
HRV Training Protocols
What You Will Learn
Heart rate variability biofeedback (HRVB) represents one of the most promising self-regulation interventions available to clinicians today. This chapter guides you through the complete process of delivering HRV biofeedback, from essential medical screening to the practice assignments that bridge clinic learning to everyday life. You will discover why the client-practitioner relationship forms the foundation of successful training, learn to recognize subtle signs of excessive effort that can sabotage progress, and master the art of selecting displays and pacing strategies that match each client's unique learning style.
Whether you work in the VA system, a hospital rehabilitation unit, a private clinic, or with elite athletes, this chapter provides practical knowledge you can apply immediately. By the end, you will understand not only what to do but why each element of the training protocol matters for your clients' long-term success.
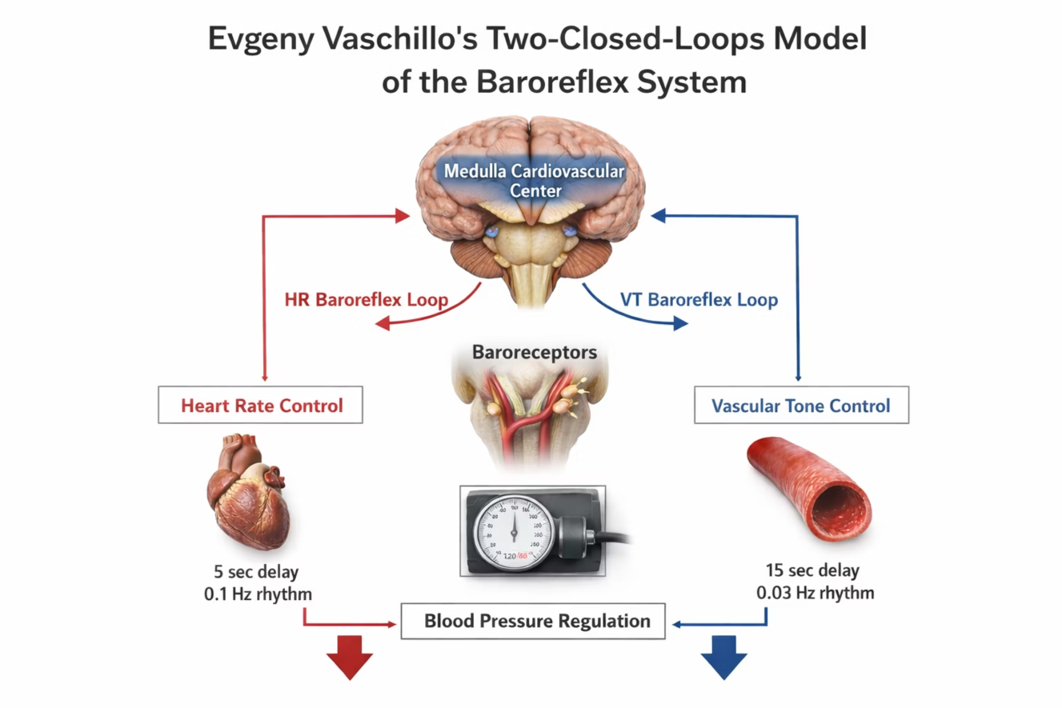
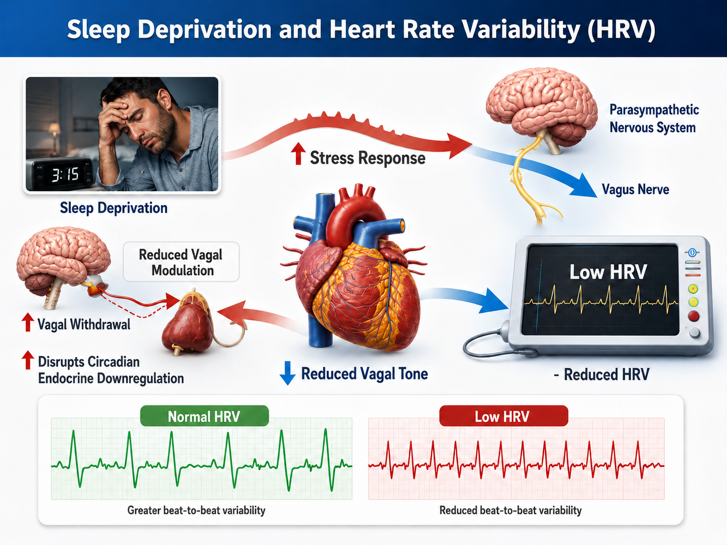
Heart rate variability (HRV) is an increasingly important biomarker. Biofeedback aims to exercise the baroreceptor reflex, a mechanism that provides negative feedback control of blood pressure, and the vascular tone rhythm, the rhythmic oscillation in blood vessel diameter that contributes to blood pressure regulation and HRV. By stimulating these systems, HRVB enhances homeostatic regulation, builds regulatory reserve, and strengthens executive functions (Gevirtz, 2021).
Think of it as taking the cardiovascular system to the gym: just as resistance training builds muscle strength and endurance, HRVB builds the cardiovascular system's capacity to respond adaptively to stress.

The field owes much of its clinical foundation to Dr. Paul Lehrer and colleagues (2000, 2013), who published detailed descriptions of their HRVB resonance frequency protocol. These protocols have become the standard reference for clinicians worldwide, providing step-by-step guidance for assessment and training that has been validated across dozens of clinical trials.
Dr. Donald Moss poses a deceptively simple question: "Why do we train?" The answer cuts to the heart of our work. Clinicians providing HRVB training seek to improve their clients' ability to self-regulate, promote health, and enhance quality of life and performance. These goals remain constant whether you are working with a combat veteran managing PTSD, a cardiac patient in rehabilitation, or an Olympic athlete pursuing peak performance.
Core Elements of HRV Biofeedback
The client-practitioner relationship stands as the foundation of all biofeedback and neurofeedback training. HRV biofeedback reaches its full potential when both clinician and client practice mindfulness, fostering the self-awareness and sense of agency that drive lasting change. Effective coaching transforms technical feedback into meaningful learning experiences (Khazan, 2019).
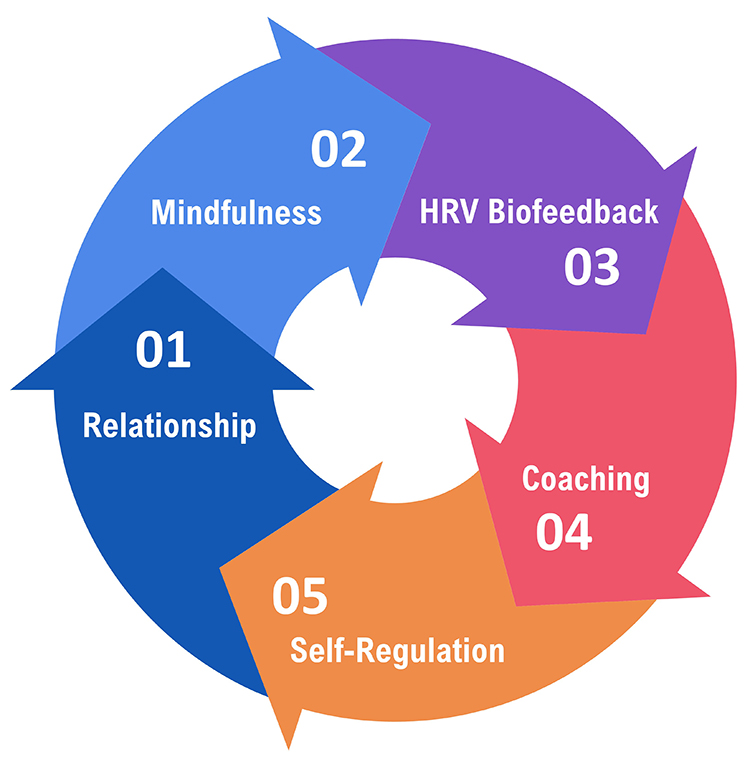
Mindfulness involves "paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally" (Kabat-Zinn, 1994). In the context of HRV training, mindfulness serves as the bridge between physiological feedback and behavioral change. When clients observe their heart rate (HR) patterns without judgment, they become curious scientists of their own physiology rather than frustrated students chasing numbers.

Mindfulness guides the trial-and-error process underlying self-regulation by helping clients draw connections between their actions, internal feedback, and results. A veteran might notice that memories of deployment increase HR irregularity, while focusing on the breath creates smoother, more wavelike patterns. These insights, accumulated through mindful observation, form the foundation of lasting self-regulation skills.
Through this process, clients discover their unique psychophysiological response patterns. One person may find that visualizing ocean waves produces the smoothest HR oscillations, while another achieves the same result through counting or prayer. This individual variability is a feature, not a bug. The feedback helps each client identify which strategies best increase their respiratory sinus arrhythmia (RSA), the rhythmic increase in HR during inhalation and decrease during exhalation, and their overall HRV.
Mindfulness also supports emotional self-regulation by teaching resilience, defined as adapting effectively to new challenges, stressors, threats, and trauma. For a first responder or military service member, resilience means returning to baseline functioning after acute stress. For a chronic pain patient, it means maintaining equilibrium despite ongoing discomfort. The skills are fundamentally the same, even as the contexts differ.
.jpg)
Modern wearable technology extends mindfulness training beyond the clinic. Devices like Lief Therapeutic's wearable signal clients with vibrations when stress responses are detected, enhancing awareness of triggers in everyday situations. This ecological momentary intervention transforms the smartphone notification into a cue for brief self-regulation practice.
Emotional self-regulation encompasses the self-monitoring, initiation, maintenance, and modulation of rewarding and challenging emotions, along with the avoidance and reduction of high levels of negative affect (Bridges, Denham, & Ganiban, 2004). This capacity matters for nearly every clinical population you will encounter, from anxiety disorders to cardiac rehabilitation to performance optimization.

Slow-paced breathing (SPB) involves healthy breathing at or near an individual's unique resonance frequency (RF), the frequency at which the cardiovascular system can be most effectively stimulated. While many practitioners default to 6 breaths per minute (bpm), adult resonance frequencies may range from 3.5 to 7.5 bpm. A client whose RF is 5.5 may see little difference in symptom severity or performance gains if trained at 6 bpm.
However, Dr. Khazan (2026) has cautioned that a client whose RF is 3.5 bpm may benefit far less if they breathe at 6.0 bpm. We don't know how much less. HRV biofeedback does not train clients to chase a magic number; rather, it helps each person find their optimal breathing or muscle contraction rate.
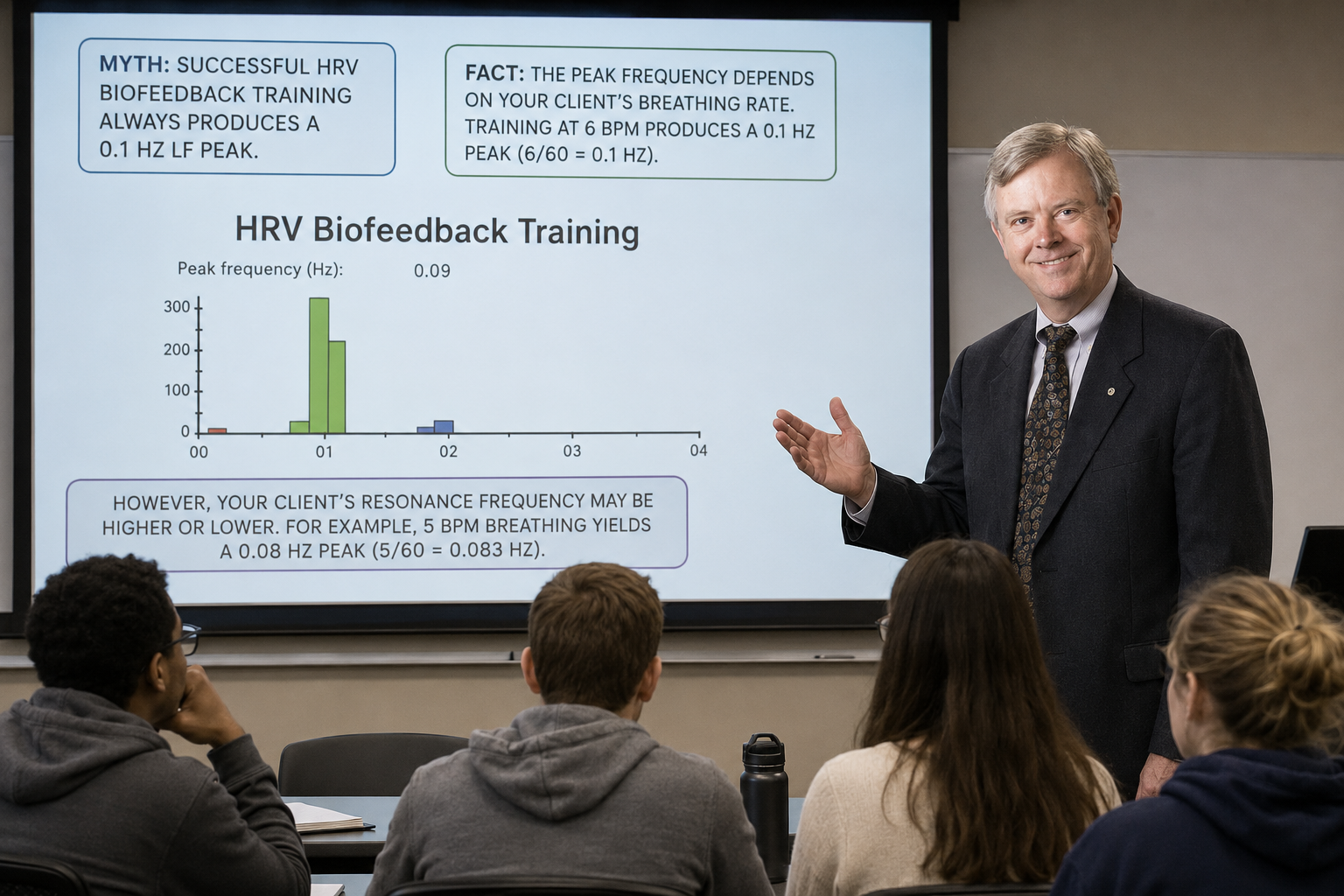
Clinicians should not conflate HRVB training with 0.1 Hz training. As Dr. Moss states in the Real Genius episode below, a client's low-frequency peak during RF training will only be at 0.1 Hz when their RF is 6 bpm (6/60 = 0.1 Hz). If their RF is 5 bpm, their peak will be 0.08 Hz (5/60 = 0.083 Hz).
The physiological mechanism is elegant: HRVB stimulates the baroreceptor reflex and vascular tone rhythm simultaneously. When breathing occurs at a client's RF, these two oscillating systems align in phase, producing maximum HR oscillation and maximum stimulation of vagal pathways. Over time, this repeated stimulation increases vagal tone and overall HRV, much like repeated weight training increases muscle strength.
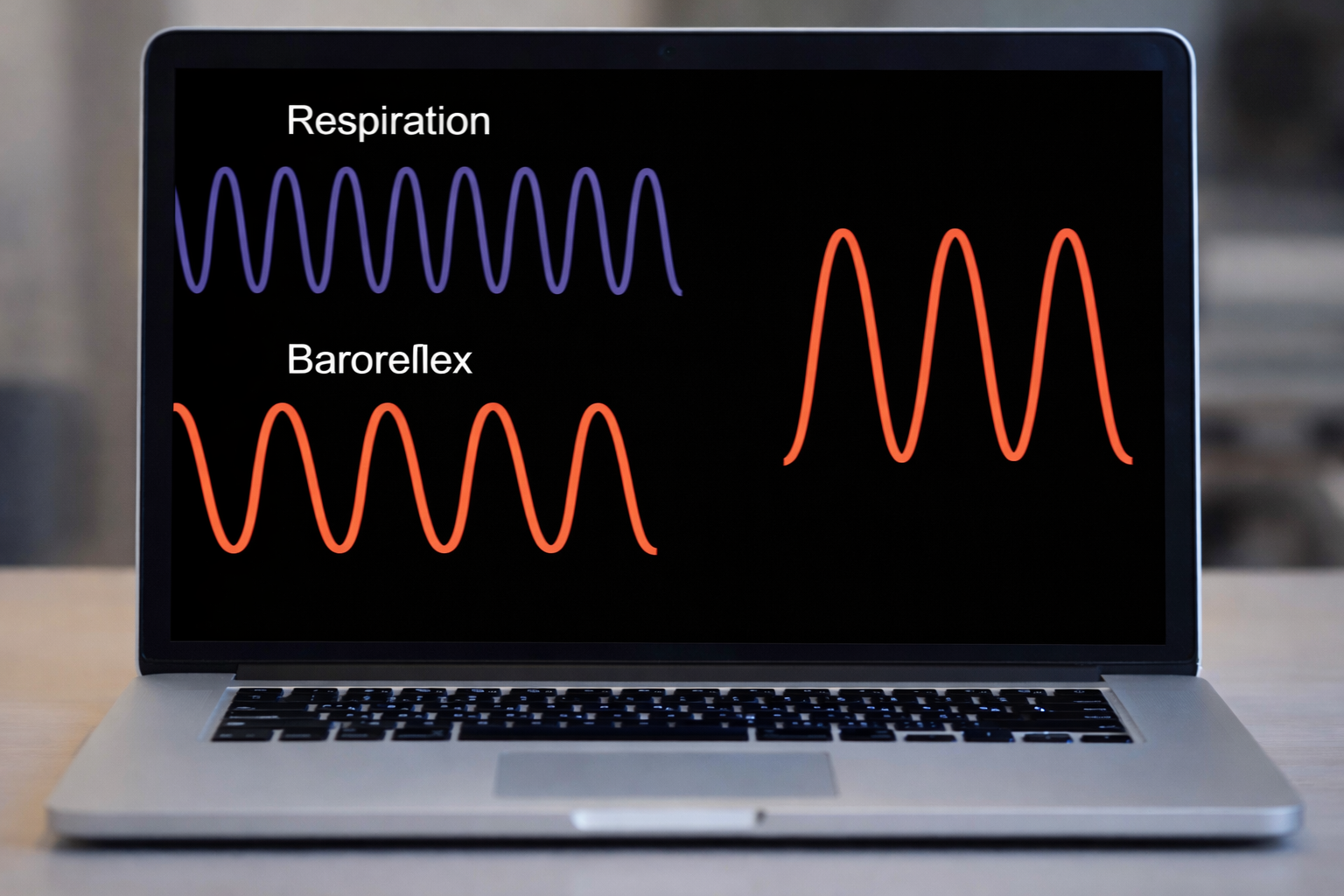
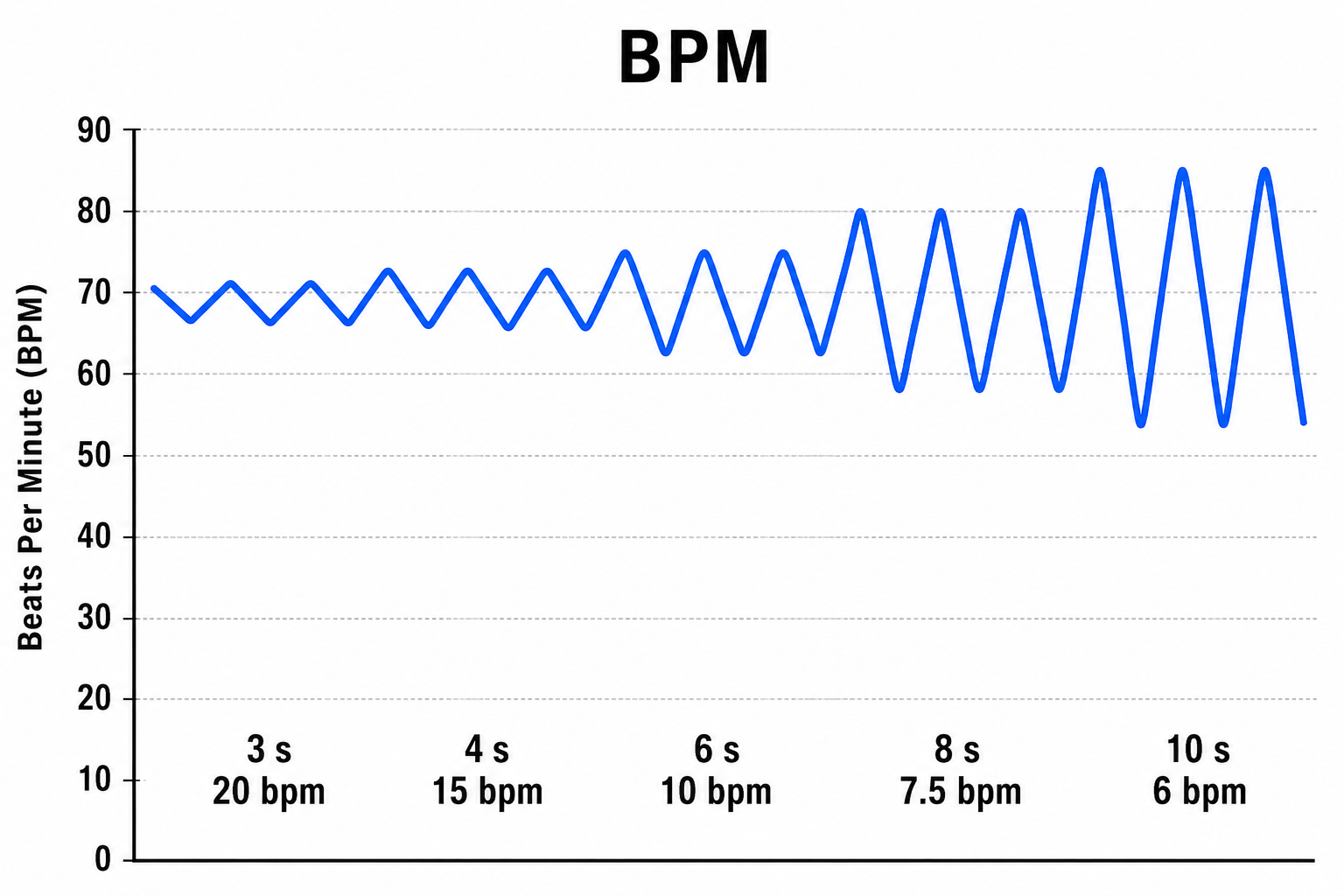
Mindful low-and-slow breathing amplifies RSA in a predictable way. The graphic below, adapted from Grossman and Kollai (1993), demonstrates that RSA (shown as the change in HR from inhalation to exhalation) increases as respiration rate approaches 6 bpm. This relationship explains why RF training is so powerful: it positions breathing at the rate that produces maximum HR oscillation.
Dr. Paul Lehrer provides an excellent introduction to these concepts in his resonance frequency breathing and heart rate variability biofeedback presentation from Breathe 2022.

