Therapeutic Relationship, Coaching, and Reinforcement Strategies
Although some of "what works" in therapy is attributable to specific techniques that therapists employ, a greater proportion of therapy's success is due to the quality of the therapeutic relationship (or "alliance") between the therapist and the client (Norcross & Wampold, 2011a; Rosenfeld, 2009; Wampold & Imel, 2015). Therapy manuals typically don't emphasize this relationship; instead, they tend to emphasize technique. In other words, they generally overlook "how" therapists relate to their clients in favor of "what" therapists do with (or to) their clients. A therapist who operates as a technician carrying out mechanical, predetermined methods can do a disservice to clients who seek a meaningful human connection (Sommers-Flanagan & Sommers-Flanagan, 2009). In fact, some psychologists argue that it's the relationship, not the technique, that should be evidence-based (Kazantzis, Cronin, Norton, Lai, & Hofmann, 2015). Along those lines, soon after proponents of the manualized treatment movement published their landmark book A Guide to Treatments That Work (Nathan & Gorman, 1998), another group of psychologists responded with contrasting viewpoints in a book fittingly titled Psychotherapy Relationships That Work (Norcross, 2002), insisting that the therapist-client relationship should not be neglected but should be recognized and studied as a focal point of what makes therapy work (Pomerantz, 2020, p. 57).

What You Will Learn in This Chapter
This unit explores the therapeutic relationship as the foundation of effective neurofeedback training. You will learn how cultural sensitivity, the therapeutic alliance, and coaching principles shape successful client outcomes. You will also examine how motivational interviewing sustains engagement, and how operant conditioning, reinforcement schedules, and shaping techniques drive the learning that underlies neurofeedback.
By the end of this chapter, you will understand why warm, collaborative relationships matter as much as technical skill, and how to apply personal training principles and reinforcement strategies to optimize your clients' progress.
BCIA Blueprint Coverage: This unit addresses VIII. Treatment Implementation - B. Therapeutic Relationship, Coaching, and Reinforcement Strategies.
Learning Objectives
After completing this unit, you will be able to:
Explain how cultural competence and the therapeutic alliance shape neurofeedback outcomes.
Describe the person effect and the evidence linking therapist manner to training success.
Apply the four personal training principles of specificity, individualization, overload, and progression to session design.
Use motivational interviewing skills to build engagement and elicit change talk.
Distinguish the four operant consequences and select reinforcement schedules that support transfer and resist extinction.

We will cover the Therapeutic Relationship, Coaching, and Reinforcement Strategies in this unit.
The Therapeutic Relationship
Culture-Specific Perspectives
This section examines how cultural background shapes the therapeutic encounter and why providers must adapt their approach accordingly. We will explore why Western therapeutic models can clash with non-Western norms and what culturally competent neurofeedback practice looks like in clinical settings.
North American and Western European psychotherapy models typically encourage clients to openly discuss their difficulties and feelings in order to develop insight and self-regulation. However, norms governing disclosure vary across cultural groups and within them, and reticence about difficult feelings may reflect culturally grounded values, prior experience of stigma, or a protective response to unequal power in the clinical encounter rather than resistance to treatment (Fontes, 2008; Toukmanian & Brouwers, 1998). Many neurofeedback providers serve diverse populations across VA medical centers, hospitals, and community clinics, and they will inevitably work with clients whose cultural backgrounds differ from their own.

Culturally competent neurofeedback providers understand their clients' expectations about the training process and recognize the cultural norms that affect each client's comfort with service delivery. This competence starts with self-awareness: providers must examine their own cultural biases before they can recognize and respect their clients' cultural values (Pomerantz, 2020). For example, a provider working with a veteran from a collectivist cultural background may need to involve family members in goal-setting rather than relying on an individualistic treatment model.
Providers should create an environment where clients feel safe and where their cultural values are respected. Cultural sensitivity should inform every aspect of training, from client orientation and skin preparation to sensor application, training instructions, feedback delivery, and practice assignments. In sum, cultural competence is not a peripheral concern but a foundational requirement that shapes every interaction between provider and client.
Therapeutic Alliance
This section covers the therapeutic alliance, the size of its contribution to clinical outcome, and the early biofeedback research indicating that therapist warmth affects training success. Understanding the alliance will help you appreciate why the human element of neurofeedback cannot be reduced to a technical procedure.
The therapeutic alliance is a trusting partnership between the therapist and client focused on achieving the client's goals. Building this alliance begins with the very first contact and continues throughout the entire relationship. Listening is only half the process; the therapist must also demonstrate that they have heard the client and that they share the client's objectives. Client education should emphasize how assessment, training, practice assignments, and progress reports all address the client's specific concerns.
Research consistently shows that the therapeutic relationship makes a substantial and reliable contribution to clinical outcome. Across 295 independent samples the alliance–outcome correlation is r = .278, about 8% of the variability in treatment outcome (Flückiger et al., 2018), and the task force that reviewed this literature concluded that the relationship accounts for why clients improve at least as much as the particular treatment method does (Norcross & Wampold, 2011a). That is a moderate effect rather than the single largest predictor, but unlike most predictors of outcome it is one the clinician can influence (Beitman & Manring, 2009; Wampold, 2010).
Crucially, it is the client's perception of the relationship that matters most, because that perception drives engagement and effort. Clients prefer warm, relatable therapists who make them feel understood (Swan & Heesacker, 2013). For the biofeedback and neurofeedback provider, this finding means that interpersonal warmth is not merely a nicety but a clinical variable with measurable impact.

An early demonstration of therapist influence comes from Taub and School (1978), whose report of a person effect, the observation that the therapist-client relationship is a critical aspect of biofeedback training, arose in hand-warming training. An experimenter who was "informal and friendly" trained 19 of 21 participants (90.5%) to control skin temperature, while an "impersonal" experimenter succeeded with only 2 of 22 (9.1%) (p. 617). The authors call that comparison "admittedly unsystematic," noting that the two experimenters worked at different times and participants were not randomly assigned, so they then manipulated manner directly, having one experimenter treat one group impersonally and another in a friendly way. Over the last three days of a 10-day series the impersonally treated group changed hand temperature by a mean of 1.3°F and the friendly-manner group by 4.2°F (p. 618), "by far the largest experimental effect we have obtained by the manipulation of any single variable." It is that controlled comparison, not the anecdote, that carries the point.
Kamiya (unpublished, quoted in Neumann, 2001, p. 32, as cited in Strehl, 2014) observed:
My experience with years of biofeedback training with various physiological modalities leaves me with the conviction that a very large portion of the total influences on learning is bio-social in nature, testifying to the evolution of the species as a social species. Though seldom discussed in the scientific literature, the nature of interpersonal relations between trainer and trainee are often decisive for learning progress.
Because the evidence linking the therapeutic relationship and treatment success is correlational, researchers cannot definitively determine the direction of causation. Good relationships may increase client commitment, effort, and success. Conversely, as clients succeed, they may develop greater trust in and affinity for their therapist (Zilcha-Mano et al., 2014). This reciprocal dynamic means that therapists who invest in the relationship early may set in motion a virtuous cycle where relational warmth fuels progress, and progress deepens the relationship.
The therapeutic relationship contributes substantially to clinical outcome, roughly 8% of outcome variability, and accounts for client improvement at least as much as the specific technique does. Cultural competence, starting with provider self-awareness, is the foundation of an effective alliance. The person effect illustrates how strongly therapist manner can affect training outcomes, and Taub and School's controlled comparison supports reading that relationship causally. Because the relationship between alliance quality and treatment success appears reciprocal, early investment in the therapeutic bond can create a positive feedback loop that benefits both client engagement and clinical results.
The Therapist Matters More Than You Might Think
In an era of sophisticated technology, it is tempting to think the equipment does the work. Research tells a different story. As the person effect described above makes clear, the same hand-warming technique delivered with the same equipment produced markedly different results depending on the experimenter's manner, a difference Taub and School (1978) went on to confirm by manipulating that manner directly. The lesson for neurofeedback is that the provider is never a neutral delivery mechanism for the protocol. The quality of the connection shapes whether learning happens at all.
Your Brain Actually Syncs with Your Therapist's Brain
Hyperscanning research has found that during therapy the brain activity of therapist and client can become correlated. This inter-brain synchrony is reported when two people engage in shared emotional and cognitive processes, and it has been studied alongside behavioral markers such as eye contact, mirrored expressions, and synchronized speech rhythms (Meehan, 2025; Sened et al., 2022).

