
Psychophysiology
What You Will Learn
Imagine sitting in a darkened movie theater as a terrifying scene unfolds on screen. Your heart races, your palms sweat, your pupils dilate, and your neck and shoulder muscles brace for impact. Yet, no one has touched you. What is happening? Your psychological experience is directly changing your body. This powerful connection between mind and body is the foundation of psychophysiology, and it will transform how you understand your clients' symptoms and design their treatment.
In this unit, you will explore the principles that govern how psychological and physiological processes influence one another. From Green, Green, and Walters' revolutionary psychophysiological principle to the nuances of autonomic balance, activation theory, and the surprisingly powerful placebo effect, you will build the conceptual toolkit you need to conduct meaningful psychophysiological assessments and design individualized biofeedback interventions.

This powerful idea is Green and Green's psychophysiological principle. Psychophysiology is the study of the interrelationship between psychological and physiological processes. As Andreassi (2007) defined it, psychophysiology examines the relations between psychological manipulations and resulting physiological responses in living organisms to clarify the connection between mental and bodily processes. This interrelationship is dynamic and bidirectional—the mind shapes the body, and the body shapes the mind.

This section introduces three foundational ideas that will guide your clinical thinking throughout this unit. First, understanding psychophysiological principles helps you see how disease processes develop and how your interventions achieve their effects. Second, the idiographic approach—which emphasizes individual differences—is essential to biofeedback because each client's response to stressors is unique, specific, and often complex. Third, this unit will challenge the simplistic view that the sympathetic fight-or-flight response is our only stress reaction; the parasympathetic branch expands our response options through immobilization, feigning death, passive avoidance, shutdown, and social engagement supported by the release of oxytocin.
To treat your clients effectively, you need to discover their characteristic responses to stressors during a psychophysiological profile administered at the assessment stage. For example, if hand temperature falls and respiration rate increases during math and visual imagery stressors, you might train your client to maintain hand temperature around 90°F (32.2°C) while breathing below 7 breaths per minute. This individualized approach may be superior to a standard protocol that disregards your client's unique response pattern, known as their response stereotypy—a consistent pattern of physiological responses to stimuli of similar intensity and emotional quality.

BCIA Blueprint Coverage
This unit complements the BCIA HRV Biofeedback Blueprint. It covers the Psychophysiological Principle, Homeostasis, Autonomic Balance, Psychophysiological Measurements, Orienting and Defensive Responses, Activation and Habituation, Situational Specificity, Law of Initial Values (LIV), Generalization of Biofeedback Training, and the Placebo Effect.
🎧 Listen to the Full Chapter Lecture
🎧 Mini-Lecture: Psychophysiology
The Psychophysiological Principle: Where Mind Meets Body
This section examines the foundational principle that links every physiological change to a corresponding psychological change, and vice versa. Understanding this bidirectional relationship is essential because it explains why biofeedback works and guides how you design interventions. Green, Green, and Walters (1970) articulated what became the psychophysiological principle:
Every change in the physiological state is accompanied by an appropriate change in the mental emotional state, conscious or unconscious, and conversely, every change in the mental emotional state, conscious or unconscious, is accompanied by an appropriate change in the physiological state.
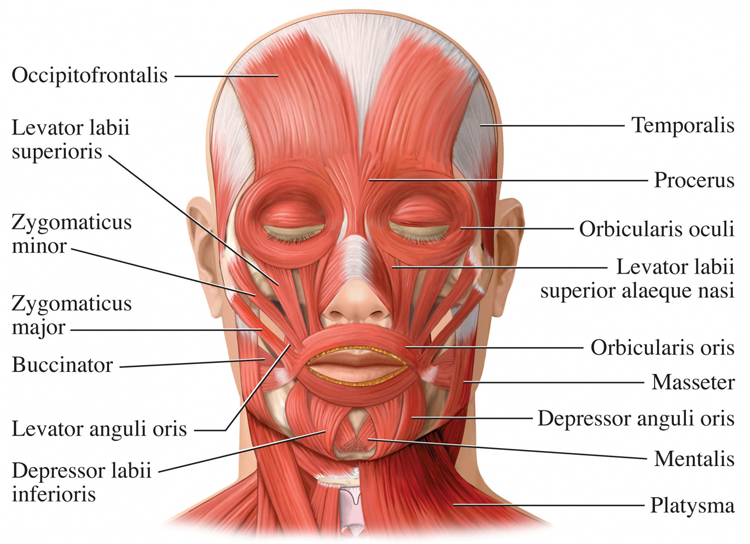
This principle was revolutionary because it formalized what clinicians had long suspected—that the mind-body relationship runs in both directions simultaneously. Consider a concrete example: facial muscle contraction can influence emotion, and emotion can influence facial muscle contraction. Botox injections, which paralyze facial muscles to treat wrinkles, actually reduce the intensity of a person's emotional experiences—a striking demonstration that changing physiology changes psychology.

The psychophysiological principle states that every physiological change is accompanied by a corresponding psychological change, and vice versa. This bidirectional relationship is the theoretical foundation of biofeedback practice.
Homeostasis: The Body's Internal Balancing Act
This section covers how the body maintains internal stability and what happens when that stability breaks down under chronic stress. You will encounter three related concepts—homeostasis, the boundary model, and allostasis—each of which has direct implications for how you assess and treat your clients. Homeostasis is the process that maintains the body's internal environment within healthy physiological limits. Claude Bernard introduced the foundational concept by asserting that the stability of the internal environment is the condition of a healthy life, and Cannon (1939) coined the term homeostasis in 1932, elaborating on it in The Wisdom of the Body.
🎧 Mini-Lecture: Homeostasis and Allostasis
The body achieves homeostasis for specific variables, like blood pressure, through interlocking negative and positive feedback systems. Check out the Bozeman Science YouTube video Positive and Negative Feedback Loops. The boundary model refines this picture by challenging the idea of rigid set points, proposing instead that physiological processes are maintained within acceptable ranges. This distinction matters clinically because it means your clients' physiological values need not hit an exact number to be healthy—they need to stay within a functional window.
Allostasis—the maintenance of stability through change—complements homeostasis by emphasizing how the body anticipates challenges and adapts through behavior and physiological adjustment. Therapists leverage allostasis when they teach patients to use an abbreviated relaxation exercise, such as low-and-slow breathing, before anticipated stressors like traffic jams. However, when stressors are acute or repeatedly occur, this adaptive system can become harmful. McEwen and Seeman's (1999) allostatic load model proposes that the cumulative burden of chronic stress produces damaging physiological changes—a concept that connects directly to many of the conditions you will treat.

Homeostasis maintains the body's internal environment within healthy limits through negative and positive feedback systems. The boundary model proposes flexible ranges rather than rigid set points. Allostasis complements homeostasis by anticipating challenges, and chronic activation can produce harmful allostatic load.
Autonomic Balance: The Sympathetic-Parasympathetic Tug of War
This section explores how the ratio of sympathetic to parasympathetic activation affects health and disease. Understanding autonomic balance will help you interpret your clients' baseline assessments and recognize when dominance by either branch may contribute to their presenting complaints. Wenger (1972) called the ratio of sympathetic to parasympathetic activation autonomic balance, proposing that resting individuals are located along a continuum ranging from sympathetic nervous system (SNS) to parasympathetic nervous system (PNS) dominance.
Wenger quantified this concept using normally distributed A-bar scores, calculated from a battery of autonomic measurements. Low A-bar scores indicate SNS dominance, while high A-bar scores suggest PNS dominance; most individuals show intermediate scores. Wenger and colleagues reported that individuals with low A-bar scores, whom he called sympathicotonics, suffered an elevated incidence of neurotic, psychotic, psychosomatic, and medical disorders.
Extreme scores on either end of the continuum appear to create clinical vulnerability. Where SNS dominance (low A-bar scores) may result in cardiac arrhythmia and essential hypertension, PNS dominance (high A-bar scores) may be associated with asthma, colitis, and hypotension. The healthiest pattern involves intermediate A-bar scores where neither the SNS nor the PNS overwhelms the other—a state of flexible, dynamic balance.
Autonomic balance is the ratio of sympathetic to parasympathetic activation. Extreme dominance of either branch predisposes individuals to different disorders. The healthiest pattern involves intermediate balance where neither branch overwhelms the other.
Comprehension Questions
- In your own words, explain the psychophysiological principle and give an example of how it applies to biofeedback practice.
- How does allostasis differ from homeostasis, and why is this distinction relevant for clinicians?
- What clinical conditions might you expect in a client who shows extreme SNS dominance versus extreme PNS dominance?
Psychophysiological Measurements: Tonic, Phasic, and Spontaneous Activity
This section introduces three categories of physiological activity that you will encounter in every assessment and training session. Distinguishing between tonic, phasic, and spontaneous activity is essential for accurate measurement and sound clinical interpretation. Tonic activity refers to the background level of physiological activity—the magnitude measured over a specified period before stimulating the subject. A resting baseline, where a participant sits quietly for 3 or 5 minutes without breathing or relaxation instructions or feedback, measures tonic activity.
🎧 Mini-Lecture: Tonic and Phasic Activity
Clinicians obtain pre- and post-baselines to measure psychophysiological change in variables like heart rate variability or hand temperature within and across training sessions. In contrast, phasic activity is a discrete response evoked by a specific stimulus, such as a startle reaction to an unexpected sound. Because subjects continuously react to environmental and internal stimuli that clinicians cannot directly observe, interpreting phasic activity can be challenging.

Spontaneous responses are physiological changes that occur in the absence of any detectable stimulus. These matter to both researchers and clinicians because they can confound the measurement of phasic activity. For example, if a spontaneous increase in skin conductance coincides with the presentation of an emotionally-charged slide, a researcher could mistakenly attribute the full conductance increase to the stimulus (Stern, Ray, & Quigley, 2001). Being aware of spontaneous responses will help you avoid similar misinterpretations in your clinical assessments.
