EEG to see whether the assessment would reflect the changes he is experiencing.
Second Recording
| Analysis Length: 01:32 | Ave. LE Split-Half Reliability: 0.97 |
| Ave. LE Test-Retest Reliability: 0.94 | Eyes: Closed |
Visual Inspection of Follow-Up 19-Channel EEG:
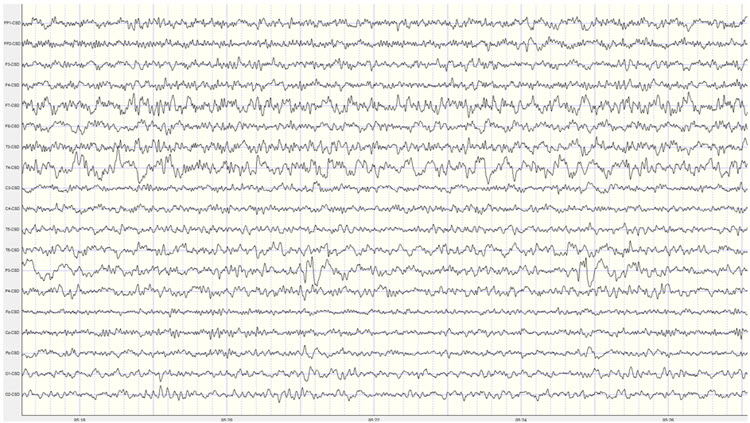
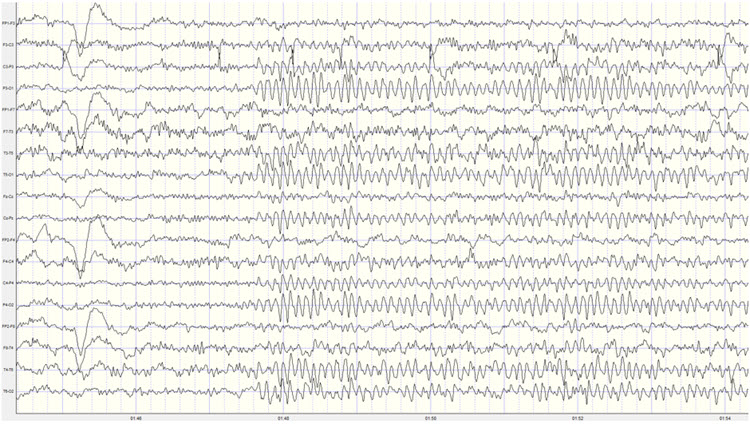
Eyes-Closed Condition: Visual inspection of the 19-channel EEG in the eyes closed condition using the longitudinal bipolar montage shows a good quality recording with typical eye movement artifact and some brief episodes of what appears to be drowsy or light sleep activity. There is no evidence of EMG artifact, mains, or other exogenous artifacts in this recording. This recording appears to be significantly lower in amplitude than the previous recording.
A well-developed posterior rhythm is seen primarily in parietal and occipital derivations with some temporal-parietal and central-parietal derivations. There is some spindling beta activity seen with the frequency of 20-25 Hz. This occasionally occurs in frontal-central derivations. There is some slow activity in the left lateral frontal areas and the right posterior temporal/parietal areas.
The posterior rhythm shows a consistent frequency of 9 Hz with a well-developed sinusoidal rhythm and amplitudes generally in the 20-30 μV range, with occasional bursts exceeding 30 μV. The posterior rhythm appears quite symmetrical between left and right locations, with the maximum voltage in parietal-occipital derivations.
The average reference montage shows more generalized alpha activity, possibly suggesting some distribution associated with the averaging method of the montage. The posterior rhythm is seen with the highest voltage at O1 and O2, closely followed by T6. The frequency remains at 9 Hz and is quite consistent, with amplitudes in the 20-30 μV range occasionally exceeding 30 μV. Again, the periods of possible drowsiness or light sleep are seen that occur quite infrequently and do not persist for any length of time.
The Laplacian montage also shows the posterior rhythm in occipital sensors and right parietal T6 and lateral parietal P3 and P4 locations. There is beta activity in the 15-25 Hz range in frontal and central sensors, and there is some slow activity in left-sided frontal and right-sided parietal areas.
The linked ears montage shows widespread alpha activity in all sensors, including the bilateral reference channels, and therefore reference contamination is present.
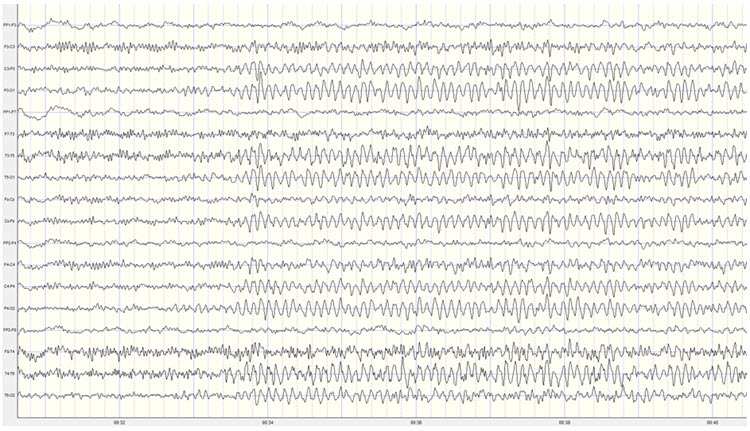
When viewed in the longitudinal bipolar montage, the repetitive eyes-open and eyes-closed segments show a clear alpha response upon eyes closing and immediate alpha blocking upon eyes opening (see example below).
Eyes-Open Condition: Visual inspection of the eyes-open longitudinal bipolar montage recording shows appropriate attenuation of the posterior rhythm with typical eyeblink and eye movement artifact. There is beta activity in the 15-25 Hz range in all electrode derivations. There are occasional alpha intrusions into the eyes-open recording, although these are infrequent and do not persist.
The average reference montage shows essentially the same findings though there is some persistent mixed frequency activity in the T4 and T6 electrodes, with alpha and beta frequencies occurring simultaneously.
The Laplacian montage shows higher amplitude mixed frequency activity at the F7 electrode and T4 and T6 electrodes. This activity includes a pattern of activity at approximately 8-9 Hz, 13 Hz, and also at 23 Hz.
The linked ears montage again shows broadly distributed activity that is quite synchronous and likely represents reference contamination.
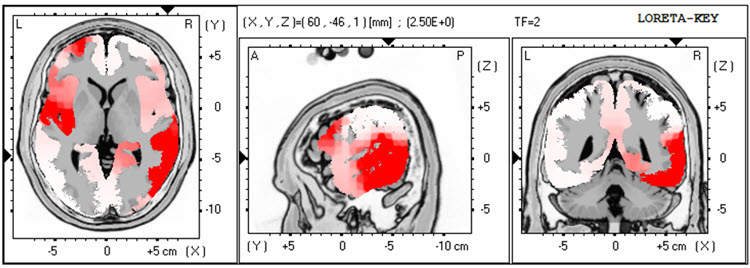
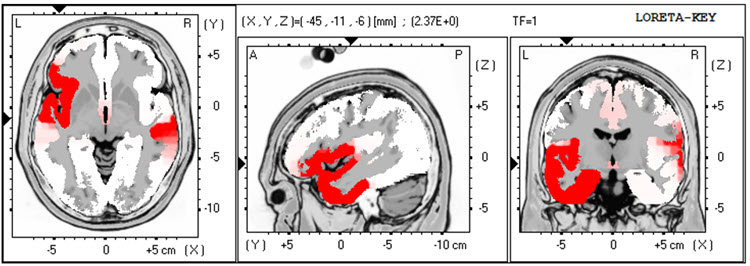
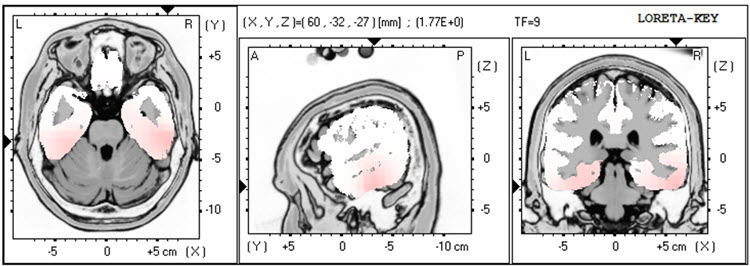
LORETA analysis of the follow-up 19-channel EEG recording shows the same lateralization exceeding 2 standard deviations seen in the previous recording, but in this case, only seen at 1 Hz in the left lateral frontal and right temporal areas. This activity is not seen at 2-3 Hz, and there is an area of excess activity in the right temporal area at 4 Hz, again exceeding 2 standard deviations. There is minimal excess activity at 9 Hz in the bilateral inferior temporal, fusiform, and parahippocampal gyri. (See LORETA images below).
Analysis of the eyes-closed average reference montage absolute power topographic maps from the 2nd recording shows the maximum in the 8-12 Hz frequency band at 9 Hz, with a power value approximately two-thirds of that seen in the previous recording.
The statistical analysis of the absolute power topographic maps in the average reference montage of the eyes-closed recording shows excess activity exceeding 2 standard deviations at F7 and T4, with lower levels of deviation at Fp1, F8, Cz, C4, and T6. Additional activity areas exceed 2 standard deviations at 2 and 3 Hz at T4 and T6. There is excess activity in the 1-1.5 standard deviation range in the left frontal and central areas and the bilateral posterior, including T6, and finally, a small area of excess activity at 13 Hz at T6 and O2. These findings are significantly diminished from the previous recording and likely reflect behavioral experience changes. Some areas of excess activity from 21-23 Hz appear associated with the Fz electrode, which will be evaluated further in other montages.
The peak alpha frequency remains within the normal range in all locations and only exceeds a -1 standard deviation at the T4 electrode location.
The Laplacian montage essentially shows the same findings except for the right temporal/parietal area activity extending up to 5 Hz and the excess 9 Hz activity in more circumscribed locations. Also, the excess 21-23 Hz activity is associated with the Cz electrode, and therefore that seen in the average reference more broadly distributed is almost certainly due to reference contamination from the averaging mechanism in that montage.
As expected, the linked ears montage shows a broadly distributed excess activity pattern from 6-15 Hz across frontal areas reflecting the reference contamination noted earlier. Otherwise, it also shows the laterality seen in the previous recording from the left lateral frontal to the right temporal, possibly related to reference contamination.
The comparison to the previous traumatic brain injury discriminant analysis shows very similar findings, with the TBI discriminant score at -0.03, the TBI probability index at 90%, and the TBI severity index at 5.42, which is similar to that seen previously.
Conclusions: The quantitative findings are substantially improved and support his self-report of improvement in multiple areas of functioning, although the TBI discriminant measures are essentially unchanged. Client B was encouraged to return for further sessions if problematic symptoms increase, to continue heart rate variability training at home, and to continue using the audiovisual entrainment device (AVE).
Patient Example C
This case demonstrates how excess frontal beta activity associated with anger and aggression can be targeted with neurofeedback, and how pre- and post-training qEEG assessments document neurophysiological changes alongside clinical improvement.
History: TR is a 41-year-old man injured in a car collision two years earlier. He sustained a mild concussion and soft tissue injuries that limited his ability to work as an independent construction contractor, though he gradually returned to part-time work.
He was referred primarily for anger and aggressive behavior directed at his insurance provider. TR believed his insurer had not provided sufficient benefits after his injury and continued to withhold deserved coverage. Beyond this specific conflict, he was also much more likely to feel and express anger in everyday situations such as traffic. TR described his experience of anger as his "brain being on fire."
In addition to anger, TR reported that his head felt "heavy and full" most of the time and that he had difficulty falling asleep, though he denied any thinking deficits. These emotional, behavioral, and somatic symptoms developed gradually following the collision but appeared to worsen a pre-injury tendency toward anger and aggression. TR reluctantly admitted that his anger, though he felt it was justified regarding his insurer, was interfering with his ability to work with his construction teammates.
TR's only medication was low-dose amitriptyline for sleep, and he did not drink alcohol. His previous medical history was significant only for a construction-related dislocated shoulder, and he had no history of psychiatric, alcohol, or drug treatment. He graduated from high school before working full-time in home and agricultural construction, with no history of legal difficulties. A paralegal assisted with his traffic collision insurance claim.
He had a significant history of conflict with his father, from whom he was estranged, though he visited his mother regularly. TR and his wife had no children.
TR is the younger of two siblings, with an older sister who lives at some distance. His family health history included his father's alcoholism and his mother's congestive heart failure. His father had not completed high school and worked building barns and other agricultural structures.
