Treatment Demonstration
What You Will Learn in This Chapter
This unit brings together the practical skills you have been developing throughout Neurofeedback Tutor II. You will observe live demonstrations of the International 10-20 System measurement process, 19-channel EEG recording, a clinical assessment (the NewQ), and a complete neurofeedback training session with a fictional client. These demonstrations illustrate the collaborative nature of the client-clinician relationship, the importance of session-to-session tracking, and how to respond when clients experience negative effects.
BCIA Blueprint Coverage: This unit addresses VIII. Treatment Implementation - F. Full Neurofeedback Session Demonstrations.
Introduction
This section covers the foundational role of client education, equipment competence, and EEG literacy in neurofeedback training (NFT). Client education is the starting point for every successful training relationship. During the initial session, professionals explain core concepts, provide a road map of the NFT process, clarify the roles of clinician and client, and summarize clinic policies. This first meeting is also the ideal time to correct misconceptions about how NFT works and what the equipment actually does. Written informed consent then codifies the terms of this relationship in a formal contract.
Applicants must also develop hands-on competence with EEG equipment setup and operation. Didactic training programs give many attendees their first exposure to instrumentation and software through demonstrations and supervised practice. The mentorship phase builds on this foundation, as applicants refine their skills by practicing on themselves, family members, and friends. BCIA's Neurofeedback Essential Skills List provides a detailed checklist of the competencies applicants must master, and it serves as the blueprint for all Demonstration units in this course.
EEG equipment literacy—the ability to operate recording hardware and interpret its output—ties these competencies together. Applicants must learn to measure the scalp, identify International 10-20 System sites, and attach electrodes accurately. They must recognize what a normal raw EEG looks like, gain experience creating and controlling artifacts (false signals that can compromise data validity), and learn to distinguish abnormal waveforms from benign activity. Without these skills, the EEG measurements and brain maps that guide clinical decisions cannot be trusted.

This unit covers the International 10-20 System, 19-channel EEG recording, NewQ Assessment with Live Demonstrations, and a Demonstration of a Full Neurofeedback Session.
Client education forms the cornerstone of effective neurofeedback training. Applicants must master EEG equipment literacy, including scalp measurement, electrode placement, artifact recognition, and the ability to distinguish normal from abnormal EEG waveforms. BCIA's Neurofeedback Essential Skills List provides the competency blueprint for these demonstrations.
International 10-20 System Demonstration
This section presents a live demonstration of the International 10-20 System, the standardized method for placing electrodes on the scalp during EEG recording. The video begins with an overview of the graphic representations of the 19 scalp locations and their coordinate designations, then shows how the skull is measured to pinpoint each site. You will then observe live demonstrations of the basic measuring techniques and a standard sensor application for two separate EEG recording channels.
Video © J. S. Anderson.
The International 10-20 System provides a standardized framework for electrode placement. Understanding how to measure the skull and identify the 19 scalp locations is essential for accurate EEG recording and reproducible results across sessions.
19-Channel EEG Recording
This section demonstrates a 19-channel EEG recording, which captures brain electrical activity from all standard International 10-20 System scalp sites simultaneously. The following video shows a 19-channel BioTrace+/NeXus-32 display in action. This comprehensive recording approach allows clinicians to evaluate whole-brain activity patterns at once, rather than sampling one or two locations. It is also the foundation for quantitative EEG (qEEG) analysis and brain mapping—tools that compare a client's EEG to normative databases to guide treatment planning.
Video © John S. Anderson.
A 19-channel EEG recording captures brain electrical activity from all standard International 10-20 System scalp sites simultaneously. This comprehensive approach enables clinicians to evaluate whole-brain patterns and is the foundation for quantitative EEG (qEEG) analysis and brain mapping.
NewQ Assessment with Live Demonstrations
This section demonstrates a clinical assessment known as the NewQ—one of several structured assessment tools that use EEG recordings during specific tasks to interpret brain activity patterns. Like the ClinicalQ developed by Paul Swingle, PhD (Swingle, 2014), and the New Mind Maps from Richard Soutar, PhD, the NewQ draws on the known relationships between EEG activity and particular cognitive or behavioral tasks. Each tool integrates findings from the standard research literature with the clinical experience of its developer, giving clinicians a structured method for identifying brain-based patterns that may guide treatment.