Psychophysiologists distinguish three types of activity: tonic (background levels), phasic (discrete responses to specific stimuli), and spontaneous (changes without detectable stimuli). Understanding these distinctions is essential for accurate measurement and interpretation of physiological data.
Orienting and Defensive Responses: How We React to Novel Stimuli
This section examines two distinct physiological response patterns that emerge when your clients encounter novel or intense stimuli. Knowing how these responses differ will sharpen your ability to interpret assessment data and understand why some physiological reactions persist while others fade. Pavlov's (1927) orienting response is essentially a "What is it?" reaction to novel stimuli, such as the sound of a vase crashing.
The orienting response is a coordinated pattern that includes increased sensory sensitivity, head (and ear) turning toward the stimulus, increased muscle tone with reduced movement, EEG desynchrony (indicating heightened cortical alertness), peripheral vasoconstriction paired with cephalic vasodilation, a rise in skin conductance, heart rate slowing, and slower, deeper breathing. Notice that this pattern is designed to increase information intake—the body prepares to learn about the new stimulus. Critically, orienting responses habituate rapidly because they are no longer needed once the organism has evaluated the novel stimulus.
The defensive response serves the opposite purpose: it is a slowly habituating pattern that limits harm from intense stimulation. This pattern includes reduced sensory sensitivity, a tendency to move away from the stimulus, heart rate increase, and both peripheral and cephalic vasoconstriction. Where the orienting response opens sensory channels to gather information, the defensive response narrows them to protect the organism—a distinction with direct implications for understanding why some clients remain hypervigilant long after a stressor has passed.
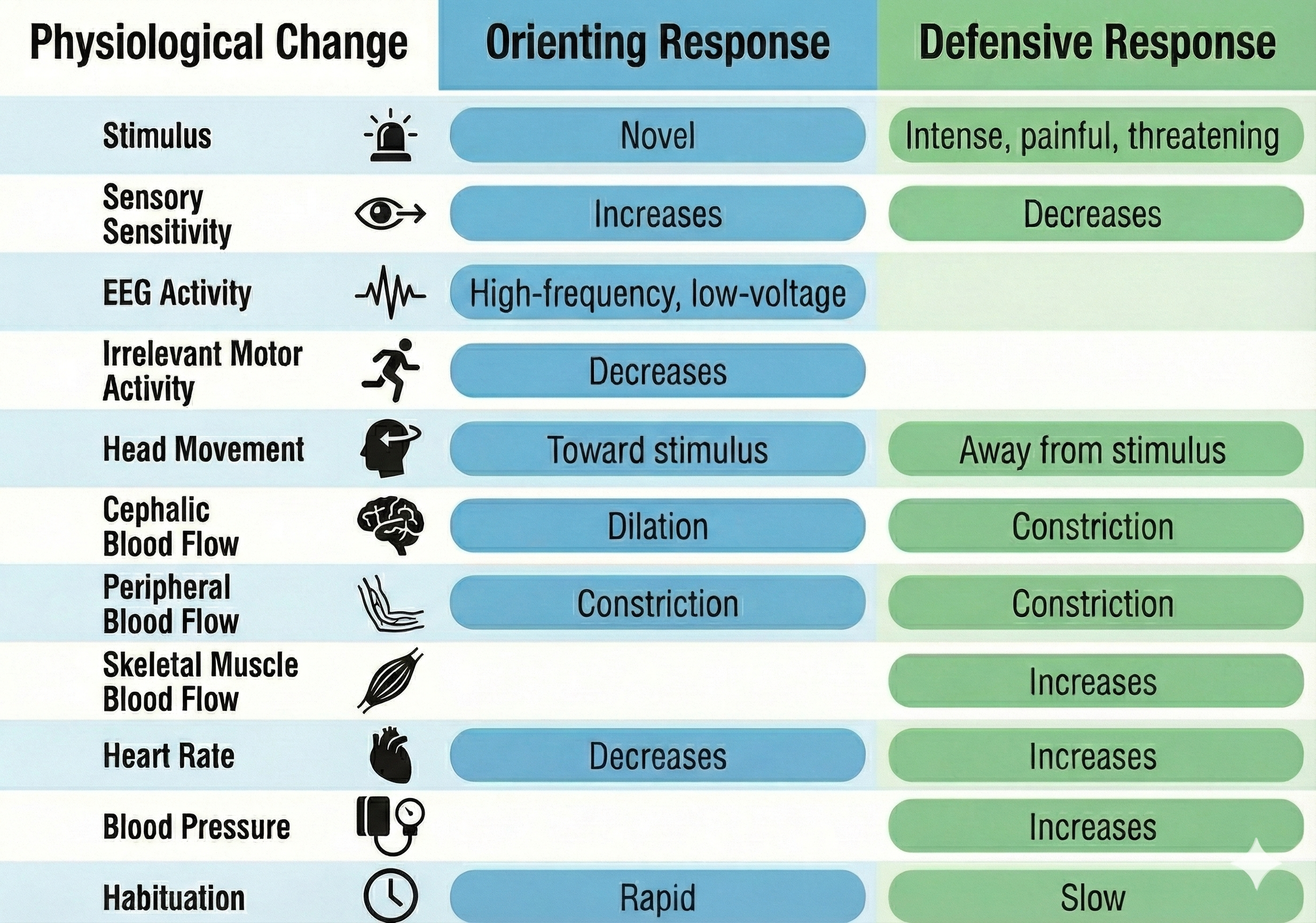
The orienting response is a rapidly habituating "What is it?" reaction that increases sensory sensitivity and information intake. The defensive response is a slowly habituating pattern that limits harm from intense stimulation by reducing sensory input. Their contrasting habituation rates have important clinical implications for understanding persistent stress responses.
Activation Theory: The Rise of Arousal
This section introduces activation theory, a foundational framework for understanding arousal, and then examines the important criticisms that reshaped how psychophysiologists think about physiological responses. These criticisms led directly to the individualized assessment approach central to biofeedback practice. Activation was Duffy's (1972) term for arousal, a concept that originated in Cannon's (1915) idea of the body's integrated preparation to fight or flee a potential threat.
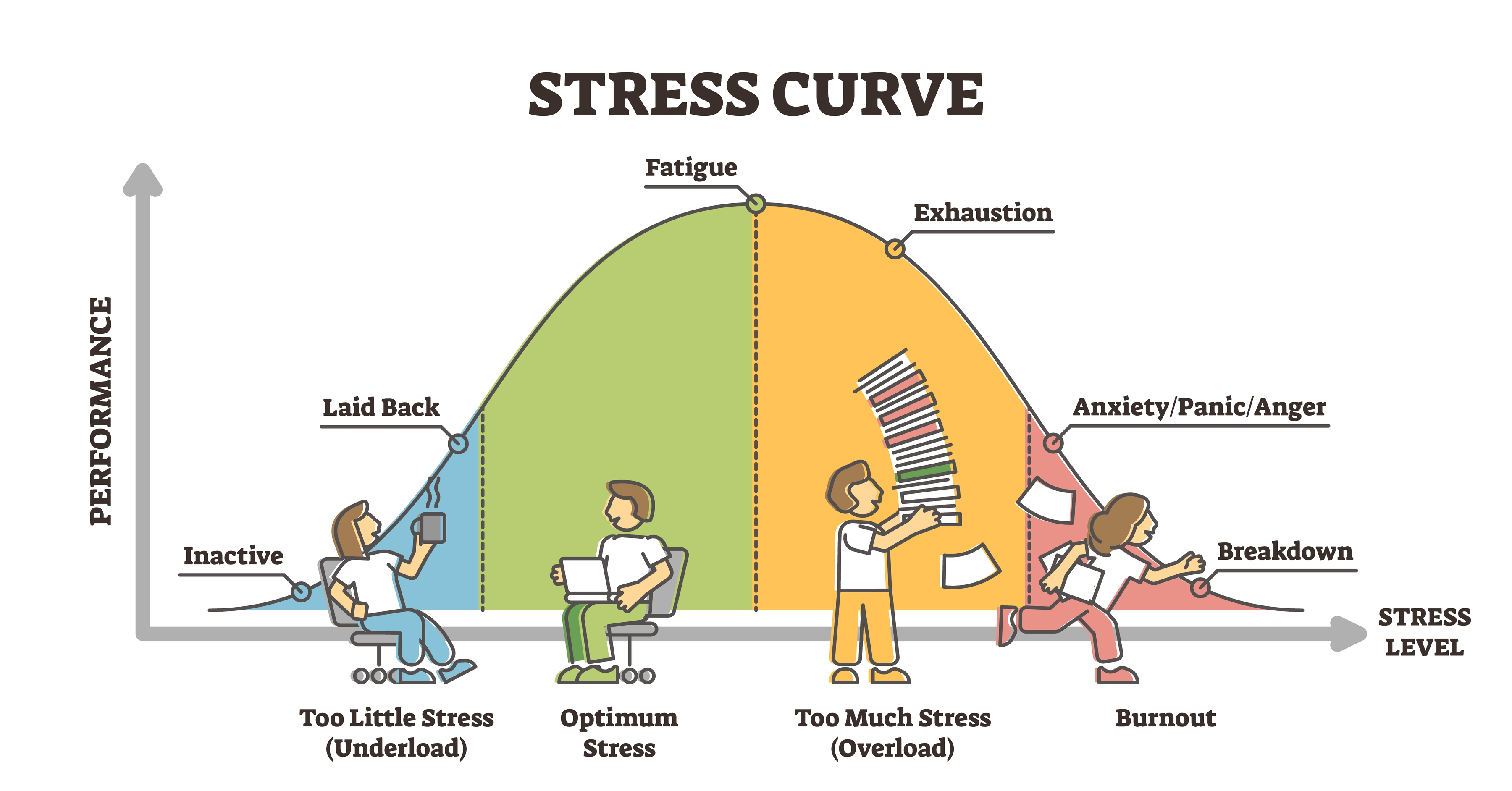
Activation implies a unidimensional continuum ranging from low to high arousal. High activation might involve elevated blood pressure, heart rate, and respiration rate, while low activation would involve reduced values for these variables. Duffy (1957) hypothesized that performance rises with increased arousal to an optimal level for a given task and then declines with further arousal—a relationship described as the inverted U-shaped curve. Task complexity and novelty influence where the optimal level falls: more complex and novel tasks require lower arousal for peak performance, a principle directly relevant to optimal performance training for athletes and military personnel.