Assessment: The information above was gathered during an interview with TR and his wife, who corroborated his history. His wife was very concerned about his anger and had facilitated his attempt to get counseling. During the assessment, TR's behavior was notable for loud and rapid speech, an intimidating posture, and a tense facial expression.
A review of health records was consistent with the history and showed no cerebral injury on a head CT performed on the day of the collision. Neuropsychological screening six months post-injury showed most cognitive domains within expectation, except for mildly deficient attention and speed of processing. Psychological assessment showed elevated anxiety and anger/aggression symptoms but did not meet all criteria for PTSD; TR did not believe he would die at the time of the collision and did not have re-experiencing symptoms. After reviewing confidentiality limits, TR agreed to a qEEG assessment.
Pre-Neurofeedback qEEG Assessment
19-channel EEG recordings were collected in both eyes-open and eyes-closed conditions, artifacted, and analyzed with NeuroGuide's software and normative database after examining EEG traces in several montages (i.e., longitudinal bipolar, linked ears, Laplacian, average reference). All artifacted data were sufficiently reliable for analysis. The range of significance in color for topographic maps extends from +1.5 standard deviations to +4.5 standard deviations to show the greatest area of localization for extremely high values of beta activity. All LORETA analyses set their significance level at 3 standard deviations.
Baseline Eyes-Closed EEG Traces: EEG traces showed good production of symmetric alpha activity, although with a peak only at 9 Hz. There appeared to be excess beta activity, most prominently at F3 and Fp1, Fp2, F4, and T4. The four montages shown below appeared consistent, with the excess high beta wave morphology consistent with EEG rather than EMG activity.
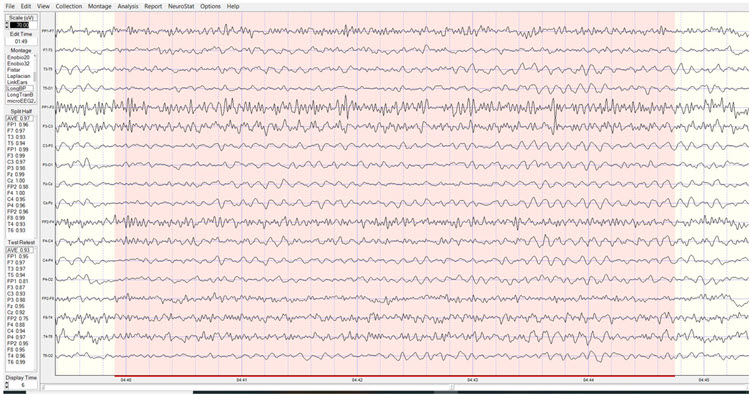
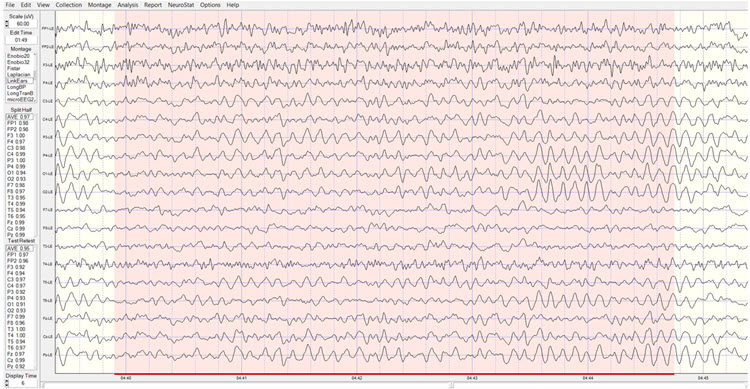
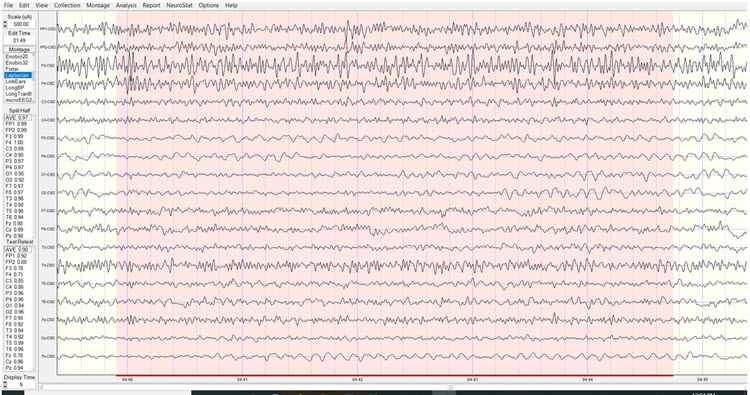
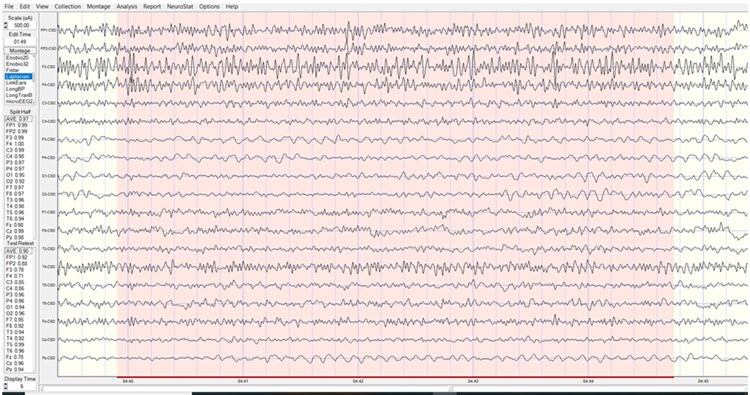
Baseline Eyes-Closed qEEG Findings: Figure 1 shows the NeuroGuide topographic map summary page for the z score FFT analysis. qEEG findings showed significantly elevated high beta, localized primarily between Fp1 and F3. Posterior hypocoherence and excessive phase lag were seen in the delta range, with significant anterior hypocoherence seen in the high-beta range.
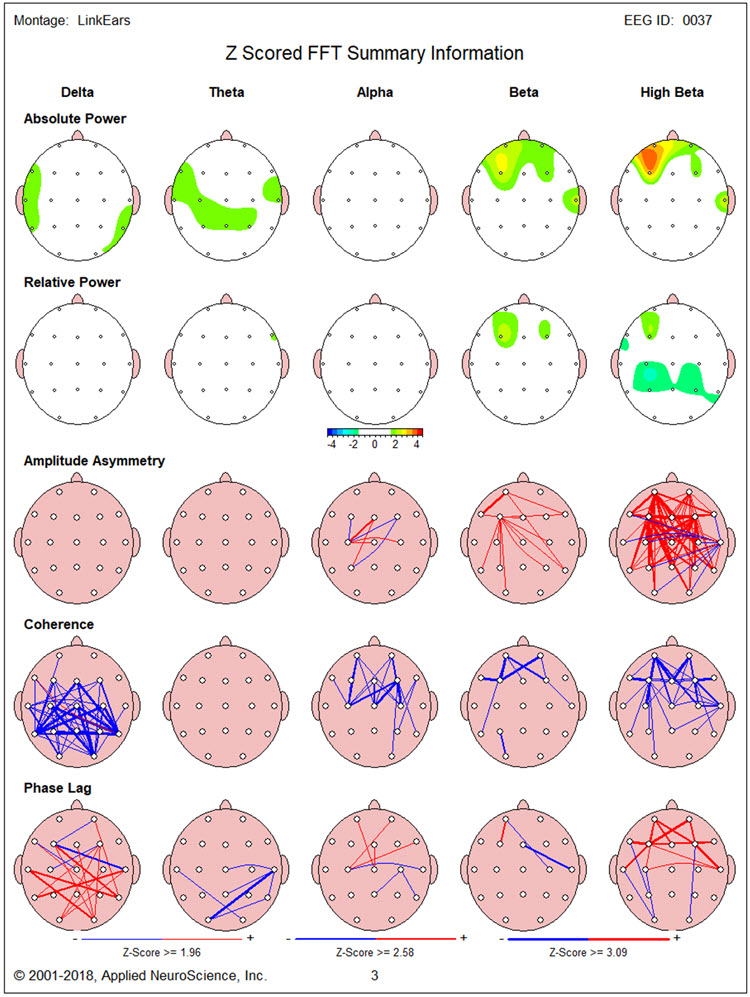
Figures 2 and 3 show single-Hz bins for the z-score FFT analysis to define the exact elevated beta activity range. This appeared to be mainly between 14 and 19 Hz and above 25 Hz. In addition, excess beta, mainly between 15 and 20 Hz, was seen at T4. Excess delta and theta between 3 and 4 Hz were also found in the region of F7.
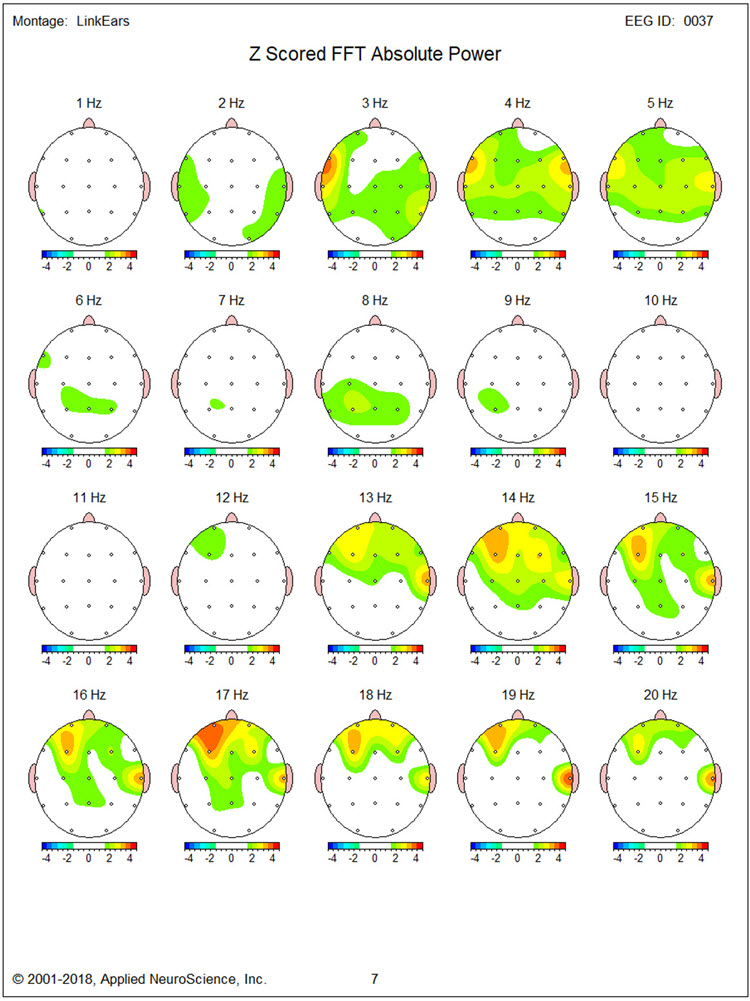
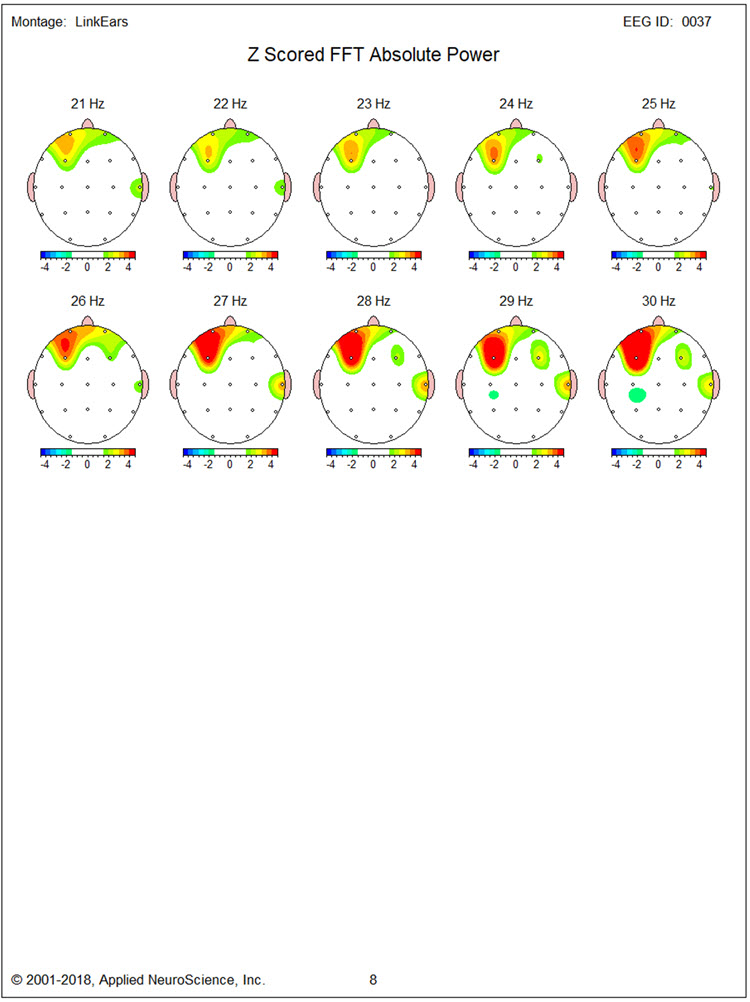
Figures 4 through 8 show LORETA analyses using the NeuroGuide normative database for 3 Hz, 17 Hz, 19 Hz, 27 Hz, and 30 Hz, respectively. Figure 4 for 3 Hz does not show regions of elevated activity to correspond with the single-Hz topographic map.