The video begins with a discussion of how the NewQ is administered, how to identify and minimize artifact during the recording, and the types of tasks the client performs. You will then observe an abbreviated administration of the assessment using a non-client volunteer, followed by a view of the recording screens and data collection process from a saved session. The video concludes with a demonstration of data analysis and a discussion of sample results.
Keep in mind that the NewQ is just one example of these assessment tools. Neurofeedback Tutor also contains videos of 19-channel recordings, normative database comparisons, and discussions of standard training protocols that can follow a clinical assessment. Familiarity with multiple assessment approaches strengthens a clinician's ability to tailor evaluations to different client presentations and clinical settings.
Video © J. S. Anderson.
Clinical assessments like the NewQ, ClinicalQ, and New Mind Maps use EEG recordings during specific tasks to interpret brain activity patterns. These tools draw on standard literature and clinical experience to guide treatment planning. Multiple assessment approaches are available, and clinicians should familiarize themselves with several options.
Full Neurofeedback Training Session Demonstration
Session Description
This section walks you through a fictional but realistic neurofeedback session, covering how clinicians manage negative effects, adjust protocols, and maintain a collaborative relationship with the client. The following video shows a demonstration of session 11 in a training sequence with a fictional client, Sharon, played by Cortney Amundson of Mindful Restoration. The session uses a single EEG channel, training one location (Cz) along the center midline in a referential (monopolar) montage—a setup that places one active electrode on the scalp with an ear reference (Cz-A2). The training protocol rewards increases in 12-15 Hz EEG activity, commonly known as the sensorimotor rhythm (SMR), over the sensory/motor cortex while concurrently inhibiting 4-8 Hz theta and 22-36 Hz high or fast beta. These figures are the session's filter settings rather than band definitions; this course defines theta as 4-7 Hz.
The session opens with the client reporting her responses to the previous session. Sharon describes a negative reaction to a right-side training protocol (P4-T4 uptraining 8-12 Hz) that had produced positive results in other clients. That previous session had also included a short five-minute training segment at Fp1, rewarding an increase in 15-18 Hz beta to address self-reported depression. She reports experiencing a headache after the session and difficulty sleeping, with gradual improvement until finally getting a good night's sleep the night before this session.
This scenario illustrates the kind of negative effects that clients sometimes experience from neurofeedback training. While not a typical occurrence, these reactions arise often enough that practitioners must be prepared to respond appropriately. The first and most important step is to accept that the client is relating an accurate experience. Validating the client's report matters for both the therapeutic relationship and the clinician's ability to evaluate training effects—if clients feel their experience will be dismissed, they may begin filtering their reports to include only positive outcomes, which blinds the clinician to critical information.
In the video, the clinician acknowledges Sharon's report and suggests that one or both training protocols may have contributed to the negative effects, specifically noting the possibility of over-activation from the left frontopolar (Fp1) beta training. This prompts Sharon to share additional information—that she "had more energy" following the training—a detail that helps clarify the nature of the reaction. The clinician then discusses returning to the previous, successful Cz SMR training approach and introduces z-score training (a protocol that reinforces real-time approximations of client EEG values to those in a normative database; Thatcher et al., 2019) as a possible future intervention.
This exchange demonstrates the collaborative and egalitarian nature of the client-clinician relationship that effective neurofeedback requires. Clinicians must always remember that all biofeedback, including EEG biofeedback or neurofeedback, is training, not treatment—a distinction that emphasizes the client's active role in the process. The clinician fosters collaboration to reach the client's goals, which demands bidirectional communication rather than a top-down, practitioner-to-recipient approach. At its best, neurofeedback training involves educating the client about their nervous system while simultaneously educating the nervous system directly through operant conditioning.