Challenges to Activation Theory: Why Arousal Is Not a Single Dimension
While activation theory provides a useful starting point, Lacey (1967) and others demonstrated that it oversimplifies the physiology of stress and arousal. This section covers four critical refinements—multidimensional arousal, response stereotypy, stimulus-response specificity, and directional fractionation—that will directly shape how you conduct assessments and interpret your clients' data.
Lacey argued that researchers should differentiate between autonomic, behavioral, and cortical arousal because these forms of activation are not interchangeable. For example, when heterosexual men observe slides of nude women, heart rate may increase while finger blood flow remains unchanged (Stern, Ray, & Davis, 1980). If a clinician relies on a single measure as an arousal index, they risk missing the full picture—a cautionary principle for anyone conducting psychophysiological assessments.
Lacey also demonstrated that individuals exhibit response stereotypy—consistent physiological response patterns when encountering stimuli of similar intensity that elicit similar emotions. A patient may raise her heart rate and blood pressure whether she is delivering a report during a business meeting or completing an assignment under time pressure. This individual-specific patterning occurs because clients possess different diatheses (vulnerabilities) and enter treatment with unique learning histories. During assessment, clinicians conduct a psychophysiological profile (PSP) to identify each client's response stereotypy by presenting several mild stressors.
Stimulus-Response Specificity and Emotional Response Patterns
This section extends the critique of activation theory by examining how specific stimuli and specific emotions each produce distinctive physiological signatures. These findings reinforce the case for individualized assessment and help explain why a single biofeedback modality may not address all of a client's symptoms. Stimulus-response specificity is the principle that specific stimuli elicit distinctive response patterns in most individuals rather than simply raising or lowering overall activation. For example, individuals tend to increase skeletal muscle tone when challenged to compete.
Situational specificity is an application of stimulus-response specificity. It means that a physiological response such as blood pressure elevation does not occur randomly—it is most likely in situations with particular characteristics, including the location, time of day, activity, people present, and the individual's emotional state. A client's elevated blood pressure may be classically or operantly conditioned, and they may be unaware of having learned this response since blood pressure symptoms are largely "silent" and both conditioning processes involve implicit learning. Due to associative learning, the presence of one or more situational cues may elicit a complete physiological response.
Primary emotions are associated with unique physiological changes, a concept known as emotional response specificity. The six primary facial expressions are surprise, anger, sadness, disgust, fear, and happiness. Research by Ekman and colleagues showed that anger increases heart rate and skin temperature, fear increases heart rate but decreases skin temperature, and happiness increases heart rate without affecting skin temperature. Schwartz, Weinberger, and Singer (1981) further demonstrated that cardiovascular patterns distinguished anger from fear (via blood pressure) and anger and fear from happiness and sadness, while Ax (1953) reported that 7 of 14 autonomic measures discriminated between fear and anger.
Responses to a stimulus can be complex, with some physiological indices increasing while others decrease. Lacey called this intricate pattern directional fractionation. For example, when a Capitol Hill police officer hears a suspicious noise, EEG and skin conductance may increase cortical activation while gastrointestinal tract activity simultaneously decreases. Directional fractionation is the final nail in the coffin of the simple arousal continuum—it shows that the body does not respond as a unified whole but produces nuanced, context-specific patterns that demand the kind of multi-channel assessment central to biofeedback practice.
Habituation: The Gradual Fading of Response
Habituation is the opposite of arousal—a gradual weakening or disappearance of a response to a constant stimulus. For example, after 15 trials of listening to a moderate-intensity tone, heart rate might no longer increase. Predictable, low-intensity stimuli that convey no new information and require no response readily produce habituation, while intense, complex, and unique stimuli that demand a response inhibit habituation.
The orienting response and defensive response differ dramatically in their speed of habituation, a distinction with clinical relevance. Orienting responses habituate rapidly, allowing the organism to redirect attention to new stimuli. Defensive responses habituate very slowly, which helps explain why clients exposed to chronic or intense stressors—such as veterans with combat trauma or first responders with repeated critical incident exposure—may maintain elevated physiological reactivity long after the original threat has passed.
Activation theory, while useful as a starting point, oversimplifies arousal as a single dimension. Lacey and others showed that individuals exhibit response stereotypy, stimuli produce specific response patterns, emotions generate unique physiological changes, and responses often involve directional fractionation. Habituation is the gradual reduction in response to constant stimulation, with orienting responses habituating rapidly and defensive responses habituating slowly.
Comprehension Questions
- Why is it important for clinicians to distinguish between tonic and phasic activity when interpreting psychophysiological data?
- How do the orienting response and defensive response differ in their physiological patterns and habituation rates?
- What are the main criticisms of activation theory, and how does the concept of response stereotypy relate to individualized biofeedback treatment?
- Explain directional fractionation and why it challenges the idea of a simple arousal continuum.
Situational Specificity: Context Shapes the Response
This section focuses on how the context surrounding a physiological response shapes its occurrence and intensity. Understanding situational specificity will transform how you take client histories, design assessments, and plan interventions. Situational specificity means that a physiological response, such as blood pressure elevation, does not occur randomly—it is most likely in situations with distinctive characteristics.
A situation's properties may include the location (office), time of day (morning), activity (conference), individuals present (employer), and the client's emotional state (anxiety). Because a client's hypertensive response may be classically or operantly conditioned through implicit learning, they may be entirely unaware of when and why their blood pressure spikes. Due to associative learning, the presence of even one or two situational cues can elicit a full physiological response.
Clinicians investigate situational specificity through multiple assessment strategies: conducting a detailed history, performing a psychophysiological stress profile (PSP), asking the client to maintain a symptom journal, and monitoring physiological responses across real-world settings—for example, measuring blood pressure both in the office and while the client is stalled in traffic. This situational information is also crucial when creating stimulus hierarchies for systematic desensitization to treat phobias.
Situational specificity means that physiological responses are tied to specific contextual features, not random. Clinicians assess this through histories, PSPs, symptom journals, and real-world monitoring. Identifying the specific situations that trigger a client's symptoms is essential for designing targeted interventions.
Law of Initial Values: Starting Points Shape Responses
This section examines how a physiological variable's starting value influences the size of the response to stimulation, and why this matters for interpreting both assessment data and training outcomes. Wilder (1967) argued that the magnitude of a physiological response depends on where that variable starts. His law of initial values (LIV) predicts that the higher the initial value of a physiological variable, the less its tendency to change. For example, a subject who normally breathes rapidly should only slightly increase their respiration rate when exposed to a loud sound, because homeostatic mechanisms (negative feedback) constrain the response.
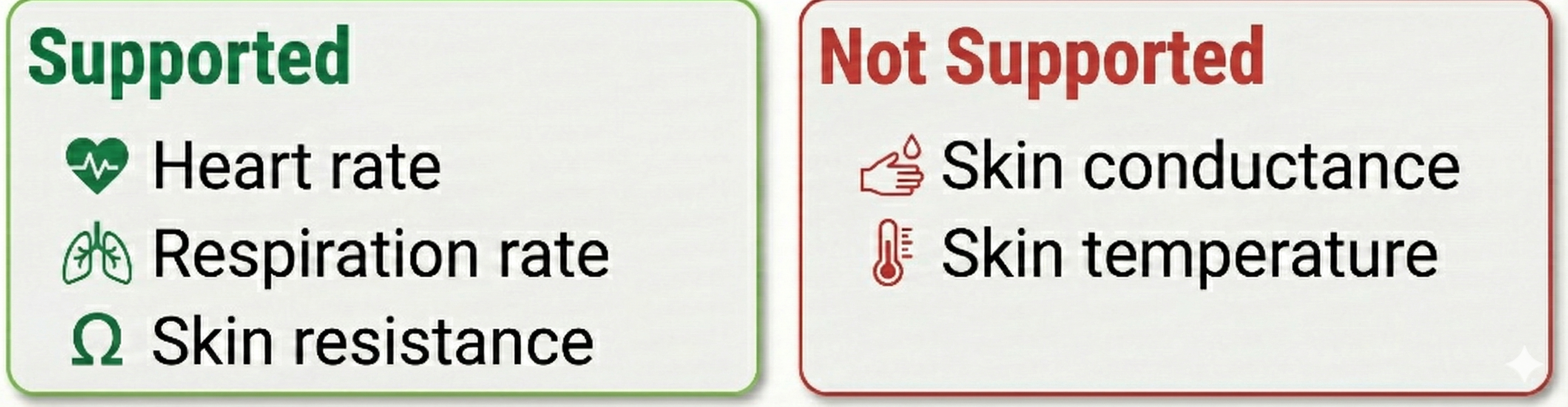
Empirical support for the LIV is selective. Hord, Johnson, and Lubin (1964) found that the LIV applies to heart rate and respiration rate but not to skin conductance or skin temperature. Stern, Ray, and Quigley (2001) confirmed support for heart rate and skin resistance but not skin conductance. Berntson and colleagues (1994) questioned the LIV's value and encouraged researchers to develop an "autonomic constraints" model tied to the underlying physiology.