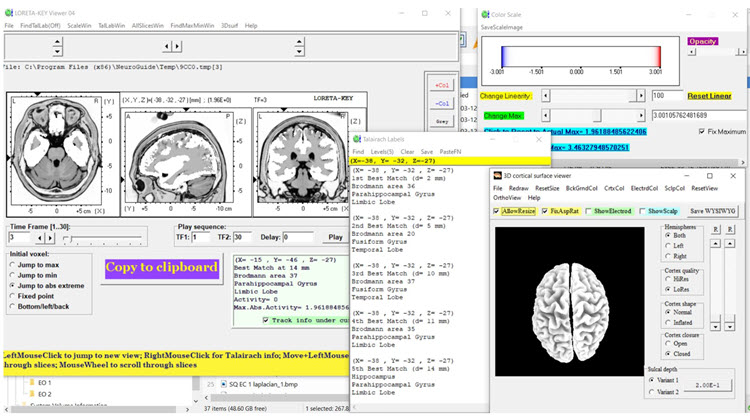
Figures 5 and 6 for 17 Hz and 19 Hz show maximal localization of the source of excess beta in that range to medial frontotemporal structures (i.e., subcallosal gyrus, parahippocampal gyrus, inferior frontal gyrus).
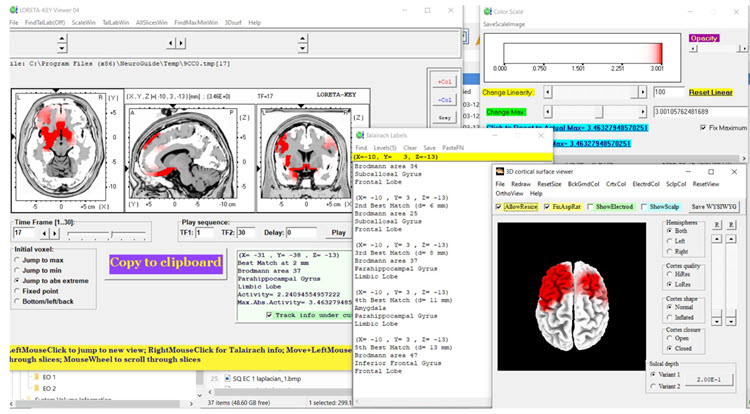
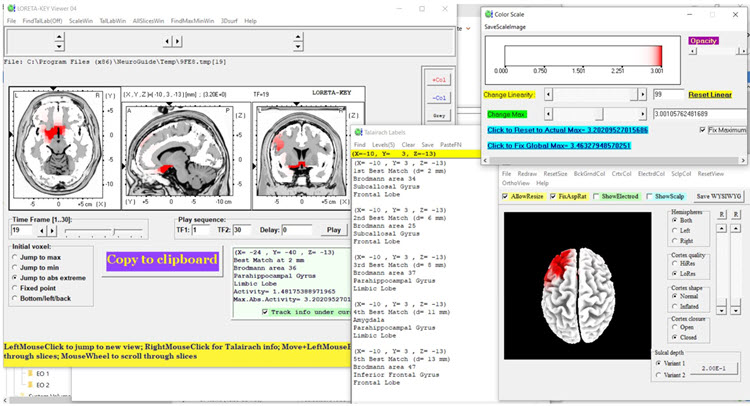
Figures 7 and 8 show maximal localization of 27 and 30 Hz excess beta to the same structures that carried the excess beta at 17 Hz and 19 Hz.
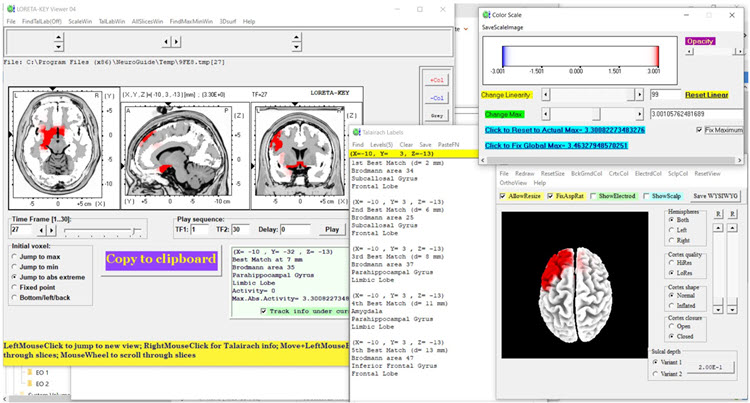
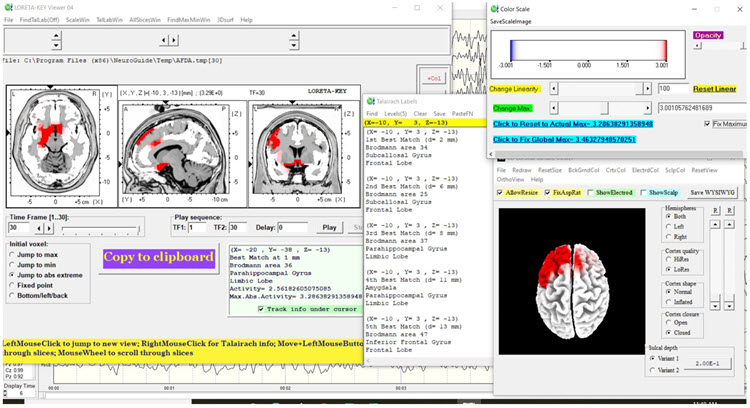
Baseline Eyes-Open EEG Traces: Findings were similar to those for the eyes-closed condition with good blocking of alpha activity. Segments of traces from each of the four montages are shown below.

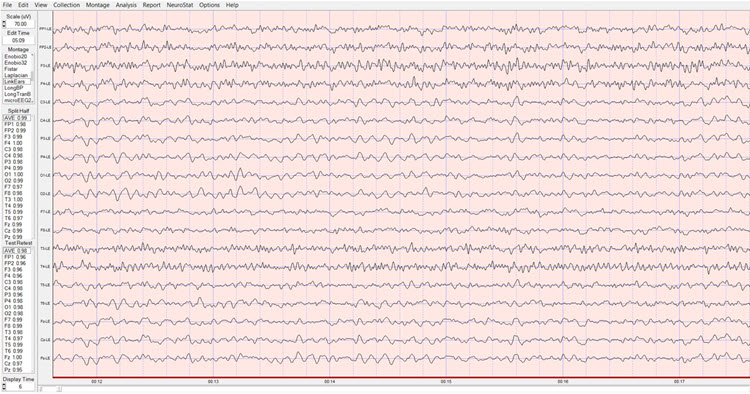
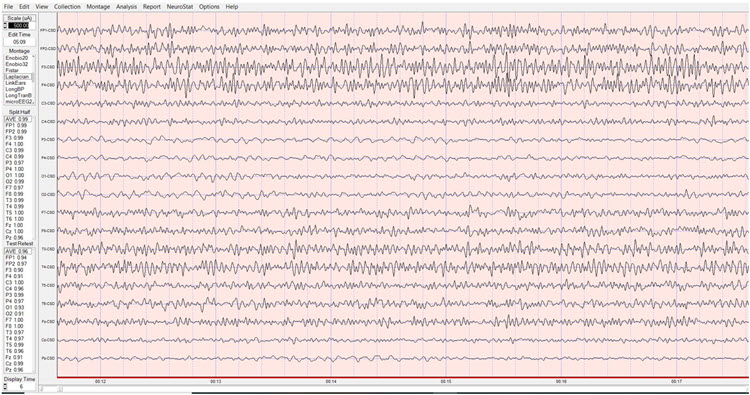
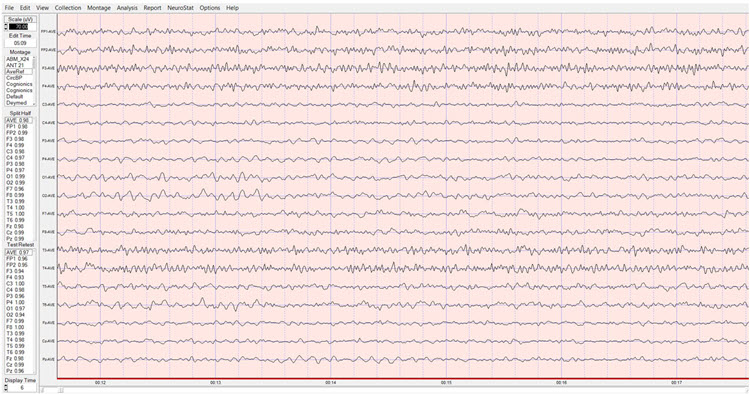
Baseline Eyes-Open qEEG Findings: Figure 9 shows the NeuroGuide summary page with similar findings to that seen in the eyes-closed condition. However, the excess beta activity appears lateralized more to the right hemisphere.
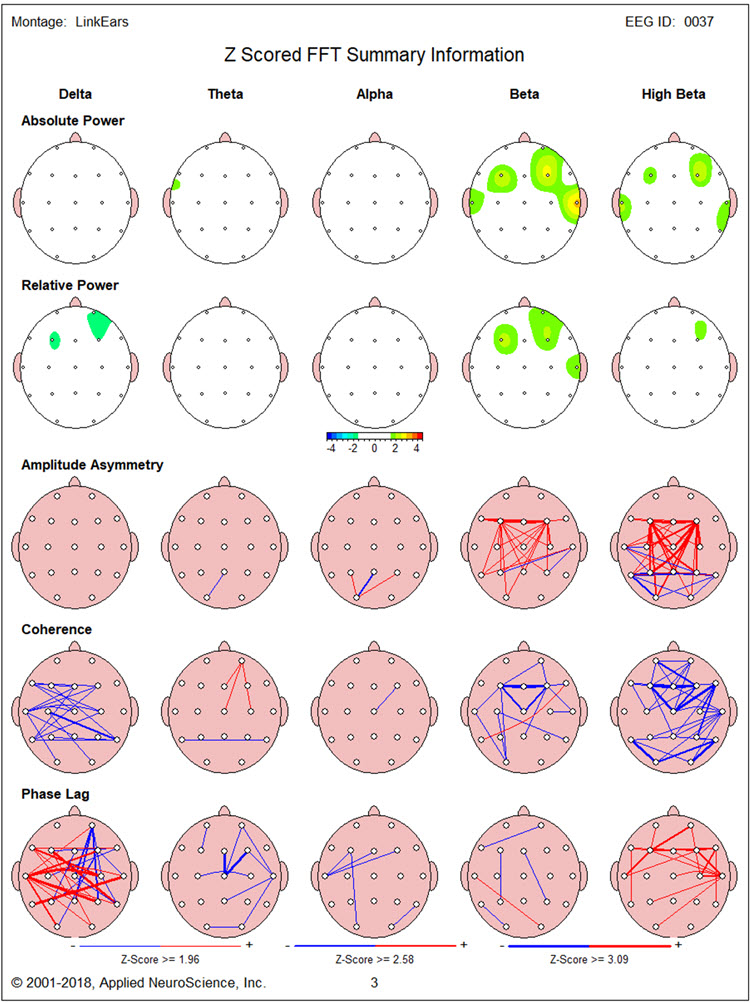
Figure 10, again, shows elevated 3 Hz activity in the region of F7. Figures 10 and 11 show prominent excess 14 Hz activity at F3, with excess 16-22 Hz activity at T4. In addition, particularly high elevations are seen of 24-30 Hz at F3 and 19-29 Hz at F4.