Relying on evidence-based training approaches helps minimize negative effects, which means that a thorough understanding of the research and clinical literature is essential. In this example, the possible negative effects of left frontopolar (Fp1) beta training include over-activation of the central nervous system (CNS), potentially resulting in headache, pain, and sleep problems when the client has not yet learned to self-correct the overaroused state. Further training in more rhythmic patterns such as SMR or alpha is widely reported to have a calming effect, and that is what this demonstration session shows; a single session cannot establish how often the effect occurs. Note also that the client felt like taking more deep breaths during the session, leading to a tingling feeling—a possible sign of overbreathing that suggests the value of adding respiration and heart rate variability (HRV) biofeedback training to give the client additional self-regulation resources.
The suggestion to shift to z-score training reflects another evidence-based strategy with a self-corrective mechanism. When training in real time to a normative database (a collection of qEEG metrics from a representative sample), any shift in trained measures away from zero standard deviations (SD) signals movement in an undesired direction. The feedback immediately responds to this change by reducing the reward, encouraging the client to shift back toward typical functioning. This built-in correction may help avoid the kind of adverse reaction Sharon experienced.
This fictional session demonstrates the collaborative nature of neurofeedback training. When clients report negative effects, clinicians must validate the experience and adjust the protocol accordingly. Neurofeedback is training, not treatment, and requires an egalitarian, bidirectional relationship between clinician and client. Evidence-based approaches and thorough knowledge of the literature help minimize adverse reactions.
Feedback Approach
This section examines how different types of feedback—proportional and event-related—are used during the training session, and why the choice of feedback strategy matters for learning outcomes. In this demonstration, the primary feedback is proportional feedback, meaning the audiovisual signals change continuously in direct response to the client's EEG activity. The flower on screen opens more as SMR amplitude increases and closes as it decreases, while the music follows a similar pattern, growing louder with increased SMR and softer as it drops. The high beta inhibit is reflected in the sound of ocean waves in the background, which become louder when high beta amplitude decreases (an inverse setting that rewards reduced high beta without interrupting the training experience).
Research favors this approach: proportional feedback produced better bidirectional heart rate control than binary feedback—a discrete signal that indicates only whether the criterion was met—in a small study of three groups of four participants (Colgan, 1977), and Strehl (2014) draws the same conclusion for slow cortical potential training. Neither source examined SMR training, so the preference is better described as well reasoned than firmly established. Binary or start/stop inhibit approaches can disrupt the training experience, particularly during relaxation-oriented protocols. In this session, the single event-related reward signal is a "bong" sound that occurs each time SMR amplitude exceeds the threshold for at least 250 ms and continues as long as amplitude stays above it. This rewards not only an increase in amplitude but also reinforces the client's ability to sustain longer bursts of 12-15 Hz activity, building a skill that matters for lasting self-regulation.
An additional feedback sound—birds chirping—activates when 4-8 Hz theta amplitude exceeds its threshold, alerting the client to increases that are often associated with drifting attention. Importantly, this signal does not stop or inhibit the other feedback, allowing training to continue uninterrupted. If this were a client with under-arousal and inattention, a different approach would be needed: more structured event-related feedback with start and stop settings, clearly defined goals, and possibly a "points" counter to encourage sustained attention and active participation. However, this fictional individual is overly attentive, anxious, and achievement-oriented, so a more fluid, less goal-directed feedback approach tends to be more effective.
Because this is a demonstration video, it is truncated to show examples of the clinician-client conversations that occur at regular intervals during training. The clinician checks in to determine whether the training is having the desired effect, and other measures—such as peripheral skin temperature and electrodermal activity (EDA), measured as skin conductance and called the galvanic skin response (GSR) in older writing, which reflects sweat gland activity—may be monitored concurrently to alert the clinician to signs of distress like decreased finger temperature or increased palm sweating. With an experienced client who understands the feedback and can independently report symptom changes, it may not be necessary to interrupt training with frequent check-ins, which also promotes client independence and reinforces the self-training nature of the process.