Sened et al. (2022) propose an inter-brain plasticity model in which repeated exposure to high synchrony gradually improves a client's capacity to synchronize with others. It is a theoretical model built on small-sample, largely correlational studies, and its authors note that no study has yet tested the complete model. They do not report that synchrony improves cognitive flexibility or produces deeper client insight. What the model does suggest is that being fully present and attuned, not merely technically competent, may be part of how therapy works rather than a preliminary to it.
Three related concepts capture what makes therapeutic relationships work. Relational presence means being fully engaged with the client so they feel genuinely seen and valued. Attunement means accurately perceiving and responding to the client's emotional signals. Co-regulation means helping clients manage their emotional states through the interaction itself, which over time teaches them to regulate themselves.
The provider is never a neutral delivery mechanism for a protocol, because the quality of the connection shapes whether learning happens at all. Hyperscanning work reports that therapist and client brain activity can become correlated during therapy, and the inter-brain plasticity model treats that synchrony as a possible mechanism of change rather than a preliminary to it. The evidence base is small and largely correlational, so treat the model as promising theory rather than established fact. Relational presence, attunement, and co-regulation name the clinical skills that make the relationship work.
Coaching
Therapists Should Be Credible Models
This section covers why effective neurofeedback coaching starts with the clinician's own self-regulation skills. We will explore credible modeling, both intentional and unintentional, and the four personal training principles that structure successful neurofeedback sessions.
Unlike the stereotypical "out-of-shape coach with a beer gut," neurofeedback providers should develop and practice the skills they teach. Erik Peper has long argued that therapists should be self-experienced, meaning that they should practice the methods they teach (Peper et al., 2008). Consider the credibility problem: if you sought treatment for anxiety, how confident would you feel if your therapist appeared "stressed out" and offered you an ice-cold handshake? Our colleague, Don Moss, has learned to warm his hands during freezing Michigan winters because children expect him to prove that he can do what he teaches.
Therapists are both intentional and unintentional models for their clients. Self-regulation training increases clinicians' awareness of their own psychophysiological responses, including cold hands, breath-holding, and incomplete muscle relaxation, that clients may unconsciously detect and imitate. This process, implicit modeling, is powerful precisely because it operates outside of conscious awareness for both clinician and client. Do not confuse it with covert modeling, a distinct technique in which the client imagines a model performing the target behavior (Kazdin, 1973). Unless therapists become aware of their own dysfunctional patterns, they risk inadvertently teaching those patterns to the people they are trying to help.
Personal training delivers three important benefits: it enables therapists to develop the self-regulation skills they intend to teach, it increases their confidence in the effectiveness of their methods, and it helps them better understand the frustrations their clients will inevitably experience. In short, a credible neurofeedback clinician practices what they preach.
Therapists Should Be Good Personal Trainers
Successful personal training follows a clear sequence: assessment, explanation of training goals, modeling of the desired skill, effective instructions delivered through systematic techniques, immediate and useful performance feedback, graduated challenge with appropriate reinforcement, and sufficient time to acquire the skill. Practice outside of the clinic is critical to skill acquisition, just as an athlete's gains depend on training between sessions with their coach.

Four personal training principles should inform neurofeedback training: specificity, individualization, overload, and progression. The authors are indebted to Crossley's (2012) Personal Training: Theory and Practice for their coverage of these concepts. Understanding these principles helps clinicians structure sessions that are both systematic and responsive to each client's unique learning trajectory.
The principle of specificity states that improvement is specific to the training provided. The closely related SAID principle proposes that we achieve Specific Adaptation to Imposed Demands; in plain terms, "we get good at what we do." However, carryover, where training on one task influences the performance of others, can extend the benefits of a session. For example, practitioners may provide heart rate variability biofeedback before neurofeedback to increase client attention and normalize breathing, leveraging carryover to enhance the primary training.
The principle of individualization reminds us to adjust training to each person because learning curves and responses to interventions differ. High responders learn self-regulation quickly, whereas low responders need more time and effort. Likewise, although most clients may benefit from an intervention, a minority may deteriorate; for example, a client presenting with anxiety whose symptoms worsened when the clinician down-trained fast beta. Clinicians can individualize training based on EEG or qEEG assessment and a detailed health or performance history that includes medication use and prior self-regulation practice.
The principle of overload proposes that we challenge clients to promote positive adaptation, meaning measurable performance improvement. There is a "Goldilocks zone," called optimal overload, in which stress and recovery are balanced to produce the best training effect. Excessive stress or insufficient recovery time can cause negative adaptation, which prevents or slows learning. Clinicians avoid this outcome by not exceeding the point of failure, the threshold where performance deteriorates. In neurofeedback, the level of challenge can be adjusted by changing reinforcement requirements (e.g., reward and inhibit thresholds and duration), task difficulty, and training length.
Finally, the principle of progression asserts that challenge must increase systematically to maintain optimal overload and avoid a plateau, where a client ceases to improve. If difficulty remains static as a client's self-regulation skills grow, adaptation and training effects will diminish. Consider the analogy of walking the same number of steps every day for years: although aerobic capacity may increase initially, it will plateau within weeks at the same workload. The same logic applies to neurofeedback: progressive challenge is what keeps the brain adapting.
Effective coaching begins with therapists who practice what they teach, because implicit modeling means that clinician behaviors, whether intentional or not, influence client learning. The four personal training principles of specificity, individualization, overload, and progression provide a practical framework for structuring neurofeedback sessions. Together, these principles help clinicians optimize client progress while avoiding plateau and negative adaptation.
Motivational Interviewing
Even the most skillful coaching and the best-engineered reinforcement will accomplish little if a client is not ready to engage. Motivational interviewing (MI) is a collaborative, person-centered counseling style designed to elicit and strengthen a person's own motivation and commitment to change by exploring and resolving ambivalence.

For neurofeedback providers, MI is a practical way to increase treatment engagement, strengthen the alliance, and support the between-session practice that skill acquisition depends on.
MI is best understood not as a warm-up that precedes the "real" training but as a clinical posture threaded through the entire encounter: assessment, feedback, treatment planning, and the ongoing work of training itself.
A Brief Review of MI Principles
MI was originally developed in the 1980s as a response to confrontational models of addiction treatment. Its foundational premise, that ambivalence about change is normal rather than pathological, represented a meaningful departure from the assumption that resistance signaled a character flaw or treatment failure (Miller & Rollnick, 2013).
Over subsequent decades, MI migrated far beyond its origins to become a transdiagnostic tool compatible with a wide range of evidence-based interventions, including cognitive behavioral therapy and neurofeedback.
MI's earlier editions organized practice around four core principles: express empathy, develop discrepancy, roll with resistance, and support self-efficacy (Miller & Rollnick, 2002). The third edition set these aside in favor of four processes (engaging, focusing, evoking, and planning) and retired resistance, separating it into sustain talk (client language favoring the status quo) and discord (strain in the working relationship) (Miller & Rollnick, 2013). The principles remain a serviceable summary, but the vocabulary has moved on.
In practice, MI unfolds through a set of communication skills summarized as OARS (open questions, affirmations, reflective listening, and summarizing), which together create a conversational environment in which people feel heard rather than directed and begin to articulate their own reasons for change. The clinician's role is collaborative rather than prescriptive. Change talk, the language in which a client expresses desire, ability, reasons, or need (preparatory change talk) and commitment, activation, or steps already taken (mobilizing change talk), is actively elicited and reinforced (Miller & Rollnick, 2013).

The evidence for integrating MI with other treatments is encouraging. Marker and Norton's (2018) meta-analysis of twelve clinical trials found a moderate effect size (Hedges g = 0.59) favoring MI delivered as a prelude to CBT over CBT alone on overall anxiety symptom reduction. Dropout rates did not differ, and moderator analyses found no significant differences by anxiety diagnosis or MI dose, though with twelve trials those null tests are underpowered and do not establish equivalence. MI is not merely a prelude to treatment; it can function as a component of intervention that enhances engagement across modalities and across time.
MI in Practice: Meeting Disagreement Without Confrontation
Consider a composite case that illustrates why MI cannot always be cordoned off as its own modality. A mother scheduled a comprehensive evaluation for her 13-year-old daughter, arriving with a clear hypothesis: her daughter had ADHD. She described concentration problems, inconsistent academic performance, panic tied to schoolwork, fidgeting, and irritability. The evaluation, however, did not support ADHD.