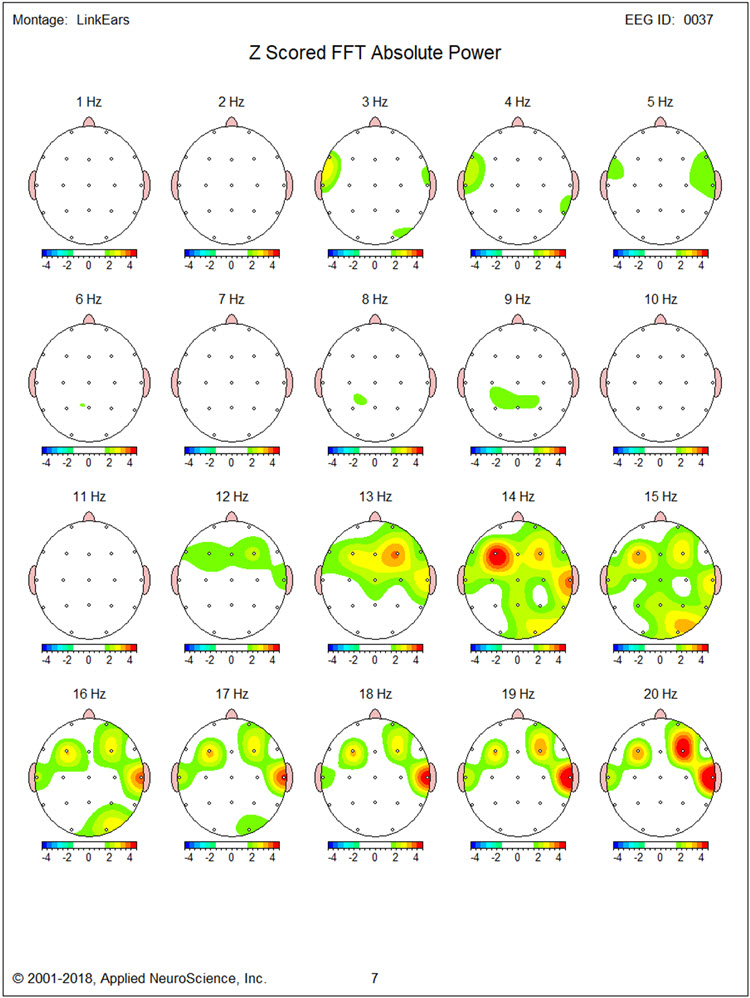
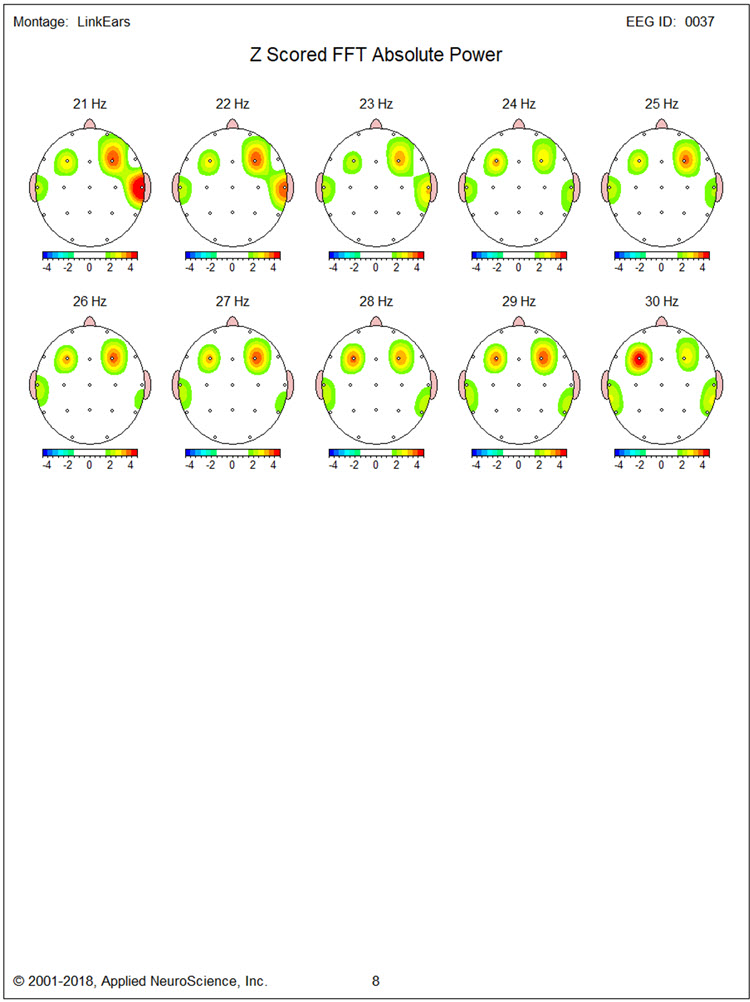
Figures 12, 13, and 14 show LORETA analyses using the NeuroGuide normative database for 14 Hz, 20 Hz, and 30 Hz, respectively. Inferiorly located structures are less involved than in the eyes-closed condition. Medial and superior frontal regions bilaterally show significantly elevated beta activity at 14 Hz and 20 Hz, though much less so at 30 Hz.
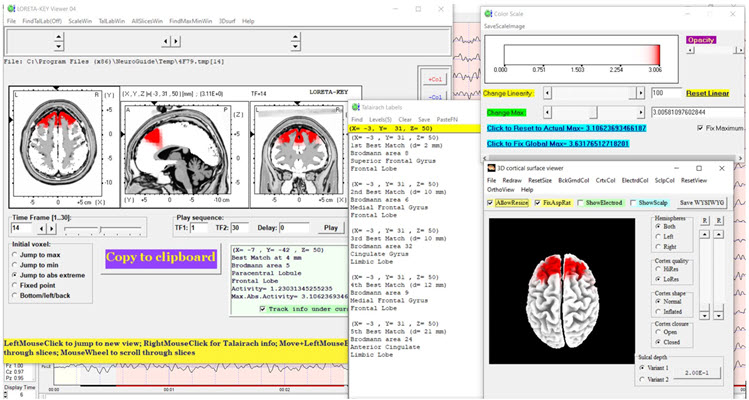
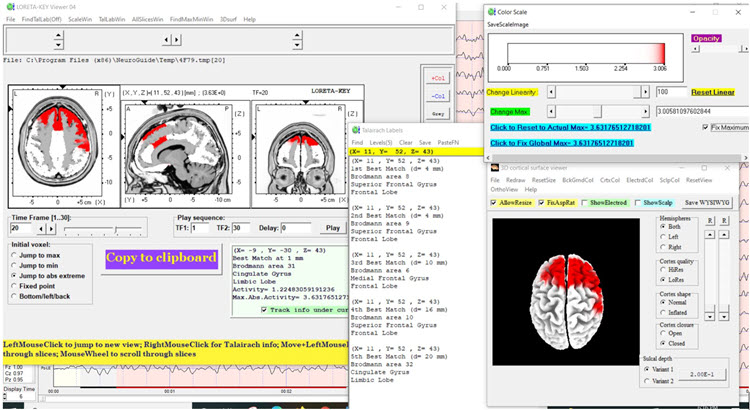
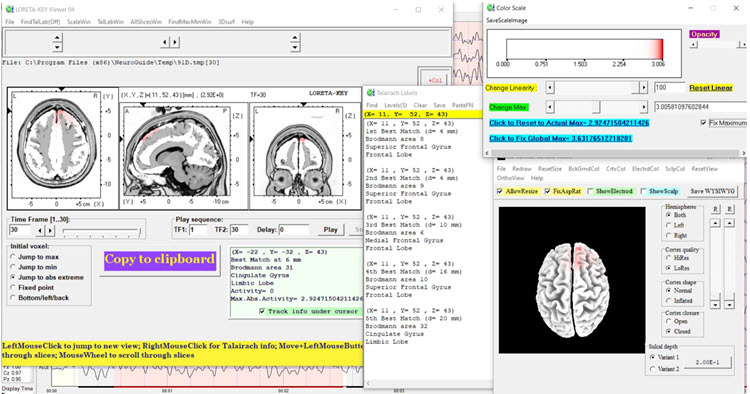
Neurofeedback Training: Neurofeedback was conducted in two stages. First, 13 sessions of 2-channel beta (20-38 Hz) downtraining at F3 and F4 were carried out with eyes open. Note that this inhibit band covers the 24-30 Hz frontal excess seen in the eyes-open baseline but sits above the 14-19 Hz excess, so it did not target the whole of the range the qEEG identified. Second, 6 sessions of alpha-theta training were provided.
Concurrent psychotherapy based on cognitive-behavioral and Acceptance and Commitment Therapy (ACT) methods included education about anger and aggression, acquisition and rehearsal of cognitive and behavioral skills during sessions, and application of those skills between sessions. Although no peripheral biofeedback was provided, TR was taught progressive muscle relaxation and slow diaphragmatic breathing skills.
Anecdotal Outcome: TR and his wife both reported significantly reduced anger expression at home and in the community. TR experienced less intense and briefer episodes of anger and expressed aggressive behavior less frequently at construction sites. During sessions, he appeared visibly less tense and voiced fewer angry complaints. Although TR remained angry at his insurer, the degree of his distress was reduced and he appeared more willing to allow his paralegal to take helpful actions on his behalf.
Post-Neurofeedback qEEG Assessment
Post-Training Eyes-Closed qEEG Findings: Figure 15 shows the post-training eyes closed z score FFT NeuroGuide summary report. Compared to the baseline eyes closed qEEG, excess high beta is reduced at F3. However, significant delta and high beta hypocoherence remain, as does delta phase lag.
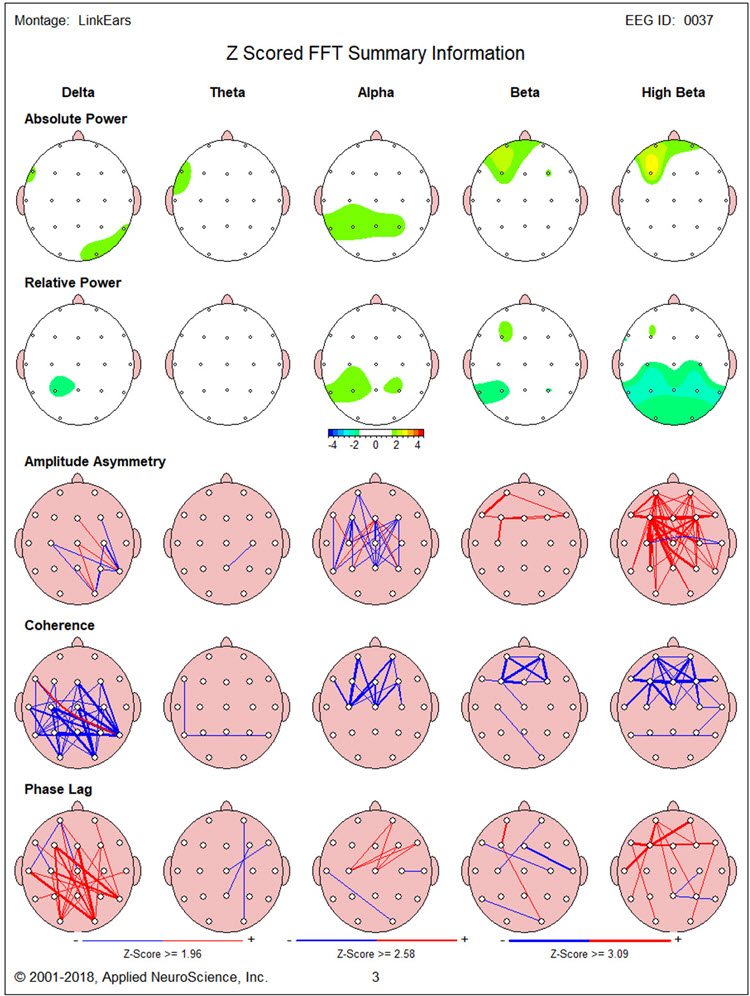
Figures 16 and 17 show single-Hz bins, showing a reduction in the excess beta and high-beta activity seen in the baseline qEEG, with reduction occurring mainly in the beta range (14-19 Hz) and less so at higher frequencies.