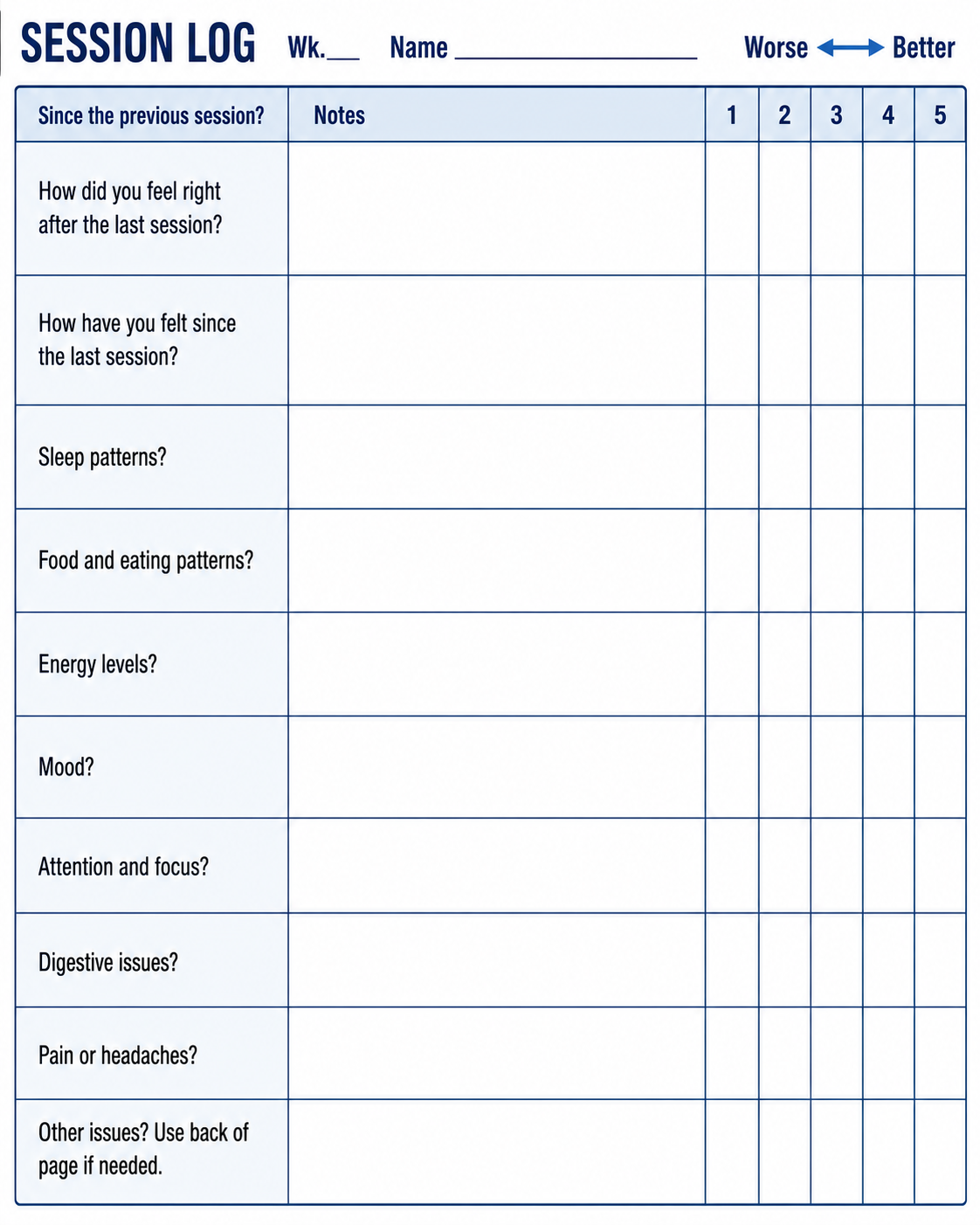
In an actual clinical session, there would likely be more discussion of emotional and psychological material, more client questions about negative effects, and conversations about relationships, energy, mood, and feedback from family, friends, and coworkers. For brevity, these discussions were not included in the video. However, the between-session tracking questionnaire the client completed is shown below. Tracking methods vary widely—some clinics use online forms (which may raise security and privacy considerations), while others prefer simple paper questionnaires. The form below pairs a five-point worse-to-better rating on each item with a notes column, and is intentionally brief to encourage clients to describe their responses in their own words, with the clinician probing for more detail during the session.
Video © J. S. Anderson.