A HRV Biofeedback Koan
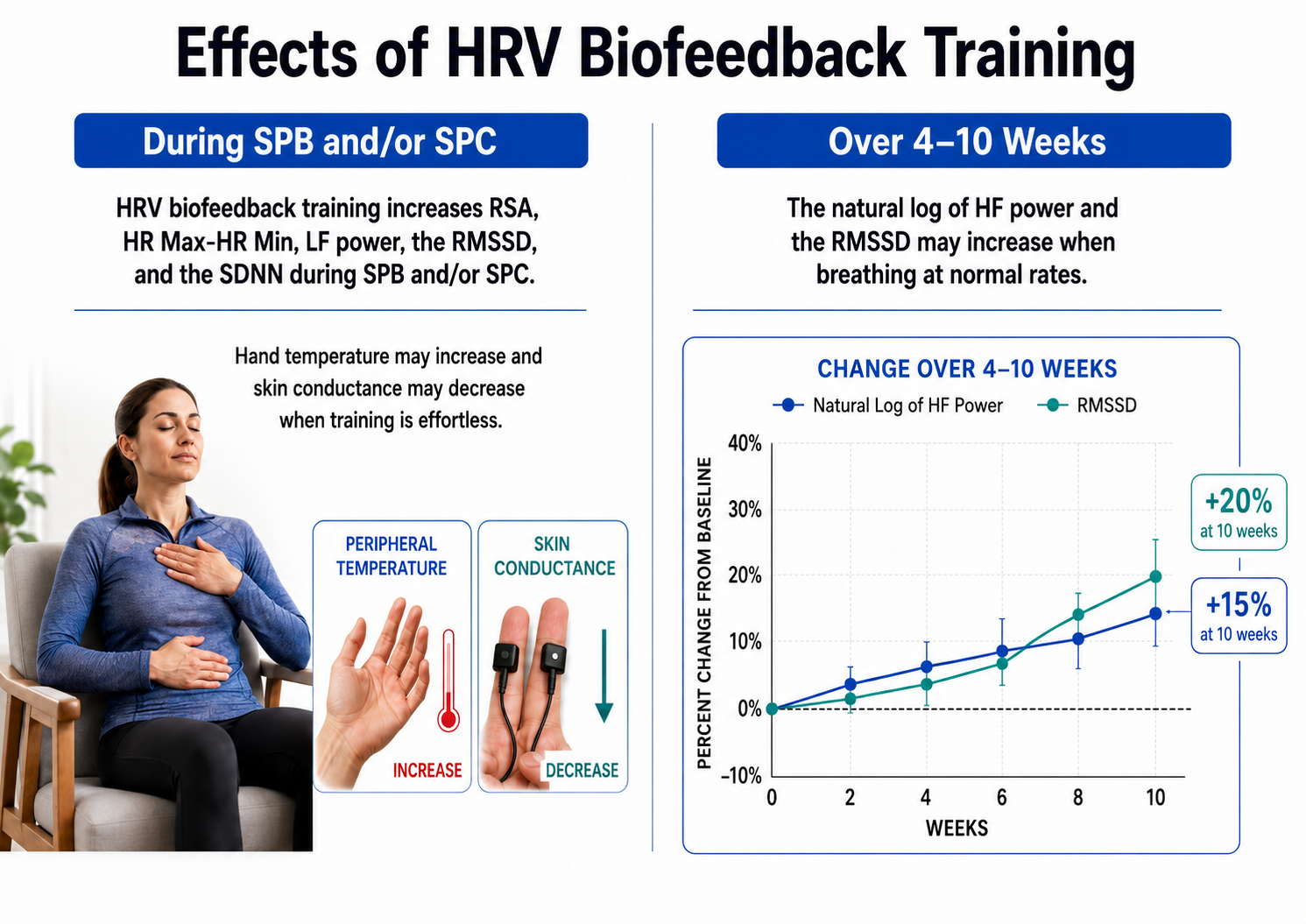
Here is a paradox that often confuses new clinicians: during SPB at resonance frequency, your client will show increased peak-to-trough HR differences, higher RMSSD, and elevated low-frequency (LF) power. However, the ultimate goal is not to increase LF power during training sessions. Instead, after weeks of practice, clients should demonstrate increased RMSSD and elevated high-frequency (HF) power when breathing at typical rates without feedback or pacing (Gevirtz, 2021).
Think of it this way: the training itself looks different from the outcome. Athletes lift heavy weights in the gym, but the goal is to perform better on the field without any weights at all. Similarly, HRVB clients breathe slowly with feedback to build cardiovascular fitness that transfers to everyday life without feedback or deliberate slow breathing.
BCIA Blueprint Coverage
This unit addresses V. HRV Biofeedback Strategies: A. How to explain HRV Biofeedback to a client, E. How to structure an HRV biofeedback training session, F. How to augment training with emotional regulation strategies, G. HRV biofeedback side effects and contraindications, and H. Practice assignments to promote generalization.
For deeper background, we encourage you to read Lehrer and Gevirtz's (2014) excellent Frontiers in Psychology overview, Heart rate variability: How and why does it work?
This unit covers Medical Cautions, Clinical Tips When You Start HRV Biofeedback Training, HRV Biofeedback Training, and Practice Assignments.
🎧 Listen to the Full Chapter Lecture
Medical Cautions
Before beginning HRVB training, clinicians must screen for cardiac abnormalities and compensatory overbreathing that could compromise patient safety. This screening is not optional; it is a fundamental part of responsible practice.
Conduction Abnormalities
Examine ECG morphology for evidence of arrhythmias, ischemia, and prolonged QT intervals (Drew et al., 2004). When abnormalities appear, encourage clients to consult with their physicians before proceeding. Training should only continue if the physician considers it appropriate.Screening for arrhythmias should inform your data cleaning and interpretation of HRV metrics. Providers must take special care in analyzing contaminated epochs, discarding them in extreme cases. Arrhythmias that cause software to miss beats or calculate extra beats will distort HRV metrics, especially wearable apps that perform limited or no artifacting.
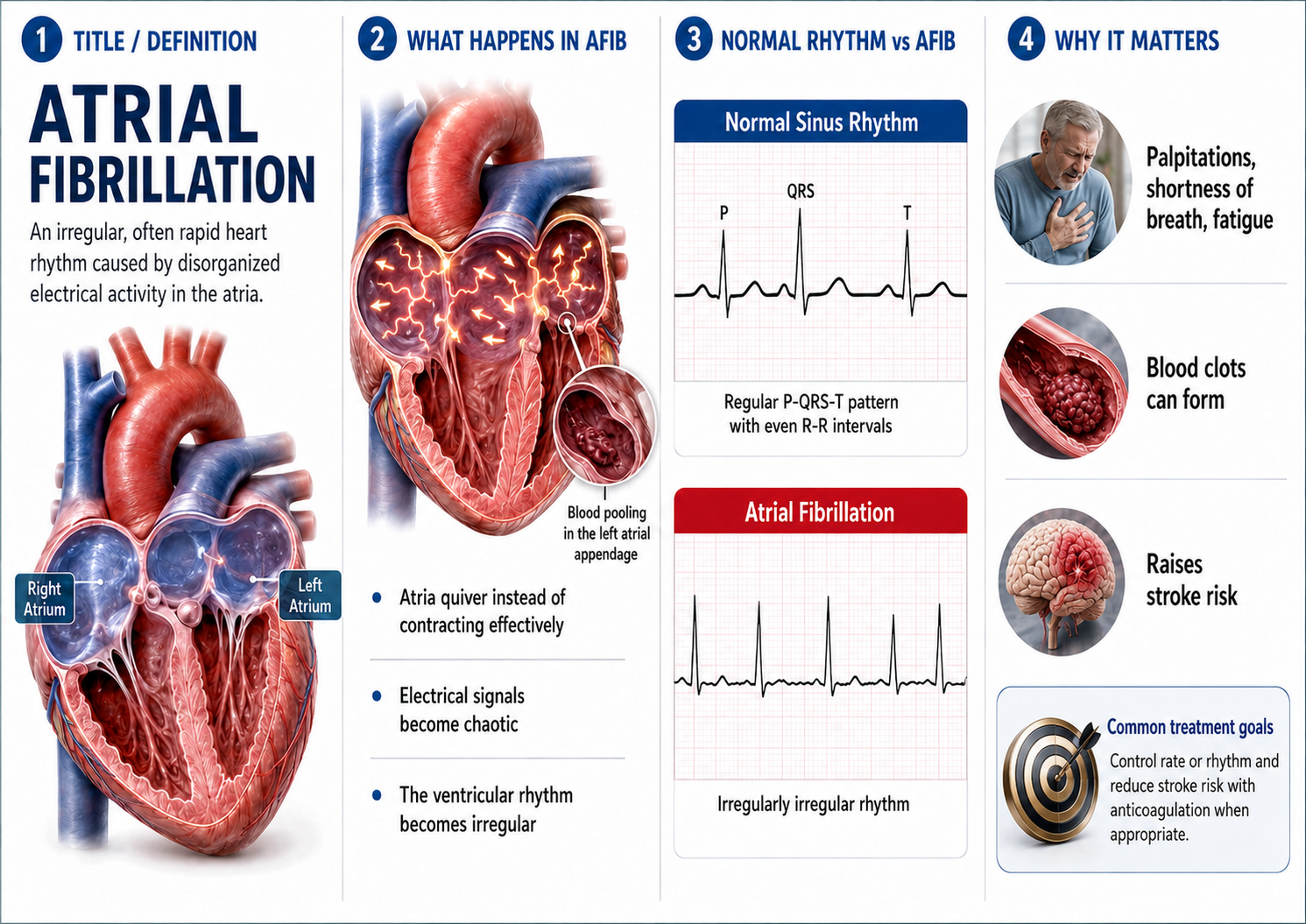
Atrial fibrillation, the most common cardiac arrhythmia, involves rapid and irregular contraction of the two upper atrial chambers. On the ECG, you will see an absence of distinct P waves and an irregularly irregular ventricular response. Clients with atrial fibrillation present unique challenges for HRV measurement because the arrhythmia itself produces extreme variability unrelated to autonomic function.
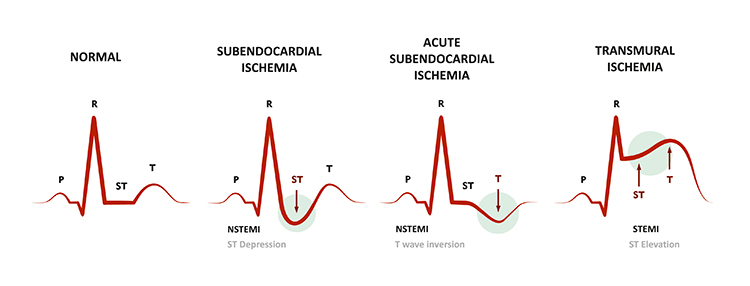
Ischemia, insufficient blood supply to cardiac tissue, produces characteristic depression of the ST segment on the ECG. The ST segment represents the period between ventricular depolarization and repolarization. Compare the normal ST segment in the left panel with the depressed segment indicating subendocardial ischemia in the right panel. If you observe ST depression during a training session, stop immediately and refer the client for medical evaluation.
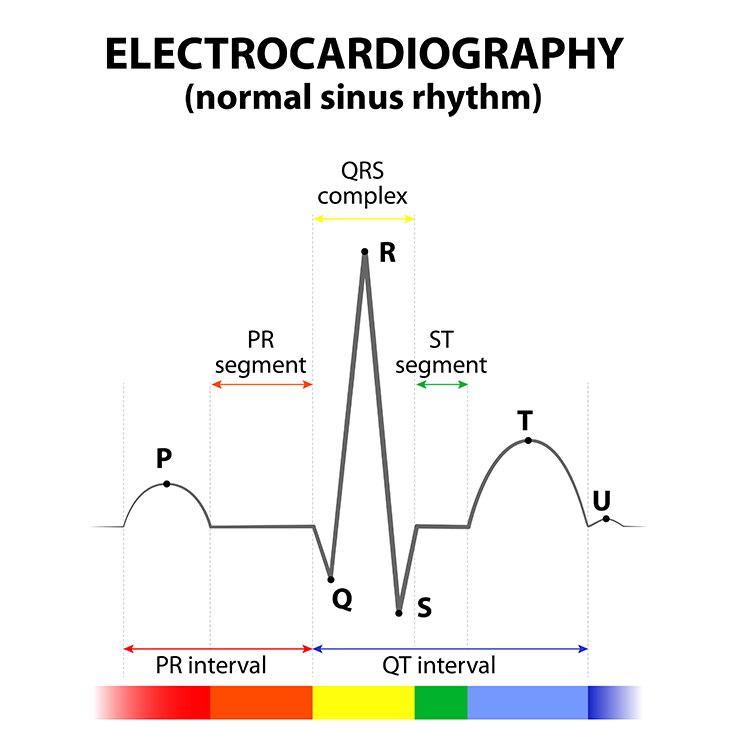
The QT interval signals the depolarization and repolarization of the ventricles. This interval, measured from the beginning of the Q wave to the end of the T wave, reflects the total time required for the ventricles to complete one electrical cycle.
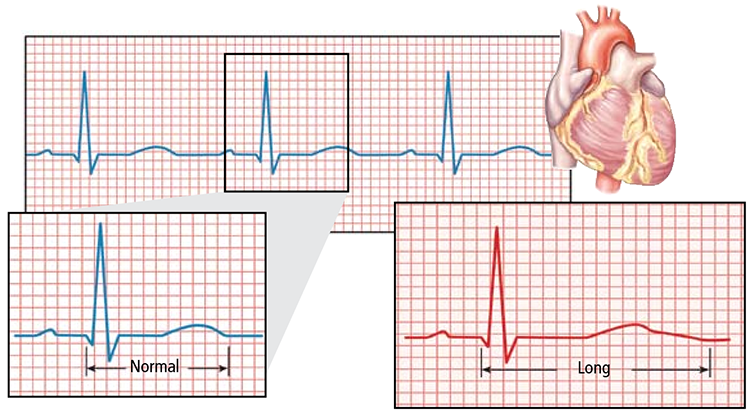
A prolonged QT interval carries significant clinical risk. This finding is associated with increased vulnerability to ventricular tachyarrhythmias, which can result in cardiac arrest and sudden death. Certain medications, electrolyte imbalances, and genetic conditions can cause QT prolongation. If you identify a prolonged QT interval, the client must be evaluated by a cardiologist before any biofeedback training that affects autonomic tone.
Compensatory Overbreathing
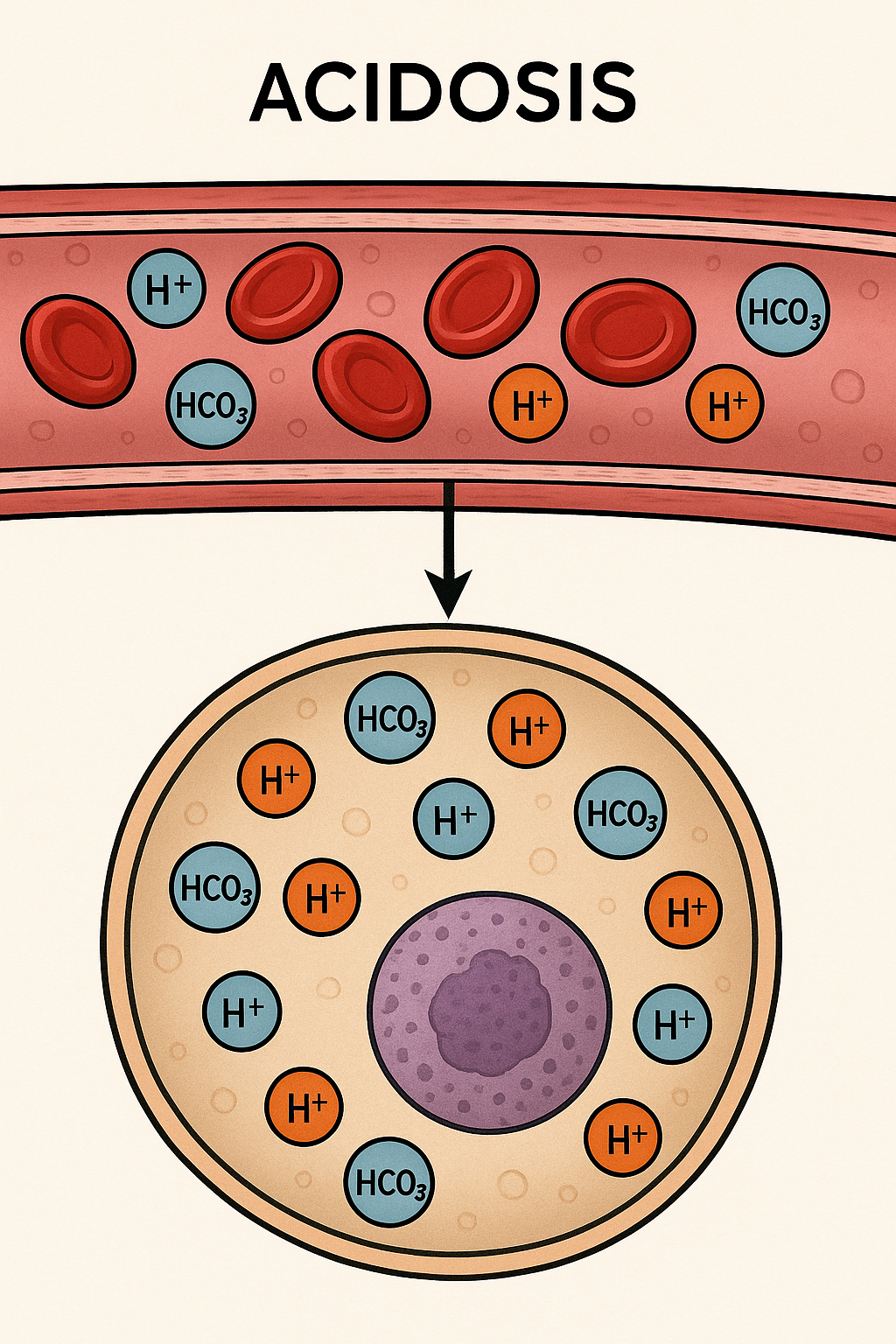
SPB may be medically contraindicated when altered breathing patterns could be hazardous for clients suffering from diabetes (Kitabchi et al., 2009) or kidney disease (Kim et al., 2021) that produce metabolic acidosis, excess acid in the body fluid. In these conditions, the body relies on specific respiratory patterns to maintain acid-base balance, making interventions that alter breathing potentially dangerous to the client's physiological homeostasis.
Respiratory Acidosis
Common respiratory acidosis causes include chronic obstructive pulmonary disease (COPD), asthma, pneumonia, and neuromuscular disorders that affect breathing muscles. These conditions impair the lungs' ability to eliminate carbon dioxide effectively, leading to respiratory acidosis. Interventions that further alter breathing patterns could exacerbate these underlying physiological imbalances.

Patients may breathe rapidly to protect acid-base balance in medical disorders that cause a decrease in blood pH, leading to acidosis. Rapid breathing helps to expel carbon dioxide (CO2) from the body, which in turn can increase the pH and counteract the acidosis.
Clinical Tips When You Start HRV Biofeedback Training
Successful HRVB training depends on numerous clinical elements working in concert. These include modeling appropriate breathing and emotional states, building a strong therapeutic relationship, cultivating passive volition, selecting appropriate monitoring equipment and displays, teaching alternatives like slow-paced contraction, detecting and addressing excessive effort, using engaging games and apps, implementing effective pacing strategies, optimizing resting HR, and integrating emotional self-regulation techniques.
Modeling
Clinicians are always on stage. Your breathing pattern, posture, and emotional state communicate more than your words. Model low-and-slow breathing and rewarding emotions throughout each session. If you are anxious, rushed, or breathing rapidly, your client will unconsciously match your state. This phenomenon, known as physiological entrainment, works both for and against you. Use it intentionally by embodying the calm, rhythmic presence you want your client to develop.

Relationship
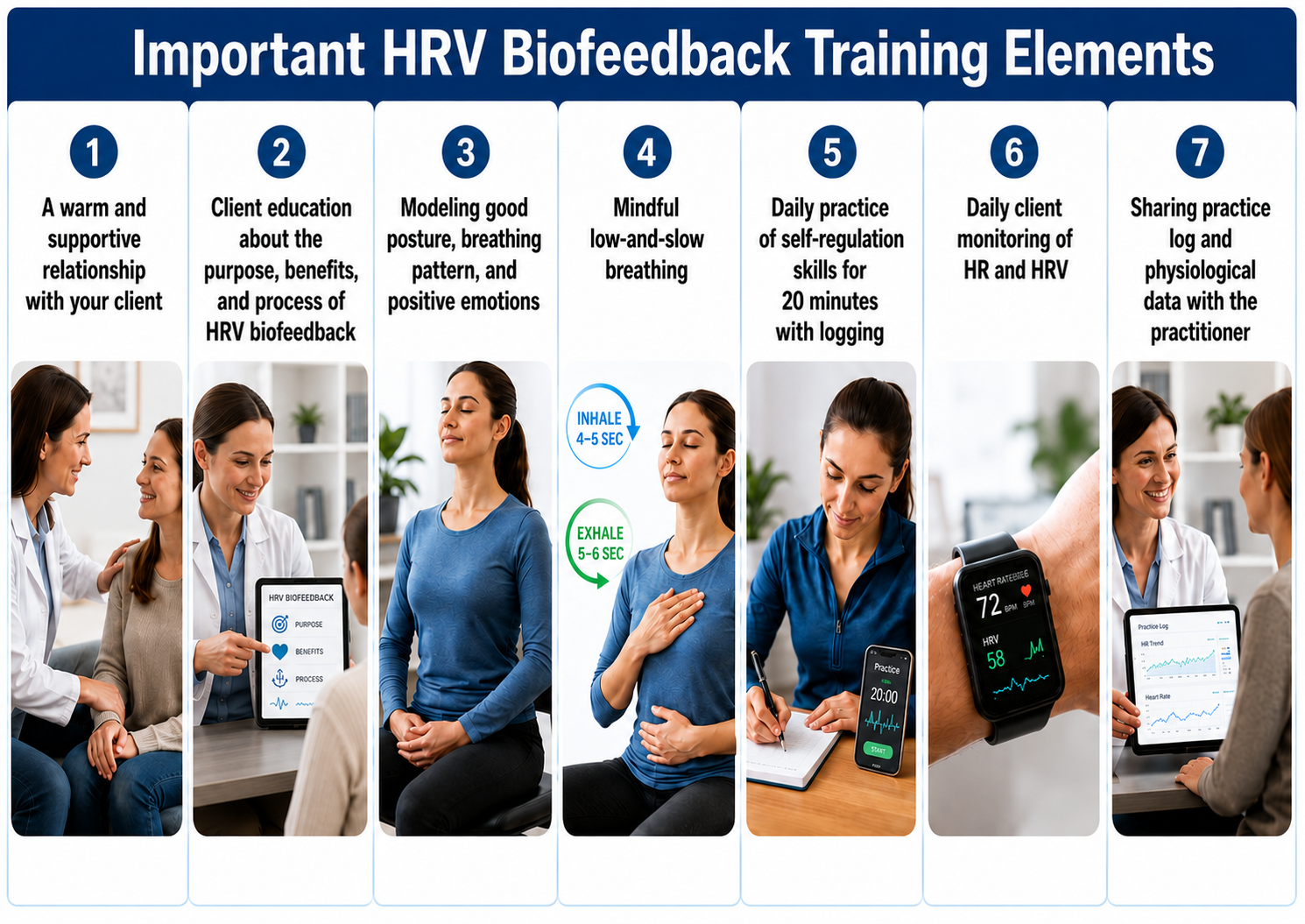
A warm and supportive relationship with your client is the foundation for successful biofeedback training (Taub & School, 1978). From a polyvagal theory perspective, the therapeutic relationship creates a neuroception of safety that enables the ventral vagal complex to come online. In plain language: clients cannot learn to activate their parasympathetic nervous system while feeling unsafe. Your relationship provides the secure base from which they can explore alternatives to fight-or-flight, freezing, or parasympathetic withdrawal.

Passive Volition
Encourage an attitude of passive volition, characterized by allowing rather than forcing, effortlessness rather than striving. Clients often describe this state as "my body breathing itself." This passive attitude is crucial because active effort triggers sympathetic nervous system (SNS) activation, which reduces vagal tone and promotes overbreathing. The harder clients try, the worse their results become. Help them understand that HRV biofeedback rewards letting go, not pushing harder.

Monitoring HRV
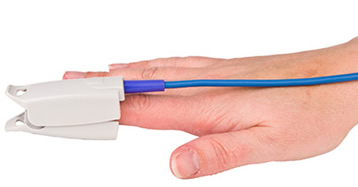
Your choice of sensor affects both accuracy and client comfort. For clinical work, consider an ECG sensor with wrist placement or a photoplethysmograph (PPG) sensor on an earlobe or finger. PPG sensors, which measure blood volume changes optically, trade some accuracy for ease of application. This tradeoff is acceptable for most clinical training.
However, certain conditions require ECG monitoring. When significant vasoconstriction occurs due to cold ambient temperature, stress, or physical activity, PPG signals degrade substantially. Movement artifacts also affect PPG more than ECG. If your client will be standing, moving, or training in challenging conditions, ECG provides more reliable data (Constant et al., 1999; Hemon & Phillips, 2016; Jan et al., 2019; Medeiros et al., 2011).