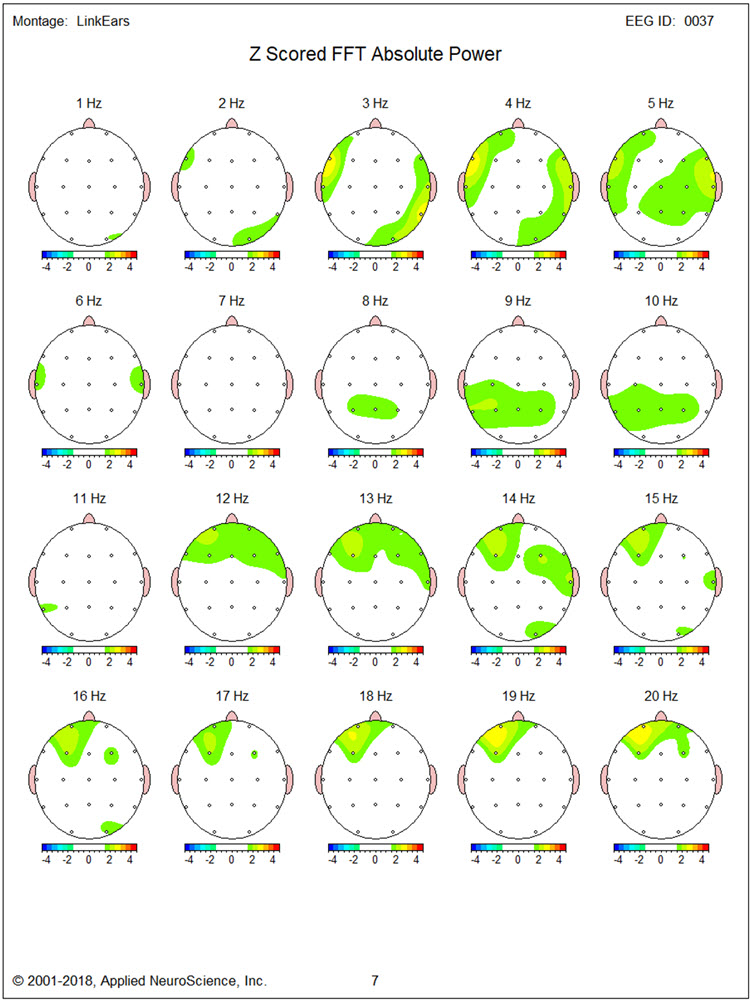
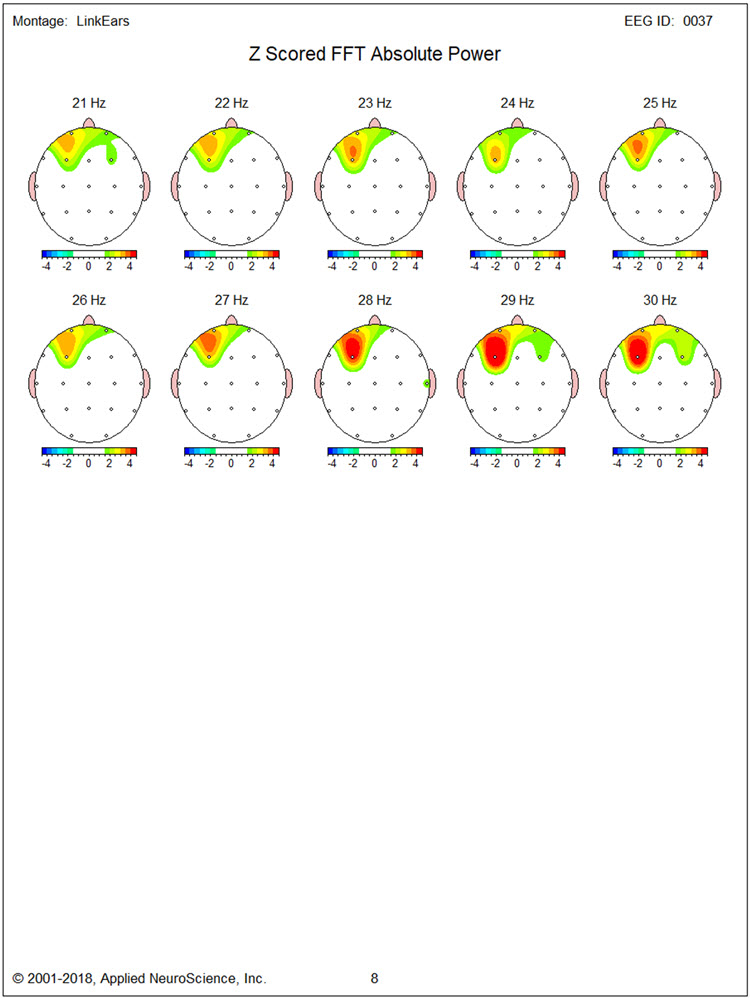
LORETA findings again show no elevated 3 Hz activity in Figure 18. Figures 19 and 20 for 17 Hz and 19 Hz, respectively, show a reduction of cortical territory with excess activity. However, Figures 21 and 22 show little discernable change for 27 Hz and 30 Hz activity.
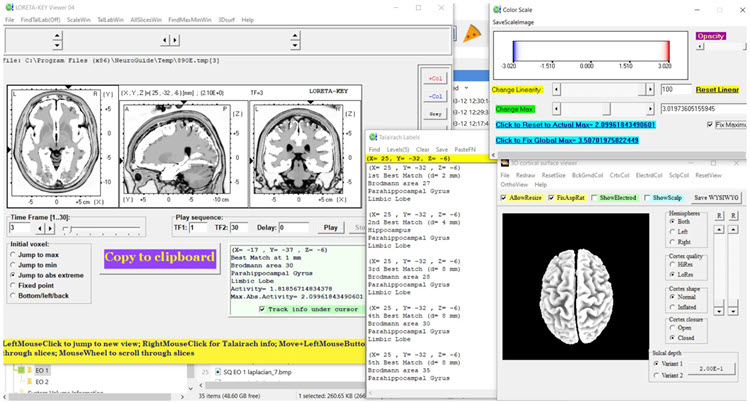
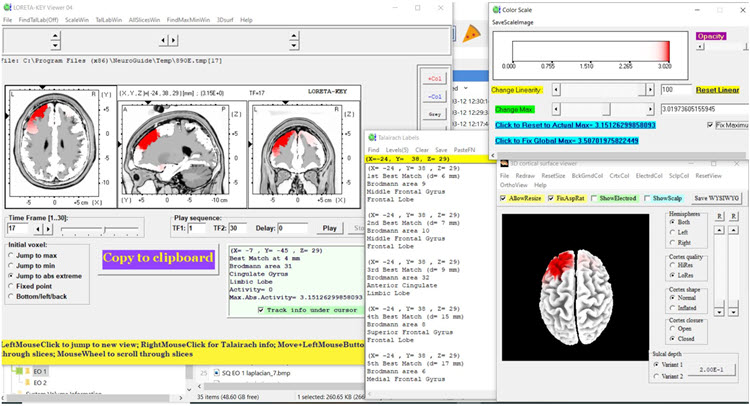
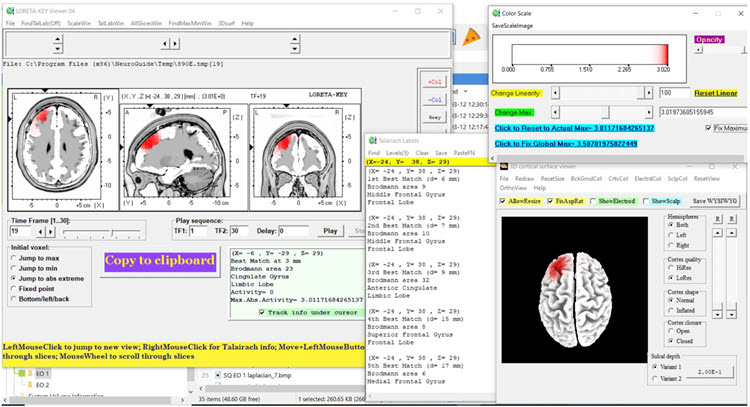
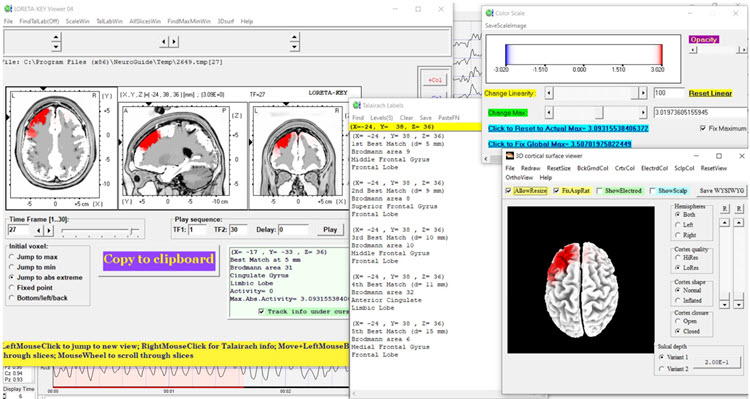
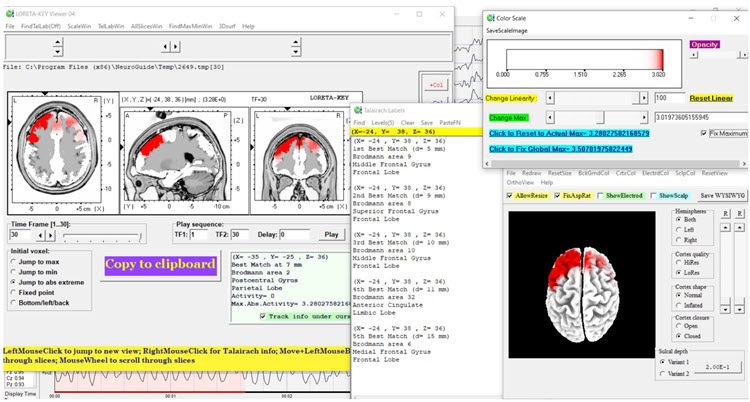
Post-training Eyes-Open qEEG Findings: Figure 23 shows the post-training eyes open z score FFT NeuroGuide summary report. The excess beta and high beta activity seen during the baseline qEEG assessment is largely absent. There is also less delta and high beta hypocoherence than baseline, although delta phase lag remains significantly elevated.
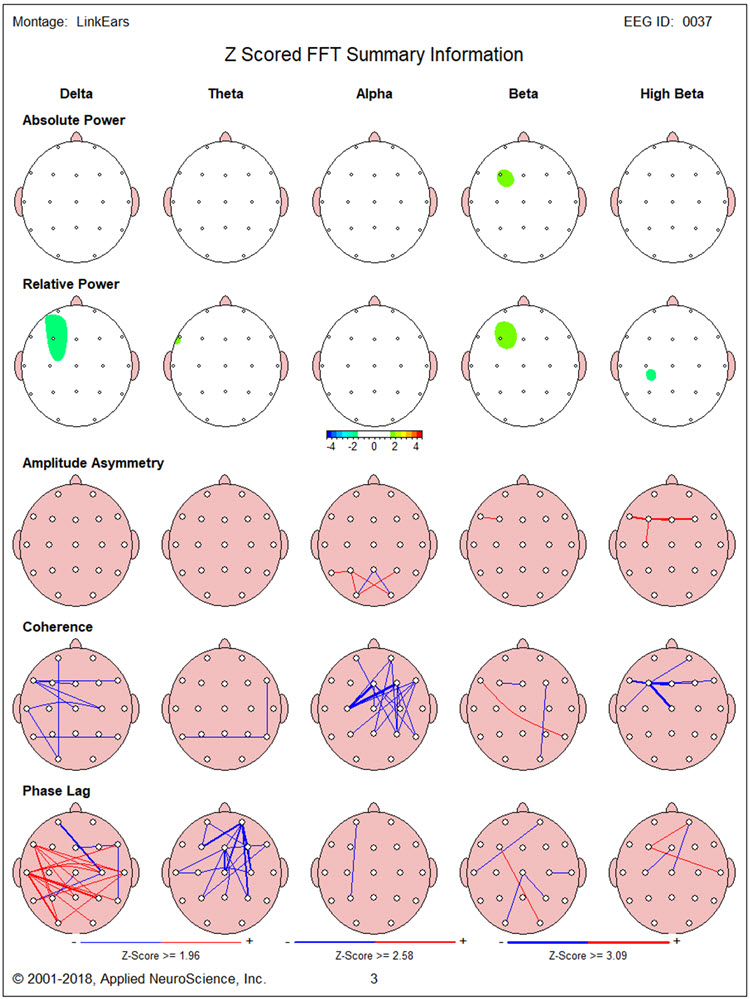
This change is seen in more detail for single-Hz bins in Figures 24 and 25.