The picture that emerged was one of generalized and social anxiety, with concentration difficulties that were situational, appearing under high perceived pressure and dissipating in low-stakes settings. When clinicians shared these impressions with the daughter, she was visibly relieved. When they shared the same impressions with the mother, she was not persuaded and left saying she would seek a second opinion.
The feedback session is an underappreciated clinical moment. Clinicians often approach it as simple information transfer, but for many families it is emotionally loaded before anything is said. Rather than presenting the anxiety diagnosis as the correction of a mistaken belief, the clinicians reflected back what the mother had actually observed, because she had observed real things: the concentration difficulties were real, the restlessness was real, the panic was real. They validated her observations first, then offered a different account of their origin, and they held space for her uncertainty without trying to resolve it immediately.
She still left unconvinced, and that was not a clinical failure. MI does not guarantee movement; it creates the conditions in which movement becomes more possible.
Several months later the mother returned, now requesting therapy for her daughter. Her position had shifted only partially: she acknowledged that CBT and exposure-based work might help, but she was not prepared to say ADHD was off the table. In MI terms she was ambivalent, which is a clinically valuable place to be. Ambivalence is not resistance; it is the coexistence of competing motivations, and it is workable. The clinicians accepted that ambivalence without trying to collapse it prematurely, framing the work inclusively: whatever was driving the difficulty, the skills being built were the right ones.
As treatment proceeded, the team invited the mother to join the final 15 minutes of every session: brief, structured, daughter-led check-ins to review skill practice and support it at home. In those windows the clinicians were not delivering psychoeducation so much as reflecting, reframing, and reinforcing.
Over weeks and months, the mother began to notice the relationship between her own expectations and her daughter's symptom severity, and eventually articulated, unprompted, that her daughter's achievements had not come without cost, and that she was no longer sure she wanted to keep paying that price. That was change talk. The clinicians reflected it, affirmed it, and let it sit. The lesson generalizes directly to neurofeedback: when the maintaining environment is misaligned with training goals, MI with the people around the client can matter as much as the primary intervention.
Motivational interviewing is a collaborative style for eliciting a client's own motivation to change by resolving ambivalence rather than confronting it. Its four classic principles (express empathy, develop discrepancy, roll with resistance, and support self-efficacy) are enacted through the OARS skills and the deliberate reinforcement of change talk, although the method's third edition recast the principles as four processes and replaced resistance with sustain talk and discord. Adding MI to CBT for anxiety disorders improves outcomes over CBT alone, and MI's usefulness extends well beyond a pretreatment warm-up: it belongs in feedback sessions, in collateral contacts with family, and in the ongoing engagement work that sustains neurofeedback practice between sessions.
Reinforcement Strategies
A Review of Operant Conditioning
This section reviews operant conditioning as the learning mechanism that drives neurofeedback. We will cover the foundational concepts from Thorndike and Skinner, the four types of consequences, and how each applies to neurofeedback practice. We will also examine reinforcement criteria, shaping, discrimination, and generalization.
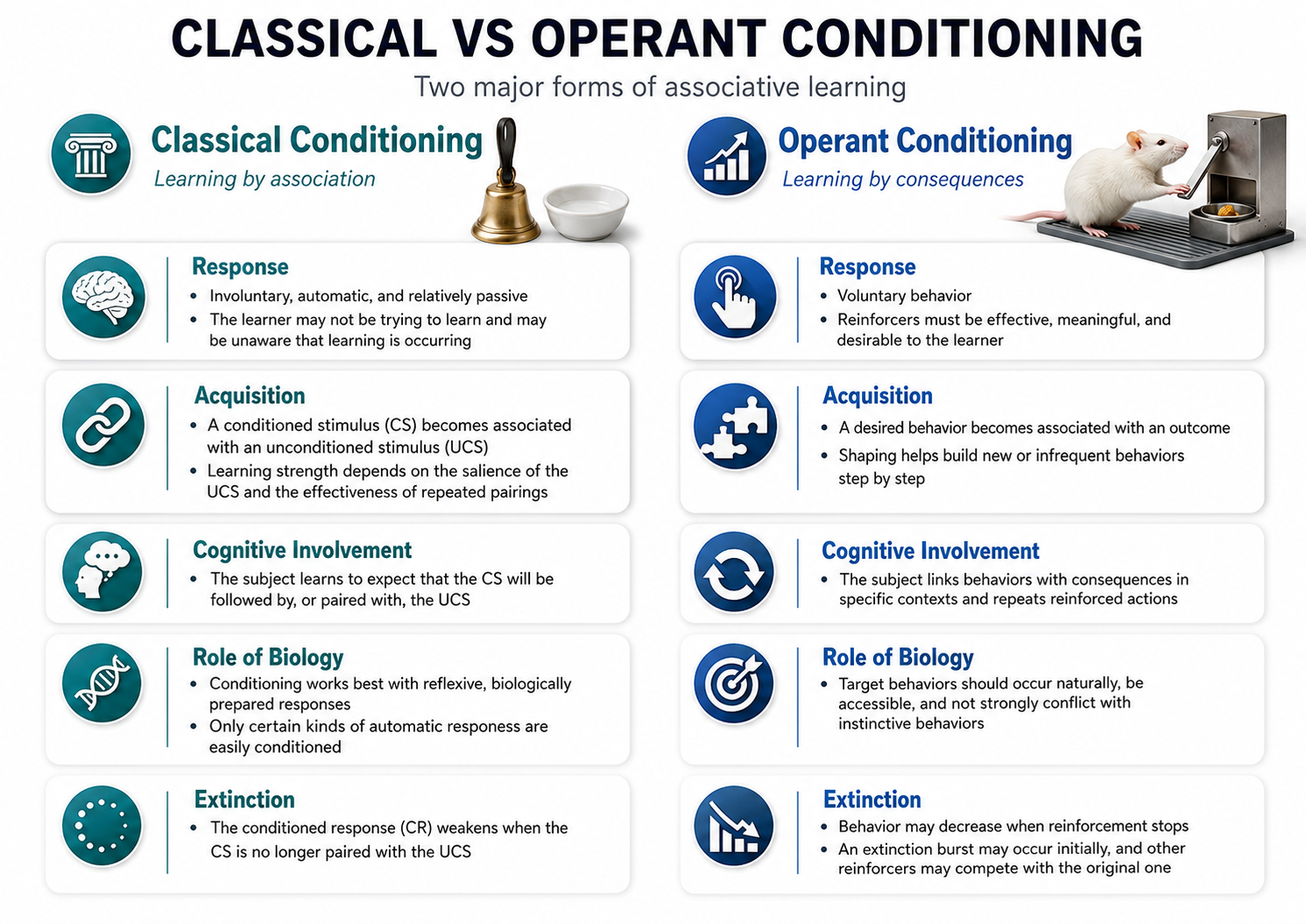
Edward Thorndike's law of effect proposed that the consequences of behavior determine whether that behavior becomes part of your repertoire. Thorndike observed that cats learned to escape "puzzle boxes" by repeating successful actions and abandoning unsuccessful ones, and gave the principle its best-known statement in Animal Intelligence: Experimental Studies (Thorndike, 1911, p. 244). Building on this foundation, operant conditioning is an unconscious associative learning process that modifies operant behaviors, voluntary actions that operate on the environment to produce an outcome, by manipulating their consequences (Miltenberger, 2016).
Operant conditioning differs from classical conditioning in a fundamental way. Where operant conditioning teaches the association between a voluntary behavior and its consequences, classical conditioning teaches the predictive relationship between two stimuli to modify involuntary behavior. Understanding this distinction matters for neurofeedback providers because the training they deliver relies primarily on operant mechanisms: clients learn to modify their own brain activity by experiencing the consequences of doing so.
Neurofeedback teaches self-regulation of neural activity and related "state changes" through operant conditioning via the selective presentation of reinforcing stimuli, including visual, auditory, and tactile displays. Sherlin et al. (2011) emphasize that clinicians should understand the specific waveforms being trained (e.g., SMR), the duration of the event to be reinforced (e.g., a 0.25-s SMR spindle rather than any excursion above the amplitude threshold), and the neurophysiology behind them in order to provide effective training. Operant conditioning always occurs within a situational context, and the identifying characteristics of that situation are called discriminative stimuli, the environmental, physical, cognitive, and emotional cues that signal when to perform operant behaviors.