Relevance of the LIV for Biofeedback
Researchers studying phasic (rapidly changing) measures may consider statistical methods to control the influence of prestimulus values on response magnitude. However, the LIV is a principle, not an absolute law, and does not apply uniformly to all subjects and response systems. Jamieson (1993) identified several factors that can influence or confound the LIV, including measurement errors, reactivity to the measurement process itself, skewed score distributions, and variance among scores. Researchers can evaluate the LIV's relevance by computing correlations between prestimulus and poststimulus values.
Geenen and van de Vijver (1993) suggested that the LIV may be less common than perceived and that statistical correction methods may harm the data more than the phenomenon itself. The practical takeaway for clinicians is straightforward: be aware that a client's starting values constrain the magnitude of change you can expect during a session, particularly for heart rate and respiration rate. However, do not assume the LIV applies to every measure you monitor, and exercise caution before applying statistical corrections that may introduce more problems than they solve.
The Law of Initial Values predicts that higher starting values produce smaller responses. While supported for heart rate and respiration rate, it does not apply to all physiological systems. It is a principle rather than an absolute law, and researchers should evaluate its relevance before applying statistical corrections.
Generalization of Biofeedback Training: Does It Transfer?
This section addresses a critical question for clinical practice: when you train one physiological site or system, does improvement automatically spread to other sites or systems? The answer has profound implications for how you design training protocols and set expectations with clients. Two well-studied cases—the key muscle hypothesis and hand-warming specificity—illustrate that generalization should never be assumed.
Key Muscle Hypothesis
The key muscle hypothesis proposed that a single muscle could serve as an index of activity in other muscle groups. Research has strongly contradicted this view: surface electromyography (SEMG) values across different sites are uncorrelated, single-site SEMG values do not correlate with generalized tension or autonomic arousal, and SEMG reductions at one site (such as the frontalis) do not automatically generalize to other sites.
The hypothesis is invalid because there is no single "key" upper body or lower body muscle group. The musculoskeletal system functions with remarkable specificity—we simultaneously contract and relax adjacent agonist-antagonist muscle pairs at a joint. This finding is clinically significant because it invalidates the once-common practice of training the frontalis muscle alone to lower autonomic arousal or relax muscles across the upper trunk. If your client presents with cervical paraspinal tension, you need to monitor and train those specific muscles, not rely on frontalis training as a proxy.

Hand-Warming Specificity
The cardiovascular system demonstrates the same precision as the musculoskeletal system. Temperature training can produce extremely site-specific changes—vasodilation in the right hand need not generalize to the left hand or the feet. Clinicians should never expect hand-warming to generalize beyond the actual site (digit) trained, though depending on the training procedure and individual differences, it may extend to other digits on the same hand or to the other hand for some clients.

The temperature map below shows mean undergraduate finger and web dorsum temperatures (Lammy et al., 2004), illustrating the natural variation in temperature across adjacent sites on the same hand.
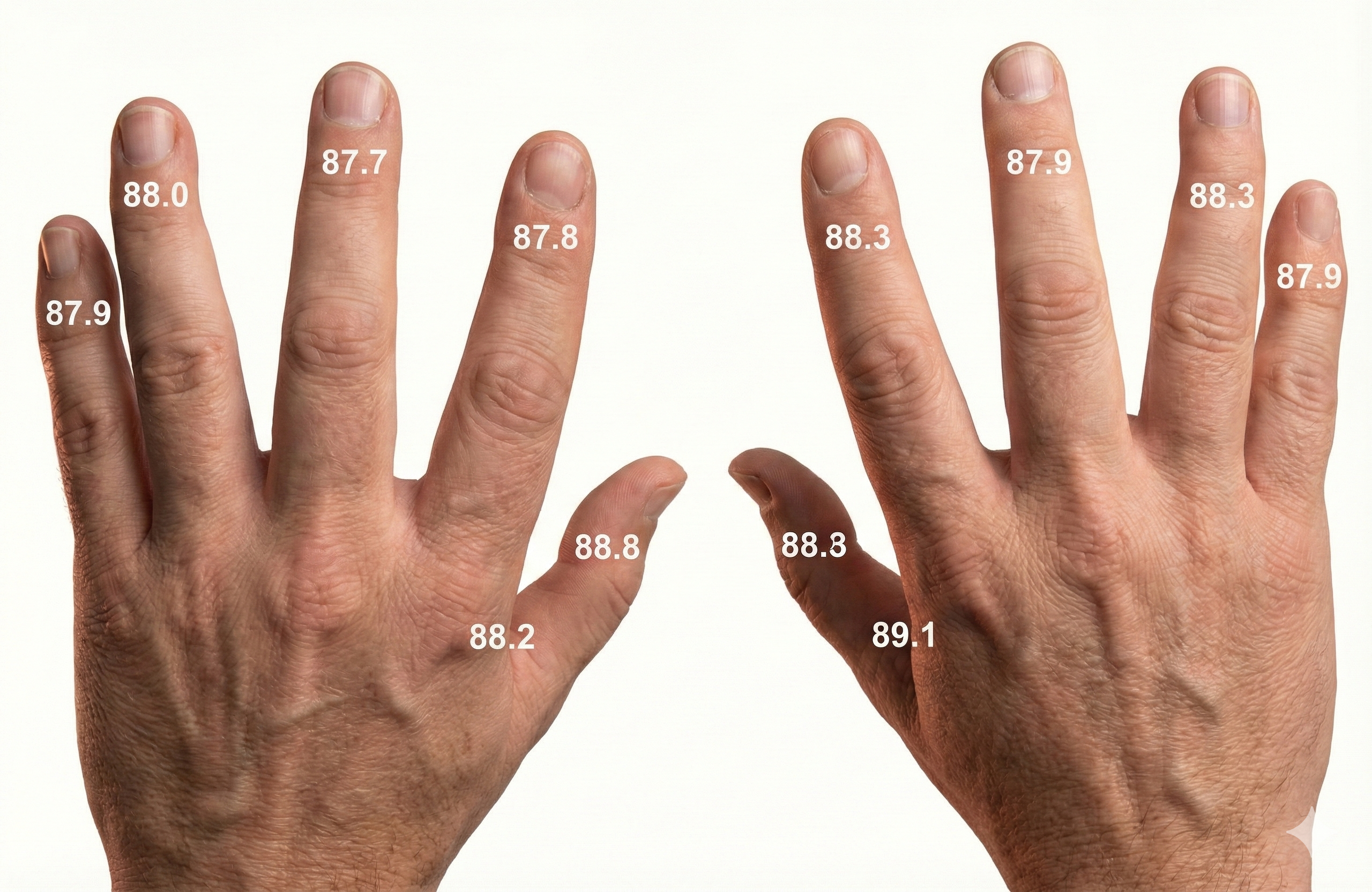
The key muscle hypothesis, which proposed that one muscle indexes activity in all others, has been thoroughly disproven. Similarly, hand temperature training produces highly site-specific changes. Clinicians should not expect biofeedback training at one site to generalize automatically to other sites.
The Placebo Effect: When Belief Becomes Biology
This section explores how inert interventions can produce real, measurable clinical responses—and why understanding this phenomenon is essential for ethical, effective biofeedback practice. Placebos are inert interventions that can produce significant clinical improvement. Both the symptoms and the therapeutic response in a placebo reaction are genuine and measurable, not imagined.
🎧 Mini-Lecture: The Placebo Effect
Check out Eric Mead's TED Talk The Magic of the Placebo.

Placebos take many forms: pharmacological (a sugar pill), procedural (sham osteopathic manipulation), psychological (a therapeutic conversation), and environmental (the clinical setting itself). Contrary to clinical lore, the percentage of patients who improve with a placebo can exceed 60%, and placebo responses can last as long as improvement with prescription drugs. Placebos are more effective when they closely follow effective medication, a result of classical conditioning and expectancy, and effective medication becomes less effective when it follows ineffective treatment.
Open-Label Placebos and Active Placebos
Open-label placebos—where patients are told they are receiving an inert substance—can still produce clinical improvement (Schaefer et al., 2018). This finding challenges the assumption that deception is necessary for placebo effects to occur. An active placebo adds an ingredient that produces an unrelated side effect and yields a therapeutic response in about 60% of people. For comparison, prescription drugs elicit a therapeutic response in 50% of patients in actual clinical practice and up to 70% in supervised drug trials.
Placebos have their most significant effects on symptoms or disorders that wax and wane over time, such as major depression and chronic pain. The placebo response to drug treatment of depression has increased by approximately 7% per decade (Advokat, Comaty, & Julien, 2019), a trend that has complicated the ability of new antidepressants to demonstrate superiority over placebo in clinical trials.
Mechanisms Behind the Placebo Response
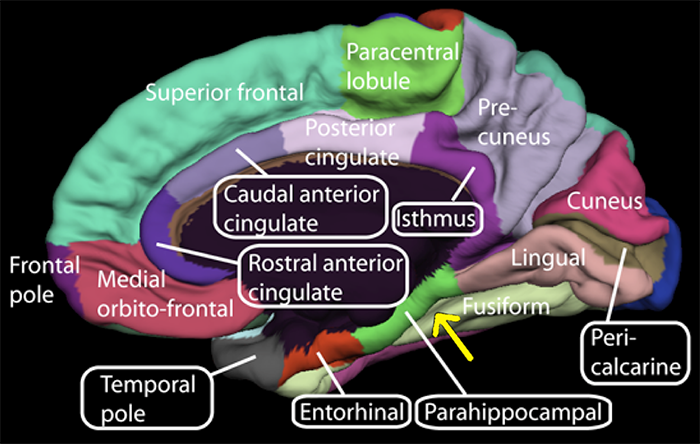
Placebos appear to trigger homeostatic responses through stimulus-response learning, expectancy, and the release of endogenous neurotransmitters like endorphins and adrenaline-like catecholamines. These mechanisms may mirror the therapeutic effects, time course, and duration of effect produced by prescription drugs. Petrovic and colleagues (2002) provided neuroimaging evidence by showing that both opioid analgesia and placebo analgesia increased activity in the rostral anterior cingulate cortex and the brainstem—suggesting shared neural pathways.