Selecting an Effective Display
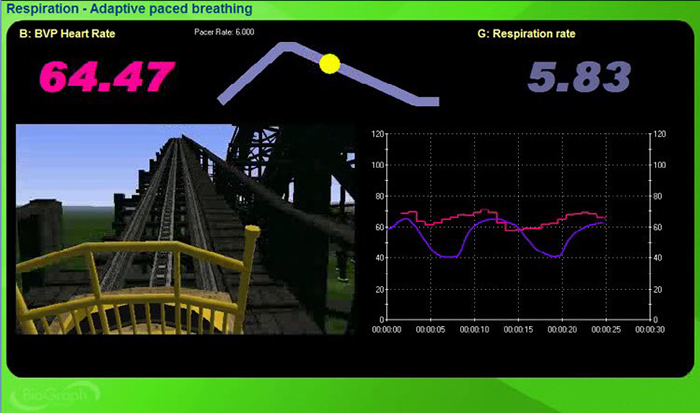
The feedback display shapes what clients learn. Provide an HRV training screen showing both respirometer and instantaneous HR waveforms. Analog displays convey incredibly detailed and intuitive information that digital numbers cannot match. Encourage your client to focus on increasing peak-to-trough swings in HR during each breathing cycle (Lehrer et al., 2013; Lehrer & Gevirtz, 2014). When they see their HR rise with inhalation and fall with exhalation, the abstract concept of RSA becomes viscerally real.
While client preference and success should guide your selection, consider starting with feedback of LF power and peak-to-trough differences. These metrics respond quickly to breathing changes and provide clear, motivating feedback.
Dr. Inna Khazan demonstrates how slow-paced and normal breathing change low- and high-frequency power in this video. Notice how the spectral distribution shifts dramatically when breathing slows to resonance frequency.
The BioGraph Infiniti screen shown below is designed to increase the percentage of power in the LF band. This three-dimensional display shows the dynamic change in HRV amplitude distribution as a client breathes effortlessly and cultivates positive emotion. Watching power concentrate at 0.1 Hz provides compelling feedback that motivates continued practice.
Some clients prefer displays showing synchrony, the alignment of peaks and troughs between respirometer and instantaneous HR signals. Synchrony matters because it amplifies the resonance effects of SPB (Vaschillo et al., 2002). When respiration and HR oscillate together in phase, the baroreceptor reflex receives maximum stimulation. The NeXus-10 BioTrace+ screen below displays synchrony between respiration and HR. The flower opens as alignment increases, providing intuitive visual feedback.
Add Slow-Paced Contraction to Your Training Toolkit
Slow-paced contraction (SPC) offers an alternative pathway to resonance frequency stimulation. Some clients find SPB challenging, whether due to anxiety, chronic pain, respiratory conditions, or a lifetime of dysfunctional breathing. Others have medical contraindications for deliberate breathing modification, such as kidney disease with metabolic acidosis, where slowing respiration could dangerously alter the acid-base balance.
SPC may benefit clients who breathe dysfunctionally and cannot slow their breathing to the adult RF range of 4.5 to 6.5 bpm without significant distress. By focusing on muscle contraction rather than breathing, these clients can access resonance frequency benefits while their breathing naturally entrains to the rhythm.
In SPC exercises, clients briefly contract and relax skeletal muscles at the same 4.5 to 6.5 cycles per minute (cpm) rates used in breathing exercises while allowing their respiration to occur naturally. The muscles involved are the wrists and ankles, or wrists, core, and ankles together.
Hypothesized Mechanism
Like SPB, SPC generates large HR oscillations and stimulates the baroreceptor reflex to increase HRV. The hypothesized mechanism, a muscle pump that increases venous return and stroke volume to produce arterial pressure fluctuations differs, but the outcome is equivalent. Although the muscle pump increases HR oscillations, these changes are not RSA because they are driven by wrist-core-and-ankle contraction instead of breathing.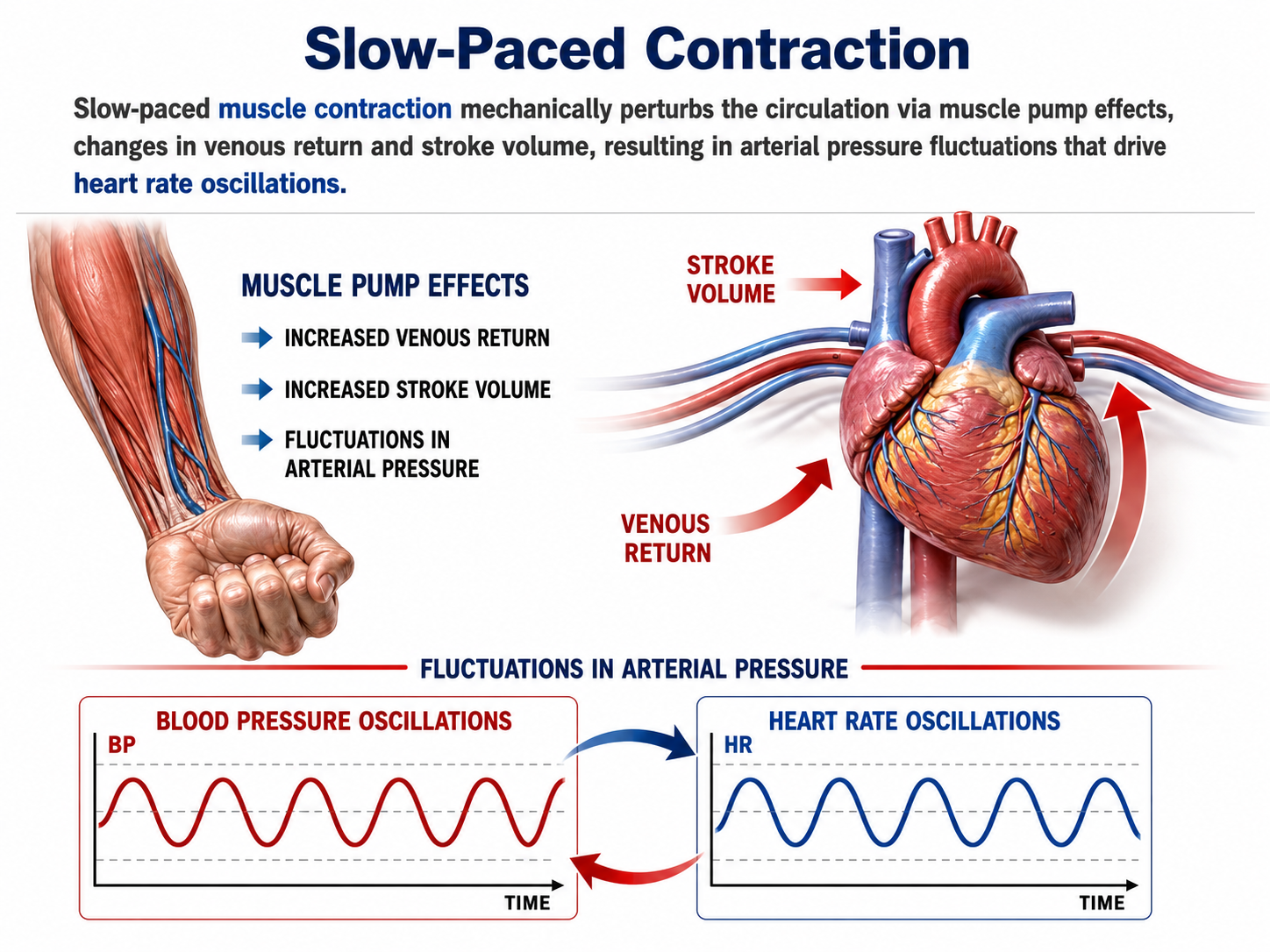
HRV Sensors
Choose an ECG sensor, like Thought Technology Ltd.'s EKG-Flex/Pro.
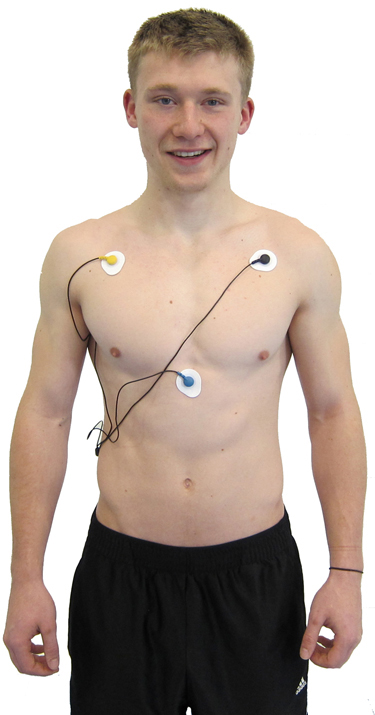
A lower torso placement preserves client modesty and reduces EMG contamination of the ECG signal.
.jpg)
You can place an Optimal HRV Reader, which uses a PPG sensor, on your client’s arm.

You may also use a PPG earlobe sensor like the Institute of HeartMath's Inner Balance.

EMG Sensor
Place an EMG sensor like Thought Technology Ltd.'s Myoscan over the forearm extensors and flexors to measure the rate of SPC.
Position
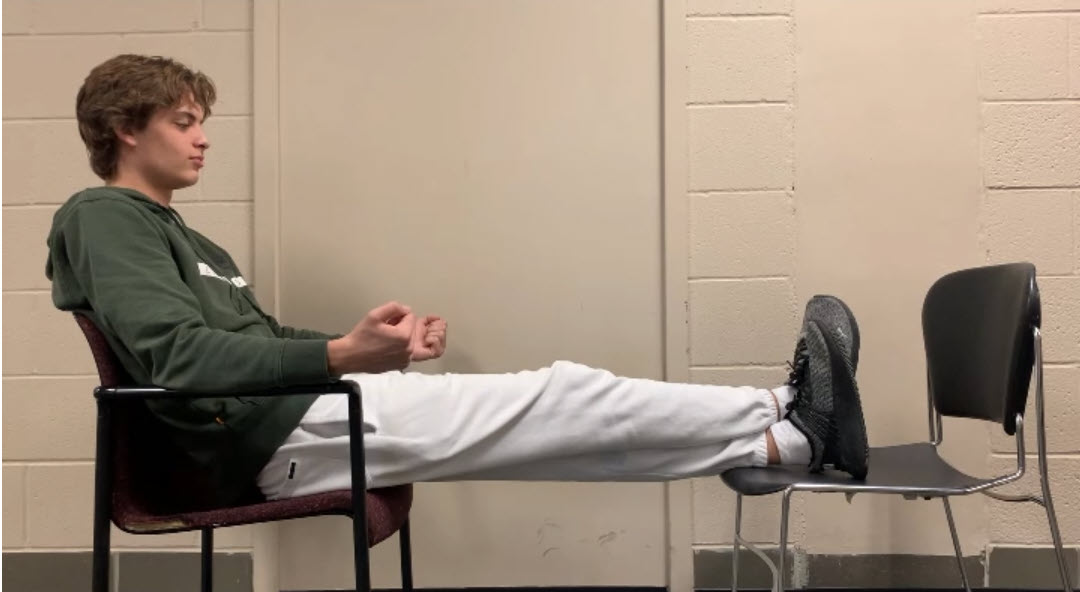
Clients should recline with their ankles crossed and feet supported by a footrest or separate chair. Although the original Vaschillo protocol only contracted the wrists and ankles with legs uncrossed, we have observed greater HR oscillations with wrist, core, and crossed-ankle contractions.
Muscle Contraction Mechanics
Instruct your clients to gently simultaneously contract their wrists, core, and ankles. If you are combining SPB with SPC, only contract the wrists and ankles. Your clients should use about 25% of their maximum effort. They should feel as if their muscles are contracting themselves, rather than their forcing the movement.

Contraction and Relaxation
They can hold each gentle contraction for 3 seconds.
Display
We repurposed this BioGraph Infiniti display for SPC training. Clients start contracting their muscles 1.5 s before and end 1.5 s after each cycle's peak. We use the verbal prompt, "contract," to reinforce the visual display.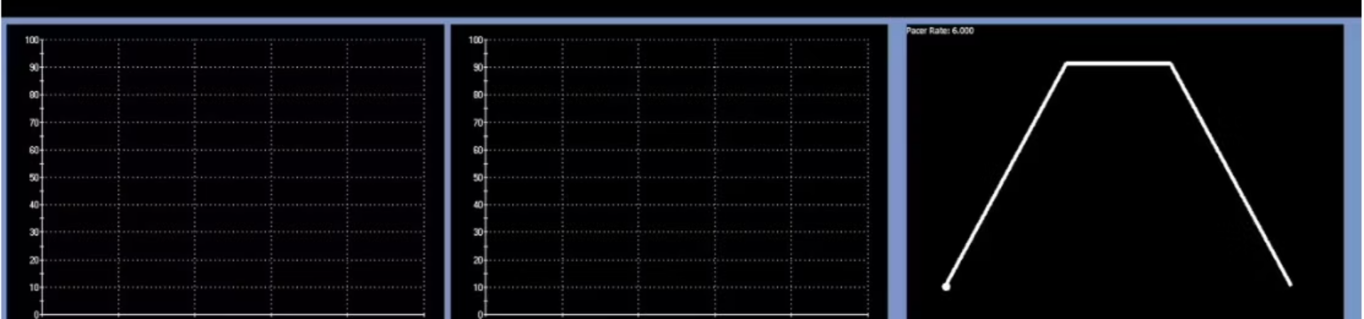
The video below demonstrates 6-cpm SPC. Observe the recruitment of core muscles, including the rectus abdominis, during the contraction phase.
This second video shows 6-cpm SPC with an interesting finding: the model was not given breathing instructions, yet the SPC naturally entrained breathing rhythm. This entrainment effect makes SPC particularly valuable for clients who struggle with deliberate breath control.
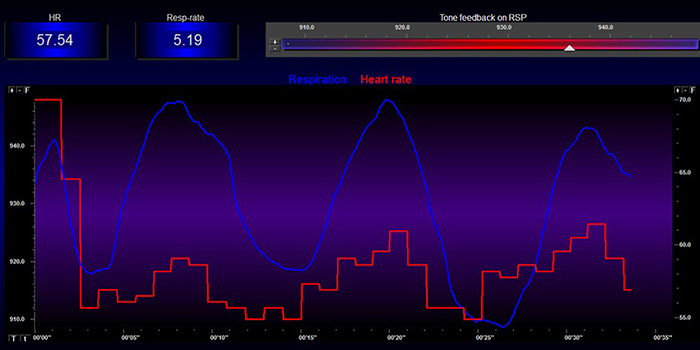
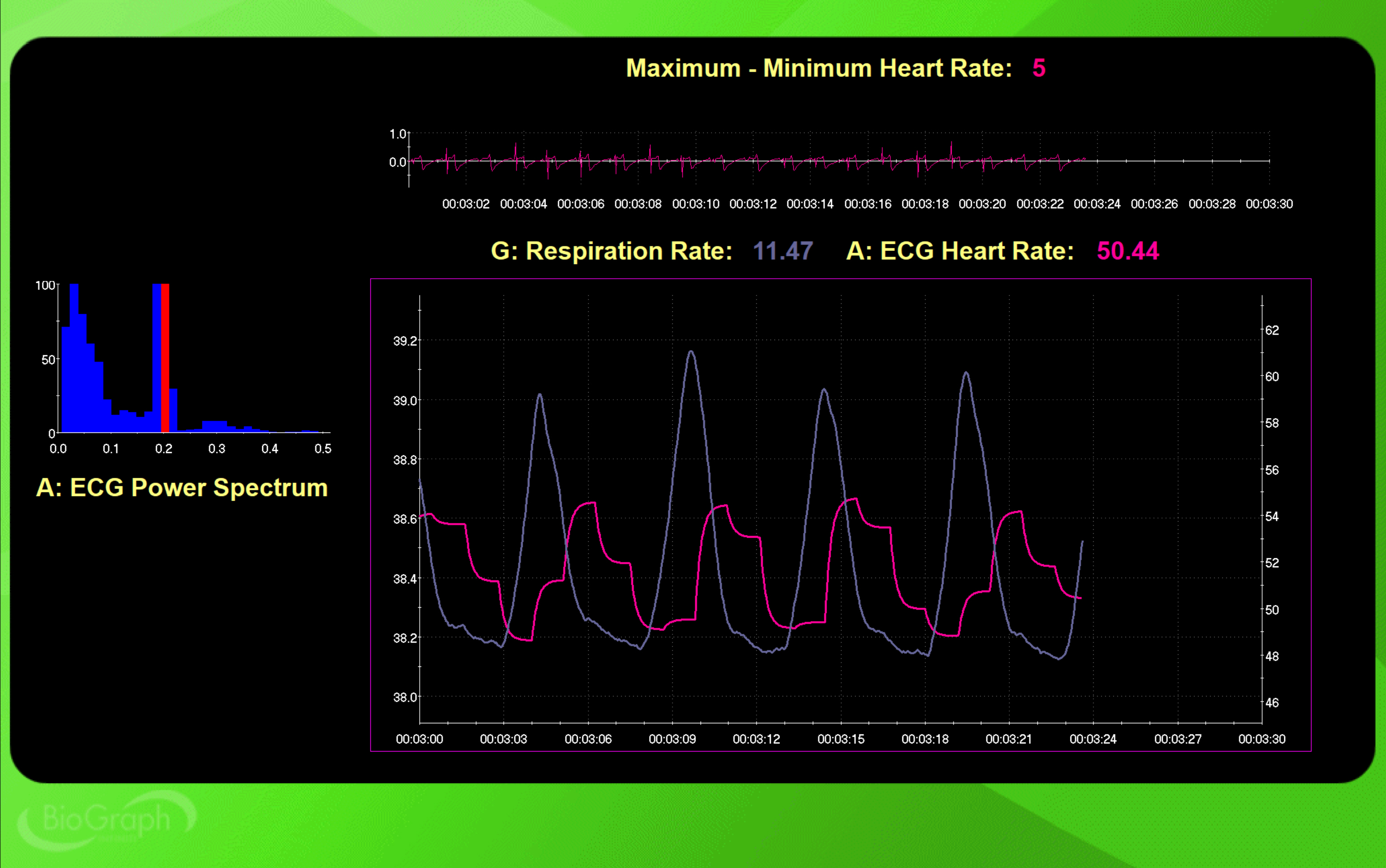
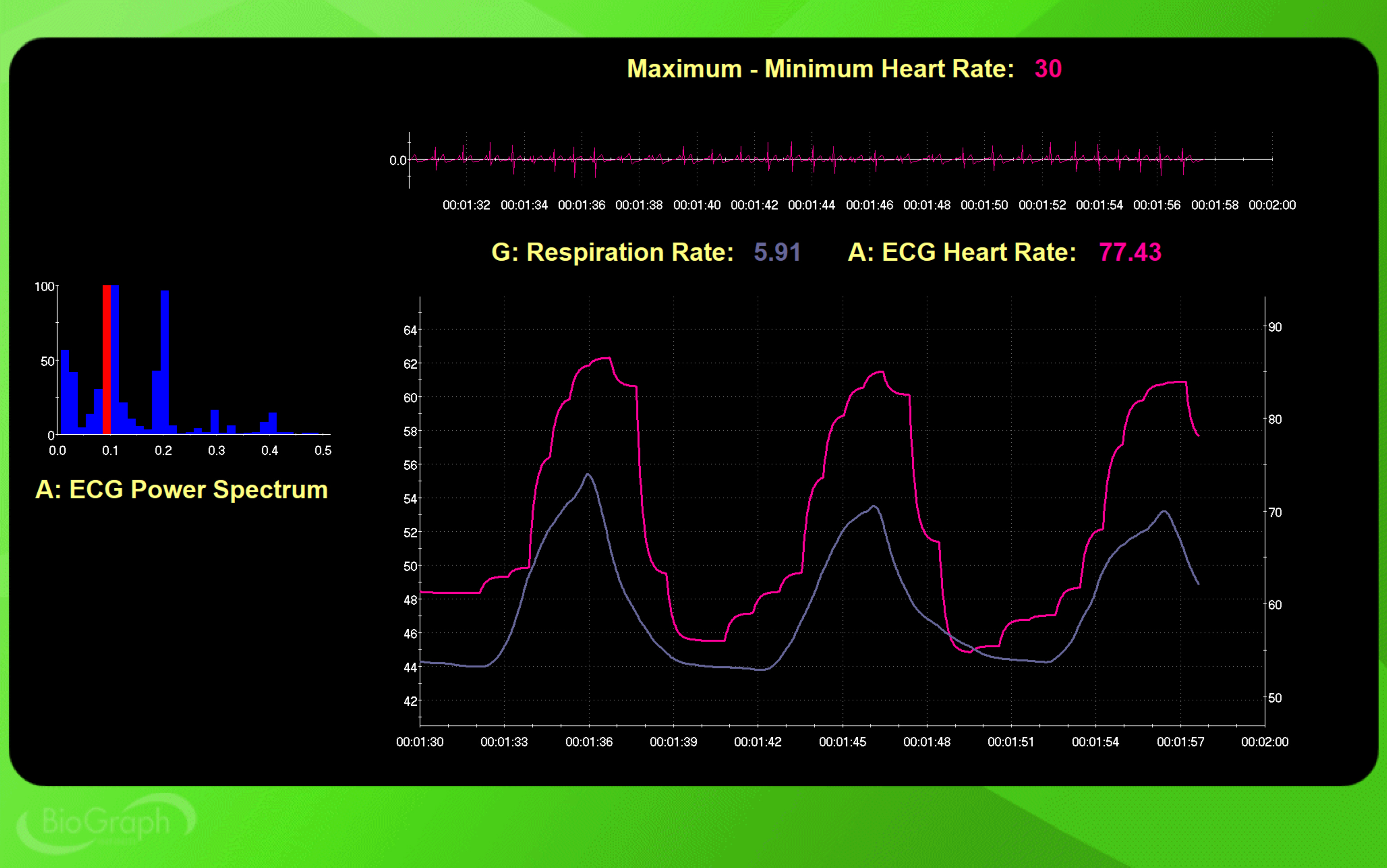
Maximum-Minimum HR for each cycle indexes HRV. The peak frequency indicates the HRV frequency with greatest power. In the screen captures below, SPC stimulated the baroreceptor reflex at the intended frequency: 0.2 Hz for 12 cpm and 0.1 Hz for 6 cpm.
This BioGraph Infiniti display shows 12-cpm SPC. At the top right, the Maximum-Minimum HR for each cycle is 5 bpm. At the left, the peak frequency is 0.2 Hz, exactly as expected from the 12-cpm rate.
Compare this to 6-cpm SPC. The Maximum-Minimum HR for each cycle is now 30 bpm, six times greater than at 12 cpm. The peak frequency has shifted to 0.1 Hz. This dramatic increase in HR oscillations demonstrates why resonance frequency training is so powerful.
Combine Slow-Paced Breathing With Slow-Paced Contraction
Dr. Inna Khazan combines SPB with SPC when her clients struggle to learn SPB. SPC can serve as a powerful pacing cue for their breathing rhythm, and a model of the effortlessness we encourage. Matt Bennett, Optimal HRV co-founder, recommends combining SPB + SPC to increase HRV for clients who have mastered SPB. He finds that their HR Max - HR Min and low-frequency values are greater when they combine SPC with SPB. They can see improved results after training trials using the Optimal HRV application.Clinicians who treat Postural Orthostatic Tachycardia Syndrome (POTS), which is characterized by an excessive increase in heart rate and dizziness when standing, report that their clients have minimal HRV and require the combined approach to achieve clinical gains.
Muscle Contraction
When combining these techniques, limit contraction to the wrists and ankles to permit the abdomen to expand and the diaphragm to descend.Coordinating Breathing with Wrist-Ankle Contraction
Using the BioGraph Infiniti display for combined training, clients start gently inhaling as the pacing ball ascends and stop inhaling at the peak. They begin exhaling after the pause until the pacer reaches the bottom right portion of the display.
The easiest way to synchronize muscle contraction with breathing is to gently contract the wrists and ankles during inhalation and relax these muscles during exhalation. Alternately, clients can begin contracting their muscles 1.5 s before the peak and end 1.5 s after each cycle's peak. We use the verbal prompt, "contract," to reinforce the visual display. The video below demonstrates combined 6-cpm SPB and SPC.
Monitoring Excessive Effort
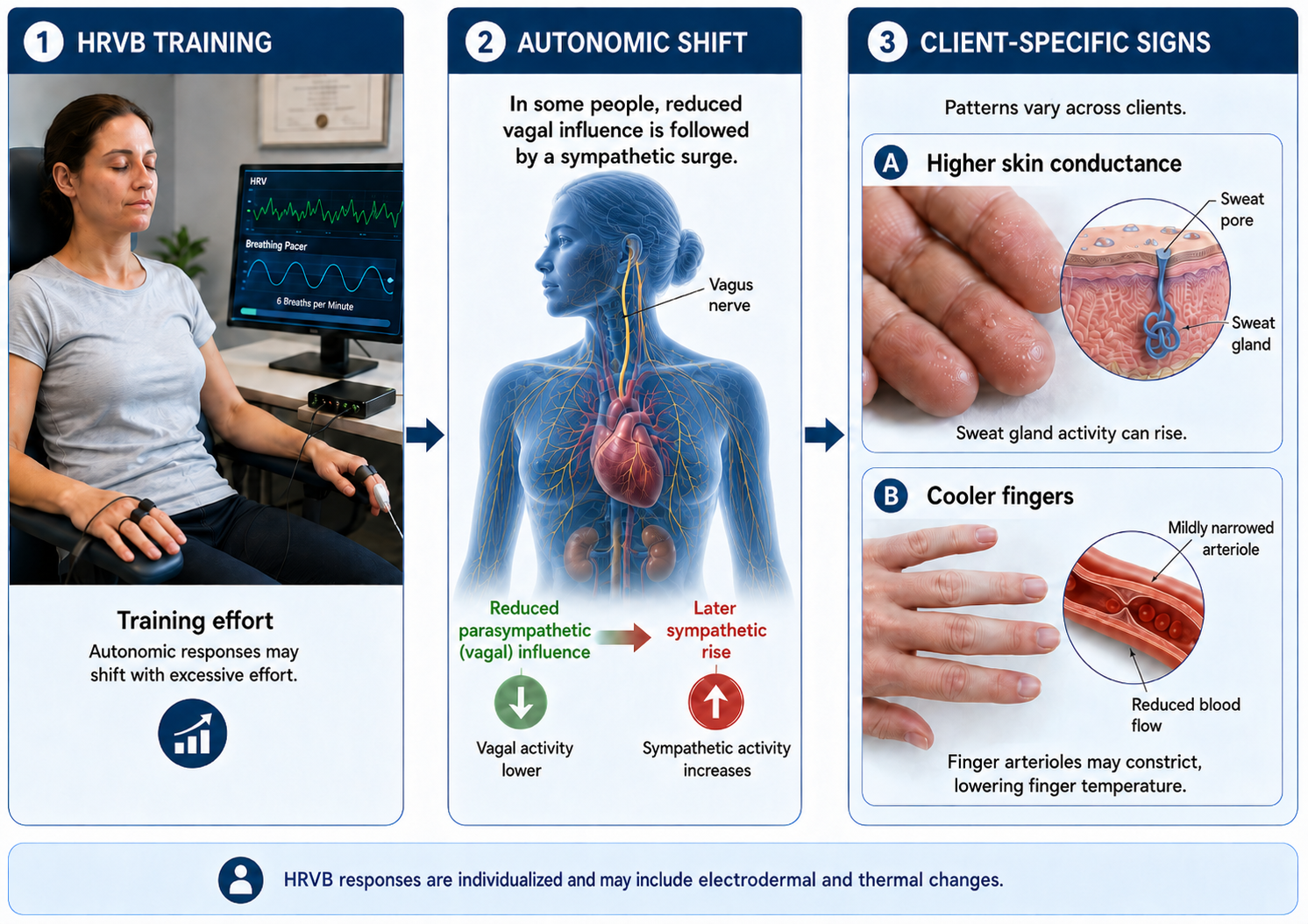
Excessive effort, or active volition, during HRVB training undermines the very goals clients are trying to achieve. When clients try too hard, they can produce vagal withdrawal, shown by increased very-low-frequency (VLF) power, increase SNS activation, indicated by increased HR and skin conductance (SC), and reduced finger temperature, and promote overbreathing which can expell too much CO2, measured by a capnometer. The paradox of biofeedback is that striving sabotages success. Your role as clinician is to detect effort early and redirect clients toward the passive, allowing attitude that produces optimal results.
Fortunately, effort leaves clear physiological signatures that you can monitor in real time. The primary excessive effort indicators are respirometer waveform irregularities, and changes in HR, VLF power, and HRV metrics like the RMSSD, and SC, temperature, accessory muscle SEMG activity, and capnometer readings.
Respirometer
Breathing effort disrupts the smooth, wavelike pattern that characterizes effortless respiration. Look for inflection points, sudden changes in the slope of the breathing waveform that indicate muscular forcing. A smooth sine wave suggests flow; a jagged waveform with sharp corners suggests struggle.