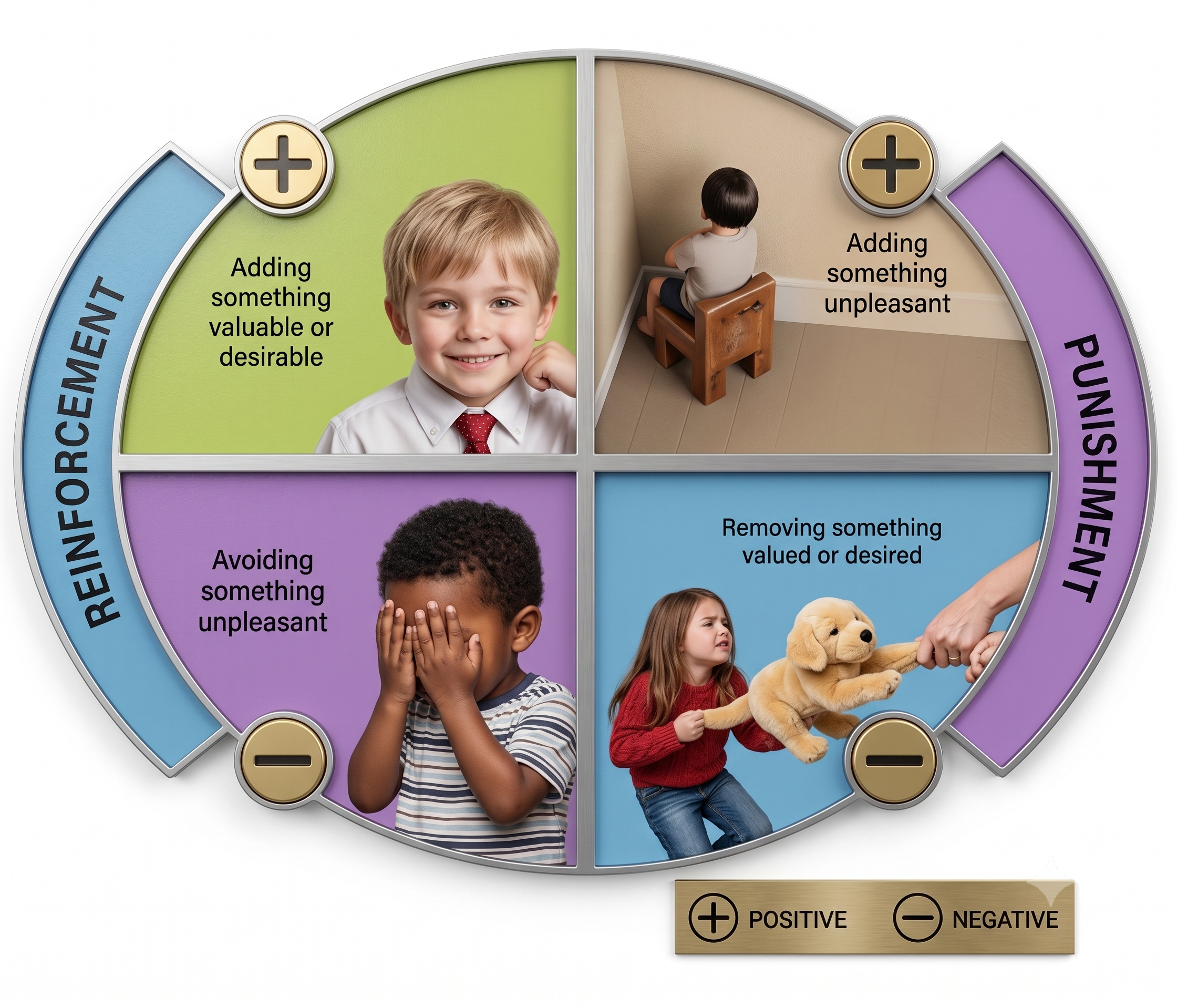
The consequences of operant behaviors can either increase or decrease their frequency. Skinner (1953) distinguished positive reinforcers, whose presentation strengthens behavior, from negative reinforcers, whose withdrawal strengthens it, and defined punishment as the two inverse operations. The familiar two-by-two table (positive reinforcement, negative reinforcement, positive punishment, and negative punishment) is a later systematization within applied behavior analysis rather than Skinner's own terminology (Cooper et al., 2019). Positive and negative reinforcement increase behavior, while positive and negative punishment decrease it.
Importantly, we cannot know in advance whether a given consequence will be reinforcing or punishing, because these are not intrinsic properties; we can only determine their effect by measuring how they change the preceding behavior. In neurofeedback, the movie or game that motivates a client's best performance is the effective reinforcer, regardless of the therapist's personal preference.
Positive reinforcement increases the frequency of a desired behavior by making a desired outcome contingent on performing the action. For example, a movie plays when a client diagnosed with attention deficit hyperactivity disorder (ADHD) increases low-beta and decreases theta activity.
Negative reinforcement increases the frequency of a desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on performing the action; for example, an athlete's anxiety decreases as they shift from high-beta to low-beta activity.
Positive punishment decreases or eliminates an undesirable behavior by adding something unwanted; for example, a burst of static or an unpleasant tone when a client's high-beta amplitude rises.
Negative punishment decreases or eliminates an undesirable behavior by removing what is desired; for example, oppositional behavior could result in a clinician turning off a popular game, and increased fidgeting could dim a favorite movie and lower its sound. The familiar neurofeedback inhibit displays, dimming the picture and reducing the volume, are negative punishment, because something appetitive is withdrawn. They feel like the addition of something unpleasant, which is why they are so often miscategorized: ask what physically happens to the stimulus, not how it feels to the client. Together, these four consequence types give clinicians a flexible toolkit for shaping client behavior during neurofeedback sessions.
Reinforcement Criteria
Current research is exploring the optimal reinforcement criteria for neurofeedback training, and the parameters chosen have a marked impact on skill acquisition. Key variables include reinforcement schedule, frequency of reward, reinforcement delay, conflicting reinforcements, conflicting expectations, and environmental alteration.
Reinforcement can be continuous or partial. In continuous reinforcement, every correct response is rewarded quickly, and many neurofeedback protocols deliver continuous reinforcement during training sessions. Neurofeedback training can also incorporate transfer trials, conditions in which clients do not receive feedback (e.g., correct or incorrect) until a trial's conclusion, to promote generalization of the skill beyond the clinic (Sherlin et al., 2011).
Although continuous reinforcement is helpful during the early stages of skill acquisition, it becomes impractical as clients attempt to transfer the skill to real-world settings where reinforcement is intermittent. Partial reinforcement schedules, where the desired behavior is only rewarded some of the time, are therefore essential as training progresses. This transition also increases resistance to extinction, the process by which failure to reinforce a desired behavior decreases that behavior's frequency.