Proportional feedback provides continuous, graded responses to EEG changes, and the available comparisons—small, and drawn from heart rate and slow cortical potential training rather than SMR—favor it over binary (on/off) feedback. Clinicians tailor feedback approaches to each client's presenting concerns: more structured, event-related feedback for inattentive clients and more fluid, less goal-directed feedback for anxious or achievement-oriented clients. Between-session tracking questionnaires help monitor client responses and guide protocol adjustments.
Conclusion
This section reviews the session outcomes, examines the graphed training data, and discusses how threshold settings and individualized approaches shape the training experience. The basic SMR training protocol demonstrated in this session has a long history in neurofeedback, and protocols that reward activity in the sensorimotor band have been examined in several published studies (Arns et al., 2009; Campos da Paz et al., 2018; Gevensleben et al., 2014; Mohammadi et al., 2015; Rajabi et al., 2020). These reports describe improved outcomes on various measures in populations ranging from children to older adults, but their designs differ sharply and none of them compared neurofeedback with medication management. Arns et al. (2009) is a meta-analysis that pools SMR training with theta/beta and slow cortical potential protocols; Gevensleben et al. (2014) reports slow cortical potential training together with a 12-15 Hz training study in children with tic disorder; Mohammadi et al. (2015) is an uncontrolled 16-child trend report whose participants all took methylphenidate; Rajabi et al. (2020) used a waiting-list control and paired neurofeedback with game-based cognitive training; and only Campos da Paz et al. (2018), in healthy older adults, included a sham feedback condition.
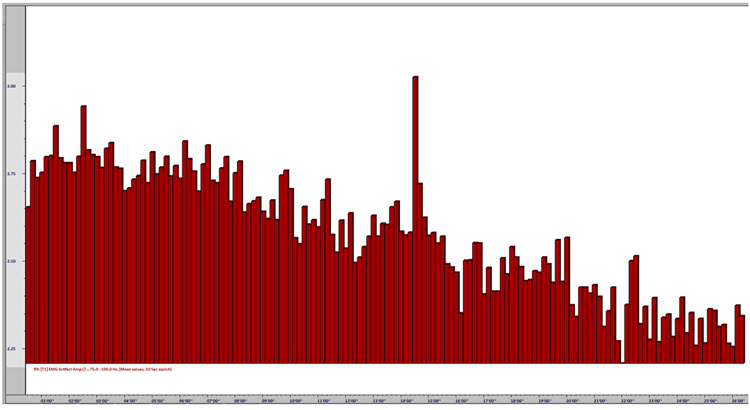
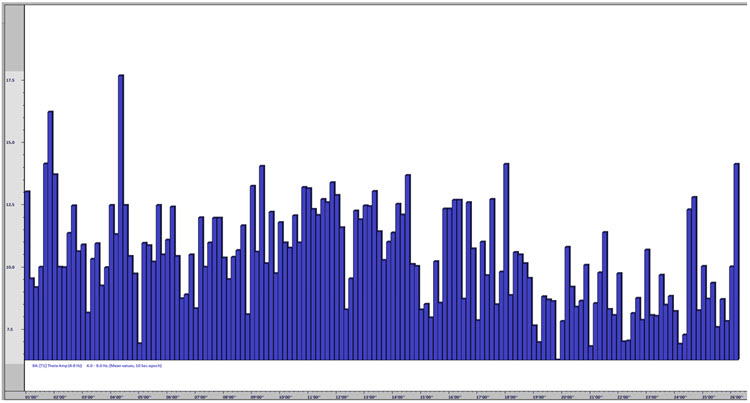
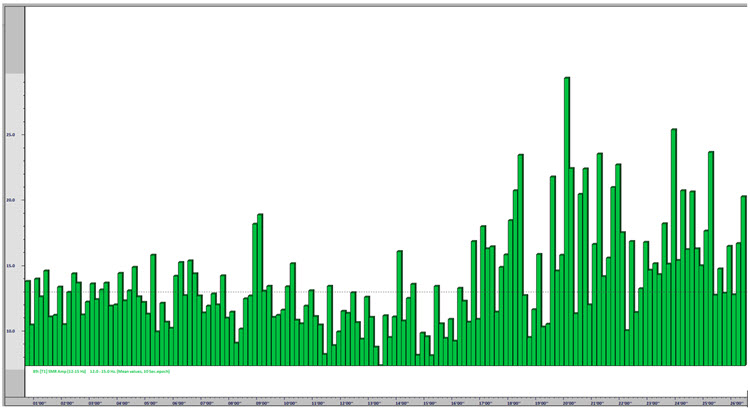
In the demonstration, the client reports "feeling more relaxed"—a subjective self-report that corresponds with the objective session data shown in the graphs below. The results indicate an increase in SMR amplitude toward the end of the session, a decrease in EMG artifact and fast beta activity, and a theta inhibit that holds steady before declining modestly in the final third. Together, these converging measures suggest a genuine shift toward greater physiological relaxation and decreased CNS arousal, not simply an artifact of one measure changing in isolation.