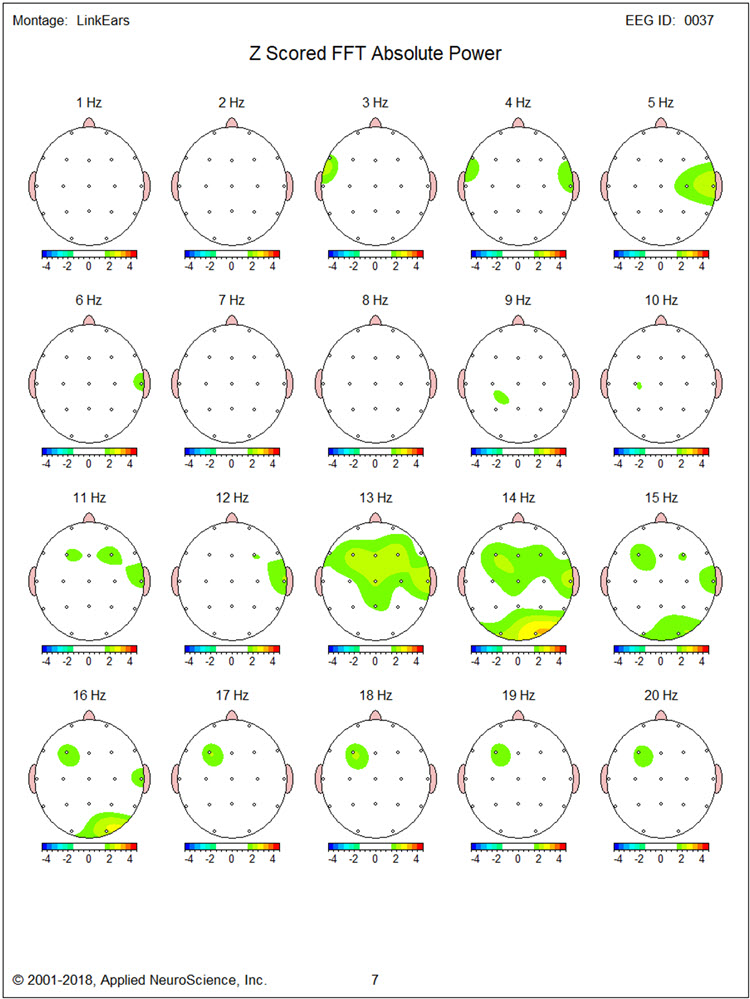
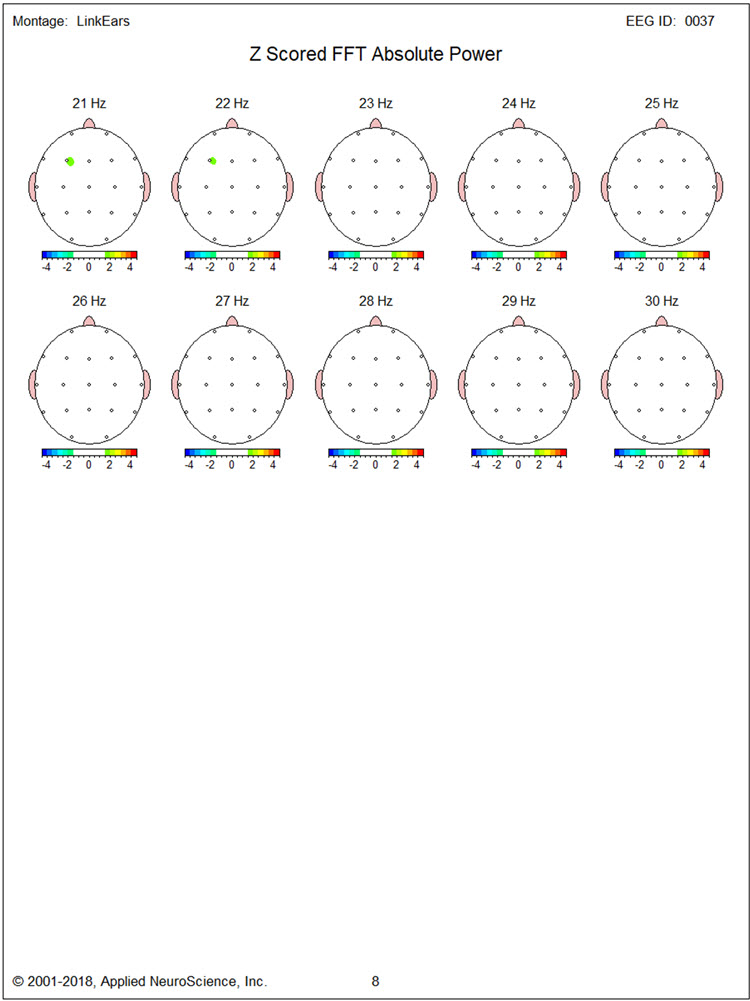
LORETA images in Figures 26, 27, and 28 show very little of the excess activity found during baseline at 14, 20, and 30 Hz.
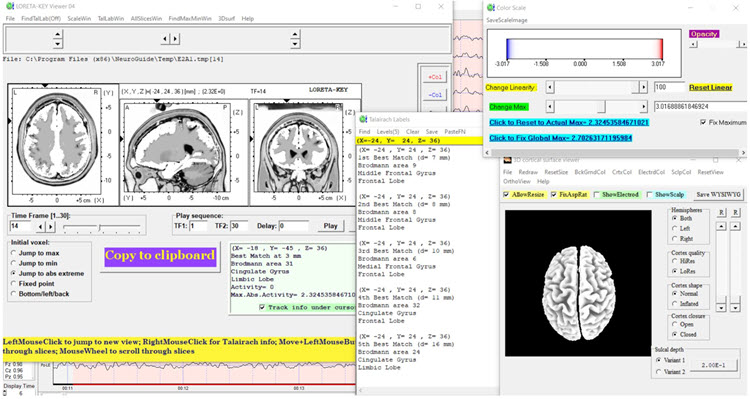
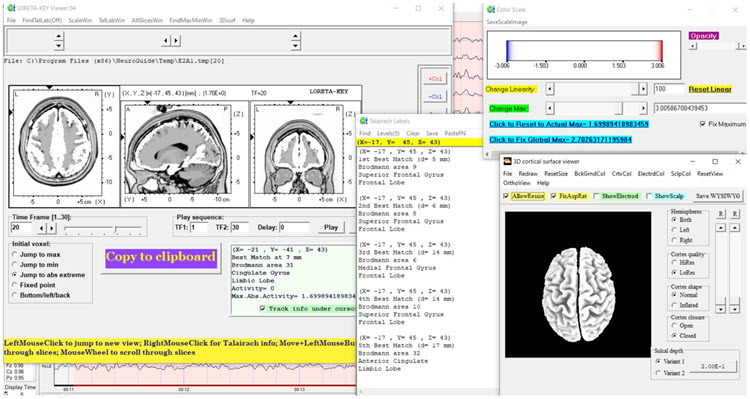
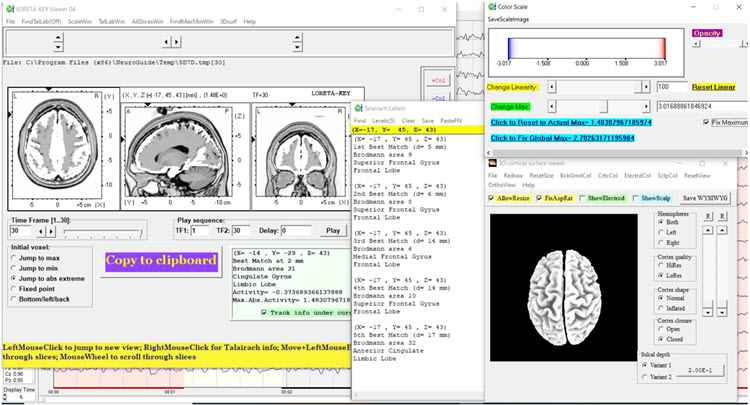
Summary: TR is a 41-year-old man who sustained a mild concussion in a traffic collision two years before neurofeedback training. He was referred primarily for excessive anger and aggressive behavior. Baseline qEEG showed predominantly bilateral frontal excess beta and high beta activity, with LORETA source localization pointing to medial and inferior frontal regions.
Neurofeedback consisted of eyes-open 2-channel beta downtraining at F3 and F4, followed by alpha-theta training. Anecdotal reports from TR, his wife, and behavioral observations by the trainer suggested a significant reduction in both the experience and expression of anger.
Post-training qEEG findings showed reduced beta activity in the eyes-closed condition. In the eyes-open condition, where most of the neurofeedback took place, excess beta was significantly reduced along with delta and high beta hypocoherence. Dynamic FFT z-score analysis of eyes-closed data showed that alpha peak frequency improved from approximately 9 Hz at baseline to about 10 Hz post-training, as seen in the figures below.
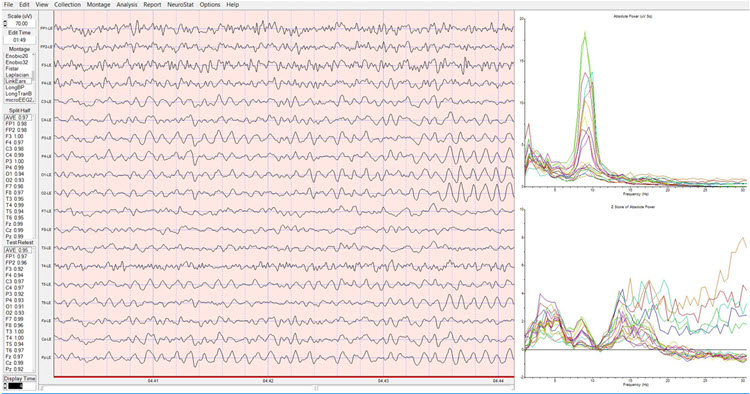
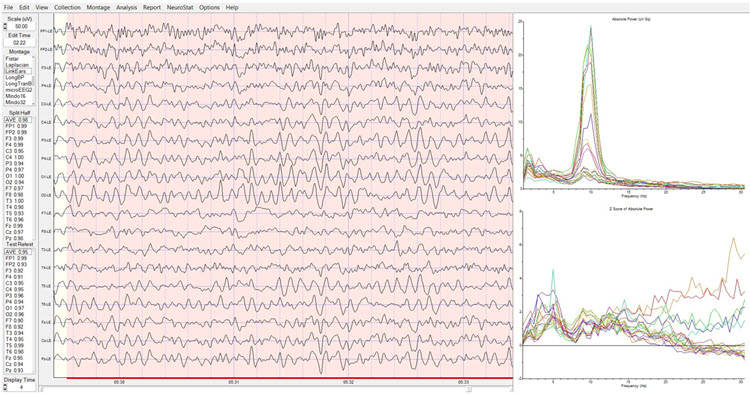
In sum, neurofeedback was associated with significant qEEG changes alongside meaningful clinical improvements in TR's emotional condition and behavior, a strong illustration of how targeted protocol selection based on assessment findings can produce measurable outcomes.
Patient Example D
This final case illustrates the assessment-to-training process for a client presenting with stress and anxiety rather than TBI. It demonstrates how the biopsychosocial framework applies to a high-functioning professional whose symptoms respond to combined biofeedback, neurofeedback, and cognitive-behavioral interventions.
Jill is a 30-year-old married lawyer who made an initial appointment with Sharon, a psychotherapist who provides neurofeedback and biofeedback, following her family physician's recommendation to seek help with stress management. Before the appointment, Sharon sent clinic information, a background questionnaire, and a standardized questionnaire for Jill to complete and bring to the first session.
At the first appointment, Sharon collected the questionnaires, documented her review of confidentiality issues with Jill, and conducted an intake interview. She also requested consent to obtain relevant reports from Jill's family physician. Sharon provided Jill with a stress model, explained why she was suffering from stress, and described treatment options, including neurofeedback and biofeedback as adjuncts to psychotherapy. Jill expressed interest, so Sharon recommended a further appointment for an EEG assessment and a psychophysiological stress assessment. After these assessments, Sharon scored the questionnaires, spoke by phone with Jill's husband and family physician, and examined all the collected data alongside the intake interview information.
Assessment Highlights
Jill is a 30-year-old married lawyer with no children who self-referred for stress management. She wants to understand what is causing her stress and what her options are for managing it.
Presenting Problem from the Interview: Stress occurs daily and varies from none to severe intensity, with intense episodes about 3 times per week lasting several hours on average. Precipitants include receiving large work assignments and encountering obstacles such as difficulty accessing information. Low-intensity stress occurs primarily at home during meals with her husband and during outdoor exercise.
During severe stress, Jill has difficulty concentrating and recalling work-related information. Physical correlates include holding her breath and tightening muscles from the shoulders up. She experiences what she believes are tension headaches approximately twice per week.
Presenting Problem History: Jill has always performed well in school, but as she advanced through her education and began working as a lawyer, her experience of stress gradually worsened. During her first year as an associate, she began avoiding some work assignments, which prompted informal criticism from other lawyers at the firm. As stress worsened, she recalled that self-criticism related to academic and professional performance also increased.