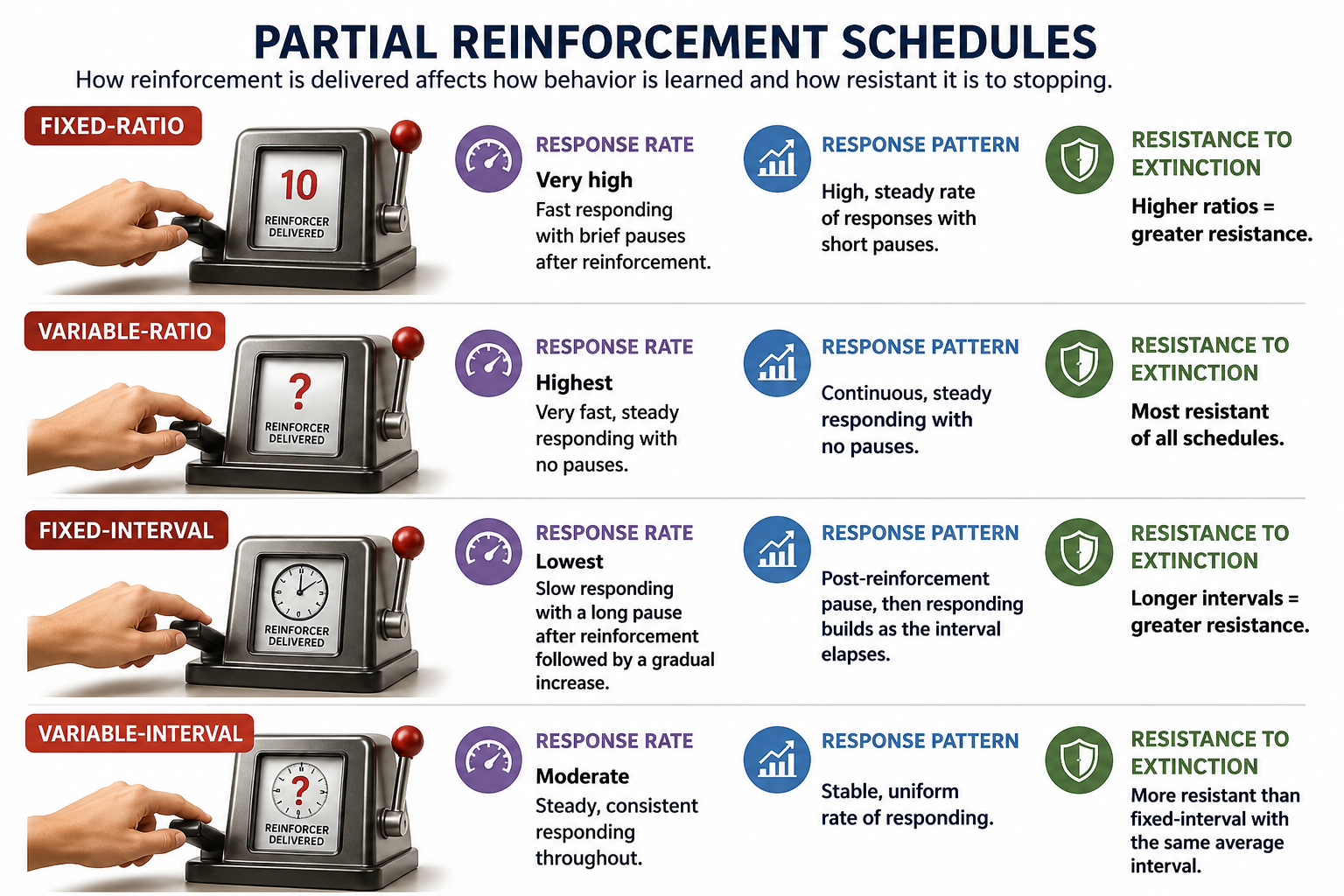
Two dimensions govern a schedule. Ratio versus interval, meaning whether reinforcement depends on the number of responses or on elapsed time, mainly determines the rate of responding, and ratio schedules produce higher rates. Fixed versus variable determines the pattern: fixed-ratio schedules produce a pause after each reinforcer and fixed-interval schedules a scalloped acceleration, whereas variable reinforcement schedules (a variable number of responses, or a variable duration of time) produce steady, uninterrupted responding and the greatest resistance to extinction, because the learner cannot predict when the next reinforcer is due (Cooper et al., 2019; Ferster & Skinner, 1957).
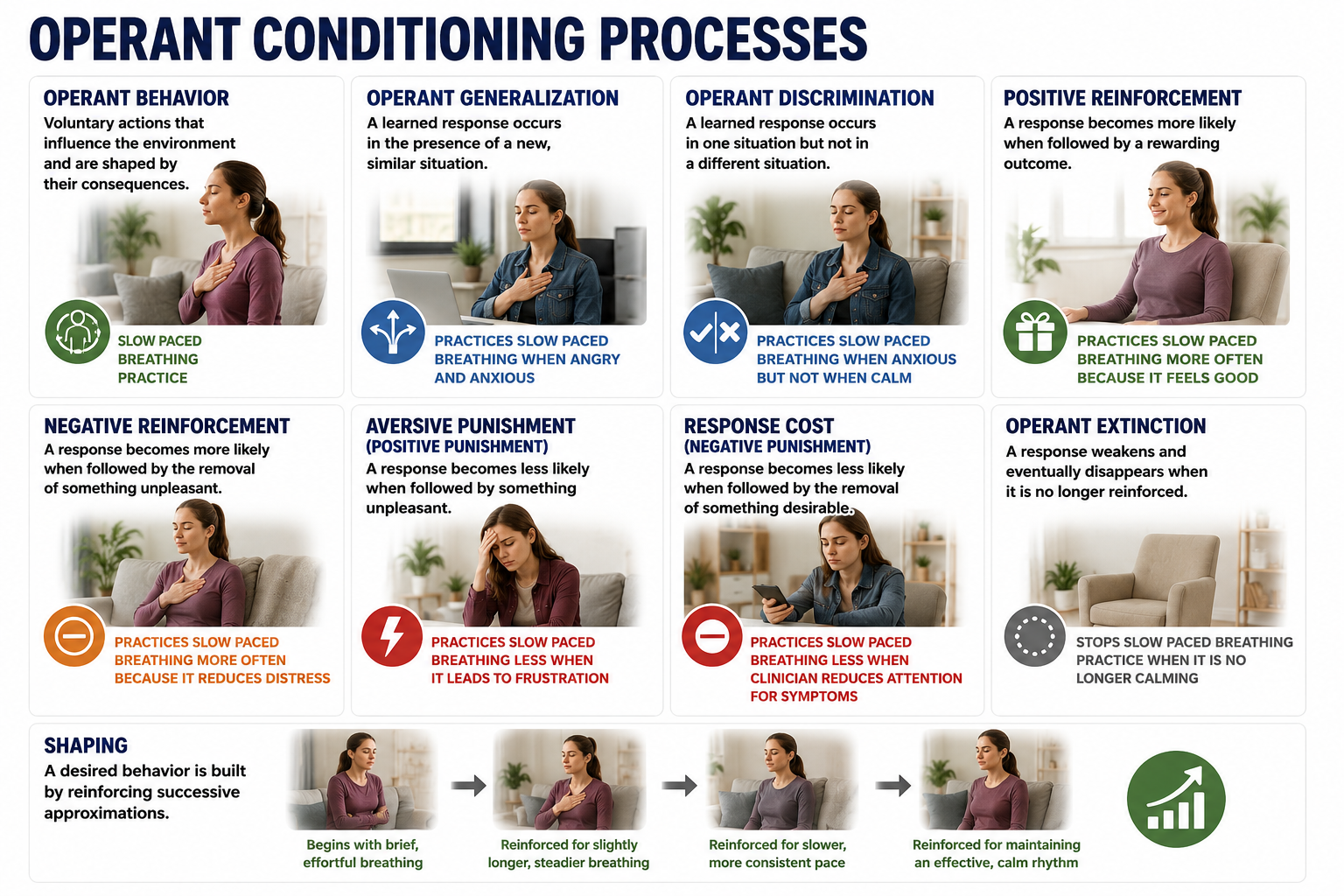
Shaping, also known as the method of successive approximations, teaches clients new behaviors and increases the frequency of rarely performed behaviors. The clinician starts by reinforcing spontaneous voluntary behaviors that resemble the target behavior and then progressively raises the reinforcement criteria to achieve the training goal. For example, the clinician can gradually require lower theta-to-beta ratios for a movie to play, so the client's brain is always working toward the next level of performance.
Discrimination and Generalization
Discrimination and generalization represent the ultimate goals of neurofeedback training: the ability to know when a skill is needed and to deploy it across diverse situations. Discrimination teaches clients when a desired behavior will be reinforced. The initial discriminative stimuli include cues from the training environment, like animations and tones. As training advances, a clinician may introduce a stressor following successful skill acquisition to "raise the bar," so that the stressor itself becomes a new discriminative stimulus for performing the desired behavior.
Generalization teaches the transfer of a desired behavior to multiple environments and in response to diverse stressors. While the ability to perform the learned response across many situations contributes to flexibility, it is not always advantageous, because discrimination, grounded in an understanding of context, helps the client determine when a response is required and which response is appropriate. For clinical and performance settings alike, the interplay between discrimination and generalization ensures that self-regulation skills are both versatile and context-sensitive.
Operant conditioning forms the learning foundation of neurofeedback, with four types of consequences (positive reinforcement, negative reinforcement, positive punishment, and negative punishment) providing a flexible toolkit for shaping client behavior. Reinforcement schedules should progress from continuous to partial and variable as training advances to promote real-world transfer and resist extinction. Shaping allows clinicians to raise the bar gradually, while discrimination and generalization ensure clients can apply self-regulation skills effectively beyond the clinic.
Research Findings
This section examines three lines of research with direct implications for how you deliver neurofeedback: post-reinforcement synchronization, the speed of reinforcement, and training strategies. These findings connect the laboratory to the clinic, showing why timing, reinforcement parameters, and instructional restraint all matter.