The images below show the results of the training session in graph form with explanations below each image.
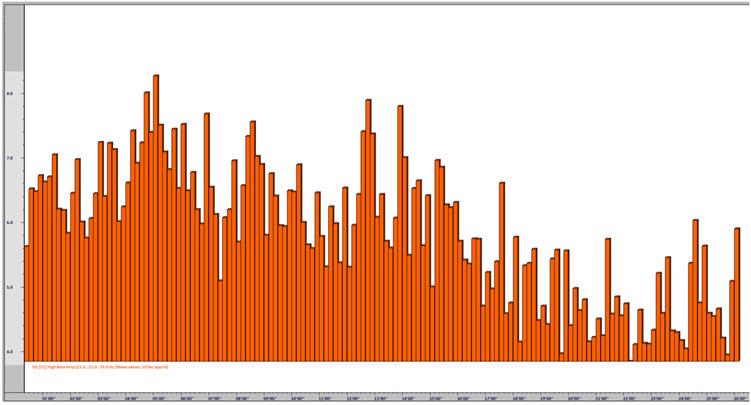
The threshold settings used in this session deserve special attention. If this session had been conducted with auto-threshold settings (which automatically adjust the reward criterion), the client would have received reward at a roughly constant rate—with little or no increase in reward frequency corresponding to her improved values toward the end. Because the threshold for the SMR discrete, event-related reward remained fixed throughout, the client could perceive her own success through the increasing frequency of the "bong" sound as the session progressed. This kind of tangible, self-evident progress can be a powerful reinforcer.
Different client presentations call for different session structures. Clients with inattentive ADHD, for example, may benefit from dividing the session into three-to-five-minute segments with pauses to evaluate progress, discuss strategies, adjust thresholds, or simply give the client a break from sustained attention demands. Clients with migraine might require frequent adjustments to reward and inhibit frequencies, regular pain-level check-ins, and possible shifts in sensor locations. There is no one-size-fits-all approach to neurofeedback training, because each client is unique and requires interventions tailored to their presenting concerns along with possible protocol adjustments based on their reactions. Children and adolescents present additional challenges that call for patience, creativity, and careful attention.
The session results confirmed the client's subjective report of increased relaxation: SMR amplitude increased toward the end of the session, EMG artifact and high beta decreased, and theta remained largely stable. Fixed thresholds allowed the client to perceive her progress through increased reward frequency. Each client requires individualized training approaches, and there is no one-size-fits-all protocol. Children, adolescents, and clients with different presenting concerns all require tailored strategies.
Check Your Understanding
- Why is it important for clinicians to validate a client's report of negative effects during neurofeedback training?
- What is the difference between proportional feedback and binary (on/off) feedback, and what does the research suggest about their relative effectiveness?
- How does the collaborative, egalitarian client-clinician relationship differ from a top-down practitioner-to-recipient approach in neurofeedback training?
- Why might a fixed threshold be preferable to an auto-threshold setting in certain training situations?
- What role does between-session symptom tracking play in guiding neurofeedback protocol adjustments?
Assignment
Now that you have completed this unit, explain the purpose of inhibits in neurofeedback training.