Wager et al. (2004) used functional MRI (fMRI)—a neuroimaging procedure that detects small changes in brain metabolism—to study the placebo effect. Volunteers exposed to painful shocks or heat reported less pain when told an "anti-pain cream" had been applied to their arms. The fMRI revealed that the placebo condition increased activity in the prefrontal cortex while decreasing activity in pain-processing regions of the thalamus, somatosensory cortex, and cerebral cortex. The brain was literally dampening its own pain signals based on expectation alone.
Kaptchuk et al. (2010) demonstrated the power of open-label placebos in a randomized controlled study of 80 Irritable Bowel Syndrome (IBS) patients. Fifty-nine percent of patients told they would receive inert pills—and that "placebo pills have been shown in rigorous clinical testing to produce significant mind-body self-healing processes"—improved, compared to only 35% in a no-treatment control group. Additionally, right parahippocampal gyrus (r-PHG) connectivity measured via fMRI predicted placebo-mediated analgesia in patients with chronic knee osteoarthritis (Tétreault et al., 2016).
Placebos are inert interventions that produce real, measurable clinical responses through mechanisms including classical conditioning, expectancy, and endogenous neurotransmitter release. Open-label placebos can be effective even when patients know they are receiving a placebo. Active placebos produce therapeutic responses in about 60% of people, comparable to prescription drug response rates.
Comprehension Questions
- Why is the key muscle hypothesis invalid, and what are the clinical implications of this finding?
- Explain why hand-warming biofeedback training at one digit may not generalize to other digits.
- What evidence supports the claim that placebos produce real physiological changes, not just subjective reports?
- How might the placebo effect influence the outcomes of biofeedback treatment, and what are the ethical implications?
Inter-Organ Communication: When Organs Talk
This section introduces a rapidly emerging field that reframes how we understand systemic health and disease. For biofeedback practitioners, inter-organ communication provides a physiological rationale for why training a single organ system—such as the heart through HRV biofeedback—can produce benefits that cascade throughout the body. A comprehensive review by Ainsworth (2026) describes how the body's organs are constantly exchanging signals in ways that extend far beyond the classical nervous and endocrine pathways.
Until recently, the body's internal coordination was understood almost entirely through two channels: the nervous system and the endocrine system. The emerging field of inter-organ communication reveals a far richer picture. Virtually every organ and tissue participates as both sender and receiver in an ongoing, body-wide dialogue mediated by hormones, metabolites, nerve signals, myokines (signaling molecules released by contracting skeletal muscle), adipokines (signaling molecules secreted by fat tissue), and a recently discovered class of membrane-bound packages called extracellular vesicles (EVs). These EVs range from large vesicles bearing intact mitochondria to tiny exosomes (30–150 nm in diameter) that carry RNA, proteins, and lipids between organs.
Several findings from this field are especially relevant to psychophysiology and biofeedback. First, bone is now recognized as a dynamic endocrine organ that produces osteocalcin, a hormone influencing metabolism, fertility, and even brain function by reducing anxiety. Second, skeletal muscle communicates with the brain, liver, and other organs through myokines released during contraction, which helps explain the well-documented systemic benefits of exercise. Third, the hypothalamus functions not only as a homeostatic regulator but as a longevity controller: stimulation of a specific subset of hypothalamic neurons in old mice extended their lifespan, the first mammalian demonstration that manipulating specific neurons can delay ageing. Researcher Shin-ichiro Imai has proposed a therapeutic concept called multi-organ communication management, which envisions simultaneous interventions to strengthen the multiple brain-organ conversations that deteriorate with age.
The cardiovascular system provides a striking example of pathological inter-organ crosstalk. When the heart is damaged, it releases EVs carrying harmful microRNAs—small molecules that alter gene expression—to the kidneys, contributing to cardiorenal syndrome. Similarly, fat tissue in obese individuals releases EVs that promote inflammation and fibrosis in the liver, driving metabolic liver disease. These findings illustrate that organs do not fail in isolation; dysfunction in one organ actively undermines others through pathological signaling.
A key factor in biological ageing is the accumulation of senescent cells—cells that have stopped dividing but release pro-inflammatory factors collectively known as the senescence-associated secretory phenotype (SASP). Among the SASP components are EVs that spread inflammation and damage throughout the body, probably contributing to the multimorbidity of the elderly, the clinical observation that older people typically suffer from several chronic conditions simultaneously.
Perhaps the most dramatic demonstration of inter-organ communication comes from regeneration research. Biologist Chunyi Li discovered that the annual regrowth of deer antlers releases signals that trigger a wider regenerative response throughout the animal, including near scar-free wound healing. Parallel findings in the axolotl show that limb amputation triggers a body-wide response, with cells in the opposite limb entering an alert state via a blood-borne signal. These discoveries suggest that restoring good communication—local, organ-wide, and body-wide—could eventually enhance the human body's capacity for tissue repair, a goal now being pursued through regenerative medicine.
Inter-organ communication is an emerging field revealing that every organ participates in a body-wide signaling network mediated by hormones, metabolites, myokines, adipokines, and extracellular vesicles. Bone, fat, muscle, the gut, and the brain all send and receive signals that coordinate health, regulate ageing, and influence disease. Pathological crosstalk—such as damaged hearts sending harmful microRNAs to the kidneys—shows that organs do not fail in isolation. For biofeedback practitioners, this framework explains why training one system (e.g., HRV) can produce cascading benefits throughout the body.
Comprehension Questions
- How does the concept of inter-organ communication expand the traditional view that bodily coordination occurs only through the nervous and endocrine systems?
- What role do extracellular vesicles play in both health and disease, and why are they considered a major discovery in physiology?
- Explain how the concept of multi-organ communication management might apply to a biofeedback practitioner designing interventions for an older adult with multiple chronic conditions.
Inter-Brain Synchrony: When Two Brains Connect
This section explores an emerging area of research that bridges neuroscience and the therapeutic relationship. Understanding inter-brain synchrony will give you a neurobiological framework for why the quality of your therapeutic presence matters as much as the specific techniques you employ. Inter-brain synchrony occurs when the neural activity of two individuals becomes aligned during social interaction. In therapeutic settings, this alignment is observed when a therapist and client engage in shared emotional and cognitive processes such as maintaining eye contact, mirroring facial expressions, and synchronizing speech rhythms (Meehan, 2025; Sened et al., 2022).
This mutual alignment of brain activity, often termed neural coupling, facilitates deeper interpersonal connection and more effective communication. Research suggests that synchrony strengthens emotional bonds and improves cognitive flexibility by facilitating better communication between brain regions associated with decision-making, problem-solving, and emotional processing. This may explain why clients who experience high levels of synchrony with their therapist often report deeper insights, improved emotional resilience, and greater capacity for behavioral change.

For therapists, these findings underscore the importance of actively fostering synchrony as a component of treatment. Beyond verbal communication, nonverbal cues—body language, tone of voice, and paced responsiveness—contribute significantly to inter-brain synchrony. Three relational skills are central to this process. Relational presence is the therapist's capacity to fully engage with the client, creating an environment of genuine connection and trust. Attunement is the process of accurately perceiving and sensitively responding to the client's emotional signals.
Co-regulation is the collaborative dynamic in which the therapist supports the client in managing emotional states, ultimately helping the client develop self-regulation skills. Clients who struggle with attachment issues, social difficulties, or trauma may particularly benefit from interventions that emphasize these relational processes. For biofeedback practitioners, this research suggests that the physiological training you provide is enhanced—and possibly mediated—by the quality of the interpersonal connection you establish with each client.
Inter-brain synchrony occurs when the neural activity of two individuals becomes aligned during social interaction. In therapeutic settings, this alignment through eye contact, expression mirroring, and speech synchronization facilitates deeper connection and lasting neurobiological change. Therapists can actively foster synchrony through relational presence, attunement, and co-regulation.
Psychophysiological Assessment: Building the Clinical Picture
This section covers the assessment process that translates the principles discussed throughout this unit into individualized treatment plans. You will learn about the components of a comprehensive assessment and how the psychophysiological stress profile (PSP) reveals each client's unique response patterns. Client assessment is a collaborative process that begins with an orientation to biofeedback, client symptom recording, a psychophysiological history, referral to physicians to investigate related medical complaints, and a psychophysiological stress profile (Moss & Shaffer, 2022).

Psychophysiological Stress Profile Overview
A psychophysiological stress profile (PSP) monitors multiple physiological variables under standardized resting, stress, and recovery conditions. Clinicians use the PSP to detect three key patterns: chronic problems that depress or elevate physiological measures at baseline, overactivation in response to stressors, and difficulty recovering from stress trials. Together, these patterns provide a comprehensive picture of the client's psychophysiological functioning and identify which biofeedback modalities will best help them achieve their training goals.
In a typical PSP, a practitioner monitors hand temperature (TEMP), heart rate (HR) and heart rate variability (HRV), respiration (RESP), skeletal muscle electrical activity (SEMG), skin conductance (SCL), and possibly brain electrical activity (EEG). The client's presenting complaints determine sensor placement—for example, a clinician treating tension-type headaches may use left and right SEMG channels to record cervical paraspinal muscle activity.