Post-Reinforcement Synchronization
Clemente et al. (1964) first described post-reinforcement synchrony (PRS) in an operant conditioning paradigm. PRS refers to parieto-occipital cortical alpha-like synchrony that appears following reinforcement of an operant behavior; it is recorded concurrently with, and is distinct from, the sensorimotor rhythm over sensorimotor cortex. Poschel and Ho (1972) showed that PRS depends on the performance of an operant behavior (e.g., pressing a lever) rather than the simple receipt of reinforcement: delivering the reinforcer without requiring a lever press causes well-developed PRS to habituate. Related reward-associated synchronization has been reported in monkeys and, for consummatory reward without an operant requirement, in humans (Sherlin et al., 2011).
In cats, the magnitude of PRS correlates with learning ability (Marczynski et al., 1981). For neurofeedback providers, PRS provides neurophysiological evidence that operant learning produces measurable cortical changes, reinforcing the scientific rationale behind the training they deliver.
Speed of Reinforcement
The timing of reinforcement is critical for associating a desired behavior with its consequences. The figure usually quoted comes from Sherlin et al. (2011, p. 297): "there is no fixed rule on what is the minimum or maximum acceptable delay . . . but based on Felsinger and Gladstone (1947) and Grice (1948), the latency should not exceed 250 to 350 ms." Two cautions belong with it.
The 250 to 350 ms is a ceiling, not an optimum, and the opening hedge is part of the recommendation. And neither 1940s paper studied feedback delay: Felsinger et al. (1947) treated reaction latency as a dependent variable, while Grice (1948) found rats needed a median of 20 trials under immediate reward, 580 at a five-second delay, and 155 when an immediate signal marked the correct response, showing that a conditioned reinforcer bridges delay, which is the warrant for marker tones and clicker-style feedback. Keep total system latency well under a second, and know what your system's actual latency is.
Training Strategies
Should clinicians tell clients how to regulate their brain activity, or let them figure it out? Strehl (2014) concluded that there are no validated interindividual strategies for slow cortical potential (SCP) feedback, which involves positive or negative polarizations of the EEG lasting from 300 ms to several seconds, originating in depolarizations of the apical dendritic tree in the upper cortical layers (Birbaumer, 1999). Participants develop individual strategies that differ between people and shift within a person during an experiment (Roberts et al., 1989). In Hardman et al. (1997), healthy participants trained on lateralized frontal SCPs showed no overall difference between a group instructed to use emotional strategies and an uninstructed group, although the uninstructed group showed a stronger within-session learning effect.
Similarly, in Kober et al. (2013) the four SMR-training participants who reported using no deliberate strategy were the only ones to improve linearly across ten sessions, which is a suggestive result drawn from a very small subgroup. Strehl concluded that clinicians should not suggest specific strategies. The practical takeaway is counterintuitive but important: explicit instruction can interfere with the implicit learning process that drives successful neurofeedback, so clinicians may serve their clients best by stepping back and letting the brain discover its own path to self-regulation.
Reinforcement Promotes Awareness and Performance
This section explores how reinforcement serves not only as a learning signal but also as a tool for building client awareness, motivation, and self-efficacy. We will cover goal-setting algorithms, the role of clinician encouragement, and why clients must understand that progress comes from their own efforts.
Auditory and visual reinforcement informs clients that they have met performance goals. Knowledge of results allows clients to perceive connections between their actions, internal sensations, and external feedback; in effect, reinforcement reveals when strategies work and how producing the desired EEG activity feels. This growing awareness is what transforms an abstract neurophysiological process into a skill the client can recognize and refine.
Positive reinforcement also enhances client motivation to improve brain performance. Training goals should reward effort while challenging clients to "up their game." A widely repeated goal-setting heuristic attributed to Olton and Noonberg (1980) is to raise goals when clients succeed more than 70% of the time and lower them when success falls below 30%. We could not locate this rule in that book, and no other source cites them for it, so treat the attribution as doubtful. The heuristic is plausible, but there is no compelling evidence that it beats a 50-50 strategy.
For a sourced anchor, Strehl (2014) reports that automatic threshold adjustment is often set to reward 60% to 70% of trials, while criticizing fixed-percentage thresholding, because it can reward performance worse than the previous session's, and recommending defined shaping goals instead. Since client learning curves and motivation can differ profoundly, clinicians should fine-tune goal-setting to each individual, ensuring that training goals fall within a "Goldilocks zone" that is neither discouraging nor unchallenging.
A clinician's encouragement is itself an essential form of reinforcement. When a client meets a goal, a simple "good job!" can be powerfully reinforcing, particularly for clients with low self-esteem. "I messages" can be especially effective. A comment such as "I'm impressed by how well you focused just then; you kept the game going for a long time" is easier for many clients to accept because it is framed as the clinician's personal observation.
Beyond moment-to-moment feedback, clinicians should regularly remind clients that progress results from the client's own efforts, not from the clinician or the equipment. Clients may have heard that neurofeedback is training rather than treatment, but regular reminders help them internalize this self-actualizing message and learn to take credit for their gains.
Post-reinforcement synchrony provides neurophysiological evidence that operant learning produces measurable cortical changes. Reinforcement latency should not exceed 250 to 350 ms, a ceiling rather than an optimum and one for which the source states there is no fixed rule, so system latency is a clinical concern. Research suggests that clinicians should avoid prescribing specific self-regulation strategies, since the available studies find no advantage for instructed strategies and some advantage for participants who report using none. Goal-setting should balance challenge with achievability, and clinician encouragement, especially "I messages" and reminders that progress belongs to the client, reinforces both performance and self-efficacy.
Neurofeedback and the Therapeutic Relationship: Emerging Research
Recent research highlights the bidirectional nature of the therapeutic relationship in neurofeedback. The inter-brain synchrony literature raises the possibility that coordinated neural activity between therapist and client contributes to learning during neurofeedback sessions. No published neurofeedback study has yet tested that possibility. What does exist is a separate, newer line of work in which synchrony is itself the training target (dyadic or multi-brain neurofeedback), and those reports are feasibility demonstrations, not outcome trials. The speculation is worth naming because it is testable: it asks whether the therapeutic relationship is not merely a psychological variable but a neurophysiological one.
Personalized Reinforcement Through Real-Time Adaptation
Advances in neurofeedback software are enabling real-time adaptation of reinforcement parameters based on individual client responses. These adaptive systems can dynamically adjust reward thresholds, feedback modality, and challenge levels within a single session, moving beyond static protocols to provide truly individualized training. Rather than relying on predetermined settings, these systems respond to moment-to-moment changes in client performance, bringing the principles of individualization and progression to life in ways that were previously impractical.
Check Your Understanding
- How does the therapeutic alliance influence neurofeedback training outcomes, and what role does cultural competence play in building this alliance?
- What are the four personal training principles that inform neurofeedback coaching, and how does each apply to session design?
- How can motivational interviewing increase treatment engagement, and why is it best threaded through the entire clinical encounter rather than used only as a warm-up?
- How do the four types of operant conditioning consequences (positive reinforcement, negative reinforcement, positive punishment, and negative punishment) function in neurofeedback training?
- Why should reinforcement schedules transition from continuous to partial as neurofeedback training progresses?
- What does research on training strategies suggest about whether clinicians should instruct clients on specific strategies during neurofeedback?
Assignment
Now that you have completed this unit, which sounds do your clients prefer when they succeed during neurofeedback training? Which visual displays motivate them?
Glossary
alpha synchrony threshold: a criterion for receiving feedback that increases alpha amplitude over the scalp.
alpha variability threshold: a criterion for receiving feedback when alpha amplitude or its variability decrease.
ambivalence: the simultaneous experience of competing motivations, such as wanting change and fearing it, or holding two explanatory frameworks at once; in motivational interviewing, understood as a normal part of the change process rather than a sign of pathology or resistance.
attunement: accurately perceiving and responding to a client's emotional signals.
carryover: training on one task can influence performance on others.
change talk: client language that reflects movement toward change, comprising preparatory change talk (desire, ability, reasons, need) and mobilizing change talk (commitment, activation, taking steps); eliciting and reflecting change talk is a core motivational interviewing strategy.
co-regulation: helping clients manage their emotional states through the interaction itself, which over time teaches them to regulate themselves.
collateral information: reports from family members, friends, and healthcare professionals.
continuous reinforcement: rewarding every correct response quickly.
covert modeling: a behavior-therapy technique in which the client imagines a model performing the target behavior rather than observing a live or filmed model (Kazdin, 1973). Contrast implicit modeling.
cultural malpractice: assessment and treatment decisions biased by cultural insensitivity and ethnocentrism.
culturally-competent assessment: assessment that is informed by and sensitive to the meaning of actions, beliefs, and feelings within a client's culture.
discrimination: a learning process that teaches when a desired behavior will be reinforced.