HR and HRV
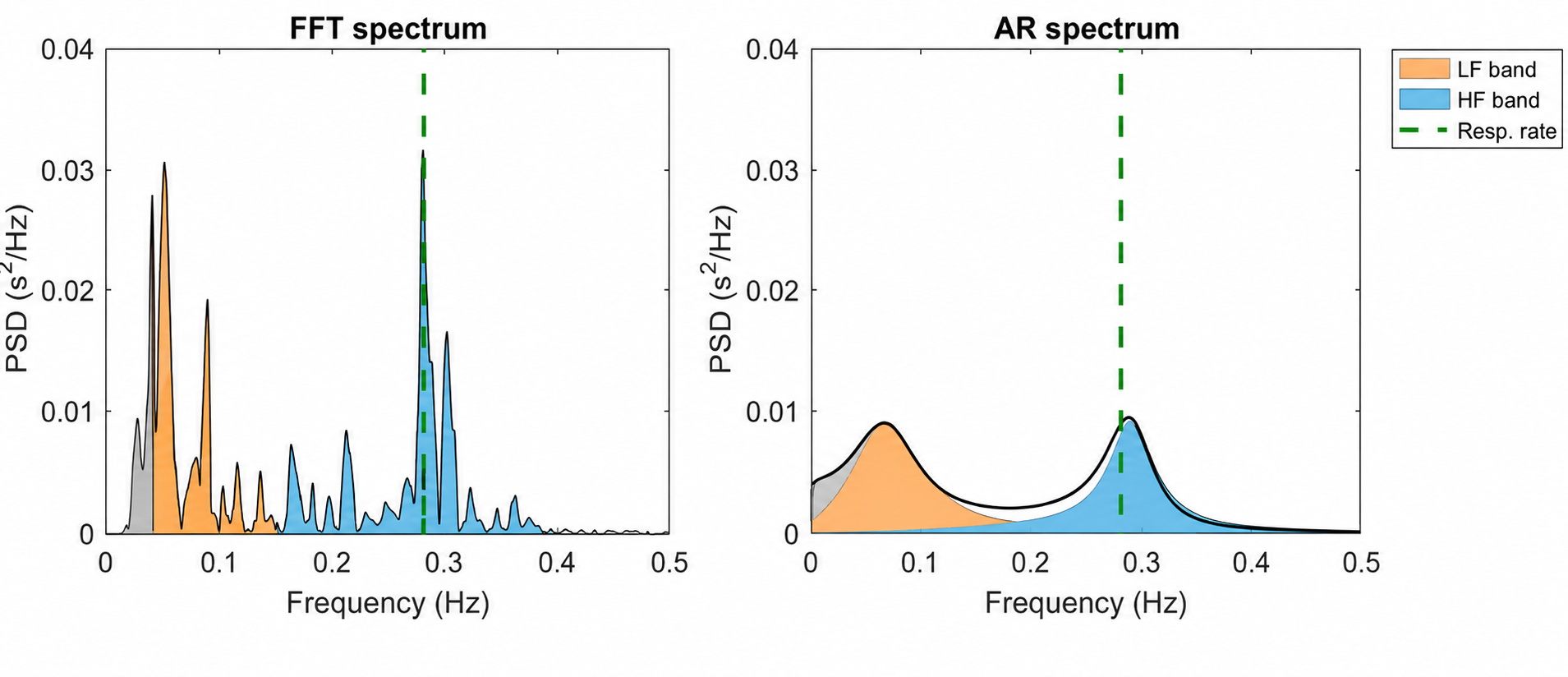
When training effort produces vagal withdrawal, a reduction of parasympathetic activity. HR may increase, time-domain metrics like the RMSSD may decrease, and VLF band power may rise. Do not confuse increased VLF power with sympathetic activation, which is too fast to contribute to this band. In the FFT spectral plot below, VLF power appears in gray. If you see rising VLF during training, consider whether your client is working too hard.
Skin Conductance and Finger Temperature
With sufficient HRVB training effort, sympathetic activation may follow vagal withdrawal. Depending on your client's unique response stereotypy, skin conductance may increase due to increased eccrine sweat gland activity and/or finger temperature may decrease due to arteriole constriction.
Accessory Muscle SEMG
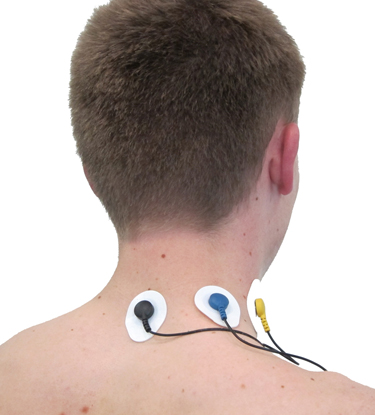
Surface electromyography can detect overuse of breathing accessory muscles, including the sternocleidomastoid, scalenes, pectoralis major and minor, serratus anterior, and latissimus dorsi. These muscles assist respiration during exercise or respiratory distress but should remain relatively quiet during relaxed diaphragmatic breathing. A trapezius-scalene placement, with active SEMG electrodes on the upper trapezius and scalene muscles, provides a window into respiratory effort. Activity above 2 microvolts during slow breathing suggests excessive effort.
This BioGraph Infiniti screen provides respiratory and SEMG biofeedback simultaneously, teaching rhythmic breathing while maintaining relaxed accessory muscles. Note the elevated SEMG activity during clavicular breathing, which relies heavily on accessory muscles rather than the diaphragm.
Capnometer
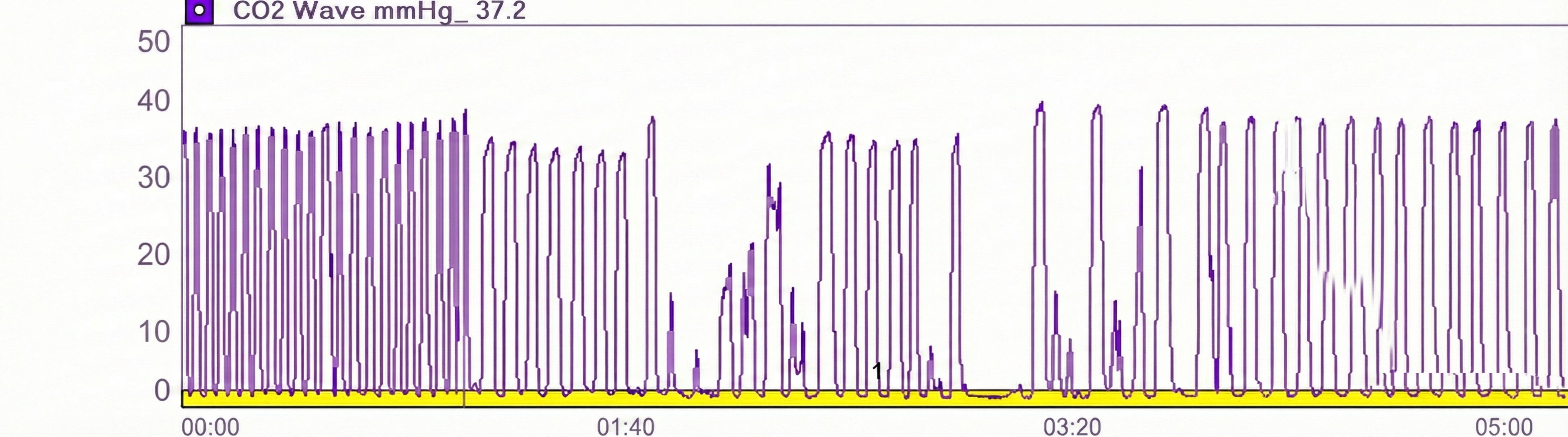
Excessive breathing effort that expels too much carbon dioxide decreases end-tidal CO2 readings. A capnometer monitors CO2 concentration in exhaled air by measuring infrared light absorption. When clients overbreathe, their end-tidal CO2 drops below the normal range of 35-45 mmHg (or torr, named after Torricelli, representing the unit of atmospheric pressure equal to 1 millimeter of mercury). In the tracing below, note the disrupted capnometer waveform after 1:40, indicating a period of overbreathing.
Engaging Games and Apps
Once your client has mastered SPB, games can transform practice from duty into pleasure. The gamification of HRV biofeedback serves two purposes: it motivates sustained practice and it tests the robustness of self-regulation skills under challenge. Biofeedback software allows clients to increase game difficulty progressively, developing the capacity to maintain regulation even when challenged. This graduated exposure is crucial for transferring skills to the unpredictable demands of everyday life.
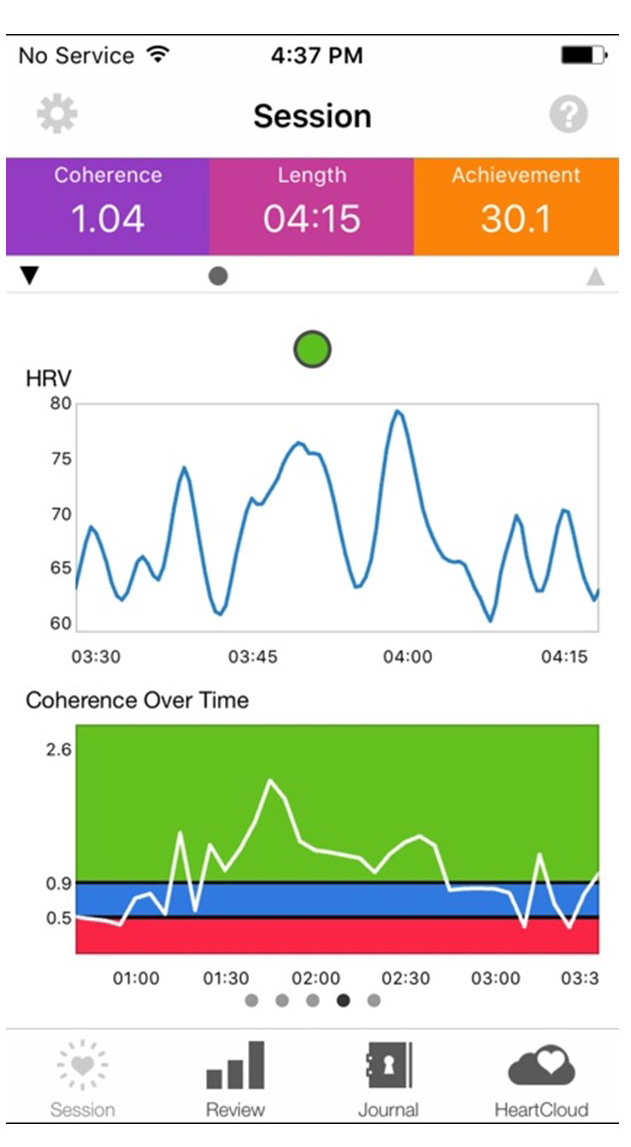
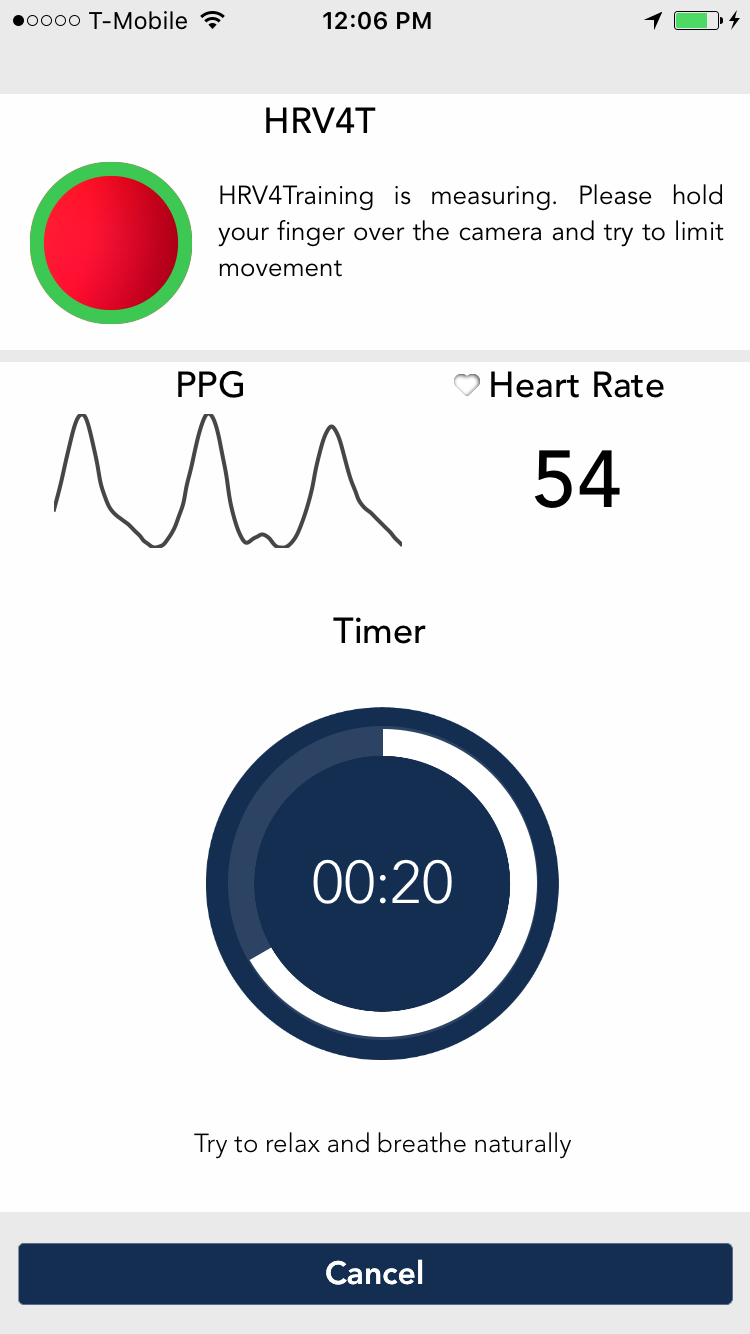
The market offers diverse options for HRV biofeedback games and apps. Professional software packages like Zukor's Drive and Zukor's Sport provide engaging visual feedback for clinic use. The HeartMath Garden Game and BioGraph Infiniti offer additional clinic-based options. For home practice, mobile apps including Inner Balance, Elite HRV, HRV4 Training, and Camera HRV enable convenient daily training.
 |
 |
 |
 |
 |
 |
 |
 |
Pacing Displays
Pacers guide breathing and slow-paced muscle tension using animation and sound. Software may integrate a pacer directly into an HRVB display or provide it as a standalone tool. The training strategy is straightforward: assign practice with breathing pacers initially, then gradually fade them as clients internalize the rhythm. The goal is autonomous self-regulation, not dependence on external pacing.
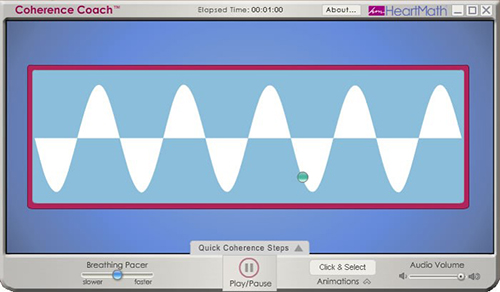
Computer, tablet, and smartphone apps offer various pacing options with different features. Try several to find apps that offer the adjustability and ease of use that best match your clients' needs. For computer-based pacing, Coherence Coach and EZ-Air Plus provide reliable options.
 |
 |
These mobile apps are available for both Android and Apple platforms, making practice accessible wherever clients go.
Auditory Pacing
Some clients prefer auditory rather than visual pacing, finding it easier to close their eyes and follow sound cues. The Alliant International University link provides downloadable auditory pacing resources at various breathing rates.
Stopwatch Pacer
For slow-paced contraction training, a simple stopwatch app that continuously loops can serve as an effective pacer. For 6 contractions per minute, select 10 seconds with no pause. Instruct your client to simultaneously contract their hands and feet for the first 3 seconds of each cycle, then relax for the remaining 7 seconds. This low-tech solution works surprisingly well.
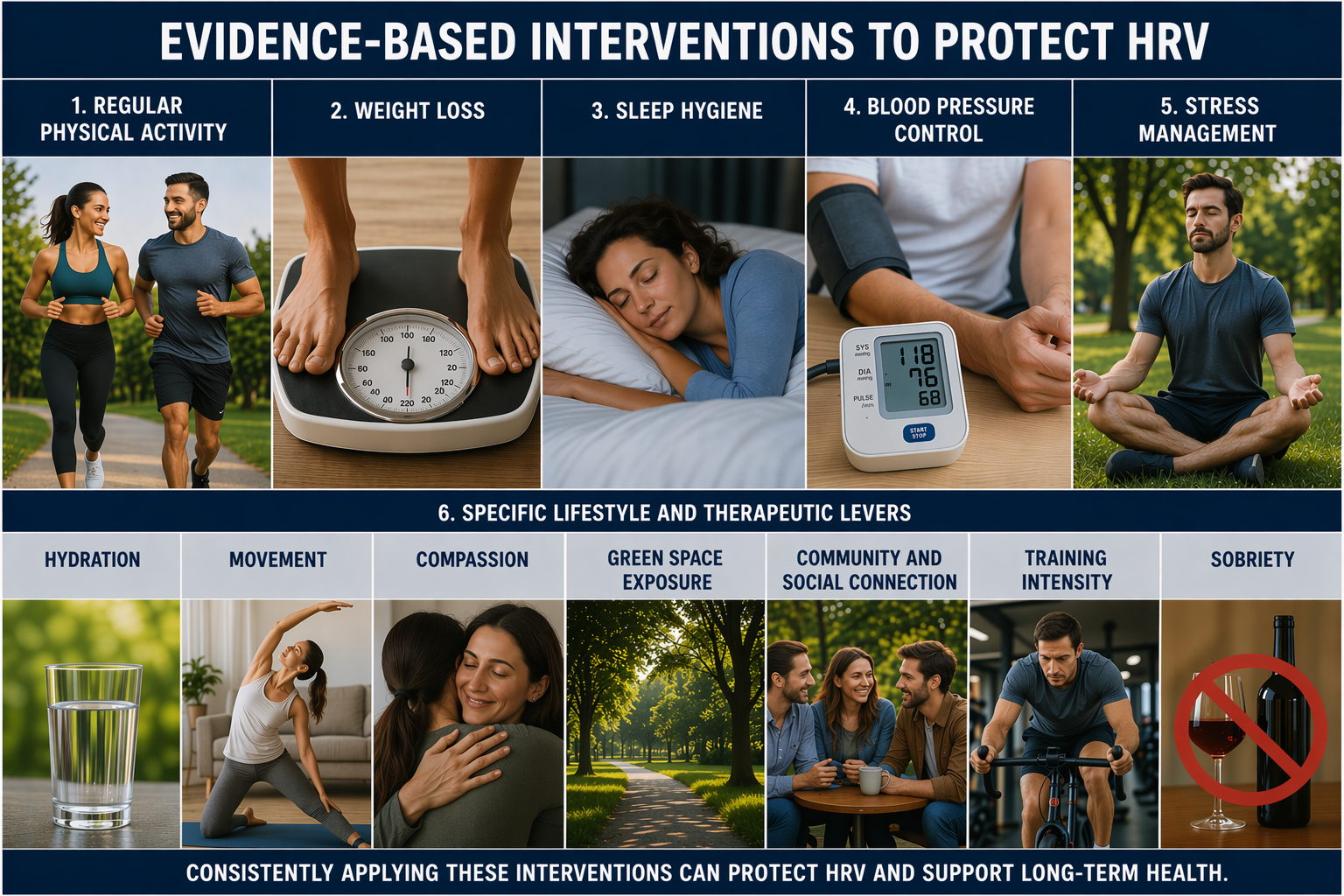
Lifestyle Choices
Unhealthy choices can erode HRV, while healthy ones help to preserve it. These are the levers you actually get to pull.
This section examines the daily behaviors and exposures that shape autonomic function, beginning with how clients move and what they carry. Physical activity stands out as the single behavior most reliably tied to better parasympathetic and global HRV, while weight loss and reduced sitting time each ease the sympathetic burden that suppresses vagal tone. Recovery matters just as much, so we examine how adequate sleep and proper hydration protect the autonomic gains that daytime habits set in motion.
From there we turn to the cardiovascular and psychological systems that HRV biofeedback already targets, considering how blood pressure reduction restores baroreflex sensitivity and how stress management lowers the allostatic load that erodes HRV over months and years. The remaining topics widen the frame to relationships, environment, and exposures, exploring how compassion practice trains the vagus, how time in green space and strong community and social connection support parasympathetic regulation, and how acute stressors such as alcohol, illness, and overtraining temporarily depress HRV. We close with drug effects on HRV, because a complete picture of any client's prescription and social drug use is essential for interpreting baseline and training values.
Physical Activity
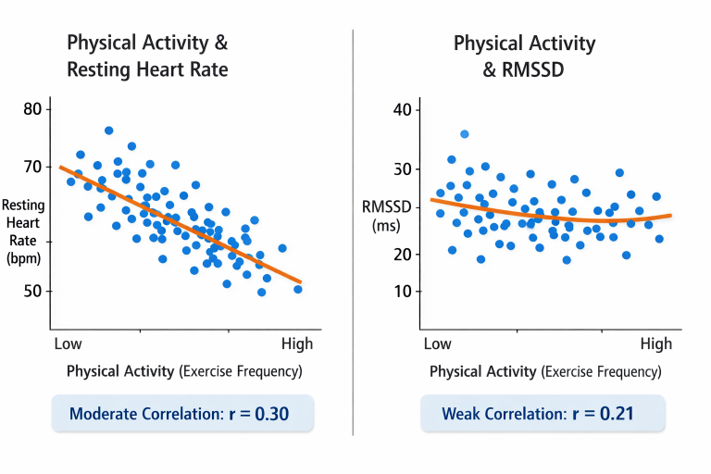
Physical activity is the only behavior that, when analyzed in isolation, was associated with better PNS and global HRV in adults (Saraiva et al., 2026).
At the population level, physical activity shows a moderate correlation with resting heart rate (r = 0.30) but only a weak correlation with the RMSSD (r = 0.21) (Altini & Plews, 2021). This is another reason not to judge your fitness by your RMSSD: it may not budge even when your cardiovascular fitness is clearly improving.
Weight Loss
Body mass index (BMI), which is weight divided by height squared, exerts a small but consistent influence on HRV. The obese category showed the highest resting heart rate (62 ± 8 bpm) and lowest RMSSD (56 ± 30 ms) compared to the normal-weight category (56 ± 8 bpm, 69 ± 35 ms; Altini & Plews, 2021).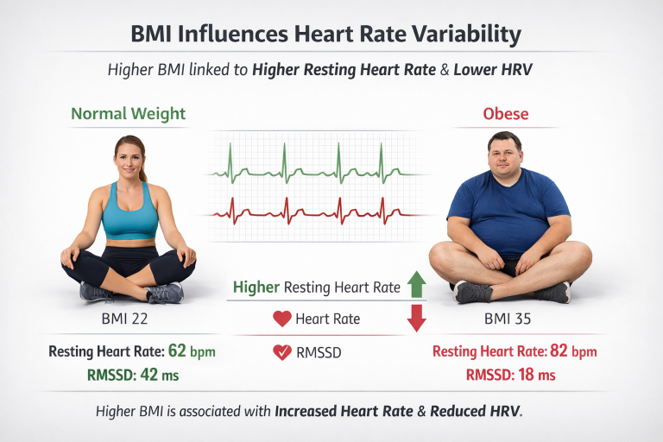
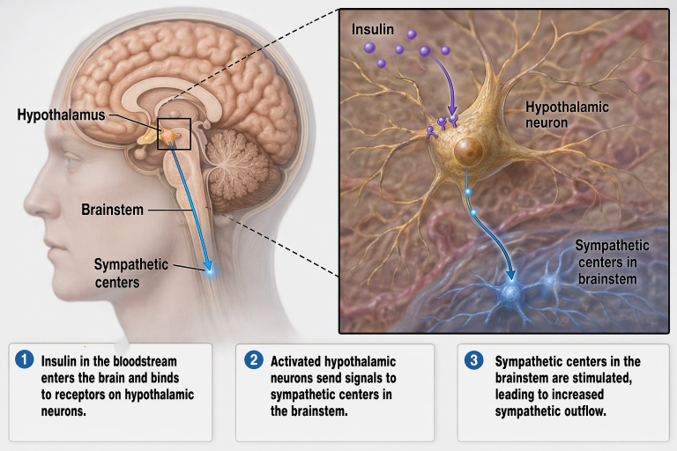
Obesity-related insulin resistance produces compensatory elevations in circulating insulin. Insulin acts directly on hypothalamic neurons to stimulate sympathetic centers in the brainstem (Guarino et al., 2017).
The good news: BMI is at least partially modifiable, and reductions in adiposity through lifestyle changes can restore the vagal brake and increase HF power and the RMSSD (Kalil & Haynes, 2012).