PSP Structure
A typical PSP includes a 5-minute baseline (no feedback or breathing instructions), a 3-minute relaxation period (with relaxation instructions), a 3-minute stress trial (such as visualizing a recent stressful event), a 3-minute recovery period, a second 3-minute stress trial, and a final 3-minute recovery period. This alternating structure allows the clinician to observe how the client's physiology responds to challenge and how efficiently it returns to baseline—information that directly shapes the treatment plan.
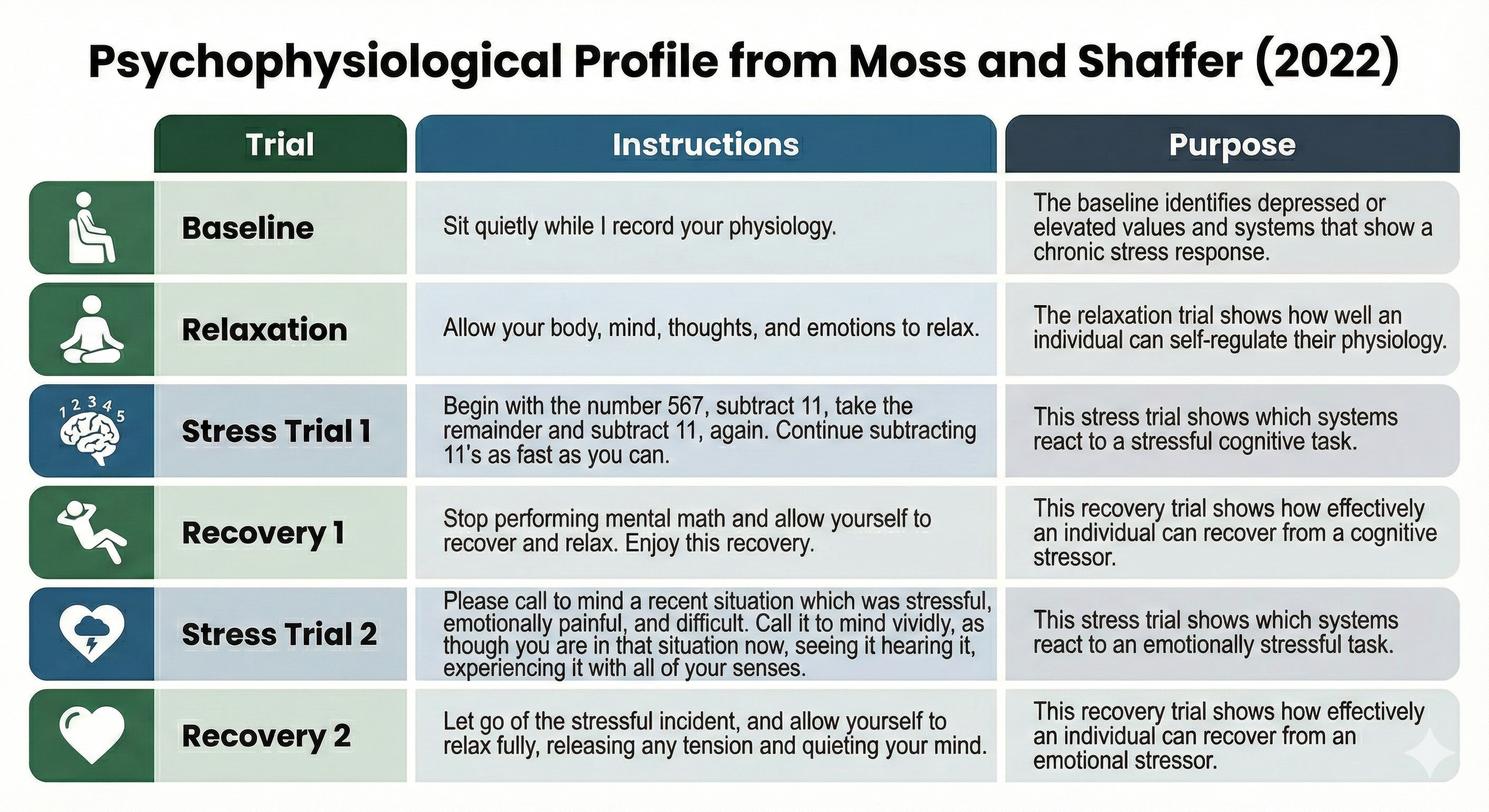
How the PSP Guides Treatment Planning
The PSP provides four types of actionable information. First, the baseline reveals which values are depressed or elevated, identifying systems dysregulated in everyday life. Second, the relaxation trial evaluates a client's ability to self-regulate their physiology. Third, the stress trials show which systems over- or under-react to cognitive and emotional challenges. Fourth, the recovery trials assess the client's ability to restore relaxed physiology following stressors.
When the psychophysiological history and PSP identify a distinct stereotypy, the practitioner can target the specific systems contributing to the client's symptoms. For example, if a client's upper back and neck muscles are excessively tense during baseline, fail to loosen during relaxation, tense further during both stressors, and do not recover afterward, the practitioner might recommend targeted muscle relaxation training. This individualized approach—driven by data rather than a one-size-fits-all manual—is what distinguishes evidence-based biofeedback practice.
A psychophysiological stress profile (PSP) monitors multiple physiological variables under standardized conditions. It reveals chronic dysregulation, overactivation to stressors, and impaired recovery. The PSP enables individualized treatment planning by identifying each client's unique response stereotypy, replacing one-size-fits-all protocols with targeted interventions.
Comprehension Questions
- How does inter-brain synchrony relate to the therapeutic relationship, and what can therapists do to foster it?
- What are the four main types of information a PSP reveals about a client's psychophysiology?
- Explain how a clinician would use PSP results to create an individualized treatment plan for a client with tension-type headaches.
Cutting Edge Topics
Inter-Brain Plasticity and Psychotherapy
One of the most exciting frontiers in psychotherapy research is inter-brain plasticity—the capacity of the brain to adapt and change based on repeated neural synchrony with another person. Sened, Zilcha-Mano, and Shamay-Tsoory (2022) proposed an integrative model suggesting that the therapeutic relationship itself can drive neuroplastic changes in the client's brain. Through repeated sessions of attuned interaction, a therapist's neural patterns may gradually shape the client's neural architecture, particularly in regions associated with emotional regulation, social cognition, and attachment.
Meehan (2025) highlighted how this research bridges relational psychotherapy and neuroscience. The implications are profound: therapy may not just change how a client thinks or feels but may literally rewire neural circuits through repeated interpersonal neural synchrony. This challenges the traditional view that therapeutic change is purely cognitive or behavioral and suggests that the quality of the therapeutic relationship has a direct neurobiological impact.
The Cholinergic Anti-Inflammatory Pathway
Tracey (2007) described the cholinergic anti-inflammatory pathway, a mechanism by which the vagus nerve modulates the immune system's inflammatory response. When vagal afferents detect peripheral inflammation, signals travel to the brainstem, which activates vagal efferents that release acetylcholine at the celiac ganglion. This process inhibits the release of pro-inflammatory cytokines like tumor necrosis factor (TNF), interleukin-1, and interleukin-6.
This pathway has significant implications for HRV biofeedback. By increasing vagal tone through resonance frequency breathing, clinicians may be able to modulate inflammatory processes that contribute to conditions ranging from rheumatoid arthritis to cardiovascular disease. Gevirtz (2013) proposed this as one of the key mechanisms by which HRV biofeedback achieves clinical improvements.
Open-Label Placebos and the Mind-Body Connection
The discovery that open-label placebos can produce clinical improvement even when patients know they are receiving an inert substance challenges fundamental assumptions about how healing works. Kaptchuk et al. (2010) demonstrated this with IBS patients, and Schaefer, Sahin, and Berstecher (2018) extended these findings to allergic rhinitis. These studies suggest that the mind-body healing response may be more robust and less dependent on deception than previously believed.
For biofeedback practitioners, this research reinforces the importance of the therapeutic context. The clinical environment, the practitioner's confidence, and the patient's engagement in the process all activate neurobiological pathways that contribute to healing, independent of the specific intervention being used.
Essential Skills
1. Interview a client about the history and prior treatment of the presenting complaints, the individual's life situation, including stressors and resources, and her understanding of the cause(s) and consequences of these symptoms.
2. Explain the purpose and procedures of a psychophysiological profile to a client.
3. Administer a psychophysiological profile to a client utilizing several modalities and containing pre-baseline, stressor, recovery, and relaxation conditions. Explain your selection of the modalities and placements used.
4. Demonstrate how to detect and remove artifacts from the raw signals that were monitored.
5. Evaluate and summarize the findings of the psychophysiological profile, relate them to the client's presenting complaints, and identify training goals based on these data.
6. Explain the results from the psychophysiological profile and training goals to your client.
7. Develop a treatment plan for your client based on the interview and psychophysiological profile.
8. Explain the treatment plan to your client.
Assignment
Now that you have completed this unit, how might it change how you explain psychophysiological concepts like the autonomic nervous system to your clients?