discriminative stimuli: environmental, physical, cognitive, and emotional cues that signal when to perform operant behaviors.
dynamic z-score thresholds: dynamic thresholds that deliver feedback almost 50% of the time calculated from brief periods (e.g., 10 seconds).
evidence-based assessment: client evaluation using instruments that are reliable, valid, and possess clinical utility.
extinction: failure to reinforce a desired behavior reduces the frequency of that behavior.
generalization: a learning process that teaches the transfer of a desired behavior to multiple environments and in response to diverse stressors.
high responders: individuals who learn self-regulation quickly.
implicit modeling: unintentional modeling by a clinician, in which psychophysiological habits such as cold hands, breath-holding, or incomplete muscle relaxation are detected and imitated by clients outside the awareness of either party.
inhibit threshold: criterion for suspending feedback, analogous to a limbo bar, designed to decrease bandpass amplitude.
inter-brain synchrony: coordinated neural activity between therapist and client that arises during shared emotional and cognitive engagement, such as eye contact, mirrored expressions, and synchronized speech rhythms.
law of effect: the consequences of behavior determine its addition to your behavioral repertoire.
low resolution electromagnetic tomography (LORETA): Pascual-Marqui et al.'s (1994) distributed inverse solution, which estimates a smoothly varying three-dimensional current density throughout the brain volume from multichannel scalp EEG. Clinical neurofeedback commonly applies it to 19-channel 10-20 recordings, but the method is not restricted to any electrode count, and localization accuracy improves substantially with higher-density arrays.
low responders: individuals who learn self-regulation slowly.
motivational interviewing (MI): a collaborative, person-centered counseling style designed to elicit and strengthen an individual's own motivation and commitment to change by exploring and resolving ambivalence.
multimethod assessment: evaluation using multiple assessment tools.
negative adaptation: the slowing or deterioration of learning due to stress or insufficient recovery time when challenged.
negative punishment: a learning process that decreases or eliminates an undesirable behavior by removing a desired outcome.
negative reinforcement: a learning process that increases the frequency of a desired behavior by making the avoidance, termination, or postponement of an unwanted outcome contingent on performing the action.
OARS: the foundational motivational interviewing communication skills: open questions, affirmations, reflective listening, and summarizing.
operant behaviors: voluntary actions that operate on the environment to produce an outcome.
operant conditioning: an unconscious associative learning process that modifies operants by manipulating their consequences.
optimal overload: stress and sufficient recovery time produce an optimal training effect.
overpathologizing: labeling culturally normal behavior as abnormal.
partial reinforcement: rewarding desired behaviors only some of the time.
percentage of success: a z-score training protocol where a client receives feedback when a predetermined percentage of EEG components fall within ±1, 2, or 3 z-scores.
person effect: Taub and School's (1978) observation that biofeedback training is a social situation and that a client's relationship with the therapist is a critical aspect of training.
plateau: performance ceases to improve.
point of failure: performance deterioration due to excessive stress or insufficient recovery time.
positive adaptation: performance improvement when clients are challenged.
positive punishment: a learning process that decreases or eliminates an undesirable behavior by associating it with unwanted consequences.
positive reinforcement: learning process that increases the frequency of a desired behavior by making a desired outcome contingent on performing the action.
post-reinforcement synchrony (PRS): parieto-occipital cortical alpha-like synchrony following reinforcement of an operant behavior, depends on the performance of an operant behavior (e.g., pressing a lever) and not simple receipt of reinforcement.
principle of individualization: adjustment of training to the individual because learning curves and responses to interventions differ.
principle of overload: challenge clients to promote positive adaptation where performance improves.
principle of progression: increase challenge systematically to achieve optimal overload.
principle of specificity: improvement is specific to the training we provide.
ratio-threshold: a criterion for receiving feedback that reinforces changes in the ratio of two EEG bandpasses.
relational presence: being fully engaged with the client so they feel genuinely seen and valued.
reward threshold: a criterion for receiving feedback analogous to a hurdle in track designed to increase bandpass amplitude.
SAID principle: we achieve Specific Adaptation to Imposed Demands.
shaping: the method of successive approximations teaches clients new behaviors and increases the frequency of rarely performed behaviors.
situational: describing difficulties that appear in particular contexts and remit in others; distinct from state-dependent learning, in which retrieval is best when the internal state at recall matches the state at encoding.
slow cortical potentials (SCPs): positive or negative polarizations of the EEG that last from 300 ms to several seconds and originate in depolarizations of the apical dendritic tree in the upper cortical layers (Birbaumer, 1999). These potentials include the contingent negative variation (CNV), readiness potential, movement-related potentials (MRPs), and P300 and N400 potentials. SCPs modulate the firing rate of cortical pyramidal neurons by exciting or inhibiting their apical dendrites. They group the classical EEG rhythms using these synchronizing mechanisms.
therapeutic alliance: a trusting partnership between the therapist and client to achieve the client's goals.
transfer trials: conditions in which clients do not receive feedback (e.g., correct or incorrect) until a trial's conclusion to aid generalization.
variable reinforcement: reinforcement occurs after a variable number of responses (variable ratio) or following a variable duration of time (variable interval). Compared with their fixed counterparts these schedules produce steadier, uninterrupted responding and greater resistance to extinction; response rate is governed mainly by whether a schedule is ratio or interval rather than by whether it is fixed or variable.
z-score training: neurofeedback protocol that reinforces in real-time closer approximations of client EEG values to those in a normative database.
References
Baer, L., & Blais, M. A. (Eds.). (2010). Handbook of clinical rating scales and assessment in psychiatry and mental health. Humana Press.
Beitman, B. D., & Manring, J. (2009). Theory and practice of psychotherapy integration. In G. O. Gabbard (Ed.), Textbook of psychotherapeutic treatments (pp. 705-726). American Psychiatric Publishing.
Birbaumer, N. (1999). Slow cortical potentials: Plasticity, operant control, and behavioral effects. The Neuroscientist, 5(2), 74-78. https://doi.org/10.1177/107385849900500211
Clemente, C. D., Sterman, M. B., & Wyrwicka, W. (1964). Post-reinforcement EEG synchronization during alimentary behavior. Electroencephalography and Clinical Neurophysiology, 16, 355-365. https://doi.org/10.1016/0013-4694(64)90069-0
Collura, T. F. (2014). Technical foundations of neurofeedback. Routledge.
Conners, C. K. (2014). Conners Continuous Performance Test (3rd ed.). Multi-Health Systems.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2019). Applied behavior analysis (3rd ed.). Pearson.
Crossley, J. (2012). Personal training: Theory and practice (2nd ed.). Routledge.
Dana, R. H. (2005). Multicultural assessment: Principles, applications, and examples. Erlbaum.
Delis, D. C., Kaplan, E. F., & Kramer, J. H. (2001). Delis-Kaplan Executive Function System. The Psychological Corporation.
Demos, J. N. (2019). Getting started with EEG neurofeedback (2nd ed.). W. W. Norton & Company.
Felsinger, J. M., Gladstone, A. I., Yamaguchi, H. G., & Hull, C. L. (1947). Reaction latency (StR) as a function of the number of reinforcements (N). Journal of Experimental Psychology, 37(3), 214-228. https://doi.org/10.1037/h0055587
Ferster, C. B., & Skinner, B. F. (1957). Schedules of reinforcement. Appleton-Century-Crofts. https://doi.org/10.1037/10627-000
Flückiger, C., Del Re, A. C., Wampold, B. E., & Horvath, A. O. (2018). The alliance in adult psychotherapy: A meta-analytic synthesis. Psychotherapy, 55(4), 316-340. https://doi.org/10.1037/pst0000172
Fontes, L. A. (2008). Interviewing clients across cultures: A practitioner's guide. Guilford Press.