Sleep
The CDC’s sleep grades for 2024 have been released, and the marks are mixed at best (Ng et al., 2026). Nearly a third of adults, 30.5%, clocked fewer than seven hours of sleep in a typical 24-hour period, falling short of what the American Academy of Sleep Medicine recommends for healthy functioning.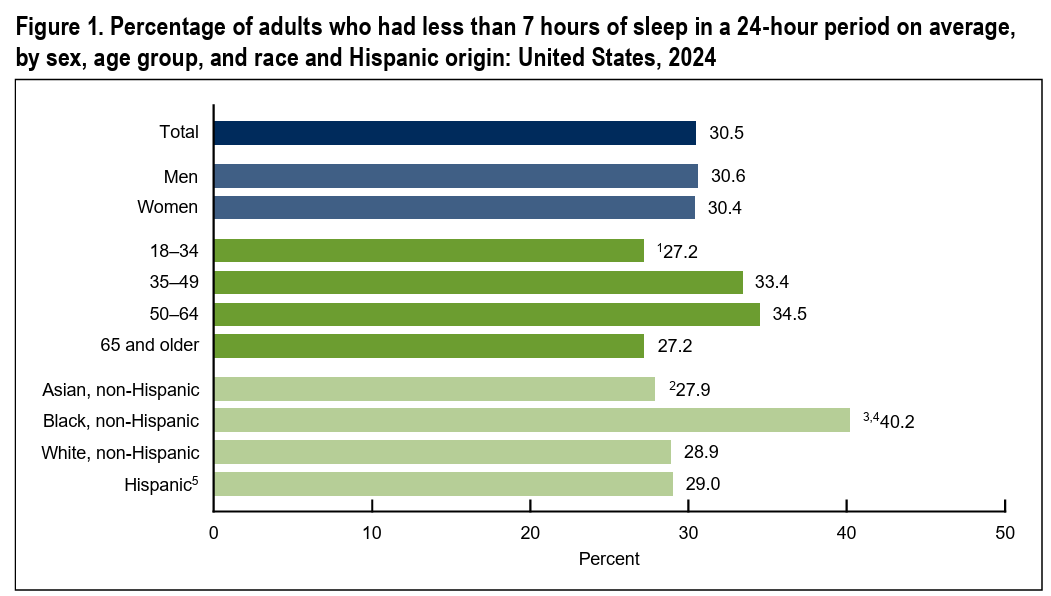
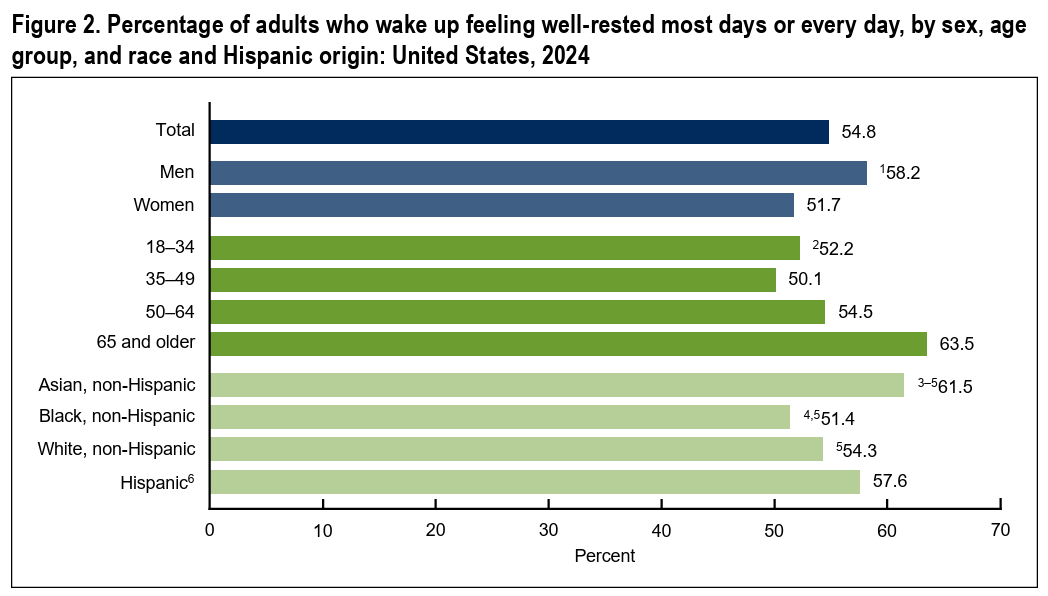
Just over half of adults (54.8%) actually woke up feeling well-rested most days, meaning the other half started their mornings already behind.
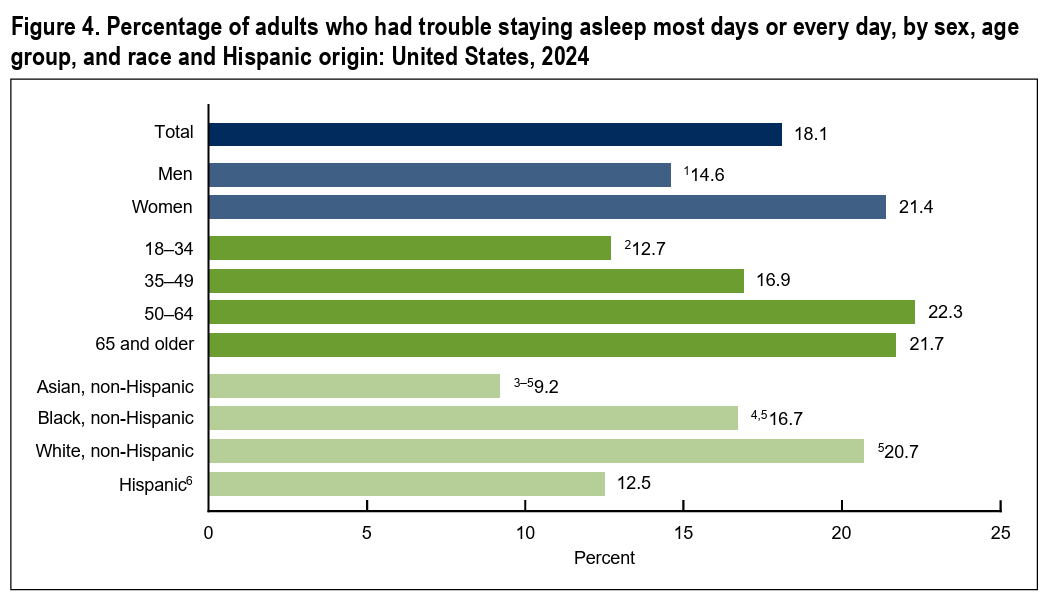
An estimated 18.1% struggled to stay asleep once they fell asleep. The data tell a story of a country that knows it should sleep more, knows it should sleep better, and routinely does neither.
Gonzales et al. (2023) found that adequate sleep duration of approximately 7 hours was related to greater HRV in middle-aged women. Once adequate, restorative sleep is achieved, further gains from additional hours become marginal. Protect the sleep you have.
Blood Pressure Reduction
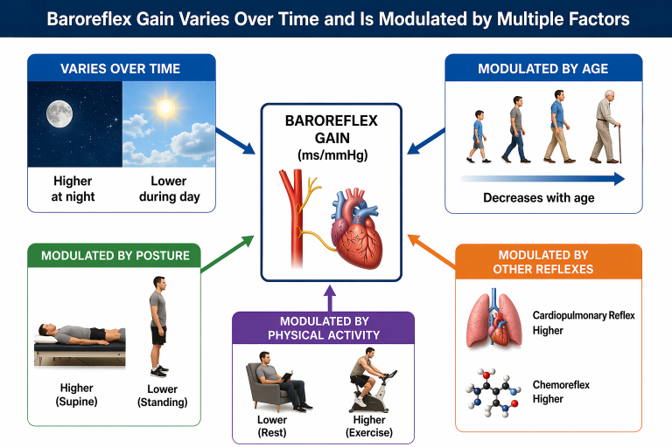
Baroreflex gain is how strongly the baroreflex adjusts heart rate in response to changes in blood pressure. Baroreflex gain varies over time, differs between daytime and nighttime, and is modulated by age, posture, physical activity, and other reflexes (Parati et al., 2009).The contribution of blood pressure control to HRV is not fixed but dynamically modulated across physiological states and across the lifespan.
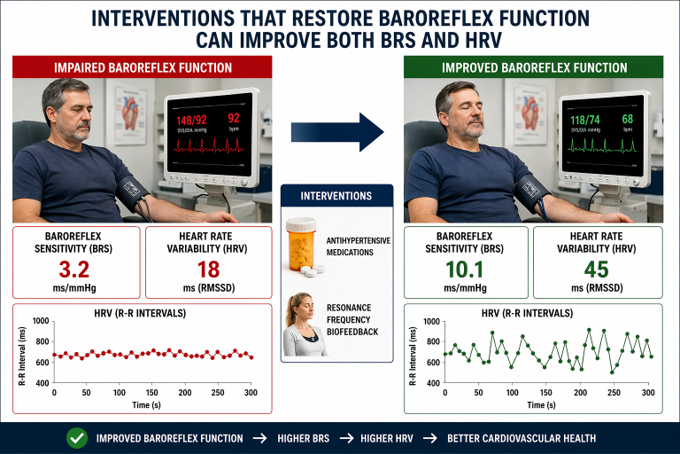
Interventions that restore baroreflex function, like antihypertensives (Ylitalo et al., 1999) or resonance frequency biofeedback (Vaschillo et al., 2006), can improve baroreflex sensitivity (BRS) and HRV.
Stress Management
Stress management increases HRV through the coordinated restoration of prefrontal inhibitory control, baroreflex sensitivity, vagal efferent activity, and reduced allostatic burden.
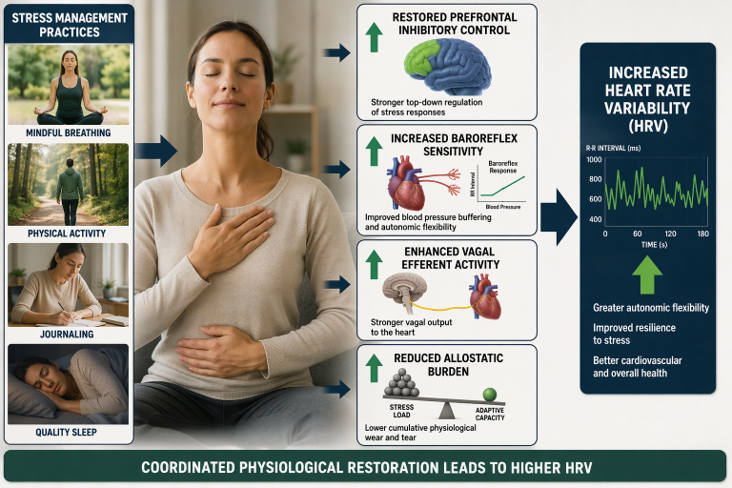
Stress management reduces allostatic load, the cumulative physiological toll of chronic stress adaptation, which itself suppresses HRV over time (Thayer & Sternberg, 2006).

By dampening HPA axis hyperactivity, reducing inflammatory cytokine levels, and normalizing sympathoadrenal output, effective stress management enhances parasympathetic cardiac regulation.
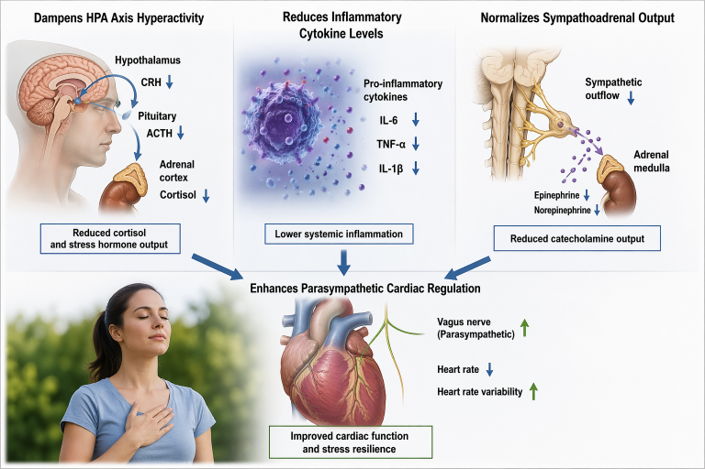
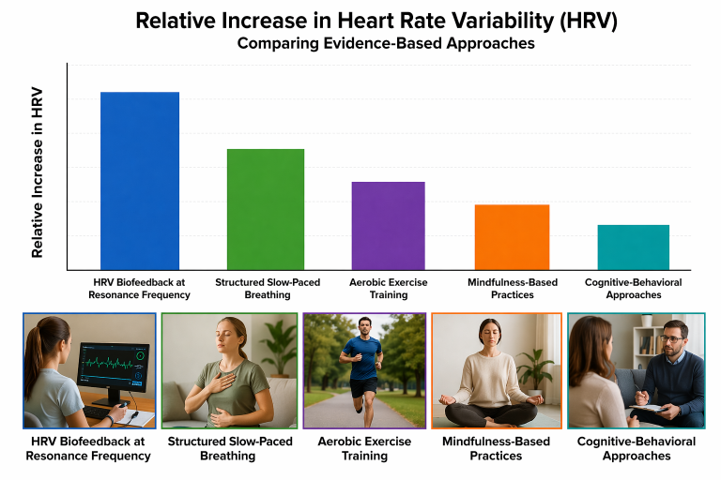
HRV biofeedback at the resonance frequency produces the largest and most consistent HRV increases, followed by structured slow-paced breathing, aerobic exercise training, mindfulness-based practices, and cognitive-behavioral approaches.
 The most effective stress management strategy for increasing HRV is one that addresses the specific autonomic dysregulation present in the individual while incorporating a component of direct physiological training (Shaffer & Ginsberg, 2017).
The most effective stress management strategy for increasing HRV is one that addresses the specific autonomic dysregulation present in the individual while incorporating a component of direct physiological training (Shaffer & Ginsberg, 2017).

Hydration
Dehydration reduces blood plasma volume, which in turn can lower baroreflex sensitivity and suppress vagal tone.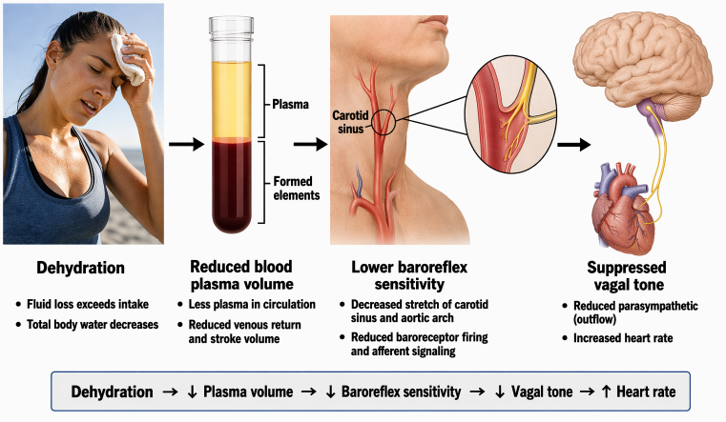
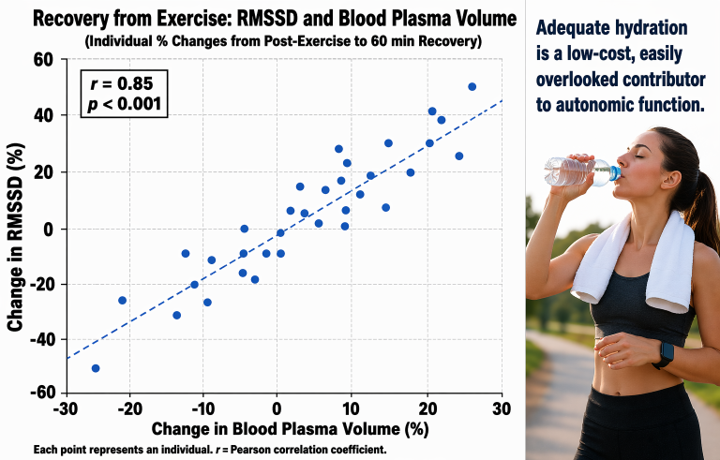
Buchheit et al. (2009) showed a large correlation (r = 0.85) between relative changes in RMSSD and changes in blood plasma volume during recovery from exercise.
Replace Sitting with Movement
Reducing sedentary behavior improves HRV. Nakayama et al. (2021) found that patients who decreased their sitting time over 6 months showed increased parasympathetic HRV.
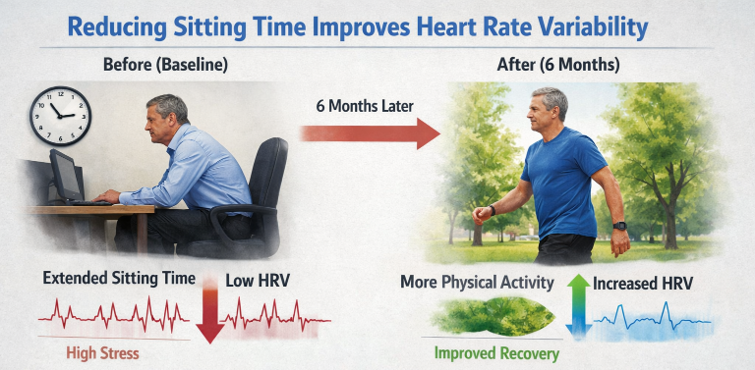
The mechanism may involve reductions in body adiposity and inflammatory markers, particularly when sedentary time is replaced with moderate-intensity physical activity (Pinto et al., 2023). The prescription is simple: move more, sit less, and break up long bouts of stillness.

At the office, take large movement breaks. Stretch or move every 20 minutes (Peper & Gibney, 2005).

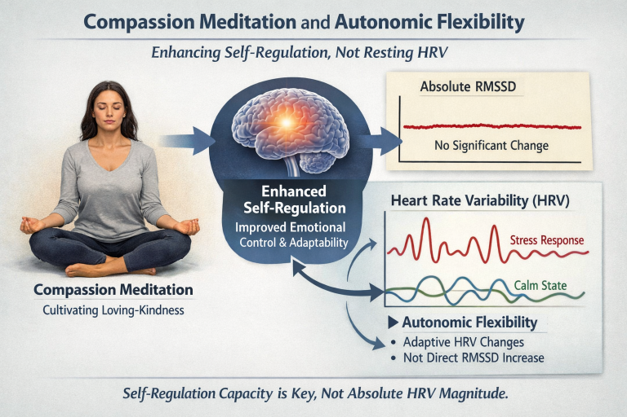
Compassion Trains the Vagus
In the landmark ReSource Project, a 9-month longitudinal mental training study, training modules on compassion, loving-kindness, and contemplative dyadic exercises increased HRV beyond what breathing alone could explain (Kok & Singer, 2017).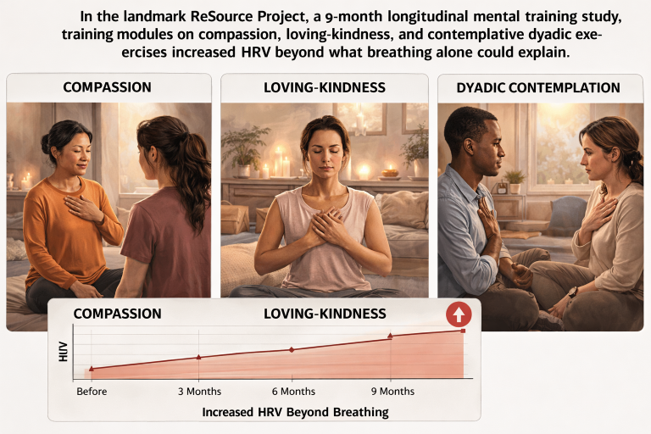
Compassion meditation may enhance self-regulatory capacity rather than directly boosting resting RMSSD, aligning with the broader theme that autonomic flexibility, not absolute HRV magnitude, is the meaningful outcome.
Green Space Exposure
Acute exposure to green spaces produces reliable short-term increases in parasympathetic HRV indices.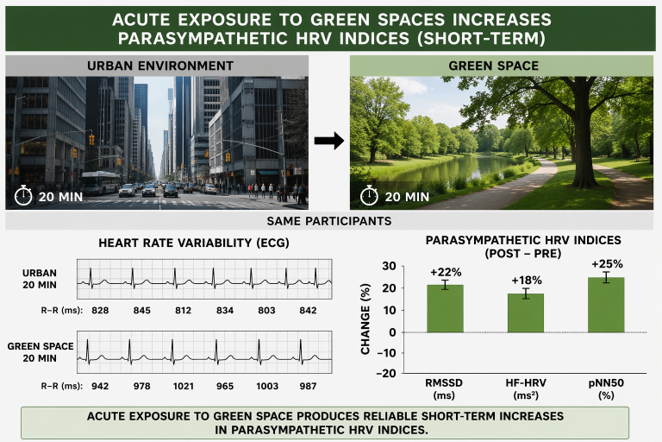
The strongest and most consistent findings emerge from controlled crossover designs comparing forest walking to urban walking. supporting autonomic health (Brown et al., 2013; Tsunetsugu et al., 2010).

The magnitude of these acute HRV effects is generally moderate and smaller than those produced by targeted physiological interventions such as HRV biofeedback (Lehrer & Gevirtz, 2014). However, the accessibility and scalability of green space exposure make it a promising population-level strategy for supporting autonomic health.

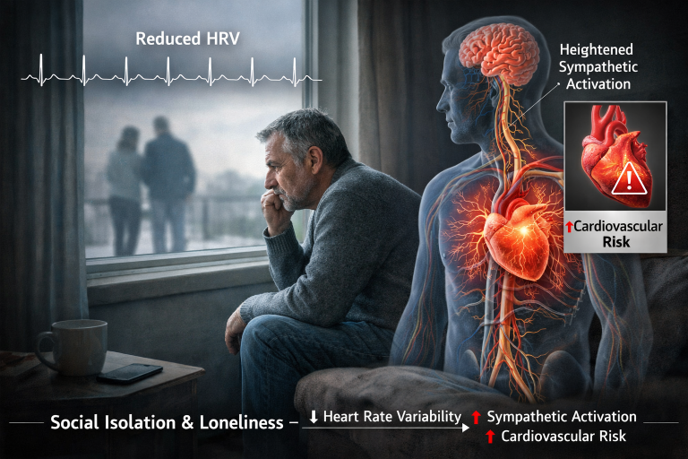
Community and Social Connection
Social isolation and loneliness have been associated with reduced HRV and heightened sympathetic activation, consistent with the broader literature linking social disconnection to cardiovascular risk.
Polyvagal theory (Porges, 2007) proposes that the ventral vagal complex supports social engagement and that perceived social safety enhances PNS regulation.
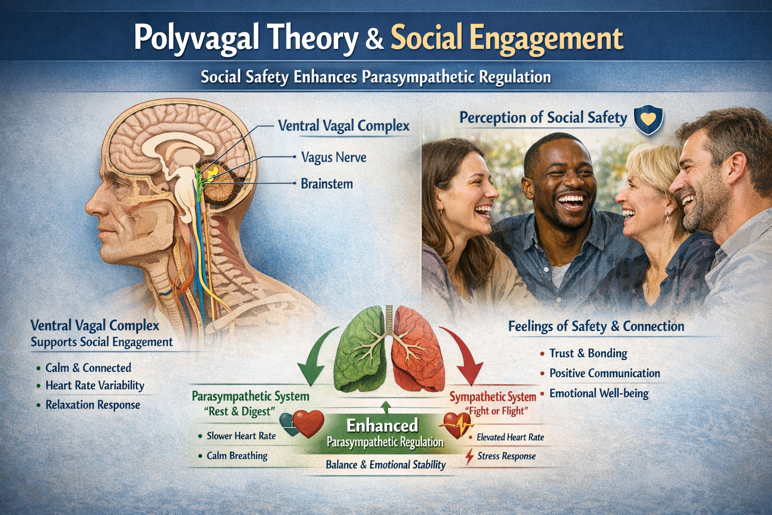
Living in an environment where one can thrive, maintaining community ties, and cultivating supportive relationships contribute to the broader context that allows HRV to reflect well-regulated autonomic function.