Glossary
A-bar: Wenger's shorthand for the ratio of sympathetic to parasympathetic excitation. Patients with low A-bar scores are sympathetic-dominant, and those with high A-bar scores are parasympathetic dominant.
accentuated antagonism: the parasympathetic nervous system's ability to directly oppose sympathetic action, such as slowing the heart by 20 or 30 beats.
activation: Duffy's term for arousal originated with Cannon's fight-or-flight response.
active placebo: a placebo combined with an additive to produce a side effect that can elicit a therapeutic response rate in about 60% of patients.
adipokines: signaling molecules secreted by adipose (fat) tissue that influence distant organs. Leptin is one of the best-characterized adipokines (Ainsworth, 2026).
allostasis: the maintenance of stability through change by mechanisms that anticipate challenges and adapt through behavioral and physiological change.
allostatic load model: McEwen and Seeman's hypothesis that biological responses to stress can harm the body when stressors are acute or repeatedly occur.
attunement: the process by which a therapist accurately perceives and responds to a client's emotional state.
autonomic balance: Wenger's concept of a ratio of sympathetic to parasympathetic excitation.
autonomic nervous system: the subdivision of the peripheral nervous system that includes enteric, parasympathetic, and sympathetic.
boundary model: the position that setpoints are not rigid and that physiological processes are maintained within acceptable ranges.
cardiorenal syndrome: a condition in which dysfunction of the heart leads to kidney damage, now understood to involve pathological signaling via extracellular vesicles carrying harmful microRNAs (Ainsworth, 2026).
central nervous system: the division of the nervous system that includes the brain, spinal cord, and retina.
co-regulation: the process through which one person helps another regulate their emotional state through interaction and connection.
defensive response: a very slowly habituating response pattern that limits harm from intense stimulation. This pattern includes reduced sensory sensitivity, a tendency to move away from the stimulus, heart rate increase, and both peripheral and cephalic vasoconstriction.
diathesis: vulnerability. For example, a genetic predisposition to gain weight.
directional fractionation: Lacey's concept of a complex pattern of physiological response to a stimulus where some indices increase and others decrease.
emotional response specificity: the hypothesis that primary emotions are associated with unique physiological changes.
endocrine organ: an organ that produces and secretes hormones into the bloodstream. Bone, fat, and muscle are now recognized as endocrine organs in addition to traditional glands (Ainsworth, 2026).
endocrine system: the collection of glands and organs that produce hormones to regulate metabolism, growth, reproduction, and other body functions (Ainsworth, 2026).
enteric division: a subdivision of the autonomic nervous system that regulates the gut and is innervated by sympathetic and parasympathetic branches.
epinephrine: an adrenal medullary hormone that increases muscle blood flow, converts stored nutrients into glucose for use by skeletal muscles, and initiates cardiac muscle contraction when it binds to β1 receptors.
exosomes: small extracellular vesicles, typically 30 to 150 nanometers in diameter, that carry fragments of RNA, proteins, and lipids between cells as part of inter-organ communication (Ainsworth, 2026).
extracellular vesicles (EVs): membrane-bound packages of molecular cargo (proteins, RNA, lipids, and sometimes mitochondria) released by cells and transported through the bloodstream to influence distant organs (Ainsworth, 2026).
fibrosis: the formation of excess fibrous connective tissue in an organ or tissue, typically as part of a reparative or reactive process. In the context of inter-organ communication, fibrosis in the liver can be driven by extracellular vesicles from adipose tissue (Ainsworth, 2026).
freeze response: immobilization when facing a threat you cannot fight or flee.
functional MRI (fMRI): magnetic resonance imaging procedure that can detect small changes in brain metabolism.
gene expression: the process by which information from a gene is used to synthesize functional products such as proteins. MicroRNAs transported by extracellular vesicles can alter gene expression in distant organs (Ainsworth, 2026).
habituation: the weakening or disappearance of a response to a constant stimulus.
heart rate variability (HRV): the organized fluctuation of time intervals between successive heartbeats defined as interbeat intervals.
homeostasis: the state of dynamic constancy achieved by stabilizing conditions about a setpoint, whose value may change over time.
homeostat: device that maintains homeostasis. For example, the hypothalamus.
hypothalamus: the forebrain structure below the thalamus that dynamically maintains homeostasis controlling the autonomic nervous system, endocrine system, survival behaviors, and interconnections with the immune system.
hypothalamic neurons: nerve cells in the hypothalamus that regulate metabolism, ageing, and inter-organ communication. Stimulation of a specific subset in old mice extended lifespan (Ainsworth, 2026).
idiographic approach: a research strategy that emphasizes individual differences.
inter-brain plasticity: the capacity of the brain to adapt and change based on repeated neural synchrony with another person.
inter-brain synchrony: the alignment of neural activity between two individuals during social or therapeutic interactions.
inter-organ communication: the exchange of signals between different organs and tissues in the body, mediated by hormones, metabolites, myokines, adipokines, extracellular vesicles, nerves, and other pathways (Ainsworth, 2026).
Irritable Bowel Syndrome (IBS): a functional gastrointestinal disorder that can respond to placebo treatment.
key muscle hypothesis: the discredited proposition that a single muscle indexes activity in other muscle groups.
law of initial values: Wilder's proposition that the size of our response to a stimulus depends on a physiological variable's starting value. This principle has only been demonstrated for heart rate, respiration rate, and skin resistance.
mass activation: the simultaneous stimulation of adjacent ganglia (cell bodies) in the sympathetic chain during emergencies allows the sympathetic nervous system to produce many coordinated changes at once. For example, increased heart rate, respiration rate, and sweat gland activity.
medulla: a brainstem structure that regulates blood pressure, defecation, heart rate, respiration, vomiting, the autonomic nervous system, and distributes signals between the brain and spinal cord.
metabolic liver disease: liver disease caused by metabolic dysfunction, previously termed non-alcoholic fatty liver disease (NAFLD), now understood to involve inter-organ signaling from adipose tissue via extracellular vesicles (Ainsworth, 2026).
metabolites: small molecules produced during metabolism that serve as substrates, intermediates, or products of biochemical reactions. Some metabolites function as inter-organ signals (Ainsworth, 2026).
microRNAs: small non-coding RNA molecules that regulate gene expression by binding to messenger RNA. MicroRNAs carried by extracellular vesicles can alter cell behavior in distant organs (Ainsworth, 2026).
mitochondria: organelles within cells that produce energy through oxidative phosphorylation. Large extracellular vesicles can transport intact mitochondria between cells as part of inter-organ communication (Ainsworth, 2026).
multi-organ communication management: a therapeutic concept proposed by Shin-ichiro Imai involving simultaneous interventions to strengthen multiple brain-organ communication pathways to slow ageing (Ainsworth, 2026).
multimorbidity: the co-occurrence of two or more chronic diseases in the same individual, particularly common in the elderly. EV-mediated spread of senescence signals may contribute to multimorbidity (Ainsworth, 2026).
myokines: signaling molecules produced and released by skeletal muscle during contraction that act on distant organs, including the brain and liver (Ainsworth, 2026).
neural coupling: the synchronization of brain activity between two individuals during social or therapeutic interactions.
norepinephrine: an adrenal medullary hormone that increases muscle blood flow and converts stored nutrients into glucose for skeletal muscles.
open-label placebo: an inert treatment disclosed as a placebo to patients.
orienting response: Pavlov's "What is it?" reaction to stimuli like the sound of a vase crashing that includes increased sensory sensitivity, head (and ear) turning toward the stimulus, increased muscle tone (reduced movement), EEG desynchrony, peripheral constriction and cephalic vasodilation, a rise in skin conductance, heart rate slowing, and slower, deeper breathing.
osteocalcin: a hormone produced by bone that influences metabolism, fertility, and brain function, including anxiety reduction. Its discovery helped establish bone as an endocrine organ (Ainsworth, 2026).
parasympathetic division: the autonomic nervous system subdivision that regulates activities that increase the body's energy reserves, including salivation, gastric (stomach) and intestinal motility, gastric juice secretion, and increased blood flow to the gastrointestinal system.
parasympathetic dominance: Wenger's concept of greater parasympathetic activation than sympathetic activation.
peripheral nervous system: nervous system subdivision that includes autonomic and somatic branches.
phasic: a brief change in physiological activity in response to a discrete stimulus. For example, a single skin potential response in reaction to a sudden tone.
placebo: an inert intervention that can produce a therapeutic response rate in about 30% of patients.
Polyvagal Theory: the theory that the unmyelinated vagus (dorsal vagus complex) and newer myelinated vagus (ventral vagal complex) mediate competing adaptive responses.
psychophysiological principle: Green, Green, and Walters' concept that there is a bidirectional relationship between physiological and psychological functioning. For example, facial muscle contraction can influence emotion, and emotion can influence facial muscle contraction.
Psychophysiological Stress Profile (PSP): structured assessment procedure that monitors multiple physiological variables under standardized resting, stress, and recovery conditions.
relational presence: a therapist's ability to be fully engaged and attuned to a client in a way that fosters connection and trust.
regenerative medicine: a branch of medicine focused on repairing or replacing damaged tissues and organs, increasingly informed by inter-organ communication research and principles observed in regenerating animals (Ainsworth, 2026).
response stereotypy: a consistent pattern of physiological responses when an individual encounters stimuli with the same intensity and elicit similar emotions. For example, a patient may raise her heart rate and blood pressure when delivering a report during a business meeting or completing an assignment under time pressure.
resting baseline: a tonic measure of psychophysiological activity (e.g., temperature) without breathing or relaxation instructions and feedback.
senescence-associated secretory phenotype (SASP): the collection of pro-inflammatory cytokines, growth factors, and extracellular vesicles released by senescent cells that promote inflammation and damage in surrounding tissues (Ainsworth, 2026).
senescent cells: cells that have irreversibly stopped dividing but continue to secrete inflammatory and damaging molecules, contributing to tissue deterioration and age-related disease (Ainsworth, 2026).
situational specificity: the occurrence of a physiological response in specific situations. For example, blood pressure increase during a dental examination.
somatic nervous system: the peripheral nervous system subdivision that receives external sensory and somatosensory information and controls skeletal muscle contraction.
spontaneous responses: physiological changes in the absence of detectable stimuli. For example, skin conductance responses when no tones are presented to a subject.
stimulus-response specificity: specific stimuli elicit a distinctive response pattern in most individuals instead of simply altering activation. For example, subjects may increase their skeletal muscle tone when challenged to compete.
sympathetic dominance: Wenger's concept of greater sympathetic activation than parasympathetic activation.
sympathetic nervous system: the autonomic nervous system branch that regulates activities that expend stored energy, such as when we are excited.
sympathicotonics: Wenger's term for sympathetic-dominant individuals who they hypothesized to suffer an elevated incidence of neurotic, psychotic, psychosomatic, and medical disorders.
therapeutic synchrony: the alignment of emotional and cognitive processes between therapist and client that enhances the therapeutic process.
thermistor: a temperature sensor used in biofeedback to measure skin temperature at specific sites.
tonic: a background level of physiological activity. For example, a 5-minute average of hand temperature.
vagal withdrawal: the inhibition of the myelinated vagus, often by daily stressors.