Functional Status: Jill works full-time as a lawyer with no significant deficits in self-care, domestic activity, mobility, or daily living. However, engagement in self-care and pleasurable activities is limited, and fatigue has reduced time spent traveling and socializing with her husband and friends.
Medication and Social Drugs: Jill uses over-the-counter remedies such as Tylenol for headaches.
Past History: Physically, Jill has had no major surgeries, illnesses, injuries, or diagnosed diseases, and she received the normal complement of childhood vaccinations plus full COVID-19 vaccination with boosters. She has never received a mental health diagnosis but did see a counselor during high school and law school for high stress levels. She has a couple of drinks with her husband two to three times per week and does not use recreational drugs. Jill completed law school 2 years ago and works in a moderately-sized corporate legal firm. She has no legal history.
Social: Jill married after completing her undergraduate degree. Earlier in their marriage, she and her husband traveled and visited friends more frequently. She maintains a small circle of friends with whom she talks by phone, texts, and occasionally goes out to dinner and shows. She is on good terms with her parents, younger sister, and her husband's family. Jill reports that her parents emphasized academic achievement and excellence in extracurricular activities during her childhood and appeared to personalize occasions when her performance was not the best.
Family History: Jill's parents have no significant concerns in areas of medical, psychiatric, substance use, academic, or work history.
Collateral Report: A phone interview with Jill's husband (conducted with her consent) essentially corroborated her account. He commented that she worries about minor issues and sometimes has difficulty falling asleep. Medical records from Jill's family physician were consistent with both interviews, with no significant test results or reports to note.
Behavioral Observation: During the interview, Jill fidgeted frequently and appeared tense. She expressed misgivings about her abilities and performance several times.
Psychological Assessment: Questionnaire results from the 21-item Depression Anxiety Stress Scales (DASS-21; Lovibond & Lovibond, 1995) showed significant elevation of stress and anxiety, but not of depression.
EEG Assessment: There was excessive posterior beta amplitude and deficient alpha production in an eyes-closed condition.
Psychophysiological Stress Test: Shoulder-neck EMG increased significantly in response to stressors, failing to return to baseline levels. Heart rate variability was deficient. Finger temperature and skin conductance were unremarkable.
Formulation
Jill is a young professional seeking help for high levels of stress that compromise her enjoyment of work and personal life. Her developmental history suggests she learned early to value high performance and feel anxious about less-than-excellent outcomes, developing critical and evaluative beliefs about herself in challenging situations. The demands of the legal profession have intensified these patterns, leading her to consult her family physician and then Sharon.
Jill brings many strengths: her intellect, capacity for strong social relationships, academic and professional success, and supportive family and friends. However, her beliefs about challenging situations and her withdrawal from pleasurable activities may perpetuate her stress cycle. The questionnaire, EEG, and psychophysiological test results are all consistent with stress and anxious mood. Treatment options include medication, cognitive-behavior therapy, neurofeedback, and biofeedback. Jill deferred medication but expressed interest in the latter three methods, all of which Sharon can provide.
Cognitive-behavior therapy for stress management is recommended. Psychophysiological stress test results suggest that a combination of respiration, HRV, and EMG biofeedback will be helpful, and will serve to familiarize Jill with the biofeedback process in advance of neurofeedback training. EEG assessment suggests using a posterior site with a referential montage at Pz or a sequential montage at P3-P4, reinforcing the alpha band while inhibiting higher beta. A review of AAPB's Evidence-Based Practice in Biofeedback and Neurofeedback (Khazan et al., 2023) supports this approach, and published EEG and neurofeedback research reports that elevated posterior beta amplitude and deficient eyes-closed alpha production are consistent with anxiety, and that training alpha amplitude increases while inhibiting excess beta has been associated with reduced anxiety.
This formulation was reviewed with Jill, who consented to the treatment options. Sharon provided several biofeedback sessions plus cognitive-behavior therapy and then introduced neurofeedback training using a referential montage at Pz to reinforce alpha and inhibit beta with eyes closed. Jill practiced cognitive-behavior therapy and HRV biofeedback skills between sessions. Sharon graphed data from the DASS-21, self-report stress ratings, HRV, and neurofeedback training, particularly session pre-training baseline values of average alpha and high beta amplitudes. Sharon also collected stress ratings at the beginning and end of each session, and she and Jill briefly reviewed these graphs together during each visit.
Summary and Conclusion
This unit has presented a systematic, evidence-based framework for neurofeedback protocol development. The model highlights the importance of a data-driven approach: initial protocols are selected based on the best available evidence, and their effectiveness is judged by measurable changes following the implementation of training. Equally important, the close involvement of the client from the outset and throughout training integrates ethical considerations of autonomy and informed consent into every step of the decision-making process.
The framework begins with ruling out functional causes through collaboration with integrative medicine professionals, then proceeds through assessment, protocol selection, training, ongoing monitoring, and reassessment. The four patient examples illustrate how this process unfolds across diverse presentations including traumatic brain injury, depression, ADHD, anger and aggression, and stress. In each case, the intersection of the client's symptoms, EEG findings, and research evidence guided protocol selection, and when initial approaches fell short, the framework provided a principled basis for adapting the training plan.
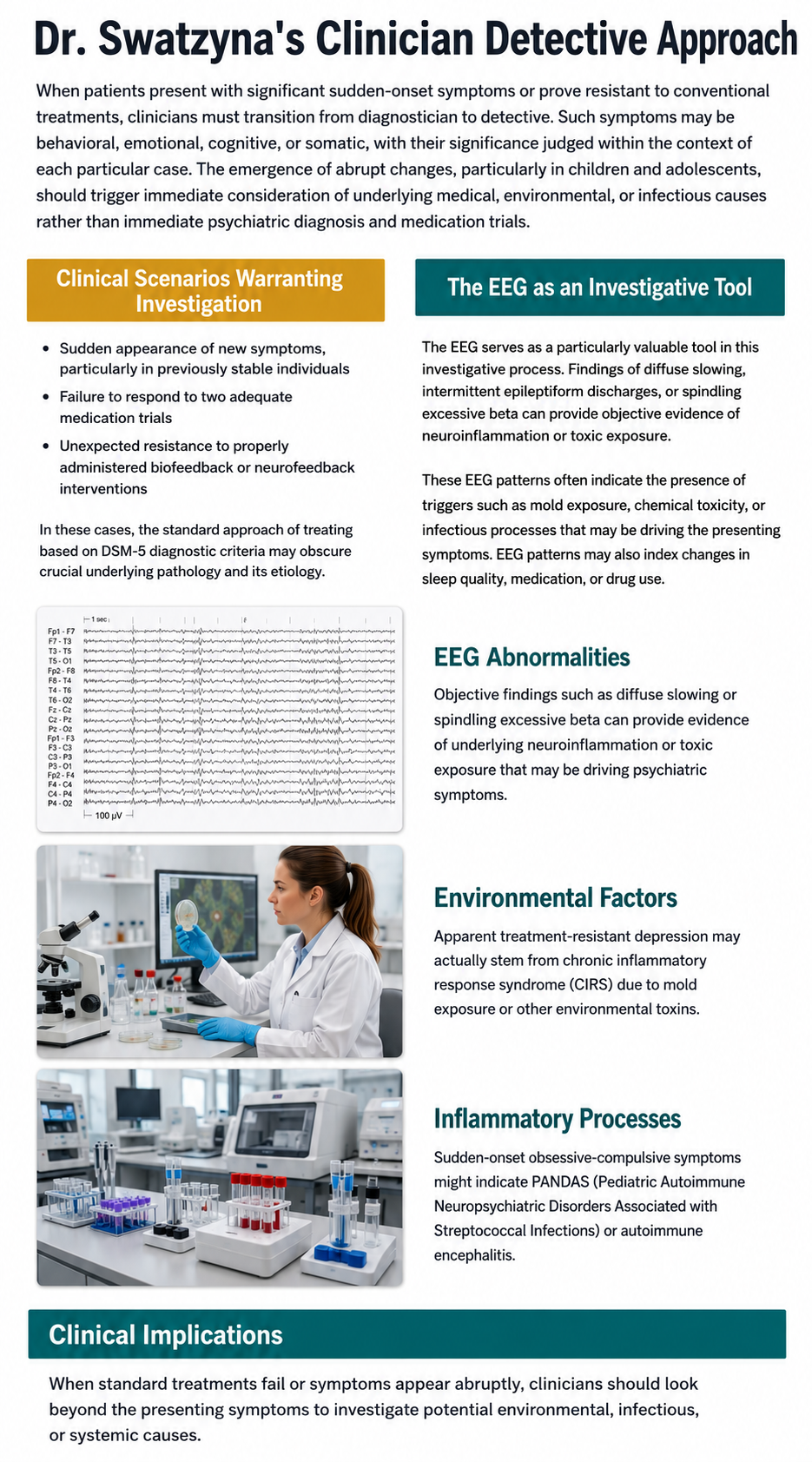
Protocol development follows a systematic, evidence-based approach that integrates six key factors: the client's condition and goals, research findings, practitioner expertise, available resources, environmental context, and client values. The process starts with screening for functional causes through integrative medicine collaboration, then moves through assessment, protocol selection, training, ongoing monitoring, and reassessment. The four patient examples demonstrate how this framework applies across diverse clinical presentations, from TBI and depression to anger, ADHD, and stress, always grounding decisions in the convergence of symptoms, EEG findings, and research evidence.
Functional and Integrative Medicine Collaboration
A growing body of evidence shows that psychiatric and neurological symptoms may stem from functional causes, including environmental toxins, infections, and gut-brain axis dysfunction. This recognition represents a paradigm shift in neurofeedback practice. Swatzyna and colleagues (2024) advocate for routine screening of EEG biomarkers such as focal slowing, spindling excessive beta, encephalopathy, and isolated epileptiform discharges. When these biomarkers appear alongside new or worsening symptoms, clinicians should partner with functional and integrative medicine professionals to identify and address underlying causes before initiating neurofeedback. For practitioners in VA settings, hospitals, and clinics, this means developing referral networks with specialists who can investigate environmental and metabolic contributors to treatment-resistant cases.
Advances in Z-Score Neurofeedback and swLORETA
The continued refinement of swLORETA source localization methods has enhanced the precision of 19-channel z-score neurofeedback training. With a growing literature, though one still short of randomized controlled trials, z-score neurofeedback offers practitioners the ability to target specific Brodmann areas, cortical structures, and brain networks with increasing individualization. These advances are particularly relevant for practitioners working with complex presentations, such as TBI or multi-symptom cases, where network-level dysfunction demands protocols that go beyond single-channel amplitude training.
Check Your Understanding
- What are the key "red flags" that should trigger a referral to a functional or integrative medicine professional before starting neurofeedback?
- Describe the three levels of analysis (biological, psychological, socially significant behavior) used to establish training goals, and give an example of each.
- Explain how the decision-making flowchart guides protocol selection when a research-based protocol proves ineffective for a particular client.
- Why is the collaborative relationship between clinician and client considered essential throughout the neurofeedback training process?
- In Patient Example C (TR), how did the baseline qEEG findings inform the neurofeedback protocol selection, and what changes were observed post-training?
Assignment
Now that you have completed this unit, explain the roles of neuroscience and peer-reviewed outcome studies in developing neurofeedback protocols. In your response, discuss how brain-behavior relationships inform electrode placement, how efficacy research guides initial protocol selection, and what the practitioner should do when a research-supported protocol proves ineffective for a particular client.
Glossary
alpha asymmetry neurofeedback for mood disorders: a protocol that trains depressed clients to relax and warm their hands using diaphragmatic breathing and autogenic phrases and then decrease left frontal alpha with respect to the right frontal alpha.
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with "relaxed wakefulness." Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
alpha spindles: regular bursts of alpha activity.
amplitude: the magnitude of the EEG signal, measured in microvolts (μV). Amplitude is not energy or power; power is amplitude squared and is measured in μV2, which equals picowatts only under the convention of a 1-ohm reference resistance.
autoimmune encephalitis: a condition characterized by brain inflammation caused by the body's immune system mistakenly attacking healthy brain cells. Symptoms can include confusion, seizures, memory loss, psychiatric symptoms, and behavioral changes. Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) are clinically defined syndromes rather than established subtypes of autoimmune encephalitis; PANDAS requires a temporal association with streptococcal infection, and PANS is the broader category with no required trigger. The postinfectious autoimmune mechanism they share with autoimmune encephalitis is hypothesized rather than established, and some clinicians expect the categories to be consolidated as that evidence develops.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in both the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
beta spindles: trains of spindle-like waveforms with frequencies that can be lower than 20 Hz but more often fall between 22 and 25 Hz. They may signal ADHD, especially with tantrums, anxiety, autistic spectrum disorders (ASD), epilepsy, and insomnia.