Glossary
A (auricular): International 10-20 system earlobe reference placement.
alpha rhythm: 8-12-Hz activity that depends on the interaction between rhythmic burst firing by a subset of thalamocortical (TC) neurons linked by gap junctions and rhythmic inhibition by widely distributed reticular nucleus neurons. Researchers have correlated the alpha rhythm with relaxed wakefulness. Alpha is the dominant rhythm in adults and is located posteriorly. The alpha rhythm may be divided into alpha 1 (8-10 Hz) and alpha 2 (10-12 Hz).
amplitude: the magnitude of the EEG signal, measured in microvolts (μV). Amplitude is not energy or power; power is amplitude squared and is measured in μV², which equals picowatts only under the convention of a 1-ohm reference resistance.
artifact: false signals like 50/60Hz noise produced by line current.
beta rhythm: 12-38-Hz activity associated with arousal and attention generated by brainstem mesencephalic reticular stimulation that depolarizes neurons in the thalamus and cortex. The beta rhythm can be divided into multiple ranges: beta 1 (12-15 Hz), beta 2 (15-18 Hz), beta 3 (18-25 Hz), and beta 4 (25-38 Hz).
bipolar (sequential) montage: in EEG, a recording method in which each channel displays the difference between two active scalp electrodes, usually linked in chains. It uses a common ground rather than a shared reference electrode. In peripheral biofeedback the same term describes two active sensors plus a reference, so the intended sense should be stated.
C (central): sites in the International 10-20 system located over the sensorimotor strip; through volume conduction they also detect frontal, parietal-occipital, and temporal EEG activity.
channel: EEG amplifier input from three leads (active, reference, and ground electrodes) placed on the head.
delta rhythm: 1-4-Hz oscillations generated by thalamocortical neurons during stage N3 (slow-wave) sleep. Activity below about 1 Hz is treated in this course as the slow cortical potential or infra-low range.
F (frontal): sites in the International 10-20 system that detect frontal lobe EEG activity.
Fp (frontopolar or prefrontal): sites in the International 10-20 system that detect prefrontal cortical EEG activity.
hertz (Hz): a unit of frequency measured in cycles per second.
impedance (Z): the complex opposition to an AC signal measured in Kohms.
impedance meter: a device that uses an AC signal to measure impedance in an electric circuit, such as between active and reference electrodes.
impedance test: automated or manual measurement of skin-electrode impedance.
inhibit training: setting a threshold to decrease unwanted EEG activity (e.g., 4-8 Hz and 22-36 Hz).
inion: a bony prominence on the back of the skull.
International 10-20 system: a standardized procedure for placing 21 recording electrodes—19 scalp sites plus the two earlobe references—and one ground electrode on adults.
mastoid bone: bony prominence behind the ear.
microvolt (μV): a unit of amplitude (signal strength) that is one-millionth of a volt.
montage: a grouping of electrodes (combining derivations) to record EEG activity.
nasion: the depression at the bridge of the nose.
normative database: qEEG metrics obtained from a representative sample of participants during resting and active-task conditions.
notch filter: a filter that suppresses a narrow band of frequencies, such as those produced by line current at 50/60Hz.
O (occipital): sites in the International 10-20 system that detect occipital lobe EEG activity.
ohm (Ω): a unit of impedance or resistance.
P (parietal): sites in the International 10-20 system that detect parietal lobe EEG activity.
posterior dominant rhythm (PDR): the highest-amplitude frequency detected at the posterior scalp when eyes are closed.
power: amplitude squared, expressed in microvolts squared (μV²). Values in picowatts appear in some software only under the convention of a 1-ohm reference resistance, which must be stated whenever picowatts are used.
preauricular point: the slight depression located in front of the ear and above the earlobe.
protocol: a rigorously organized plan for training.
reference electrode: an electrode placed on the scalp, earlobe, or mastoid.
referential (monopolar) montage: the placement of one active electrode (A) on the scalp and a neutral reference (R) and ground (G) on the ear or mastoid.
rhythmic midtemporal theta of drowsiness (RMTD): a benign drowsiness variant, not an epileptiform pattern, consisting of notched or sharply contoured rhythmic theta waveforms localized to the midtemporal regions. It may be seen over either hemisphere, and its asymmetry shifts within and between recordings.
sensorimotor rhythm (SMR): the 12-15 Hz spindle-shaped sensorimotor rhythm, with a spectral peak usually around 12-14 Hz, detected from the sensorimotor strip when individuals reduce attention to sensory input and reduce motor activity.