Acute Stressors
Three acute stressors, alcohol, illness, and excessive physical training can raise HR and lower HRV.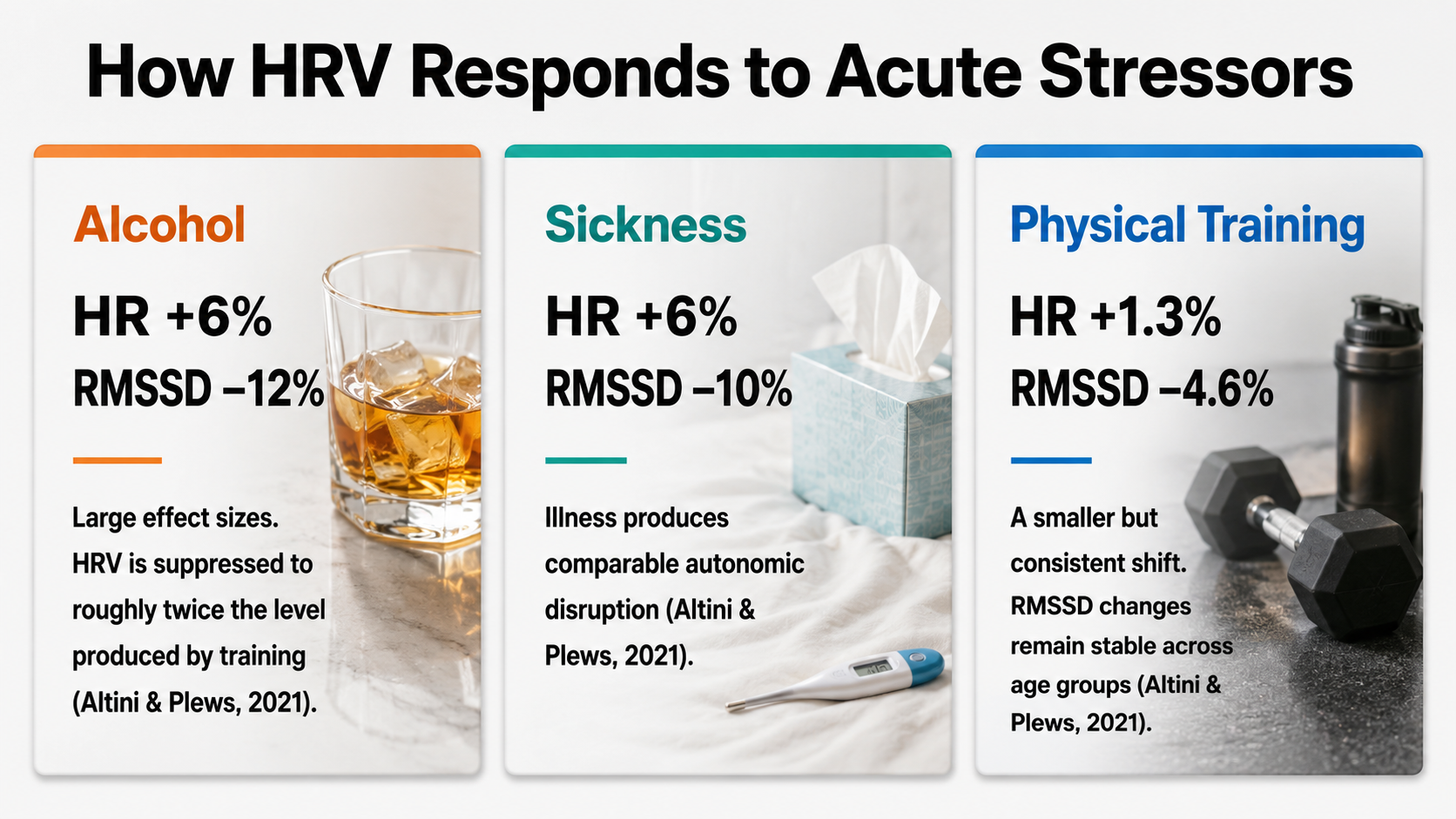
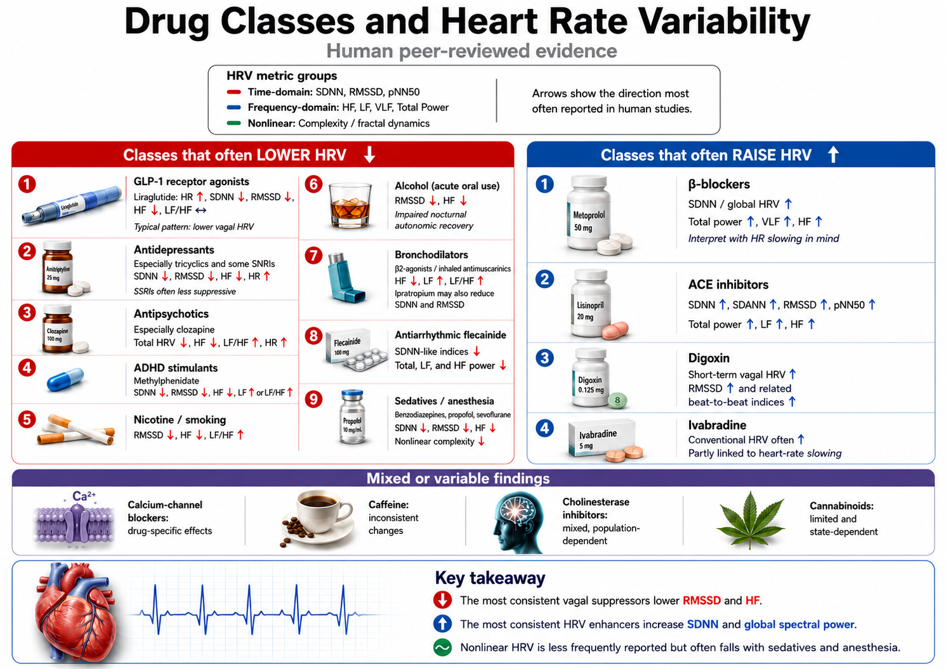
Drug Effects on HRV
Providers should obtain a complete list of a client's prescription and social drugs to better understand baseline and training HRV values.
Comprehension Questions: Clinical Tips
- Why is passive volition important during HRV biofeedback training, and what happens when clients use too much effort?
- What are the four physiological indicators that clinicians can monitor to detect excessive effort during training?
- For which types of clients might slow-paced contraction be preferable to SPB?
- How might hydration status affect HRV biofeedback training outcomes?
- What role does the therapeutic relationship play in HRV biofeedback, according to polyvagal theory?
HRV Biofeedback Training
Overview
Clients often experience measurable improvements during their very first training session, demonstrating increased RSA and improved HRV time- and frequency-domain measurements. After approximately four 30-minute sessions, many clients have corrected dysfunctional breathing patterns and show increased vagal tone and HRV. However, achieving maximum health and performance gains typically requires extended training of ten or more sessions combined with consistent home practice (Lagos et al., 2011).
This section covers the essential elements of training: session structure, resting baseline measurements, selecting initial respiration rates, introducing training to clients, recognizing success and difficulty indicators, reviewing training segments, promoting mindful breathing, conducting session reviews, comparing pre- and post-session values, key training elements, and determining how many sessions are needed.
Session Structure
A well-organized session flows through three phases: pre-baseline measurement, active training, and post-baseline measurement. This structure serves both clinical and motivational purposes. By bracketing training with baseline measurements, you create clear before-and-after comparisons that document learning and motivate continued practice.

Resting Pre- and Post-Baseline Measurements
Resting baselines capture your clients' psychophysiological activity without feedback or paced breathing. Instructions should be minimal and neutral: "Please sit quietly and breathe normally for the next few minutes." Depending on your clinical goals, you might monitor HRV, breathing parameters including depth, pattern, and rate, autonomic indicators such as skin conductance and temperature, blood pressure, and end-tidal CO2.
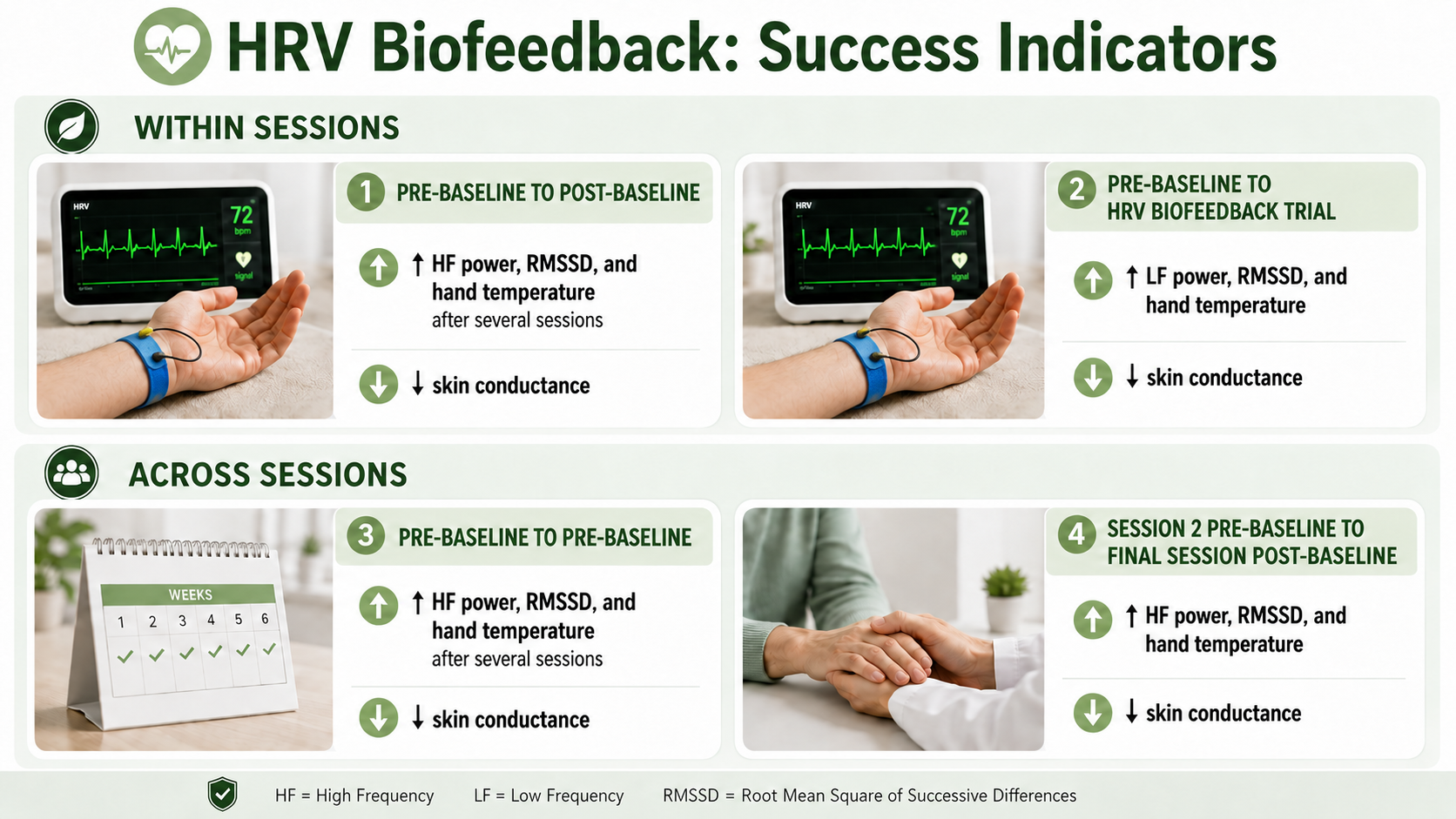
The comparison between pre-baseline and post-baseline values within a single session demonstrates within-session learning. Even more valuable is tracking pre-baseline changes across sessions, which reveals the combined effect of clinic training and home practice. A client whose pre-baseline HRV improves from session to session is integrating the skills into daily life.
During baselines, clients breathe at typical rates of approximately 12-16 bpm, so do not expect increases in LF power. Instead, look for increased HF power, improved HRV time-domain metrics such as RMSSD, elevated hand temperature, and reduced skin conductance level. These changes indicate genuine improvements in vagal tone and autonomic regulation.
We train clients to increase LF power during SPB to increase HF power during baselines when they breathe at typical rates.
How to Select a Starting Respiration Rate
Select an initial respiration rate for the animated pacing display based on your client's determined resonance frequency. However, shaping is crucial to client motivation and success. Rather than jumping immediately to the RF, choose a starting respiration rate within 1 or 2 breaths per minute of the client's baseline mean. This ensures early success, building confidence before gradually shifting toward the target rate.
Training Introduction
How you introduce training shapes your client's understanding and approach. Sample instructions that have proven effective include the following:
A healthy heart is not a metronome. As you inhale, your HR speeds, and as you exhale, your HR slows. This rhythmic speeding and slowing of your heart produces heart rate variability, which is vital to your health, performance, and resilience against stressors. The purpose of heart rate variability biofeedback training is to teach you to increase the healthy speeding and slowing of your heart by breathing effortlessly at the rate that is best for you and by increasing your ability to experience positive emotions like feelings of appreciation and gratitude.
Adopt a passive attitude in which you trust your body to breathe itself. Allow your attention to settle on your waist. Let your exhalation continue until your body initiates your next breath. Your inhalations should be no deeper than if you were smelling a flower. Allow your breathing to follow the yellow ball effortlessly.
Allow your stomach to gradually plop out as you inhale and then slowly draw inward as you exhale. As you practice, we will adjust the speed of the pacing display. Let it guide your inhalation and exhalation. Allow your stomach to gradually plop out as you inhale and then slowly draw inward as you exhale.
The computer can help you learn slow, effortless breathing. The pink tracing shows your HR, while the violet tracing shows the movement of the sensor around your stomach. As you gradually learn low-and-slow breathing, the two tracings should resemble smooth, repeating ocean waves.

After providing instructions, start recording data for a 3-minute training segment. At the end of each segment, engage the client in reflection: "How was the speed of the pacing display? Should we change it? Should we adjust the inhalation and exhalation lengths? What did you experience as you practiced breathing effortlessly?" These questions promote mindfulness and collaborative adjustment.
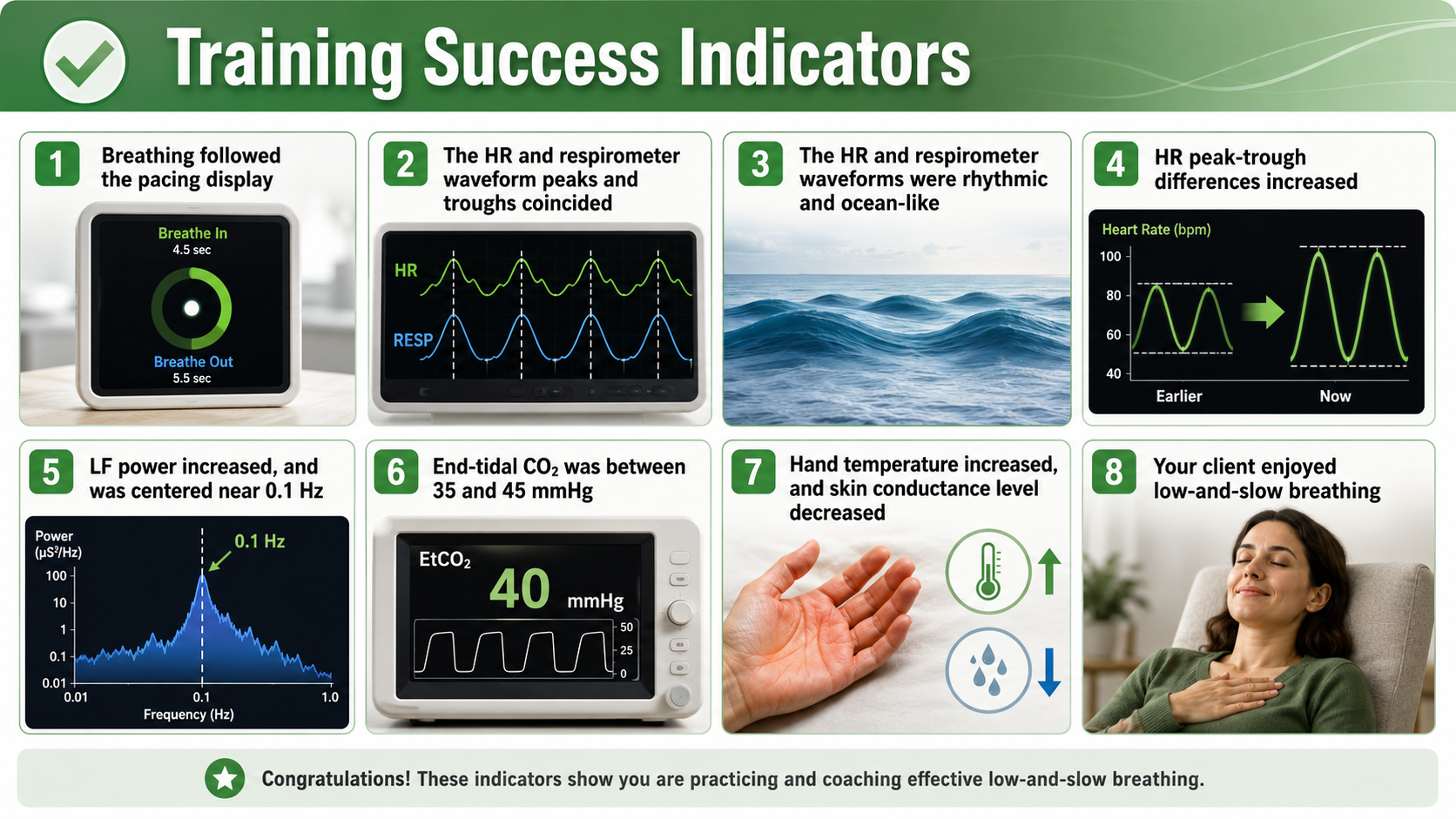
Training Success Indicators
Several signs indicate that training is proceeding well. Look for smooth, wavelike tracings in both respiration and HR signals. The peaks and troughs of these waveforms should align, indicating synchrony. Peak-to-trough HR differences should increase as the session progresses. The client should appear relaxed and report a sense of calm or ease.
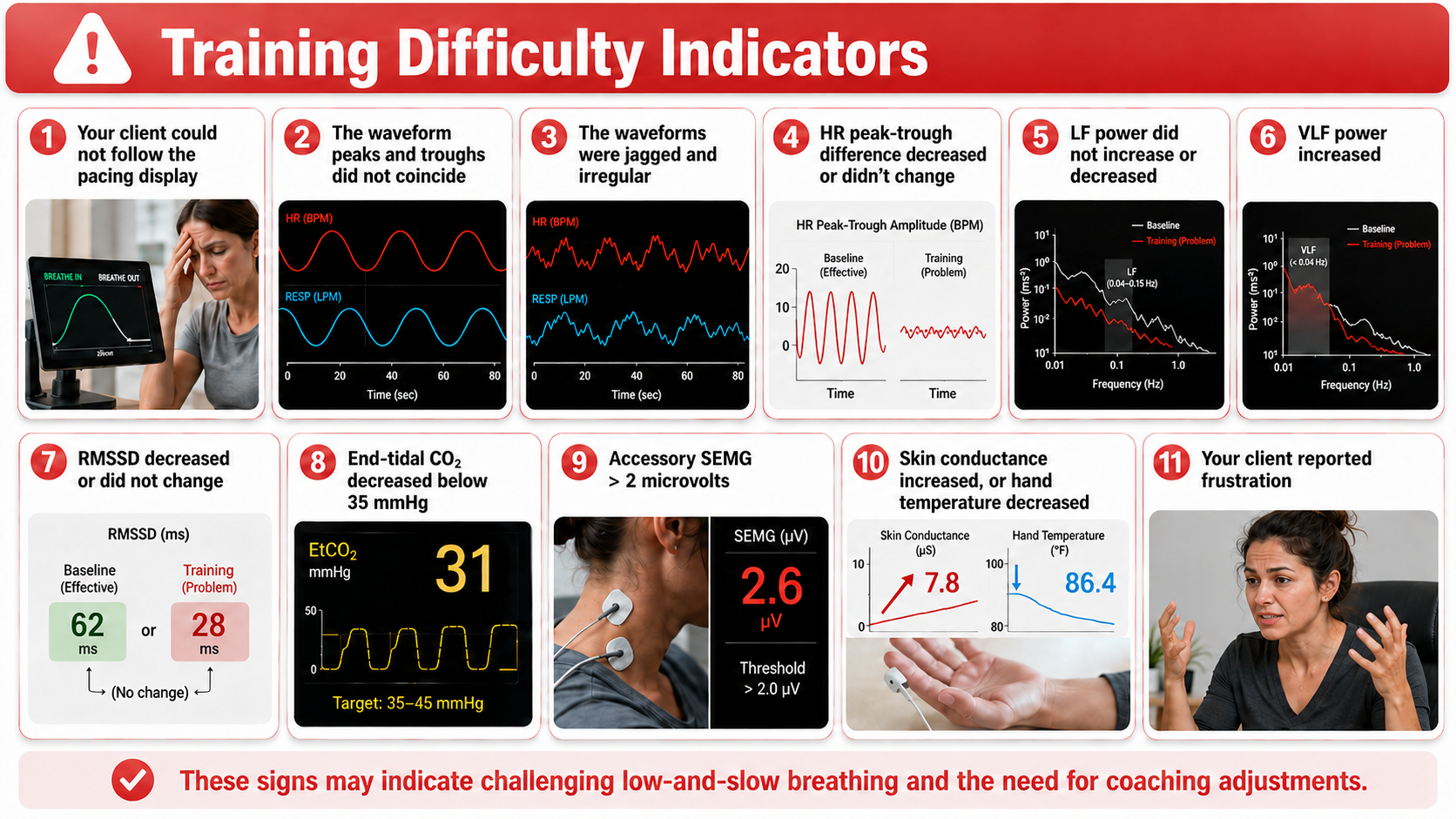
Training Difficulty Indicators
Equally important is recognizing when clients struggle. Warning signs include jagged, irregular waveforms with frequent inflection points. Misalignment between respiration and HR tracings suggests poor synchrony. Decreasing or stagnant peak-to-trough differences indicate the client may be working too hard or breathing at the wrong rate. Physical signs of tension or client reports of frustration or discomfort warrant immediate attention.
Training Segment Review
After each 3-minute segment, fit the entire recording on one screen and review it collaboratively with your client. If they succeeded, point out specific moments of success: "See how smooth your breathing became here? And notice how your HR waveform synchronized with your breathing signal in this section." Concrete positive feedback builds confidence and clarifies what success looks and feels like.

Promote Mindful Breathing
Before starting the next segment, engage the client's curiosity about their own physiology. Ask questions like: "What were you doing when the display became wavelike and regular? What happened when the display became more jagged and irregular?" If accessory SEMG exceeded 2 microvolts, show this on the display, ask whether they noticed heightened breathing effort, and encourage them to "let your shoulders relax and allow yourself to breathe."
Reassure clients that choppy tracings are normal at the start of training. The waveforms will gradually become more wavelike as breathing becomes more rhythmic and regular. Rather than overwhelming clients with corrections, ask them to experiment with one or two changes at a time. For example: "Effortless breathing is rhythmic like ocean waves. Allow your stomach to gently expand and contract as you follow the pacing display."
Session Review
After your client has completed six 3-minute training segments, conduct a 3-minute post-baseline recording without feedback. Following this final baseline, ask your client how they felt and what they learned during the session. Display the entire session on one screen, highlighting moments of success and areas that need continued work. This comprehensive review helps clients understand their trajectory and sets expectations for future sessions.

Comparing Pre- and Post-Session Values
Without pacing or feedback, your client will breathe at typical rates during both baselines. The meaningful comparisons between pre- and post-baseline involve metrics that reflect vagal tone at normal breathing rates: HF power, RMSSD, and hand temperature should increase, while skin conductance level should decrease.
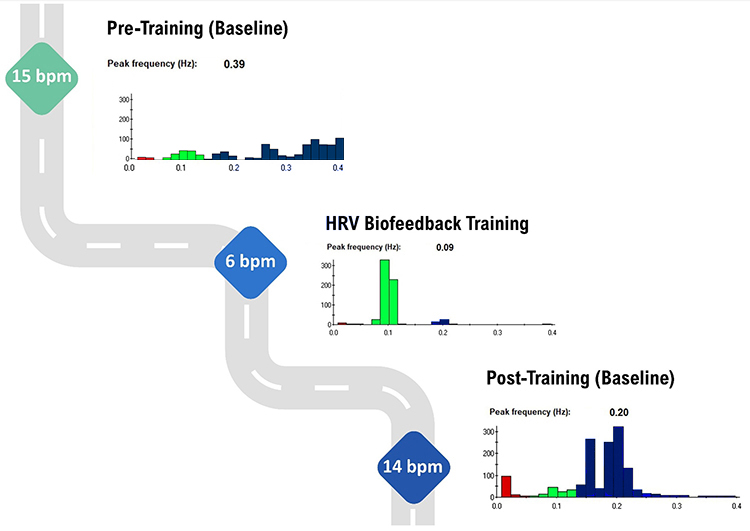
The graphic below shows HF power (in blue) during a pre-training baseline, HRVB training, and a post-training baseline. On the y-axis, power in each band is displayed in absolute units. HF power increases from approximately 100 μV during the pre-training baseline to approximately 300 μV during the post-training baseline. This threefold increase indicates meaningfully enhanced vagal tone.
Also note the greater LF power concentration in the post-training baseline compared with pre-training, even though the client breathed at typical rates in both baselines. This carryover effect demonstrates that resonance frequency training benefits persist beyond the training itself. These spectral plots were generously provided by Dr. Inna Khazan.
HRV Biofeedback Training Elements
Effective training integrates multiple elements working together. These include appropriate sensor selection, engaging feedback displays, individualized breathing rates based on resonance frequency assessment, a supportive therapeutic relationship, passive volition and effortlessness, mindful attention to body sensations, integration of positive emotion, and consistent home practice.
How Many HRVB Sessions Are Required?
Many clients begin to breathe more effortlessly and show increased HRV during their very first training session. However, there is typically a several-week lag between increased HRV during training and improved health or performance in daily life. Clients require this time to consolidate their learning and transfer enhanced skills to the diverse settings of their lives.
Practice is the bridge between the clinic and everyday life. Without consistent home practice, even excellent in-clinic performance may not translate to real-world benefits.