Broca's area: the area located in the inferior frontal gyrus (BA 44 and 45) of the dominant hemisphere (F7-T3 in the left hemisphere) concerned with speech production, grammar, language comprehension, and sequencing.
Brodmann areas: cytoarchitectural zones of the cerebral cortex distinguished by Nissl staining. Brodmann numbered areas 1-52, but areas 12-16 and 48-51 were defined in non-human species and are absent from the human map, so roughly 43-47 areas are delineated in humans.
chronic inflammatory response syndrome (CIRS): a proposed condition attributed to biotoxin exposure and said to produce chronic inflammation and multi-system symptoms. It is not an established diagnosis; it appears in neither the DSM nor the ICD, and several professional bodies dispute its evidence base. The provider's role is to notice a possible environmental exposure and refer for medical evaluation, not to assign or treat the diagnosis.
connectivity training: a strategy designed to correct deficient or excessive communication between two brain sites measured by indices like coherence and comodulation.
default mode network (DMN): a cortical network of sites located in frontal, temporal, and parietal regions that is most active during introspection and daydreaming and relatively inactive when we pursue external goals.
delta rhythm: 1-4-Hz oscillations generated by thalamocortical neurons during N3 (slow-wave) sleep.
diffuse encephalopathy: a condition characterized by widespread brain dysfunction, often resulting from various causes such as infections, toxins, metabolic imbalances, or systemic diseases. It typically manifests as altered mental status, confusion, lethargy, and other cognitive impairments. Diagnosis usually involves clinical assessment and imaging studies like EEG or MRI, and treatment focuses on addressing the underlying cause to alleviate the symptoms.
dominant frequency: the EEG frequency with the greatest amplitude.
evidence-based assessment: client evaluation using instruments that are reliable, valid, and possess clinical utility.
focal slowing (FS): the presence of slower-than-normal brainwave activity in a specific, localized region of the brain, as detected by EEG. This slowing is typically characterized by an increase in delta (1-4 Hz) or theta (4-7 Hz) wave activity in the affected area, while the rest of the brain exhibits normal or faster frequencies. Focal slowing often indicates underlying structural abnormalities, such as lesions, tumors, or areas of localized brain damage. It can be a marker of localized cerebral dysfunction and may be associated with conditions like strokes, brain injuries, or tumors.
functional medicine: a medical approach that focuses on identifying and addressing the root causes of disease.
gamma rhythms: 28-80 Hz rhythm that includes the 38-42 Hz Sheer rhythm and is associated with learning and problem-solving, meditation, mental acuity, and peak brain function in children and adults.
glyphosate: a common herbicide used to kill weeds, known to have potential health effects.
hertz (Hz): the unit of frequency, equal to one cycle per second.
high alpha (alpha 2): 10-12-Hz alpha associated with open awareness.
high beta (beta 4): 25-38-Hz activity mostly seen in the frontal lobes and associated with hyper-perfusion and increased glucose metabolism. High or fast beta activity may be related to peak performance and cognitive processing and related to specificity and precision in information processing. Excessive high beta is associated with alcoholism, anxiety, OCD, rumination, and worry.
isolated epileptiform discharges (IEDs): brief, abnormal bursts of electrical activity in the brain that appear on an EEG. These discharges are typically characterized by spikes or sharp waves that stand out from the background EEG activity. IEDs are often associated with epilepsy, but they can also occur in individuals without a history of seizures. When present in non-epileptic individuals, IEDs may indicate cortical irritability or a predisposition to seizures, and they can be linked to transient cognitive or behavioral disturbances.
local loops: neighboring cortical macrocolumns that share input generate frequencies above 30 Hz in the high-beta and gamma ranges.
local synchrony: synchrony that occurs when the coordinated firing of cortical neurons produces high-amplitude EEG signals.
low alpha (alpha 1): 8-10-Hz alpha below a client's peak alpha frequency when eyes are closed.
low resolution electromagnetic tomography (LORETA): Pascual-Marqui and colleagues' (1994) mathematical inverse solution to identify the cortical sources of quantitative EEG data acquired from 19 or more scalp electrodes.
microbiome: the collection of microorganisms living in and on the human body, particularly in the gut.
module: a set of interconnected nodes in a neural network.
MTHFR gene: a gene that encodes the enzyme methylenetetrahydrofolate reductase, which is crucial for processing amino acids, particularly homocysteine, into methionine, impacting methylation and folate metabolism.
negative SCPs: slow cortical potentials attributed chiefly to synchronous depolarization of pyramidal apical dendrites, with a possible glial contribution, that increase the probability of neuron firing.
neural network: a system of interconnected ensembles of neurons that collaborate to achieve a goal. These networks communicate and perform functions via hub- or node-based communication systems.
node: vertex within a neural network.
normative database: means and standard deviations for EEG variables such as amplitude, power, coherence, and phase that are calculated for single hertz bins, frequency bands, or band ratios based on the EEG data collected from healthy normal subjects who are grouped by age, eyes-open or eyes-closed conditions, and sometimes gender and task, which also allows for the specification of z-scores with a mean of 0 and standard deviation of 1 for the various combinations of EEG variables, frequency ranges, subject ages, eyes open or eyes closed conditions, and other variables.
positive SCPs: slow cortical potentials attributed chiefly to reduced depolarization of pyramidal apical dendrites, with a possible glial contribution, that decrease the probability of neuron firing.
quantitative EEG (qEEG): the digitized statistical analysis of EEG amplitude, power, and connectivity within specific frequency bins. Topographic brain mapping typically uses 19 or more channels, but abbreviated and single-channel applications exist, the theta/beta ratio at Cz being the validated example.
sensorimotor rhythm (SMR): 12-15 Hz spindle-shaped sensorimotor rhythm detected from the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
slow cortical potential (SCP) training: neurofeedback that teaches clients to produce voluntary shifts in the membrane potentials of cortical dendrites that last from 300 milliseconds to several seconds. Because cortical negativity increases and cortical positivity decreases the probability of neuron firing, protocols for conditions such as drug-resistant epilepsy and migraine train both directions, using the ability to generate positivity to reduce cortical excitability. (Generalized tonic-clonic seizures were formerly called grand mal.)
slow cortical potentials (SCPs): gradual changes in the membrane potentials of cortical dendrites that last from 300 ms to several seconds. These potentials include the contingent negative variation (CNV), readiness potential, movement-related potentials (MRPs), and P300 and N400 potentials. SCPs modulate the firing rate of cortical pyramidal neurons by exciting or inhibiting their apical dendrites. They group the classical EEG rhythms using these synchronizing mechanisms.
spindling excessive beta (SEB): a specific pattern observed in electroencephalography (EEG) characterized by bursts of beta wave activity that appear as spindles. In the case of SEB, this beta activity becomes excessive and is often synchronous, occurring at specific frequencies within the beta range. SEB is considered abnormal and is often linked to conditions involving hyperarousal or cortical irritability. It has been observed in various psychiatric and neurological disorders, including anxiety disorders.
swLORETA: a version of sLORETA that adds a singular-value-decomposition-based weighting of the lead field to improve source localization under noisy conditions and for deep sources (Palmero-Soler et al., 2007).
theta/beta ratio (T/B ratio): the ratio between 4-7 Hz theta and 13-21 Hz beta, measured most typically along the midline at the vertex, 10-20 system location Cz (Monastra et al., 1999, 2001).
theta/beta training: a protocol that decreases theta amplitude and increases beta amplitude.
Wernicke's area: the area of the temporoparietal cortex (BA 22) of the dominant hemisphere specialized for speech comprehension. Damage can result in an inability to understand the meaning of speech and construct intelligible sentences.
z-score training: a strategy that attempts to normalize brain function with respect to mean values in a normative database. EEG amplitudes that are 2 or more standard deviations above or below the database means are down-trained or uptrained to treat symptoms and improve performance.
References
Amzica, F., & Lopes da Silva, F. H. (2018). Cellular substrates of brain rhythms. In D. L. Schomer & F. H. Lopes da Silva (Eds.), Niedermeyer's electroencephalography: Basic principles, clinical applications, and related fields (7th ed.). Oxford University Press.
Arnold, L. E., Arns, M., Barterian, J., Bergman, R., Black, S., Conners, C. K., Connor, S., Dasgupta, S., deBeus, R., Higgins, T., Hirshberg, L., Hollway, J. A., Kerson, C., Lightstone, H., Lofthouse, N., Lubar, J., McBurnett, K., Monastra, V., Buchan-Page, K., . . . Williams, C. E. (2021). Double-blind placebo-controlled randomized clinical trial of neurofeedback for attention-deficit/hyperactivity disorder with 13-month follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 60(7), 841-855. https://doi.org/10.1016/j.jaac.2020.07.906
Breedlove, S. M., & Watson, N. V. (2020). Behavioral neuroscience (9th ed.). Sinauer Associates, Inc.
Collura, T. F. (2014). Technical foundations of neurofeedback. Taylor & Francis.
Demos, J. N. (2019). Getting started with neurofeedback (2nd ed.). W. W. Norton & Company.
Gollan, J. K., Hoxha, D., Chihade, D., Pflieger, M. E., Rosebrock, L., & Cacioppo, J. (2014). Frontal alpha EEG asymmetry before and after behavioral activation treatment for depression. Biological Psychology, 99, 198-208. https://doi.org/10.1016/j.biopsycho.2014.03.003
Herbet, G., & Duffau, H. (2020). Revisiting the functional anatomy of the human brain: Toward a meta-networking theory of cerebral functions. Physiological Reviews, 100, 1181-1228. https://doi.org/10.1152/physrev.00033.2019
Kaiser, D. A. (2008). Functional connectivity and aging: Comodulation and coherence differences. Journal of Neurotherapy, 12, 123-139. https://doi.org/10.1080/10874200802398790
Khazan, I., Shaffer, F., Moss, D., Lyle, R., & Rosenthal, S. (Eds.). (2023). Evidence-based practice in biofeedback and neurofeedback (4th ed.). Association for Applied Psychophysiology and Biofeedback.
La Vaque, T. J., Hammond, D. C., Trudeau, D., Monastra, V., Perry, J., Lehrer, P., Matheson, D., & Sherman, R. (2002). Template for developing guidelines for the evaluation of the clinical efficacy of psychophysiological interventions. Applied Psychophysiology and Biofeedback, 27(4), 273-281.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety Stress Scales (2nd ed.). Psychology Foundation of Australia.
Monastra, V. J., Lubar, J. F., & Linden, M. (2001). The development of a quantitative electroencephalographic scanning process for attention deficit-hyperactivity disorder: Reliability and validity studies. Neuropsychology, 15(1), 136-144. https://doi.org/10.1037/0894-4105.15.1.136
Monastra, V. J., Lubar, J. F., Linden, M., VanDeusen, P., Green, G., Wing, W., Phillips, A., & Fenger, T. N. (1999). Assessing attention deficit hyperactivity disorder via quantitative electroencephalography: An initial validation study. Neuropsychology, 13(3), 424-433. https://doi.org/10.1037/0894-4105.13.3.424
Nunez, P. L., & Srinivasan, R. (2006). Electric fields of the brain (2nd ed.). Oxford University Press.
Palmero-Soler, E., Dolan, K., Hadamschek, V., & Tass, P. A. (2007). swLORETA: A novel approach to robust source localization and synchronization tomography. Physics in Medicine and Biology, 52(7), 1783-1800.
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49-65. https://doi.org/10.1016/0167-8760(84)90014-X
Swatzyna, R. J., Morrow, L. M., Collins, D. M., Barr, E. A., Roark, A. J., & Turner, R. P. (2024). Evidentiary significance of routine EEG in refractory cases: A paradigm shift in psychiatry. Clinical EEG and Neuroscience, 15500594231221313. Advance online publication. https://doi.org/10.1177/15500594231221313
Swingle, P. G. (2015). Adding neurofeedback to your practice: Clinician's guide to ClinicalQ, neurofeedback, and braindriving. Springer.
Tan, G., Shaffer, F., Lyle, R., & Teo, I. (Eds.). (2016). Evidence-based practice in biofeedback and neurofeedback (3rd ed.). Association for Applied Psychophysiology and Biofeedback.
Thatcher, R. W. (1998). Normative EEG databases and EEG biofeedback. Journal of Neurotherapy, 2(4), 8-39. https://doi.org/10.1300/J184v02n04_02
Thatcher, R. W., Lubar, J. F., & Koberda, J. L. (2019). Z-Score EEG biofeedback: Past, present, and future. Biofeedback, 47(4), 89-103. https://doi.org/10.5298/1081-5937-47.4.04
Thompson, M., & Thompson, L. (2015). The neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Return to Top