theta/beta ratio (T/B ratio): the ratio between 4-7 Hz theta and 13-21 Hz beta, measured at the vertex (Cz) in the studies that validated it (Monastra, Lubar, & Linden, 2001).
theta rhythm: 4-7-Hz rhythms generated by a cholinergic septohippocampal system that receives input from the ascending reticular formation and a noncholinergic system that originates in the entorhinal cortex, which corresponds to Brodmann areas 28 and 34 at the caudal region of the temporal lobe.
tragus: the flap at the opening of the ear.
transient: isolated waveforms or complexes that can be distinguished from background activity.
vertex (Cz): the intersection of imaginary lines drawn from the nasion to inion and between the two preauricular points in the International 10-10 and 10-20 systems.
z-score training: a neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Arns, M., de Ridder, S., Strehl, U., Breteler, M., & Coenen, A. (2009). Efficacy of neurofeedback treatment in ADHD: The effects on inattention, impulsivity and hyperactivity: A meta-analysis. Clinical EEG and Neuroscience, 40(3), 180-189. https://doi.org/10.1177/155005940904000311
Campos da Paz, V. K., Garcia, A., Campos da Paz Neto, A., & Tomaz, C. (2018). SMR neurofeedback training facilitates working memory performance in healthy older adults: A behavioral and EEG study. Frontiers in Behavioral Neuroscience, 12, 321. https://doi.org/10.3389/fnbeh.2018.00321
Colgan, M. (1977). Effects of binary and proportional feedback on bidirectional control of heart rate. Psychophysiology, 14(2), 187-191. https://doi.org/10.1111/j.1469-8986.1977.tb03374.x
Gevensleben, H., Kleemeyer, M., Rothenberger, L. G., Studer, P., Flaig-Röhr, A., Moll, G. H., Rothenberger, A., & Heinrich, H. (2014). Neurofeedback in ADHD: Further pieces of the puzzle. Brain Topography, 27(1), 20-32. https://doi.org/10.1007/s10548-013-0285-y
Mohammadi, M. R., Malmir, N., Khaleghi, A., & Aminiorani, M. (2015). Comparison of sensorimotor rhythm (SMR) and beta training on selective attention and symptoms in children with attention deficit/hyperactivity disorder (ADHD): A trend report. Iranian Journal of Psychiatry, 10(3), 165-174. PMCID: PMC4749686
Monastra, V. J., Lubar, J. F., & Linden, M. (2001). The development of a quantitative electroencephalographic scanning process for attention deficit-hyperactivity disorder: Reliability and validity studies. Neuropsychology, 15(1), 136-144. https://doi.org/10.1037/0894-4105.15.1.136
Rajabi, S., Pakize, A., & Moradi, N. (2020). Effect of combined neurofeedback and game-based cognitive training on the treatment of ADHD: A randomized controlled study. Applied Neuropsychology: Child, 9(3), 193-205. https://doi.org/10.1080/21622965.2018.1556101
Soutar, R., & Longo, R. (2022). Doing neurofeedback: An introduction (2nd ed.). ISNR Research Foundation.
Strehl, U. (2014). What learning theories can teach us in designing neurofeedback treatments. Frontiers in Human Neuroscience, 8, 894. https://doi.org/10.3389/fnhum.2014.00894
Swingle, P. G. (2014, Spring). Clinical versus normative databases: Case studies of Clinical Q assessments. NeuroConnections.
Thatcher, R. W. (1998). Normative EEG databases and EEG biofeedback. Journal of Neurotherapy, 2(4), 8-39. https://doi.org/10.1300/J184v02n04_02
Thatcher, R. W., Lubar, J. F., & Koberda, J. L. (2019). Z-Score EEG biofeedback: Past, present, and future. Biofeedback, 47(4), 89-103. https://doi.org/10.5298/1081-5937-47.4.04
Thomas, C. (2007). What is a montage? In EEG instrumentation. American Society of Electroneurodiagnostic Technologists, Inc.
Thompson, M., & Thompson, L. (2015). Neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for the Advancement of Psychophysiology and Biofeedback.
Return to Top