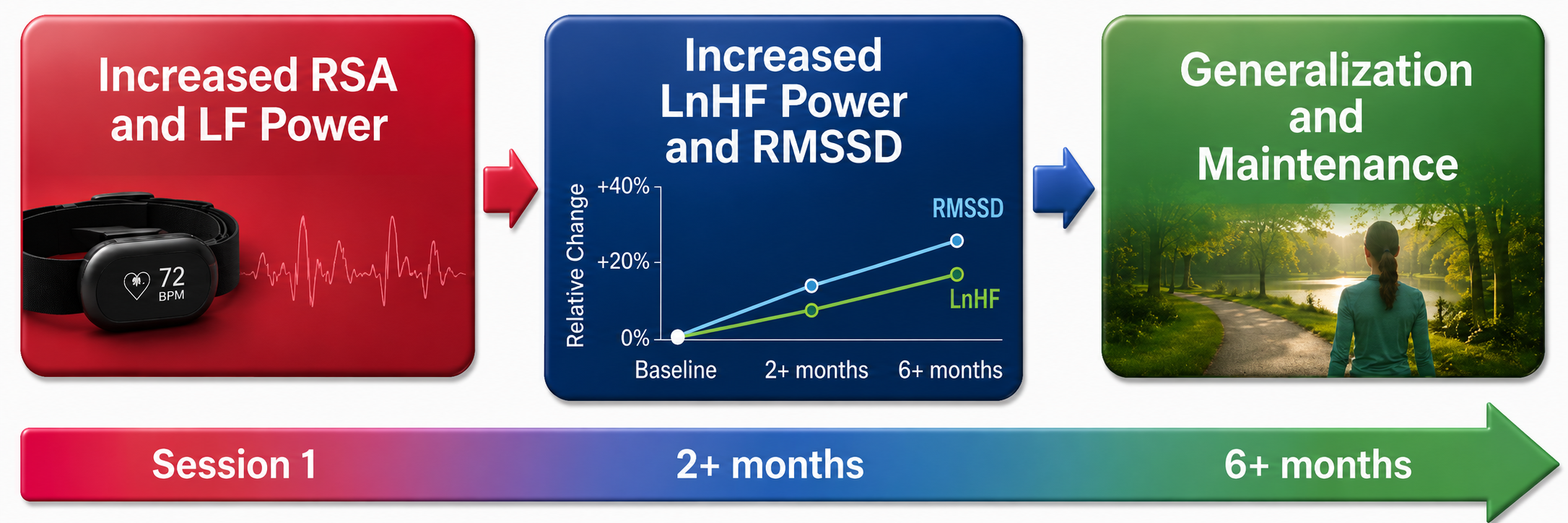
The physiological changes follow a predictable timeline. Increased RSA immediately exercises the baroreflex without necessarily changing baseline vagal tone or improving blood pressure regulation. Those deeper adaptations require months of consistent practice (Gevirtz, Lehrer, & Schwartz, 2016; Lagos et al., 2011). Think of it like exercise: a single workout feels good, but cardiovascular fitness develops over months of training.
Comprehension Questions: Training Sessions
- Why should clinicians measure both pre- and post-baseline values during HRV biofeedback sessions?
- What HRV changes would you expect to see during pre- and post-baselines (when clients breathe at typical rates) versus during paced breathing training?
- How should you select a starting respiration rate for a new client?
- What questions can you ask between training segments to promote mindful breathing?
- Why is there often a lag between initial HRV improvements and measurable health or performance gains?
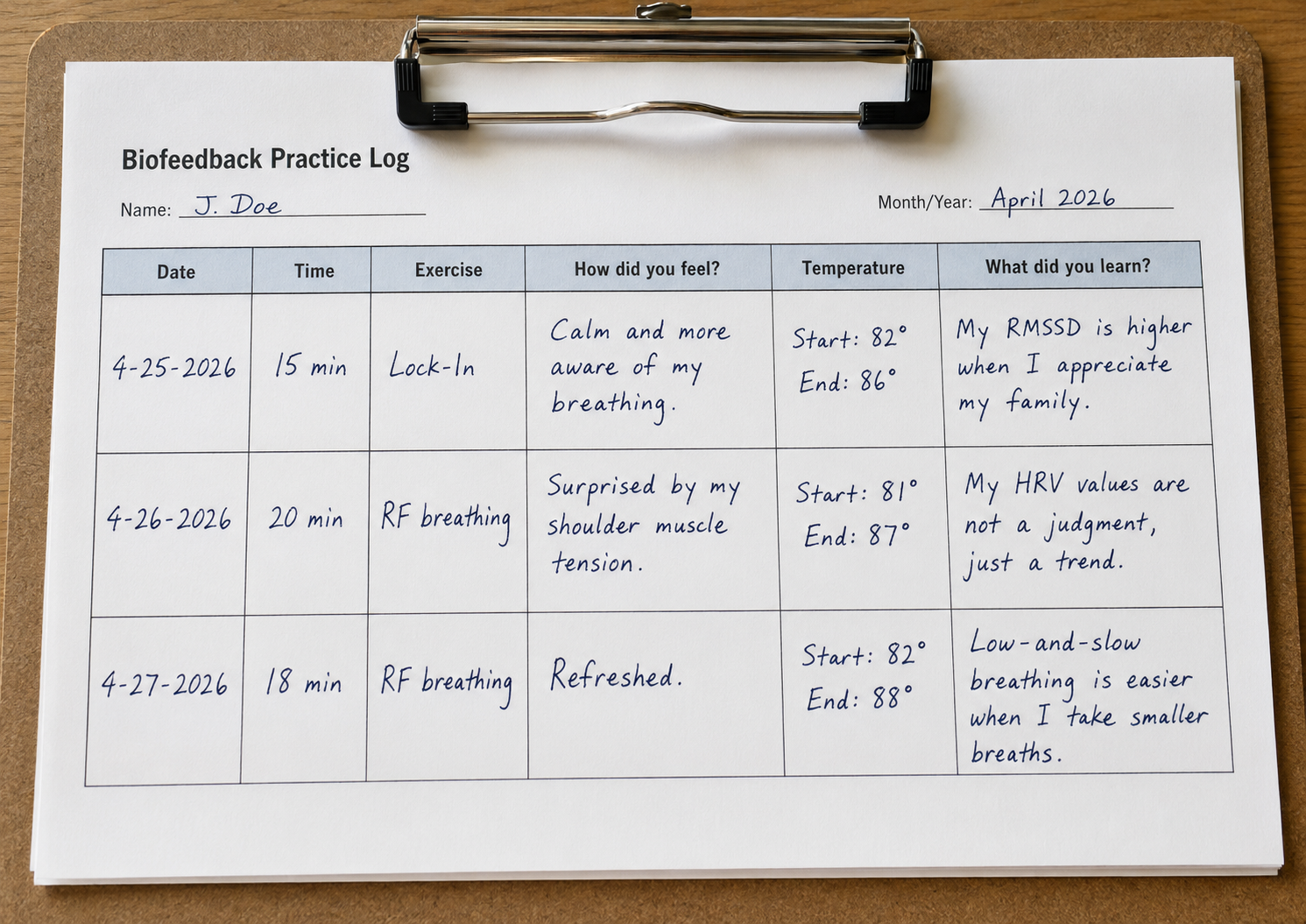
Practice Assignments
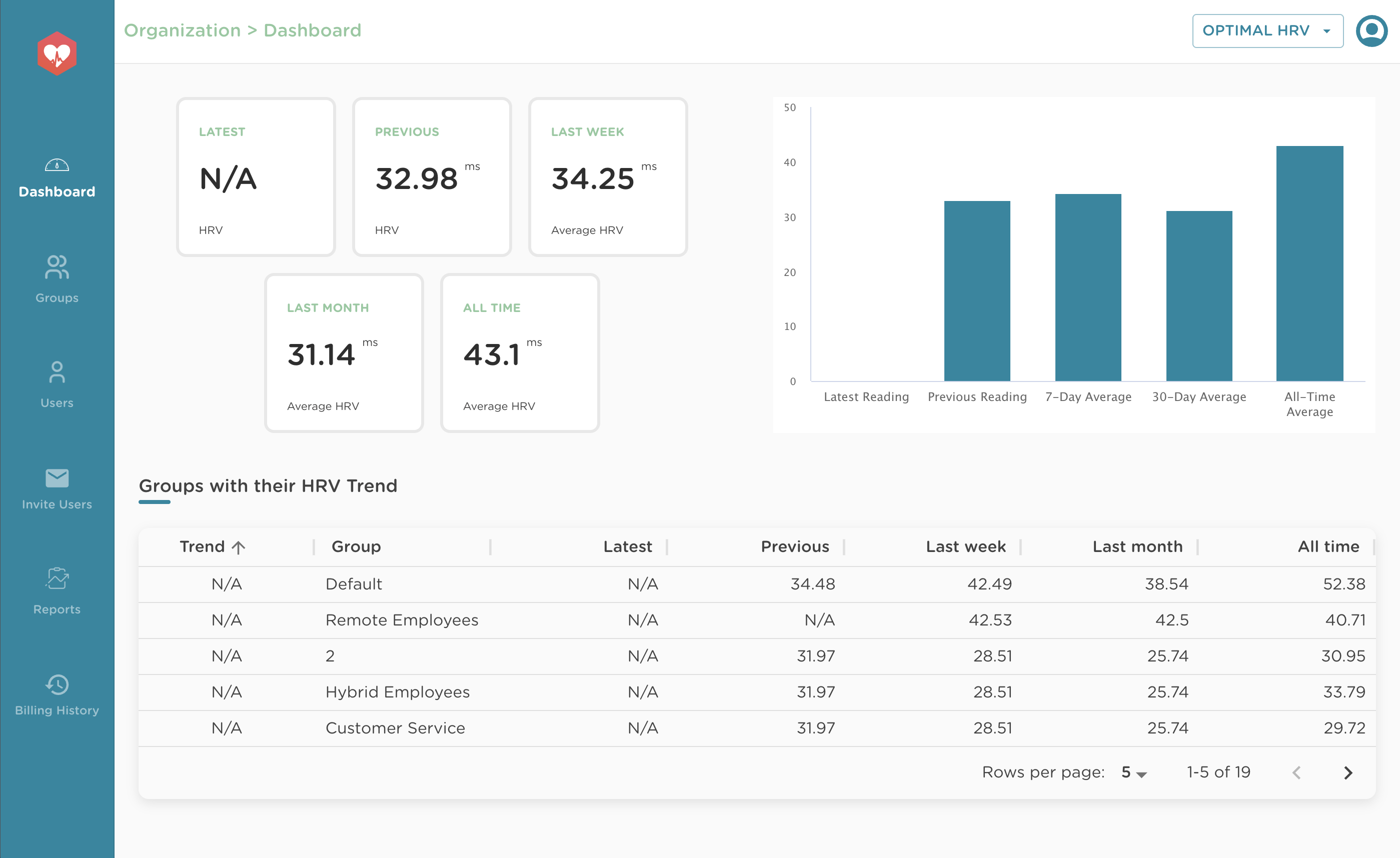
Home practice transforms clinic learning into lasting change. Encourage clients to measure their HRV while breathing at typical rates immediately after waking, when circadian influences are relatively stable. They can send weekly reports showing trends in their HRV, and products like Optimal HRV automate data sharing between clients and clinicians.
The standard recommendation is 20 minutes of daily practice with HRV monitoring. After each practice session, clients can complete an online diary and share their interbeat interval data with you. Khazan (2013) provides excellent practice logs in The Clinical Handbook of Biofeedback that you can adapt for your clinical needs.
Reality often differs from recommendations. Some clients will practice diligently; others will not. You may have to settle for 10 minutes once a day or practice "as needed." Interestingly, Lehrer et al. (2020) concluded that the frequency and length of home practice did not significantly impact effect size. The practice of resonance frequency breathing as needed may have produced most of the observed gains (p. 125). This finding suggests that even brief, strategically-timed practice can be valuable.
Following Dr. Gevirtz's recommendation, include starting and ending hand temperatures in practice logs, since successful HRVB practice may produce peripheral warming as increased CO2 in the bloodstream promotes nitric oxide release and vasodilation.
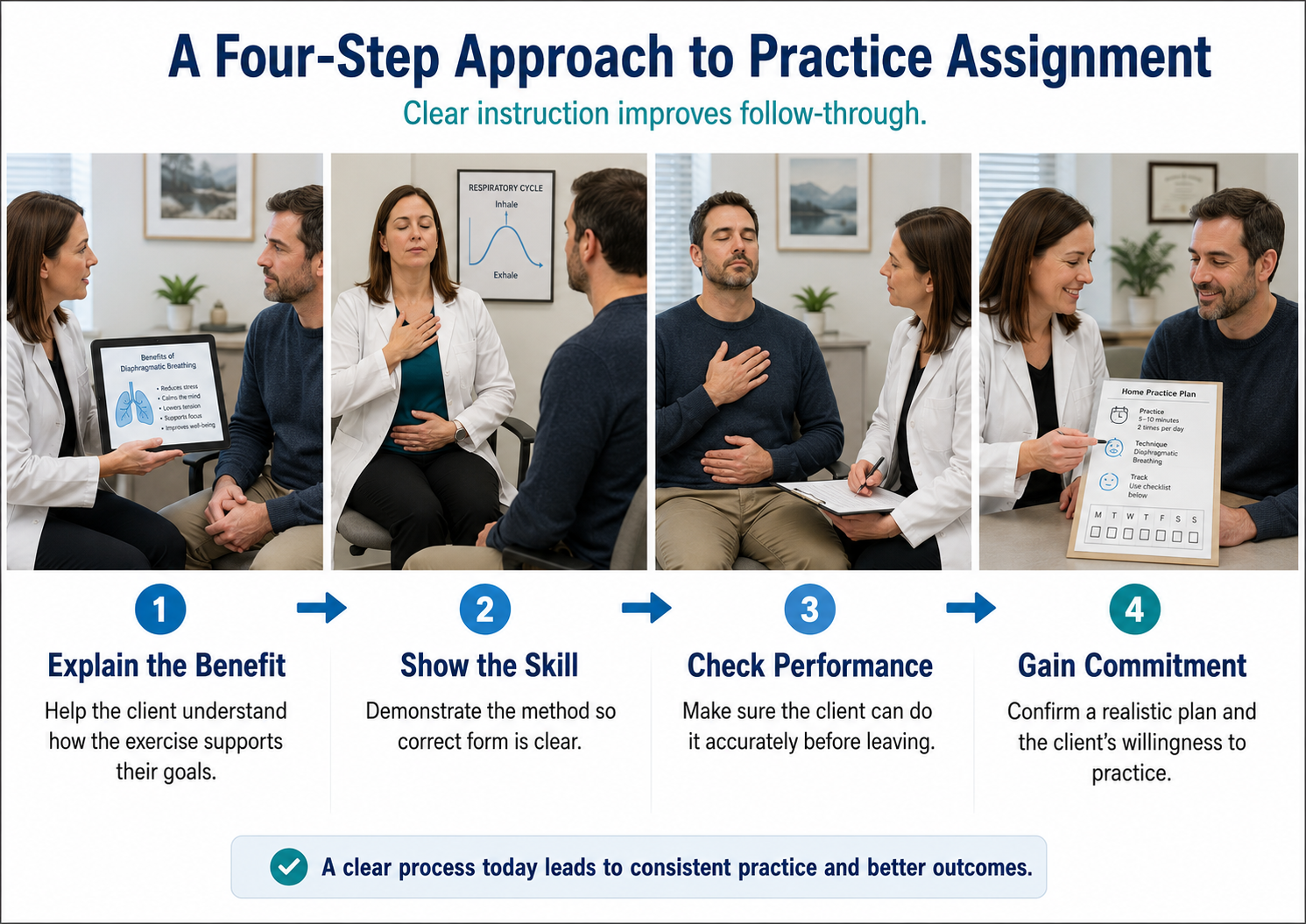
Effective practice assignment requires four steps. First, explain the purpose of the exercise so clients understand why it matters. Second, demonstrate the skill in the clinic so they can see correct technique. Third, confirm that they can correctly perform it before leaving. Fourth, secure their agreement to practice. To build a collaborative relationship and empower your clients, encourage them to find ways to improve exercises or develop alternatives that work better for their lives.
Overview
This section addresses practice in diverse settings, aerobic activity, HR monitoring, HRV monitoring, emotional self-regulation techniques, home HRV practice equipment, advanced HRV assessment, and finger temperature monitoring.
Practice in Diverse Settings
Encourage clients to practice resonance frequency breathing during everyday activities in diverse settings including commuting, work, and home. This varied practice promotes generalization, the ability to apply skills across different contexts. A veteran who practices only in a quiet clinic may struggle to access those skills during a stressful meeting at work. Practice in multiple environments builds robust, flexible self-regulation.

Aerobic Activity
Assign 20 minutes daily of aerobic activity, particularly for sedentary clients. Aerobic exercise produces cardiovascular adaptations that complement HRV biofeedback: it lowers resting HR and raises baseline HRV. These effects are additive with HRVB training, creating synergies that neither intervention achieves alone.

Monitor HR
Invite clients to monitor their HR during daily activities and emotional states using wearable devices. This practice increases mindfulness of stressors and physiological responses to challenges. When a client notices that checking email raises their HR by 15 bpm, they gain insight that motivates behavior change. Self-monitoring transforms abstract concepts into personal discoveries.

Monitor HRV
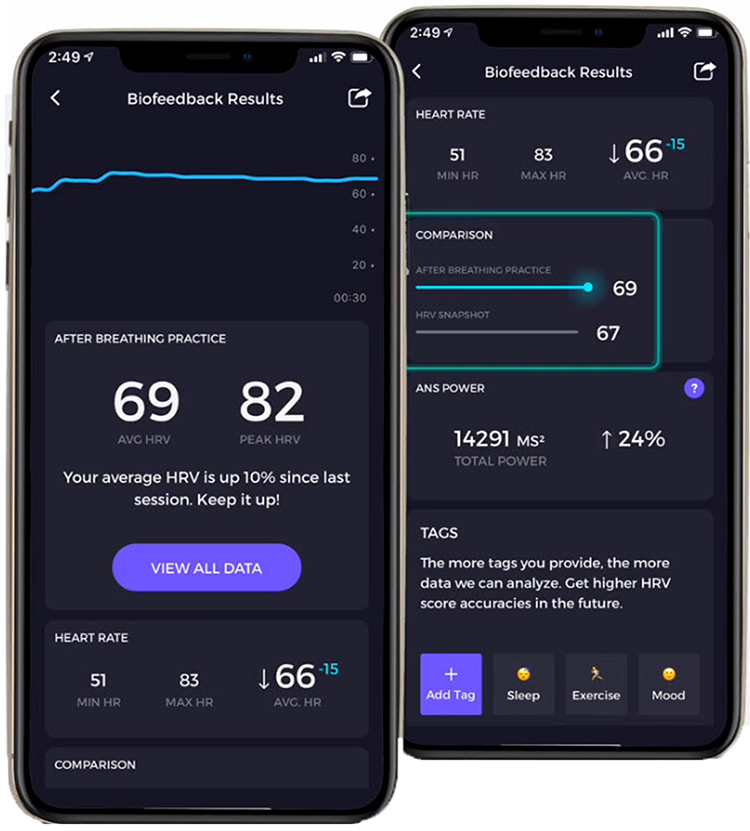
Apps like Elite HRV and Optimal HRV enable clients to take HRV snapshots with built-in artifact correction. These brief measurements, taken consistently over time, reveal patterns and progress that motivate continued practice. The data also provides valuable clinical information about how clients respond to life stressors.
 |
 |
Emotional Self-Regulation Practice
Emotional self-regulation practice complements breathing training by addressing the psychological dimension of stress response. These techniques may reduce parasympathetic withdrawal, cultivate the tend-and-befriend response, and increase resilience. For many clients, emotional regulation proves as important as breathing technique.

The Institute of HeartMath's Lock-In Technique provides a structured approach to emotional self-regulation. Instructions for the technique are as follows:
Try to focus your attention on the area around your heart. Maintain your heart focus and, while breathing, imagine that your breath is flowing in and out through the heart area. Breathe casually, just a little deeper than normal.
Now try to recall a positive emotion or feeling that makes you relaxed and comfortable. Find a positive feeling like appreciation, care, joy, kindness, or compassion. You can recall a time you felt appreciation or care. This could be the appreciation or care you feel towards a special person, a pet, a place you enjoy, or an activity that was fun for you.
If you cannot feel anything, that is okay. Just try to find a sincere attitude of appreciation or care. Continue to think of this positive feeling or emotion.
Home HRV Practice
Portable HRV biofeedback devices bring the training experience home. The Institute of HeartMath's Inner Balance and similar devices allow personal training whenever clients choose, removing the constraint of clinic-only practice. This accessibility dramatically increases potential practice time and supports skill maintenance after formal treatment ends.

Advanced HRV Assessment
For clients who want detailed progress tracking, the Institute of HeartMath's emWave Pro Plus provides comprehensive HRV assessment using an automated deep breathing protocol. The software reports commonly used HRV metrics referenced to age-related norms, allowing clients to see how they compare to healthy populations and track their improvement over time.