References
Advokat, C. D., Comaty, J. E., & Julien, R. M. (2019). Julien's primer of drug action (14th ed.). Worth Publishers.
Ainsworth, C. (2026, February 2). The secret signals our organs send to repair tissues and slow ageing. New Scientist. https://www.newscientist.com
Andreassi, J. L. (2007). Psychophysiology: Human behavior and physiological response (5th ed.). Lawrence Erlbaum Associates, Publishers.
Begley, S. (2005). How mirror neurons help us empathize, really feel others' pain. The Wall Street Journal, B1.
Berntson, G. G., Cacioppo, J. T., & Quigley, K. S. (1993). Cardiac psychophysiology and autonomic space in humans: Empirical perspectives and conceptual implications. Psychological Bulletin, 114, 296-322. https://doi.org/10.1037/0033-2909.114.2.296
Berntson, G. G., Uchino, B. N., & Cacioppo, J. T. (1994). Origins of baseline variance and the Law of Initial Values. Psychophysiology, 31(2), 204-210. https://doi.org/10.1111/j.1469-8986.1994.tb01042.x
Brannon, L., Updegraff, J. A., & Feist, J. (2022). Health psychology: An introduction to behavior and health (10th ed.). Wadsworth.
Breedlove, S. M., & Watson, N. V. (2020). Behavioral neuroscience (9th ed.). Sinauer Associates, Inc.
Cacioppo, J. T., Tassinary, L. G., & Berntson, G. G. (Eds.). (2007). Handbook of psychophysiology (3rd ed.). Cambridge University Press.
Coull, J. A., Beggs, S., Boudreau, D., Boivin, D., Tsuda, M., Inoue, K., Gravel, C., Salter, M. W., & De Koninck, Y. (2005). BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature, 438, 1017-1021. https://doi.org/10.1038/nature04223
Dhar, A. K., Lambert, G. W., & Barton, D. A. (2016). Depression and cardiovascular disease: Psychobiological mechanisms. In M. E. Alvarenga & D. Byrne (Eds.), Handbook of psychocardiology. Springer Singapore.
Fox, S. I., & Rompolski, K. (2022). Human physiology (16th ed.). McGraw-Hill.
Gevirtz, R. (2013). The nerve of that disease: The vagus nerve and cardiac rehabilitation. Biofeedback, 41, 32-38. https://doi.org/10.5298/1081-5937-41.1.01
Green, E., Green, A. M., & Walters, E. D. (1970). Voluntary control of internal states: Psychological and physiological. Journal of Transpersonal Psychology, 2, 1-26.
Gurung, R. A. R. (2018). Health psychology: Well-being in a diverse world (4th ed.). Thompson Wadsworth.
Hugdahl, K. (1995). Psychophysiology: The mind-body perspective. Harvard University Press.
Kaptchuk, T. J., Friedlander, E., Kelley, J. M., Sanchez, M. N., Kokkotou, E., Singer, J. P., Kowalczykowski, M., Miller, F. G., Kirsch, I., & Lembo, A. J. (2010). Placebos without deception: A randomized controlled trial in Irritable Bowel Syndrome. PLoS ONE, 5(12), Article e15591. https://doi.org/10.1371/journal.pone.0015591
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. John Wiley & Sons, Ltd.
Khazan, I. Z. (2019). A guide to normal values for biofeedback. In D. Moss & F. Shaffer (Eds.), Physiological recording technology and applications in biofeedback and neurofeedback (pp. 2-6). Association for Applied Psychophysiology and Biofeedback.
Kingsley, R. E. (2000). Concise textbook of neuroscience (2nd ed.). Lippincott Williams & Wilkins.
LeDoux, J. (2002). Synaptic self. Viking Penguin.
Malta, L. S., Blanchard, E. B., Freidenberg, B. M., Galovski, T. E., Karl, A., & Holzapfel, S. R. (2001). Psychophysiological reactivity of aggressive drivers: An exploratory study. Applied Psychophysiology and Biofeedback, 26(2), 95-116.
Meehan, Z. M. (2025). 5-min science: Inter-brain plasticity can enhance psychotherapy. https://www.biosourcesoftware.com/post/5-min-science-inter-brain-plasticity-can-enhance-psychotherapy
Moss, D., & Shaffer, F. (2022). A primer of biofeedback. Association for Applied Psychophysiology and Biofeedback.
Nunan, D., Sandercock, G. R. H., & Brodie, D. A. (2010). A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing and Clinical Electrophysiology, 33(11), 1407-1417. https://doi.org/10.1111/j.1540-8159.2010.02841.x
Olshansky, B., Sabbah, H. N., Hauptman, P. J., & Colucci, W. S. (2008). Parasympathetic nervous system and heart failure: Pathophysiology and potential implications for therapy. Circulation, 118, 863-871. https://doi.org/10.1161/CIRCULATIONAHA.107.760405
Pennebaker, J. W., Kiecolt-Glaser, J. K., & Glaser, R. (1988). Disclosure of traumas and immune function: Health implications for psychotherapy. Journal of Consulting and Clinical Psychology, 56, 239-245. https://doi.org/10.1037//0022-006x.56.2.239
Petrovic, P., Kalso, E., Petersson, K. M., & Ingvar, M. (2002). Placebo and opioid analgesia: Imaging a shared neuronal network. Science, 295, 1737-1740. https://doi.org/10.1126/science.1067176
Pinel, P. J., & Barnes, S. (2017). Biopsychology (10th ed.). Pearson Education, Inc.
Poole, L., Dickens, C., & Steptoe, A. (2011). The puzzle of depression and acute coronary syndrome: Reviewing the role of acute inflammation. Journal of Psychosomatic Research, 71(2), 61-68. https://doi.org/10.1016/j.jpsychores.2010.12.009
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Rao, M., & Gershon, M. D. (2016). The bowel and beyond: The enteric nervous system in neurological disorders. Nature Reviews Gastroenterology & Hepatology, 13, 517-528. https://doi.org/10.1038/nrgastro.2016.107
Rizzolatti, G., & Sinigaglia, C. (2006). Mirrors in the brain. Oxford University Press.
Schaefer, M., Sahin, T., & Berstecher, B. (2018). Why do open-label placebos work? A randomized controlled trial of an open-label placebo induction with and without extended information about the placebo effect in allergic rhinitis. PLoS ONE, 13(3), Article e0192758. https://doi.org/10.1371/journal.pone.0192758
Schwartz, G. E., Weinberger, D. A., & Singer, J. A. (1981). Cardiovascular differentiation of happiness, sadness, anger, and fear following imagery and exercise. Psychosomatic Medicine, 43, 343-364. https://doi.org/10.1097/00006842-198108000-00007
Schwartz, M. S., & Andrasik, F. (Eds.). (2003). Biofeedback: A practitioner's guide (3rd ed.). The Guilford Press.
Schwartz, S. (2015). Viva vagus: Wandering nerve could lead to range of therapies. Science News, 188(11), 18.
Sened, H., Zilcha-Mano, S., & Shamay-Tsoory, S. (2022). Inter-brain plasticity as a biological mechanism of change in psychotherapy: A review and integrative model. Frontiers in Human Neuroscience, 16, Article 955238. https://doi.org/10.3389/fnhum.2022.955238
Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: An integrative review of the heart's anatomy and heart rate variability. Frontiers in Psychology, 5, Article 1040. https://doi.org/10.3389/fpsyg.2014.01040
Shaffer, F., Meehan, Z. M., & Zerr, C. L. (2020). A critical review of ultra-short-term heart rate variability norms research. Frontiers in Neuroscience, 14, Article 594880. https://doi.org/10.3389/fnins.2020.594880
Stern, R. M., Ray, W. J., & Quigley, K. S. (2001). Psychophysiological recording (2nd ed.). Oxford University Press.
Tétreault, P., Mansour, A., Vachon-Presseau, E., Schnitzer, T. J., Apkarian, A. V., & Baliki, M. N. (2016). Brain connectivity predicts placebo response across chronic pain trials. PLoS Biology, 14(10), Article e1002570. https://doi.org/10.1371/journal.pbio.1002570
Thompson, M. (2005). Intentions, empathy, and theory of mind: Implications for personality and psychotherapy. Presentation to the Annual Meeting of the American Association for the Advancement of Science (AAAS).
Tortora, G. J., & Derrickson, B. H. (2021). Principles of anatomy and physiology (16th ed.). John Wiley & Sons, Inc.
Tracey, K. J. (2007). Physiology and immunology of the cholinergic anti-inflammatory pathway. Journal of Clinical Investigation, 117(2), 289-296. https://doi.org/10.1172/JCI30555
White, C., & Lammy, D. (2004). Infrared hand temperature mapping [Abstract]. Applied Psychophysiology and Biofeedback, 29(4), 306.
Wickramasekera, I. A. (1988). Clinical behavioral medicine: Some concepts and procedures. Plenum Press.
Wilson, J. F. (2003). Biological foundations of human behavior. Thomson/Wadsworth.
Return to Top