Grice, G. R. (1948). The acquisition of a visual discrimination habit following response to a single stimulus. Journal of Experimental Psychology, 38(6), 633-642. https://doi.org/10.1037/h0056158
Gualtieri, C. T., & Johnson, L. G. (2006). Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Archives of Clinical Neuropsychology, 21(7), 623-643. https://doi.org/10.1016/j.acn.2006.05.007
Hardman, E., Gruzelier, J., Cheesman, K., Jones, C., Liddiard, D., Schleichert, H., & Birbaumer, N. (1997). Frontal interhemispheric asymmetry: Self regulation and individual differences in humans. Neuroscience Letters, 221, 117-120. https://doi.org/10.1016/s0304-3940(96)13303-6
Hardt, J. V., & Kamiya, J. (1976). Conflicting results in EEG alpha feedback studies: Why amplitude integration should replace percent time. Biofeedback and Self-Regulation, 1(1), 63-75. https://doi.org/10.1007/BF00998691
Kaiser, D. A. (2008). Functional connectivity and aging: Comodulation and coherence differences. Journal of Neurotherapy, 12, 123-139. https://doi.org/10.1080/10874200802398790
Kazantzis, N., Cronin, T. J., Norton, P. J., Lai, J., & Hofmann, S. G. (2015). Reservations about the conclusions of the interdivisional (APA Divisions 12 & 29) task force on evidence-based therapy relationships: What do we know, what don't we know? Journal of Clinical Psychology, 71(5), 423-427. https://doi.org/10.1002/jclp.22178
Kazdin, A. E. (1973). Covert modeling and the reduction of avoidance behavior. Journal of Abnormal Psychology, 81(1), 87-95. https://doi.org/10.1037/h0034036
Khazan, I. Z. (2013). Clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. Wiley-Blackwell.
Kober, S. E., Witte, M., Ninaus, M., Neuper, C., & Wood, G. (2013). Learning to modulate one's own brain activity: the effect of spontaneous mental strategies. Frontiers in Human Neuroscience, 7, 695. https://doi.org/10.3389/fnhum.2013.00695
Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel, D. (2012). Neuropsychological assessment (5th ed.). Oxford University Press.
Marczynski, T. J., Harris, C. M., & Livezey, G. T. (1981). The magnitude of post-reinforcement EEG synchronization (PRS) in cats reflects learning ability. Brain Research, 204, 214-219. https://doi.org/10.1016/0006-8993(81)90667-3
Marker, C. D., & Norton, P. J. (2018). The efficacy of incorporating motivational interviewing to cognitive behavior therapy for anxiety disorders: A review and meta-analysis. Clinical Psychology Review, 62, 1-10. https://doi.org/10.1016/j.cpr.2018.04.004
Meehan, Z. M. (2025). 5-min science: Inter-brain plasticity can enhance psychotherapy. https://www.biosourcesoftware.com/post/5-min-science-inter-brain-plasticity-can-enhance-psychotherapy
Miller, W. R., & Rollnick, S. (2002). Motivational interviewing: Preparing people for change (2nd ed.). Guilford Press.
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). Guilford Press.
Miltenberger, R. G. (2016). Behavior modification: Principles and procedures. Cengage Learning.
Nathan, P. E., & Gorman, J. M. (Eds.). (1998). A guide to treatments that work. Oxford University Press.
Neumann, N. (2001). Gehirn-Computer-Schnittstelle: Einflussfaktoren der Selbstregulation Langsamer Kortikaler Hirnpotentiale. Dissertation Tübingen: Schwäbische Verlagsgesellschaft.
Norcross, J. C. (Ed.). (2002). Psychotherapy relationships that work: Therapist contributions and responsiveness to patients. Oxford University Press.
Norcross, J. C., & Wampold, B. E. (2011a). Evidence-based therapy relationships: Research conclusions and clinical practices. Psychotherapy, 48(1), 98-102. https://doi.org/10.1037/a0022161
Olton, D. S., & Noonberg, A. R. (1980). Biofeedback: Clinical applications in behavioral medicine. Prentice-Hall, Inc.
Pascual-Marqui, R. D., Michel, C. M., & Lehmann, D. (1994). Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. International Journal of Psychophysiology, 18(1), 49-65. https://doi.org/10.1016/0167-8760(84)90014-X
Peper, E., Tylova, H., Gibney, K. H., Harvey, R., & Combatalade, D. (2008). Biofeedback mastery: An experiential teaching and self-training manual. Association for Applied Psychophysiology and Biofeedback.
Pomerantz, A. M. (2020). Clinical psychology: Science, practice, and diversity (5th ed.). Sage Publications.
Poschel, B. P. H., & Ho, P. M. (1972). Post-reinforcement EEG synchronization depends on the operant response. Electroencephalography and Clinical Neurophysiology, 32(5), 563-567. https://doi.org/10.1016/0013-4694(72)90067-3
Psychology Tools. (n.d.). Psychological assessment tools for mental health. Retrieved March 9, 2021, from https://www.psychologytools.com/download-scales-and-measures/
Ribas, V. R., Ribas, R. de M. G., & Martins, H. A. de L. (2016). The learning curve in neurofeedback of Peter Van Deusen: A review article. Dementia and Neuropsychologia, 10, 98-103. https://doi.org/10.1590/s1980-5764-2016dn1002005
Roberts, L. E., Birbaumer, N., Rockstroh, B., Lutzenberger, W., & Elbert, T. (1989). Self-report during feedback regulation of slow cortical potentials. Psychophysiology, 26, 392-403. https://doi.org/10.1111/j.1469-8986.1989.tb01941.x
Rosenfeld, G. W. (2009). Beyond evidence-based psychotherapy: Fostering the eight sources of change in child and adolescent treatment. Routledge.
Sadock, B. J., Sadock, V. A., & Ruiz, P. (2017). Kaplan and Sadock's comprehensive textbook of psychiatry (10th ed.). Wolters Kluwer.
Schwartz, M. S. (2016). Intake and preparation for intervention. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: A practitioner's guide (4th ed., pp. 217-232). Guilford Press.
Sened, H., Zilcha-Mano, S., & Shamay-Tsoory, S. (2022). Inter-brain plasticity as a biological mechanism of change in psychotherapy: A review and integrative model. Frontiers in Human Neuroscience, 16, 955238. https://doi.org/10.3389/fnhum.2022.955238
Sherlin, L. H., Arns, M., Lubar, J., Heinrich, H., Kerson, C., Strehl, U., & Sterman, M. B. (2011). Neurofeedback and basic learning theory: Implications for research and practice. Journal of Neurotherapy, 15, 292-304. https://doi.org/10.1080/10874208.2011.623089
Silverman, J., Kurtz, S., & Draper, J. (2013). Skills for communicating with patients (3rd ed.). CRC Press.
Skinner, B. F. (1953). Science and human behavior. Macmillan.
Soutar, R., & Longo, R. (2022). Doing neurofeedback: An introduction (2nd ed.). ISNR Research Foundation.
Strehl, U. (2014). What learning theories can teach us in designing neurofeedback treatments. Frontiers in Human Neuroscience, 8, 894. https://doi.org/10.3389/fnhum.2014.00894
Stucky, J., & Bush, S. S. (2017). Neuropsychology fact-finding casebook: A training resource. Oxford University Press.
Swan, L. K., & Heesacker, M. (2013). Evidence of a pronounced preference for therapy guided by common factors. Journal of Clinical Psychology, 69(9), 869-879. https://doi.org/10.1002/jclp.21967
Swingle, P. G. (2015). Adding neurofeedback to your practice: Clinician's guide to ClinicalQ, neurofeedback, and braindriving. Springer.
Taub, E., & School, P. J. (1978). Some methodological considerations in thermal biofeedback training. Behavior Research Methods & Instrumentation, 10(5), 617-622. https://doi.org/10.3758/BF03205359
Thatcher, R. W. (2020). Handbook of quantitative EEG and EEG biofeedback (2nd ed.). ANI Publishing.
Thompson, M., & Thompson, L. (2015). Neurofeedback book: An introduction to basic concepts in applied psychophysiology (2nd ed.). Association for Applied Psychophysiology and Biofeedback.
Thorndike, E. L. (1911). Animal intelligence: Experimental studies. Macmillan.
Thorndike, E. L. (1914). Educational psychology: Briefer course. Teachers College, Columbia University.
Toukmanian, S. G., & Brouwers, M. C. (1998). Cultural aspects of self-disclosure and psychotherapy. In S. S. Kazarian & D. R. Evans (Eds.), Cultural clinical psychology (pp. 106-124). Oxford University Press.
Wampold, B. E. (2010). The research evidence for the common factors model: A historically situated perspective. In B. L. Duncan, S. D. Miller, B. E. Wampold, & M. A. Hubble (Eds.), The heart and soul of change: Delivering what works in therapy (2nd ed., pp. 49-81). American Psychological Association.
Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.). Routledge.
Zilcha-Mano, S., Dinger, U., McCarthy, K. S., & Barber, J. P. (2014). Does alliance predict symptoms throughout treatment, or is it the other way around? Journal of Consulting and Clinical Psychology, 82(6), 931-935. https://doi.org/10.1037/a0035141
Return to Top