The emWave Pro Plus also provides resting metrics for training sessions ranging from 1 to 99 minutes, offering flexibility for different clinical protocols and client preferences.
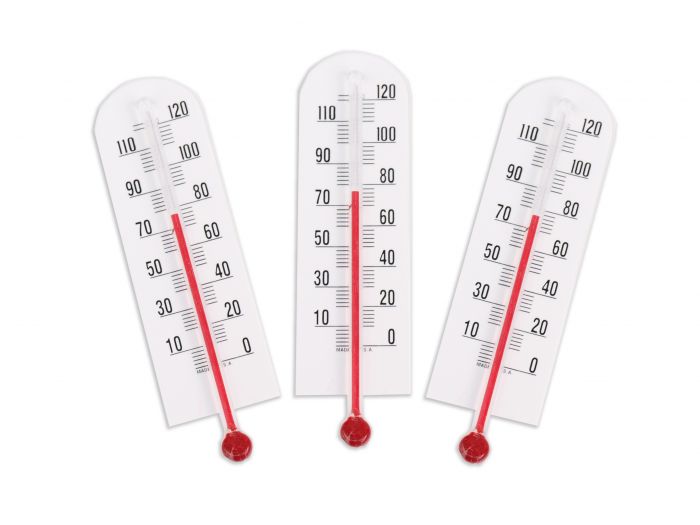
Monitor Finger Temperature
Encourage your clients to monitor their hand temperature using inexpensive alcohol thermometers to see whether their practice produced warming or cooling. Hand temperature provides a simple, low-tech indicator of autonomic state. Warming typically indicates reduced sympathetic activation and increased blood flow, suggesting successful practice.
HRV Myths
Dr. Inna Khazan addresses common misconceptions about HRV and HRV biofeedback in this video. Understanding these myths helps clinicians provide accurate information to clients and avoid common pitfalls in training.
Comprehension Questions: Practice and Myths
- What is the recommended frequency and duration for home HRV biofeedback practice?
- Why should clinicians encourage practice in diverse settings rather than just at home?
- What role does hand temperature monitoring play in home practice?
- How does aerobic exercise complement HRV biofeedback training?
- What is the HeartMath Lock-In Technique and how does it integrate with HRV training?
Assignment
Which of the two screens below shows better HRV performance? What is the basis for your judgment? Take a moment to examine each display carefully before reading the analysis.
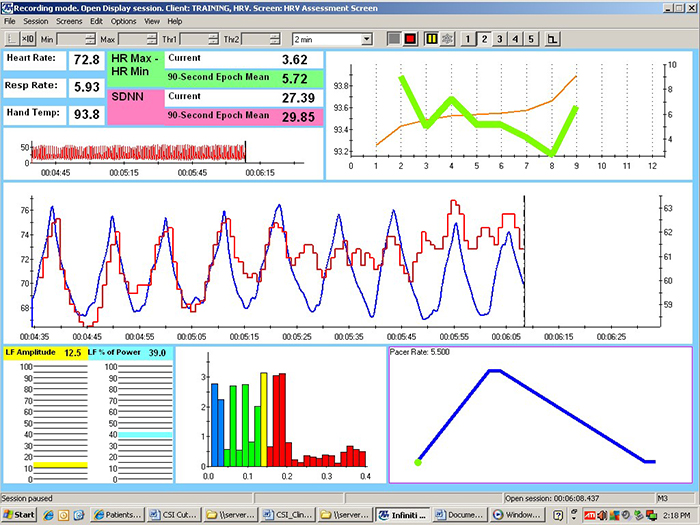
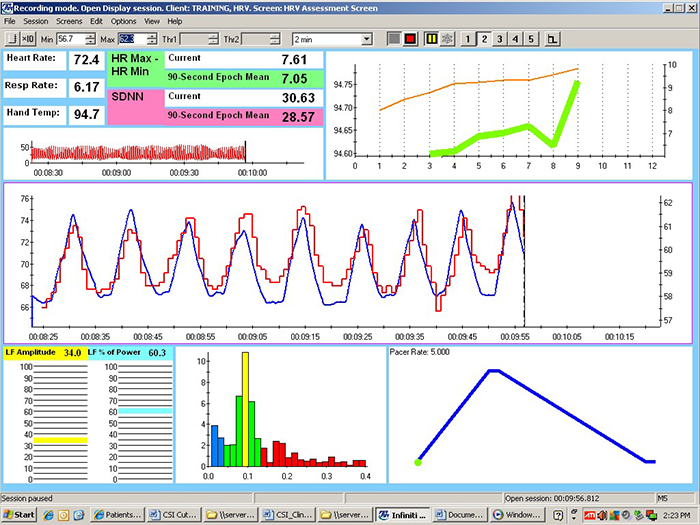
Begin by checking the mean respiration rates to confirm that this client breathed around 6 breaths per minute in each session. She did. Now examine the values for HR Max minus HR Min and LF amplitude. Both were substantially higher in the second session. The greater HR Max minus HR Min is visually evident in the peak-to-trough differences, which show larger swings in the second session.
Next, look at the distribution of signal power at 0.1 Hz. In the second session, signal energy is more tightly concentrated at and around this dominant frequency, indicating better resonance. Inspect the synchrony of the HR and respirometer tracings. The peaks and valleys align more closely in the second session. Finally, compare hand temperatures. Her hands were almost 1 degree Fahrenheit warmer in the second session, indicating reduced sympathetic activation.
These recordings were from a chronic pain patient who received treatment in an interdisciplinary chronic pain program. The improvement from Session 1 to Session 2 demonstrates the kind of progress clinicians can expect with consistent training and practice.
Cutting Edge Topics
Wearable Technology and Continuous HRV Monitoring
The proliferation of wearable devices capable of continuous HRV monitoring is transforming both research and clinical practice. Devices like the Oura Ring, Google Air band, and WHOOP strap now provide overnight and continuous HRV metrics that were previously available only in clinical settings. While these consumer devices have accuracy limitations compared to clinical-grade equipment, they offer unprecedented opportunities for longitudinal tracking and ecological momentary assessment.
Clinicians increasingly use wearable data to supplement clinic-based training. These devices reveal how clients' HRV responds to real-world stressors, sleep quality, and recovery. Continuous data streams can uncover patterns invisible in periodic clinic assessments, such as the cumulative effects of work stress or the impact of lifestyle changes on autonomic function.
Artificial Intelligence in HRV Analysis
Machine learning algorithms are being developed to detect subtle patterns in HRV data that may predict health outcomes or identify optimal training parameters. These AI systems analyze the complex, nonlinear dynamics of heart rate variability to provide personalized recommendations for breathing rates, practice timing, and intervention strategies. While still in early development, these tools promise to enhance HRV biofeedback precision by tailoring protocols to individual physiological signatures.
Virtual Reality Enhanced HRV Training
Virtual reality environments are being explored as immersive contexts for HRV biofeedback training. By placing clients in calming virtual environments such as beaches, forests, or meditation spaces while they practice resonance frequency breathing, VR may enhance the learning process and improve engagement. Early research suggests that VR-enhanced training may produce stronger initial effects, though questions remain about long-term transfer to real-world settings. For populations like veterans with PTSD, VR may also allow graduated exposure to challenging scenarios while practicing regulation skills.
Telehealth Delivery of HRV Biofeedback
The COVID-19 pandemic accelerated the adoption of telehealth for HRV biofeedback delivery. Clinicians discovered that many aspects of HRV training can be effectively delivered remotely using video conferencing combined with client-side PPG sensors or smartphone apps. While telehealth cannot replicate all aspects of in-person training, particularly initial sensor placement and equipment troubleshooting, it has proven valuable for follow-up sessions, practice coaching, and reaching clients in underserved areas. Research continues to establish best practices and compare outcomes between telehealth and traditional delivery, but early results are encouraging for hybrid models that combine initial in-person training with telehealth follow-up.
Glossary
accessory muscles: the sternocleidomastoid, pectoralis minor, scalene, and trapezius muscles, which are used during forceful breathing, as well as clavicular and thoracic breathing.
apnea: breath suspension.
atrial fibrillation: the most common cardiac arrhythmia involving rapid, irregular contraction of the two upper atrial chambers.
baroreceptor reflex (baroreflex): a mechanism that provides negative feedback control of BP. Elevated BP activates the baroreflex to lower BP, and low BP suppresses the baroreflex to raise blood pressure.
baroreflex gain: how strongly the baroreflex adjusts heart rate in response to a change in blood pressure; it varies over time and is modulated by age, posture, and physical activity.
body mass index (BMI): weight divided by height squared, which exerts a small but consistent influence on HRV.
capnometer: an instrument that monitors the carbon dioxide (CO2) concentration in an air sample (end-tidal CO2) by measuring the absorption of infrared light.
clavicular breathing: a breathing pattern that primarily relies on the external intercostals and the accessory muscles to inflate the lungs, resulting in a more rapid respiration rate, excessive energy consumption, and incomplete ventilation of the lungs.
coherence: a narrow peak in the BVP and ECG power spectrum between 0.09 and 0.14 Hz.
diaphragm: the dome-shaped muscle whose contraction enlarges the vertical diameter of the chest cavity and accounts for about 75% of air movement into the lungs during relaxed breathing.
emotional self-regulation: the self-monitoring, initiation, maintenance, and modulation of rewarding and challenging emotions and the avoidance and reduction of high levels of negative affect.
end-tidal CO2: the percentage of CO2 in exhaled air at the end of exhalation.
frequency-domain measures of HRV: the calculation of the absolute or relative power of the HRV signal within four frequency bands.
heart rate variability (HRV): the variation in time intervals between consecutive heartbeats.
high-frequency (HF) band: the HRV frequency range from 0.15-0.40 Hz that represents the inhibition and activation of the vagus nerve by breathing (respiratory sinus arrhythmia).
interbeat interval (IBI): the time interval between the peaks of successive R-spikes (initial upward deflections in the QRS complex). This is also called the NN (normal-to-normal) interval after removing artifacts.
ischemia: insufficient blood supply to tissue, which depresses the ST segment of the ECG.
large movement breaks: brief interruptions of sedentary behavior, such as stretching or moving every 20 minutes, that help preserve parasympathetic HRV.
loneliness: the distressing perception of social disconnection, which has been associated with reduced HRV and heightened sympathetic activation.
low-frequency (LF) band: the HRV frequency range of 0.04-0.15 Hz that may represent the influence of PNS and baroreflex activity when breathing at the RF.
metabolic acidosis: a pH imbalance in which the body has accumulated excessive acid and has insufficient bicarbonate to neutralize its effects. In diabetes and kidney disease, hyperventilation attempts to compensate for abnormal acid-base balance, and slower breathing could endanger health.
mindfulness: a nonjudgmental focus of attention on the present on a moment-to-moment basis.
passive volition: an attitude of allowing and effortlessness during biofeedback training, in which the body feels as if it is performing the target behavior (like breathing) by itself.
peak frequency: the HRV frequency with the greatest power.
photoplethysmograph (PPG): an optical sensor placed on an earlobe or finger that measures blood volume changes to derive pulse rate, trading some accuracy for ease of application.
physiological entrainment: the unconscious tendency of one person's physiological state, such as breathing rate or arousal, to match that of another person during interaction.
polyvagal theory: Porges's theory proposing that the ventral vagal complex supports social engagement and that perceived social safety enhances parasympathetic regulation.
prolonged QT interval: an extended QT interval associated with increased risk of ventricular tachyarrhythmias, cardiac arrest, and sudden death.
pulse oximeter: a device that measures dissolved oxygen in the bloodstream using a photoplethysmograph sensor placed against a finger or earlobe.
QT interval: the period signaling depolarization and repolarization of the ventricles.
resilience: adapting effectively to stressors, threats, and trauma.
resonance frequency (RF): the frequency at which a system, like the cardiovascular system, can be activated or stimulated.
respiratory sinus arrhythmia (RSA): the rhythmic increase in heart rate during inhalation and decrease during exhalation.
reverse breathing: the abdomen expands during exhalation and contracts during inhalation, often resulting in incomplete ventilation of the lungs.
slow-paced breathing (SPB): diaphragmatic breathing between 4.5 to 6.5 bpm.
slow-paced contraction (SPC): the simultaneous contraction of the wrists, core, and ankles to increase RSA.
social isolation: an objective lack of social contact or connection, which has been associated with reduced HRV and heightened sympathetic activation.
ST segment: the portion of the ECG between ventricular depolarization and repolarization, which becomes depressed during ischemia.
synchrony: the phase relationship between two signals in which their peaks and valleys are aligned (e.g., HR and respirometer expansion reach their maximum and minimum values simultaneously).
thoracic breathing: a breathing pattern that primarily relies on the external intercostals to inflate the lungs, resulting in a more rapid respiration rate, excessive energy consumption, and incomplete ventilation of the lungs.
time-domain measures of HRV: indices like SDNN that measure the degree to which the IBIs between successive heartbeats vary.
torr: the unit of atmospheric pressure, named after Torricelli, which equals 1 millimeter of mercury (mmHg) and is used to measure end-tidal CO2.
trapezius-scalene placement: active SEMG electrodes are located on the upper trapezius and scalene muscles to measure respiratory effort.
ultra-low-frequency (ULF) band: the HRV frequency range below 0.003 Hz. Very-slow biological processes may contribute to this band, including circadian rhythms, core body temperature, metabolism, and the renin-angiotensin system. PNS and SNS contributions are possible.
vagal withdrawal: reduced parasympathetic (vagal) activity, often occurring in response to stress or excessive effort during training.
vascular tone rhythm: the rhythmic oscillation in blood vessel diameter that contributes to blood pressure regulation and HRV.
ventral vagal complex: in polyvagal theory, the myelinated vagal pathway proposed to support social engagement and calm physiological states.
very-low-frequency (VLF) band: the HRV frequency range of 0.003-0.04 Hz that may represent temperature regulation, plasma renin fluctuations, endothelial and physical activity influences, and possible intrinsic cardiac, PNS, and SNS contributions.
References
Altini, M., & Plews, D. (2021). What is behind changes in resting heart rate and heart rate variability? Sensors, 21(23), 7932. https://doi.org/10.3390/s21237932
Bridges, L. J., Denham, S. A., & Ganiban, J. M. (2004). Definitional issues in emotion regulation research. Child Development, 75(2), 340-345. https://doi.org/10.1111/j.1467-8624.2004.00675.x
Brown, D. K., Barton, J. L., & Gladwell, V. F. (2013). Viewing nature scenes positively affects recovery of autonomic function following acute-mental stress. Environmental Science & Technology, 47(11), 5562-5569. https://doi.org/10.1021/es305019p
Buchheit, M., Laursen, P. B., Al Haddad, H., & Ahmaidi, S. (2009). Exercise-induced plasma volume expansion and post-exercise parasympathetic reactivation. European Journal of Applied Physiology, 105, 471-481. https://doi.org/10.1007/s00421-008-0925-1
Carter, R., Cheuvront, S. N., Wray, D. W., Kolka, M. A., Stephenson, L. A., & Sawka, M. N. (2005). The influence of hydration status on heart rate variability after exercise heat stress. Journal of Thermal Biology, 30(7), 495-502. https://doi.org/10.1016/j.jtherbio.2005.05.006
Constant, I., Laude, D., Murat, I., & Elghozi, J.-L. (1999). Pulse rate variability is not a surrogate for heart rate variability. Clinical Science, 97(4), 391-397. https://doi.org/10.1042/cs0970391
de Oliveira, R. A. M., Araújo, L. F., de Figueiredo, R. C., Goulart, A. C., Schmidt, M. I., Barreto, S. M., & Ribeiro, A. L. P. (2017). Coffee consumption and heart rate variability: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) Cohort Study. Nutrients, 9(7), 741. https://doi.org/10.3390/nu9070741
Drew, B. J., Califf, R. M., Funk, M., Kaufman, E. S., Krucoff, M. W., Laks, M. M., Macfarlane, P. W., Sommargren, C., Swiryn, S., & Van Hare, G. F. (2004). Practice standards for electrocardiographic monitoring in hospital settings: An American Heart Association scientific statement. Circulation, 110(17), 2721-2746. https://doi.org/10.1161/01.CIR.0000145144.56673.59
Gevirtz, R. N. (2021). Personal communication regarding HRVB training goals.
Gevirtz, R. N., Lehrer, P. M., & Schwartz, M. S. (2016). Cardiorespiratory biofeedback. In M.S. Schwartz & F. Andrasik (Eds.). Biofeedback: A practitioner's guide (4th ed.). The Guilford Press.
Gilbert, C. (2012). Pulse oximetry and breathing training. Biofeedback, 40(4), 137-141. https://doi.org/10.5298/1081-5937-40.4.04
Ginsberg, J. P., Berry, M. E., & Powell, D. A. (2010). Cardiac coherence and posttraumatic stress disorder in combat veterans. Alternative Therapies in Health and Medicine, 16(4), 52-60.
Gonzales, J. U., Elavsky, S., Cipryan, L., Jandačková, V., Burda, M., & Jandačka, D. (2023). Influence of sleep duration and sex on age-related differences in heart rate variability: Findings from program 4 of the HAIE study. Sleep Medicine, 106, 69-77. https://doi.org/10.1016/j.sleep.2023.03.029
Grant, J., Wally, C., & Truitt, A. (2010). The effects of Kargyraa throat-singing and singing a fundamental note on heart rate variability [Abstract]. Poster presented at the meeting of the Biofeedback Foundation of Europe, Rome, Italy.
Grossman, P., & Kollai, M. (1993). Respiratory sinus arrhythmia, cardiac vagal tone, and respiration: Within- and between-individual relations. Psychophysiology, 30(5), 486-495. https://doi.org/10.1111/j.1469-8986.1993.tb02072.x
Guarino, D., Nannipieri, M., Iervasi, G., Taddei, S., & Bruno, R. M. (2017). The role of the autonomic nervous system in the pathophysiology of obesity. Frontiers in Physiology, 8, 665. https://doi.org/10.3389/fphys.2017.00665
Hemon, M. C., & Phillips, J. P. (2016). Comparison of foot finding methods for deriving instantaneous pulse rates from photoplethysmographic signals. Journal of Clinical Monitoring and Computing, 30(2), 157-168. https://doi.org/10.1007/s10877-015-9695-6
Jan, H.-Y., Chen, M.-F., Fu, T.-C., Lin, W.-C., Tsai, C.-L., & Lin, K.-P. (2019). Evaluation of coherence between ECG and PPG derived parameters on heart rate variability and respiration in healthy volunteers with/without controlled breathing. Journal of Medical and Biological Engineering, 39, 783-795. https://doi.org/10.1007/s40846-019-00468-9
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. Hyperion Books.
Kalil, G. Z., & Haynes, W. G. (2012). Sympathetic nervous system in obesity-related hypertension: Mechanisms and clinical implications. Hypertension Research, 35(1), 4-16. https://doi.org/10.1038/hr.2011.173
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. Wiley-Blackwell.
Khazan, I. Z. (2019). Biofeedback and mindfulness in everyday life: Practical solutions for improving your health and performance while managing stress. New Harbinger Publications.
Khazan, I. Z. (2026). Personal communication regarding resonance frequency and breathing rate.
Kim, H. J., Ryu, H., Kang, E., Kang, M., Han, M., Song, S. H., Lee, J., Jung, J. Y., Lee, K.-B., Sung, S., Seong, E. Y., Ahn, C., & Oh, K.-H. (2021). Metabolic acidosis is an independent risk factor of renal progression in Korean chronic kidney disease patients: The KNOW-CKD study results. Frontiers in Medicine, 8, 707588. https://doi.org/10.3389/fmed.2021.707588
Kitabchi, A. E., Umpierrez, G. E., Miles, J. M., & Fisher, J. N. (2009). Hyperglycemic crises in adult patients with diabetes. Diabetes Care, 32(7), 1335-1343. https://doi.org/10.2337/dc09-9032
Kok, B. E., & Singer, T. (2017). Phenomenological fingerprints of four meditations: Differential state changes in affect, mind-wandering, meta-cognition, and interoception. Mindfulness, 8, 218-231. https://doi.org/10.1007/s12671-016-0594-9
Lagos, L., Vaschillo, E., Vaschillo, B., Lehrer, P., Bates, M., & Pandina, R. (2011). Virtual reality assisted heart rate variability biofeedback as a strategy to improve golf performance: A case study. Biofeedback, 39(1), 15-20. https://doi.org/10.5298/1081-5937-39.1.11
Lehrer, P. M. (2007). Biofeedback training to increase heart rate variability. In P. M. Lehrer, R. M. Woolfolk, & W. E. Sime (Eds.). Principles and practice of stress management (3rd ed.). The Guilford Press.
Lehrer, P. M. (2013). How does heart rate variability biofeedback work? Resonance, the baroreflex, and other mechanisms. Biofeedback, 41, 26-31. https://doi.org/10.5298/1081-5937-41.1.02
Lehrer, P. M., & Gevirtz, R. (2014). Heart rate variability: How and why does it work? Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2014.00756
Lehrer, P., Vaschillo, B., Zucker, T., Graves, J., Katsamanis, M., Aviles, M., & Wamboldt, F. (2013). Protocol for heart rate variability biofeedback training. Biofeedback, 41(3), 98-109.
Lehrer, P. M., Vaschillo, E., & Vaschillo, B. (2000). Resonant frequency biofeedback training to increase cardiac variability: Rationale and manual for training. Applied Psychophysiology and Biofeedback, 25(3), 177-191. https://doi.org/10.1023/a:1009554825745
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., Sgobba, P., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Applied Psychophysiology and Biofeedback, 45(3), 109-129. https://doi.org/10.1007/s10484-020-09466-z
McCraty, R. (2013). Personal communication regarding the benefits of heartfelt emotion.
McCraty, R., Atkinson, M., Tiller, W. A., Rein, G., & Watkins, A. D. (1995). The effects of emotions on short-term power spectrum analysis of heart rate variability. American Journal of Cardiology, 76(14), 1089-1093. https://doi.org/10.1016/s0002-9149(99)80309-9
McCraty, R., Atkinson, M., Tomasino, D., & Bradley, R. T. (2006). The coherent heart. Institute of HeartMath.
McCraty, R., Atkinson M., Tomasino, D., & Bradley, R. T. (2009). The coherent heart: Heart-brain interactions, psychophysiological coherence, and the emergence of system-wide order. Integral Review, 5(2), 10-115.
Medeiros, R. F., Silva, B. M., Neves, F. J., Rocha, N. G., Sales, A. R. K., & Nobrega, A. C. (2011). Impaired hemodynamic response to mental stress in subjects with prehypertension is improved after a single bout of maximal dynamic exercise. Clinics, 66(9), 1523-1529. https://doi.org/10.1590/S1807-59322011000900003
Nakayama, N., Miyachi, M., Tamakoshi, K., Hayashi, T., Negi, K., Watanabe, K., & Hirai, M. (2021). Decreased continuous sitting time increases heart rate variability in patients with cardiovascular risk factors. PLoS ONE, 16(6), e0253399. https://doi.org/10.1371/journal.pone.0253399
Ng, A. E., Black, L. I., & Adjaye-Gbewonyo, D. (2026). Short sleep duration and sleep difficulties among adults: United States, 2024 (NCHS Data Brief No. 559). National Center for Health Statistics. https://doi.org/10.15620/cdc/252438
Peper, E., & Gibney, K. H. (2005). Muscle biofeedback at the computer: A manual to prevent repetitive strain injury (RSI) by taking the guesswork out of assessment, monitoring, and training. Biofeedback Foundation of Europe.
Pinto, A. J., Bergouignan, A., Dempsey, P. C., Roschel, H., Owen, N., Gualano, B., & Dunstan, D. W. (2023). Physiology of sedentary behavior. Physiological Reviews, 103(4), 2561-2622. https://doi.org/10.1152/physrev.00022.2022
Porges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2), 116-143. https://doi.org/10.1016/j.biopsycho.2006.06.009
Saraiva, B. T. C., Tebar, W. R., Furuta, D. T., Silva, S. C. B., Antunes, E. P., Sousa, G., Ferrari, G., Vanderlei, L. C. M., & Christofaro, D. G. D. (2026). Association of meeting the 24-hour movement guidelines with heart rate variability in adults. European Journal of Applied Physiology. https://doi.org/10.1007/s00421-025-06115-3
Shaffer, F., & Moss, D. (2006). Biofeedback. In Y. Chun-Su, E. J. Bieber, & B. Bauer (Eds.). Textbook of complementary and alternative medicine (2nd ed.). Informa Healthcare.
Shaffer, F., Bergman, S., & Dougherty, J. (1998). End-tidal CO2 is the best indicator of breathing effort [Abstract]. Applied Psychophysiology and Biofeedback, 23(2).
Shaffer, F., Bergman, S., & White, K. (1997). Indicators of diaphragmatic breathing effort [Abstract]. Applied Psychophysiology and Biofeedback, 22(2), 145.
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 258. https://doi.org/10.3389/fpubh.2017.00258
Shaffer, F., Greve, E., & Reinagel, K. (1996). Predictors of inhalation volume [Abstract]. Biofeedback and Self-Regulation, 21(4), 352.
Shaffer, F., Mayhew, J., Bergman, S., Dougherty, J., & Irwin, D. (1999). Designer jeans increase breathing effort [Abstract]. Applied Psychophysiology and Biofeedback, 24(2), 124-125.
Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: An integrative review of the heart's anatomy and heart rate variability. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2014.01040
Taub, E., & School, P. J. (1978). Some methodological considerations in thermal biofeedback training. Behavior Research Methods & Instrumentation, 10(5), 617-622. https://doi.org/10.3758/BF03205359
Thayer, J. F., & Sternberg, E. (2006). Beyond heart rate variability: Vagal regulation of allostatic systems. Annals of the New York Academy of Sciences, 1088(1), 361-372. https://doi.org/10.1196/annals.1366.014
Tsunetsugu, Y., Park, B. J., & Miyazaki, Y. (2010). Trends in research related to "Shinrin-yoku" (taking in the forest atmosphere or forest bathing) in Japan. Environmental Health and Preventive Medicine, 15(1), 27-37. https://doi.org/10.1007/s12199-009-0091-z
Vansickle, J., Putnam, R., Harris, M., Garcia, M., Bell, B., Nelson, M., & Lowery, L. (2020). Caffeine intake does not negatively affect heart rate variability in physically active university students: Preliminary findings. Current Development in Nutrition, 4(Supplement 2), 1770. https://doi.org/10.1093/cdn/nzaa066_025
Vaschillo, E., Lehrer, P., Rishe, N., & Konstantinov, M. (2002). Heart rate variability biofeedback as a method for assessing baroreflex function: A preliminary study of resonance in the cardiovascular system. Applied Psychophysiology and Biofeedback, 27, 1-27. https://doi.org/10.1023/a:1014587304314
Vaschillo, E. G., Vaschillo, B., & Lehrer, P. M. (2006). Characteristics of resonance in heart rate variability stimulated by biofeedback. Applied Psychophysiology and Biofeedback, 31(2), 129-142. https://doi.org/10.1007/s10484-006-9009-3
Vaschillo, E. G., Vaschillo, B., Pandina, R. J., & Bates, M. E. (2011). Resonances in the cardiovascular system caused by rhythmical muscle tension. Psychophysiology, 48, 927-936. https://doi.org/10.1111/j.1469-8986.2010.01156.x
Wally, C., Korenfeld, I., Brooks, K., Carrell, D., Lau, D., Peterson, J., Schafer, M., Truitt, A., Fuller, J., Westermann-Long, A., & Korenfeld, D. (2011). Chanting "Om" increases heart rate variability by slowing respiration [Abstract]. Applied Psychophysiology and Biofeedback, 36, 223.
Watso, J. C., & Farquhar, W. B. (2019). Hydration status and cardiovascular function. Nutrients, 11(8), 1866. https://doi.org/10.3390/nu11081866
Ylitalo, A., Airaksinen, K. E. J., Sellin, L., & Huikuri, H. V. (1999). Effects of combination antihypertensive therapy on baroreflex sensitivity and heart rate variability in systemic hypertension. American Journal of Cardiology, 83(6), 885-889. https://doi.org/10.1016/s0002-9149(98)01067-4
Zerr, C., Kane, A., Vodopest, T., Allen, J., Fluty, E., Gregory, J., DeBold, M., Schultz, D., Robinson, G., Golan, R., Hannan, J., Bowers, S., Cangelosi, A., Korenfeld, D., Jones, D., Shepherd, S., Burklund, Z., Spaulding, K., Hoffman, W., & Shaffer, F. (2014). HRV biofeedback training raises temperature and lowers skin conductance. Applied Psychophysiology and Biofeedback, 39(3), 299. https://doi.org/10.1007/s10484-014-92549
Zerr, C., Kane, A., Vodopest, T., Allen, J., Hannan, J., Fabbri, M., Williams, C., Cangelosi, A., Owen, D., Cary, B., & Shaffer, F. (2015). Does inhalation-to-exhalation ratio matter in heart rate variability biofeedback? Applied Psychophysiology and Biofeedback, 40(2), 135. https://doi.org/10.1007/s10484-015-9282-0
Return to Top